
Submitted:
06 January 2026
Posted:
07 January 2026
You are already at the latest version
Abstract
Airway management in head/neck cancer patients with post-radiotherapy is challenging in the real world. In this case report, we described our practice with StyleTubation (using video intubating stylet technique) in combination of awake intubation strategy (local anesthetics topicalization, nerve blocks, deep sedation, and nasal high-flow oxygenation) in a patient with nasopharyngeal carcinoma, neck radiation fibrosis, and instrumented with halo-vest stabilization. The trans-oral endotracheal intubation was smooth (with first-pass success) and swift (28 s) without any complications.
Keywords:
StyleTubation
; video intubating stylet
; laryngoscopy
; videolaryngoscope
; Shikani technique
; endotracheal intubation
; airway management
; emergency
; critical care
; intensive care unit
; nasopharyngeal carcinoma
; radiation fibrosis
; Halo vest
; cervical collar
; stereotactic headframe
1. Introduction
Nasopharyngeal carcinoma (NPC) is one of the most common head and neck cancers and prevalent worldwide, especially in Asia.[1,2] The effective treatment modalities rely on radiation therapy (RT) including three-dimensional spatial cis-radiation and intensity-modulated radiation therapy are advocated. Surgical removal of cervical lymph nodes and current chemoradiotherapy (CCRT) is an important treatment option following CCRT. [3]
Among the wide range of side effects and complications associated with radiation therapy and CCRT for NPC, cervical radiation-induced fibrosis (RIF), osteoradionecrosis, trismus, vocal cords palsy and laryngeal edema impose significant airway compromise in these patient population.[4,5] Thorough airway assessment is one of the most important pre-procedural evaluation which includes history of surgery or radiation on the head/neck, circumference and mobility of the neck, and mouth-opening.[6,7] The difficult airway guidelines provide good reference for anesthesia clinician to provide optimal airway management including options of direct laryngoscopy (DL), videolaryngoscopy (VL) or fiber-optic intubation when endotracheal intubation is anticipated.[8,9]
Awake fiber-optic bronchoscopic (FOB) intubation has been the classic and gold standard for endotracheal intubation with difficult airway (DA) scenarios such as in patients with head and neck cancers, [10,11] although awake VL technique has also been advocated.[12,13,14] Studies have shown comparable success rate and safety profile between the two intubating modalities.[15,16,17,18] Failed intubation with both FOB and VL was reported in patients with head/neck cancers following radiation therapy.[19,20]
In this case report, we present StyleTubation technique (trans-oral endotracheal intubation using a video intubating stylet) to intube a patient wearing a halo-vest stabilization with rigid cervical spine from CCRT for a nasopharyngeal carcinoma.[21,22,23] This technique was performed after sedating the patient and supplemented with nerve blocks and local anesthetics topicalization, and giving nasal high-flow oxygenation.
2. Case Presentation
A 62-year-old man (height 159 cm, weight 40 kg, body mass index [BMI] 15.8 kg/m2) with past medical history significant for lung adenocarcinoma (right lower lobe, treated with RT 5 years ago) and NPC (treated with CCRT 10 years ago) was admitted for increasing neck pain and numbness radiating to right upper limb for two months.
Physical examination showed cervical and thoracic kyphosis deformity, positive Hoffmann sign, positive knee jerk, and impaired tandem gait. X-ray and MRI revealed C4/C5 endplate erosion with kyphosis and myelomalacia. CT showed destruction of C4 inferior endplate and C5 superior endplate erosion with kyphosis, grade I retrolisthesis at C4-5 level, narrowing of C3-4 and C5-6 disc spaces with mild diffuse bulging discs (Figure 1). He was admitted for surgical intervention (Crutchfield cervical traction; C2~T1 posterior fusion; C3~C6 laminoplasty; C6 laminectomy; C5 Trocar puncture biopsy).
Pre-anesthesia airway examinations revealed difficult intubation due to neck stiffness and instrumentation of halo vest stabilization. Mouth opening was 4 cm wide with missing incisors. The rest airway examination showed neck circumference of 33 cm, sternomental distance of 19 cm, thyromental distance of 5 cm, and Mallampati class IV (Figure 2). Awake trans-oral endotracheal intubation was planned using the StyleTubation technique, a well-established technique in our institution.[21,22,23]
Standard monitors recommended by the American Society of Anesthesiologists’ (ASA) standards including pulse oximetry (SpO2), capnography (ETCO2), electrocardiogram (ECG), non-invasive (NIBP) were applied. Radial artery catheter was placed for arterial blood pressure monitoring. We felt that mask ventilation would likely be jeopardized if neuromuscular blocking agents be given. Therefore, a spontaneous breathing was maintained with deep for subsequent StyleTubation. The oropharynx was topicalized with 10% lidocaine sprayed. Intra-oral glossopharyngeal nerves blocks and superior laryngeal nerves blocks (external approach) were performed with 2% lidocaine, respectively. Finally, trans-laryngeal block with 2% lidocaine was performed through cricothyroid membrane with a 22-gauge IV catheter.
After the topicalization and regional nerve blocks, the deep sedation was then started using glycopyrrolate 0.2 mg, midazolam 2.5 mg, and ketamine 25 mg, followed by the slowly titrated administration of propofol 80 mg. An airway assistant performed the jaw-thrust maneuver and opened the patient’s mouth. A nasal–pharyngeal airway with a suction tube was inserted into the patient’s oropharyngeal space to clear the secretions. It also served as a guide for subsequent intubation. Endotracheal intubation was performed using the StyleTubation technique (video-assisted intubating stylet). A 6.5 mm endotracheal tube was used for intubation. The whole process was smooth (with first-pass success) and swift (28 s) (Figure 3). The patient maintained spontaneous breathing during the entire endotracheal intubation process. Endotreacheal intubation was confirmed with capnography and chest auscultation before paralytics was administered. The ventilator strategy and parameters were set as follows: pressure control ventilation volume guaranteed (PCV-VG) with tidal volume: 450 mL; positive end-expiratory pressure (PEEP): 5 cm H2O; respiratory rate: 10-12 breaths/min; fresh gas flow rate: 2 L/min; fraction of inspired oxygen: 60%; maintenance partial pressure of end-tidal carbon dioxide: 33–45 mmHg. Anesthesia was maintained using sevoflurane 2.5–3% (MAC 0.6–0.8, BIS 40–50). Fentanyl and cisatracurium (creatinine was 1.58 mg/dL, with an estimated glomerular filtration rate (eGFR) of 47.63 mL/min/1.73m2) were supplemented based on the SPI and TOF values. No post-operative pulmonary complications, e.g., respiratory depression, pneumonia, hypoxia, upper airway obstruction, were reported.
