
Submitted:
07 January 2026
Posted:
08 January 2026
You are already at the latest version
Abstract
Physical activity (PA) improves health and well-being, and helps prevent long-term conditions. Yet opportunities to be active are not evenly distributed, with social, economic, and environmental disadvantages constraining access to PA among populations who may benefit most. Since the extent to which PA interventions incorporate equity considerations remains insufficiently characterised, risking exacerbation of health inequity, this scoping review aims to synthesise trial evidence on interventions of PA to improve health outcomes in populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks. PubMed, Web of Science, and Scopus were searched for randomised controlled trials of PA interventions with at-risk populations published between 2020 and 2025. Study characteristics, intervention design, and equity-relevant factors were extracted. Two reviewers independently screened and synthesised findings narratively. Results indicate that of 2,480 articles identified, 23 trials met eligibility criteria. Most reported positive effect of PA on health outcomes amongst at-risk populations, including weight loss, improved motor skills and gait speed, reduced anxiety and PTSD, and fewer fractures or hospital visits. Interventions commonly included strength and balance training, group exercise, stretching, and aerobic fitness. UK-based studies and subgroup analyses by e.g. sex or age were largely absent, and many populations at risk of health inequity were underrepresented. Explicit equity considerations throughout design, implementation, or evaluation were rare across trials and few assessed differential effects between social or economic groups. Integrating equity frameworks and engaging with at-risk populations is recommended in future physical activity interventions to mitigate exacerbation of health inequity.
Keywords:
physical activity
; exercise
; interventions
; inequality
; equity
Contribution to Health Promotion
- This review identifies populations that are underrepresented in physical activity research to promote health, including ethnic minorities, people with long-term conditions, and low-income individuals. By mapping which populations are assessed and overlooked, it provides an equity-oriented evidence base to inform the design of future interventions.
- The findings inform policy and practice by highlighting that greater attention to intersectionality and co-production is needed in physical activity research to reach populations at risk of health inequity. By emphasising the importance of inclusive and scalable interventions, this review aligns with health promotion principles that support populations to increase control over their health.
Background
Physical activity (PA), defined as “any bodily movement produced by skeletal muscles that requires energy expenditure” (World Health Organisation, 2024), is an established intervention for preventing and managing long-term conditions (LTCs). However, only 69% of the world’s population meets recommended PA guidelines of 150–300 minutes of moderate or 75–150 minutes of vigorous activity per week (Kohl et al., 2012; Piercy et al., 2018), despite higher dosages being associated with greater health benefits (Celis-Morales et al., 2012; Fukushima et al., 2024; Lee et al., 2022; Lopez et al., 2019). Regular PA is linked with a 30–40% reduction in all-cause mortality, with adoption later in life still associated with a 20–25% reduction (Yu et al., 2025). Benefits extend across cardiovascular disease, type 2 diabetes, some cancers, and mental health (Mahindru et al., 2023; Pearce et al., 2025; Wahid et al., 2016; Yang et al., 2024; Yu et al., 2025).
Physical inactivity contributes to approximately one in six deaths in the UK, over 5 million global premature deaths annually (Lee et al., 2012), and is associated with an estimated annual cost of £7.4 billion including £0.9 billion to the NHS (Government UK, 2023). Yet engagement in PA is not evenly distributed. Inequity by age, sex, socioeconomic position, disability, ethnicity, and geography persists, and these factors intersect to shape access. Individuals experiencing LTCs, socioeconomic disadvantage, or constrained local environments frequently face barriers such as limited facilities, transport challenges, financial pressures, and competing health needs (Avraham et al., 2024; Bantham et al., 2021; Guthold et al., 2016). Consequently, populations who may benefit most from PA interventions often have the least opportunity to participate. Where interventions do not explicitly address equity, differential uptake and outcomes may contribute to “intervention-generated inequality” (Lorenc et al., 2013).
Frameworks have been developed to support systematic assessment of equity within health research. The PROGRESS-Plus framework, endorsed by the Cochrane Methods Equity Group, outlines domains of social stratification including place of residence (P), race/ethnicity/culture/language (R), occupation (O), gender/sex (G), religion (R), education (E), socioeconomic status (S) and social capital (S), with the “Plus” component capturing additional context-specific characteristics such as age, disability, sexual orientation and migration status (Oliver et al., 2008). The CORE20PLUS5 framework established by NHS England similarly identifies the most deprived 20% of the population (CORE20), five clinical priority areas (maternity, early cancer, COPD, severe mental illness, and hypertension), and additional groups at risk of inequity such as people experiencing homelessness, migrants or refugees, individuals with multiple LTCs, ethnic minorities, LGBTQ+ communities, people with experience of substance misuse or the justice system, and individuals living in underserved rural or urban areas (NHS England, 2021).
Although these frameworks provide structured approaches for examining equity, their application within PA interventions has not been systematically characterised. Limited understanding of how contemporary PA trials incorporate equity considerations restricts the ability to evaluate whether at-risk populations are effectively included and supported. This study therefore aims to synthesise trial evidence on interventions of physical activity to improve health outcomes in populations at risk of health inequity, as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks.
Methods
Design
This scoping review followed a standardised methodological framework (Arksey and O’Malley, 2005; Levac et al., 2010), adhering to the Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) (Tricco et al., 2018) (App. 1).
Eligibility Criteria
Eligibility criteria were defined a priori.
Inclusion criteria:
- Population – adults and children from marginalised socioeconomic groups or health backgrounds as defined by PROGRESS-Plus and CORE20PLUS5 frameworks.
- Interventions – interventions with a described PA component aimed at promoting health.
- Comparators – any comparator (usual care, no intervention, or alternative PA intervention).
- Study design – full randomised controlled trials.
- Outcomes – any health outcome.
- Publication characteristics – peer-reviewed journal articles published between January 2020 and October 2025 in English.
Exclusion criteria:
- Population – non-human or populations not listed in equity frameworks (e.g. not income deprived, from an ethnic/religious minority, immigrant, in a rural area, older, disabled, traveller, LGBTQ+, pregnant, a cancer or respiratory/heart disease patient, mentally ill, in the justice system, with a history of substance misuse, or homeless).
- Interventions – interventions not utilising PA aimed at promoting health.
- Comparators – studies not reporting comparators.
- Study design – any design other than full randomised controlled trials.
- Outcomes – studies not reporting health outcomes.
- Publication characteristics – non-peer-reviewed sources, publications in languages other than English, studies carried out before 2020.
