
Submitted:
08 January 2026
Posted:
09 January 2026
You are already at the latest version
Abstract
Sepsis is a complex infection-driven inflammatory syndrome that can lead to life-threatening multi-organ failure and septic shock, characterized by cardiovascular instability, tissue hypoperfusion, and impaired oxygen utilization. Myocardial dys-function is a frequent and multifaceted complication in both adults and children, with sepsis-induced cardiomyopathy (SCM) representing an acute, reversible form of non-ischemic cardiac failure involving left and sometimes right ventricular impairment. Diagnosis relies on excluding acute coronary syndromes and recognizing refractory shock, low mixed venous oxygen saturation, and elevated cardiac biomarkers, espe-cially in patients with known risk factors such as pre-existing heart disease or elevated lactate. The pathophysiology reflects an interplay of systemic inflammation, circulatory redistribution, and mitochondrial dysfunction, while clinical recognition remains challenging, particularly in pediatrics where hypotension is a late sign. Early fluid re-suscitation is vital to restore perfusion, yet excessive administration risks fluid overload, underscoring the need for precise hemodynamic assessment. Conventional echocar-diographic measures of heart function may give misleading results in SCM because they depend on preload and afterload, often underestimating the true degree of myocardial impairment. Advanced hemodynamic monitoring, ranging from invasive to minimally invasive and non-invasive methods, is currently being studied for managing sepsis. Minimally invasive techniques offer detailed, dynamic data that complement echocar-diography and help identify specific hemodynamic profiles to guide septic shock treatment. Contemporary management increasingly favors multimodal monitoring and individualized strategies over protocol-driven approaches to optimize timely, goal-directed therapy.
Keywords:
sepsis
; septic cardiomyopathy
; children
; adults
; hemodynamic
; monitoring
1. Introduction
Sepsis is a complicated, infectious-driven, inflammatory process with life-threatening consequences due to cascades of interdependent multi-organ failures. At the same time, septic shock is the clinical manifestation of septic cardiovascular instability, tissue hypoperfusion, and increased metabolic demands, associated with inadequacy in oxygen delivery or in mitochondrial oxygen consumption. [1,2]. Myocardial dysfunction is a common complication of sepsis, with multifaceted manifestations among pediatric and adult patients. [3]. Sepsis-induced cardiomyopathy (SCM) is a common sepsis-related, acute, reversible condition of non-ischemic myocardial dysfunction, which may range from subclinical biventricular impairment to overt cardiogenic shock [4]. Moreover, current definitions of SCM include a reversible myocardial dysfunction, unresponsiveness to fluid or vasoactive therapies, and the essential exclusion of an acute ischemic coronary syndrome [5]. Importantly, septic cardiomyopathy may not be regarded as synonymous with septic cardiogenic shock. SCM represents a dynamic and heterogenous spectrum of myocardial dysfunction that may occur across a wide range of hemodynamic states, including preserved or even elevated cardiac output in the setting of profound vasoplegia. On the other hand, cardiogenic shock is characterized by inadequate cardiac output and tissue hypoperfusion, despite optimized preload and afterload [6,7].
On clinical grounds, sepsis and septic shock mainly comprise vasoplegia, a hyperdynamic cardiac contractility state, and low systemic vascular resistance, with treatment primarily aiming at restoring vascular tone, while low cardiac output, high left ventricle (LV) filling pressures, high systemic vascular resistance, decreased perfusion, and evidence of end-organ damage characterize cardiogenic shock [6]. Moreover, refractory shock to fluid and vasopressor therapy, low mixed venous oxygen saturation (SvO2), prior history of heart disease, and elevated cardiac biomarkers highly suggest the diagnosis [7]. Known risk factors for SCM include younger age, pre-existing cardiac conditions, higher lactic acid levels, and positive blood cultures [8,9].
Myocardial and circulatory compromise is a devastating complication of sepsis, closely linked to systemic inflammation and blood redistribution. The intertwinement of direct myocardial depression and circulatory alterations, along with mitochondrial dysregulation, is being highlighted in current literature [10]. The clinical parameters of septic shock and septic cardiomyopathy are often elusive, with moderate sensitivity and poor specificity. This especially concerns the pediatric population, where hypotension is a late sign, and microcirculatory markers, such as lactate, mixed venous saturation (SvO2) and base deficit, provide better estimations of tissue perfusion [2].
Timely fluid resuscitation is a critical intervention in septic shock to increase venous return, cardiac output, and oxygen delivery (DO2) to tissues. However, monitoring the deleterious effects of excessive resuscitation is equally essential to prevent fluid overload [11]. According to recent studies, only 50-60% of patients are fluid responders in the early stages of sepsis, while over-treatment might be imminent in a significant number of patients [12,13]. Therefore, objective hemodynamic tools are urgently required for timely and goal-directed therapeutic interventions. Detailed and continuous hemodynamic assessments are of paramount importance when caring for septic patients, given that echocardiographic “snapshots” cannot fulfill the whole picture [14,15]. Over the past few decades, scientific focus has shifted to multifaceted approaches for adult and pediatric sepsis, with multimodality monitoring instead of standard clinical techniques, and personalized practices instead of protocolized-based care [2].
The present review aims to provide a comprehensive synthesis of current knowledge on septic cardiomyopathy in both adult and pediatric populations. Specifically, it focuses on the epidemiology, pathophysiology, diagnostic challenges, invasive and non-invasive hemodynamic assessment, and contemporary treatment strategies, seeking to highlight evidence gaps and prompt future research on characterization and treatment of SCM.
2. Epidemiology
Reported epidemiological estimates of SCM vary across studies, reflecting differences in patient populations, diagnostic criteria and monitoring techniques. Consequently, prevalence and outcome data should be interpreted with caution. Age-specific clinical and developmental norms, comorbidities, and prognostic outcomes differentiate pediatric septic sequelae from adult responses [16]. However, children's and adults' septic processes are complicated by myocardial dysfunction at similar rates [3]. Recent studies have shown that sepsis accounts for 25% of global mortality and 7% of all pediatric mortality, while the majority of pediatric sepsis cases are complicated by cardiovascular dysfunction [17,18]. Global reports also provide mortality rate estimations for septic shock of up to 40-80% [19], while hospital mortality is higher in septic myocardial dysfunction compared to non-septic cardiomyopathies [20].