3. Discussion
Nasopharyngeal carcinoma (NPC) is endemic and a national burden in global areas, including southern China and southeast Asia.[24] Undifferentiated carcinoma of the nasopharynx (highly associated with EBV) is the most common histological type in endemic regions which is highly sensitive to radiation therapy and chemotherapy.[25] Multimodal treatment consisted of chemotherapy, radiotherapy (IMRT), and surgery is the choice of recommend therapy for majority of the patients.[26,27] Neck fibrosis, trismus, and oropharyngeal distortion are common complications from the treatment. Airway management for these patients imposes a challenge for anesthesia providers when they come for initial surgery or subsequent procedures needing anesthesia services.
In this case report, the patient presented with severe radiation fibrosis over the neck without severe trismus. This allows us to apply the trans-oral approach of endotracheal intubation. The impact of HNRT in HNC patients showed a higher likelihood of difficult intubation (DI) due to shorter thyromental distance (TMD), limited range of motion over neck, higher degrees of Mallampatti scores.[28] The incidence of DA in NPC patient after RT was reported higher than that in general surgical patients (e.g., 28% versus 0.36–2.0%) and the rate of failure to intubate was also higher (e.g., 2.0% versus 0.003–0.15%).[29,30,31] Such required complex airway management is mainly due to both patient’s concurrent cervical mobility restriction and trismus. The incidences of poor laryngoscopic view, failed intubation, and intubation related complications are higher. Although the patient had severe radiation fibrosis, limited cervical spine mobility and mouth opening are reliable predictors for DA.[32]
Approximately 4 to 10% of patients with NPC present with metastases including cervical spine.[33] Wearing halo-vest is common in patients with bone metastasis to stabilize the cervical spine to avoid pathological fracture and pain control. The halo fixation device introduces a significant obstacle for airway management making intubation laryngoscope almost impossible.[34,35] Limited mouth-opening and reduced neck extension further impede the access to oropharynx and glottis.[36] Successful awake intubation via FOB and VL have been reported in patients mounted on halo fixation device.[35,36,37] StyleTubation in patients with stereotactic headframe,[38] manual in-line stabilization (MILS),[39] cervical collar,[38,40] and halo-vest stabilization has been recently demonstrated.[41] In this case, the patient with halo-vest was scheduled for cervical spine surgery and complicated by CCRT due to NPC. Radiation fibrosis severely restricted cervical mobility. Nasal obstruction of NPC disease precluded the option for naso-tracheal intubation with FOB. Trans-oral endotracheal intubation was the only viable option (Figure 4). The back up plans included VL or FOB with removal of the halo-vest as well as surgical airway. We successfully applied the StyleTubation intubated him in 28 s on the first attempt.
Elective or emergency tracheostomy is an option in patients with HNC and upper airway obstruction even FOB or laryngoscopy is planned.[42,43,44] Awake FOB tracheal intubation is considered the standard of care in patients with HNC anticipated for DA.[11,18,45] However, FOB technique may fail or maybe impossible in certain difficult scenarios.[46,47] VL has frequently been reported as an effective rescue. With a vast clinical experiences with StyleTubation in our institution, we practiced with caution in this patient with NPC, severe radiation fibrosis, and halo-vest stabilization for the scheduled cervical spine surgery. StyleTubation has become a routine endotracheal intubation modality including in patients with difficult airways.[21] This technique could be a potential option in the algorithm of difficult airway management.[9,14,48]
