
Submitted:
06 January 2026
Posted:
07 January 2026
You are already at the latest version
Abstract
Background: Cryptococcal meningitis (CM) remains a leading cause of mortality among people with advanced HIV disease (AHD) in sub-Saharan Africa. Current guidelines recommend induction therapy with amphotericin B and flucytosine, typically administered in an inpatient setting due to concerns over severe clinical presentation and drug-related toxicities. This requirement poses a significant burden on resource-limited health systems. We evaluated the real-world outcomes of a fully outpatient model for CM therapy in Maputo, Mozambique. Methods: A longitudinal retrospective cohort study was conducted at the Centro de Referência de Alto-Maé (CRAM), a specialized AHD outpatient clinic. We included 83 PLWH with laboratory-confirmed CM treated between October 2020 and December 2024. The primary outcome was hospitalization-free survival (HFS) within the first 10 weeks of treatment. Secondary outcomes included the frequency and severity of adverse drug reactions (ADRs), analysed by tracking haemoglobin (Hgb), potassium (K+), and creatinine (Creat) levels on days 1, 3, and 7 of induction therapy, and retention in care (RIC) at 6, 12, and 24 months. Statistical analyses included Kaplan-Meier survival estimates and paired t-tests. Results: The median age was 37 years (IQR: 27-42), 63.9% were male, and the median CD4 count was 62 cells/µL (IQR: 27-105). Most patients (95.2%) were symptomatic at presentation, and 56.6% had concurrent tuberculosis. For the 52 patients who completed the full induction protocol at CRAM, the HFS rate at 10 weeks was 84.6% (44/52), with an overall survival of 90.4% (47/52). ADR analysis (n=52) showed a predictable pattern of mild, manageable toxicity: a significant decline in Hgb (11.2 ± 1.8 to 10.6 ± 2.0 g/dL, p<0.001) and K+ (4.27 ± 0.66 to 3.86 ± 0.78 mmol/L, p=0.008), and a transient increase in Creat (0.83 ± 0.42 to 1.13 ± 0.64 mg/dL, p=0.001) from day 1 to day 3, with stabilization or trend toward recovery by day 7. No significant differences in ADRs were found between single-dose (47%) and multiple-dose (53%) L-AmB regimens. RIC for the entire cohort (n=83) was high, at 81.9% at 6 months, declining to 74.0% at 12 months and 70.4% at 24 months. Conclusion: An ambulatory model for CM therapy is feasible and effective in a resource-limited setting, demonstrating high hospitalization-free survival, manageable and reversible adverse drug reactions, and excellent medium-term retention in care. These findings provide compelling evidence to reconsider the standard of inpatient care and support the integration of outpatient CM management into AHD care packages to alleviate health system burdens and improve patient outcomesAn integrated care approach is essential to improving survival in resource-limited settings.
Keywords:
cryptococcal meningitis
; advanced HIV disease
; hospitalization-free survival
; ambulatory therapy model
; Mozambique
1. Introduction
Cryptococcal Meningitis (CM) is a major concern and leading cause of meningitis in adults in Sub-Saharan Africa (SSA) and other regions with high prevalence of the Human Immunodeficiency Virus (HIV) infection, accounting for more than 100,000 incident cases of meningitis per year in the region. Globally, about 15% of HIV-related deaths are attributable to CM and 75% of these occur in SSA [1,2,3]
To date, studies on the management of CM advocate the administration of liposomal amphotericin B (L-AmB) during the induction phase which can be done in multiple doses or in a higher single dose, associated with oral Flucitosine [4,5]. The induction phase has always been carried out in-hospital. This is due to the perception that CM involves patients in a serious clinical situation, as well as to ensure better management of medical complications and adverse reactions to medications [4].
Outpatient management of CM has not been recommended in existing national or international guidelines. However, noteworthy experience have been described by Medical Action Myanmar (MAM), a medical aid organization in Myanmar [6]. These instances demonstrated the potential to address limitations encountered in providing CM care in resource-limited settings. A retrospective cohort from Myanmar, including 66 patients, reported that using intravenous amphotericin B-deoxycholate (0.7–1.0 mg/kg) and oral fluconazole (800 mg orally/day) on an outpatient basis during the induction phase, saved 1,029 days of hospital beds and had better survival outcomes [6]. In this context, additional evidence is required to show feasibility of a differentiated model of care that simplifies provision of CM care.
Until now, there has been a paucity of data describing the results of a completely ambulatory model of CM treatment. This analysis aimed to evaluate the results of an ambulatory model of CM management in the first 10 weeks of treatment at CRAM, Mozambique, between 2020–2024. It also describes the occurrence of adverse drugs reactions (ADR) to CM treatment in the sub-cohort of patients that received complete CM treatment at CRAM. Finaly, it presents cohort retention data at 6 months.
2. Materials and Methods
2.1. Setting
The prevalence of HIV in Maputo City stands at 16.2% among individuals aged 15 and older [7], and a cumulative total of 170,161 people living with HIV (PLWH) who were receiving antiretroviral therapy (ART) by mid-2024 [8].
Since 2013 MSF and I-TECH, have managed the Centro de Referência do Alto-Maé (CRAM) in partnership with the Ministry of Health (MoH) as an outpatient clinic to offer ART treatment for HIV patients in Mozambique [7]. CRAM provides a range of outpatient services, with special focus on rapid and comprehensive screening and management of AHD [9]. As of the end of 2024, its cumulative registry included approximately 25,600 HIV-positive individuals, of whom 1,700 remained actively engaged in care [10].
2.2. Study Design
This evaluation employed a longitudinal retrospective design to assess real-world implementation of CM management, with the aim of informing future program enhancements. The program implemented a longitudinal tracking system to evaluate patient outcomes by comparing initial baseline measurements with follow-up data. The included data were retrospectively collected as part of screening and management of AHD program from CRAM between October 2020 and December 2024.
2.2.1. Eligible Participants
The eligibility criteria consisted of PLWH of all ages who had AHD and a CM diagnosis, followed up at CRAM between October 2020 and Dezember 2024
2.2.2. Sampling and Sample Size
The sample encompassed the entire population of PLWH who had AHD and tested positive for cryptococcal antigen in their cerebrospinal fluid (CSF), as recorded in AHD registration book at CRAM, in accordance with the specified eligibility criteria.
Among the 83 CM patients, 38 (45.8%) received their first CM treatment at CRAM, and the remaining 45 patients (54.2%) had received at least one antifungal drug before CRAM admission.
Of those 45 patients previously treated, 14 (31.1%) were reinitiated on antifungal therapy, due to inconsistent/incomplete previous treatment (generally without amphotericin B and/or flucytosine). The remaining 31 patients were considered correctly treated prior to arrival at CRAM and follow up continued without the need of induction therapy. The full cohort (n = 83) was included in the retention analyses, while the subcohort of patients who completed treatment for CM (n = 52) was used in the analyses of hospitalization-free survival and treatment-related adverse events (see Figure 1).
2.2.3. Program Data Collection
The study team extracted routine clinical data from paper-based patient files, during the period under analysis, between 2020 and 2024. Exposure variables were categorized into five fields: (1) demographic profile: gender and age; (2) Immunological and nutritional assessments: T-CD4 Cell count (Cell/μL), body mass index (BMI); (3) Treatment specifics: site of initial antifungal therapy for CM (CRAM or other HF), dose of L-AmB (Single or Multiple), ART status on admission (pre-ART, on ART, ART Interruption); (4) CM Symptoms: headache, vomiting, and meningeal signs [neck stiffness, Kernig’s sign, Brudzinski’s sign], decreased visual acuity or blindness, diplopia, agitation or unusual behaviour, photophobia, hypoacusis, seizures, reduced level of consciousness(5) Concurrent opportunistic infections (OIs): tuberculosis (TB), oral candidiasis, wasting syndrome, chronic diarrhoea and Kaposi sarcoma (Table 1).
Data collected from eligible PLWH were anonymized to remove identifying details: each patient was given an alphanumeric code, and the anonymized data were included in the data sheet. Spreadsheet data were exported to SPSS for further data analysis.
2.3. Outcome Data and Statistical Analysis of Data
Statistical analysis was performed using the statistical software IBM® Statistical Package for the Social Sciences (SPSS) version 25 (International Business Machines Corporation, IBM Corp, Release 2017, https://www.ibm.com/legal/copytrade, USA).
2.3.1. Primary Outcome
The primary outcome was hospitalization-free survival (HFS) within the first 10 weeks of treatment/follow-up, among participants with CM.
First, we characterized the study population by calculating frequencies and proportions with 95% confidence intervals (CI) for categorical variables, and medians with interquartile ranges (IQR) for continuous data. We then employed Kaplan-Meier analysis to estimate HFS within the 10 weeks of treatment/follow-up.
Conceptual definitions
- Hospitalization referrals were guided by two main criteria: First, the presence of clinical danger signs, including an altered level of consciousness (observed or reported), seizures, or other critical symptoms such as respiratory distress. Second, anticipated logistical barriers that would prevent regular clinic attendance, for instance, living a significant distance from the health facility without access to reliable transportation.
- HFS was defined as the proportion of patients who survived for at least 10 weeks following cryptococcal meningitis diagnosis without requiring inpatient admission at any point during this follow-up period.
2.3.2. Secondary Outcomes
Trends in haemoglobin (Hgb [g/dL), potassium (K+ [mmol/L]), and creatinine (creat [mg/dL]) levels on the first, third, and seventh day of CM treatment were assessed to identify related ADR.