Extensive prospective studies in adult septic patients have demonstrated an incidence of up to 70% for septic myocardial dysfunction, depending on study design and diagnostic criteria [21,22,23], but a recent meta-analysis reported that the pooled prevalence of SCM was 20%, and was associated with a pooled odds ratio of 2.3 for mortality risk (95% CI: 1.43-3.69) [24]. In addition, clinical studies currently report notably high ICU mortality rates of 40-70% for SCM cases [25]. The epidemiologic variance emphasizes the complexity of sepsis phenotyping and treatment approaches [7].
Similarly, an overall prevalence of 30-70% for pediatric septic cardiomyopathy has been reported [3,14]. A few studies have reported that 32-47% of children present with systolic dysfunction, while 25-31.5% of cases present with severe impairment and dilatation of all chambers [14,18,26]. Pediatric septic patients seem to present with low cardiac output (58%), while high cardiac output states concern a smaller percentage (20%) of septic children [27]. However, a recent study found that septic shock pediatric patients tend to have higher cardiac output and cardiac contractility, compared to cardiogenic shock [19]. In addition, these children often do not respond to initial interventions with fluid resuscitation and vasoactive or inotropic agents, which complicates their clinical course and necessitates extracorporeal life support [5]. Pediatric mortality for SCM has been reported as high as 55%, in contrast to septic shock cases without SCM, with reported mortality rates of about 7.5% [18].
3. Pathophysiological Mechanisms in Adult and Pediatric Sepsis
Cardiovascular compromise in sepsis is not yet completely elucidated. The initial hypothesis of myocardial ischemia in SCM has recently been abandoned, based on evidence of high coronary blood flow, limited myocardial oxygen utilization, and absence of irreversible anatomical abnormalities or myocardial apoptotic processes. At the cellular level, reduced myocardial calcium responsiveness, dysregulated intramyocyte calcium homeostasis, oxidative/nitrosative stress, with subsequent mitochondrial dysfunction and energetic failure, seem to be the basic pathophysiologic abnormalities in septic myocardial tissues [5,28]. Given that the heart is rich in mitochondria [22] and based on the theory of hibernation, mitochondrial inhibition might serve as a protective bioenergetic response for the failing myocardium [29,30]. Current studies have also associated septic cardiomyopathy with the NLRP3 inflammasome-driven activation of caspase-1 and pyroptosis, especially in macrophages, cardiomyocytes, and endothelial cells [31,32]. The reversibility of myocardial dysfunction has recently been postulated, as global myocardial edema and inflammation, but not focal fibrosis, are characteristic, reversible cardiac magnetic resonance imaging (MRI) findings, differentiating SCM from myocardial ischemia or acute myocarditis [33]. Overall, nitrosative stress induced vasoplegia, autonomic dysfunction due to sympathetic overstimulation and β-adrenergic receptor desensitization, as well as microcirculatory dysfunction with capillary leakage, endothelial dysfunction, and procoagulant phenomena seem to complete the puzzle of SCM physiology [28,34]. As a consequence, the complexity of myocardial dysfunction in sepsis might be even more complicated by a profound autonomic dysregulation [35].
4. Echocardiographic Findings in Adult and Pediatric Sepsis
Non-invasive monitoring with transthoracic echocardiography seems to be part of precision-medicine strategies in adult and pediatric shock [36]. Bedside echocardiography might show variable abnormalities in septic patients and enables clinicians to profile the type of cardiogenic dysfunction (left, right, biventricular, regional, or apical wall motion abnormalities, e.g., in Takotsubo cardiomyopathy) [6]. Most studies primarily focus on left ventricular systolic or diastolic abnormalities. At the same time, right ventricular dysfunction might also have a significant and independent role in SCM and seems to be associated with worse outcome [37]. Moreover, echocardiography is a technique that enables a rapid estimation of the cause of low cardiac output (CO) and the identification of patients who require mechanical cardiac support [38]. Overall, most patients seem to present with global left ventricular (LV) hypokinesia upon admission, or this finding might even be unmasked after vasopressor support initiation. Other patients may show up with left ventricular dilatation with systolic dysfunction, while right ventricular (RV) dysfunction might also complicate the clinical course in a smaller subset of patients [29]. Left ventricular ejection fraction (LVEF) is commonly used for myocardial contractility estimation, but its dependency on afterload seems to limit its accuracy [4]. On the contrary, an extensive body of literature focuses on global longitudinal strain (GLS) as a more sensitive and specific parameter for SCM, and as a significant predictor of higher mortality [4].
When it comes to functional cardiac abnormalities in SCM, a hypodynamic or even hyperdynamic myocardial contractility response with preserved cardiac output (CO) in around 30-50% of patients might be noted in the acute phase [39]. One of the hallmark changes in SCM is diastolic dysfunction with LV dilatation and increased LV end-diastolic volume (LVEDV), despite low or normal filling pressures, which seems to act as a compensatory mechanism to preserve stroke volume. RV dysfunction is another common finding in approximately two-thirds of patients with SCM, and is probably associated with worse outcome [7,39]. It seems that the combination of decreased preload, increased RV afterload, and compromised RV contractility is the main reason why the RV cannot keep pace with the LV, despite ventricular interdependence in steady states [37].
Biventricular dysfunction seems to be common in SCM. In particular, LV systolic and diastolic dysfunction seem to be present in 50-60% of adult patients with sepsis, while RV dysfunction is present in 30-50% of cases [10,25]. Based on this, a recent study reported that 78% of adult patients had elevated EF and low afterload, while only 22% of cases presented with low EF [40]. In addition, it seems that LV diastolic dysfunction is implicated in the majority of cases, especially in adults, with recent studies reporting high incidence rates of more than 65-80% [25], while some researchers also report RV diastolic dysfunction in 35% of SCM cases [41,42]. Interestingly, there are multiple reports, especially in adults, supporting that a low LV ejection fraction (EF) combined with LV dilatation tends to correlate with a “paradoxical” lower mortality and better outcomes [43,44]. This paradox might be explained by the fact that vasoplegia and distributive shock (warm shock phenotype) may often pseudo-normalize a low EF and mask cardiac impairment, enabling a severely dysfunctional heart to pump a seemingly normal cardiac output, while less severe patients with not profound shock will tend to reveal their actual low EF [7,35]. Clinicians should also keep in mind that LV dysfunction may occur due to vasopressor-driven afterload increase, with dynamic obstruction by inotropic or vasopressor agents, and that RV dysfunction may be due to mechanical ventilation. It is also essential to carefully assess CO, as inotropic medications are only indicated if the cardiogenic shock is associated with low CO and hypoperfusion [38]. Echocardiography studies can roughly estimate cardiac output using left ventricular outflow tract velocity integral (LVOT VTI). The normal LVOT VTI in adults is above 18cm, while patients with SCM present with lower LVOT VTI, and a cutoff of less than 13.2cm has been associated with a higher risk for mortality [45,46].
