Submitted:
06 January 2026
Posted:
08 January 2026
You are already at the latest version
Abstract
Feline pulmonary carcinomas are rare and often carry a poor prognosis, particularly when associated with feline lung–digit syndrome. We report a cat with primary pulmonary carcinoma and extensive metastases—including digits, pleura, mandible, scapula, spleen, skeletal muscle, and distant lymph nodes—supporting the broader “MODAL syndrome” concept. Adjuvant therapy with toceranib phosphate and meloxicam achieved prolonged survival and excellent quality of life, with no adverse effects despite dose escalation. Rapid progression after discontinuation suggests a role for toceranib in delaying tumour growth. Immunohistochemistry revealed c-kit expression in one metastatic lesion but not in the primary tumour or most metastases, highlighting intratumoral heterogeneity and the complexity of targeted therapy. The observed benefit likely reflects toceranib’s multi-target activity (VEGFR2, PDGFR), impacting angiogenesis and tumour progression. This case represents the first report of toceranib use in feline pulmonary carcinoma and underscores its potential as a palliative option.
Keywords:
toceranib phosphate
; pulmonary carcinoma
; feline lung-digit syndrome
; MODAL syndrome
; c-kit
; immunohistochemistry
1. Introduction
Feline lung-digit syndrome (FLDS) is rare and refers to an unusual metastatic pattern from a primary pulmonary carcinoma into one or more digits, which can possibly affect multiple limbs [1]. Recently, the replacement of FLDS by MODAL (muscle/ocular/digit/aorta/lung) syndrome has been suggested, as a reminder that other sites of metastasis frequently occur [2]. Additional reported locations for metastases are the pleural cavity, bronchial lymph nodes, skin, liver, spleen, heart, brain, kidney, eye, intestine, bone, omentum and adrenal gland [1].
Primary pulmonary tumours might be clinically silent, and the patients might only show clinical signs related to the metastases and their location when the disease has often progressed considerably [2]. Consequently, the late presence of clinical signs and delayed diagnosis leads into a short mean survival time of 58 days, ranging from 12 to 122 days [3]. Treatment for this disease has proved to be difficult due to its rapid progression [2].
Toceranib phosphate (TOC) is a tyrosine kinase inhibitor that was first approved as a therapy for mast cell tumours in dogs, but that has proved to be useful in canines against other neoplasms, such as carcinomas [4]. It blocks different surface receptors in the tumoral cells, such as c-kit, vascular endothelial growth factor receptor 2 (VEGFR2), platelet derived growth factor receptor (PDGFR) and Feline McDonough Sarcoma tyrosine kinase 3 [4,5]. These receptors, when activated or overexpressed in neoplastic cells, promote tumour growth and metastatic dissemination [6].
This pharmaceutical agent has been used off label in cats with different types of carcinomas and appears to be well tolerated [5,7,8,9,10,11,12]. The major side effects reported are uncommon and can include gastrointestinal upset (21.8%), thrombocytopenia (16.3%), azotaemia (14.5%), neutropenia (9.1%) and alanine aminotransferase elevations (7.2%) [13].
This case report describes a cat that was treated with adjuvant TOC, after being diagnosed with FLDS.
2. Case Presentation
A 12-year-old, domestic long-haired, indoor, neutered female cat was presented to the veterinary clinic with a forelimb lameness graded 7 out of 10, accompanied by swelling of the fourth distal digit on the left forelimb. An additional nodular lesion was found on the fifth digit of the same limb. A seven-day course of oral meloxicam at a dosage of 0.1 mg/kg every 24h was initiated. One week following initial presentation, ulceration of the fourth digit was observed, prompting culture and sensitivity testing, which identified an Escherichia coli infection. Oral co-amoxiclav (Penamoxvet® 25 mg/ml + 6.25 mg/ml) was subsequently administered at a dosage of 20.0 mg/kg. No clinical improvement was noted after seven days of antimicrobial therapy.
