1. Introduction
Breast cancer is the most common cancer among women in the United States and represents a significant public health burden [
1]. Globally, the burden of breast cancer is expected to rise substantially, with projections estimating a 38% increase in incidence and a 68% increase in annual mortality by 2050, according to the International Agency for Research on Cancer (IARC), a specialized agency of the World Health Organization (WHO) [
3]. The increased detection of early-stage breast cancer has resulted in a higher rate of breast-conserving surgeries followed by adjuvant radiotherapy (RT), now a standard component of multimodal treatment [
4,
5,
6,
7]. While advances in early detection and management have improved survival, treatment-related secondary malignancies have become increasingly recognized.
Although RT has significantly improved tumor control and survival outcomes, it also exposes adjacent thoracic structures to low dose ionizing radiation, an important and established factor in the development of second primary lung cancer (SPLC), especially among long-term survivors [
8,
9,
10,
11,
12,
13]. Previous studies have shown that breast cancer patients treated with RT may have up to double the risk of developing SPLC within ten years of treatment [
9,
10,
11,
12,
13,
14]. Additionally, recent evidence suggests that low-to-moderate radiation doses may be more carcinogenic than previously thought, and modern RT techniques have altered lung exposure patterns in clinically relevant ways. Specifically, intensity-modulated radiotherapy (IMRT) increases the volume of lung tissue exposed to low-dose radiation due to greater beam modulation, potentially elevating SPLC risk, whereas proton therapy reduces integral lung dose and may lower this risk, although long-term data remain limited [
15,
16,
17] . Consequently, studies with extended follow-up beyond 10 years are needed to better define SPLC risk associated with contemporary RT techniques.
Beyond biological and treatment-related factors, social determinants of health (SDOH), including socioeconomic status, insurance coverage, race/ethnicity, education, and neighborhood environment, are key drivers of cancer outcomes [
18]. Among breast cancer survivors, inequities in access to care, health behaviors such as smoking, and continuity of follow-up contribute to disparities in both primary outcomes and long-term risks, including secondary lung cancer [
19]. These factors may modify radiation-associated risk by shaping baseline susceptibility and post-treatment surveillance: in a large prospective cohort, ever-smokers had more than a threefold higher risk of second primary lung cancer than never-smokers (adjusted HR ~3.5), with risk increasing by ~24% per 10 pack-years, and nearly 80% of affected survivors did not meet current lung cancer screening criteria [
20]. Understanding how SDOH intersect with cancer therapy and survivorship is essential to contextualizing observed disparities in secondary lung cancer incidence.
Research examining racial and ethnic disparities in second primary lung cancer following radiation exposure remains limited, despite consistent evidence that race and ethnicity modify cancer incidence, treatment delivery, survivorship care, and outcomes across oncology. The role of marital status in SPLC is even less well characterized; however, prior cancer research suggests that marital status may modify access to social support, adherence to post-treatment surveillance, and timeliness of medical follow-up, thereby potentially influencing SPLC detection and survival rather than risk alone. Given these gaps, a clearer understanding of how race, ethnicity, and marital status act as modifiers of SPLC risk and outcomes after radiotherapy is critically needed [
21,
22].
This study addresses these gaps by quantifying the incidence and survival outcomes of SPLC among breast cancer survivors treated with radiotherapy, with a specific focus on racial and ethnic disparities and the modifying effect of marital status. Using population-based data from the Surveillance, Epidemiology, and End Results (SEER) database, this analysis provides contemporary estimates of SPLC risk in the setting of modern breast cancer management and highlights the importance of incorporating demographic and social determinants into survivorship planning and lung cancer screening strategies.
2. Methods
2.1. Data Source
Patient diagnosed with a SPLC, following prior diagnosis of breast cancer treated with radiation therapy, from January 1, 2000 to December 31,
2022 were collected from the Surveillance, Epidemiology, and End Results (SEER) (
www.seer.cancer.gov) using SEER* Stat software. We used the Incidence - SEER Research Data, 17 Registries, Nov 2023 Sub (2000-2022) - Linked to County Attributes - Time Dependent (1990-2022) Income/Rurality, 1969-2022 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, released April 2024, based on the November 2024 submission. Because SEER data are publicly available and de-identified, institutional review board (IRB) approval and informed consent were not required for this study.
2.2. Patient Selection
We included patients from the SEER database who met the following inclusion criteria: (1) diagnosed with primary breast cancer, using Site Recode ICD-O-3/WHO 2008 as “Breast” (ICD-O codes: 500-509); (2) received radiation therapy; (3) developed a SPLC (defined by SEER criteria for second primary malignancies (
https://training.seer.cancer.gov/arc_neoplasms/); (4) and had a minimum latency exclusion period of 2 months to avoid synchronous malignancies. Patients meeting the following criteria were excluded: prior cancer diagnoses, using the SEER filter for “First Primary Only” as Breast Cancer (Sequence Number = 0 or 1); incomplete follow-up or missing racial information. Race was determined based on the “Race record” variable, which included (white, black, American Indian, Asian or pacific islander). Ethnicity was determined based on “race and ethnicity” variable, which was classified into (Hispanic, Non-Hispanic).
2.3. Outcome Definition
The primary outcome was the development of secondary primary malignancies (SPMs), defined as: 1) A new malignancy diagnosed ≥2 months after the initial breast cancer diagnosis to exclude synchronous cancers. 2) SPMs were identified based on SEER definitions of primary tumor sites and behavior codes, excluding recurrences and metastases. Patients were followed until death or end of follow-up period.
2.4. Covariates
We collected clinicopathological data for each patient, including the following variables: Patient ID, age, gender, race, ethnicity, marital-status, histological type, radiation therapy types, chemotherapy, and survival duration in months, tumor size, stage at diagnosis of primary tumor, metastasis at diagnosis, and laterality.
2.5. Statistical Analysis
The Multiple Primary Standardized Incidence Ratio (MP-SIR) session in SEER*Stat software version 8.4.4 and SPSS v.27 was used for all analyses. Standardized Incidence Ratios (SIRs) were calculated as the ratio of observed SPM cases in the study cohort to the expected cases in the general population. Expected cases were estimated based on age-, sex-, race-, and calendar year-adjusted incidence rates from the SEER reference population. Formula: SIR=Observed Cases / Expected Cases. 95% Confidence Intervals (CIs): Poisson distribution methods were used to compute confidence intervals for statistical significance. Survival analysis was performed, where OS was estimated using Kaplan-Meier survival analysis. Survival differences among patient groups were assessed using log-rank tests. To account for potential confounding factors, multivariable Cox proportional hazards regression models were used. A p-value of <0.05 was considered significant. All statistical analyses were conducted using IBM SPSS Statistics version 27.0. For subgroup analysis, SIRs were further stratified by race, ethnicity, and marital status.
3. Results
3.1. Cohort Profile
This analysis included 6,674 breast cancer survivors who received radiotherapy between 2000 and 2022 and were later diagnosed with second primary lung cancer (SPLC). On average, SPLC developed 7.01 years after the initial breast cancer diagnosis (SD 5.00), with latency ranging from 0 to 22 years. At diagnosis, the average age was 71.17 years (SD 9.90), and patients’ ages ranged from 32 to 92. Most of the cohort was female (99.6%). In terms of race, 85.4% of the patients were White (n = 5,700), followed by 9.1% Black (n = 605), 5.1% Asian or Pacific Islander (n = 340), and 0.4% American Indian or Alaska Native (n = 29). Most patients (93.8%) were non-Hispanic, and 43.4% were married at the time they were first diagnosed with breast cancer. The location of the original breast tumor was almost evenly split, with 50.7% on the left side and 49.1% on the right. However, when SPLC developed, it occurred more often in the right lung (54.3%) than in the left (40.1%). The most common radiation (RA) type was beam radiation (n=6256), accounting for (94.3%) of the total sample, while radioisotopes were the least common, with only four cases in total. (
Table 1).