Combination of local anesthetics topicalization, nerve blocks, and optimal sedation have be recommended for awake or asleep (instead of anesthetized) endotracheal intubation in patients with anticipated or highly suspected DA.[49,50] To maximize the effectiveness and safety of awake endotracheal intubation, the high-flow pre-oxygenation, airway topicalization and nerve blocks, and experienced clinician are also important.[51]
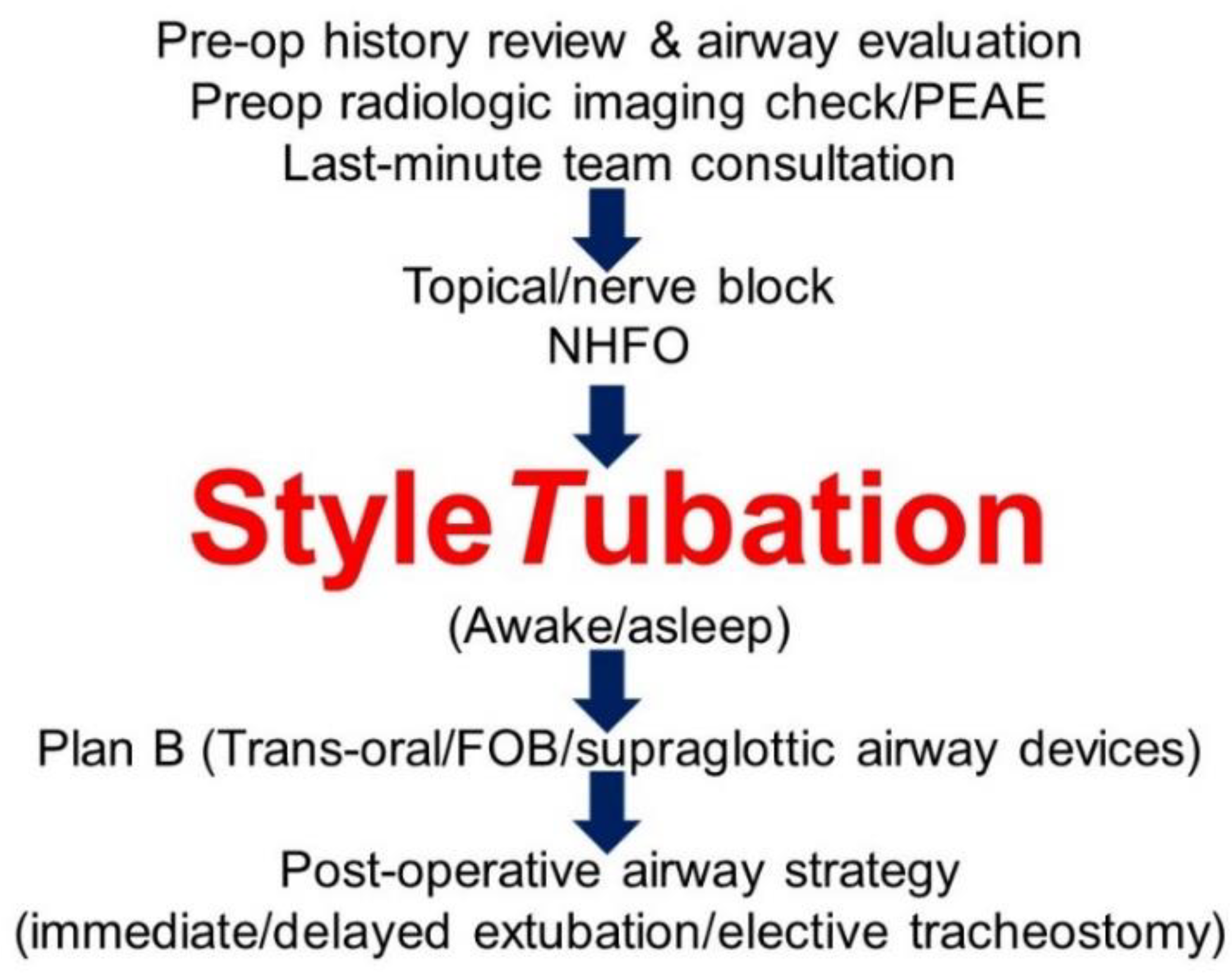
Several pre-operative airway-related risk factors (e.g., previous intubation difficulties, physical examination, rating of difficult airway indicators, and pharyngolaryngeallesions/transnasal videoendoscopy findings) were proposed as the DA algorithm bases for video-assisted intubation technique (VL or FOB) and anesthesia strategy (awake or asleep).[52] Awake FOB and VL are not fail-proof.[16] We share our own institutional airway algorithm, i.e., with StyleTubation, in a patient with NPC, severe radiation fibrosis, and halo vest fixation (Figure 5).
4. Conclusions
Airway management in NPC/HNC patients with post-RT neck radiation fibrosis and halo-vest fixation can be extremely challenging and requires a cautious and comprehensive preparation by the airway operator. StyleTubation could be an option for difficult airway.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
References
- Zhang, Y.; Gu, S.; Deng, H.; Shen, Z. Global epidemiological profile in nasopharyngeal carcinoma: a prediction study. BMJ. Open 2024, 14(12):e091087. [CrossRef]
- Chen, X.; Xia, W.; Xu, Z.H.; Suo, Y.X.; Xie, L. Trends in incidence and mortality of nasopharyngeal cancer in China (2004-2018): an age-period-cohort analysis. Front. Oncol. 2025, 15:1592217. [CrossRef]
- Bongiovanni, A.; Vagheggini, A.; Fausti, V.; Mercatali, L.; Calpona, S.; Di Menna, G.; Miserocchi, G.; Ibrahim, T. Induction chemotherapy plus concomitant chemoradiotherapy in nasopharyngeal carcinoma: An updated network meta-analysis. Crit. Rev. Oncol. Hematol. 2021, 160:103244. [CrossRef]
- Wang, C.; Wang, F.; Min, X.; Zhang, Q.; Shen, L.J.; Jiang, Y.; Yan, J. Toxicities of chemoradiotherapy and radiotherapy in nasopharyngeal carcinoma: an updated meta-analysis. J. Int. Med. Res. 2019, 47, 2832-2847. [CrossRef]
- Ramia, P.; Bodgi, L.; Mahmoud, D.; Mohammad, M.A.; Youssef, B.; Kopek, N.; Al-Shamsi, H.; Dagher, M.; Abu-Gheida, I. Radiation-induced fibrosis in patients with head and neck cancer: A review of pathogenesis and clinical outcomes. Clin. Med. Insights Oncol. 2022, 16:11795549211036898. [CrossRef]
- Kheterpal, S.; Healy, D.; Aziz, M.F.; Shanks, A.M.; Freundlich, R.E.; Linton, F.; Martin, L.D.; Linton, J.; Epps, J.L.; Fernandez-Bustamante, A.; Jameson, L.C.; Tremper, T.; Tremper, K.K.; Multicenter Perioperative Outcomes Group (MPOG) Perioperative Clinical Research Committee. Incidence, predictors, and outcome of difficult mask ventilation combined with difficult laryngoscopy: a report from the multicenter perioperative outcomes group. Anesthesiology 2013, 119, 1360-1369. [CrossRef]
- Higgs, A.; McGrath, B.A.; Goddard, C.; Rangasami, J.; Suntharalingam, G.; Gale, R.; Cook, T.M.; Difficult Airway Society; Intensive Care Society; Faculty of Intensive Care Medicine; Royal College of Anaesthetists. Guidelines for the management of tracheal intubation in critically ill adults. Br. J. Anaesth. 2018, 120, 323-352. [CrossRef]
- Heidegger, T. Management of the difficult airway. N Engl. J. Med. 2021, 384, 1836-1847. [CrossRef]