A complete blood count, serum biochemistry, and digital and thoracic radiographs were performed. Both the haematological and biochemical parameters were within normal limits. Radiographic examination of the digits revealed osteolysis of the third phalanx of the fourth digit, without evidence intra-articular invasion, as well as another lesion affecting the fifth digit. Right lateral, left lateral, and dorsoventral thoracic radiographs demonstrated a solitary, well-circumscribed mass located in the caudal lung lobe. A round, air-filled cavitary lesion surrounded by soft tissue was also observed. No pleural effusion or enlargement of the tracheobronchial lymph nodes was noted.
Thoracic auscultation revealed no abnormalities, and there were no clinical signs of dyspnoea, tachypnoea, or increased respiratory effort. At the time, the cat was clinically stable and in good general condition.
A partial amputation of the fourth digit was performed due to the 2.0 cm ulcerative mass. In addition, the lesion on the fifth digit, measuring 1.1 cm, was excised. Both tissue samples were submitted for histopathological evaluation in a third-party laboratory, revealing a poorly differentiated squamous cell carcinoma on the fourth digit and an infundibular follicular cyst on the fifth digit. A presumptive diagnosis of FLDS was made.
The cat recovered well from the surgery, with no post-operative complications observed. During the post-operative recovery period, a new round lesion was detected on the lateral side of the left mandible, measuring about 1.7 cm in diameter, and suspected to represent an osseous metastatic lesion. Despite this finding, the cat remained clinically well, with no reduction in appetite or other clinical signs.
The poor prognosis was discussed with the owners, along with potential palliative treatment options, including carboplatin and TOC. Due to concerns regarding potential adverse effects, TOC was initiated at a dose of 2.3 mg/kg administered every Monday, Wednesday and Friday. After two weeks of treatment, the dosage was increased to 3.1 mg/kg. The cat was concurrently receiving meloxicam at 0.1 mg/kg once daily, with no side effects reported. The owner was provided with a “Pet Quality of Life Scale and Daily Diary” and throughout TOC treatment, the cat’s quality of life was assessed with a mean score of 10.5 out of 12 [14].
A complete haematology and serum biochemistry profile were performed prior to the first administration of TOC, two weeks after initiating treatment, and subsequently monthly. No evidence of myelosuppression or elevations in hepatic or renal parameters were observed, and no gastrointestinal adverse effects were reported. For analgesia, buprenorphine was administered transmucosally at a dose of 0.03 mg/kg every 6 hours. Time to progression was defined as the interval from the first TOC administration until radiographic and clinical evidence of disease progression, based on serial measurements of the mandibular mass, made with a calliper. Progression was documented at 65 days, at which point TOC treatment was discontinued. Following this, rapid disease progression was observed, not only in the mandibular lesion but also with enlargement of the right popliteal lymph node and the appearance of additional nodular lesions, the most prominent located in the right scapular region. Severe weight loss was also noted during the progression of the disease. Due to the rapid advancement of the disease condition and the resulting compromise in quality of life, euthanasia was elected. Survival time was calculated from the initial clinical presentation until the time of death, totalling 122 days.
3. Materials and Methods
3.1. Necropsy and Histopathological Evaluation
Written consent for necropsy was obtained from the owners, and the cadaver was submitted to the Veterinary Pathology Laboratory of the School of Medicine and Biomedical Sciences (ICBAS), University of Porto, for post-mortem examination. A full necropsy protocol was performed to assess the extent of the neoplastic condition. Tissue samples were collected from all identified lesions, which were systematically documented and measured. In cases where no macroscopic abnormalities were observed, representative samples of all major organs were nonetheless collected for histopathological evaluation, ensuring a comprehensive microscopic assessment.
