
Submitted:
06 January 2026
Posted:
07 January 2026
You are already at the latest version
Abstract
Mesonephric-like adenocarcinoma is a rare uterine neoplasm recognized in the fifth edition of the World Health Organization Classification of Female Genital Tumors and poses diagnostic challenges due to its morphologic and immunophenotypic overlap with other endometrial carcinomas. We retrospectively reviewed three cases diagnosed at our institution, evaluating clinical presentation, histologic features, immunohistochemical profile, and available molecular findings, and performed a literature review of approximately 200 reported cases with emphasis on comorbidities and potential predisposing factors. All three patients presented with abnormal uterine bleeding and had hypothyroidism, and one patient had Down syndrome, representing the first reported case in this population. Tumors consistently expressed thyroid transcription factor 1, showed variable GATA3 expression, and demonstrated limited or absent hormone receptor expression. Literature review revealed frequent association with Müllerian-type lesions and recurrent KRAS mutations, while thyroid disease was not identified as a consistent comorbidity. These findings support a Müllerian origin for mesonephric-like adenocarcinoma and suggest that hypothyroidism is unlikely to represent a defining association. The occurrence in a patient with Down syndrome raises the possibility of an underlying genetic susceptibility that warrants further investigation.
Keywords:
mesonephric-like adenocarcinoma (MLA)
; uterine carcinoma
; endometrial neoplasms
; Müllerian differentiation
; hypothyroidism
; Down syndrome
; immunohistochemistry
; KRAS mutation
; rare gynecologic tumors
1. Introduction
Mesonephric-like adenocarcinoma (MLA) is an emerging subtype of gynecologic carcinoma that primarily involves the uterine corpus and, less frequently, the ovary. First characterized as a distinct entity by McFarland, Quick, and McCluggage in 2016 [1]and formally incorporated into the 2020 WHO Classification of Female Genital Tumors, MLA poses diagnostic challenges due to its rarity, morphologic heterogeneity, and overlap with other uterine carcinomas.
Histologically, MLA recapitulates features of mesonephric adenocarcinoma, including tubular, glandular, and solid growth patterns, often with eosinophilic luminal secretions. Immunohistochemically, MLA frequently expresses PAX8 and mesonephric-associated markers such as GATA3 and thyroid transcription factor 1 (TTF-1), while typically lacking strong, diffuse estrogen receptor (ER) and progesterone receptor (PR) expression. In contrast to true mesonephric adenocarcinomas of the cervix, MLA often arises in the endometrium or ovary and usually lacks demonstrable mesonephric remnants, supporting a Müllerian origin with mesonephric-like differentiation.
Molecular studies have shown that MLA is commonly driven by recurrent KRAS mutations, with additional alterations in genes such as PIK3CA, ARID1A, and CTNNB1 in a subset of cases. In contrast, mutations in PTEN, TP53, and SMARCA4 are generally less frequent, further distinguishing MLA from conventional endometrioid and serous endometrial carcinomas. These findings suggest that MLA represents a distinct molecular and morphologic pathway within the spectrum of Müllerian neoplasia.
Down syndrome is the most common chromosomal cause of intellectual disability worldwide and is associated with characteristic phenotypic features, immune dysregulation, and an altered cancer profile.[1] Individuals with Down syndrome exhibit an increased risk of hematologic malignancies, but a decreased risk of many solid tumors, including breast, lung, and prostate cancers.[2,3,4] However, the relationship between Down syndrome and rare gynecologic malignancies like MLA has not been previously described.
In this case series, we report three patients with MLA of the uterine corpus, all with documented hypothyroidism. One patient is, to our knowledge, the first reported individual with Down syndrome diagnosed with MLA. We correlate the clinical, histopathologic, and immunohistochemical findings of these cases with a literature review of approximately 200 reported MLA cases and discuss potential links between MLA, thyroid dysfunction, and genetic predisposition.
2. Materials and Methods
2.1. Study Design and Case Selection
This retrospective case series was conducted at a single academic medical center. Cases were identified through a review of the institutional pathology database over a defined study period. Inclusion criteria consisted of endometrial carcinomas with histopathologic and immunophenotypic features consistent with mesonephric-like adenocarcinoma (MLA). Cases with insufficient diagnostic material or incomplete immunohistochemical evaluation were excluded.
2.2. Clinical and Pathologic Data Collection
Clinical data extracted from the medical record included patient age, presenting symptoms, relevant medical history, imaging findings, treatment modality, and available follow-up information. Pathologic variables collected included tumor size, depth of myometrial invasion, histologic architecture, cytologic features, lymphovascular invasion, and pathologic stage when available.
2.3. Histopathologic Evaluation
Hematoxylin and eosin–stained slides from endometrial biopsies, curettage specimens, and hysterectomy specimens were reviewed by board-certified pathologists. Histologic features assessed included glandular architecture, nuclear atypia, mitotic activity, presence of solid growth, and cytoplasmic characteristics. Tumors were classified according to the current World Health Organization (WHO) classification of female genital tumors.
2.4. Immunohistochemistry
Immunohistochemical studies were performed on formalin-fixed, paraffin-embedded tissue sections using standard laboratory protocols. Antibodies evaluated across cases included GATA3, TTF-1, ER, PR, p16, p53, Napsin A, glypican-3, AFP, CDX2, CD10, and calretinin, as clinically indicated. Immunoreactivity was assessed qualitatively and recorded as diffuse, patchy, focal, or negative.
2.5. Staging and Ancillary Studies
Pathologic staging was performed according to the American Joint Committee on Cancer (AJCC) 8th edition staging system and corresponding FIGO criteria when surgical specimens were available. Molecular or germline testing results, when performed, were recorded from clinical reports.
2.6. Ethical Approval
This study was conducted in accordance with institutional guidelines for retrospective studies. Institutional review board approval was obtained, with waiver of informed consent due to the retrospective nature of the study.
2.7. Use of Generative Artificial Intelligence
Generative artificial intelligence tools were used for language refinement and formatting assistance only. No GenAI tools were used for data generation, analysis, or interpretation.
3. Results
3.1. Cohort Characteristics
Three patients with endometrial mesonephric-like adenocarcinoma were identified. Patient ages ranged from 28 to 74 years. All patients presented with abnormal uterine bleeding, including heavy menstrual bleeding in premenopausal patients and postmenopausal bleeding in the postmenopausal patient. Two patients had a history of hypothyroidism. One patient had a prior history of breast carcinoma.
3.2. Clinical and Imaging Findings
Pelvic imaging demonstrated endometrial abnormalities in two cases, including a hypervascular uterine mass and a focal endometrial lesion. One patient had no discrete mass identified on ultrasound despite significant clinical symptoms. Severe anemia was present in two patients at presentation, requiring transfusion in one case.
3.3. Histopathologic Findings
Endometrial sampling demonstrated crowded, back-to-back glands with high nuclear-to-cytoplasmic ratios, hyperchromatic nuclei, and variable mitotic activity across all cases. Focal solid growth and clear cell–like cytoplasmic changes were observed in select cases. Initial diagnostic interpretations included high-grade endometrial adenocarcinoma or hyperplasia in some cases, prompting further immunophenotypic evaluation.
3.4. Immunophenotypic Profile
All tumors demonstrated an immunoprofile supportive of mesonephric-like adenocarcinoma. GATA3 and/or TTF-1 expression was identified in all cases, with staining patterns ranging from patchy to focal. Estrogen and progesterone receptor expression was absent or limited, with one case showing patchy ER and PR positivity. Napsin A expression was variable. p53 demonstrated wild-type staining patterns in evaluated cases. The combined morphologic and immunophenotypic findings supported the final diagnosis of MLA in all patients (Figure 1 and Figure 2).
3.5. Surgical Pathology, Treatment, and Outcomes
Two patients underwent total hysterectomy with bilateral salpingo-oophorectomy. One tumor demonstrated deep myometrial invasion and was staged as pT1b pN0 pMNa, corresponding to FIGO stage II. Peritoneal washings were negative for malignant cells. One patient received neoadjuvant carboplatin and paclitaxel. One patient pursued conservative management with levonorgestrel-releasing intrauterine device placement due to fertility preservation considerations. Available staging, treatment, and outcome data are summarized in Table 1.