Search Strategy
PubMed, Web of Science, and Scopus were searched for articles published between 1 January 2015 and 1 October 2025, later refining the scope to include only full randomised controlled trials from 1 January 2020 to 1 October 2025. The search strategy, developed with input from an information specialist, combined terms across three core concepts:
- Physical activity (PA) – including exercise, sport, fitness, movement, walking, cycling, and active travel.
- Populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks – including disadvantaged, underserved, deprived, low-income, marginalised, minority, migrant, refugee, homeless, learning disabled, and queer.
- Study design – including randomised controlled trial, clinical trial, and pragmatic trial.
Both controlled vocabulary (e.g., MeSH and Emtree headings) and free-text keywords were used, with strategies adapted for each database’s indexing system. Grey literature was also searched. Full search terms are provided in Appendix 2.
Study Selection
Search results were imported into Rayyan for duplicate removal and screening. Titles and abstracts were independently screened by two reviewers, followed by full-text screening, with disagreements resolved through discussion. A PRISMA flow diagram summarises the selection process (Figure 1).
Data Extraction
Data was extracted into a piloted standardised form and verified by a second reviewer. Extraction focused on study characteristics (author, year, population), intervention design, co-production, study duration, comparators, outcome measures, subgroup analysis, key findings, study effects, and study limitations. Which populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks were included was also assessed.
Data Synthesis
Given the heterogeneity in interventions, populations, and outcome measures, findings were synthesised narratively following the Synthesis Without Meta-analysis (SWiM) guideline (Campbell et al., 2020), focusing on the extent to which recent PA interventions include at-risk populations.
Results
Our search identified 2,480 articles, of which 23 were eligible and included in this review, with no additional articles identified through grey literature (Figure 1).
Study Characteristics
Sample sizes ranged from 30 to over 30,000 participants, with most (n = 16) enrolling between 30 and 150. Study duration ranged from eight to 113 weeks, with a mean of 29 weeks. Most studies were conducted in high-income countries, predominantly the USA (n = 5), followed by Taiwan (n = 3), South Korea (n = 2), Germany (n = 2), and Greece (n = 2). Spain, Slovenia, and Denmark had one study each. The remainder were from middle-income countries: China (n = 2), Myanmar (n = 1), Iran (n = 1), South Africa (n = 1), and Nigeria (n = 1). No UK-based studies met eligibility criteria (Table 1).
Intervention Content
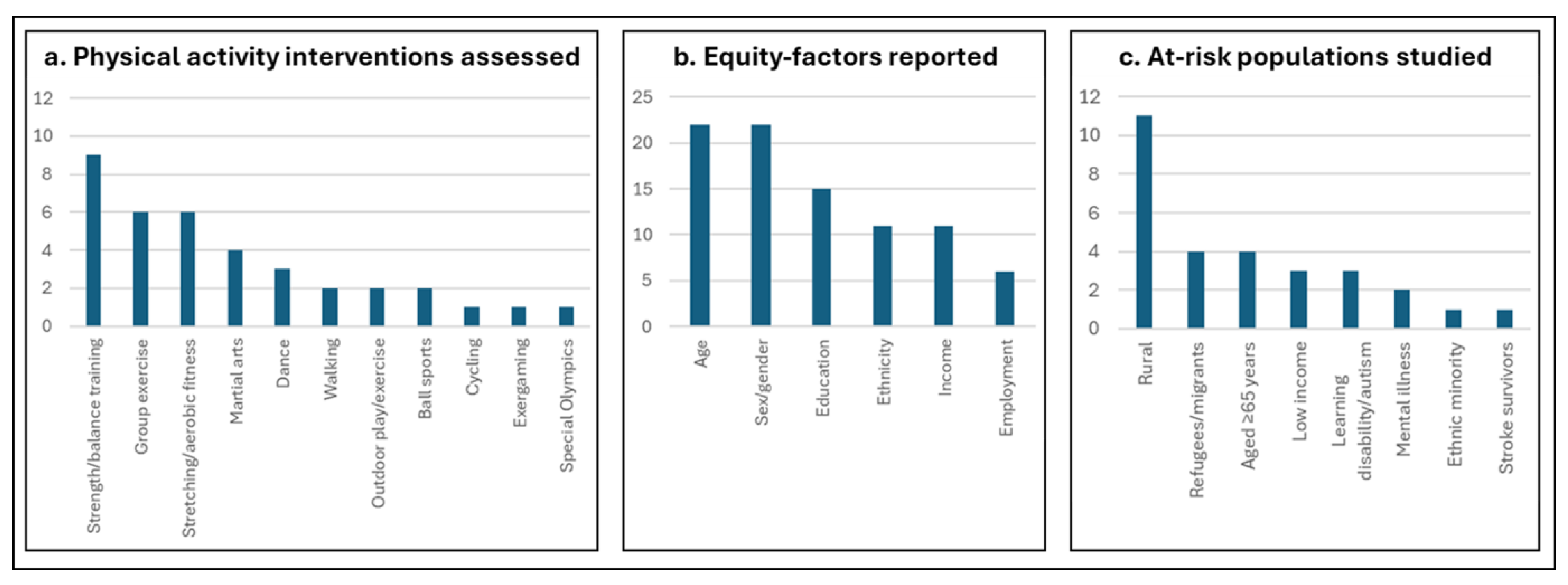
Most studies examined a PA-only intervention to improve health outcomes (n = 11), followed by a programme combining PA with health education or nutritional support (n = 9), and a combined PA and psychosocial intervention (including counselling, self-efficacy work, or behavioural work) (n = 3). In several, the intervention involved multiple PA components (n = 11). These included predominantly strength or balance training, followed by group exercise classes and stretching or aerobic fitness, martial arts, and then dance, walking, and outdoor activity (Figure 2a, Table 1). Specifics on the exact activities performed alone or in groups were often lacking, but one example of strength and balance training involved weekly sessions with three sets of 15 seated repetitions targeting functional muscle groups using different strength resistance bands, following a 10-minute warm-up and followed by a 10-minute cool-down [ID2]. Stretching and aerobic fitness may involve 10-minute sets of moderate intensity jumping, running in place, movement, and side shuffles at 65–85% of maximum heart rate three times a week [ID7]. Lastly, martial arts often involved Tai Chi up to twice a week, a multimodal mind-body exercise combining physical, meditative, cognitive, and social aspects [ID17].