The collected samples were submerged and fixed in 10% neutral buffered formalin, routinely processed, embedded in paraffin wax, sectioned at 2 μm thickness, and stained with haematoxylin and eosin (H&E) for microscopic evaluation. Additionally, unstained histological sections from the first identified digital lesion were kindly provided by the external laboratory, enabling reassessment, inclusion and comprehensive evaluation of all lesions, as well as comparative molecular analyses between lesions before and after the instituted treatment.
3.2. Immunohistochemical Study
With the aim of confirming the histogenesis of the lesions, evaluating the expression of therapeutic targets relevant to the treatment administered, and gaining further insight into the biological behaviour and progression of the neoplastic disease, a targeted immunohistochemical panel was performed on selected samples considered representative and diagnostically relevant. Antigen retrieval was carried out using a Target Retrieval Solution (Dako, Santa Clara, CA) and for visualization, the NovolinkTM Max-Polymer detection system (Novocastra, Newcastle, UK) was used, in accordance with the manufacturer's instructions. The slides were incubated in a humid chamber overnight at 4º C, with anti-pancytokeratin (clone AE1/AE3, Invitrogen; dilution factor 1:300), anti-thyroid transcription factor-1 (TTF-1) (clone IHC141, GenomeMe; ready to use) and anti-c-kit (clone CD117, Leica Biosystems; dilution factor 1:450). Between each step of the procedure, sections were washed with triphosphate-buffered saline. The 3,3-diamino-benzidine (DAB) (Sigma, St. Louis, MO) was then used as the chromogen, with haematoxylin serving as counterstaining. For negative controls, the primary antibody was replaced with another of the same immunoglobulin isotype. Positive controls consisted of canine tissue sections of normal uterine tissue, normal thyroid and a cutaneous mast cell tumour, known to express AE1/AE3, TTF-1 and c-kit, respectively.
4. Results
4.1. Necropsy
At necropsy, the animal exhibited poor body condition, with evident signs of cachexia, including marked loss of adipose tissue and muscle masses. Necropsy examination confirmed the previously reported masses and revealed additional metastatic lesions, compatible with advanced metastatic disease. A comprehensive list of all identified masses and their anatomical locations is provided in Figure 1 and the radiograph of the lesion on the fourth digit, previously excised, is presented in Figure 2a.
The lesion previously identified through imaging in the caudal left pulmonary lobe measured 3.0×2.5×2.0 cm. It was white to yellow in colour, umbilicated, elevated, and exhibited poorly defined margins (Figure 2b). All pulmonary lobes contained randomly distributed, white, grey or yellow nodules, up to 1.0 cm in diameter (Figure 2b). Another prominent lesion included a mass located in the left hemiface, extending from the oral cavity and involving the parotid area and the orbit. It measured approximately 5.0×4.5×3.0 cm, consisted of firm, white tissue, and contained a central area of purulent material (Figure 2c). Additionally, the masses located in the region of the right popliteal lymph node and in the tissues surrounding the scapula were also confirmed (Figure 2d). Other masses, of variable size and with morphological characteristics similar to those previously described, were identified in several locations, including the spleen, sublumbar lymph node, left femoral quadriceps and right gastrocnemius muscles (Figure 1).