3.2. Histopathology
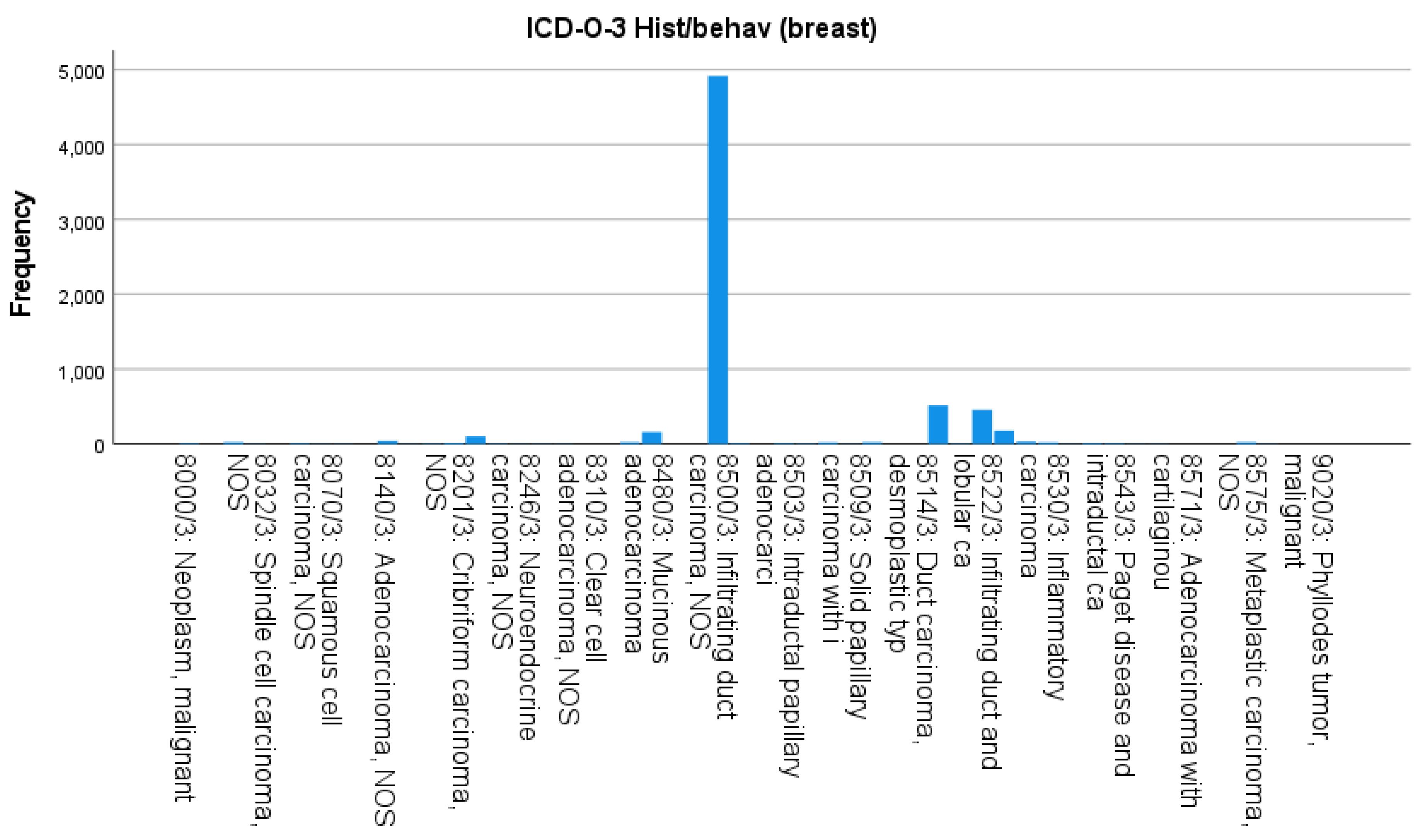
The histopathological types of primary breast cancer in the cohort varied, with the most common being infiltrating duct carcinoma, not otherwise specified (NOS; ICD-O-3 8500/3), which accounted for 74.6% of cases (n= 4,980). Other frequently observed subtypes included mixed infiltrating duct and lobular carcinoma (8522/3) at 8.1%, and solid papillary carcinoma with intraductal features (8523/3) at 6.2%. Each of the remaining subtypes made up less than 5% of the total cases (
Figure 1).
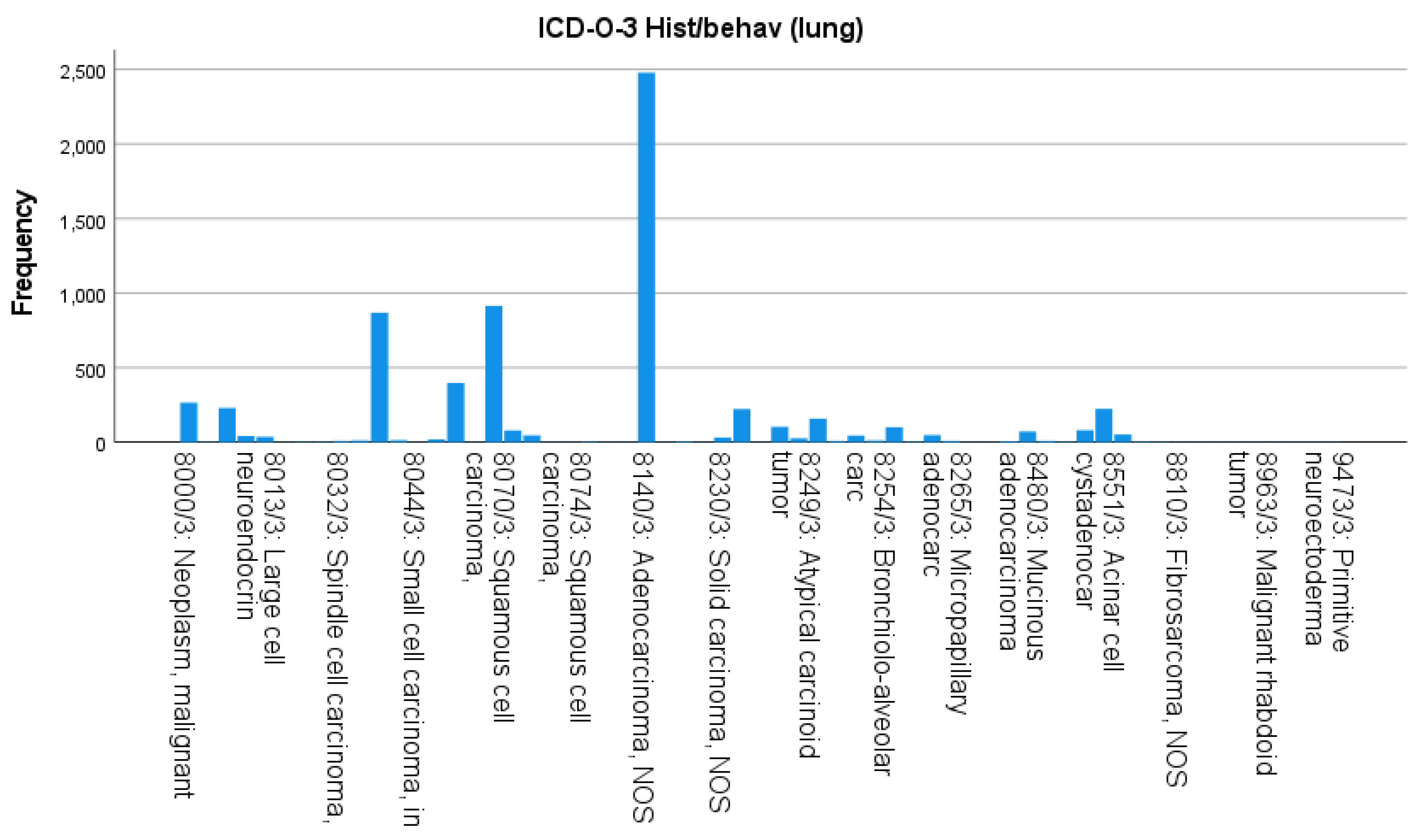
In terms of SPLC histology, adenocarcinoma NOS (8140/3) was the most diagnosed type, accounting for 37.5% (n = 2,500). This was followed by squamous-cell carcinoma NOS (8070/3) at 13.9% (n = 930), combined small-cell carcinoma variants (8044/3 and 8041/3) at 19.3% (n = 1,288), solid carcinoma NOS (8230/3) at 4.0% (n = 268), and atypical carcinoid tumor (8249/3) at 3.4% (n = 225). All remaining subtypes together represented 21.9% of the SPLC cases (
Figure 2).