We first assessed normality using the Shapiro-Wilk test, with results presented as mean ± standard deviation (SD). The dependent variables analysed were Hgb, K⁺, and creat. A paired t-test was used to compare values between the first, third, and seventh days of CM treatment, with a p-value <0.05 considered statistically significant.
An additional secondary outcome, retention in care at 6, 12, and 24 months, was evaluated using Kaplan-Meier analysis to determine its probability over time.
3. Results
3.1. Baseline Clinical and Demographic Characteristics of Patients with CM Followed Up at CRAM
Between October 2020 and Dezember 2024, 83 individuals with CM were enrolled at CRAM.
Median age at admission was 37 years (interquartile range [IQR]: 27–42), with 36 (43.4%) falling within the 35–44 age range. Furthermore, 53 (63.9%) of the participants were male (Table 1).
Among the 83 patients with CM, the median CD4 cell count was 61 cells/µL (IQR: 27–105). Notably, 34 (41.0%) had a CD4 cell count below 50 cells/µL, while 39 (50.0%) had a body mass index (BMI) under 18.5 kg/m², indicating malnutrition (Table 1).
We defined as ART experienced those patients’ receiving ART for at least 30 days before the event of CM. 44 patients (53.0%) were ART experienced according to our definition and 39 (47.0%) were considered naïve to ART.
79 patients (95.2%) were symptomatic. The most common signs and symptoms included headache (78, 94%), vomiting (27, 32.5%), and meningeal signs (26, 31.3%). Other reported symptoms were decreased visual acuity (19, 22.9%), agitation or unusual behaviour (16, 19.3%), photophobia (16, 19.3%), hypoacusis (8, 9.6%), diplopia (8, 9.6%), seizures (6, 7.2%), and coma (1, 1.2%) (Table 1).
Of 79 patients, 34 (43.0%) had one lumbar puncture (LP), 45 (57.0%) had multiple—38 (48.1%) with 2–5 and 7 (8.9%) with ≥6. In four cases (5.1%) LP was not successful. Opening cerebrospinal fluid pressure (OP CSF) was recorded in 70 cases: 9 (12.9%) were normal (≤20 cmH₂O), 29 (41.4%) moderately elevated (21–40 cmH₂O), and 32 (45.7%) severely elevated (≥41 cmH₂O).
Concurrent OIs were also common, 47 patients (56.6%) had a concomitant TB diagnosis, 18 (21.7%) presented with oral candidiasis, and 15 (18.1%) exhibited wasting syndrome. Other conditions included chronic diarrhoea (6, 7.2%) and Kaposi sarcoma (5, 6%) (Table 1).
3.2. HFS Within the First 10 Weeks of Treatment Among Patients with CM
Regarding HFS analysis, we included 52 patients who completed the full CM treatment protocol at CRAM. The remaining 31 patients were excluded from the analysis, as they were presumed to have been appropriately induced on CM treatment prior to their arrival at CRAM, in a hospital setting under inpatient care. Among those 52 patients, 6 (11.5%) required hospitalization during the first 10 weeks of treatment. Mortality among these patients requiring hospitalization was 50% (3 out of 6 died). Two patients died at home, 2 and 23 days after initiation of treatment. HFS reached 84.6% by week 10 of treatment. Overall survival was 90.4%. (see Figure 2).
Kaplan–Meier analysis indicates a high probability of HFS within the first 10 weeks of treatment follow-up, with an estimated incidence of 84.6% at week 10 (Figure 3).
When analysing overall mortality in the cohort of patients who completed treatment for CM at CRAM, we observed 5 deaths during the first 10 weeks of follow-up. The overall survival rate of the cohort was 90.4% (47/52).
3.3. ADR of Treatment (Frequency and Severity) Among Patients with CM
Regarding analysis of ADR of CM treatment, we considered the sub-cohort of patients that received complete CM treatment at CRAM (n = 52). The remaining 31 patients were excluded, as they did not receive L-AmB at CRAM and no accurate laboratory data was available.
The analysis of laboratory parameters revealed a clear pattern of initial minimum toxicity followed by stabilization, in patients receiving L-AmB and flucitosine induction therapy. Of the 52 patients who completed treatment for CM at CRAM, 27 (52%) received the 7-day protocol with intravenous liposomal L-AmB. The following 25 patients (48%) received the single-dose L-AmB protocol, introduced at CRAM in September 2022. No differences were observed in the occurrence of adverse effects between the two protocols; therefore, toxicity data are presented jointly.
Haemoglobin (Hgb) levels showed a mild decline of 0.6 g/dL, from a baseline mean (plus ± SD) of 11.2 ± 1.8 g/dL on Day 1 to 10.6 ± 2.0 g/dL by Day 3 (p < 0.001), suggesting the early onset of drug-induced anemia. No significant recovery was observed, with levels remaining at 10.6 ± 1.8 g/dL through Day 7 (p = 0.738) (Table 2).
Potassium (K⁺) levels, which were within the normal range at 4.27 ± 0.66 mmol/L on Day 1, showed a mild decline of 0.26 mmol/L to a below-normal nadir of 3.86 ± 0.78 mmol/L by Day 3 (p = 0.008), confirming hypokalaemia. By Day 7, a trend toward recovery was observed, with levels rising to 3.97 ± 0.61 mmol/L (p = 0.175) (Table 2).
Creatinine (Creat), showed a mild increase of 0.39 mg/dL, rising from a normal baseline of 0.83 ± 0.42 mg/dL on Day 1 to 1.13 ± 0.64 mg/dL on Day 3 (p = 0.001), indicating mild nephrotoxicity. Encouragingly, by Day 7, the mean decreased to 0.99 ± 0.43 mg/dL (p = 0.370), suggesting a trend toward recovery (Table 2).
3.4. Retention in Care (RIC) Among Patients with CM (at 6, 12, and 24 Months)
At the time of analysis, 83 patients with CM had completed 6 months of follow-up, 73 had completed 12 months, and 54 had reached 24 months of clinical follow-up.
As expected, the analysis revealed a decline in patients RIC over time, dropping from 81.9% at 6 months to 70.4% at 24 months (p < 0.001) (see Figure 4).
Death was the leading cause of loss to follow-up, accounting for 60% of losses at 6 months, 52% at 12 months, and 43% at 24 months of follow-up. The remaining losses to follow-up were evenly distributed between cases of discontinuation and patient-requested transfers to other healthcare facilities (see Table 3).
4. Discussion
This analysis presents the outcomes of treating cryptococcal meningitis (CM), a severe opportunistic infection, in a resource-limited setting. Mozambique faces a generalized HIV epidemic, with recent estimates placing adult HIV prevalence at 12.5%, corresponding to over 2 million PLWH. Consistent with regional trends, CM is considered one of the most prevalent and deadly opportunistic infections.
A study conducted by Médecins Sans Frontières (MSF) at a general hospital in Maputo city between 2018 and 2019 reported a 7.5% prevalence of cryptococcal antigenemia among patients with CD4 cell counts below 200 cells/mm³. In the overall screened cohort (n = 1,795), CM prevalence was 5.4%. Among the 87 CM cases with available treatment outcome data, the cumulative 12-week mortality rate was 37.9% (33 patients), including 24 deaths during hospitalization and 9 post-discharges. Loss to follow-up by week 12 occurred in 25.3% of cases (16 patients), and 38 patients (43.6%) remained in care 12 weeks after diagnosis [11].
These short-term unfavourable outcomes, consistent with findings from other cohorts of hospitalized CM patients in Southern Africa, combined with low medium-term retention in care, prompted the adoption of an innovative outpatient treatment model offering liposomal amphotericin B, and the only one with access to flucytosine. This therapeutic regimen, now more widely available nationally, is considered the optimal treatment for CM. When paired with on-demand therapeutic lumbar punctures, it has yielded promising results in terms of both survival and medium-term retention in care.
4.1. High HFS and Overall Survival
Our findings demonstrate favourable clinical outcomes, with high rates of hospitalization-free survival and overall survival among patients who received ambulatory treatment for CM. Specifically, 84.6% (44/52) remained alive without requiring hospitalization during the critical first 10 weeks of therapy, while overall survival was 90.4% (47/52), including those referred for inpatient care post-diagnosis who ultimately survived.
When compared to previous data from the region, these results suggest a substantial improvement in prognosis. A study conducted in Maputo and published in 2024 reported a 12-week mortality rate of 37.9% [11], whereas our cohort achieved an overall survival of 90.4% during the first 10 weeks of treatment. This contrast underscores significant advances in CM management, reflecting an approximate fourfold reduction in early mortality.
Additional multicentre data reinforce the relevance of these findings. A prospective cohort study conducted in sub-Saharan Africa (SSA) which aimed to describe short-term mortality outcomes of HIV-associated CM, found that 10-week all-cause mortality was similar between antiretroviral therapy (ART)-experienced and ART-naive patients—38% versus 36%, respectively (p = 0.64; hazard ratio [HR], 1.03; 95% CI: 0.80–1.32; p = 0.82) [12].
10-week survival rate observed in the CRAM cohort also exceeded that of other studies conducted in Southern Africa. For instance, compared to the Ambition study cohort, which reported a 10-week survival of 75.2% in the L-AmB group, CRAM achieved a rate 15 percentage points higher over the same period among patients who received ambulatory treatment for CM [13].
Similarly, a prospective cohort study conducted in Uganda between 2022 and 2023, where adult CM patients were treated with the single-dose L-AmB regimen. Among 179 participants, the 10-week survival probability—estimated via the Kaplan-Meier method—was 68.6% (95% CI: 61.6%–76.3%). Although this represents one of the strongest outcomes reported outside a controlled research setting, mortality remains substantial [14].