- Apfelbaum, J.L.; Hagberg, C.A.; Connis, R.T.; Abdelmalak, B.B.; Agarkar, M.; Dutton, R.P.; Fiadjoe, J.E.; Greif, R.; Klock, P.A.; Mercier, D.; Myatra, S.N.; O’Sullivan, E.P.; Rosenblatt, W.H.; Sorbello, M.; Tung, A. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology 2022, 136, 31-81. [CrossRef]
- Huitink, J.M.; Balm, A.J.; Keijzer, C.; Buitelaar, D.R. Awake fibrecapnic intubation in head and neck cancer patients with difficult airways: new findings and refinements to the technique. Anaesthesia 2007, 62, 214-219. [CrossRef]
- Desai, N.; Ratnayake, G.; Onwochei, D.N.; El-Boghdadly, K.; Ahmad, I. Airway devices for awake tracheal intubation in adults: a systematic review and network meta-analysis. Br. J. Anaesth. 2021, 127, 636-647. [CrossRef]
- Law, J.A.; Morris, I.R.; Brousseau, P.A.; de la Ronde, S.; Milne, A.D. The incidence, success rate, and complications of awake tracheal intubation in 1,554 patients over 12 years: an historical cohort study. Can. J. Anaesth. 2015, 62, 736-744. [CrossRef]
- Taboada, M.; Fernández, J.; Estany-Gestal, A.; Vidal, I.; Dos Santos, L.; Novoa, C.; Pérez, A.; Segurola, J.; Franco, E.; Regueira, J.; Mirón, P.; Sotojove, R.; Cortiñas, J.; Cariñena, A.; Peiteado, M.; Rodríguez, A.; Seoane-Pillado, T. First-attempt awake tracheal intubation success rate using a hyperangulated unchannelled videolaryngoscope vs. a channelled videolaryngoscope in patients with anticipated difficult airway: a randomised controlled trial. Anaesthesia 2024, 79, 1157-1164. [CrossRef]
- Ahmad, I.; El-Boghdadly, K.; Iliff, H.; Dua, G.; Higgs, A.; Huntington, M.; Mir, F.; Nouraei, S.A.R.; O’Sullivan, E.P.; Patel, A.; Rivett, K.; McNarry, A.F. Difficult Airway Society 2025 guidelines for management of unanticipated difficult tracheal intubation in adults. Br. J. Anaesth. 2025, Nov 7:S0007-0912(25)00693-2. Epub ahead of print. [CrossRef]
- Rosenstock, C.V.; Thøgersen, B.; Afshari, A.; Christensen, A.L.; Eriksen, C.; Gätke, M.R. Awake fiberoptic or awake video laryngoscopic tracheal intubation in patients with anticipated difficult airway management: a randomized clinical trial. Anesthesiology 2012, 116, 1210-1216. [CrossRef]
- Alhomary, M.; Ramadan, E.; Curran, E.; Walsh, S.R. Videolaryngoscopy vs. fibreoptic bronchoscopy for awake tracheal intubation: a systematic review and meta-analysis. Anaesthesia 2018, 73, 1151-1161. [CrossRef]
- Moore, A.; Schricker, T. Awake videolaryngoscopy versus fiberoptic bronchoscopy. Curr. Opin. Anaesthesiol. 2019, 32, 764-768. [CrossRef]
- Xu, W.; Zhu, C.; Wu, Q.; Zhao, B.; Zhou, M.; Liu, Y.; Hu, Y.; Xia, J.; Yuan, H.; Yu, Y.; Zou, Z. Comparison of SEEKflex/videolaryngoscopy and fibreoptic bronchoscope for awake tracheal intubation: a randomized clinical trial. BMC. Anesthesiol. 2025, 25(1):360. [CrossRef]
- Oishi, A.; Nomoto, Y.; Nemoto, C.; Inoue, S. Post-radiotherapy suggests a possible difficult airway even with an asymptomatic supraglottic change. JA. Clin. Rep. 2022, 8(1):102. [CrossRef]
- Ito, T.; Wakita, R,; Ichihashi, Y.; Kutsumizu, C.; Suzuki, C.; Shimada, N.; Maeda, S. Three cases of persistent laryngeal edema postradiation therapy. Anesth. Prog. 2024, 71, 24-28. [CrossRef]
- Luk, H.N.; Qu, J.Z.; Shikani, A. StyleTubation: The paradigmatic role of video-assisted intubating stylet technique for routine tracheal intubation. Asian J. Anesthesiol. 2023, 61, 102-106. [CrossRef]
- Luk, H.N.; Qu, J.Z. StyleTubation versus laryngoscopy: A new paradigm for routine tracheal intubation. Surgeries 2024, 5, 135-161. [CrossRef]
- Cheong, M.W.; Luk, H.N.; Qu, J.Z.; Shikani, A. Four approaches of StyleTubation for handling the orotracheal intubation: A technical tip. Asian J. Anesthesiol. 2024, 62, 100-103. [CrossRef]