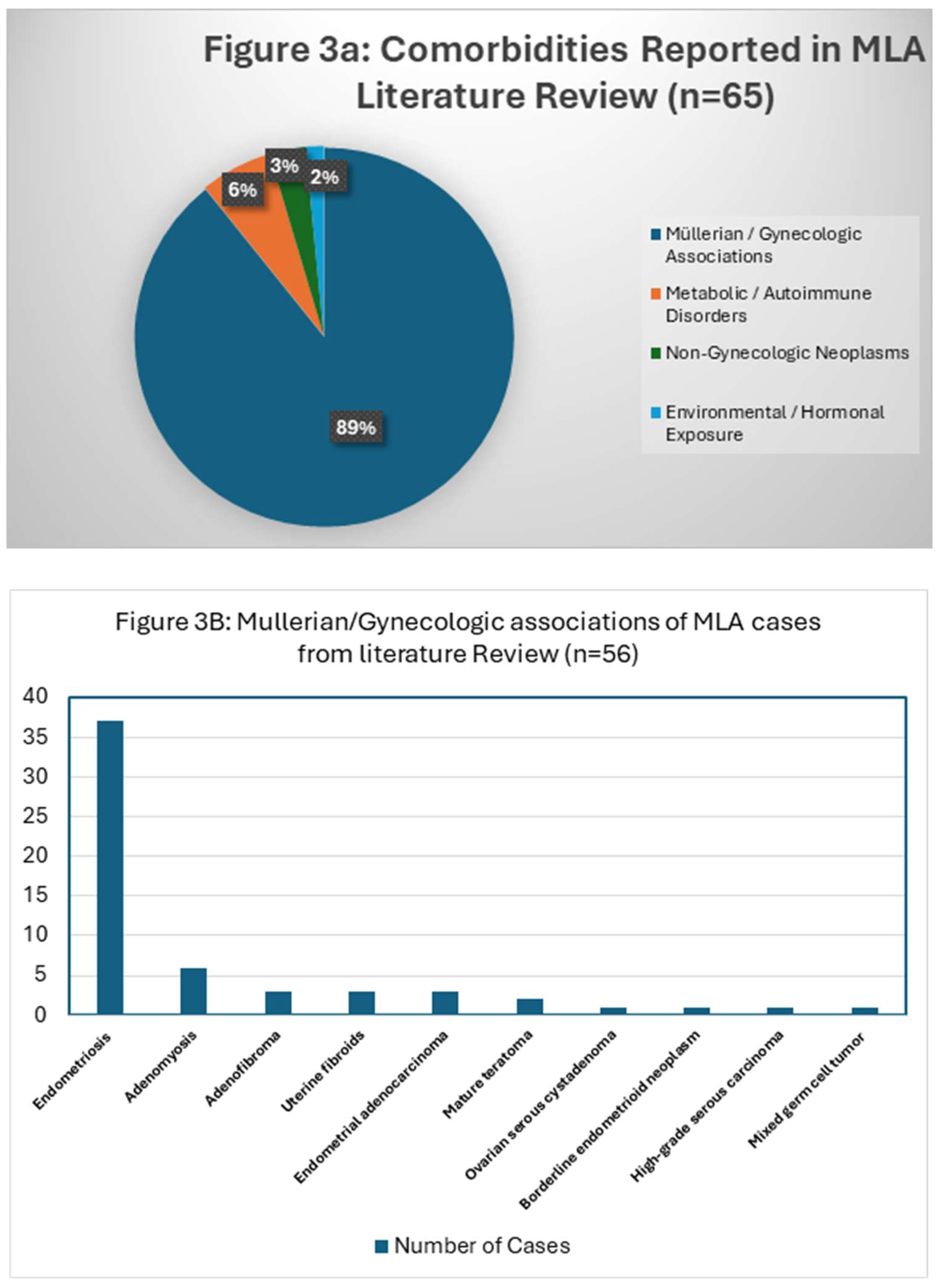
A PubMed search of mesonephric-like adenocarcinoma revealed 256 papers of which 51 cases of mesonephric-like adenocarcinoma was included in our study comprising approximately 200 MLA cases. Comorbidity reporting was inconsistent: only 32.5% (65/200 cases) had comorbidity reports. No comorbidity data available in 135/200 cases (67.5%). Table 2 shows a summary of the reported cases, immunohistochemical profile, FIGO stage at diagnosis, and the associated molecular findings.
The literature strongly supports a Müllerian origin: among the 65 cases with available data, 86% were associated with Müllerian lesions, especially endometriosis and adenomyosis as seen in Table 3.
4. Discussion
Mesonephric-like adenocarcinoma occupies a unique niche within gynecologic pathology, combining morphologic and immunophenotypic features of mesonephric adenocarcinoma with a likely Müllerian origin. While no true mesonephric duct remnants are present, these tumors closely resemble mesonephric adenocarcinomas by their morphology and immunohistochemistry staining patterns, and are characterized by joint endometrial and mesonephric differentiation.[55] Similar to mesonephric adenocarcinomas, MLA tumors generally present as hormone receptor negative (though may be focally positive for estrogen, as observed in our third case presentation), but are positive for PAX-8, TTF-1, and GATA-3.[56,57] Unlike mesonephric adenocarcinomas, the primary site of this malignancy appears to be restricted to the uterus and ovaries and frequently coexists with other Müllerian lesions, including endometrioid adenocarcinoma, endometrioid adenofibroma, and endometriosis. These associations, together with its PAX8 positivity and characteristic KRAS-driven molecular profile, support the concept of a Müllerian-derived carcinoma undergoing mesonephric-like differentiation.
The origin of MLA is still controversial, primarily because of its rarity and shortage of literature, but some of the recent evidence suggests that it may originate from the Müllerian epithelium. For example, these tumors often coexist with other Mullerian neoplasms. Molecular data indicates an association with KRAS and PIK3CA mutations; however, mutations in PTEN, p53, and SMARCA4 have not been commonly observed.[58] The embryologic context provides a useful framework. The mesonephric (Wolffian) duct gives rise to the epididymis, vas deferens, and seminal vesicles in males, while regressing in females, leaving behind occasional mesonephric remnants in the cervix and uterine ligaments. These remnants can give rise to mesonephric hyperplasia and mesonephric adenocarcinoma. In contrast, the paramesonephric (Müllerian) ducts form the fallopian tubes, uterus, cervix, and upper vagina.[59]MLA appears to arise from Müllerian-derived epithelium that acquires a mesonephric-like immunophenotype (GATA3 and TTF-1 positivity, ER/PR negativity), resulting in a lesion that mimics mesonephric carcinoma but lacks true mesonephric rests.
Our three cases are concordant with previously described MLA in several respects: all showed TTF-1 positivity, two showed GATA3 expression, and all had limited or absent diffuse ER/PR expression. Morphologically, they demonstrated crowded glands with high-grade cytologic atypia and, in one case, clear cell-like changes, highlighting the potential for diagnostic confusion with endometrioid or clear cell carcinoma. Two of the three tumors were initially misclassified, emphasizing the need for heightened awareness and appropriate immunohistochemical workup, particularly in hormone receptor–negative endometrial carcinomas with unusual morphology.
A salient finding in our series is the consistent presence of hypothyroidism in all three patients. However, our systematic review of ~200 published MLA cases did not identify thyroid dysfunction as a recurrent or well-described comorbidity. This discrepancy likely reflects incomplete reporting rather than absence of disease, as 67.5% of published cases lacked any comorbidity information. Thus, although endocrine abnormalities were observed in our cohort, their significance remains speculative. In contrast, the literature strongly supports a Müllerian origin: among the 65 cases with available data, 86% were associated with Müllerian lesions, especially endometriosis and adenomyosis as seen in Table 3.
This trend reinforces the proposal that MLA arises from Müllerian epithelium undergoing mesonephric-like differentiation. While causality cannot be inferred from observational data, thyroid hormone pathways intersect with cell proliferation, metabolism, and immune regulation, any of which could hypothetically influence tumor biology in susceptible tissues. Our findings reinforce the need for systematic evaluation of thyroid status in larger MLA cohorts and for mechanistic studies exploring thyroid–tumor crosstalk.