Concerning pediatric echocardiographic patterns, studies in septic children have shown reversible left ventricular dysfunction and myocardial wall motion abnormalities [47]. Infants and young children with septic shock often seem to present with elevated parameters of afterload and low cardiac output, possibly following a cold shock pathway [3,48,49]. In a pediatric study with refractory septic shock, 72% of patients had LV dysfunction, while 63% had some degree of RV dysfunction [41]. Another study showed that 37% of septic children had isolated LV systolic dysfunction, 33% LV diastolic dysfunction, and 17% of cases had both LV systolic and diastolic dysfunction at admission. Multiple studies have also shown that serum troponin levels seem to be elevated in one-third of pediatric sepsis cases [14]. However, most studies highlight that the potential direct or indirect interactions between myocardial dysfunction and mechanical ventilation, pulmonary vascular resistance, hypoxemia or medications are currently incompletely understood [14].
Based on these observations, multiple studies postulate that conventional echocardiographic parameters evaluating cardiac function, like ejection fraction (EF), fractional shortening (FS), fractional area change (FAC) and tricuspid annular plane systolic excursion (TAPSE), might be misleading and do not reflect the actual underlying myocardial contractility, since they are dependent on preload and afterload, and often underestimate the severity of SCM [35]. On the other hand, emerging, objective echocardiographic techniques, like tissue Doppler imaging (TDI) and strain imaging with speckle-tracking echocardiography (STE), are currently under investigation and seem to detect early changes of myocardial contractility before conventional parameters [5,25]. Therefore, a growing body of current literature highlights that LVEF is a poor diagnostic tool and that myocardial strain measurements hold greater diagnostic and prognostic value [7]. Another study suggested that the RV wall strain might be the strongest predictor of mortality in SCM. Interestingly, conventional echocardiography seems to have a diagnostic ability of 33% and 32% for LV and RV dysfunction, respectively, while speckle tracking echocardiography revealed LV and RV dysfunction in 69% and 72% of cases, respectively [50]. Future research will likely shed light on the diagnostic value of myocardial strain imaging, informing appropriate therapeutic interventions for SCM.
5. Basic Hemodynamic Monitoring
Hemodynamic monitoring is a critical component of SCM management, serving in cardiac function and fluid status evaluation, fluid resuscitation, and vasopressor/inotropic therapy optimization, as well as monitoring response to interventions [51].
Several static hemodynamic parameters have been used for the assessment of patient volume status. Among these, heart rate (HR), blood pressure (BP), urine output, capillary refill time (CRT), serum lactate levels, central venous pressure (CVP), pulmonary capillary wedge pressure, cardiac output (CO), mixed venous saturation (SvO2) and venous-to-arterial carbon dioxide difference (Pv-aCO2) seem to be less specific and are not currently recommended as isolated modalities to direct the necessary interventions [2]. However, these indices have been proposed as alarming signs of hypoperfusion, guiding clinical interventions to improve tissue perfusion. SvO2 reflects tissue oxygen delivery and oxygen consumption. It is expected to be normal or elevated in septic patients. At the same time, a low SvO2 <70% may identify those patients in circulatory stress, who would benefit by increasing CO with fluids or inotropes, or by blood transfusions. Pv-aCO2 is a direct indicator of anaerobic metabolism with faster responses to resuscitation compared to lactate. Pv-aCO2 is inversely related to CO, and a high Pv-aCO2 (Pv-aCO2 >6 mmHg) may identify septic patients who are inadequately resuscitated [38,51]. Other studies have emphasized the importance of monitoring trends in lactate, as elevated serum lactate was a strong predictor of SCM [18]. Moreover, multiple biomarkers have shown significant correlations with myocardial dysfunction and the severity of septic shock. Elevated B-natriuretic peptide (BNP) is inversely correlated with fractional shortening and directly associated with the severity of sepsis, especially in the pediatric population. However, the diagnostic utility in adult sepsis has not been confirmed. Conversely, although cardiac troponin-T correlates well with myocardial dysfunction and mortality in adult sepsis, the utility of troponin measurement in pediatric septic shock prognostication is less clear [3].
On the other hand, dynamic parameters, such as the passive leg raising test (PLR), variations in inferior vena cava dimensions, stroke volume variation (SVV), and pulse pressure variation (PPV), are considered better indicators of fluid responsiveness, measuring the change in stroke volume in response to a preload fluid challenge. However, even these dynamic parameters are still debatable for their performance and applicability in septic patients, especially in children [2]. Even though specific goals in terms of macrohemodynamics seem to be easily achieved in sepsis, occult microcirculatory failure might be imminent, making up a strong determinant of the evolution of septic shock [17]. Therefore, evolving parameters of microcirculatory perfusion (sublingual microcirculatory alterations, tissue red blood cell perfusion) are currently analyzed for any clinically relevant benefits in patient outcomes [11].
6. Advanced Multimodal Hemodynamic Monitoring
Invasive, minimally invasive, and non-invasive advanced monitoring techniques are currently being evaluated regarding their performance in hemodynamic interpretations in adult and pediatric sepsis. Invasive and minimally invasive monitoring is increasingly being used to provide more stable and pluripotential information guiding management of septic shock [17,51]. Besides non-invasive assessments with echocardiography, multiple studies highlight the critical information provided by minimally invasive monitoring of cardiovascular performance, which enables the definition of every hemodynamic phenotype with objective and dynamic parameters [28,52,53]. Cardiac output monitoring devices, such as transpulmonary thermodilution (TPTD) devices like the pulse index continuous CO (PICCO), coupled with bedside echocardiography, are currently considered the initial monitoring modalities for patients with SCM, providing invaluable dynamic hemodynamic evaluations of fluid responsiveness or the risk of volume overload. TPTD offers calibrated measurements of CO and cardiac contractility, continuous estimations of SV and afterload parameters, static volumetric preload assessments (global end-diastolic volume/ GEDV), as well as valuable data on the severity of pulmonary edema, with extravascular lung water (EVLW) and vascular permeability indicators [19,38]. A recent study in critically ill children demonstrated that a decreased afterload assessment provided by TPTD (systemic vascular resistance/ SVR) was significantly associated with mortality in septic shock. In contrast, cardiac index was associated with mortality only in cardiogenic shock patients [19]. Other studies demonstrated that the agreement of CO measurements between echocardiography and TPTD was strong [54], even though variations in individual patients were considerable, suggesting that these two modalities should not be used interchangeably [53,55]. Concerning pulmonary edema estimations, even though elevated EVLW measurements in TPTD highly correlate with the amount of pulmonary fluid in adults, researchers have not confirmed this association in children [56]. In addition, current reference values measured for GEDV and EVLW do not apply to children, since measured GEDV values tend to be lower and EVLW values tend to be higher in young children [57].