3.3. Standardized Incidence Ratios (SIRs)
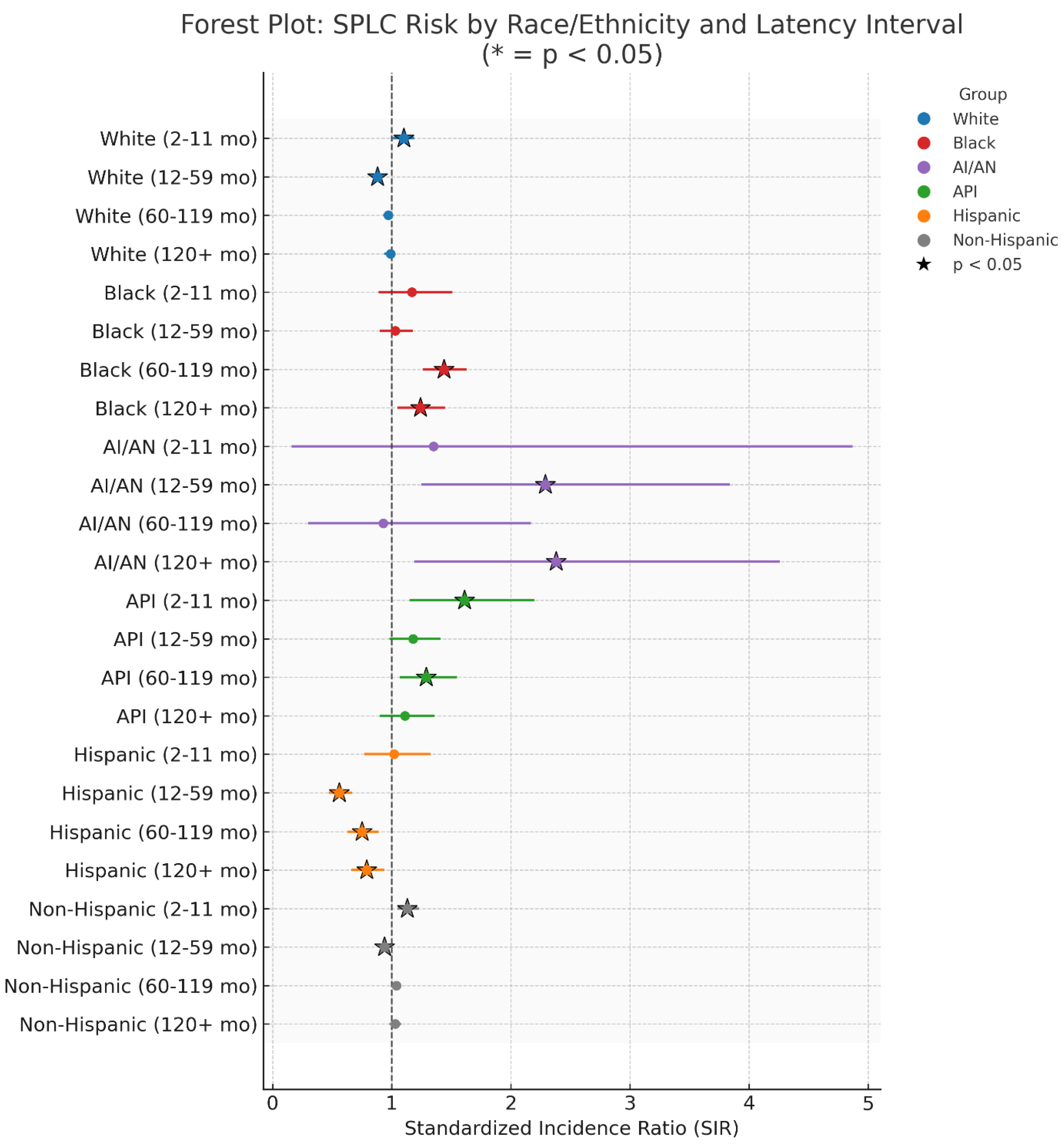
SIRs varied based on race and latency period. In the early phase (2–11 months), elevated SIRs were seen in Whites (1.11; 95% CI: 1.01–1.19), Blacks (1.47; 1.09–1.51), Asian/Pacific Islanders (1.61; 1.15–2.22), and American Indian/Alaska Natives (1.35; 0.16–4.87), though the latter was not statistically significant. Among White patients, risk decreased in the 12–59 month window (0.88; 0.80–0.92) and overall (0.96; 0.93–0.98). In contrast, Black patients experienced elevated risk across later periods—60–119 months (1.44; 1.26–1.63), ≥120 months (1.24; 1.05–1.45), and overall (1.21; 1.12–1.31). Asian/Pacific Islanders showed a consistently elevated overall risk (1.23; 1.11–1.36). Meanwhile, American Indian/Alaska Natives had significantly high SIRs at 12–59 months (2.29; 1.32–3.74), ≥120 months (2.38; 1.29–4.38), and overall (1.82; 1.24–2.57) (
Table 3,
Figure 8,
Figure 9).
Table 2.
Overall and subgroup survival following second primary lung cancer.
Table 2.
Overall and subgroup survival following second primary lung cancer.
| Characteristic |
Mean Age of Survival |
Confidence Interval (95%) |
5 Year Survival |
p-Value |
| Race |
| Ameri |
66.165 |
38.89-93.439 |
32.5% |
0.002 |
| Asian |
68.819 |
56.761-80.877 |
32.2% |
0.002 |
| Black |
54.391 |
45.667-63.114 |
25.6% |
0.002 |
| White |
54.943 |
52.3-57.586 |
28% |
0.002 |
| Marital Status |
| unmarried |
48.638 |
45.702-51.575 |
25% |
0.000 |
| married |
64.306 |
60.255-68.357 |
31.80% |
0.000 |
| Ethnicity |
| Hispanic |
65.480 |
55.085-75.876 |
37.40% |
0.005 |
| Non-Hisp |
54.969 |
52.436-57.503 |
27% |
0.005 |
Table 3.
Standardised incidence ratios of second primary lung cancer by race and latency interval.
Table 3.
Standardised incidence ratios of second primary lung cancer by race and latency interval.
| Among Races |
|---|
| Duration |
Observed |
Expected |
SIR |
CI |
| White |
| 2-11 Months |
579 |
527.37 |
1.1 # |
1.01-1.19 |
| 12-59 Months |
1,985 |
2,243.39 |
0.88 # |
0.85-0.92 |
| 60-119 Months |
1,957 |
2,018.48 |
0.97 |
0.93-1.01 |
| 120+ Months |
1,732 |
1,756.82 |
0.99 |
0.94-1.03 |
| Total |
6,253 |
6,546 |
0.96 # |
0.93-0.98 |
| Black |
| 2-11 Months |
59 |
50.36 |
1.17 |
0.89-1.51 |
| 12-59 Months |
207 |
200.81 |
1.03 |
0.9-1.18 |
| 60-119 Months |
235 |
163.44 |
1.44 # |
1.26-1.63 |
| 120+ Months |
155 |
125.5 |
1.24 # |
1.05-1.45 |
| Total |
656 |
540.11 |
1.21 # |
1.12-1.31 |
| American Indian/Alaska Native |
| 2-11 Months |
2 |
1.48 |
1.35 |
0.16-4.87 |
| 12-59 Months |
14 |
6.12 |
2.29 # |
1.25-3.84 |
| 60-119 Months |
5 |
5.39 |
0.93 |
0.3-2.17 |
| 120+ Months |
11 |
4.63 |
2.38 # |
1.19-4.26 |
| Total |
32 |
17.61 |
1.82 # |
1.24-2.57 |
| Asian or Pacific Islander |
| 2-11 Months |
39 |
24.21 |
1.61 # |
1.15-2.2 |
| 12-59 Months |
120 |
101.47 |
1.18 |
0.98-1.41 |
| 60-119 Months |
119 |
92.03 |
1.29 # |
1.07-1.55 |
| 120+ Months |
95 |
85.28 |
1.11 |
0.9-1.36 |
| Total |
373 |
302.99 |
1.23 # |
1.11-1.36 |
| Unknown |
| 2-11 Months |
1 |
2.02 |
0.5 |
0.01-2.76 |
| 12-59 Months |
1 |
7.57 |
0.13 # |
0-0.74 |
| 60-119 Months |
0 |
5.74 |
0 # |
0-0.64 |
| 120+ Months |
0 |
4.4 |
0 # |
0-0.84 |
| Total |
2 |
19.73 |
0.10 # |
0.01-0.37 |
Ethnic differences were also notable. Hispanic patients had consistently lower risk of developing SPLC. Their overall SIR was 0.72 (0.65–0.79), with further reductions during 12–59 months (0.56; 0.47–0.67), 60–119 months (0.75; 0.63–0.89), and ≥120 months (0.79; 0.66–0.94). By comparison, non-Hispanic patients showed a brief spike in early risk (2–11 months: 1.13; 1.05–1.23), followed by a small decrease at 12–59 months (0.94; 0.90–0.98), resulting in an overall neutral risk (1.01; 0.99–1.04) (
Table 5,
Figure 8).
Marital status also showed associations with SPLC risk. Married individuals had a lower overall risk (SIR 0.88; 0.85–0.91), with statistically significant reductions at 12–59 months (0.82; 0.77–0.87), 60–119 months (0.91; 0.86–0.96), and beyond 120 months (0.89; 0.84–0.94). In contrast, those who were unmarried had a higher risk during the 2–11 month interval (1.12; 1.04–1.21), a decreased risk at 12–59 months (0.91; 0.87–0.95), and a neutral overall risk (0.99; 0.96–1.01) (
Table 4).
Table 4.
Standardized incidence ratios by ethnicity and latency interval.
Table 4.