The most novel aspect of our series is the occurrence of MLA in a young woman with Down syndrome. Down syndrome is characterized by trisomy 21, involving the Down Syndrome Critical Region with genes such as ETS2, RCAN1, and DYRK1A that modulate immune function and carcinogenesis. Epidemiologic studies consistently show an increased risk of hematologic malignancies in individuals with Down syndrome but a reduced incidence of many solid tumors, suggesting complex, context-dependent roles for chromosome 21–encoded genes in tumorigenesis.
Down syndrome is the most prevalent genetic culprit of intellectual disability globally. The addition of part or an entire twenty-first chromosome is associated with numerous consequences, including loss of muscle tone, craniofacial abnormalities, delays in speech and language development, and learning impairment. Triploidy of chromosome 21 is also associated with immunodeficiency: children with Down syndrome are more susceptible to infections, especially respiratory infections.[60] An area on chromosome 21 of particular interest is commonly called the Down Syndrome Critical Region (DSCR), and includes 33 genes believed to be responsible for many of the abnormalities seen in patients with Down syndrome. Particularly, genes on the DSCR including protein-encoding genes for the erythroblast transformation-specific 2 protein (ETS2), regulator of calcineurin 1/calcipressin-1 (RCAN1), and dual-specificity tyrosine phosphorylation-regulated kinase 1A (DYRK1A), are all being studied for their suspected tumor-suppressing roles.[61,62] There are numerous studies describing the relationship between Down syndrome and malignancy. These studies describe a positive correlation between Down syndrome and hematologic malignancies and negative correlation between patients and solid tumor malignancies, specifically breast, lung, and prostate.[61,63,64]However, there is also literature describing young patients with Down syndrome acquiring rare solid tumor malignancies, which demands further investigation.[65] To date, MLA has not been described in patients with Down syndrome. The coexistence of MLA, Down syndrome, and hypothyroidism in our first case may represent coincidence; however, it also raises the hypothesis that immune dysregulation, endocrine disturbance, and trisomy 21–related gene dosage effects could converge to alter the risk profile for rare Mullerian neoplasms. Larger datasets and molecular profiling will be required to test this hypothesis.
5. Conclusions
Mesonephric-like adenocarcinoma is an uncommon and diagnostically challenging uterine malignancy that often mimics endometrioid carcinoma on initial evaluation. In this case series, all three patients presented with abnormal uterine bleeding and shared overlapping histopathologic and immunohistochemical features characteristic of MLA, including TTF-1 positivity and relative absence of hormone receptor expression. The consistent presence of hypothyroidism across all cases reinforces previously suggested endocrine associations and supports the need for further investigation into thyroid dysfunction as a potential contributing factor in MLA pathogenesis.
Notably, we report the first known case of MLA occurring in a patient with Down syndrome. Although a causal relationship cannot be established from a single case, the finding raises the possibility of an underlying genetic susceptibility, potentially involving chromosome 21–associated pathways, and highlights an area for future research. As recognition of MLA continues to expand, heightened awareness of its morphologic spectrum, immunophenotype, and possible molecular underpinnings will be essential for improving diagnostic accuracy and optimizing patient outcomes.
Our case series and literature review of approximately 200 reported MLA cases confirms several key themes:
- MLA is uncommon but likely underrecognized.
- It often presents at an early stage but carries a higher risk of recurrence and metastasis than low-grade endometrioid carcinoma.
- KRAS mutations are highly prevalent; additional alterations in PIK3CA, ARID1A, and CTNNB1 occur in a subset. These observations suggest important prognostic and therapeutic implications, including potential eligibility for targeted therapies directed at KRAS or PI3K/AKT/mTOR pathway alterations.
- The immunophenotypic pattern of PAX8+/TTF-1+/GATA3+/ER– (or ER-focal) is highly characteristic but not entirely specific.
- Endocrine comorbidities, including hypothyroidism, appear in case reports and small series, though systematic data remains limited. Recognition of these associations can improve diagnostic accuracy and promote further research into molecular and endocrine pathways underlying MLA pathogenesis.
Author Contributions
Conceptualization, A.I.U. and E.E.; methodology, A.I.U, T.S, E.E.; validation, A.I.U. and E.E.; investigation, T.S.; resources, T.S., A.I.U.; data curation, A.I.U.; formal analysis, A.I.U.; writing—original draft preparation, A.I.U, T.S.; writing—review and editing, A.I.U., T.S., and E.E.; visualization, E.E.; supervision, E.E.; project administration, E.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to not meeting the definition of “human subject research”, as defined by the regulations at 45 CFR 46.102.
Informed Consent Statement
Patient consent was waived due to a retrospective review.
Data Availability Statement
Data available on request from the authors.
Acknowledgments
The authors would like to acknowledge the administrative and information technology teams for their support in maintaining telecytology infrastructure and digital pathology systems. During the preparation of this manuscript, the authors used ChatGPT (OpenAI, GPT-5.2) for assistance with language refinement, organization of text, and formatting. The authors reviewed and edited all generated content and take full responsibility for the accuracy, integrity, and originality of this work.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| Abbreviation | Definition |
| MLA | Mesonephric-like adenocarcinoma |
| ER | Estrogen receptor |
| PR | Progesterone receptor |
| AJCC | American Joint Committee on Cancer |
| FIGO | International Federation of Gynecology and Obstetrics |
| PCOS | Polycystic ovary syndrome |
| IHC | Immunohistochemistry |
Appendix A
Figure A1.
Comorbidities and Müllerian Associations in Reported MLA Cases. 3A: Pie chart summarizes comorbidities among 65 of 200 reported mesonephric-like adenocarcinoma (MLA) cases with available data. 3B: Bar chart highlights specific Müllerian lesions, with endometriosis (37 cases) and adenomyosis (6 cases) as the most common associations with MLA.
Figure A1.
Comorbidities and Müllerian Associations in Reported MLA Cases. 3A: Pie chart summarizes comorbidities among 65 of 200 reported mesonephric-like adenocarcinoma (MLA) cases with available data. 3B: Bar chart highlights specific Müllerian lesions, with endometriosis (37 cases) and adenomyosis (6 cases) as the most common associations with MLA.