Finally, studies in adults have indicated that patients with SCM might benefit from early invasive hemodynamic monitoring with a pulmonary artery catheter (PAC), which combines measurements of CO, pulmonary pressures, and SvO2 [6,38]. However, while it provides essential data, its use is not favored, especially in pediatric patients, as it has not been found to improve survival. At the same time, equally essential and reproducible information may also be provided by minimally invasive techniques. Current literature has also reported that TPTD stands up quite well to the gold standard of PAC, with the ability to discern changes in CO down to 12% [53,56]. However, some pitfalls of TPTD have been reported, since TPTD provides no direct measurements of the cardiac contractility, LV or RV filling pressures, and intracardiac shunts make this method highly unreliable due to recirculation of the infused ice-cold saline [53,58]. In addition, as already analyzed, a normal CO does not rule out SCM, especially in patients with low SVR. Therefore, a recent study suggested that cardiac output be assessed only by taking into account SVR (afterload) [35]. Moreover, arrhythmias, low sedation levels, changes in ventilator pressures, and tricuspid regurgitation may also affect CO measurements [55]. Increasing accuracy in measured CO has been reported with software updates in the latest TPTD machinery [59].
7. Current Treatment Concepts Based on Hemodynamic Monitoring
Given the marked heterogeneity of SCM, therapeutic strategies should be personalized to the underlying hemodynamic phenotype. Patients with preserved cardiac output and vasoplegia primarily require restoration of vascular tone, whereas patients with impaired myocardial contractility and low cardiac output may benefit from cautious inotropic support after preload and afterload optimization. Importantly, these phenotypes may evolve dynamically over the course of sepsis, highlighting the need for repeated hemodynamic evaluations [6,7,38]. Multiple studies advocate that early treatment of vasoplegia with norepinephrine seems to facilitate the increase of venous return, mean arterial pressure (MAP), and cardiac output, thus improving microcirculatory perfusion. Vasopressin, as an adjunct to norepinephrine, aims at further increasing MAP while sparing an additional adrenergic burden. There are no clear recommendations yet on other medications aiming at improving hemodynamics, like angiotensin II or methylene blue. When it comes to inodilators, low dose dobutamine seems to be the initial choice, followed by continuous assessments of its effects. Finally, current evidence favors the use of adrenergic modulation agents, like a2-agonists (dexmedetomidine), due to the anti-inflammatory impacts, beneficial microcirculatory actions, and attenuation of vasopressor requirements [11]. Notably, most therapeutic recommendations in SCM are derived from physiological rationale, observational studies or expert consensus, and require careful bedside interpretation, particularly in pediatric patients [11,38].
8. Refractory Septic Shock
Refractory septic shock is defined as elevated serum lactate >8mmol/L, along with vasoactive inotrope score (VIS) >200mcg/kg/min. Moreover, refractory shock may be suspected in those patients with normal SvO2 and Pv-aCO2, where microcirculatory and/or mitochondrial dysfunction will probably lead to a poorly responsive condition to macrohemodynamic therapeutic interventions [51]. Reversible causes or underlying cardiac pathologies (myocarditis, myocardial infarction, cardiomyopathy, congenital heart disease) should initially be ruled out. Echocardiography should always be stratified in refractory shock to rule out complications from high vasopressor support, like LV outflow obstruction [11]. Invasive cardiac support, like ventricular assist devices (VAD) or venous-arterial extracorporeal membrane oxygenation (VA-ECMO), might be considered as bridge therapies and seem to be life-saving in refractory septic shock cases [2].
9. Discussion
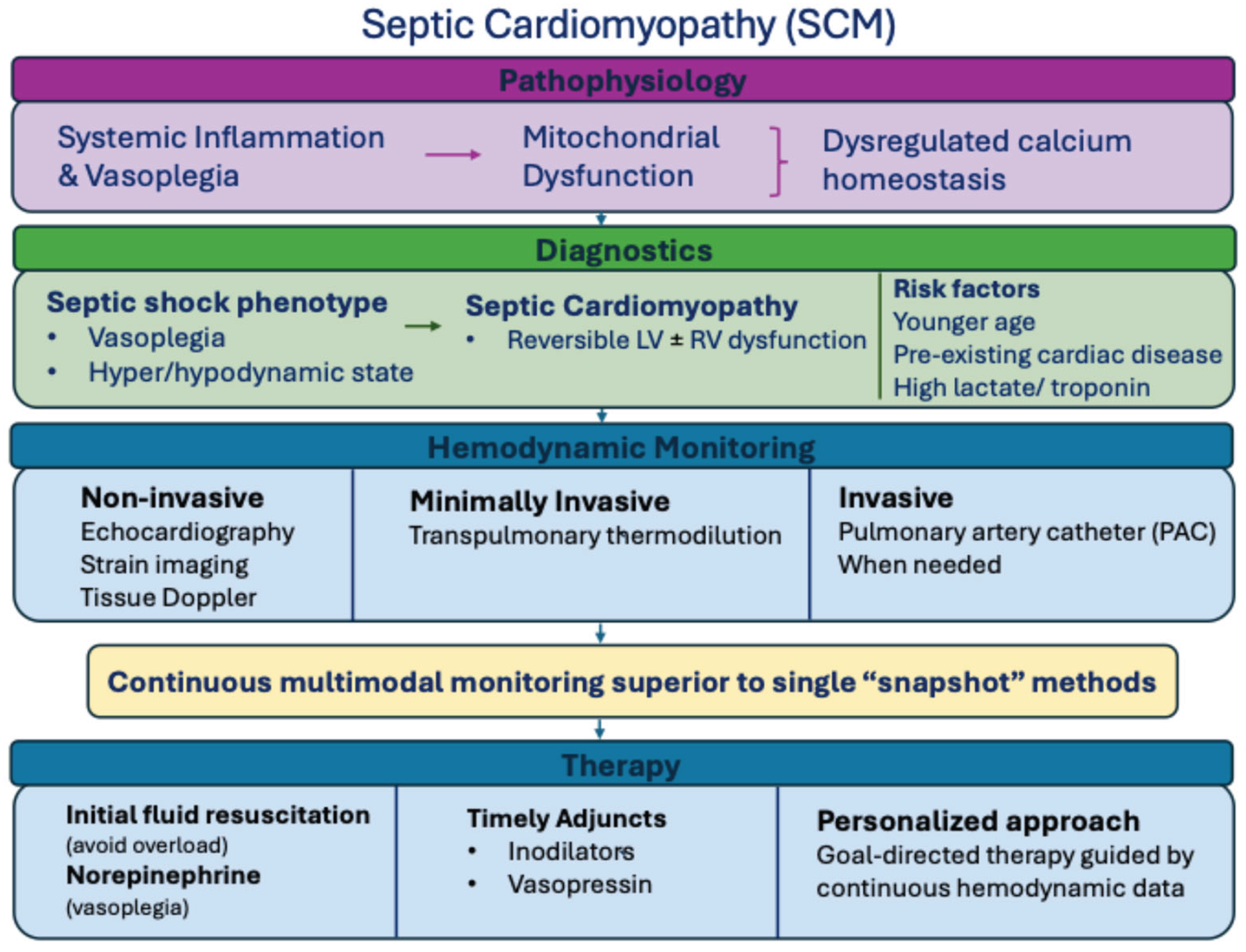
Septic cardiomyopathy represents a complex, heterogeneous and frequently underdiagnosed manifestation of sepsis, affecting both adult and pediatric populations. The present review highlights that myocardial dysfunction in sepsis cannot be understood as an isolated cardiac phenomenon, but rather as the integrated result of systemic inflammation, vasoplegia, autonomic dysregulation, microcirculatory failure and mitochondrial energetic impairment [4,7,28,34]. This multifactorial pathophysiology possibly explains the wide variability in reported prevalence, phenotypes and outcomes across studies [21,22,23,24]. As illustrated in Figure 1, the interaction between inflammatory, myocardial and circulatory abnormalities in sepsis highlights the need for integrated diagnostic and monitoring strategies.