- Jang, W.; Kim, S.; Son, Y.; Kim, S.; Lee, S.; Kim, H.J.; Jo, H.; Park, J.; Lee, K.; Lee, H.; Rahmati, M.; Woo, S.; Hwang, J.; Kang, J.; Smith, L.; Yon, D.K. Global, regional, and national burden of pharyngeal cancer and projections to 2050 in 185 Countries: A population-based systematic analysis of GLOBOCAN 2022. J. Korean Med. Sci. 2025, 40(30):e177. [CrossRef]
- Liu, Y.; Liu, X.; Sun, S.; Han, Y.; Feng, M.; Zhang, Y.; Wang, K.; Qu, Y.; Chen, X.; Zhang, J.; Luo, J.; Wu, R.; Li, Y.; Huang, X.; Guo, S.; Wang, J.; Yi, J. Evidence of being cured for nasopharyngeal carcinoma: results of a multicenter patient-based study in China. Lancet Reg. Health West. Pac. 2024, 49:101147. [CrossRef]
- Zhang, B.; Li, M.M.; Chen, W.H.; Zhao, J.F.; Chen, W.Q.; Dong, Y.H.; Gong, X.; Chen, Q.Y.; Zhang, L.; Mo, X.K.; Luo, X.N.; Tian, J.; Zhang, S.X. Association of chemoradiotherapy regimens and survival among patients with nasopharyngeal carcinoma: A systematic review and meta-analysis. JAMA. Netw. Open 2019, 2(10):e1913619. doi: 10.1001/jamanetworkopen.2019.13619. Erratum in: JAMA. Netw. Open 2019, 2(11):e1917197. [CrossRef]
- Chen, Y.P.; Ismaila, N.; Chua, M.L.K.; Colevas, A.D.; Haddad, R.; Huang, S.H.; Wee, J.T.S.; Whitley, A.C.; Yi, J.L.; Yom, S.S.; Chan, A.T.C.; Hu, C.S.; Lang, J.Y.; Le, Q.T.; Lee, A.W.M.; Lee, N.; Lin, J.C.; Ma, B.; Morgan, T.J.; Shah, J.; Sun, Y.; Ma, J. Chemotherapy in combination with radiotherapy for definitive-intent treatment of stage II-IVA nasopharyngeal carcinoma: CSCO and ASCO Guideline. J. Clin. Oncol. 2021, 39, 840-859. [CrossRef]
- Muthukumar, A.; Dong, W.; Zheng, G. Effects of head and neck radiotherapy on airway management outcomes. JCA. Advances 2024 ,1, 100039. [CrossRef]
- Sharma, I.; Dong, W.; Vu, C.N.; Zheng, G. The impact of head and neck radiation on airway management: a retrospective data review. Can. J. Anaesth. 2022, 69, 1562-1564. [CrossRef]
- Huang, A.E.; Camiré, D.; Hwang, P.H.; Nekhendzy, V. Difficult tracheal intubation and airway outcomes after radiation for nasopharyngeal carcinoma. Laryngoscope 2024, 134, 120-126. [CrossRef]
- Akazawa, M.; Shimizu, M.; Fujino, Y.; Kato H. Radiation-induced nasopharyngeal fibrosis resulting in a difficult airway: A case report. Cureus 2025, 17(2):e79130. [CrossRef]
- Artime, C.A.; Roy, S.; Hagberg, C.A. The difficult airway. Otolaryngol. Clin. North Am. 2019, 52, 1115-1125. [CrossRef]
- Lin, C.; Lin, S.; Zhu, L.; Lin, S.; Pan, J.; Xu, Y. Optimizing the treatment mode for de novo metastatic nasopharyngeal carcinoma with bone-only metastasis. BMC. Cancer 2022, 22(1):35. [CrossRef]
- Azurdia, A.R.; Walters, J.; Mellon, C.R.; Lettieri, S.C.; Kopelman, T.R.; Pieri, P.; Feiz-Erfan, I. Airway risk associated with patients in halo fixation. Surg. Neurol. Int. 2024, 15:104. [CrossRef]
- White, A.N.; Wong, D.T.; Goldstein, C.L.; Wong, J. Cervical spine overflexion in a halo orthosis contributes to complete upper airway obstruction during awake bronchoscopic intubation: a case report. Can. J. Anaesth. 2015, 62, 289-293. [CrossRef]
- El-Orbany, M. Airway management strategies in patients with halo vest fixation devices. Can. J. Anesth. 2015, 62, 932–933. [CrossRef]
- Huang, S.J.; Lee, C.L.; Wang, P.K.; Lin, P.C.; Lai, H.Y. The use of the GlideScope® for tracheal intubation in patients with halo vest. Acta Anaesthesiol. Taiwan 2011, 49, 88-90. [CrossRef]
- Shih, T.L.; Koay, K.P.; Hu, C.Y.; Luk, H.N.; Qu, J.Z.; Shikani, A. The use of the Shikani video-assisted intubating stylet technique in patients with restricted neck mobility. Healthcare (Basel) 2022, 10(9):1688. [CrossRef]
- Chan, W.H.; Cheng, C.P.; Chiu, Y.L.; Hsu, Y.C.; Hu, M.H.; Huang, G.S. Two head positions for orotracheal intubation with the trachway videolight intubating stylet with manual in-line stabilization: A randomized controlled trial. Medicine (Baltimore) 2020, 99(17):e19645. [CrossRef]