References
- Y. Dieudonné et al., ‘Immune Defect in Adults With Down Syndrome: Insights Into a Complex Issue’, Front Immunol, vol. 11, May 2020. [CrossRef]
- H. Hasle, J. M. Friedman, J. H. Olsen, and S. A. Rasmussen, ‘Low risk of solid tumors in persons with Down syndrome’, Genetics in Medicine, vol. 18, no. 11, pp. 1151–1157, Nov. 2016. [CrossRef]
- A. C. Xavier, Y. Ge, and J. W. Taub, ‘Down Syndrome and Malignancies: A Unique Clinical Relationship’, The Journal of Molecular Diagnostics, vol. 11, no. 5, pp. 371–380, Sep. 2009. [CrossRef]
- K. Fosu, J. T. Quarshie, K. A. N. Sarpong, and A. R. Aikins, ‘Inverse Comorbidity between Down Syndrome and Solid Tumors: Insights from In Silico Analyses of Down Syndrome Critical Region Genes’, Genes (Basel), vol. 14, no. 4, p. 800, Mar. 2023. [CrossRef]
- D. B. Chapel, N. M. Joseph, T. Krausz, and R. R. Lastra, ‘An Ovarian Adenocarcinoma With Combined Low-grade Serous and Mesonephric Morphologies Suggests a Müllerian Origin for Some Mesonephric Carcinomas.’, Int J Gynecol Pathol, vol. 37, no. 5, pp. 448–459, Sep. 2018. [CrossRef]
- J. Pors, A. Cheng, J. M. Leo, M. A. Kinloch, B. Gilks, and L. Hoang, ‘A Comparison of GATA3, TTF1, CD10, and Calretinin in Identifying Mesonephric and Mesonephric-like Carcinomas of the Gynecologic Tract.’, Am J Surg Pathol, vol. 42, no. 12, pp. 1596–1606, Dec. 2018. [CrossRef]
- V. Patel, B. Kipp, and J. K. Schoolmeester, ‘Corded and hyalinized mesonephric-like adenocarcinoma of the uterine corpus: report of a case mimicking endometrioid carcinoma.’, Hum Pathol, vol. 86, pp. 243–248, Apr. 2019. [CrossRef]
- S. Yamamoto and Y. Sakai, ‘Pulmonary metastasis of mesonephric-like adenocarcinoma arising from the uterine body: a striking mimic of follicular thyroid carcinoma.’, Histopathology, vol. 74, no. 4, pp. 651–653, Mar. 2019. [CrossRef]
- D. L. Kolin, D. C. Costigan, F. Dong, M. R. Nucci, and B. E. Howitt, ‘A Combined Morphologic and Molecular Approach to Retrospectively Identify KRAS-Mutated Mesonephric-like Adenocarcinomas of the Endometrium.’, Am J Surg Pathol, vol. 43, no. 3, pp. 389–398, Mar. 2019. [CrossRef]
- W. G. McCluggage, H. Vosmikova, and J. Laco, ‘Ovarian Combined Low-grade Serous and Mesonephric-like Adenocarcinoma: Further Evidence for A Mullerian Origin of Mesonephric-like Adenocarcinoma.’, Int J Gynecol Pathol, vol. 39, no. 1, pp. 84–92, Jan. 2020. [CrossRef]
- M. Yano et al., ‘Coexistence of endometrial mesonephric-like adenocarcinoma and endometrioid carcinoma suggests a Müllerian duct lineage: a case report.’, Diagn Pathol, vol. 14, no. 1, p. 54, Jun. 2019. [CrossRef]
- B. Kezlarian et al., ‘Cytologic features of upper gynecologic tract adenocarcinomas exhibiting mesonephric-like differentiation.’, Cancer Cytopathol, vol. 127, no. 8, pp. 521–528, Aug. 2019. [CrossRef]
- L.-C. Horn, A. K. Höhn, I. Krücken, M. Stiller, U. Obeck, and C. E. Brambs, ‘Mesonephric-like adenocarcinomas of the uterine corpus: report of a case series and review of the literature indicating poor prognosis for this subtype of endometrial adenocarcinoma.’, J Cancer Res Clin Oncol, vol. 146, no. 4, pp. 971–983, Apr. 2020. [CrossRef]
- P. Dundr et al., ‘Ovarian mesonephric-like adenocarcinoma arising in serous borderline tumor: a case report with complex morphological and molecular analysis.’, Diagn Pathol, vol. 15, no. 1, p. 91, Jul. 2020. [CrossRef]
- K. Seay, T. Akanbi, B. Bustamante, S. Chaudhary, and G. L. Goldberg, ‘Mesonephric-like adenocarcinoma of the ovary with co-existent endometriosis: A case report and review of the literature.’, Gynecol Oncol Rep, vol. 34, p. 100657, Nov. 2020. [CrossRef]
- Q. Chen, Y. Shen, and C. Xie, ‘Mesonephric-like adenocarcinoma of the ovary: A case report and a review of the literature.’, Medicine, vol. 99, no. 48, p. e23450, Nov. 2020. [CrossRef]
- E. Deolet, J. Van Dorpe, and K. Van de Vijver, ‘Mesonephric-Like Adenocarcinoma of the Endometrium: Diagnostic Advances to Spot This Wolf in Sheep’s Clothing. A Review of the Literature.’, J Clin Med, vol. 10, no. 4, Feb. 2021. [CrossRef]
- S. Al Nabhani, A. Doyle, S. Kennedy, R. McVey, J. Crown, and D. Gibbons, ‘Endometrial Mesonephric-like Adenocarcinoma Presenting as an Ocular Lesion: A Case Report.’, Int J Gynecol Pathol, vol. 41, no. 2, pp. 161–167, Mar. 2022. [CrossRef]
- S. Choi, K. Na, S.-W. Kim, and H.-S. Kim, ‘Dedifferentiated Mesonephric-like Adenocarcinoma of the Uterine Corpus.’, Anticancer Res, vol. 41, no. 5, pp. 2719–2726, May 2021. [CrossRef]
- A. d’Amati et al., ‘Mesonephric-Like Carcinosarcoma of the Ovary Associated with Low-Grade Serous Carcinoma: A Case Report.’, Diagnostics (Basel), vol. 11, no. 5, May 2021. [CrossRef]
- E. Deolet et al., ‘Extrauterine Mesonephric-like Neoplasms: Expanding the Morphologic Spectrum.’, Am J Surg Pathol, vol. 46, no. 1, pp. 124–133, Jan. 2022. [CrossRef]
- S. Shen, M. M. Rubinstein, K. J. Park, J. A. Konner, and V. Makker, ‘Sustained response to lenvatinib and pembrolizumab in two patients with KRAS-mutated endometrial mesonephric-like adenocarcinoma.’, Gynecol Oncol Rep, vol. 37, p. 100844, Aug. 2021. [CrossRef]
- M. Ujita, K. Abiko, R. Kuwahara, I. Emoto, Y. Amano, and I. Konishi, ‘Mesonephric-like adenocarcinoma of the ovary in an elderly woman: A case report and a review of the literature.’, J Obstet Gynaecol Res, vol. 47, no. 12, pp. 4490–4495, Dec. 2021. [CrossRef]
- H. Kim, G. E. Bae, Y. Y. Jung, and H.-S. Kim, ‘Ovarian Mesonephric-like Adenocarcinoma With Multifocal Microscopic Involvement of the Fimbrial Surface: Potential for Misdiagnosis of Tubal Intraepithelial Metastasis as Serous Tubal Intraepithelial Carcinoma Associated With Ovarian High-grade Serous Carcinoma.’, In Vivo, vol. 35, no. 6, pp. 3613–3622, 2021. [CrossRef]
- H. G. Kim et al., ‘Mesonephric-like Adenocarcinoma of the Uterine Corpus: Comprehensive Analyses of Clinicopathological, Molecular, and Prognostic Characteristics With Retrospective Review of 237 Endometrial Carcinoma Cases.’, Cancer Genomics Proteomics, vol. 19, no. 4, pp. 526–539, 2022. [CrossRef]
- N. L. Hardy and P. N. Staats, ‘Metastatic mesonephric-like endometrial adenocarcinoma diagnosed on transbronchial needle aspirate cytology.’, Diagn Cytopathol, vol. 50, no. 2, pp. 86–90, Feb. 2022. [CrossRef]
- C. S. Chang, M. E. Carney, and J. L. Killeen, ‘Two Cases of Mesonephric-like Carcinoma Arising From Endometriosis: Case Report and Review of the Literature.’, Int J Gynecol Pathol, vol. 42, no. 1, pp. 101–107, Jan. 2023. [CrossRef]
- A. M. Mills, T. M. Jenkins, B. E. Howitt, J. Fan, K. L. Ring, and I. Cook, ‘Mesonephric-like Endometrial Carcinoma: Results From Immunohistochemical Screening of 300 Endometrial Carcinomas and Carcinosarcomas for This Often Overlooked and Potentially Aggressive Entity.’, Am J Surg Pathol, vol. 46, no. 7, pp. 921–932, Jul. 2022. [CrossRef]
- H. H. Koh, E. Park, and H.-S. Kim, ‘Mesonephric-like Adenocarcinoma of the Ovary: Clinicopathological and Molecular Characteristics.’, Diagnostics (Basel), vol. 12, no. 2, Jan. 2022. [CrossRef]
- E. Arslanian, K. Singh, C. James Sung, and M. R. Quddus, ‘Somatic mutation analysis of Mesonephric-Like adenocarcinoma and associated putative precursor Lesions: Insight into pathogenesis and potential molecular treatment targets.’, Gynecol Oncol Rep, vol. 42, p. 101049, Aug. 2022. [CrossRef]