Diagnostic challenges in SCM always remain, since traditional echocardiographic parameters, such as left ventricular ejection fraction (LVEF), are highly dependent on preload and afterload, possibly underestimating myocardial impairment [4,7,35,40]. This limitation may partially explain the paradoxical observation that reduced LVEF accompanied by ventricular dilatation has been associated with better outcomes in some studies, potentially reflecting preserved preload reserve and adaptive myocardial responses rather than irreversible myocardial failure [43,44]. Consequently, reliance on isolated static echocardiographic measurements is possibly insufficient for accurate characterization of SCM [35]. Emerging echocardiographic techniques, including tissue Doppler imaging and speckle-tracking-derived myocardial strain, seem to be more sensitive in detecting early and subtle myocardial abnormalities and may offer superior prognostic value compared to conventional indices [4,5,25]. In particular, global longitudinal strain and right ventricular strain have demonstrated consistent associations with mortality in observational studies of septic patients [50]. However, the clinical integration of strain imaging is currently limited due to operator variability and lack of standardized reference values, especially in pediatric populations. Therefore, while myocardial strain imaging holds promise as a diagnostic tool, its routine use is currently complementary [5,14].
Hemodynamic monitoring constitutes another cornerstone in SCM. Static macrohemodynamic parameters, such as heart rate, blood pressure, central venous pressure, or even cardiac output, often fail to reflect tissue perfusion and myocardial performance in sepsis [2,11,38,51]. Multimodal approaches combining echocardiography, fluid responsiveness dynamic indices and minimal invasive cardiac output monitoring may provide a more thorough understanding of the variety of hemodynamic phenotypes [17,36,38]. Transpulmonary thermodilution techniques offer valuable information regarding preload, afterload, cardiac output and pulmonary edema, and seem to show reasonable agreement with echocardiographic parameters [19,54,55]. However, their interpretation requires caution, particularly in pediatric patients, due to limited normative data, and large interindividual or methodological variability [56,57].
Importantly, advanced monitoring does not always lead to improved outcomes, unless embedded within a personalized and pathophysiology-guided clinical context [11,38]. Current evidence does not seem to support uniform resuscitation targets for all septic patients, while indiscriminate fluid loading or inotropic support may exacerbate myocardial stress, pulmonary edema, or ventricular-arterial uncoupling [12,13,35]. Instead, clinical decisions should be guided by repeated or continuous assessments of cardiac function, systemic vascular resistance and tissue perfusion, recognizing that a “normal” cardiac output may mask significant myocardial dysfunction in vasoplegic states [7,35,38].
10. Limitations
Substantial knowledge gaps still remain despite increasing recognition of SCM, especially regarding specific diagnostic criteria and treatment strategies, which mostly derive from small, single-center, observational studies or expert consensus [4,7,24]. Adult guidelines are frequently also implemented in pediatric patients, despite important developmental and physiological differences in myocardial reserve and vascular responses [3,14,16]. Future research should prioritize prospective, multicentre studies, to establish standardized definitions and to evaluate advanced diagnostic modalities and phenotype-guided therapeutic interventions. Crucially, interventional studies will also determine whether targeted management based on echocardiographic and hemodynamic profiling could be associated with more favourable outcomes in SCM.
11. Conclusions
Septic cardiomyopathy often complicates the course of sepsis and is characterized by diverse phenotypic expressions involving left, right, or biventricular dysfunction. A unified consensus and diagnostic criteria for septic cardiomyopathy remains a challenging issue, due to the dynamic interaction between intrinsic myocardial depression and sepsis-related alterations in preload, afterload and vascular tone. Both non-invasive and minimally invasive techniques seem to provide complementary information that may facilitate more precise hemodynamic phenotyping for SCM. However, the clinical value of these tools depends on careful interpretation, based on individualized and physiology-based interventions rather than protocolized resuscitation. Future research on this field will elucidate whether specific echocardiographic imaging techniques, such as myocardial strain imaging, in combination with continuous transpulmonary thermodilution monitoring, might guide more targeted therapeutic strategies for septic shock and septic cardiomyopathy. Until such evidence is available, clinicians should maintain a high index of suspicion for this under-recognized condition, especially in septic patients unresponsive to initial fluid and vasopressor therapy, and adopt a personalized, multimodal hemodynamic assessment for both adult and pediatric septic patients.