- Kim, J.K.; Kim, J.A.; Kim, C.S.; Ahn, H.J.; Yang, M.K.; Choi, S.J. Comparison of tracheal intubation with the Airway Scope or Clarus Video System in patients with cervical collars. Anaesthesia 2011, 66, 694-698. [CrossRef]
- Cheng, W.C.; Lan, C.H.; Lai, H.Y. The Clarus Video System (Trachway) intubating stylet for awake intubation. Anaesthesia 2011, 66, 1178-1180. [CrossRef]
- Wandell, G.M.; Merati, A.L.; Meyer, T.K. Update on tracheostomy and upper airway considerations in the head and neck cancer patient. Surg. Clin. North Am. 2022, 102, 267-283. [CrossRef]
- Kim, C.Y.; Cho, S.; Ryoo, S.H. Anesthetic management for emergency tracheostomy in patients with head and neck cancer: a case series. J. Dent. Anesth. Pain Med. 2022, 22, 457-464. [CrossRef]
- Cleere, E.F.; Read, C.; Prunty, S.; Duggan, E.; O’Rourke, J.; Moore, M.; Vasquez, P.; Young, O.; Subramaniam, T.; Skinner, L.; Moran, T.; O’Duffy, F.; Hennessy, A.; Dias, A.; Sheahan, P.; Fitzgerald, C.W.R.; Kinsella, J.; Lennon, P.; Timon, C.V.I.; Woods, R.S.R.; Shine, N.; Curley, G.F.; O’Neill, J.P. Airway decision making in major head and neck surgery: Irish multicenter, multidisciplinary recommendations. Head Neck 2024, 46, 2363-2374. [CrossRef]
- Ahmad, I.; El-Boghdadly, K.; Bhagrath, R.; Hodzovic, I.; McNarry, A.F.; Mir, F.; O’Sullivan, E.P.; Patel, A.; Stacey, M.; Vaughan, D. Difficult Airway Society guidelines for awake tracheal intubation (ATI) in adults. Anaesthesia 2020, 75, 509-528. [CrossRef]
- Huitink, J.M.; Zijp, L. Laryngeal radiation fibrosis: a case of failed awake flexible fibreoptic intubation. Case Rep. Anesthesiol. 2011, 2011:878910. [CrossRef]
- Karlsen, K.A.H.; Gisvold, S.E.; Nordseth, T.; Fasting, S. Incidence, causes, and management of failed awake fibreoptic intubation-A retrospective study of 833 procedures. Acta Anaesthesiol. Scand. 2023, 67, 1341-1347. [CrossRef]
- Frerk, C.; Mitchell, V.S.; McNarry, A.F.; Mendonca, C.; Bhagrath, R.; Patel, A.; O’Sullivan, E.P.; Woodall, N.M.; Ahmad, I.; Difficult Airway Society intubation guidelines working group. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br. J. Anaesth. 2015, 115, 827-848. [CrossRef]
- Kolb, B.; Lewis, T.; Large, J.; Wilson, M.; Ode, K. Remimazolam sedation for awake tracheal intubation. Anaesth. Rep. 2024, 12(1):e12298. [CrossRef]
- Bruijstens, L.; Koch, R.; Van Der Wal, R.; Van Eijk, L.; Bruhn, J. Remimazolam for sedation and trachospray for topicalization during flexible nasal intubation in a spontaneously breathing patient. Cureus 2025, 17(1):e77406. [CrossRef]
- El-Boghdadly, K.; Desai, N.; Jones, J.B.; Elghazali, S.; Ahmad, I.; Sneyd, J.R. Sedation for awake tracheal intubation: A systematic review and network meta-analysis. Anaesthesia 2025, 80, 74-84. [CrossRef]
- Popal, Z.; Sieg, H.H.; Müller-Wiegand, L.; Breitfeld, P.; Dankert, A.; Sasu, P.B.; Wünsch, V.A.; Krause, L.; Zöllner, C.; Petzoldt, M. Decision-making tool for planning camera-assisted and awake intubation in head and neck surgery. JAMA. Otolaryngol. Head Neck Surg. 2025, 151, 585-594. [CrossRef]
Figure 1.
Pre- and post-operative imaging studies. (A) Chest X ray: pleural thickening in right lung apex & base. (B)~(D) Dynamic cervical spine studies: destruction and retrolisthesis at C4/5 and C5/6. (E)~(G) CT scans: no signs of laryngeal or hypopharyngeal obstruction. (H) and (I): Posterior instrumentation from C2 to T1.
Figure 1.
Pre- and post-operative imaging studies. (A) Chest X ray: pleural thickening in right lung apex & base. (B)~(D) Dynamic cervical spine studies: destruction and retrolisthesis at C4/5 and C5/6. (E)~(G) CT scans: no signs of laryngeal or hypopharyngeal obstruction. (H) and (I): Posterior instrumentation from C2 to T1.
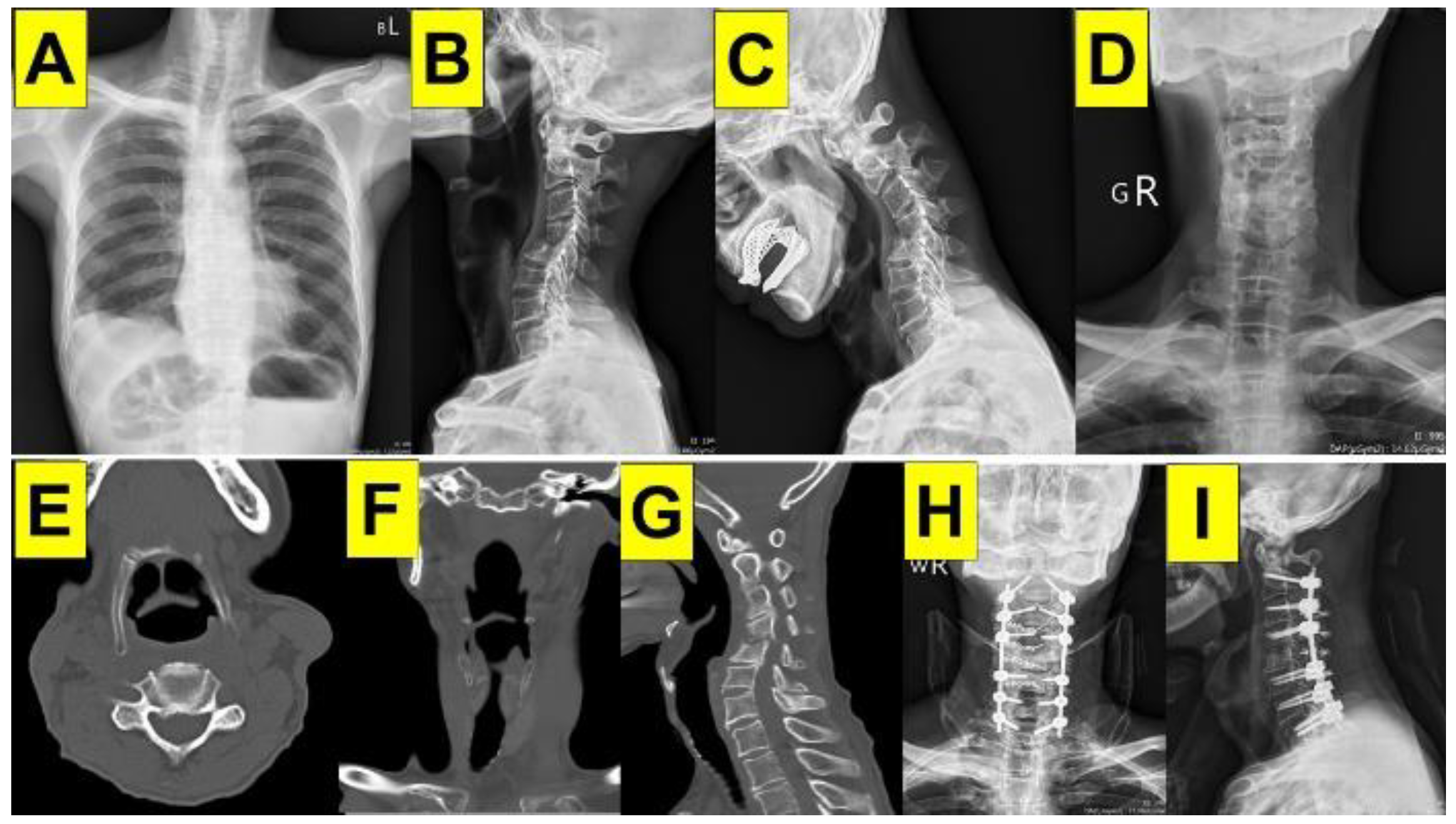
Figure 2.