Health Outcomes
Health outcome measures varied across trials, with 11 studies including self-reported outcomes such as quality of life, mental health symptoms, self-efficacy, dietary intake, pain, and disability. Three used standardised surveys or questionnaires with rating scales exclusively (Revised Impact of Event Scale, Patient Health Questionnaire-9, General Anxiety Disorder-5, Perceived Stress Scale-10, WHO Well-being Index-5, Short Form-12, Healthy Eating Index-2015, Rapid Eating Assessment for Participants-S, and Hausa Pain and Belief Scales) [ID5,8,13], while remaining studies incorporated at least one physiological measure. Most assessed physical function (n = 8) and body composition (n = 6), with other outcomes including acute care utilisation, physical performance or skill, muscle mass, and risk factors for cardiovascular disease or brain function. These were generally measured via supervised mobility tests (n = 11, e.g. Short Physical Performance Battery or Timed 10-Meter Walk Test), wearable devices (n = 5, e.g. pedometer or smart watch), and weight scales (n = 4), with other tools including spectroscopy, magnetic resonance imaging, dual-energy x-ray absorptiometry, bioelectrical impedance analysis, stadiometers, dynamometers, saliva swabs, ergometers, ultrasound, stress tests, cognitive tests, and skinfold thickness tests. All studies reported a positive impact of PA on health, except one which reported no effect of mixed PA on PTSD in refugees [ID14]. Increased PA led to weight loss, improved motor skills and gait speed, reduced anxiety and PTSD, and fewer fractures or hospital visits across remaining studies. Some of the greatest effect sizes in Cohen’s d (reported in n = 14) were seen using aerobics for autistic children with anxiety (1.32 [ID7]) and resistance training for older adults with sarcopenia (2.45 [ID9]) (Table 1).
Populations at Risk of Health Inequity
All individuals participating in the included trials belonged to at least one population at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks, as this was required for eligibility. Six studies included two populations at risk of health inequity [ID9,10,14,16,17,19], mostly a demographic characteristic combined with a condition. Five studies performed subgroup analysis [ID2,3,6,9,16], whereby the sample is divided and compared, mostly between sex or age groups. Of these, two included both multiple at-risk populations and subgroup analysis [ID9,16], while the remainder included neither (n = 14). Age (not in [ID20]) and sex/gender (not in [ID12]) were recorded in the majority of articles. However, education, ethnicity, income, and employment of participants or their parents were inconsistently reported (Figure 2b). Co-production of interventions utilising PA to improve health outcomes with the populations they intended to serve was not mentioned in any study (Table 1).
The “Core 20%” (income deprived) was considered in three studies. Three of the five clinical priority areas were absent, COPD, maternity, and early cancer, while mental illness and hypertension were underrepresented. Rural populations were examined most, followed by refugees or migrants and individuals aged ≥65. The remainder focused on individuals with learning disabilities or neurodivergence, with one study exclusively including an ethnic minority (Korean-Chinese [ID10]). No studies addressed multiple LTCs, homelessness, travelling communities, LGBTQ+ populations, substance misuse, or people with experience of the justice system. Mention of religion or social capital was also absent in all included trials (Figure 2c, Table 1).

Table 1.
Study characteristics, populations, outcomes, findings, and limitations for articles with trial evidence of interventions of physical activity to improve health outcomes which include populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks.
Table 1.
Study characteristics, populations, outcomes, findings, and limitations for articles with trial evidence of interventions of physical activity to improve health outcomes which include populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks.
| Author, year [ID] | Population | Intervention design | Co-production with at risk population | Duration | Comparator |
|---|---|---|---|---|---|
| Cai et al., 2022 [1] | Rural 60+ year-olds in China (n = 72) | Group exercise classes and at home walking via app | No | 3 months | Intervention vs control |
| Chang et al., 2025 [2] | Rural 50+ year-olds in Taiwan (n = 528) | Stretching and resistance training, nutritional support | No | 12 months | Intervention vs osteoporosis care vs control |
| Deng et al., 2024 [3] | Rural 60+ year-olds in China (n = 508) | Tai Chi and stretching exercises, counselling | No | 26 months | Intervention vs control |
| Errisuriz et al., 2023 [4] | Low-income Latino 3-year-olds in the United States (n = 310) | Home-based recommendations for children and parents on PA and nutrition (HBI), centre-based structured outdoor play sessions and healthy meals (CBI) | No | 8 months | HBI and CBI or CBI vs control |
| Filippou et al., 2025 [5] | Forcibly displaced individuals from Asia and Africa at refugee camps in Greece (n = 98) | Football, volleyball, basketball, martial arts, fitness, aerobics, and dancing | No | 10 weeks | Intervention vs control |
| Fulkerson et al., 2022 [6] | Rural 7 to 10-year-olds with parent/guardian in the United States (n = 114) | Goal-setting calls on PA and nutrition, monthly sessions including family exercise | No | 7 months | Intervention vs control |
| Gehricke et al., 2022 [7] | Latino or rural 6 to 12-year-olds with ASD in the United States (n = 148) | Aerobic exercise and muscle strength activities | No | 16 weeks | Intervention vs sedentary gaming group |
| Ibrahim et al., 2023 [8] | Rural community-dwelling adults in Nigeria (n = 120) | Aerobic exercise, stretching, motor control exercise (MCE) or patient education (PE) | No | 20 weeks | MCE and PE vs MCE vs PE |
| Ji et al., 2025 [9] | Rural community-dwelling 65+ year-olds in South Korea (n = 41) | Nutritional support and group exercise with stretching, resistance, aerobic activity | No | 12 weeks | Intervention vs control |
| Kim et al., 2022 [10] | Female Korean-Chinese migrant workers with low PA in South Korea (n = 46) | Regular walking via app (ST), regular walking with self-efficacy and social support (ET) | No | 24 weeks | ET vs ST |
| Knappe et al., 2024 [11] | Forcibly displaced individuals from Southwest Asia and Sub-Saharan Africa at refugee camps in Greece (n = 142) | Fitness training, martial arts, ball sports, dance | No | 10 weeks | Intervention vs control |
| Kovačič et al., 2020 [12] | Inactive adults with Down syndrome, cerebral palsy, ASD, ADHD, Prader-Willi syndrome in Slovenia (n = 150) | Balance exercise, wellness, Special Olympics athletic training (SO) | No | 16 weeks | Balance and SO vs wellness and SO vs SO |
| MacMillan Uribe et al., 2023 [13] | Rural women in the United States (n = 87) | Group exercise, PA and nutrition education | No | 24 weeks | Intervention vs control |