- S. Restaino et al., ‘Mesonephric-Like Adenocarcinomas a Rare Tumor: The Importance of Diagnosis.’, Int J Environ Res Public Health, vol. 19, no. 21, Nov. 2022. [CrossRef]
- K. Ishida, T. Ashihara, M. So, S. Minamiguchi, N. Matsumura, and T. Nonogaki, ‘Synchronous ovarian and uterine mesonephric-like carcinoma that potentially arose from endometrioid adenofibroma: A case report.’, J Obstet Gynaecol Res, vol. 49, no. 3, pp. 1052–1056, Mar. 2023. [CrossRef]
- S. Stolnicu, R.-J. Bartalis, Q. Ye, A. Da Cruz Paula, B. Weigelt, and R. A. Soslow, ‘Ovarian RASoma With Mesonephric-like Adenocarcinoma and Mixed Mullerian Components: A Case Report With Molecular Analysis Demonstrating Multidirectional Mullerian Differentiation.’, Int J Gynecol Pathol, vol. 42, no. 6, pp. 620–626, Nov. 2023. [CrossRef]
- D. Xing, S. X. Liang, F. F. Gao, and J. I. Epstein, ‘Mesonephric Adenocarcinoma and Mesonephric-like Adenocarcinoma of the Urinary Tract.’, Mod Pathol, vol. 36, no. 1, p. 100031, Jan. 2023. [CrossRef]
- J. Xu, K. J. Park, W. M. Rehrauer, and P. S. Weisman, ‘Mesonephric-like adenocarcinoma of the ovary with squamoid morular metaplasia, aberrant β-catenin expression, and concurrent FGFR2 and CTNNB1 mutations: a case report.’, Virchows Arch, vol. 484, no. 1, pp. 147–150, Jan. 2024. [CrossRef]
- J. Mirkovic et al., ‘Mesonephric-like adenocarcinoma of the female genital tract: novel observations and detailed molecular characterisation of mixed tumours and mesonephric-like carcinosarcomas.’, Histopathology, vol. 82, no. 7, pp. 978–990, Jun. 2023. [CrossRef]
- E. D. Euscher et al., ‘Extrauterine Mesonephric-like Carcinoma: A Comprehensive Single Institution Study of 33 Cases.’, Am J Surg Pathol, vol. 47, no. 6, pp. 635–648, Jun. 2023. [CrossRef]
- H. J. Kim, K. A. Kim, Y. Chun, J. W. Kim, J. Lee, and C. H. Lee, ‘Radiologic Findings of Mesonephric-Like Adenocarcinoma of the Uterine Corpus: A Case Report.’, Journal of the Korean Society of Radiology, vol. 84, no. 3, pp. 698–704, May 2023. [CrossRef]
- A.Sugitani et al., ‘Ovarian Mesonephric-Like Adenocarcinoma With Recurrent Liver Metastases: A Case Report with Analysis of Therapeutic Molecular Targets.’, Int J Surg Pathol, vol. 32, no. 3, pp. 578–585, May 2024. [CrossRef]
- J. Linck and W. Torres, ‘Mesonephric-like adenocarcinoma arising from endometrioid adenofibroma in a patient with in-utero exposure to diethylstilbestrol: A case report’, Case Rep Womens Health, vol. 39, p. e00531, Sep. 2023. [CrossRef]
- H.-H. Koh, E. Park, and H.-S. Kim, ‘Mesonephric-like Adenocarcinoma of the Uterine Corpus: Genomic and Immunohistochemical Profiling with Comprehensive Clinicopathological Analysis of 17 Consecutive Cases from a Single Institution.’, Biomedicines, vol. 11, no. 8, Aug. 2023. [CrossRef]
- C. E. Brambs et al., ‘Mesonephric-like adenocarcinoma of the female genital tract: possible role of KRAS-targeted treatment-detailed molecular analysis of a case series and review of the literature for targetable somatic KRAS-mutations.’, J Cancer Res Clin Oncol, vol. 149, no. 17, pp. 15727–15736, Nov. 2023. [CrossRef]
- Z. Zhao, R. Nadarajah, and I. Busmanis, ‘Synchronous Bilateral Ovarian Mesonephric-like Adenocarcinomas with Separate Origins from High-Grade Mullerian Adenosarcoma and Endometriosis: Report of a Rare Case.’, Int J Gynecol Pathol, vol. 43, no. 4, pp. 382–388, Jul. 2024. [CrossRef]
- S. Nagase, H. Saeki, A. Ura, Y. Terao, T. Matsumoto, and T. Yao, ‘Mixed Mesonephric-like Adenocarcinoma, Clear Cell Carcinoma, and Endometrioid Carcinoma Arising from an Endometriotic Cyst.’, Int J Surg Pathol, vol. 32, no. 6, pp. 1140–1148, Sep. 2024. [CrossRef]
- A. Yamamoto et al., ‘Ovarian Mesonephric-like Adenocarcinoma Recurring With a Rhabdomyosarcoma Component: A Case Report.’, Int J Gynecol Pathol, vol. 43, no. 3, pp. 296–301, May 2024. [CrossRef]
- G. Angelico et al., ‘The first evidence of mismatch repair deficiency in mesonephric-like adenocarcinoma of the endometrium: clinicopathological and molecular features of a case emphasising a possible endometrioid carcinogenesis.’, Histopathology, vol. 84, no. 6, pp. 1068–1070, May 2024. [CrossRef]
- M. R. Quddus, C. A. Mathews, and K. Singh, ‘Ever Expanding Morphologic Patterns of Mesonephric-like Adenocarcinomas of the Uterine Corpus: A Report of Two Tumors and a Brief Review of the Literature.’, Int J Surg Pathol, vol. 32, no. 7, pp. 1398–1403, Oct. 2024. [CrossRef]
- Y. Yang et al., ‘Mesonephric-like adenocarcinoma of the ovary.’, J Ovarian Res, vol. 17, no. 1, p. 57, Mar. 2024. [CrossRef]
- H. Omine et al., ‘Endometrial cytological findings for a mesonephric-like endometrial adenocarcinoma: A case report.’, Diagn Cytopathol, vol. 52, no. 6, pp. E129–E133, Jun. 2024. [CrossRef]
- Y. Lee, M. R. Alam, J.-H. Kim, C. J. Kim, S. L. Lee, and K. Yim, ‘Collision Tumor of the Ovary: Adult Granulosa Cell Tumor and Mesonephric-like Adenocarcinoma.’, Diagnostics (Basel), vol. 14, no. 13, Jul. 2024. [CrossRef]
- M. Tahir et al., ‘Identifying mesonephric-like adenocarcinoma of the endometrium by combining SOX17 and PAX8 immunohistochemistry.’, Histopathology, vol. 86, no. 2, pp. 268–277, Jan. 2025. [CrossRef]
- D. Maharjan, K. Collins, T. Hou, B. Umphress, S. E. Robertson, and S. Segura, ‘Synchronous Bilateral Ovarian Carcinomas With Right Mesonephric-like Adenocarcinoma and Left High-grade Serous Carcinoma: A Case Report and Review of the Literature.’, Int J Gynecol Pathol, vol. 44, no. 2, pp. 193–197, Mar. 2025. [CrossRef]
- A. Ogawa et al., ‘Ovarian Mesonephric-like Adenocarcinoma: Its Prevalence in a Japanese High-Volume Cancer Center and a Literature Review on Therapeutic Targets.’, Curr Oncol, vol. 31, no. 9, pp. 5107–5120, Aug. 2024. [CrossRef]
- M. McFarland, C. M. Quick, and W. G. McCluggage, ‘Hormone receptor-negative, thyroid transcription factor 1-positive uterine and ovarian adenocarcinomas: report of a series of mesonephric-like adenocarcinomas.’, Histopathology, vol. 68, no. 7, pp. 1013–20, Jun. 2016. [CrossRef]
- J. Pors, A. Cheng, J. M. Leo, M. A. Kinloch, B. Gilks, and L. Hoang, ‘A Comparison of GATA3, TTF1, CD10, and Calretinin in Identifying Mesonephric and Mesonephric-like Carcinomas of the Gynecologic Tract.’, Am J Surg Pathol, vol. 42, no. 12, pp. 1596–1606, Dec. 2018. [CrossRef]
- J. Pors et al., ‘Clinicopathologic Characteristics of Mesonephric Adenocarcinomas and Mesonephric-like Adenocarcinomas in the Gynecologic Tract: A Multi-institutional Study.’, Am J Surg Pathol, vol. 45, no. 4, pp. 498–506, Apr. 2021. [CrossRef]
- A. M. Mills, T. M. Jenkins, B. E. Howitt, J. Fan, K. L. Ring, and I. Cook, ‘Mesonephric-like Endometrial Carcinoma: Results From Immunohistochemical Screening of 300 Endometrial Carcinomas and Carcinosarcomas for This Often Overlooked and Potentially Aggressive Entity.’, Am J Surg Pathol, vol. 46, no. 7, pp. 921–932, Jul. 2022. [CrossRef]
- J. Pors, A. Cheng, J. M. Leo, M. A. Kinloch, B. Gilks, and L. Hoang, ‘A Comparison of GATA3, TTF1, CD10, and Calretinin in Identifying Mesonephric and Mesonephric-like Carcinomas of the Gynecologic Tract.’, Am J Surg Pathol, vol. 42, no. 12, pp. 1596–1606, Dec. 2018. [CrossRef]
- D. Wilson and B. Bordoni, Embryology, Mullerian Ducts (Paramesonephric Ducts). 2025.