Taken together, these comparisons highlight the relative success of the CRAM model. We believe a key factor contributing to the improved survival is the delivery of treatment at a primary-level health facility, within a setting where systematic screening for cryptococcal antigenemia is being more comprehensively implemented, which enables earlier diagnosis and intervention. This approach, combined with same-day clinical response, likely facilitated timely initiation of therapy and led to better outcomes.
Our study confirms that outpatient CM induction therapy is feasible and highly effective in resource-limited settings. The 84.6% HFS rate over the initial 10 weeks provides compelling real-world evidence that challenges the traditional reliance on prolonged inpatient care. These findings align with and reinforce limited existing literature on ambulatory CM management [6].
4.2. Manageable and Reversible ADRs
Initial safety concerns regarding outpatient CM management were rapidly mitigated, given the excellent safety outcomes and minimal serious adverse drug reactions (ADRs). Declines in haemoglobin and serum potassium were limited, and no hospitalizations occurred due to laboratory changes. Serum creatinine increased mildly but returned to baseline within the first week.
L-AmB showed a favourable safety profile under both the 10 mg/kg single-dose and 3 mg/kg/day 7-day regimens. This was supported by baseline renal and electrolyte monitoring and intravenous potassium supplementation for patients with normal renal function; only six patients required extra oral supplementation due to hypokalaemia.
ADR analysis revealed a predictable pattern of mild, manageable toxicity. We observed a statistically significant but clinically modest decline in haemoglobin and potassium, and a transient increase in creatinine within the first three days, with stabilization or recovery by day seven. These findings align with the known toxicity profile of L-AmB and confirm that outpatient monitoring is feasible without hospitalization. The absence of significant differences between regimens further supports the flexibility of this approach..
4.3. High RIC at 6 Months
No published data were identified regarding treatment retention among patients with cryptococcal meningitis, as most studies focus on short-term mortality, typically assessed up to 10 weeks after diagnosis.
Among 83 CM patients assessed, 52 who initiated treatment at CRAM and 31 referred post-induction from other facilities, the retention remained high: 81.9% (68/83) at six months, 74% (54/73) at 12 months, and 70.4% (38/54) at 24 months. The retention outcomes in the CRAM cohort can be attributed to the fact that patients receive comprehensive care in a single facility, eliminating the need to navigate multiple health services.
By incorporating induction therapy within a specialized ambulatory clinic, the CRAM model effectively bridges the gap between inpatient and outpatient care. This integration mitigates patient drop-off commonly driven by the complexity of care pathways for advanced HIV disease (AHD), which frequently lead to disengagement [15]. CRAM’s “one-stop-shop” approach, encompassing cryptococcal meningitis (CM) treatment, antiretroviral therapy (ART), and management of other opportunistic infections (OIs) addresses structural barriers and care fragmentation, thereby promoting sustained patient engagement. These findings suggest that a dedicated outpatient model for AHD is not only feasible but may outperform traditional systems in retaining patients over time.
4.4. Other Findings: High Burden of Concurrent TB
In our cohort, TB was diagnosed and treated in 56.6% of patients (n=47), reflecting the CRAM’s rigorous and systematic TB screening protocol at entry. This protocol includes clinical examination, digital chest radiography (CXR), TB LAM and other molecular tests as indicated, as well as focused assessments using sonography and retinoscopy to detect extrapulmonary TB in patients with CD4 counts below 100 cells/μL.
A study about short-term mortality in 678 CM patients in 4 African countries (Malawi, Tanzania, Zambia and Cameroon), recruited between 2013 and 2016, reported TB co-infection in 98 patients (14.5% of CM enrolled patients) [12]
The remarkably high rate observed in our Mozambican cohort underscores the critical importance of integrated “AHD care packages” that bundle CrAg screening with intensive TB diagnostics, such as systematic symptom screening and WHO-recommended urine lateral flow lipoarabinomannan (LF-LAM) testing. The presence of TB in over half of patients highlights a key challenge in CM management: TB co-infection can complicate clinical presentation, exacerbate drug interactions and toxicities, and potentially worsen outcomes. Therefore, the success of the CRAM ambulatory model may not solely be due to the effective delivery of antifungal therapy but could also stem from its capacity to provide simultaneous, coordinated management for TB and other AHD-defining conditions within a single, patient-centred facility. This integrated approach is essential for addressing the complex syndemic of HIV, TB, and cryptococcosis in the region.
4.5. Strengths and Limitations
This study has several strengths. Firstly, it provides critical real-world evidence from a programmatic setting in SSA, demonstrating the feasibility and effectiveness of a fully ambulatory model for CM induction therapy, a care approach not yet widely endorsed in international guidelines. The cohort represents a typical, highly vulnerable population with AHD, characterized by severe immunosuppression and a high burden of comorbidities like TB, thus enhancing the generalizability of our findings to similar resource-limited contexts. Furthermore, the analysis of retention over a 24-month period provides valuable long-term insights that go beyond the typical short-term outcomes reported in many CM studies.
However, several limitations must be acknowledged. The single-centre, observational design of our study limits causal inference and may affect the generalizability of findings to other settings with different healthcare infrastructures or patients’ populations. The relatively small sample size reduces analytical power and the ability to detect rare adverse events. The retrospective collection of data from routine clinical records carries a risk of missing or inconsistently recorded information, such as the precise grading of ADR or detailed neurological outcomes. Finally, the exclusion of 31 patients who received induction therapy elsewhere, while methodologically sound for the HFS analysis, means our primary safety and efficacy results are based on a subset of the total cohort managed at the clinic. Future prospective, multi-centre studies with larger sample sizes are warranted to confirm these promising findings.
5. Conclusions
Despite the widespread perception that CM is a severe condition that can only be managed in a hospital setting under inpatient care, the results from the CRAM cohort demonstrate that this disease can be effectively treated and achieve excellent outcomes without the need for hospitalization.
It is likely that CRAM’s status as a primary-level health unit has facilitated earlier access to care and diagnosis of advanced HIV disease and cryptococcal infection, which may have contributed to improved treatment outcomes.
Author Contributions
M.R. major contribution to the study design, data acquisition, study implementation, analysis and implementation of data, first draft writing and approved the final version. A.C, I.G., E.F., I.N. contributed equally to study implementation, writing, reading and approved final version. L.A., G.M., A.G. & R.B., contributed to data acquisition, and read and approved final version. J.L., F.M. & E.N. equally contributed to the analysis and interpretation of data, reviewing, writing, reading and approved the final version.
Funding
This work results from a collaborative among MSF, I-TECH and the Mozambican MoH. I-TECH was responsible for the clinical management of PLWH, including diagnose, lab results interpretation, and clinical follow up. Data analysis and manuscript writing were conducted through an equal collaboration between I-TECH, and the MoH. The I-TECH Mozambique clinical work at the facility (CRAM) was funded by the U.S. Department of Health and Human Services (HHS) – CDC (NU2GGH002374). The content and conclusions presented herein are solely the responsibility of the authors and should not be interpreted as representing official statements or policies. Consequently, no endorsement by CDC, HHS, or the U.S. Government should be inferred.
Institutional Review Board Statement
Ethical clearance was obtained from the Gaza Institutional Bioethics Committee for Health (IRB0002657 – Comité Institucional de Bioética para a Saúde de Gaza, nr: 58/CIBS-Gaza/2024) and National Bioethics Committee for Health (IRB0002657 - Comité Nacional de Bioética para a Saúde, nr: 21/CIBS/2025. permission to perform this evaluation was also obtained from the Health Service of Maputo city (Serviço de Saúde da Cidade, N/Ref. no. 7002/2103/SSCM/2024). Because this analysis only involved assessment of routine administrative data collected for programmatic purposes, this analysis is considered Non-Research from the University of Washington and CDC. This evaluation fulfilled the exemption criteria set by the CDC – Atlanta Ethics Review Board for a posteriori analyzes of routinely-collected clinical data and thus did not require, PRA, CDC IRB or HRPO review.
Informed Consent Statement
Informed consent to participate in the routine program was waived by IRB because we performed our analysis on routine administrative data. All information obtained during the analysis was kept confidential. The analysis was performed on de-identified aggregated data. Furthermore, this analysis was conducted in accordance with the principles of the Declaration of Helsinki.
Data Availability Statement
The datasets utilized in this study are available from the corresponding author upon reasonable request; however, they are not publicly accessible due to privacy constraints.