| Nordbrandt et al., 2020 [14] | Refugees with PTSD in Denmark (n = 318) | Body awareness therapy or mixed physical activity with strength, endurance, balance, coordination exercise | No | 20 weeks | Awareness vs mixed vs control |
| Nqweniso et al., 2021 [15] | 8 to 11-year-olds from low socioeconomic groups in South Africa (n = 898) | Physical education, dance, play, health and hygiene education, nutritional support | No | 10 weeks | PA vs PA and education vs PA and education and nutrition vs education and nutrition |
| Peng et al., 2025 [16] | Urban and rural community-dwelling 65+ year-olds in Taiwan (n = 88) | Strength and balance exercise, nutritional support, cognitive training | No | 12 months | Intervention vs control |
| Perloff et al., 2021 [17] | Low-income 65+ year-olds in the United States (n = 142) | Group and video-directed at home Tai Chi exercise | No | 12 months | Intervention vs control |
| Prats-Arimon et al., 2024 [18] | Rural adults in Spain (n = 42) | Group exercise, personalised at home activity, nutritional support | No | 9 months | Intervention vs control |
| Rapp et al., 2022 [19] | Rural community-dwelling 70 to 85-year-olds in Germany (n = 36,726) | Group and at home mobility and fall prevention exercise classes | No | 12 months | Intervention vs control |
| Shariat et al., 2021 [20] | Stroke patients in Iran (n = 30) | Cycling, functional electrical stimulation | No | 8 weeks | Interval vs linear |
| Thein Tun et al., 2025 [21] | Children with Down syndrome in Myanmar (n = 30) | Exercise focused on stability, object control skills, and locomotor skills | No | 12 weeks | Intervention vs control |
| Tuan et al., 2024 [22] | Rural 60+ year-olds in Taiwan (n = 55) | Exergame-based functional movement and progressive resistance training | No | 12 weeks | Intervention vs control |
| Wolf et al., 2024 [23] | Patients with depression, insomnia, PTSD, panic disorder, agoraphobia in Germany (n = 400) | Supervised evidence-based outdoor exercise, behavioural techniques | No | 12 months | Intervention vs control |
Table 1.
(continued). Study characteristics, populations, outcomes, findings, and limitations for articles with trial evidence of interventions of physical activity to improve health outcomes which include populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks.
Table 1.
(continued). Study characteristics, populations, outcomes, findings, and limitations for articles with trial evidence of interventions of physical activity to improve health outcomes which include populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks.
| Author, year [ID] | PROGRESS-Plus/CORE20PLUS5 characteristics | Equity-relevant subgroup analysis | Intervention outcome measures | Key findings | Study limitations |
|---|---|---|---|---|---|
| Cai et al., 2022 [1] | Rural, predominantly 65+ years | No | Physical activity by pedometer, physical function by tests, body composition by spectroscopy, physical activity self-efficacy, quality of life by survey | PA interventions increased grip strength and gait speed | PA intensity not specified, challenges in adherence, changes in daily energy expenditure unknown, short duration, diet not recorded |
| Chang et al., 2025 [2] | Rural, predominantly 65+ years | Yes, by sex, age, education, income | Osteoporosis diagnosis, self-reported quality of life and depression, institutionalisation, intrinsic and cognitive capacity including locomotion and audiovisual characteristics | PA interventions resulted in better intrinsic capacity and a lower reduction in quality of life | Controls may experience integrated care, recall bias, no cost-effectiveness analysis |
| Deng et al., 2024 [3] | Rural, predominantly 65+ years | Yes, by sex, age, education, income | Weight, BMI, body fat, waist circumference, hip circumference, waist-to-hip ratio, waist-to-height ratio | PA interventions resulted in weight loss | Short duration, diet not recorded |
| Errisuriz et al., 2023 [4] | Low income, predominantly ethnic minority (87%) | No | General motor quotient, locomotive skills, ball skills | PA interventions increased children’s motor skills | Multiple components so unsure of cause, tests carried out by single observer, tests do not reflect natural play, quality of implementation not assessed |
| Filippou et al., 2025 [5] | Asylum seekers | No | PTSD, depression, anxiety, stress, well-being symptoms | PA interventions reduced PTSD if attended over twice a week | High attrition, poor literacy |
| Fulkerson et al., 2022 [6] | Rural | Yes, by sex | BMI, BMIz, body fat, fidelity | PA interventions reduced obesity in boys not girls | Selection bias, low contact hours |
| Gehricke et al., 2022 [7] | Intellectual disabilities and autism, predominantly rural or ethnic minority | No | Parent- and self-reported anxiety, sleep, physical activity, heart rate by smart watch, stress by salivary cortisol | PA interventions improved anxiety and sleep | No non-activity control, medication effect not considered |
| Ibrahim et al., 2023 [8] | Rural | No | Self-reported pain intensity, disability, quality of life, global perceived recovery, fear-avoidance beliefs, pain catastrophising, back pain consequences belief, pain medication use | PA interventions reduced back pain, especially with combined MCE and PE | High attrition, short duration, no non-activity control |
| Ji et al., 2025 [9] | Rural, 65+ years | Yes, by sex, age | Gait speed, physical performance, grip strength, muscle mass, fatigue, disability, frailty, mental illness, quality of life | PA interventions improved gait speed, physical performance, grip strength, disability, frailty, quality of life | Limited generalisability, short duration, small sample size |
| Kim et al., 2022 [10] | Ethnic minority, immigrant status | No | Step adherence by smart watch, risk of cardiovascular disease, lipid profiles, fasting blood sugar | PA interventions reduced risk of cardiovascular disease | Multiple components so unsure of cause, poor recruitment |
| Knappe et al., 2024 [11] | Asylum seekers | No | Cognitive function, cognitive reaction time, pain, cardiorespiratory fitness | PA interventions improved cognitive reaction and cardiorespiratory fitness | High attrition, variability in sports type and amount, short duration, effect of age and PTSD not considered |
| Kovačič et al., 2020 [12] | Intellectual disabilities and autism | No | Static balance, dynamic balance, fall frequency | PA interventions increased balance, especially in balance-specific exercise group | Diet not recorded, short duration, no cost-effectiveness analysis |
| MacMillan Uribe et al., 2023 [13] | Rural | No | Self-reported dietary intake, dietary behaviour, diet-related psychosocial measures | PA interventions improved dietary patterns and diet-related psychosocial wellbeing | Multiple components so unsure of cause, mostly white participants, high attrition |
| Nordbrandt et al., 2020 [14] | Refugees, mental illness, predominantly multimorbid and chronic | No | PTSD severity | PA interventions did not affect PTSD symptoms | Personalised low-intensity PA |
| Nqweniso et al., 2021 [15] | Low income | No | BMI, body fat | PA interventions mitigated weight gain | Short duration, cofounders |