- A. J. Laham, M. Saber-Ayad, and R. El-Awady, ‘DYRK1A: a down syndrome-related dual protein kinase with a versatile role in tumorigenesis’, Cellular and Molecular Life Sciences, vol. 78, no. 2, pp. 603–619, Jan. 2021. [CrossRef]
- H. Ehara, K. Ohno, and H. Ito, ‘Benign and malignant tumors in Down syndrome: Analysis of the 1514 autopsied cases in Japan’, Pediatrics International, vol. 53, no. 1, pp. 72–77, Feb. 2011. [CrossRef]
Figure 1.
Case 1: Histopathology findings. A. Mesonephric-like carcinoma of the corpus uteri: crowded tubules and branching glands lined by cuboidal to low columnar cells with mild to moderate nuclear atypia, overlapping, angulated nuclei with focal nuclear grooves (H&E stain x400 magnification); B.TTF1 Diffuse strong nuclear immunopositivity in tumor cells; C. GATA3, diffuse moderate immunopositivity in tumor cells; D. ER negativity in tumor cells (internal control shows adequate positivity).
Figure 1.
Case 1: Histopathology findings. A. Mesonephric-like carcinoma of the corpus uteri: crowded tubules and branching glands lined by cuboidal to low columnar cells with mild to moderate nuclear atypia, overlapping, angulated nuclei with focal nuclear grooves (H&E stain x400 magnification); B.TTF1 Diffuse strong nuclear immunopositivity in tumor cells; C. GATA3, diffuse moderate immunopositivity in tumor cells; D. ER negativity in tumor cells (internal control shows adequate positivity).
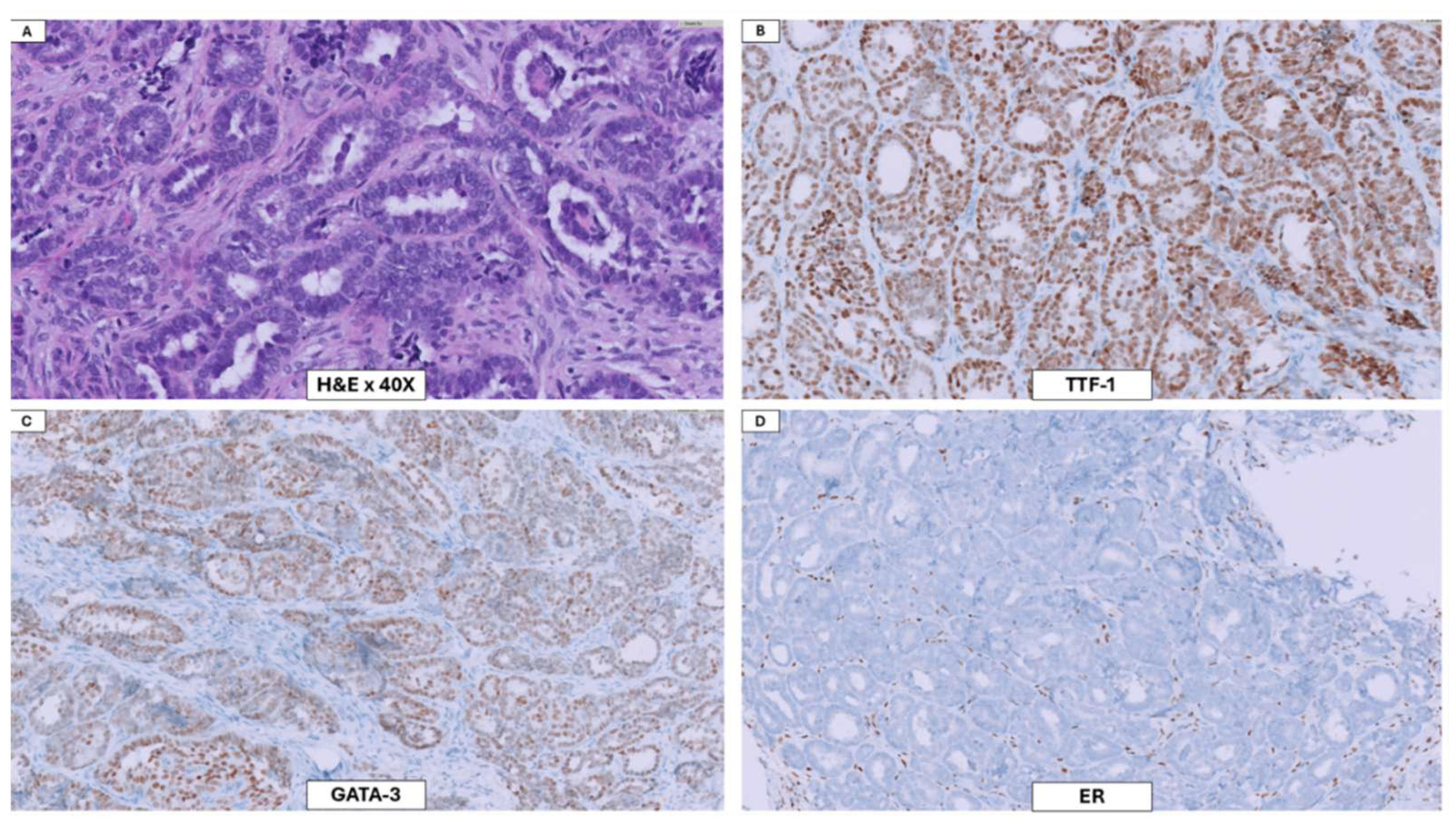
Figure 2.
Case 2: Histopathology findings. H&E-stained slides. As observed in Case 1, this lesion displayed overcrowding of glands (black arrow) with hyperchromatic nuclei and solid areas(star)(A). Additionally, some nuclei display central clearing (C) and hob nailing (D) These cells were negative for ER and PR, patchy positive for GATA-3 and positive for TTF-1(not shown).
Figure 2.
Case 2: Histopathology findings. H&E-stained slides. As observed in Case 1, this lesion displayed overcrowding of glands (black arrow) with hyperchromatic nuclei and solid areas(star)(A). Additionally, some nuclei display central clearing (C) and hob nailing (D) These cells were negative for ER and PR, patchy positive for GATA-3 and positive for TTF-1(not shown).