Acknowledgments
The authors thank all the staff of the Centro de Referência de Alto-Maé (CRAM), Gaza, Mozambique for their co-operation, and their excellent technical assistance.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| aOR: | Adjusted odds ratios |
| ADR: | Adverse drug reactions |
| AHD: | Advanced HIV Disease |
| ART: | Antiretroviral therapy |
| CI: | Confidence intervals |
| CM: | Cryptococcal meningitis |
| CrAg: | Cryptococcal Antigen |
| CSF: | Cerebrospinal fluid |
| CRAM: | Centro de Referência de Alto-Maé |
| IQR: | Interquartile range |
| HFS: | Hospitalization-free survival |
| I-TECH | International training and education center for health |
| L-AmB | Liposomal Amphotericin B |
| OIs: | Opportunistic infections |
| PHC: | Primary healthcare centre |
| PLWH: | People living with HIV |
| MoH: | Ministry of Health |
| MSF: | Médecins Sans Frontières |
| SD: | Standard deviation |
| SSA: | sub-Saharan Africa |
| TB: | Tuberculosis |
References
- Lin, F. Tuberculous meningitis diagnosis and treatment: classic approaches and high-throughput pathways. Front. Immunol. 2025, 15, 1543009. [Google Scholar] [CrossRef]
- Kalita, J.; Misra, U.K.; Ranjan, P. Predictors of long-term neurological sequelae of tuberculous meningitis: a multivariate analysis. Eur. J. Neurol. 2007, 14, 33–37. [Google Scholar] [CrossRef]
- Manyelo, C.M.; Solomons, R.S.; Walzl, G.; Chegou, N.N. Tuberculous Meningitis: Pathogenesis, Immune Responses, Diagnostic Challenges, and the Potential of Biomarker-Based Approaches. J. Clin. Microbiol. 2021, 59. [Google Scholar] [CrossRef]
- Estela Isabel, B.; Pando Rogelio, H. Pathogenesis and Immune Response in Tuberculous Meningitis. 2014, 21, 4–10. [Google Scholar]
- Dastur, D.K.; Manghani, D.K.; Udani, P. PATHOLOGY AND PATHOGENETIC MECHANISMS IN NEUROTUBERCULOSIS. Radiol. Clin. North Am. 1995, 33, 733–752. [Google Scholar] [CrossRef] [PubMed]
- Thwaites, G.; Chau, T.T.H.; Mai, N.T.H.; Drobniewski, F.; McAdam, K.; Farrar, J. Neurological aspects of tropical disease: Tuberculous meningitis. J. Neurol. Neurosurg. Psychiatry 2000, 68, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.-F.; Leng, E.-L.; Liu, S.-M.; Zhou, Y.-L.; Luo, C.-Q.; Xiang, Z.-B.; Cai, W.; Rao, W.; Hu, F.; Zhang, P.; et al. Recent advances in microbiological and molecular biological detection techniques of tuberculous meningitis. Front. Microbiol. 2023, 14, 1202752. [Google Scholar] [CrossRef]
- WHO, “Global Tuberculosis Report 2024,” World Health Organization, Geneva, 2024. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2024.
- Kwan, C.K.; Ernst, J.D. HIV and Tuberculosis: a Deadly Human Syndemic. Clin. Microbiol. Rev. 2011, 24, 351–376. [Google Scholar] [CrossRef]
- von Gottberg, A.; Meintjes, G. Meningitis: a frequently fatal diagnosis in Africa. Lancet Infect. Dis. 2019, 19, 676–678. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Gertz, A.M.; Lawrence, D.S.; Wills, N.K.; Guthrie, B.L.; Farquhar, C.; Jarvis, J.N. Mortality from HIV-associated meningitis in sub-Saharan Africa: a systematic review and meta-analysis. J. Int. AIDS Soc. 2020, 23, e25416. [Google Scholar] [CrossRef]
- MISAU PNCT (Programa Nacional de Controlo da Tuberculose), Relatorio Anual de Tuberculose 2024, Moçambique; Ministério da Saúde de Moçambique.
- MISAU PNCT (Programa Nacional de Controlo da Tuberculose), “Relatorio Anual de Tuberculose 2023, Moçambique,” MISAU, Maputo, 2023. Accessed: Jun. 27, 2025. Available online: https://www.scribd.com/document/860655980/Relatorio-Anual-Do-PNCT-2023-29042024.
- MISAU PNCT (Programa Nacional de Controlo da Tuberculose), Plano Estratégico Nacional para acabar com a Tuberculose em Moçambique 2023 - 2030; Ministério da Saúde: Maputo, 2023.
- MISAU PNCT (Programa Nacional de Combate a Tuberculose, “Manuais de Directrizes e Guiões de TB, Moçambique,” Ministério da Saúde de Moçambique. 24 Mar 2022. Available online: https://www.misau.gov.mz/index.php/manuais-directrizes-e-guioes-tb.
- MISAU PNCT (Programa Nacional de Controlo da Tuberculose), Manual de Manejo Clínico e Programático da Tuberculose Multirresistente; Moçambique, Sep 2019.
- Nacarapa, E.; Muchiri, E.; Moon, T.D.; Charalambous, S.; E Verdu, M.; Ramos, J.M.; Valverde, E.J. Effect of Xpert MTB/RIF testing introduction and favorable outcome predictors for tuberculosis treatment among HIV infected adults in rural southern Mozambique. A retrospective cohort study. PLOS ONE 2020, 15, e0229995. [Google Scholar] [CrossRef]
- Poh, X.Y.; Loh, F.K.; Friedland, J.S.; Ong, C.W.M. Neutrophil-Mediated Immunopathology and Matrix Metalloproteinases in Central Nervous System – Tuberculosis. Front. Immunol. 2022, 12, 788976. [Google Scholar] [CrossRef]
- Nacarapa, E.; Verdu, M.E.; Nacarapa, J.; Macuacua, A.; Chongo, B.; Osorio, D.; Munyangaju, I.; Mugabe, D.; Paredes, R.; Chamarro, A.; et al. Predictors of attrition among adults in a rural HIV clinic in southern Mozambique: 18-year retrospective study. Sci. Rep. 2021, 11, 17897. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Su, B.; Zhang, X.; Liu, Y.; Wu, H.; Zhang, T. Incomplete immune reconstitution in HIV/AIDS patients on antiretroviral therapy: Challenges of immunological non-responders. J. Leukoc. Biol. 2020, 107, 597–612. [Google Scholar] [CrossRef]
- ASHM Developing a sustainable HIV, “Immunological failure: persistent CD4+ T cell deficiency”. 20 Apr 2022. Available online: https://hivmanagement.ashm.org.au/long-term-management-of-antiretroviral-therapy/immunological-failure-persistent-cd4-t-cell-deficiency/.
- WHO. HIV PREVENTION, INFANT DIAGNOSIS. In ANTIRETROVIRAL INITIATION AND MONITORING GUIDELINES; 2021. [Google Scholar]
- MISAU PNC ITS-HIV/SIDA, “Guião de manejo do paciente com doença avançada por HIV - 2022,” Ministério da Saúde de Moçambique. Accessed: Oct. 15, 2023. Available online: https://www.misau.gov.mz/index.php/guioes-de-prevencao-e-de-cuidados-e-tratamento?download=1352:guiao-de-manejo-do-paciente-com-doenca-avancada-por-hiv-2022.
- MISAU PNC ITS-HIV/SIDA, “Normas Clinicas Actualizadas para o seguimento do paciente HIV Positivo,” Comite TARV Mozambique. 14 Nov 2023. Available online: https://comitetarvmisau.co.mz/docs/orientacoes_nacionais/Circular_Normas_Cl%C3%ADnicas_Actualizadas_29_11_19.pdf.
- MISAU PNC ITS-HIV/SIDA, “Programa Nacional de Controle de ITS-HIV/SIDA - Directrizes nacionais,” Ministério da Saúde de Moçambique, Accessed: Mar. 26, 2022. Available online: https://www.misau.gov.mz/index.php/hiv-sida-directrizes-nacionais.
- Chun, H.M.; Milligan, K.; Boyd, M.A.; Abutu, A.; Bachanas, P.; Dirlikov, E. Reaching HIV epidemic control in Nigeria using a lower HIV viral load suppression cut-off. AIDS 2023, 37, 2081–2085. [Google Scholar] [CrossRef] [PubMed]
- Bavinton, B.R.; Rodger, A.J. Undetectable viral load and HIV transmission dynamics on an individual and population level: where next in the global HIV response? Curr. Opin. Infect. Dis. 2020, 33, 20–27. [Google Scholar] [CrossRef] [PubMed]
- HIV.gov. “Viral Suppression and an Undetectable Viral Load,” HIV.gov. 13 Feb 2025. Available online: https://www.hiv.gov/hiv-basics/staying-in-hiv-care/hiv-treatment/viral-suppression.