Author Contributions
Conceptualization, M.M. and I.S.; methodology, M.M., D.E. and B.P.; software, M.M. and D.E..; validation, M.M., B.G. and I.S.; formal analysis, M.M.; investigation, resources and data curation, M.M. and I.S.; writing—original draft preparation, M.M.; writing—review and editing, B.G., and I.S.; visualization, I.S.; supervision, M.M. and I.S.; project administration, M.M. and I.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
No new data were created.
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.”
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BP | Blood pressure |
| CO | Cardiac Output |
| CRT | Capillary refill time |
| CVP | Central venous pressure |
| DO2 | Oxygen Delivery |
| EVLW | Extravascular lung water |
| FAC | Fractional area change |
| FS | Fractional shortening |
| GEDV | Global end-diastolic volume |
| GLS | Global longitudinal strain |
| HR | Heart rate |
| ICU | Intensive Care Unit |
| LVEF | Left ventricular ejection fraction |
| LV | Left ventricle/ventricular |
| MAP | Mean arterial pressure |
| PAC | Pulmonary artery catheter |
| Pv-aCO2 | Venous-to-arterial carbon dioxide difference |
| RV | Right ventricle/ventricular |
| SCM | Sepsis-induced cardiomyopathy |
| STE | Speckle-tracking echocardiography |
| TAPSE | Tricuspid annular plane systolic excursion |
| TDI | Tissue Doppler imaging |
| TPTD | Transpulmonary thermodilution |
| VA-ECMO | Veno-arterial extracorporeal membrane oxygenation |
| VAD | Ventricular assist device |
| VIS | Vasoactive inotrope score |
| SvO2 | Mixed venous oxygen saturation |
| PICCO | Pulse index continuous cardiac output |
References
- Beesley, SJ; Weber, G; Sarge, T; Nikravan, S; Grissom, CK; Lanspa, MJ; et al. Septic Cardiomyopathy. Critical Care Medicine 2018, 46, 625. [Google Scholar] [CrossRef]
- Gupta, S; Sankar, J. Advances in Shock Management and Fluid Resuscitation in Children. Indian J Pediatr 2023, 90, 280–8. [Google Scholar] [CrossRef]
- Lautz, AJ; Zingarelli, B. Age-Dependent Myocardial Dysfunction in Critically Ill Patients: Role of Mitochondrial Dysfunction. Int J Mol Sci 2019, 20, 3523. [Google Scholar] [CrossRef] [PubMed]
- Boissier, F; Aissaoui, N. Septic cardiomyopathy: Diagnosis and management. J Intensive Med 2022, 2, 8–16. [Google Scholar] [CrossRef]
- Chan, JC; Menon, AP; Rotta, AT; Choo, JTL; Hornik, CP; Lee, JH. Use of Speckle-Tracking Echocardiography in Septic Cardiomyopathy in Critically Ill Children: A Narrative Review. Crit Care Explor 2024, 6, e1114. [Google Scholar] [CrossRef] [PubMed]
- Sato, R; Hasegawa, D; Guo, S; Nuqali, AE; Moreno, JEP. Sepsis-induced cardiogenic shock: controversies and evidence gaps in diagnosis and management. J Intensive Care 2025, 13, 1. [Google Scholar] [CrossRef]
- L’Heureux, M; Sternberg, M; Brath, L; Turlington, J; Kashiouris, MG. Sepsis-Induced Cardiomyopathy: a Comprehensive Review. Curr Cardiol Rep 2020, 22, 35. [Google Scholar] [CrossRef] [PubMed]
- Sato, R; Kuriyama, A; Takada, T; Nasu, M; Luthe, SK. Prevalence and risk factors of sepsis-induced cardiomyopathy: A retrospective cohort study. Medicine (Baltimore) 2016, 95, e5031. [Google Scholar] [CrossRef]
- Jeong, HS; Lee, TH; Bang, CH; Kim, J-H; Hong, SJ. Risk factors and outcomes of sepsis-induced myocardial dysfunction and stress-induced cardiomyopathy in sepsis or septic shock: A comparative retrospective study. Medicine (Baltimore) 2018, 97, e0263. [Google Scholar] [CrossRef]
- Lukić, I; Mihić, D; Varžić, SC; Relatić, KS; Zibar, L; Loinjak, D; et al. Septic Cardiomyopathy. Rev Cardiovasc Med 2024, 25, 23. [Google Scholar] [CrossRef]
- Bakker, J; Kattan, E; Annane, D; Castro, R; Cecconi, M; De Backer, D; et al. Current practice and evolving concepts in septic shock resuscitation. Intensive Care Med 2022, 48, 148–63. [Google Scholar] [CrossRef]
- Hernández, G; Ospina-Tascón, GA; Damiani, LP; Estenssoro, E; Dubin, A; Hurtado, J; et al. Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients With Septic Shock: The ANDROMEDA-SHOCK Randomized Clinical Trial. JAMA 2019, 321, 654–64. [Google Scholar] [CrossRef] [PubMed]
- Guarracino, F; Bertini, P; Pinsky, MR. Heterogeneity of Cardiovascular Response to Standardized Sepsis Resuscitation. Crit Care 2020, 24, 99. [Google Scholar] [CrossRef]
- Raj, S; Killinger, JS; Gonzalez, JA; Lopez, L. Myocardial dysfunction in pediatric septic shock. J Pediatr 2014, 164, 72–77.e2. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J; Carcillo, JA; Choong, K; Cornell, T; Decaen, A; Deymann, A; et al. Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine. Crit Care Med 2009, 37, 666–88. [Google Scholar] [CrossRef] [PubMed]
- Schlapbach, LJ; Watson, RS; Sorce, LR; Argent, AC; Menon, K; Hall, MW; et al. International Consensus Criteria for Pediatric Sepsis and Septic Shock. JAMA 2024, 331, 665–74. [Google Scholar] [CrossRef]
- Fernández-Sarmiento, J; Carcillo, JA; Díaz Del Castillo, AME; Barrera, P; Orozco, R; Rodríguez, MA; et al. Venous-arterial CO2 difference in children with sepsis and its correlation with myocardial dysfunction. Qatar Med J 2019, 2019, 18. [Google Scholar] [CrossRef]