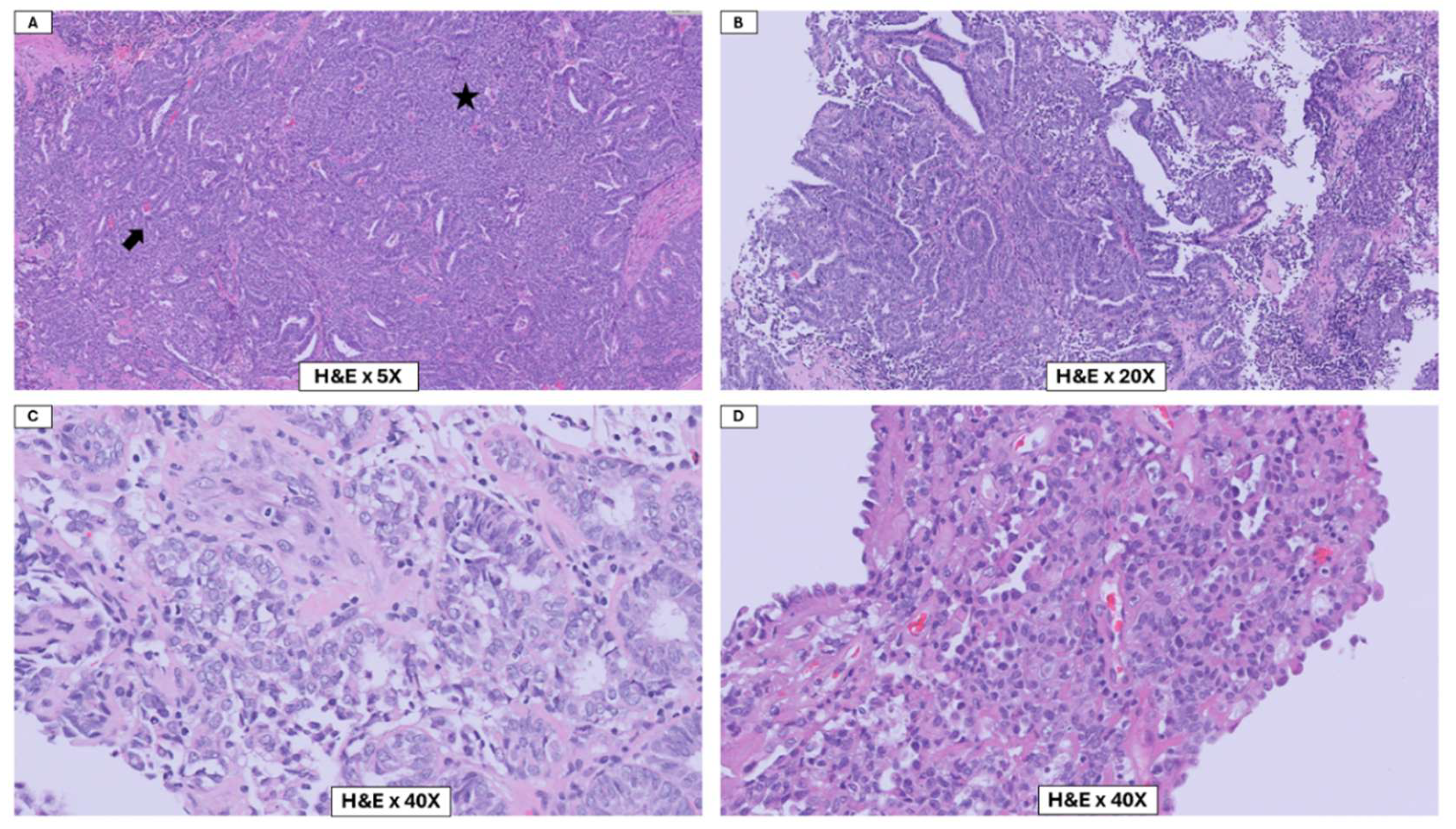

Table 1.
Clinical, Radiologic, and Immunohistochemical Features of Three Mesonephric-like Adenocarcinomas of the Uterine Corpus.
Table 1.
Clinical, Radiologic, and Immunohistochemical Features of Three Mesonephric-like Adenocarcinomas of the Uterine Corpus.
| Case | Age | C/P | Comorbidities | Location | TVUS | IHC |
| 1 | 28 | HVB | Down’s Syndrome Hypothyroidism |
Corpus | 3.0 cm mass in endometrial cavity | GATA3: positive ER : negative Napsin-A: negative TTF1: positive P16: patchy P53: |
| 2 | 29 | HVB | PCOS Hypothyroidism |
Corpus | Unremarkable | GATA3: positive ER: negative PR: negative TTF1: Patchy positive |
| 3 | 74 | HVB | Hypothyroidism Breast Cancer (IDC) |
Corpus | Thickened endometrial stripe | GATA3: negative ER: patchy (20%) PR: positive (60%) Napsin-A: patchy TTF1: patchy P16: patchy P53: wild-type |
Table 2.
Comprehensive Literature Review of Mesonephric-like Adenocarcinoma: Analysis of ~200 Published Cases Across 51 Studies.
Table 2.
Comprehensive Literature Review of Mesonephric-like Adenocarcinoma: Analysis of ~200 Published Cases Across 51 Studies.
| S/N | PMID | Authors | # of Cases | Case Source | Age | Other Comorbidities | PAX8 | GATA3 | TTF-1 | ER/PR | MSI | p53 (WT) | FIGO Stage | Molecular |
| 1 | 28863071 | David B Chapel et al. [5] | 1 | Chicago, UCSF | 80 | None | 100% | 100% | 100% | 0% | 100% | NRAS | ||
| 2 | 30148742 | Jennifer et al. [6] | 5 | Univ. of British Columbia | 65.8 (31-91) | None | 100% | 80%* | 100% | 20% | IB, IC, IIIA, IIIA, IVB | |||
| 3 | 30172914 | Patel et al. [7] | 1 | Mayo | 71 | None | 100% | 100% | 100% | 0% | MSS | 100% | ||
| 4 | 30471132 | Yamamoto et al. [8] | 1 | Japan | 70 | None | 100%* | 100%* | 100% | 0% | ||||
| 5 | 30489318 | Kolin et al. [9] | 4 | Boston/Stanford | 60.3 (57-64) | None | 100% | 33%* | 100% | 25% | 100% | IA, IB, IIIC, IVB | KRAS | |
| 6 | 30575604 | McCluggage et al. [10] | 1 | UK | 61 | None | 100% | 100%* | 100% (patchy) | 0% | 100% | KRAS | ||
| 7 | 31174566 | Yano et al. [11] | 1 | Japan | 32 | None | 100% | 100% | 0% | 100% | IA | KRAS | ||
| 8 | 31318491 | Kezlarian et al. [12] | 8 | 55.9 (36-77) | None | 100% | 100% | 33% | 14% | IA, IA, IB, III, III, IIIA, IIIB | ||||
| 9 | 31927619 | Horn et al. [13] | 4 | Germany | 63.3 (54-74) | None | 100% | 100% | 0% | MSS | 100% | IB, IB, II, IIIA | KRAS | |
| 10 | 32693840 | Dundr et al. [14] | 1 | 71 | None | 100% | 0% | 100% | 0% | 100% | IVB | KRAS | ||
| 11 | 33088886 | Seay et al. [15] | 1 | New York | 67 | Endometriosis | 100% | 100%* | 100% (patchy) | 0% | MSS | 100% | IA | |
| 12 | 33235131 | Chen et al. [16] | 1 | China | 29 | None | 100% | 100% | 100% | 0% | 0% | IC | ||
| 13 | 33670088 | Deolet et al. [17] | 1 | Belgium | 76 | None | 100% | 100% | 0% | 0% | MSS | 100% | IV | KRAS |
| 14 | 33935158 | Al Nabhani et al. [18] | 1 | Ireland | 58 | None | 100% | 0% | 100% | 0% | MSS | 100% | IV | KRAS |
| 15 | 33952503 | Choi et al. [19] | 1 | Korea | 54 | None | 100% | 100% | 0% | MSS | 100% | KRAS | ||
| 16 | 34063676 | d’Amati et al. [20] | 1 | Switzerland | 74 | Ovarian serous cystadenoma | 100% | 100% | 100% | 0% | 100% | IIIC | ||
| 17 | 34183523 | Deolet et al. [21] | 5 | UK | 61 (33-82) | Mature teratoma, mixed germ cell tumor, borderline endometrioid neoplasm, high-grade serous carcinoma, endometriosis | 100% | 100% | 80% | 0% | 100% | IA, IVB, IC, IIIC, unstaged | KRAS | |
| 18 | 34430690 | Shen et al. [22] | 2 | Memorial Sloan Kettering | 54 (60, 48) | 100% | 50% | 100% | 0% | KRAS | ||||
| 19 | 34580958 | Mari Ujita et al. [23] | 1 | Japan | 84 | Hypertension, hyperlipidemia | 100% | 0% | 100% | 0% | IC | |||
| 20 | 34697203 | Kim et al. [24] | 1 | Korea | 47 | Adenomyosis | 100% | 100% | 0% | MSS | 100% | KRAS | ||
| 21 | 34829389 | Kim et al. [25] | 25 | 59 (43-77) | None | IA (4), IB (3), II (2), IIIA, IIIB (3), IIIC1 (4), IIIC2 (2), IVB (6) | ||||||||
| 22 | 34928073 | Hardy et al. [26] | 1 | Maryland | 62 | None | 100% | 0% | 100% | 0% | 100% | KRAS | ||
| 23 | 35191427 | Chang et al. [27] | 2 | Hawaii | 54 (51,57) | Fibroids, adnexal mass, adenomyosis, endometriosis; DCIS, endometriosis | 100% | 100% | 100% | 0% | IA, IIIA1 | |||
| 24 | 35195579 | Mills et al. [28] | 2 | Virginia | None | 50% | 100% | 0% | KRAS | |||||
| 25 | 35204416 | Koh et al. [29] | 5 | Korea | 53 (42-61) | endometriosis (80%) | 100% | 100% | 80% | 60% | MSS | 100% | IA, IC, IC, IC, IIB, IVB | |
| 26 | 35732320 | Kim et al. [25] | 7 | Korea | 63 (59-72) | None | 86% | 71% | 14% | 100% | IB (3), IIIA (2), IIIC, IVB | |||
| 27 | 35880223 | Arslanian et al. [30] | 3 | 65 (65-67) | endometriosis (100%), cystadenofibroma (33%) | 100% | 100% | 33% | 33% | 100% | IC, IIA2, IIIA1 | KRAS | ||