| Peng et al., 2025 [16] | Urban/rural, 65+ years | Yes, by residence | Brain structure by MRI, handgrip strength, walking speed, chair rise, cognitive function, body composition | PA interventions improved brain matter volume reduction, chair rise, cognitive function, body composition | Limited comparability, low sample size, possible cognitive impairment |
| Perloff et al., 2021 [17] | 65+ years, low income, predominantly multimorbid and chronic | No | Acute care utilisation, adjusted estimated cost of utilisation | PA interventions reduced emergency department visits | Recall bias, underreporting in controls |
| Prats-Arimon et al., 2024 [18] | Rural | No | Physical activity by smart watch, metabolic and body composition, self-reported diet adherence | PA interventions reduced fat and cholesterol | No metabolic markers controls, short duration, low sample size |
| Rapp et al., 2022 [19] | 65+ years, rural | No | Fragility fracture incidence by DXA | PA interventions reduced risk of femoral fractures | Only fractures requiring hospitalisation captured |
| Shariat et al., 2021 [20] | Hypertension | No | Walk test, functional ambulation, spasticity, active range of motion, functional mobility, balance | PA interventions improved walking, functional ambulation, functional mobility, balance in both, spasticity in interval | Small sample size, short duration, no non-activity control |
| Thein Tun et al., 2025 [21] | Intellectual disability | No | Functional strength, static balance, motor skills | PA interventions improved functional strength, static balance, motor skills | Small sample size, short duration |
| Tuan et al., 2024 [22] | Rural, predominantly 65+ years | No | Frailty, sarcopenia, functional performance, muscle condition, daily living activities, health-related quality of life, cognitive function | PA interventions improved muscle function, brain function, living conditions | Small sample size, short duration, personalised PA |
| Wolf et al., 2024 [23] | Mental illness | No | Symptom severity | PA interventions reduced mental illness symptoms | Attrition bias, cofounders, ethnicity not recorded, no patient involvement |
Discussion
This scoping review examined trial evidence on physical activity interventions aimed at improving health outcomes in populations at risk of health inequity, as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks. Across 23 eligible full randomised controlled trials, PA interventions were generally associated with positive health outcomes, with reported improvements in physical and cognitive function, cardiovascular outcomes, weight, frailty, fractures, hospital utilisation, mental health, and quality of life, predominantly among older adults in rural settings. However, equity considerations were rarely integrated: only two studies included multiple at-risk populations and subgroup analysis, leaving intersectionality largely unexamined. Reporting of equity-relevant factors such as education, ethnicity, income, and employment was inconsistent, limiting cross-study comparability and generalisability. Consequently, several populations at risk of health inequity, particularly ethnic minority groups and individuals with multiple long-term conditions, were underrepresented in the evidence base.
Comparison to Existing Literature
The heterogeneity observed across trials in this review aligns with findings from other systematic reviews of interventions utilising PA to improve health outcomes, which consistently highlight variability in intervention design, duration, and outcomes (Mahon et al., 2025). These also confirm that only a small proportion of PA trials conducts subgroup analysis whereby populations are compared (Montoye et al., 2016). Similarly, while community-based interventions are found to increase PA overall, equity-specific effects are rarely examined and most trials are not designed to test differences between groups defined by socioeconomic status, sex/gender, ethnicity, or disability as observed here (Skender et al., 2016). Mental illness, for example, is disproportionately common among adolescents (Ruiz-Ranz and Asín-Izquierdo, 2025), yet this group was largely absent from the studies included in our review. Such omission reflects a wider tendency to exclude younger populations from equity-focused analyses, despite activity in early adolescence being an established predictor of activity in adulthood (Telama et al., 2005). Other reviews have also reported omission of literacy, sexual orientation, and immigration status as demographic details, as identified in this work too (Band et al., 2025; Welch et al., 202). Overrepresentation of older individuals may then be due to easier recruitment as a result of established community-based programmes and infrastructure, making trials relatively practical and cost-effective (Jackman, 2025). These gaps constrain understanding of who benefits from interventions and under what conditions, ultimately reducing the translational value of the evidence base.
Consistent with our findings, previous studies show that research on health inequity typically addresses a single dimension rather than examining multiple factors (Popay et al., 2023). These approaches are found to perpetuate a mismatch between research frameworks and lived experience, as individuals simultaneously embody intersecting identities (Holman and Walker, 2021). The narrow focus has important implications for PA research, as interventions may fail to capture complex contextual mechanisms shaping behaviour when intersectionality is overlooked. As a result, programmes that appear effective within controlled trial environments may have limited scalability in real-world settings (Holt et al., 2025). Addressing these structural and contextual determinants, for example through cultural adaptation within trials by tailoring to linguistic and religious practices (El Masri et al., 2020; Mendoza-Vasconez et al., 2016), is therefore critical in designing PA interventions that produce equitable and enduring health benefits.
Strengths and Limitations
To our knowledge, this is the first review utilising PROGRESS-Plus and CORE20PLUS5 frameworks to systematically capture representation of populations at risk of health inequity in PA trials. Strengths include the application of a predefined protocol with adherence to PRISMA-ScR and SWiM guidance, the use of independent reviewers, and the structured classification of equity integration, which supports reproducibility and comparability. However, limitations include possible selection or extraction bias from observers, as well as restriction to English and peer-reviewed publications which may exclude relevant evidence. By only focusing on full randomised controlled trials published in the last five years, observational or qualitative evidence providing contextual insights into barriers and facilitators of equitable interventions utilising PA to improve health outcomes could have been overlooked. Lastly, heterogeneity in intervention types and outcome measures limited opportunities for quantitative synthesis, and equity-relevant factors were inconsistently reported, which restricts cross-study analysis.