Pictures before and after endotracheal intubation. (A) Halo vest instrumentation. (B)~(D) Mouth opening and teeth conditions. (E) and (F) Cervical spines immobility and severe stiff neck.
Figure 2.
Pictures before and after endotracheal intubation. (A) Halo vest instrumentation. (B)~(D) Mouth opening and teeth conditions. (E) and (F) Cervical spines immobility and severe stiff neck.

Figure 3.
Serial images recorded from StyleTubation. (A) and (B): A nasal airway-suction tube unit to clear and oral cavity and as a conduit. (C)~(E): The video stylet was approaching into patient’s right hypopharyngeal space. The white star label indicates the collapsed epiglottis. (F)~(H): Changing the lateral approach from right to left side of patient’s collapsed epiglottis. (I): Left arytenoid. (J) and (K): Glottic opening and visibility of the trachea. (L) Advancing endotracheal tube into patient’s trachea.
Figure 3.
Serial images recorded from StyleTubation. (A) and (B): A nasal airway-suction tube unit to clear and oral cavity and as a conduit. (C)~(E): The video stylet was approaching into patient’s right hypopharyngeal space. The white star label indicates the collapsed epiglottis. (F)~(H): Changing the lateral approach from right to left side of patient’s collapsed epiglottis. (I): Left arytenoid. (J) and (K): Glottic opening and visibility of the trachea. (L) Advancing endotracheal tube into patient’s trachea.
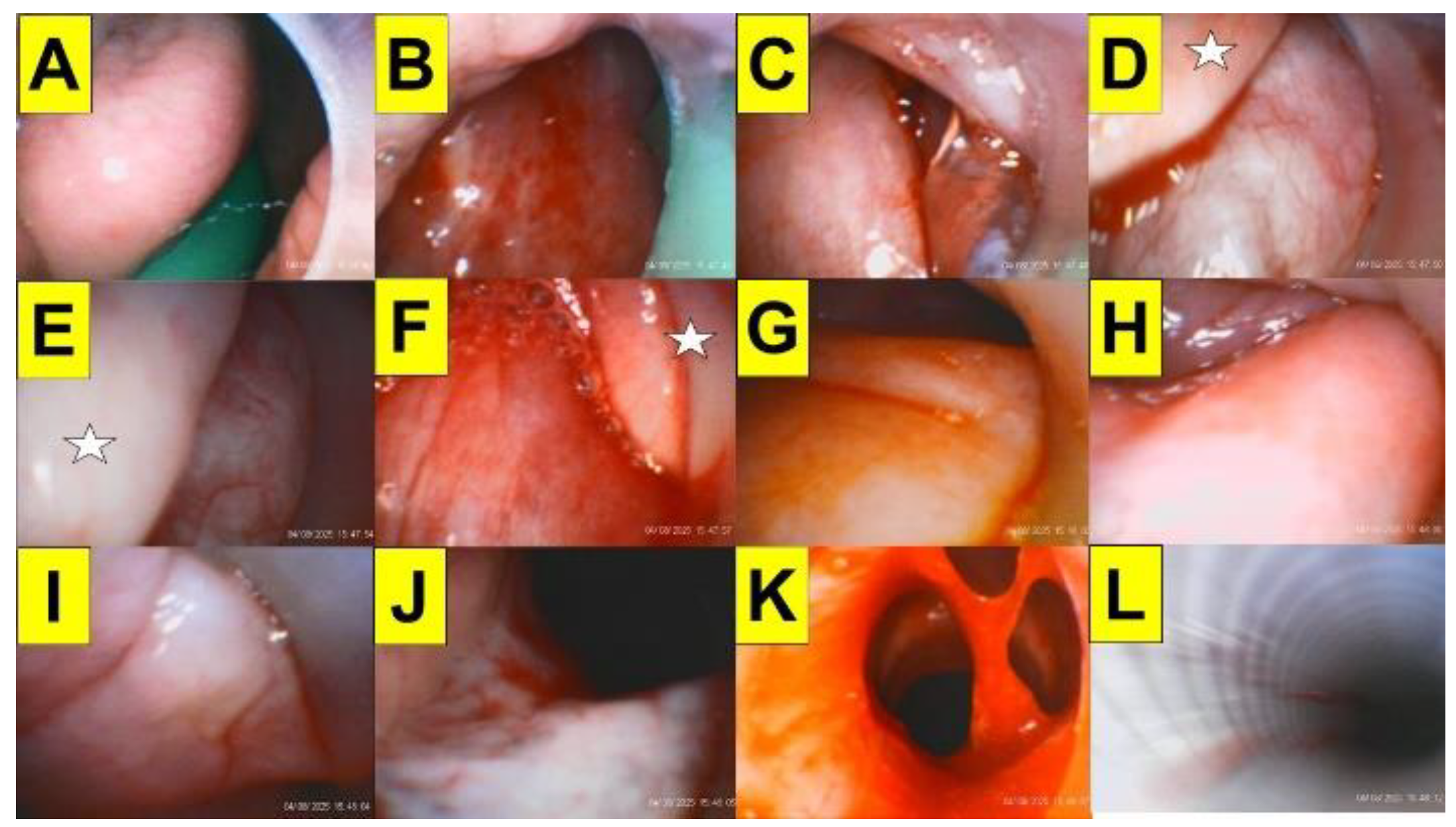
Figure 4.