| 28 | 36361332 | Restaino et al. [31] | 1 | Italy | 57 | previous hysteroscopy for endometrial polyp | 100% | 100% | 100% | 100% | MSS | 100% | KRAS | |
| 29 | 36597276 | Ishida et al. [32](Ishida et al., 2023) | 1 | Japan | 69 | endometrioid adenofibroma, adenomyosis | 100% | 100% | 0% | KRAS | ||||
| 30 | 36617679 | Stolnicu et al. [33] | 1 | Memorial Sloan Kettering | 63 | endometriosis | 100% | 100% | 0% | I | KRAS | |||
| 31 | 36788068 | Xing et al. [34] | 1 | Johns Hopkins | 72 | endometriosis; previous ovarian mass | 100% | 100% | 0% | 0% | 100% | KRAS | ||
| 32 | 36856760 | Xu et al. [35] | 1 | Wisconsin | 78 | endometrioid adenofibroma, adenomyosis | 100% | 100% | 0% | 0% | MSS | FGFR2and CTNNB1 | ||
| 33 | 36860193 | Mirkovic et al. [36] | 5 | Toronto | 61 (51-66) | endometrial adenocarcinoma (3); sarcoma (2); colon cancer (1) | 100% | 75% | 0% | 100% | IB (1), II (1), IIB (2), IV (1) | KRAS | ||
| 34 | 37026792 | Euscher et al. [37] | 33 | MD Anderson | 59 (37-74) | Endometriosis (64%); occult synchronous endometrial LGEC (9%) | 96% | 94% | 75% | 38% | 100% | I (19) (12 cases), II (7 cases), III (9), IV (4) | KRAS (15),PIK3CA (4); ARID1A (2); CTNNB1 (2); ATM (2) | |
| 35 | 37324981 | Kim et al. [38] | 1 | Korea | 65 | 100% | 100% | 0% | IB | |||||
| 36 | 37345348 | Sugitani et al. [39] | 1 | Japan | 53 | endometriosis, Brenner tumor (5 mm), serous cystadenoma; Adenomyosis and leiomyomas | 100% | 100% | 100% | 0% | MSS | 100% | IC1 | |
| 37 | 37560022 | Linck et al. [40] | 1 | Florida | 65 | in-utero exposure to diethylstilbestrol (DES); endometrioid adenofibroma; uterine fibroids | 100% | 100% | 100% | 0% | ||||
| 38 | 37626765 | Koh et al. [41] | 17 | None | MSS | IA (3/17), IB (6/17), IIIB (3/17), IIIC (2/17), and IVB (3/17) | KRAS(16); PIK3CA (3); PTEN (5) | |||||||
| 39 | 37668797 | Brambs et al. [42] | 8 | 60.3 (52- 74) | None | KRAS | ||||||||
| 40 | 37922943 | Zhao et al. [43] | 1 | Singapore | 58 | Endometriosis, diabetes | 100% | 100% | 100% | 0% | MSS | IC (Left), IIA (right) | ||
| 41 | 37994045 | Nagase et al. [44] | 1 | Japan | 48 | endometriosis, uterine leiomyoma and ovarian mucinous cystadenoma (5 years prior) | 100% | 100% | 0% | 100% | IV | KRAS | ||
| 42 | 38085954 | Yamamoto et al. [45] | 1 | 51 | endometriosis | 100% | 100% | 100% | 100% | 100% | IVB | KRAS | ||
| 43 | 38173293 | Angelico et al. [46] | 1 | Italy | 59 | None | 100% | 100% | 0% | MSI | 100% | IB | ||
| 44 | 38311895 | Quddus et al. [47] | 2 | Rhode Island | 64.5 (62, 67) | Fibroids | 50% | 100% | weak and focal | MSS | 100% | I, IB | KRAS, PTEN | |
| 45 | 38444000 | Yang et al. [48] | 1 | 45 | “Chocolate cyst” removal 5 years ago; concurrent teratoma | 100% | 100% | 100% | weak and focal | MSS | 100% | |||
| 46 | 38454318 | Omine et al. [49] | 1 | Japan | 76 | None | 100% | 100% | 0% | |||||
| 47 | 39001303 | Lee et al. [50] | 1 | Korea | 63 | concomitant granulosa cell tumor | 100% | 100% | 0% | 0% | IIA | |||
| 48 | 39233315 | Tahir et al. [51] | 17 | Ohio | None | 100% | 100% | 59% | 0% | 100% | ||||
| 49 | 39254222 | Maharjan et al. [52] | 1 | Indiana | 56 | None | 100% | 100% | 100% | 0% | 100% | IC2 | KRAS | |
| 50 | 39330006 | Ogawa et al. [53] | 3 | 66.3 (52-76) | endometriosis (3); obesity (2); fibroids (3); adenomyosis (2); breast cancer (1); rheumatoid arthritis (1) | 100% | 100% | 0% | MSS | 100% | ||||
| 51 | 26484981 | McFarland et al. [54] | 12 | Arkansas | 42-72 | Endometriosis (3); adenomyosis (1) | 73% | 92% | 0% | 100% | IA (5), IB (2), II (2) and IIIC (2), IV (1) |
Table 3.
Distribution of Reported Comorbidities in the MLA Literature: Müllerian, Neoplastic, Metabolic, and Environmental Associations.
Table 3.
Distribution of Reported Comorbidities in the MLA Literature: Müllerian, Neoplastic, Metabolic, and Environmental Associations.
| Reported Comorbidities associated with MLA | Number of cases |
| Müllerian/Gynecologic Associations | |
| Endometriosis | 37 |
| Adenomyosis | 6 |
| Adenofibroma | 3 |
| Uterine fibroids | 3 |
| Endometrial adenocarcinoma | 3 |
| Mature teratoma | 2 |
| Ovarian serous cystadenoma | 1 |
| Borderline endometrioid neoplasm | 1 |
| High-grade serous carcinoma | 1 |
| Mixed germ cell tumor | 1 |
| Non-Gynecologic Neoplasms | |
| Breast cancer | 1 |
| Colon cancer | 1 |
| Metabolic/Autoimmune Disorders | |
| Hypertension | 1 |
| Hyperlipidemia | 1 |
| Diabetes | 1 |
| Rheumatoid arthritis | 1 |
| Environmental/Hormonal Exposure | |
| In-utero diethylstilbestrol (DES) exposure | 1 |
| Unknown | 135 |
| Total | 200 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