Standardized incidence ratios by ethnicity and latency interval.
| Ethnicity |
|---|
| Duration |
Observed |
Expected |
SIR |
CI |
| Hispanic |
| 2-11 Months |
55 |
53.83 |
1.02 |
0.77-1.33 |
| 12-59 Months |
125 |
221.33 |
0.56 # |
0.47-0.67 |
| 60-119 Months |
144 |
191.52 |
0.75 # |
0.63-0.89 |
| 120+ Months |
127 |
161.58 |
0.79 # |
0.66-0.94 |
| Total |
451 |
628.26 |
0.72 # |
0.65-0.79 |
| Non-Hispanic |
| 2-11 Months |
624 |
550.24 |
1.13 # |
1.05-1.23 |
| 12-59 Months |
2,202 |
2,332.61 |
0.94 # |
0.9-0.98 |
| 60-119 Months |
2,172 |
2,088.90 |
1.04 |
1-1.08 |
| 120+ Months |
1,866 |
1,811.24 |
1.03 |
0.98-1.08 |
| Total |
6,864 |
6,782.99 |
1.01 |
0.99-1.04 |
| Unknown |
| 2-11 Months |
1 |
1.37 |
0.73 |
0.02-4.06 |
| 12-59 Months |
0 |
5.42 |
0.00 # |
0-0.68 |
| 60-119 Months |
0 |
4.64 |
0.00 # |
0-0.79 |
| 120+ Months |
0 |
3.81 |
0.00 # |
0-0.97 |
| Total |
1 |
15.25 |
0.07 # |
0-0.37 |
Table 5.
Standardized incidence ratios by marital status and latency interval.
Table 5.
Standardized incidence ratios by marital status and latency interval.
| Marital Status |
|---|
| Duration |
Observed |
Expected |
SIR |
CI |
| Married |
| 2-11 Months |