Implications for Practice and Policy
This scoping review shows that physical activity interventions are generally associated with positive health outcomes, however consideration of health equity was limited and inconsistently reported across the included trials. Most studies focused on a single at-risk population, most commonly rural or older adults, with few explicitly including or comparing multiple populations at risk of health inequity. Equity-relevant factors were infrequently reported and subgroup analyses were rare, resulting in limited examination of intersectionality and underrepresentation of several at-risk populations. Deliberate integration of equity frameworks and meaningful engagement with populations at risk of health inequity is recommended in the design and delivery of PA interventions to support inclusive and effective practice and policy, thereby mitigating exacerbation of health inequity.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Authors’ contributions
Conceptualisation: LVM, LS, JK, HDM; methodology: LVM, LS, HDM; data collection: LVM, LS; data analysis: LVM, LS; writing and review: LVM, LS, JK, HDM.
Funding
This work was supported by the National Institute for Health Research Artificial Intelligence for Multiple Long-Term Conditions (AIM) project, “The development and validation of population clusters for integrating health and social care: A mixed-methods study on Multiple Long-Term Conditions” (NIHR202637), and the National Institute for Health and Care Research Multiple Long-Term Conditions (MLTC) Cross NIHR Collaboration (CNC) (NIHR207000).
Ethics approval and consent
Not applicable.
Availability of data and materials
All articles utilised are publicly available.
Acknowledgments
Not applicable.
Competing interests
No competing interests declared by all authors.
Disclaimer
The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research, or the Department of Health and Social Care.
Appendix A
Appendix A1. PRISMA Checklist for the Presented Review of Trial Evidence on Interventions of Physical Activity to Improve Health Outcomes in Populations at Risk of Health Inequity as Defined by the PROGRESS-Plus and CORE20PLUS5 Frameworks
Appendix A2. Search Terms to Systematically Identify Trial Evidence on Interventions of Physical Activity to Improve Health Outcomes in Populations at Risk of Health Inequity as Defined by the PROGRESS-Plus and CORE20PLUS5 Frameworks Before Scope Refinement
| MeSH and Free Text Search Terms | Filters/Refined by | Databases |
| (“physical activity” OR “physical activities” OR “exercise” OR “exercising” OR “workout” OR “working out” OR “fitness” OR “sport” OR “walking” OR “cycling” OR “movement” OR “active travel”) AND (“intervention”) AND (“underserved” OR “under-served” OR “minoritised” OR “minoritized” OR “minority” OR “marginalised” OR “marginalized” OR “disadvantaged” OR “underprivileged” OR “under-privileged” OR “deprived” OR “underrepresented” OR “under-represented” OR “neglected” OR “poverty” OR “impoverished” O”underresourced” OR “under-resourced” OR “low-income” OR “lower-income” OR “migrant” OR “immigrant” OR “migrants” OR “immigrants” OR “refugee” OR “refugees” OR “asylum seeking” OR “asylum seekers” OR “disabled” OR “queer” OR “LGBTQI+” OR “LGBT” OR “homeless” OR “homelessness” OR “non-White” OR “non-white” OR “rural”) AND (“randomised controlled trial” OR “randomized controlled trial” OR “clinical trial” OR “pragmatic trial” OR “adaptive trial” OR “cluster trial” OR “evaluation study” OR “quasi-experimental study” OR “experimental study”) |
Restricted to the English language, randomised controlled trials using PA as intervention with results, populations at risk of health inequity only | PubMed (n = 674 before screening) |
| Web of Science (n = 845 before screening) | ||
| Scopus (n = 750 before screening) |
References
- Arksey; O’Malley. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Avraham; et al. Determinants of physical activity habit formation: a theory-based qualitative study among young adults. Int J Qual Stud Health Well-being 2024, 19, 2341984. [Google Scholar] [CrossRef] [PubMed]
- Band; et al. Social network intervention for loneliness and social isolation in a community setting: The PALS cluster-RCT. Public Health Research 2025, 13, 1–86. [Google Scholar] [CrossRef]
- Bantham; et al. Overcoming barriers to physical activity in underserved populations. Progress in Cardiovascular Diseases 2021, 64, 64–71. [Google Scholar] [CrossRef]
- Cai; et al. Effects of peer support and mobile application-based walking programme on physical activity and physical function in rural older adults: a cluster randomized controlled trial. Eur Geriatr Med 2022, 13, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Campbell; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [PubMed]
- Celis-Morales; et al. Objective vs self-reported physical activity and sedentary time: effects of measurement method on relationships with health outcomes. Int J Epidemiol 2012, 41, 1328–1339. [Google Scholar]
- Chang; et al. Effects of osteoporosis treatment and multicomponent integrated care on intrinsic capacity and happiness among rural community-dwelling older adults: the Healthy Longevity and Ageing in Place (HOPE) randomised controlled trial. Age and Ageing 2025, 54, afaf017. [Google Scholar] [CrossRef]
- Deng; et al. Effect of physical activity intervention on weight change in rural older Chinese: a cluster randomized controlled trial. Int J Obes 2024, 48, 1758–1766. [Google Scholar] [CrossRef]
- El Masri; et al. Physical activity interventions among culturally and linguistically diverse populations: a systematic review. Ethnicity & Health 2022, 27, 40–60. [Google Scholar]
- Errisuriz; et al. ¡Miranos! An 8-Month Comprehensive Preschool Obesity Prevention Program in Low-Income Latino Children: Effects on Children’s Gross Motor Development. Int J Environ Res Public Health 2023, 20, 6974. [Google Scholar] [CrossRef] [PubMed]
- Filippou; et al. Effects of an exercise and sport intervention on symptoms of post-traumatic stress disorder and other mental health indices among asylum seekers in a camp: A pragmatic randomized controlled trial. Mental Health and Physical Activity 2025, 28, 100676. [Google Scholar] [CrossRef]
- Fukushima; et al. Dose-Response Relationship of Physical Activity with All-Cause Mortality among Older Adults: An Umbrella Review. JAMDA 2024, 25, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Fulkerson; et al. Weight outcomes of NU-HOME: a randomized controlled trial to prevent obesity among rural children. Int J Behav Nutr Phys Act 2022, 19, 29. [Google Scholar] [CrossRef]
- Gehricke; et al. The effects of a physical exercise program, LEGOR and Minecraft activities on anxiety in underserved children with autism spectrum disorder. Research in Autism Spectrum Disorders 2022, 97, 102005. [Google Scholar] [CrossRef]
- Government UK, 2023. Physical activity: applying All Our Health (online).