- Swami, VS; LA, V; Ghosh, S; Reddy, M. Sepsis-Induced Myocardial Dysfunction in Pediatric Septic Shock: Prevalence, Predictors, and Outcome-A Prospective Observational Study. J Pediatr Intensive Care 2024, 13, 87–94. [Google Scholar] [CrossRef]
- Lee, E-P; Hsia, S-H; Lin, J-J; Chan, O-W; Lee, J; Lin, C-Y; et al. Hemodynamic Analysis of Pediatric Septic Shock and Cardiogenic Shock Using Transpulmonary Thermodilution. Biomed Res Int 2017, 2017, 3613475. [Google Scholar] [CrossRef]
- Liang, Y-W; Zhu, Y-F; Zhang, R; Zhang, M; Ye, X-L; Wei, J-R. Incidence, prognosis, and risk factors of sepsis-induced cardiomyopathy. World J Clin Cases 2021, 9, 9452–68. [Google Scholar] [CrossRef]
- Pulido, JN; Afessa, B; Masaki, M; Yuasa, T; Gillespie, S; Herasevich, V; et al. Clinical Spectrum, Frequency, and Significance of Myocardial Dysfunction in Severe Sepsis and Septic Shock. Mayo Clinic Proceedings 2012, 87, 620–8. [Google Scholar] [CrossRef]
- Yu, Y-Y; Wang, R; Chen, G-Q; Gui, Y-F; Ma, J; Ma, J-H; et al. Mechanisms and Targeted Therapeutic Strategies in Sepsis-Induced Myocardial Dysfunction: The Role of NLRP3 Inflammasome-Mediated Inflammation. J Inflamm Res 2025, 18, 8875–97. [Google Scholar] [CrossRef] [PubMed]
- Beesley, SJ; Weber, G; Sarge, T; Nikravan, S; Grissom, CK; Lanspa, MJ; et al. Septic Cardiomyopathy. Crit Care Med 2018, 46, 625–34. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, D; Ishisaka, Y; Maeda, T; Prasitlumkum, N; Nishida, K; Dugar, S; et al. Prevalence and Prognosis of Sepsis-Induced Cardiomyopathy: A Systematic Review and Meta-Analysis. J Intensive Care Med 2023, 38, 797–808. [Google Scholar] [CrossRef]
- Lu, N-F; Niu, H-X; Liu, A-Q; Chen, Y-L; Liu, H-N; Zhao, P-H; et al. Types of Septic Cardiomyopathy: Prognosis and Influencing Factors - A Clinical Study. Risk Manag Healthc Policy 2024, 17, 1015–25. [Google Scholar] [CrossRef]
- Jain, A; Sankar, J; Anubhuti, A; Yadav, DK; Sankar, MJ. Prevalence and Outcome of Sepsis-induced Myocardial Dysfunction in Children with “Sepsis” “With” and ’Without Shock’-A Prospective Observational Study. J Trop Pediatr 2018, 64, 501–9. [Google Scholar] [CrossRef]
- Ceneviva, G; Paschall, JA; Maffei, F; Carcillo, JA. Hemodynamic support in fluid-refractory pediatric septic shock. Pediatrics 1998, 102, e19. [Google Scholar] [CrossRef]
- Carbone, F; Liberale, L; Preda, A; Schindler, TH; Montecucco, F. Septic Cardiomyopathy: From Pathophysiology to the Clinical Setting. Cells 2022, 11, 2833. [Google Scholar] [CrossRef] [PubMed]
- Zanotti-Cavazzoni, SL; Hollenberg, SM. Cardiac dysfunction in severe sepsis and septic shock. Curr Opin Crit Care 2009, 15, 392–7. [Google Scholar] [CrossRef]
- Stanzani, G; Duchen, MR; Singer, M. The role of mitochondria in sepsis-induced cardiomyopathy. Biochim Biophys Acta Mol Basis Dis 2019, 1865, 759–73. [Google Scholar] [CrossRef]
- Fujimura, K; Karasawa, T; Komada, T; Yamada, N; Mizushina, Y; Baatarjav, C; et al. NLRP3 inflammasome-driven IL-1β and IL-18 contribute to lipopolysaccharide-induced septic cardiomyopathy. J Mol Cell Cardiol 2023, 180, 58–68. [Google Scholar] [CrossRef]
- Zheng, Y; Lin, J; Wan, G; Gu, X; Ma, J. Macrophage Notch1 drives septic cardiac dysfunction by impairing mitophagy and promoting NLRP3 activation. Biology Direct 2025, 20, 65. [Google Scholar] [CrossRef]
- Muehlberg, F; Blaszczyk, E; Will, K; Wilczek, S; Brederlau, J; Schulz-Menger, J. Characterization of critically ill patients with septic shock and sepsis-associated cardiomyopathy using cardiovascular MRI. ESC Heart Fail 2022, 9, 2147–56. [Google Scholar] [CrossRef]
- Hollenberg, SM; Singer, M. Pathophysiology of sepsis-induced cardiomyopathy. Nat Rev Cardiol 2021, 18, 424–34. [Google Scholar] [CrossRef]
- Werdan, K; Oelke, A; Hettwer, S; Nuding, S; Bubel, S; Hoke, R; et al. Septic cardiomyopathy: hemodynamic quantification, occurrence, and prognostic implications. Clin Res Cardiol 2011, 100, 661–8. [Google Scholar] [CrossRef]
- Ranjit, S; Aram, G; Kissoon, N; Ali, MK; Natraj, R; Shresti, S; et al. Multimodal monitoring for hemodynamic categorization and management of pediatric septic shock: a pilot observational study*. Pediatr Crit Care Med 2014, 15, e17-26. [Google Scholar] [CrossRef] [PubMed]
- Lanspa, MJ; Cirulis, MM; Wiley, BM; Olsen, TD; Wilson, EL; Beesley, SJ; et al. Right Ventricular Dysfunction in Early Sepsis and Septic Shock. Chest 2021, 159, 1055–63. [Google Scholar] [CrossRef]
- De Backer, D; Cecconi, M; Chew, MS; Hajjar, L; Monnet, X; Ospina-Tascón, GA; et al. A plea for personalization of the hemodynamic management of septic shock. Crit Care 2022, 26, 372. [Google Scholar] [CrossRef]
- Furian, T; Aguiar, C; Prado, K; Ribeiro, RVP; Becker, L; Martinelli, N; et al. Ventricular dysfunction and dilation in severe sepsis and septic shock: relation to endothelial function and mortality. J Crit Care 2012, 27, 319.e9–15. [Google Scholar] [CrossRef] [PubMed]
- Boissier, F; Razazi, K; Seemann, A; Bedet, A; Thille, AW; de Prost, N; et al. Left ventricular systolic dysfunction during septic shock: the role of loading conditions. Intensive Care Med 2017, 43, 633–42. [Google Scholar] [CrossRef] [PubMed]