321 |
331.45 |
0.97 |
0.87-1.08 |
| 12-59 Months |
1,180 |
1,443.96 |
0.82 # |
0.77-0.87 |
| 60-119 Months |
1,236 |
1,362.23 |
0.91 # |
0.86-0.96 |
| 120+ Months |
1,145 |
1,284.98 |
0.89 # |
0.84-0.94 |
| Total |
3,882 |
4,422.63 |
0.88 # |
0.85-0.91 |
| Unmarried |
| 2-11 Months |
680 |
605.44 |
1.12 # |
1.04-1.21 |
| 12-59 Months |
2,327 |
2,559.36 |
0.91 # |
0.87-0.95 |
| 60-119 Months |
2,316 |
2,285.07 |
1.01 |
0.97-1.06 |
| 120+ Months |
1,993 |
1,976.63 |
1.01 |
0.96-1.05 |
| Total |
7,316 |
7,426.50 |
0.99 |
0.96-1.01 |
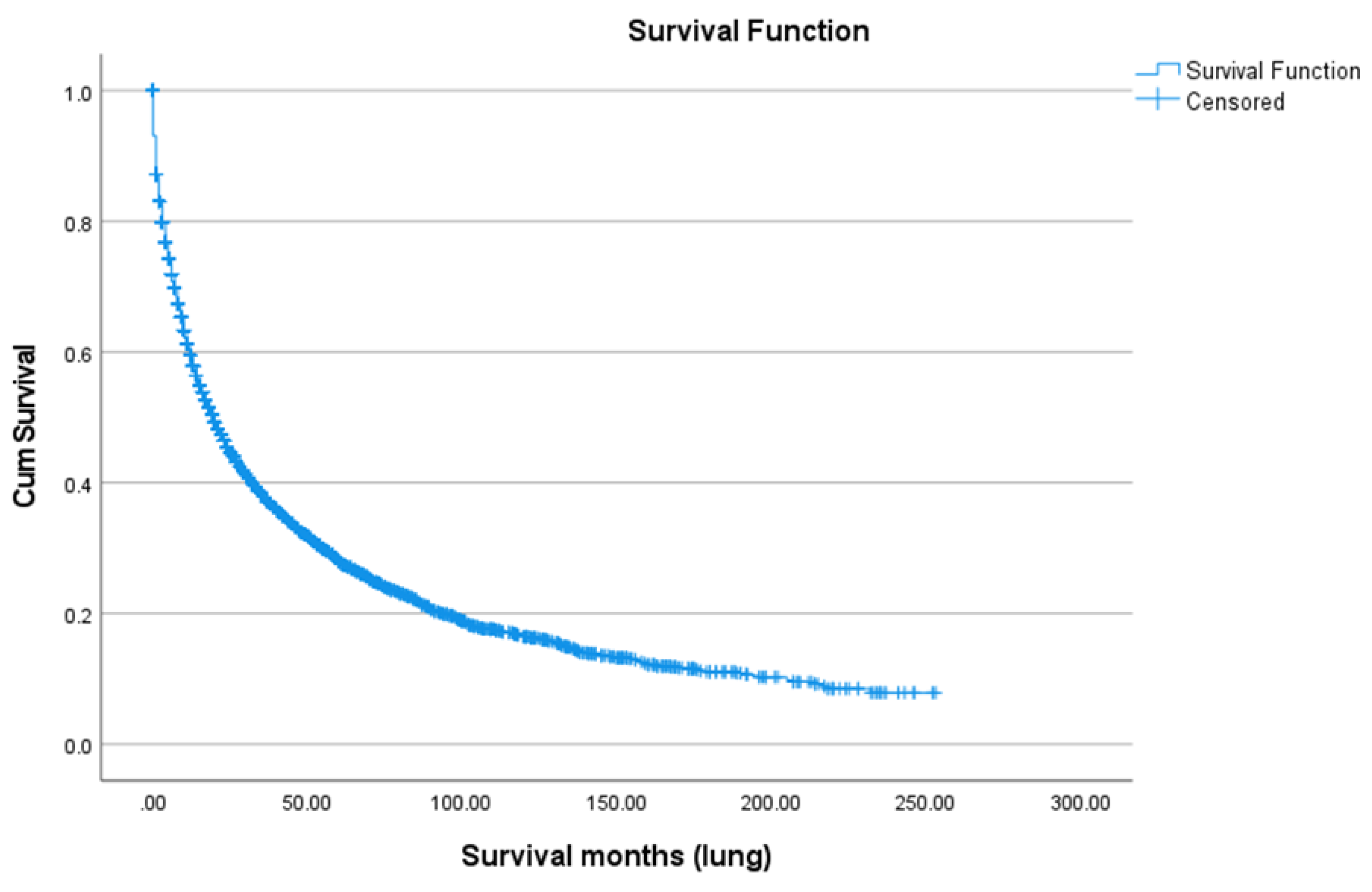
3.4. Survival Analysis
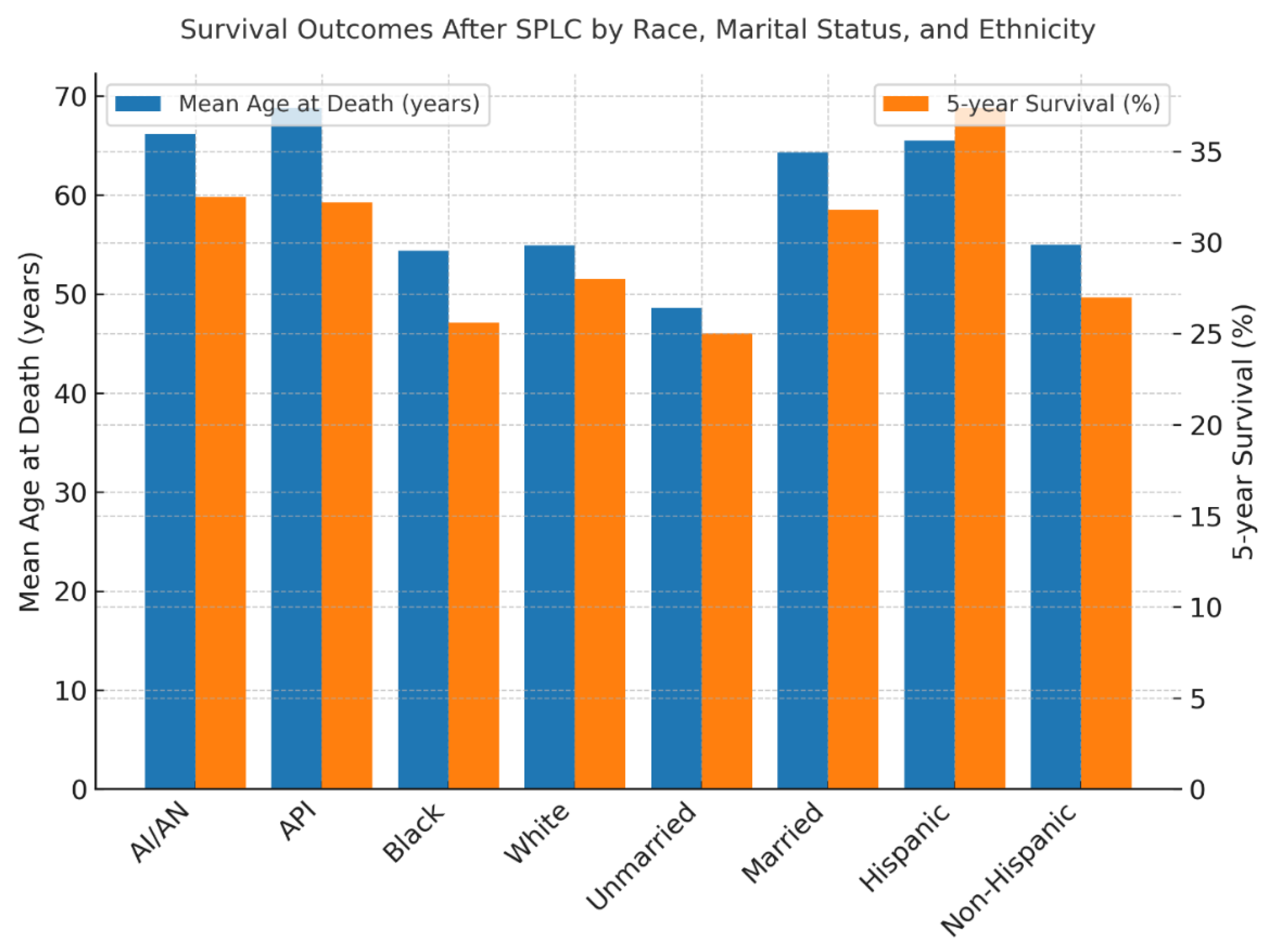
Survival after SPLC diagnosis was generally poor, with a five-year overall survival rate of 28.0% (
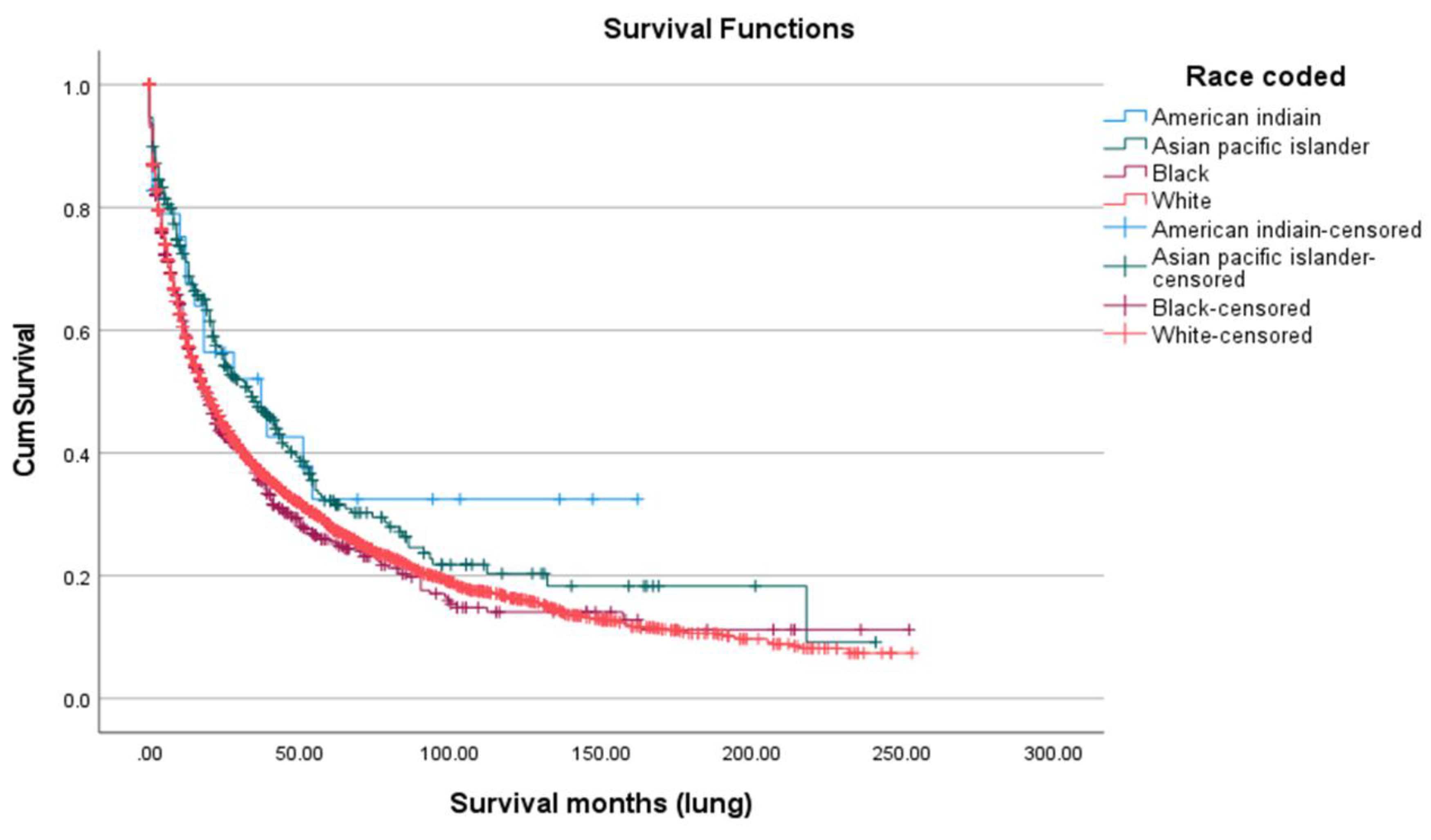
Figure 3). There were notable differences by race and ethnicity. Asian/Pacific Islanders had the highest five-year survival (32.2%) and the highest mean age at death (68.82 years), followed by American Indian/Alaska Natives (32.5%; 66.17 years), Whites (28.0%; 54.94 years), and Blacks (25.6%; 54.39 years), with a statistically significant difference (p = 0.002) (