- Guthold; et al. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys. Lancet Glob Health 2016, 6, e1077–86. [Google Scholar]
- Holman; Walker. Understanding unequal ageing: towards a synthesis of intersectionality and life course analyses. Eur J Ageing 2021, 18, 239–255. [Google Scholar] [CrossRef]
- Holt; et al. The person-based approach to intervention development: A scoping review of methods and applications. Digit Health 2025, 11, 20552076241305934. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim; et al. Effectiveness of patient education plus motor control exercise versus patient education alone versus motor control exercise alone for rural community-dwelling adults with chronic low back pain: a randomised clinical trial. BMC Musculoskelet Disord 2023, 24, 142. [Google Scholar] [CrossRef]
- Jackman; et al. Physical activity in age-friendly cities and communities: a scoping review with recommendations to support policy and practice. BMC Public Health 2025, 25, 4107. [Google Scholar] [CrossRef]
- Ji; et al. Effect of Exercise and Nutrition Intervention for Older Adults with Impaired Physical Function with Preserved Muscle Mass (Functional Sarcopenia): A Randomized Controlled Trial. Clin Interv Aging 2025, 20, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Kim; et al. Living labs for a mobile app-based health program: effectiveness of a 24-week walking intervention for cardiovascular disease risk reduction among female Korean-Chinese migrant workers: a randomized controlled trial. Arch Public Health 2022, 80, 181. [Google Scholar] [CrossRef] [PubMed]
- Knappe; et al. The impact of an exercise and sport intervention on cognitive function and pain among forcibly displaced individuals at risk for PTSD: a secondary analysis of the SALEEM randomized controlled trial. BMC Medicine 2024, 22, 387. [Google Scholar] [CrossRef] [PubMed]
- Kohl; et al. The pandemic of physical inactivity: global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef]
- Kovačič; et al. The impact of multicomponent programmes on balance and fall reduction in adults with intellectual disabilities: a randomised trial. J Intellect Disabil Res 2020, 64, 381–394. [Google Scholar] [CrossRef]
- Lee; et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Lee; et al. Long-term leisure-time physical activity intensity and all-cause and cause-specific mortality: a prospective cohort of US adults. Circulation 2022, 146, 523–534. [Google Scholar] [CrossRef]
- Levac; et al. Scoping studies: advancing the methodology. Implementation Science 2010, 5, 69. [Google Scholar] [CrossRef]
- Lorenc; et al. What types of interventions generate inequalities? Evidence from systematic reviews. J Epidemiol Community Health 2013, 67, 190–193. [Google Scholar] [CrossRef]
- Lopez; et al. Associations of vigorous physical activity with all-cause, cardiovascular and cancer mortality among 64 913 adults. BMJ Open Sport Exerc Med 2019, 5, e000596. [Google Scholar] [CrossRef]
- Uribe, MacMillan; et al. Improvements in dietary intake, behaviors, and psychosocial measures in a community-randomized cardiovascular disease risk reduction intervention: Strong Hearts, Healthy Communities 2.0. Am J Clin Nutr 2023, 118, 1055–1066. [Google Scholar] [CrossRef] [PubMed]
- Mahindru; et al. Role of Physical Activity on Mental Health and Well-Being: A Review. Cureus 2023, 15, e33475. [Google Scholar] [CrossRef] [PubMed]
- Mahon; et al. A scoping review of physical activity interventions to support the mental health of students aged 16 to 25. Discov Public Health 2025, 22, 538. [Google Scholar] [CrossRef]
- Mendoza-Vasconez; et al. Promoting Physical Activity among Underserved Populations. Translational Journal of the ACSM 2016, 1, 125–132. [Google Scholar] [CrossRef]
- Montoye; et al. Reporting accelerometer methods in physical activity intervention studies: a systematic review and recommendations. Prev Med 2016, 94, 50–57. [Google Scholar] [CrossRef]
- NHS England, 2021. Core20PLUS5 (adults): an approach to reducing healthcare inequalities.
- Nordbrandt; et al. Trauma-affected refugees treated with basic body awareness therapy or mixed physical activity as augmentation to treatment as usual-A pragmatic randomised controlled trial. PLoS One 2020, 15, e0230300. [Google Scholar] [CrossRef]
- Nqweniso; et al. Effect of school-based interventions on body composition of grade-4 children from lower socioeconomic communities in Gqeberha, South Africa. S Afr J Child Health 2021, 15, 89–98. [Google Scholar] [CrossRef]
- Oliver; et al. 2008. Health promotion, inequalities and young people’s health. A systematic review of research. EPPI-Centre Report 1611. 2008.
- Pearce; et al. Association between physical activity and risk of depression: A systematic review and meta-analysis. JAMA Psychiatry 2022, 79(6), 550–559. [Google Scholar] [CrossRef]
- Peng; et al. Enhancing Neurocognitive Health via Activity, Nutrition and Cognitive Exercise (ENHANCE): A Randomized Controlled Trial. J Cachexia Sarcopenia Muscle 2025, 16, e13830. [Google Scholar] [CrossRef]
- Perloff; et al. The Impact of Tai Chi Exercise on Health Care Utilization and Imputed Cost in Residents of Low-Income Senior Housing. Glob Adv Health Med 2021, 22, 164956120985479. [Google Scholar] [CrossRef]
- Piercy; et al. The physical activity guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- Popay; et al. Strengthening the equity focus of applied public health research: introducing the FOR EQUITY platform. Public Health 2023, 215, 12–16. [Google Scholar] [CrossRef]
- Prats-Arimon; et al. An Interdisciplinary Intervention Based on Prescription of Physical Activity, Diet, and Positive Mental Health to Promote Healthy Lifestyle in Patients with Obesity: A Randomized Control Trial. Nutrients 2024, 16, 2776. [Google Scholar] [CrossRef] [PubMed]
- Rapp; et al. Effect of an osteoporotic fracture prevention program on fracture incidence in routine care: a cluster-randomized trial. BMC Medicine 2022, 20, 49. [Google Scholar] [CrossRef]
- Ruiz-Ranz; Asín-Izquierdo. Physical activity, exercise, and mental health of healthy adolescents: A review of the last 5 years. Sports Medicine and Health Science 2025, 7, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Shariat; et al. Effect of cycling and functional electrical stimulation with linear and interval patterns of timing on gait parameters in patients after stroke: a randomized clinical trial. Disabil Rehabil 2021, 43, 1890–1896. [Google Scholar] [CrossRef] [PubMed]
- Skender; et al. Accelerometry and physical activity questionnaires: a systematic review. BMC Public Health 2016, 16, 515. [Google Scholar] [CrossRef]
- Telama; et al. Physical activity from childhood to adulthood. American Journal of Preventive Medicine 2005, 28, 267–273. [Google Scholar] [CrossRef]
- Thein Tun; et al. Effect of structured exercise program on fundamental motor skills in children with Down syndrome: A randomized controlled trial. Journal of Associated Medical Sciences 2025, 58, 48–57. [Google Scholar] [CrossRef]
- Tricco; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Annals of Internal Medicine 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Tuan; et al. Assessing the Clinical Effectiveness of an Exergame-Based Exercise Training Program Using Ring Fit Adventure to Prevent and Postpone Frailty and Sarcopenia Among Older Adults in Rural Long-Term Care Facilities: Randomized Controlled Trial. J Med Internet Res 2024, 26, e59468. [Google Scholar] [CrossRef]
- Wahid; et al. Quantifying the association between physical activity and cardiovascular disease and diabetes: a systematic review and meta-analysis. J Am Heart Assoc 2016, 5, e002495. [Google Scholar] [CrossRef]
- Welch; et al. How effects on health equity are assessed in systematic reviews of interventions. Cochrane Database of Systematic Reviews 2022, 1, MR000028. [Google Scholar] [CrossRef]
- Wolf; et al. A transdiagnostic group exercise intervention for mental health outpatients in Germany (ImPuls): results of a pragmatic, multisite, block-randomised, phase 3 controlled trial. The Lancet Psychiatry 2024, 11, 417–430. [Google Scholar] [CrossRef]
- World Health Organisation, 2024. Physical activity (online).