StyleTubation. (A) Examples of various commercial video stylets products. (B) Two-person operation model of StyleTubation. (C) Parts of video stylets-endotracheal tube unit. Clinical application of StyleTubation in patients instrumented with (D) cervical collar; (E) halo vest stabilizer; (F) stereotactic head frame.
Figure 4.
StyleTubation. (A) Examples of various commercial video stylets products. (B) Two-person operation model of StyleTubation. (C) Parts of video stylets-endotracheal tube unit. Clinical application of StyleTubation in patients instrumented with (D) cervical collar; (E) halo vest stabilizer; (F) stereotactic head frame.
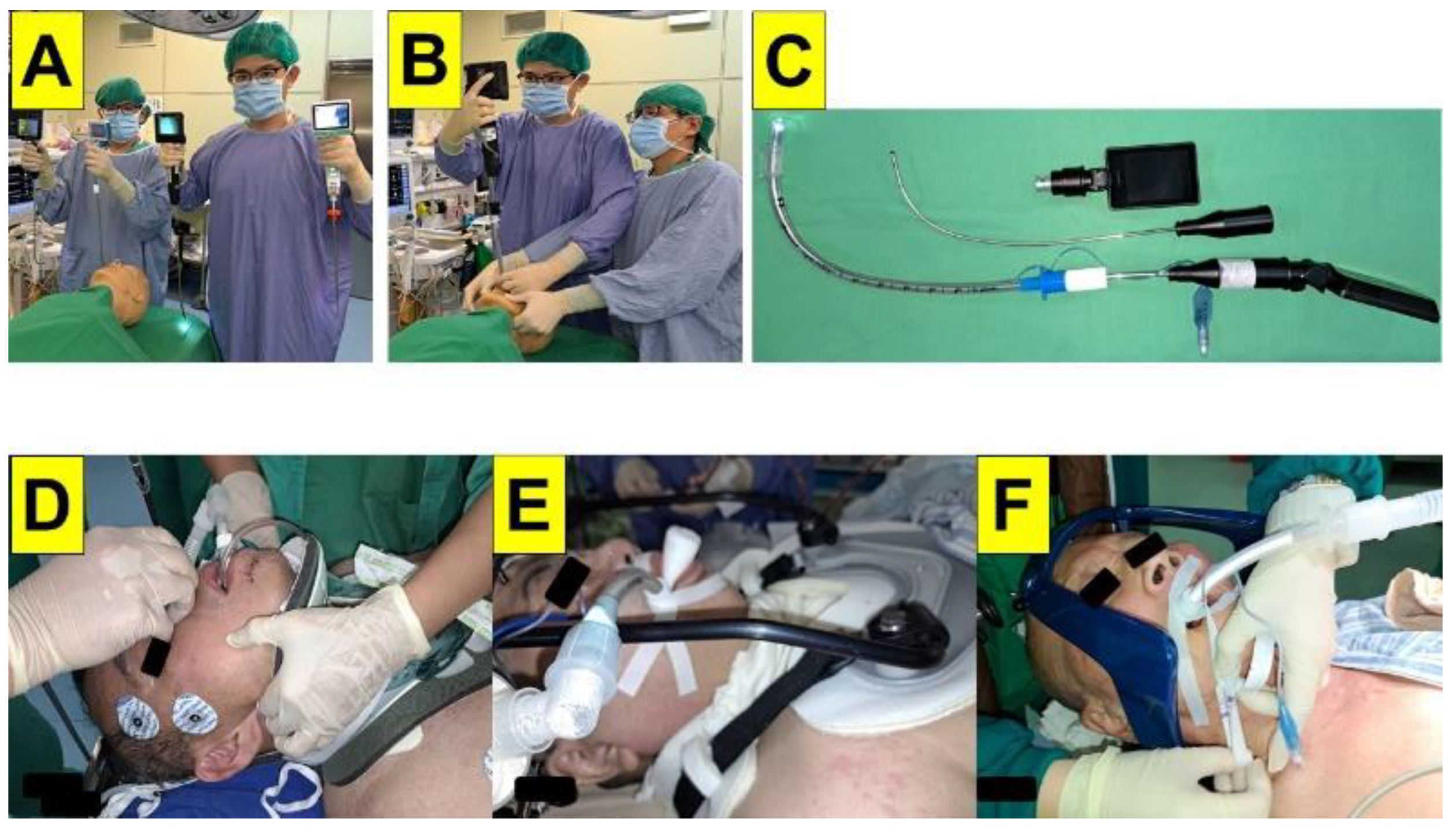
Figure 5.
Proposed standard operation procedure for StyleTubation in patients with predicted DA. PEAE: preoperative endoscopic airway examination. NHFO: nasal high flow oxygenation.
Figure 5.
Proposed standard operation procedure for StyleTubation in patients with predicted DA. PEAE: preoperative endoscopic airway examination. NHFO: nasal high flow oxygenation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