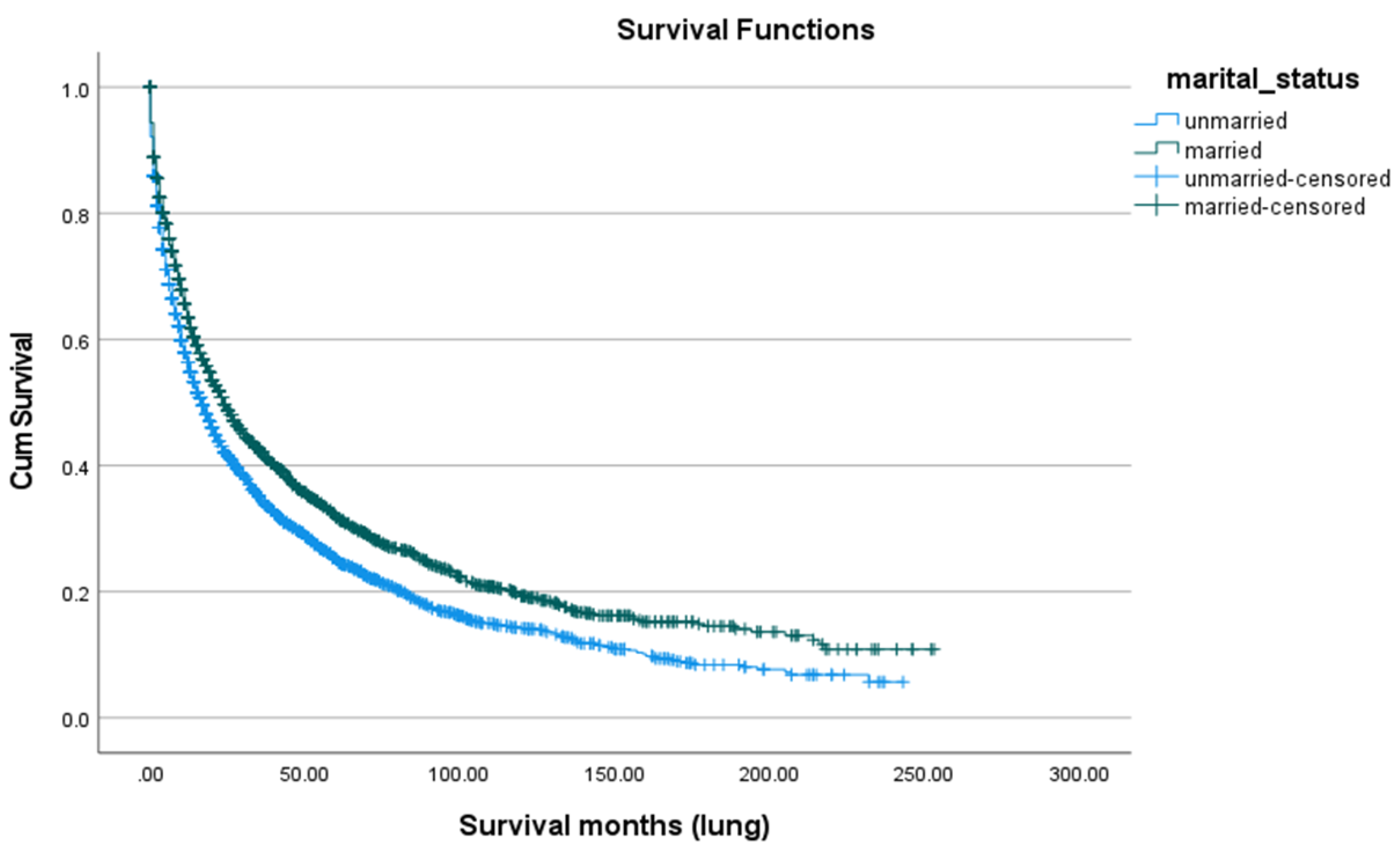
Figure 6). Marital status also played a role: married patients lived longer (mean age at death 64.31 years) and had a higher five-year survival rate (31.8%) compared to unmarried individuals (48.64 years; 25.0%, p < 0.001) (
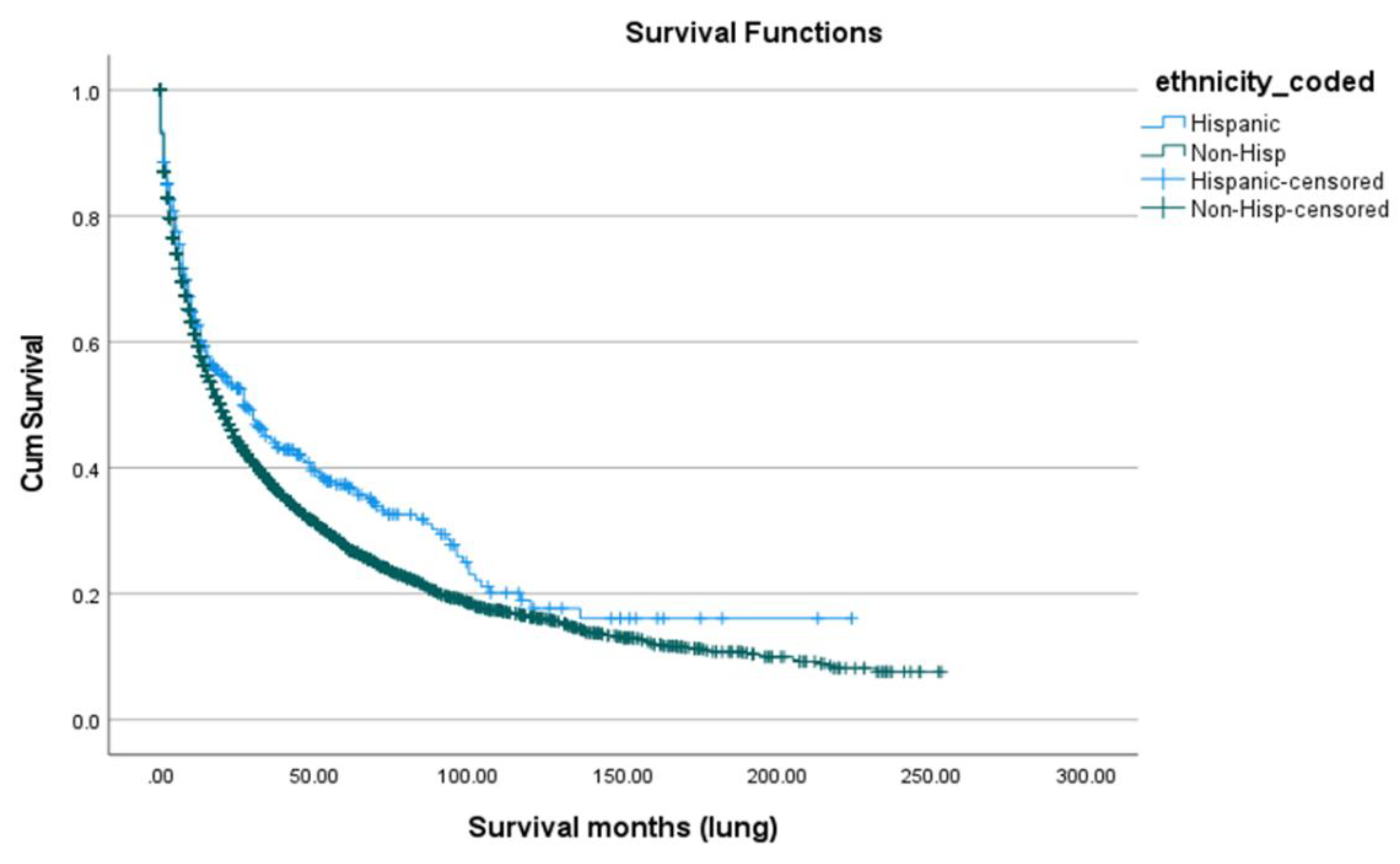
Figure 5. Hispanic patients also fared better than non-Hispanics, with a mean survival age of 65.48 years and a five-year survival of 37.4%, compared to 55.0 years and 27.0% in non-Hispanics (p = 0.005) (
Table 2,
Figure 4,
Figure 7).
Figure 3.
Overall survival among SPLC patients.
Figure 3.
Overall survival among SPLC patients.
Figure 4.
Survival according to marital status.
Figure 4.
Survival according to marital status.
Figure 5.
Survival according to ethnicity.
Figure 5.
Survival according to ethnicity.
Figure 6.
Survival according to race.
Figure 6.
Survival according to race.
Figure 7.
Combined groups’ survival outcomes.
Figure 7.
Combined groups’ survival outcomes.
Figure 8.
SPLC risk and latency interval according to race and ethnicity.
Figure 8.
SPLC risk and latency interval according to race and ethnicity.
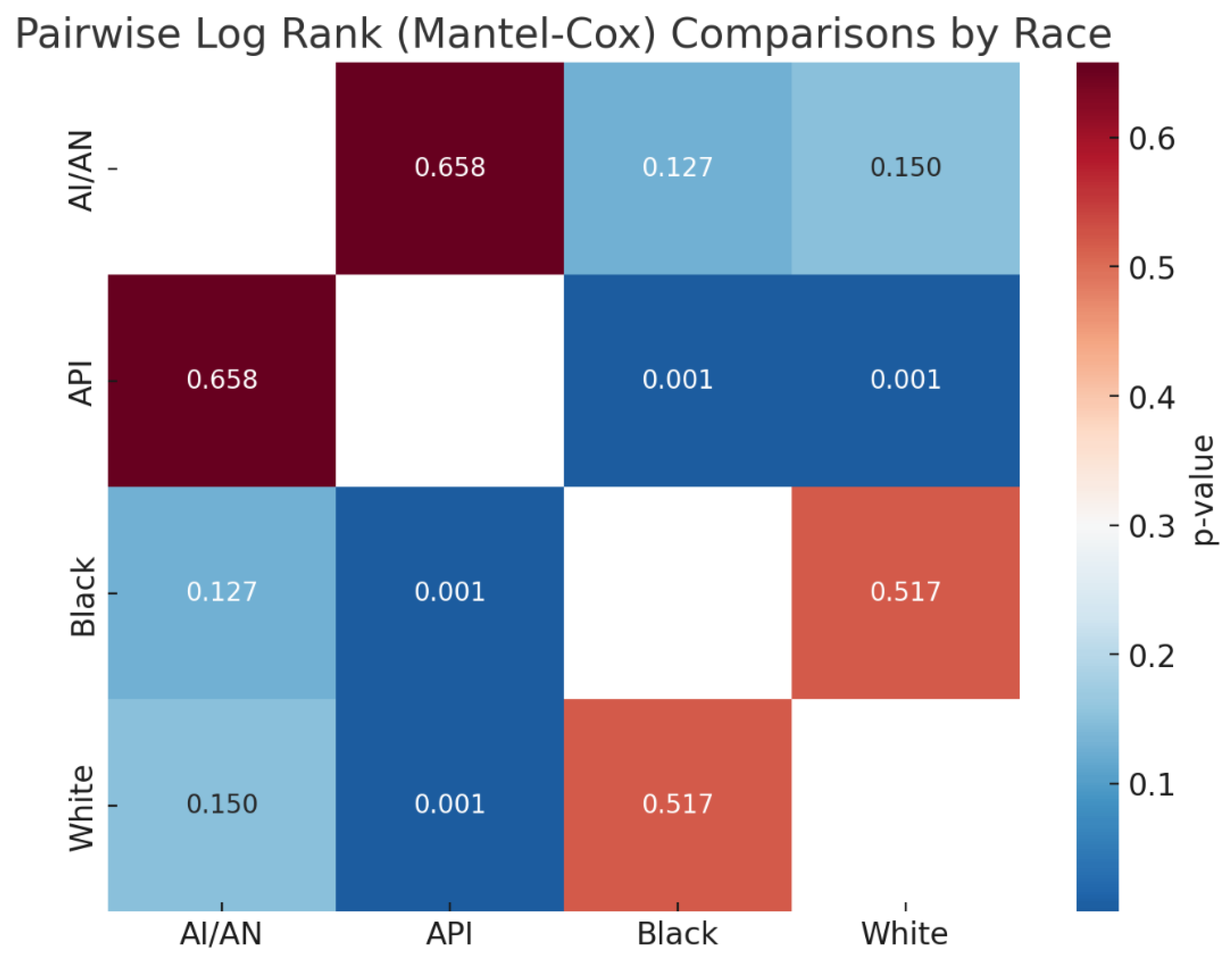
Figure 9.