- Handoko, R.; Colby, D.J.; Kroon, E.; Sacdalan, C.; de Souza, M.; Pinyakorn, S.; Prueksakaew, P.; Munkong, C.; Ubolyam, S.; Akapirat, S.; et al. Determinants of suboptimal CD4+ T cell recovery after antiretroviral therapy initiation in a prospective cohort of acute HIV-1 infection. J. Int. AIDS Soc. 2020, 23. [Google Scholar] [CrossRef]
- Rad, M.M.; Haddad, M.; Sheybani, F.; Shirazinia, M.; Dadgarmoghaddam, M. Mortality predictors and diagnostic challenges in adult tuberculous meningitis: a retrospective cohort of 100 patients. Trop. Med. Heal. 2025, 53, 58. [Google Scholar] [CrossRef]
- Yasar, K.K.; Pehlivanoglu, F.; Sengoz, G. Predictors of mortality in tuberculous meningitis: a multivariate analysis of 160 cases. 2010, 14, 1330–5. [Google Scholar]
- Chen, X.; Wei, J.; Zhang, M.; Su, B.; Ren, M.; Cai, M.; Zhang, Y.; Zhang, T. Prevalence, incidence, and case fatality of tuberculous meningitis in adults living with HIV: a systematic review and meta-analysis. BMC Public Heal. 2024, 24, 2145. [Google Scholar] [CrossRef]
- Loghin, I.I.; Vâță, A.; Miftode, E.G.; Cobaschi, M.; Rusu, Ș.A.; Silvaș, G.; Frăsinariu, O.E.; Dorobăț, C.M. Characteristics of Tuberculous Meningitis in HIV-Positive Patients from Northeast Romania. Clin. Pr. 2023, 13, 1488–1500. [Google Scholar] [CrossRef]
- Kosgei, R.J.; Callens, S.; Gichangi, P.; Temmerman, M.; Kihara, A.-B.; David, G.; Omesa, E.N.; Masini, E.; Carter, E.J. Gender difference in mortality among pulmonary tuberculosis HIV co-infected adults aged 15-49 years in Kenya. PLOS ONE 2020, 15, e0243977. [Google Scholar] [CrossRef] [PubMed]
- Alebel, A.; Demant, D.; Petrucka, P.; Sibbritt, D. Effects of undernutrition on mortality and morbidity among adults living with HIV in sub-Saharan Africa: a systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 1–20. [Google Scholar] [CrossRef]
- Min, J.; Kim, J.S.; Kim, H.W.; Ko, Y.; Oh, J.Y.; Jeong, Y.-J.; Lee, E.H.; Yang, B.; Lee, K.M.; Ahn, J.H.; et al. Effects of underweight and overweight on mortality in patients with pulmonary tuberculosis. Front. Public Heal. 2023, 11, 1236099. [Google Scholar] [CrossRef]
- Guo, C.; Liu, K.-W.; Tong, J.; Gao, M.-Q. Prevalence and prognostic significance of malnutrition risk in patients with tuberculous meningitis. Front. Public Health 12, 1391821. [CrossRef] [PubMed]
- Huang, M.; Ma, Y.; Ji, X.; Jiang, H.; Liu, F.; Chu, N.; Li, Q. A study of risk factors for tuberculous meningitis among patients with tuberculosis in China: An analysis of data between 2012 and 2019. Front. Public Heal. 10, 1040071. [CrossRef] [PubMed]
- Ojo, T.; Ruan, C.; Hameed, T.; Malburg, C.; Thunga, S.; Smith, J.; Vieira, D.; Snyder, A.; Tampubolon, S.J.; Gyamfi, J.; et al. HIV, Tuberculosis, and Food Insecurity in Africa—A Syndemics-Based Scoping Review. Int. J. Environ. Res. Public Heal. 2022, 19, 1101. [Google Scholar] [CrossRef]
- Wambua, J.; Ali, A.; Ukwizabigira, J.B.; Kuodi, P. Prevalence and risk factors of under-five mortality due to severe acute malnutrition in Africa: a systematic review and meta-analysis. Syst. Rev. 2025, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Gu, Z.; Chen, X.; Yu, X.; Meng, X. Analysis of risk factors for long-term mortality in patients with stage II and III tuberculous meningitis. BMC Infect. Dis. 2024, 24, 656. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.C.; Sawaya, A.L.; Wibaek, R.; Mwangome, M.; Poullas, M.S.; Yajnik, C.S.; Demaio, A. The double burden of malnutrition: aetiological pathways and consequences for health. Lancet 2019, 395, 75–88. [Google Scholar] [CrossRef]
- Azomahou, T.T.; Diene, B.; Gosselin-Pali, A. Transition and persistence in the double burden of malnutrition and overweight or obesity: Evidence from South Africa. Food Policy 2022, 113, 102303. [Google Scholar] [CrossRef]
- Dodd, P.J.; Osman, M.; Cresswell, F.V.; Stadelman, A.M.; Lan, N.H.; Thuong, N.T.T.; Muzyamba, M.; Glaser, L.; Dlamini, S.S.; Seddon, J.A. The global burden of tuberculous meningitis in adults: A modelling study. PLOS Glob. Public Heal. 2021, 1, e0000069. [Google Scholar] [CrossRef]
- Thao, L.T.P.; Heemskerk, A.D.; Geskus, R.B.; Mai, N.T.H.; Ha, D.T.M.; Chau, T.T.H.; Phu, N.H.; Chau, N.V.V.; Caws, M.; Lan, N.H.; et al. Prognostic Models for 9-Month Mortality in Tuberculous Meningitis. Clin. Infect. Dis. 66, 523–532. [CrossRef] [PubMed]
- Vinnard, C.; Macgregor, R.R. Tuberculous meningitis in HIV-infected individuals. Curr. HIV/AIDS Rep. 2009, 6, 139–145. [Google Scholar] [CrossRef]
- Nacarapa, E.; Munyangaju, I. Isabelle; Osório, D.; Ramos-Rincon, J.-M. “Mortality and Predictors of Poor Outcomes among Persons with HIV and Tuberculous Meningitis, in Mozambique,” Jul. 02, 2025, Preprints. [CrossRef]
- Jain, S.K.; Tobin, D.M.; Tucker, E.W.; Venketaraman, V.; Ordonez, A.A.; Jayashankar, L.; Siddiqi, O.K.; Hammoud, D.A.; Prasadarao, N.V.; et al.; on behalf of the NIH Tuberculous Meningitis Writing Group Tuberculous meningitis: a roadmap for advancing basic and translational research. Nat. Immunol. 2018, 19, 521–525. [Google Scholar] [CrossRef]
- A Seddon, J.; Tugume, L.; Solomons, R.; Prasad, K.; Bahr, N.C. Tuberculous Meningitis International Research Consortium The current global situation for tuberculous meningitis: epidemiology, diagnostics, treatment and outcomes. Wellcome Open Res. 2019, 4, 167. [Google Scholar] [CrossRef]
- Slane, V. H.; Unakal, C. G. Tuberculous Meningitis; 2025. [Google Scholar]
- Chin, J.H. Tuberculous meningitis. Neurol. Clin. Pr. 2014, 4, 199–205. [Google Scholar] [CrossRef]