- Yang; et al. The Physical Activity and Cancer Control (PACC) framework: update on the evidence, guidelines, and future research priorities. British Journal of Cancer 2024, 131, 957–969. [Google Scholar] [CrossRef]
- Yu; et al. Physical activity trajectories and accumulation over adulthood and their associations with all-cause and cause-specific mortality: a systematic review and meta-analysis. British Journal of Sports Medicine 2025, 59, 1228–1241. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flow diagram with number of records identified, screened, excluded, and included for articles with trial evidence on interventions of physical activity to improve health outcomes in populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks.
Figure 1.
PRISMA flow diagram with number of records identified, screened, excluded, and included for articles with trial evidence on interventions of physical activity to improve health outcomes in populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks.
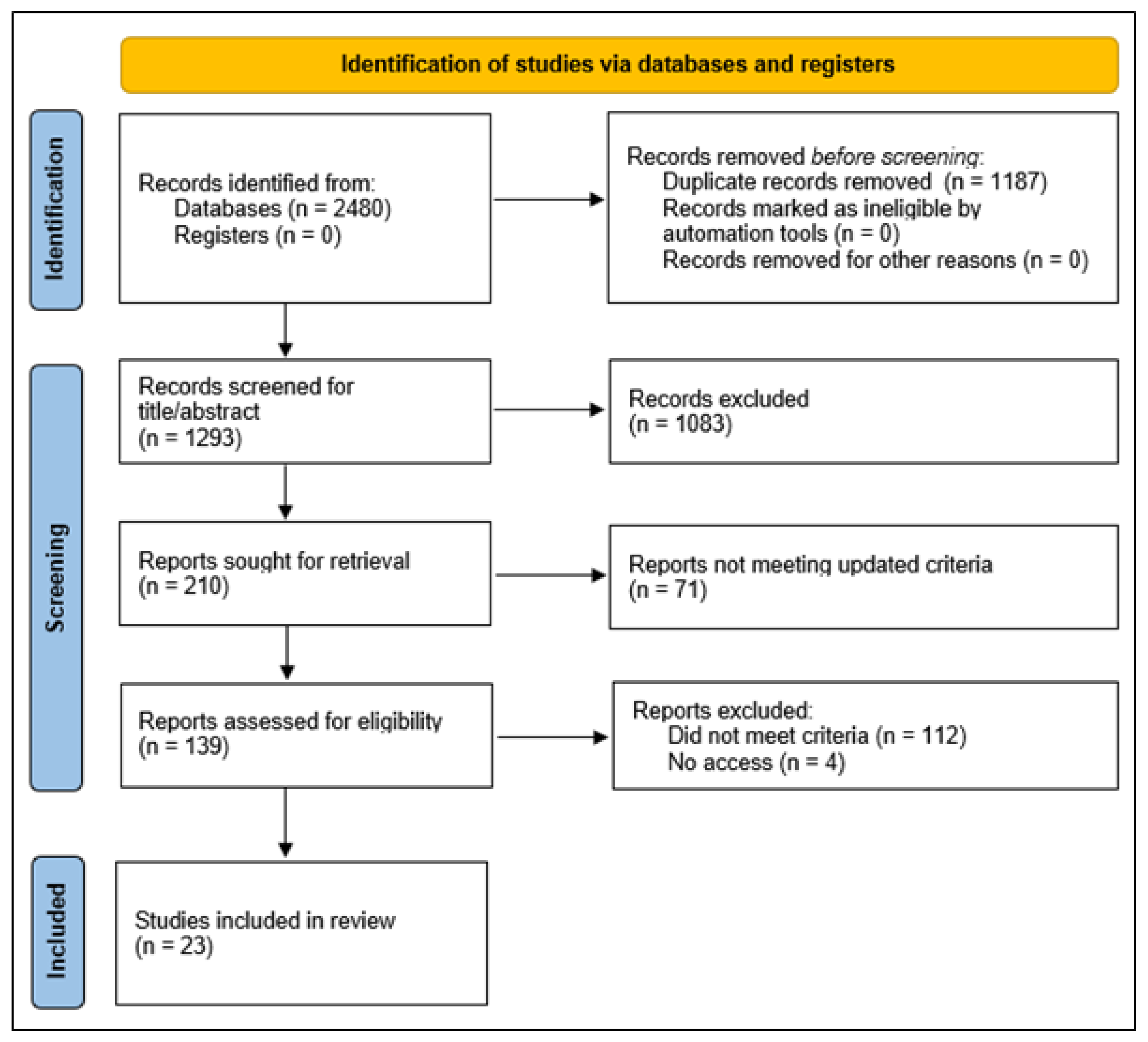
Figure 2.
Physical activity interventions assessed (a), equity-relevant factors reported (b), and populations at risk of health inequity studied (c) across articles with trial evidence on interventions of physical activity to improve health outcomes in populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks.
Figure 2.
Physical activity interventions assessed (a), equity-relevant factors reported (b), and populations at risk of health inequity studied (c) across articles with trial evidence on interventions of physical activity to improve health outcomes in populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