Pairwise Log Rank (Mantel-Cox) Comparisons by Race*.
Figure 9.
Pairwise Log Rank (Mantel-Cox) Comparisons by Race*.
3.5. Cox Proportional Hazards Regression
The analysis identified several significant demographic and clinical predictors of mortality. Marital status was a key factor, with unmarried patients showing a higher risk of death than married patients (HR 1.139, 95% CI 1.072–1.209; p<0.001). Hispanic ethnicity was associated with a lower hazard compared with non-Hispanic ethnicity (HR 0.842, 95% CI 0.741–0.957; p=0.009). Overall stage was not significant (p=0.270); however, Stage IV predicted increased mortality (HR 1.366, 95% CI 1.011–1.847; p=0.043). Breast histology was significant in outcomes (overall p=0.001), with ductal, lobular, adenocarcinoma, and mixed ductal/lobular subtypes demonstrating reduced hazards (HR range 0.680–0.772; all p≤0.012). Race was significant overall (p=0.049), largely due to the lower risk among Asian/Pacific Islander patients (HR 0.857, 95% CI 0.744–0.986; p=0.031). Mortality increased with age (HR 1.024 per year, 95% CI 1.020–1.027; p<0.001), while tumor side (p=0.465) and sex (p=0.869) were not significantly associated with survival. Radiation type was not significantly associated with mortality (overall p = 0.149). Across radiation categories, there were no statistically significant differences in HR (beam radiation: HR 1.197, p = 0.799; combination: HR 1.563, p = 0.546; radiation NOS: HR 1.320, p = 0.700; radioactive implants: HR 1.017, p = 0.982) (
Table 6)
4. Discussion
In this population-based study using SEER data, we investigated the incidence and survival outcomes of SPLC following breast cancer radiotherapy, with a focus on racial/ethnic disparities and the influence of marital status. Our study demonstrated that the incidence of secondary primary lung cancer (SPLC) following breast cancer radiotherapy was elevated most significantly in American Indians and Alaska natives (AI/AN), who experienced risks more than double the expected rate. The incidence was also higher among Black individuals, as well as Asians and Pacific Islanders (API). Additionally, we observed consistently low SPLC risks among married patients, suggesting a potential protective effect.
The results on incidence of SPLC align with the findings of the current literature, which report an elevated long-term risk of SPLC after breast radiotherapy. The increased risk of SPLC following breast radiotherapy observed in Black patients, API, and AI/AN suggests a persistent biological vulnerability or environmental exposures that are not mitigated by modern radiotherapy protocols. Nevertheless, the risk is thought to be lower than previously published, with an incidence of 1.19% in our study compared to 1.74% in [
23]. While the primary lung cancer incidence rate in Black individuals has been consistently higher than that in Whites [
24], data showed that AI/AN had a lower incidence of primary lung cancer than Whites [
25]. Our study reveals that the risk in AI/AN populations is more pronounced than previously reported. This is a significant contribution, as few studies have specifically examined this group in the context of radiation-induced cancers.
Our analysis showed that married patients have had a lower likelihood of SPLC over both 5-year and 10-year periods. While unmarried patients had a higher likelihood of SPLC during the first year, this likelihood decreased over time. This suggests that social support has a vital role to play in reducing the risk of having lung cancer, as it helps patients to recognize respiratory symptoms as they arise and may also contribute to a reduction in smoking rates [
26].
The median overall survival (OS) for patients with SPLC in our study differed significantly among racial groups, with API having the longest OS at 68.8 months, followed by AI/AN and White individuals; Black patients showed the shortest OS at 54.4 months. The five-year survival also varied between racial groups, for it was highest amongst Hispanics and lowest amongst Black individuals. This is likely due to multiple variables on different levels, including
patient-level factors such as socioeconomic barriers, cultural stigma, mistrust, and insurance limitations, physician-level
variables such as implicit bias, stereotyping, and inconsistent treatment recommendations. Finally, system-level factors play a crucial role and include, but are not limited to, unequal access to high-quality care, underrepresentation in trials, and delayed treatment [
27].
Our study found that Hispanic breast cancer survivors had a lower risk of SPLC and better five-year survival compared with non-Hispanic patients. This pattern is consistent with the well-described lower baseline incidence of lung cancer among Hispanic populations, a trend largely attributed to lower smoking prevalence, cultural factors, and differences in environmental exposures. These established population patterns likely contribute to the reduced SPLC risk observed in our cohort. Further research is needed to clarify how these factors interact with prior radiation exposure and to ensure appropriate risk-based follow-up. [
28,
29,
30].
For married individuals, survival outcomes were superior to those of unmarried patients. Likely due to psychosocial, economic, and environmental factors, having a partner or spouse is associated with a healthier lifestyle, a greater chance of detecting the disease at an earlier stage, and a higher likelihood of opting for active treatment [31].
Multiple risk factors have been described to affect the incidence of SPLC following breast radiotherapy, including smoking [32], dose [33], and type of radiation (proton vs photon therapies) [34]. Findings from our study suggest the increased risk in certain racial groups and people who are unmarried, raising the need to design a risk stratification tool to include the abovementioned risk factors and better predict the risk of SPLC associated with breast radiotherapy. Better screening and surveillance should also be implemented based on such a tool.
This study is limited by its reliance on retrospective data and the SEER database. As a registry-based dataset, SEER lacks important clinical variables such as smoking status, radiation dose,treatment details, and key comorbidities, which restricts the ability to adjust for major confounders. SEER also does not capture some essential socioeconomic indicators, limiting the robustness of statistical adjustments for social determinants of health. Additionally, SEER covers approximately half of the U.S. population, which may limit the generalizability of our findings to non-SEER regions. Follow-up and latency definitions are based on SEER multiple primary rules, which may result in shorter follow-up windows than ideal for capturing radiation-associated SPLCs. Future research using prospective cohorts with comprehensive clinical and socioeconomic information is needed to better evaluate the roles of smoking, radiation dose, comorbidities, and marital status in SPLC risk after breast radiotherapy. Moreover, further studies are needed to better characterize the biological and clinical significance of SPLCs occurring shortly after breast cancer diagnosis and radiotherapy.
5. Conclusions
This population-based cohort study demonstrates that the risk and survival outcomes of second primary lung cancer (SPLC) after breast cancer radiotherapy vary significantly by race, ethnicity, and marital status. These findings highlight the need to integrate sociodemographic factors into survivorship care and long-term surveillance strategies for breast cancer patients receiving radiotherapy. Future work should prioritize developing personalized risk-stratification models that incorporate race, social context, and treatment history to guide equitable lung cancer screening and follow-up.
Author Contributions
Fares A. Qtaishat: Conceptualization, study design, data acquisition, analysis, interpretation, manuscript drafting, visualization, and supervision. Mohammad Hamad: Review of background literature, analysis, visualization, manuscript formatting, and quality control. Adham Musa : Methodology, statistical analysis, writing—original draft, critical revision, and correspondence. Theeb Natsheh: Data curation, literature review, results interpretation, writing—review and editing. Othman Al-Barghouthi: Data cleaning, coding validation, and manuscript editing. Basil A. Abusalameh: Literature search, formatting, and reference management. Anas A. Younis: Writing—review and editing, interpretation of findings, figure and table preparation. Hamzeh Al-Qarallah: Visualization, supplemental analysis, and critical review of statistical content. Sara Qutaishat: Data verification, manuscript review, and editorial support. Matthew P. Banegas: Study design consultation, statistical methodology review, and manuscript editing. H. Irene Su: Study design consultation, statistical methodology review, and manuscript editing. Winta T. Mehtsun: Study design consultation, statistical methodology review, and manuscript editing. Tala Al-Rousan: Design, data interpretation, manuscript drafting and overall supervision. All authors have read and approved the final version of the manuscript.
Funding
TA is supported through a grant from the National Heart, Lung and Blood Institute (R01HL173155) and National Intsitue of Aging (#P30AG059299).
Ethics Approval and Consent to Participate
Not applicable.
Availability of Data and Materials
All data generated or analyzed during this study are included in the published article.
Acknowledgments
Preliminary results from this study were presented in abstract form at the 18th AACR Conference on The Science of Cancer Health Disparities, September 18–21, 2025, Baltimore, Maryland, USA.
Competing Interests
The authors declare no competing interests.
References
- Bartelink, H., Maingon, P., Poortmans, P., Weltens, C., Fourquet, A., Jager, J., Schinagl, D., Oei, B., Rodenhuis, C., Horiot, J. C., Struikmans, H., Van Limbergen, E., Kirova, Y., Elkhuizen, P., Bongartz, R., Miralbell, R., Morgan, D., Dubois, J. B., Remouchamps, V., … Collette, L. (2015). Whole-breast irradiation with or without a boost for patients treated with breast-conserving surgery for early breast cancer: 20-year follow-up of a randomised phase 3 trial. The Lancet Oncology, 16(1), 47–56. [CrossRef]
- Bliss, A., Cobb, N., Solomon, T., Cravatt, K., Jim, M. A., Marshall, L., & Campbell, J. (2008). Lung cancer incidence among American Indians and Alaska Natives in the United States, 1999–2004. Cancer, 113(S5), 1168–1178. [CrossRef]
-
Breast Cancer Surgery - PubMed. (n.d.). Retrieved July 26, 2025, from https://pubmed.ncbi.nlm.nih.gov/31971717/.