- Ieque, A.L.; Palomo, C.T.; Moreira, D.d.C.; Meneguello, J.E.; Murase, L.S.; Silva, L.L.; Baldin, V.P.; Caleffi-Ferracioli, K.R.; Siqueira, V.L.D.; Cardoso, R.F.; et al. Systematic review of tuberculous meningitis in high-risk populations: mortality and diagnostic disparities. Futur. Microbiol. 20, 559–571. [CrossRef]
- Zhu, X.; Li, R.; Zhang, X.; Wang, D.; Wang, Y.; Lin, W.; Zhang, S.; Chu, M.; Wei, L. Clinical indicators associated with tuberculous meningitis using multiple correspondence analysis. Diagn. Microbiol. Infect. Dis. 2025, 113, 116932. [Google Scholar] [CrossRef]
- Nacarapa, E.; Munyangaju, I.; Osório, D.; Zindoga, P.; Mutaquiha, C.; Jose, B.; Macuacua, A.; Chongo, B.; De-Almeida, M.; Verdu, M.-E.; et al. Extrapulmonary tuberculosis mortality according to clinical and point of care ultrasound features in Mozambique. Sci. Rep. 2022, 12, 16675. [Google Scholar] [CrossRef]
- Saukkonen, J.J.; Duarte, R.; Munsiff, S.S.; Winston, C.A.; Mammen, M.J.; Abubakar, I.; Acuña-Villaorduña, C.; Barry, P.M.; Bastos, M.L.; Carr, W.; et al. Updates on the Treatment of Drug-Susceptible and Drug-Resistant Tuberculosis: An Official ATS/CDC/ERS/IDSA Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2025, 211, 15–33. [Google Scholar] [CrossRef] [PubMed]
- Nacarapa, E.; Jose, B.; Munyangaju, I.; Osório, D.; Ramos-Rincon, J.-M. “Incidence and Predictors of Mortality Among Persons With Drug Resistant Tuberculosis, and HIV, Mozambique (2015-2020),” Oct. 17, 2024, PREPRINT (Version 1) available at Research Square; Berlin/Heidelberg, Germany. [CrossRef]
- Navarro-Flores, A.; Fernandez-Chinguel, J.E.; Pacheco-Barrios, N.; Soriano-Moreno, D.R.; Pacheco-Barrios, K. Global morbidity and mortality of central nervous system tuberculosis: a systematic review and meta-analysis. J. Neurol. 2022, 269, 3482–3494. [Google Scholar] [CrossRef] [PubMed]
- Marx, G.E.; Chan, E.D. Tuberculous Meningitis: Diagnosis and Treatment Overview. Tuberc. Res. Treat. 2011, 2011, 798764. [Google Scholar] [CrossRef] [PubMed]
- Murthy, J.M.K. Management of Intracranial Pressure in Tuberculous Meningitis. Neurocritical Care 2005, 2, 306–312. [Google Scholar] [CrossRef]
- Abdella, A.; Deginet, E.; Weldegebreal, F.; Ketema, I.; Eshetu, B.; Desalew, A. Tuberculous Meningitis in Children: Treatment Outcomes at Discharge and Its Associated Factors in Eastern Ethiopia: A Five Years Retrospective Study. Infect. Drug Resist. 2022, 15, 2743–2751. [Google Scholar] [CrossRef] [PubMed]
- Feng, B.; Fei, X.; Sun, Y.; Zhang, X.; Shang, D.; Zhou, Y.; Sheng, M.; Xu, J.; Zhang, W.; Ren, W. Prognostic factors of adult tuberculous meningitis in intensive care unit: a single-center retrospective study in East China. BMC Neurol. 2021, 21, 308. [Google Scholar] [CrossRef]
- Seid, G.; Alemu, A.; Dagne, B.; Gamtesa, D.F. Microbiological diagnosis and mortality of tuberculosis meningitis: Systematic review and meta-analysis. PLOS ONE 2023, 18, e0279203. [Google Scholar] [CrossRef]
- Oo, N.; K, D. Epidemiology, Pathogenesis, Clinical Manifestations, and Management Strategies of Tuberculous Meningitis. Arch. Intern. Med. Res. 2025, 8, 48–58. [Google Scholar] [CrossRef]
- Gupta, M.; Tobin, E. H.; Munakomi, S. CNS Tuberculosis. 2025. [Google Scholar] [CrossRef]
- Malik, M.A.; Kamran, A.; Ahsan, D.; Amjad, A.; Moatter, S.; Noor, A.; Sohaib, A.; Shaukat, M.; Masood, W.; Hasanain, M.; et al. Advances in management and treatment of tubercular meningitis – a narrative review. Ann. Med. Surg. 2025, 87, 3673–3681. [Google Scholar] [CrossRef] [PubMed]
- Madadi, A.K.; Sohn, M.-J. Comprehensive Therapeutic Approaches to Tuberculous Meningitis: Pharmacokinetics, Combined Dosing, and Advanced Intrathecal Therapies. Pharmaceutics 2024, 16, 540. [Google Scholar] [CrossRef]
- Ariza-Vioque, E.; Ello, F.; Andriamamonjisoa, H.; Machault, V.; González-Martín, J.; Calvo-Cortés, M.C.; Eholié, S.; Tchabert, G.A.; Ouassa, T.; Raberahona, M.; et al. Capacity Building in Sub-Saharan Africa as Part of the INTENSE-TBM Project During the COVID-19 Pandemic. Infect. Dis. Ther. 2022, 11, 1327–1341. [Google Scholar] [CrossRef] [PubMed]
- Evans, E.E.; Avaliani, T.; Gujabidze, M.; Bakuradze, T.; Kipiani, M.; Sabanadze, S.; Smith, A.G.C.; Avaliani, Z.; Collins, J.M.; Kempker, R.R. Long term outcomes of patients with tuberculous meningitis: The impact of drug resistance. PLOS ONE 2022, 17, e0270201. [Google Scholar] [CrossRef]
- Ahinkorah, B.O.; Amadu, I.; Seidu, A.-A.; Okyere, J.; Duku, E.; Hagan, J.E.; Budu, E.; Archer, A.G.; Yaya, S. Prevalence and Factors Associated with the Triple Burden of Malnutrition among Mother-Child Pairs in Sub-Saharan Africa. Nutrients 2021, 13, 2050. [Google Scholar] [CrossRef]
- Maitre, T.; Bonnet, M.; Calmy, A.; Raberahona, M.; Rakotoarivelo, R.A.; Rakotosamimanana, N.; Ambrosioni, J.; Miró, J.M.; Debeaudrap, P.; Muzoora, C.; et al. Intensified tuberculosis treatment to reduce the mortality of HIV-infected and uninfected patients with tuberculosis meningitis (INTENSE-TBM): study protocol for a phase III randomized controlled trial. Trials 2022, 23, 928. [Google Scholar] [CrossRef] [PubMed]
- ANRS Emerging Infectious Diseases, “INTENSE-TBM – Partnering for better care in TB meningitis | Intensified tuberculosis treatment with or without aspirin to reduce the mortality of tuberculous meningitis in HIV infected and uninfected patients: a phase III randomized controlled trial (INTENSE-TBM) | NCT04145258,” European and Developing Countries Clinical Trials Partnership (EDCTP). 19 Aug 2025. Available online: https://intense-tbm.org/clinical-trial/.
Figure 1.
Flowchart of sub-cohort analysis.
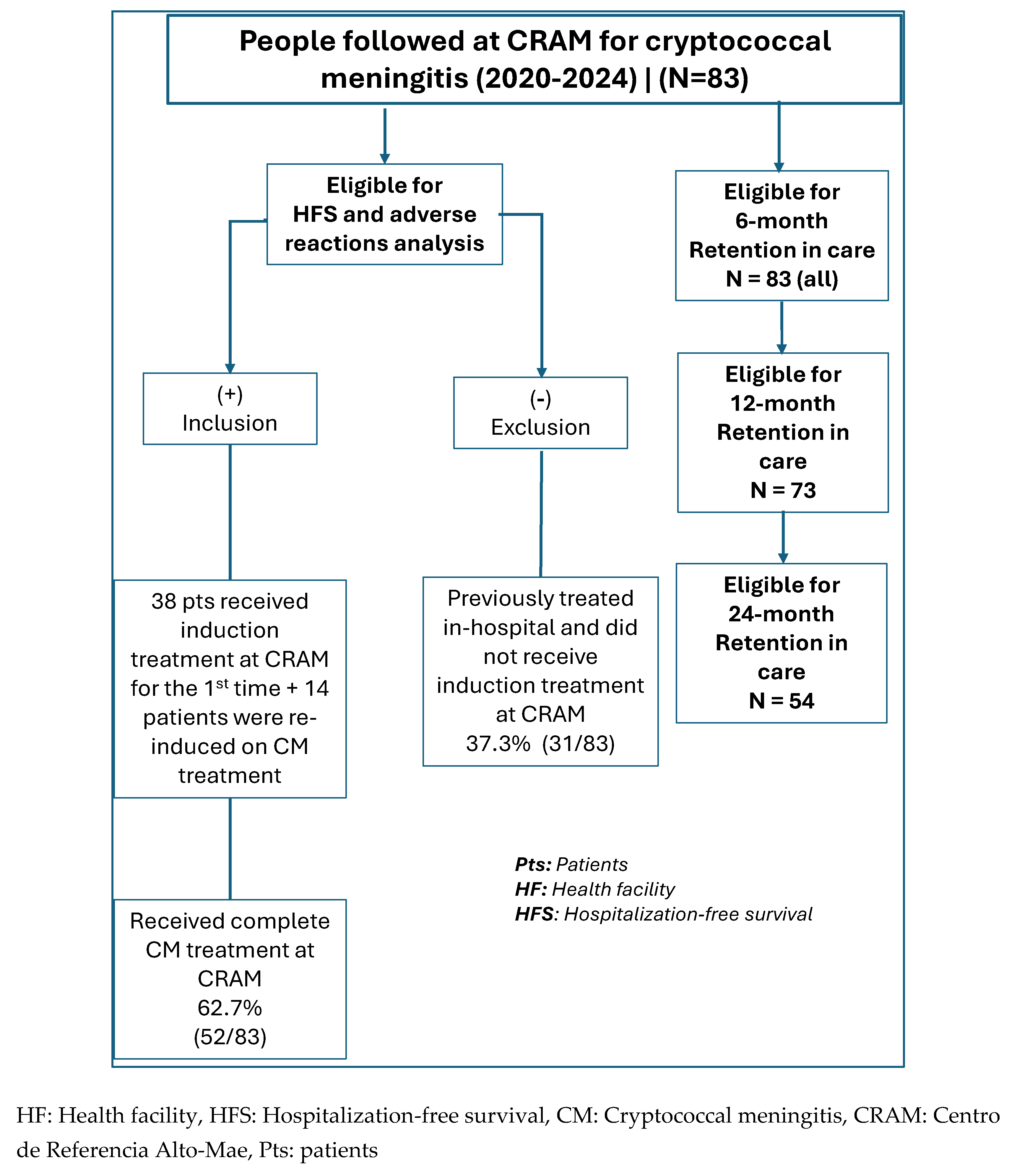
Figure 2.
Short outcome: Hospitalization needs < 10 weeks.
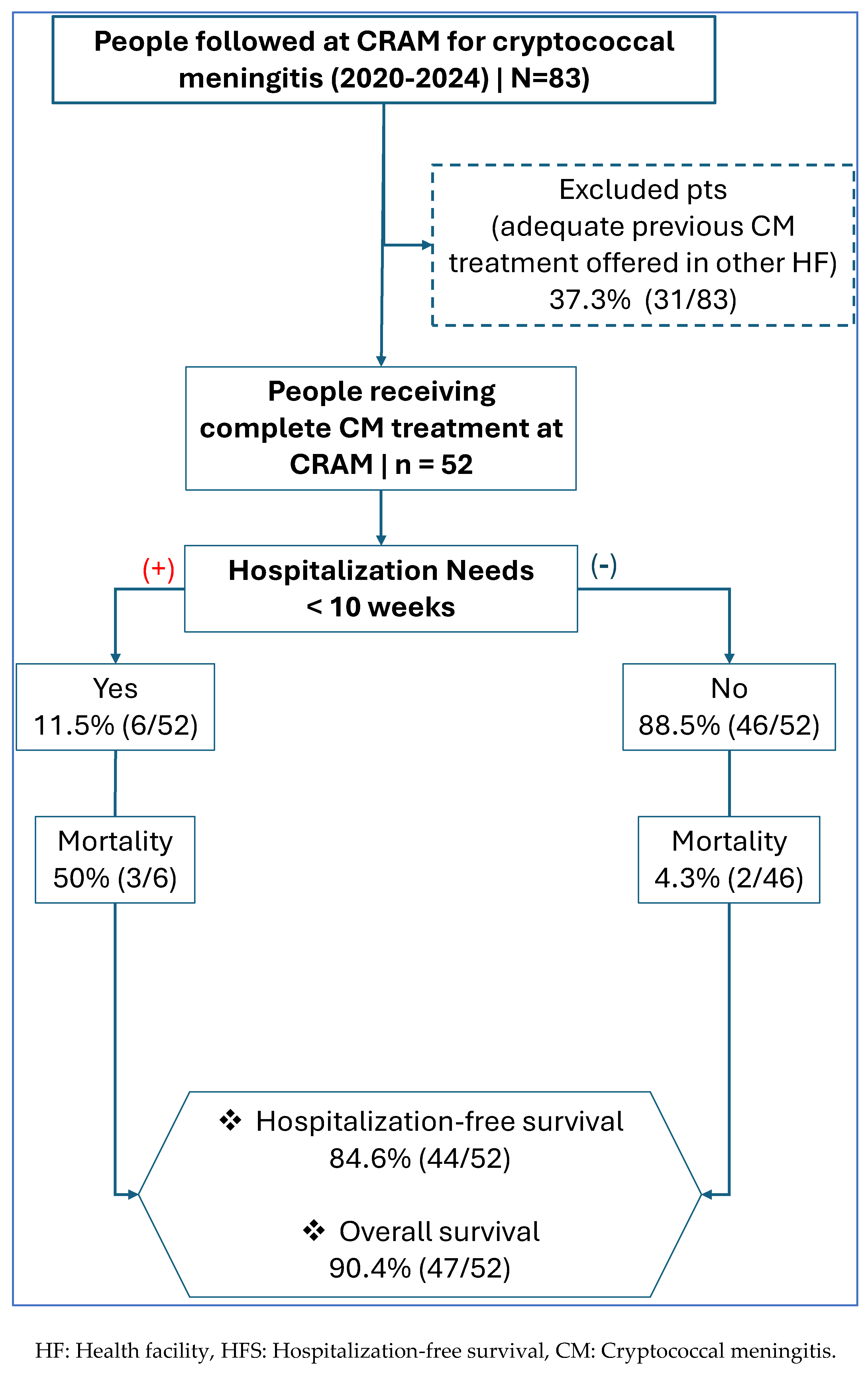
Figure 3.