- Williams, FZ; Sachdeva, R; Travers, CD; Walson, KH; Hebbar, KB. Characterization of Myocardial Dysfunction in Fluid- and Catecholamine-Refractory Pediatric Septic Shock and Its Clinical Significance. J Intensive Care Med 2019, 34, 17–25. [Google Scholar] [CrossRef]
- Sankar, J; Das, RR; Jain, A; Dewangan, S; Khilnani, P; Yadav, D; et al. Prevalence and outcome of diastolic dysfunction in children with fluid refractory septic shock--a prospective observational study. Pediatr Crit Care Med 2014, 15, e370-378. [Google Scholar] [CrossRef]
- Kakihana, Y; Ito, T; Nakahara, M; Yamaguchi, K; Yasuda, T. Sepsis-induced myocardial dysfunction: pathophysiology and management. J Intensive Care 2016, 4, 22. [Google Scholar] [CrossRef]
- Merx, MW; Weber, C. Sepsis and the Heart. Circulation 2007, 116, 793–802. [Google Scholar] [CrossRef]
- Porter, TR; Shillcutt, SK; Adams, MS; Desjardins, G; Glas, KE; Olson, JJ; et al. Guidelines for the use of echocardiography as a monitor for therapeutic intervention in adults: a report from the American Society of Echocardiography. J Am Soc Echocardiogr 2015, 28, 40–56. [Google Scholar] [CrossRef] [PubMed]
- Jentzer, JC; Tabi, M; Wiley, BM; Singam, NSV; Anavekar, NS. Echocardiographic Correlates of Mortality Among Cardiac Intensive Care Unit Patients With Cardiogenic Shock. Shock 2022, 57, 336–43. [Google Scholar] [CrossRef]
- Fenton, KE; Sable, CA; Bell, MJ; Patel, KM; Berger, JT. Increases in serum levels of troponin I are associated with cardiac dysfunction and disease severity in pediatric patients with septic shock. Pediatr Crit Care Med 2004, 5, 533–8. [Google Scholar] [CrossRef] [PubMed]
- Deep, A; Goonasekera, CDA; Wang, Y; Brierley, J. Evolution of haemodynamics and outcome of fluid-refractory septic shock in children. Intensive Care Med 2013, 39, 1602–9. [Google Scholar] [CrossRef]
- Abdalaziz, FA; Algebaly, HAF; Ismail, RI; El-Sherbini, SA; Behairy, A. The use of bedside echocardiography for measuring cardiac index and systemic vascular resistance in pediatric patients with septic shock. Rev Bras Ter Intensiva 2018, 30, 460–70. [Google Scholar] [CrossRef]
- Orde, SR; Pulido, JN; Masaki, M; Gillespie, S; Spoon, JN; Kane, GC; et al. Outcome prediction in sepsis: speckle tracking echocardiography based assessment of myocardial function. Crit Care 2014, 18, R149. [Google Scholar] [CrossRef] [PubMed]
- Pinsky, MR; Cecconi, M; Chew, MS; De Backer, D; Douglas, I; Edwards, M; et al. Effective hemodynamic monitoring. Crit Care 2022, 26, 294. [Google Scholar] [CrossRef]
- Giraud, R; Siegenthaler, N; Merlani, P; Bendjelid, K. Reproducibility of transpulmonary thermodilution cardiac output measurements in clinical practice: a systematic review. J Clin Monit Comput 2017, 31, 43–51. [Google Scholar] [CrossRef]
- Pernbro, F; Wåhlander, H; Romlin, B. Haemodynamic monitoring after paediatric cardiac surgery using echocardiography and PiCCO. Cardiol Young 2024, 34, 2636–40. [Google Scholar] [CrossRef]
- Zhang, Y; Wang, Y; Shi, J; Hua, Z; Xu, J. Cardiac output measurements via echocardiography versus thermodilution: A systematic review and meta-analysis. PLoS One 2019, 14, e0222105. [Google Scholar] [CrossRef]
- Wetterslev, M; Møller-Sørensen, H; Johansen, RR; Perner, A. Systematic review of cardiac output measurements by echocardiography vs. thermodilution: the techniques are not interchangeable. Intensive Care Med 2016, 42, 1223–33. [Google Scholar] [CrossRef] [PubMed]
- Lemson, J; van Die, LE; Hemelaar, AEA; van der Hoeven, JG. Extravascular lung water index measurement in critically ill children does not correlate with a chest x-ray score of pulmonary edema. Crit Care 2010, 14, R105. [Google Scholar] [CrossRef]
- Grindheim, G; Eidet, J; Bentsen, G. Transpulmonary thermodilution (PiCCO) measurements in children without cardiopulmonary dysfunction: large interindividual variation and conflicting reference values. Paediatr Anaesth 2016, 26, 418–24. [Google Scholar] [CrossRef] [PubMed]
- Monnet, X; Persichini, R; Ktari, M; Jozwiak, M; Richard, C; Teboul, J-L. Precision of the transpulmonary thermodilution measurements. Crit Care 2011, 15, R204. [Google Scholar] [CrossRef]
- Slagt, C; de Leeuw, MA; Beute, J; Rijnsburger, E; Hoeksema, M; Mulder, JWR; et al. Cardiac output measured by uncalibrated arterial pressure waveform analysis by recently released software version 3.02 versus thermodilution in septic shock. J Clin Monit Comput 2013, 27, 171–7. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Integrated overview of septic cardiomyopathy, serving as a conceptual framework. Systemic inflammation triggers myocardial dysfunction, requiring careful diagnostic steps, multimodal hemodynamic monitoring, and tiered therapeutic strategies.
Figure 1.
Integrated overview of septic cardiomyopathy, serving as a conceptual framework. Systemic inflammation triggers myocardial dysfunction, requiring careful diagnostic steps, multimodal hemodynamic monitoring, and tiered therapeutic strategies.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