- Choi, E., Hua, Y., Su, C. C., Wu, J. T., Neal, J. W., Leung, A. N., Backhus, L. M., Haiman, C., Le Marchand, L., Liang, S. Y., Wakelee, H. A., Cheng, I., & Han, S. S. (2024). Racial and ethnic differences in second primary lung cancer risk among lung cancer survivors. JNCI Cancer Spectrum, 8(5). [CrossRef]
- DiMarco, PharmD, BCPS, BCOP, R., & Milli, MSN, RN, WHNP-BC, L. (2022). Race, Social Determinants of Health, and Cancer: How Can APs Address and Improve Patient Outcomes? Journal of the Advanced Practitioner in Oncology, 13(3), 221. [CrossRef]
- Edwards, B. K., Noone, A. M., Mariotto, A. B., Simard, E. P., Boscoe, F. P., Henley, S. J., Jemal, A., Cho, H., Anderson, R. N., Kohler, B. A., Eheman, C. R., & Ward, E. M. (2014). Annual Report to the Nation on the status of cancer, 1975-2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer, 120(9), 1290–1314. [CrossRef]
- Emdin, S., Granstrand, B., Ringberg, A., Sandelin, K., Arnesson, L. G., Nordgren, H., Anderson, H., Garmo, H., Holmberg, L., & Wallgren, A. (2006). SweDCIS: Radiotherapy after sector resection for ductal carcinoma in situ of the breast. Results of a randomised trial in a population offered mammography screening. Acta Oncologica, 45(5), 536–543. [CrossRef]
- Esnaola, N. F., & Ford, M. E. (2012). Racial Differences and Disparities in Cancer Care and Outcomes: Where’s the Rub? Surgical Oncology Clinics of North America, 21(3), 417. [CrossRef]
- Gadgeel, S. M., & Kalemkerian, G. P. (2003). Racial differences in lung cancer. Cancer and Metastasis Reviews, 22(1), 39–46. [CrossRef]
- Grantzau, T., & Overgaard, J. (2015). Risk of second non-breast cancer after radiotherapy for breast cancer: A systematic review and meta-analysis of 762,468 patients. Radiotherapy and Oncology, 114(1), 56–65. [CrossRef]
- Grantzau, T., Thomsen, M. S., Væth, M., & Overgaard, J. (2014). Risk of second primary lung cancer in women after radiotherapy for breast cancer. Radiotherapy and Oncology, 111(3), 366–373. [CrossRef]
- Hall, E. J., & Wuu, C. S. (2003). Radiation-induced second cancers: The impact of 3D-CRT and IMRT. International Journal of Radiation Oncology Biology Physics, 56(1), 83–88. [CrossRef]
- Hayat, M. J., Howlader, N., Reichman, M. E., & Edwards, B. K. (2007). Cancer Statistics, Trends, and Multiple Primary Cancer Analyses from the Surveillance, Epidemiology, and End Results (SEER) Program. The Oncologist, 12(1), 20–37. [CrossRef]
- Krajc, K., Miroševič, Š., Sajovic, J., Klemenc Ketiš, Z., Spiegel, D., Drevenšek, G., & Drevenšek, M. (2023). Marital status and survival in cancer patients: A systematic review and meta-analysis. Cancer Medicine, 12(2), 1685–1708. [CrossRef]
- Miao, E., Klugman, M., Rohan, T., & Dean Hosgood, H. (2023). Hypothesized Explanations for the Observed Lung Cancer Survival Benefit Among Hispanics/Latinos in the United States. Journal of Racial and Ethnic Health Disparities, 10(3), 1339–1348. [CrossRef]
- Neugut, A. I., Lee, W. C., Murray, T., Robinson, E., Karwoski, K., & Kutcher, G. J. (1993). Lung cancer after radiation therapy for breast cancer. Cancer, 71(10), 3054–3057. [CrossRef]
- Neugut, A. I., Murray, T., Santos, J., Amols, H., Hayes, M. K., Flannery, J. T., & Robinson, E. (1994). Increased risk of lung cancer after breast cancer radiation therapy in cigarette smokers. Cancer, 73(6), 1615–1620. [CrossRef]
- Pinheiro, L. C., Reshetnyak, E., Akinyemiju, T., Phillips, E., & Safford, M. M. (2021). Social Determinants of Health and Cancer Mortality in the REasons for Geographic and Racial differences in Stroke (REGARDS) cohort study. Cancer, 128(1), 122. [CrossRef]
- Ruiz, J. M., Steffen, P., & Smith, T. B. (2013). Hispanic Mortality Paradox: A Systematic Review and Meta-Analysis of the Longitudinal Literature. American Journal of Public Health, 103(3), e52. [CrossRef]
- Siegel, R. L., Kratzer, T. B., Giaquinto, A. N., Sung, H., & Jemal, A. (2025). Cancer statistics, 2025. CA: A Cancer Journal for Clinicians, 75(1), 10–45. [CrossRef]
- Siegel, R. L., Miller, K. D., Fuchs, H. E., & Jemal, A. (2021). Cancer Statistics, 2021. CA: A Cancer Journal for Clinicians, 71(1), 7–33. [CrossRef]
- Siegel, R. L., Miller, K. D., Fuchs, H. E., & Jemal, A. (2022). Cancer statistics, 2022. CA: A Cancer Journal for Clinicians, 72(1), 7–33. [CrossRef]
- Siva Kumar, S., Bradley, J. A., Mendenhall, N. P., Mailhot Vega, R. B., Brooks, E. D., Okunieff, P. G., Giap, F., Burchianti, T., Daily, K., Heldermon, C. D., Galochkina, Z., Lee, J. H., Swarts, S., & O’Dell, W. G. (2024). Effects on Lung Tissue After Breast Cancer Radiation: Comparing Photon and Proton Therapies. International Journal of Particle Therapy, 11, 100006. [CrossRef]
- Tannenbaum, S. L., Zhao, W., Koru-Sengul, T., Miao, F., Lee, D., & Byrne, M. M. (2013). Marital status and its effect on lung cancer survival. SpringerPlus, 2(1), 1–10. [CrossRef]
- Taylor, C., Duane, F. K., Dodwell, D., Gray, R., Wang, Z., Wang, Y., Peto, R., McGale, P., Correa, C., Aznar, M. C., Ewertz, M., Anderson, S. J., Bergh, J., Jagsi, R., Pierce, L., Pritchard, K. I., Whelan, T., & Swain, S. (2017). Estimating the Risks of Breast cancer radiotherapy: Evidence from modern radiation doses to the lungs and Heart and From previous randomized trials. Journal of Clinical Oncology, 35(15), 1641–1649. [CrossRef]
- Wapnir, I. L., Dignam, J. J., Fisher, B., Mamounas, E. P., Anderson, S. J., Julian, T. B., Land, S. R., Margolese, R. G., Swain, S. M., Costantino, J. P., & Wolmark, N. (2011). Long-term outcomes of invasive ipsilateral breast tumor recurrences after lumpectomy in NSABP B-17 and B-24 randomized clinical trials for DCIS. Journal of the National Cancer Institute, 103(6), 478–488. [CrossRef]
- Wennstig, A. K., Wadsten, C., Garmo, H., Johansson, M., Fredriksson, I., Blomqvist, C., Holmberg, L., Nilsson, G., & Sund, M. (2021). Risk of primary lung cancer after adjuvant radiotherapy in breast cancer—a large population-based study. Npj Breast Cancer, 7(1). [CrossRef]
- Wong, L. Y., Kapula, N., He, H., Guenthart, B. A., Vitzthum, L. K., Horst, K., Liou, D. Z., Backhus, L. M., Lui, N. S., Berry, M. F., Shrager, J. B., & Elliott, I. A. (2023). Risk of developing subsequent primary lung cancer after receiving radiation for breast cancer. JTCVS Open, 16, 919. [CrossRef]
- Woodward, W. A., Strom, E. A., McNeese, M. D., Perkins, G. H., Outlaw, E. L., Hortobagyi, G. N., Buzdar, A. U., & Buchholz, T. A. (2003). Cardiovascular death and second non-breast cancer malignancy after postmastectomy radiation and doxorubicin-based chemotherapy. International Journal of Radiation Oncology Biology Physics, 57(2), 327–335. [CrossRef]
- Zablotska, L. B., & Neugut, A. I. (2003). Lung carcinoma after radiation therapy in women treated with lumpectomy or mastectomy for primary breast carcinoma. Cancer, 97(6), 1404–1411. [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).