Kaplan-Meier plot estimating the probability of HFS within the first 10 weeks of outpatient antifungal therapy for CM.
Figure 3.
Kaplan-Meier plot estimating the probability of HFS within the first 10 weeks of outpatient antifungal therapy for CM.
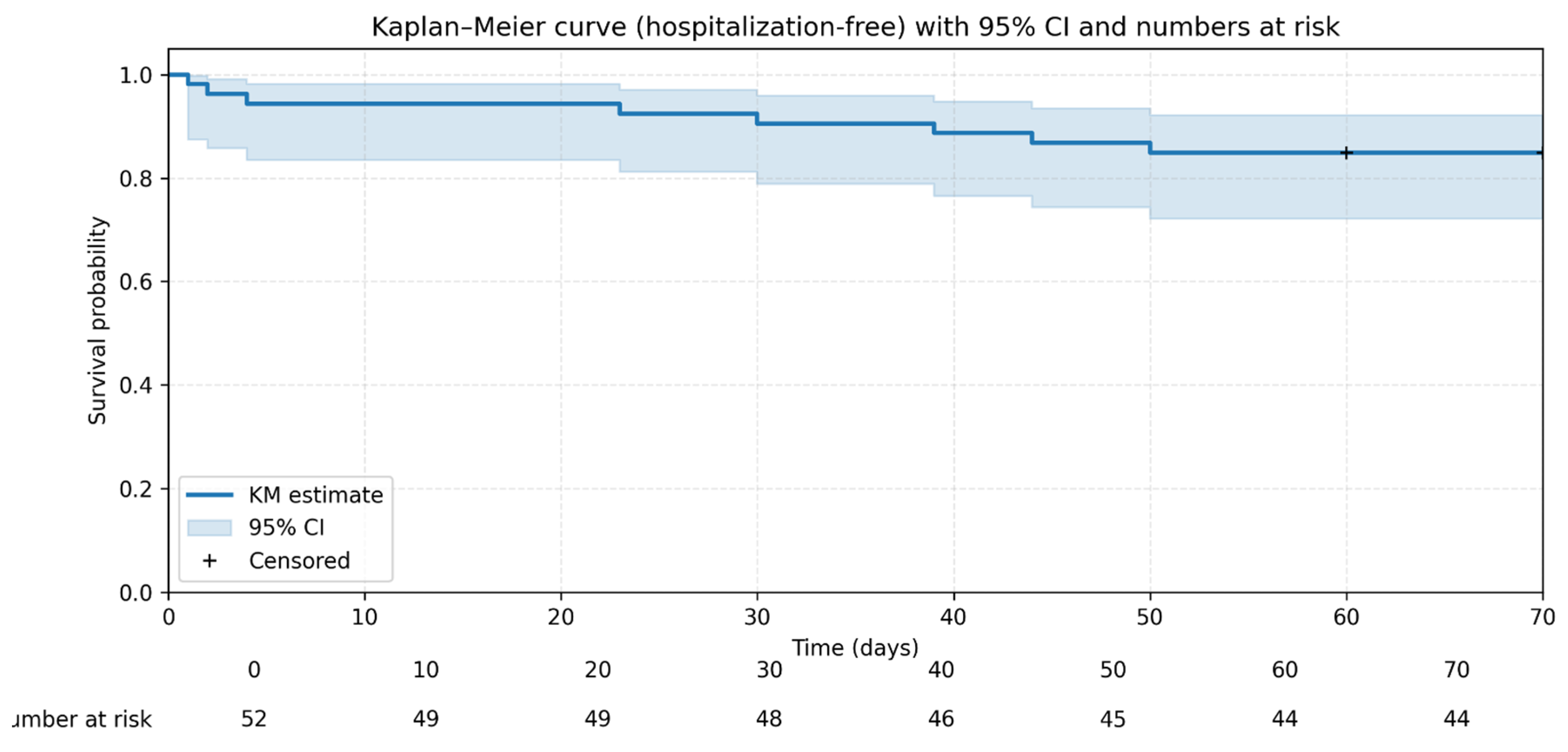
Figure 4.
Retention Trends in CM Follow-up.
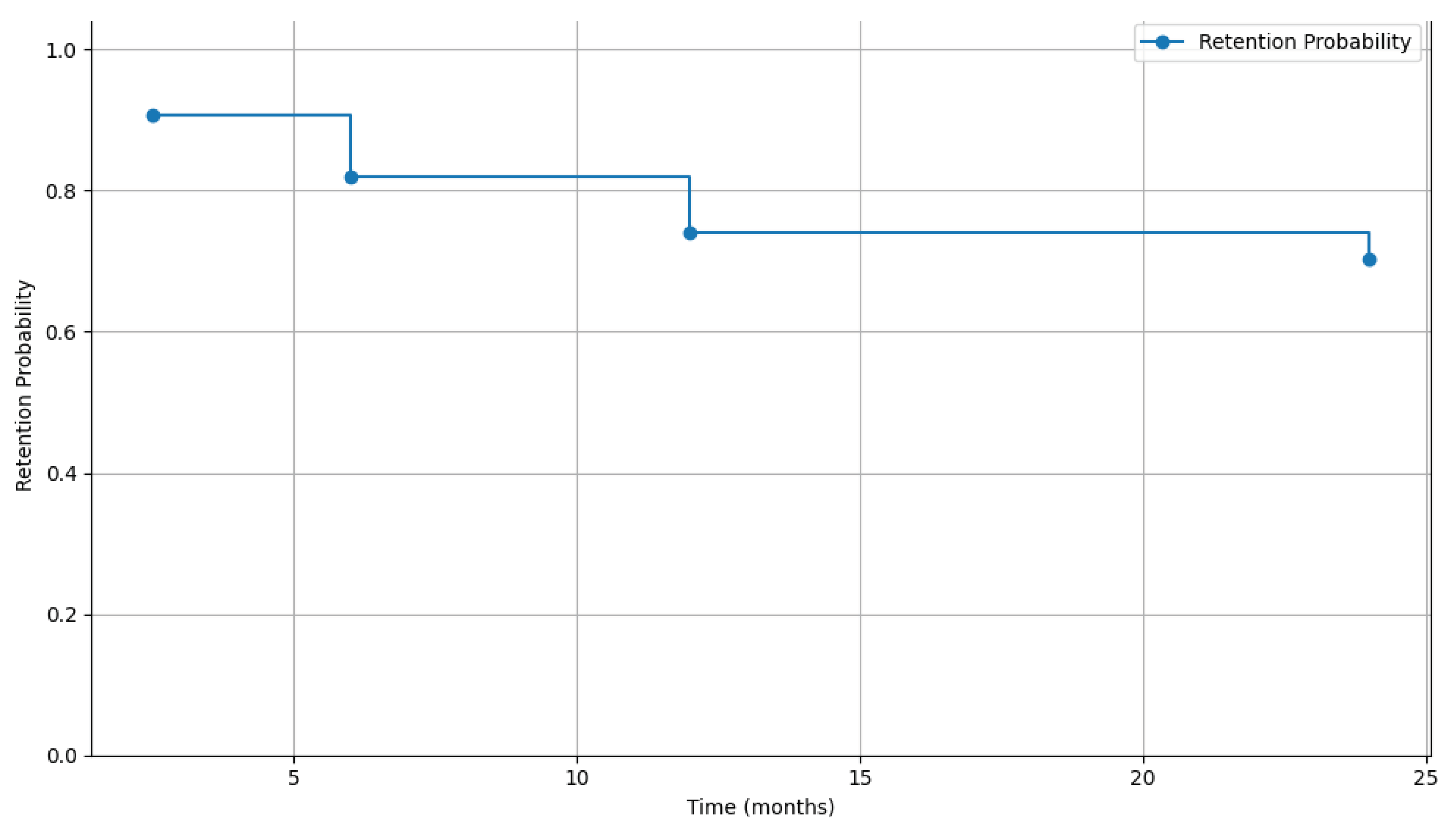

Table 1.
Demographic and clinical characteristics of 83 people followed at CRAM and diagnosed/treated for CM 2020–2024.
Table 1.
Demographic and clinical characteristics of 83 people followed at CRAM and diagnosed/treated for CM 2020–2024.
| Table 1: Demographic and clinical characteristics of 83 people treated with antifungal treatment for cryptococcal meningitis in CRAM, Mozambique 2020–2024 | |||
| Column, N(%) | 95% CI | ||
| N=83 | |||
| Gender | Women | 30 (36.1) | (26.4 - 46.8) |
| Men | 53 (63.9) | (53.2 - 73.6) | |
| Age | Median, Interquartile Range (IQR) | 37 | 27 – 42 |
| Age_band | ≤24 yrs old | 11 (13.3) | (5.8 – 22.5) |
| 25-34 yrs old | 21 (25.3) | (16.5 – 36.0) | |
| 35-44 yrs old | 36 (43.4) | (32.5 – 54.8) | |
| 45-54 yrs old | 11 (13.3) | (6.8 – 22.5) | |
| ≥55 yrs old | 4 (4.8) | (1.3 – 11.9) | |
| Year of diagnosis | 2020 | 7 (8.4) | (3.9 - 15.8) |
| 2021 | 22 (26.5) | (17.9 - 36.7) | |
| 2022 | 20 (24.1) | (15.9 - 34.1) | |
| 2023 | 14 (16.9) | (10.0 - 26.0) | |
| 2024 | 20 (24.1) | (15.9 - 34.1) | |
| Body Mass Index Band | BMI > 18.5 | 39 (50.0) | (39.1 - 60.9) |
| BMI < 18.4 | 39 (50.0) | (39.1 - 60.9) | |
| CD4 cell count cells/uL | Median, Interquartile Range (IQR) | 61 | 27 – 105 |
| CD4 Band at CRAM Entry | CD4 < 50 Cell/uL | 34 (41.0) | (30.3 – 52.3) |
| CD4 [51-99] Cell/uL | 27 (32.5) | (22.7 – 43.6) | |
| CD4 > 100 Cell/uL | 22 (26.5) | (17.4 – 37.4) | |
| Antifungal therapy prior to CRAM | Antifungal therapy initiated at CRAM | 38 (45.8) | (35.4 - 56.5) |
| Antifungal therapy prior to CRAM | 45 (54.2) | (43.5 - 64.6) | |
| Induction therapy at CRAM | No (amphotericin received at other HF) | 31 (37.3) | (27.5 - 48.0) |
| Yes (amphotericin received at CRAM) | 52 (62.7) | (52.0 - 72.5) | |
| Amphotericin | Single Dose | 39 (47.0) | (36.5 - 57.7) |
| Multiple Dose | 44 (53.0) | (42.3 - 63.5) | |
| ART vs CM Timeline | Pre-ART or ≤ 30 days on ART | 39 (47.0) | (36.5 - 57.7) |
| Experienced ART > 30 days and active | 21 (25.3) | (16.9 - 35.4) | |
| Experienced ART > 30 days but with ART interruption on admission | 23 (27.7) | (19.0 - 38.0) | |
| Clinical features: Asymptomatic | Asymptomatic | 4 (4.8) | (1.6 - 11.1) |
| Symptomatic | 79 (95.2) | (88.9 - 98.4) | |
| Clinical features: Cefaleia | No headache | 5 (6.0) | (2.3 - 12.7) |
| headache | 78 (94.0) | (87.3 - 97.7) | |
| Clinical features: Vomiting | No vomiting | 56 (67.5) | (56.9 - 76.8) |
| Vomiting | 27 (32.5) | (23.2 - 43.1) | |
| Clinical features: Agitation/bizarre behavior, Incoherent speech, Delusions and/or hallucination | No Agitation/bizarre behavior | 67 (80.7) | (71.3 - 88.1) |
| Agitation/bizarre behavior | 16 (19.3) | (11.9 - 28.7) | |
| Clinical features: Meningeal signs | No Meningeal signs | 57 (68.7) | (58.2 - 77.9) |
| Meningeal signs | 26 (31.3) | (22.1 - 41.8) | |
| Clinical features: Decreased visual acuity/Blindness | No Decreased visual acuity/Blindness; | 64 (77.1) | (67.2 - 85.1) |
| Decreased visual acuity/Blindness; | 19 (22.9) | (14.9 - 32.8) | |
| Clinical features: Photophobia | No Photophobia | 67 (80.7) | (71.3 - 88.1) |
| Photophobia | 16 (19.3) | (11.9 - 28.7) | |
| Clinical features: Diplopia /CN-VI palsy | No Diplopia /CN-VI palsy | 75 (90.4) | (82.6 - 95.3) |
| Diplopia /CN-VI palsy | 8 (9.6) | (4.7 - 17.4) | |
| Clinical features: Hypoacusis | No Hypoacusis | 75 (90.4) | (82.6 - 95.3) |
| Hypoacusis | 8 (9.6) | (4.7 - 17.4) | |
| Clinical features: Seizures | No Seizures | 77 (92.8) | (85.7 - 96.9) |
| Seizures | 6 (7.2) | (3.1 - 14.3) | |
| Clinical features: Reduced Glasgow Coma Scale | No Reduced GCS | 82 (98.8) | (94.5 - 99.9) |
| Reduced | 1 (1.2) | (0.1 - 5.5) | |
| Frequency of lumbar punctures (LP) | Not performed | 4 (5.1) | (1.4 - 12.5) |
| 1 LP (initial) | 34 (43.0) | (32.1 - 54.6) | |
| 2-5 LP | 38 (48.1) | (36.9 - 59.5) | |
| ≥6 LP | 7 (8.9) | (3.6 - 17.5) | |
| Opening cerebrospinal fluid pressure (OP CSF) | OP CSF ≤20 cmH₂O | 9 (12.9) | (6.1 - 23.0) |
| OP CSF [21-40] cmH₂O | 29 (41.4) | (29.9 - 53.7) | |
| OP CSF ≥41 cmH₂O | 32 (45.7) | (34.0 - 57.9) | |
| Other Active Opportunistic Disease: TB | No Acive TB | 36 (43.4) | (33.1 - 54.1) |
| Active TB | 47 (56.6) | (45.9 - 66.9) | |
| Other Active Opportunistic Disease: Oral Candida | No Active Oral Candida | 65 (78.3) | (68.6 - 86.1) |
| Active Oral Candida | 18 (21.7) | (13.9 - 31.4) | |
| Other Active Opportunistic Disease: Chronic Diarrhoea | No Active Chronic diarrhea | 77 (92.8) | (85.7 - 96.9) |
| Active Chronic Diarrhea | 6 (7.2) | (3.1 - 14.3) | |
| Active Opportunistic Disease: Kaposi sarcoma | No Kaposi Sarcoma | 78 (94.0) | (87.3 - 97.7) |
| Active Kaposi Sarcoma | 5 (6.0) | (2.3 - 12.7) | |
IQR: interquartile range, GCS: Glasgow Coma Scale, CSF: Cerebrospinal fluid, CNS: central nervous system, OP: Opening pressure, LP: Lumbar pressure, CN: Cranial nerve.
Table 2.
laboratory parameters evolution during antifungal treatment for CM at CRAM.
| Table 2: Adverse drug reactions of antifungal treatment for cryptococcal meningitis at CRAM, Mozambique 2020–2024, | (N=52) | ||||||
|
Parameter (Day 1 vs. Day 3) |
1st Day (Mean ± SD), [n] | 3rd Day (Mean ± SD), [n] | Mean Paired Diff | t-value | p-value | |
| Hgb (g/dL) | 11.2 ± 1.8 (n=52) | 10.6 ± 2.0 (n=38) | -0.6 | +4.73 | <0.001 | ↓ |
| K+ (mmol/L) | 4.27 ± 0.66 (n=49) | 3.86 ± 0.78 (n=40) | -0.26 | -2.81 | 0.008 | ↓ |
| Creat (mg/dL) | 0.83 ± 0.42 (n=52) | 1.13 ± 0.64 (n=40) | +0.39 | +3.46 | 0.001 | ↑ |
|
Parameter (Day 3 vs. Day 7) |
3rd Day (Mean ± SD), [n] | 7th Day (Mean ± SD), [n] | Mean Paired Diff | t-value | p-value | |
| Hgb (g/dL) | 10.6 ± 2.0 (n=38) | 10.6 ± 1.8 (n=38) | +0.05 | +0.35 | 0.738 | --- |
| K+ (mmol/L) | 3.86 ± 0.78 (n=40) | 3.97 ± 0.61 (n=38) | +0.11 | +0.23 | 0.175 | --- |
| Creat (mg/dL) | 1.13 ± 0.64 (n=40) | 0.99 ± 0.43 (n= 40) | -0.14 | -0.91 | 0.370 | --- |
| Abbreviations: SD = Standard Deviation; n = sample size; NS = Not Significant (p > 0.05), Diff = Differences | ||||||
SD = Standard Deviation; n = sample size; NS = Not Significant (p > 0.05); Diff = Differences.
Table 3.
Retention and Attrition Trends in MCC Follow-up.
| Table 3: Retention and Attrition Trends in MCC Follow-up |
Cochran-Armitage test for trend, p-value |
||||||
| Follow-up Period | Retained, N (%) | Censored = Died + Lost to Follow-up (LFU) + Transferred Out (TO) | Total, N (%) | ||||
| Censored, N (%) | Died, N (%) | LFU, N (%) | TO, N (%) | ||||
| 6 months | 68 (81.9) | 15 (18.1) | 9 (10.8) | 3 (3.6) | 3 (3.6) | 83 (100) | <0.001 |
| 12 months | 54 (74.0) | 19 (26.0) | 10 (13.7) | 5 (6.8) | 4 (5.5) | 73 (100) | |
| 24 months | 38 (70.4) | 16 (29.6) | 7 (13.0) | 4 (7.4) | 5 (9.3) | 54 (100) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