4.2. Histopathology
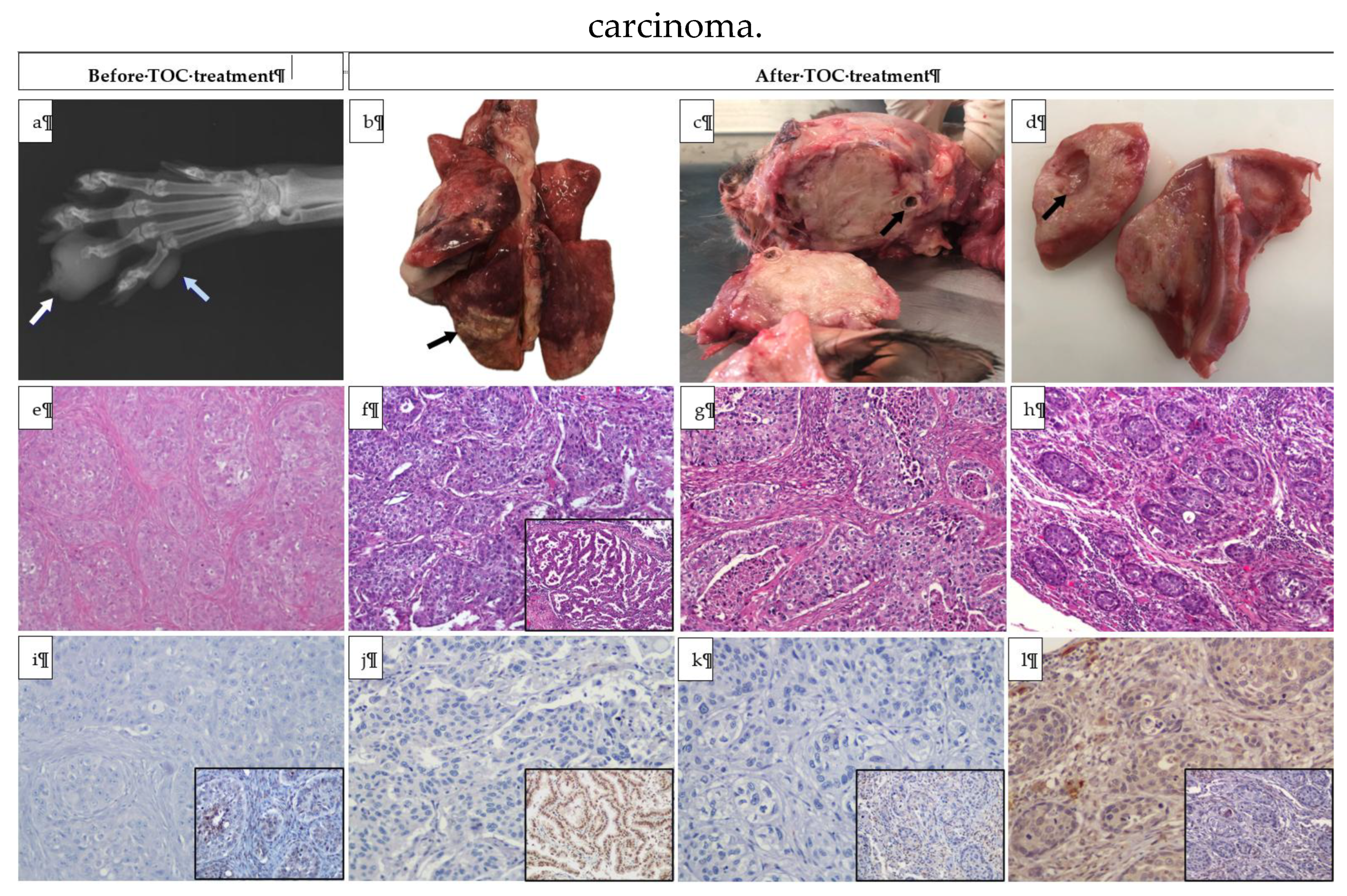
Microscopically, the pulmonary mass consisted of a population of neoplastic epithelial cells displaying two distinct patterns. The predominant pattern comprised polygonal cells arranged in sheets and nests, supported by scant fibrovascular stroma and infiltrating alveolar spaces. These cells exhibited granular to fibrillar eosinophilic or occasionally optically empty cytoplasm, variably defined borders, and round to oval nuclei with stippled chromatin. There was moderate anysokaryosis and marked anisocytosis (Figure 2f). The second and less prominent pattern consisted of papillae lined by simple columnar epithelium supported by scant fibrovascular stroma. These epithelial cells had eosinophilic cytoplasm with well-defined borders, frequently bore cilia, and contained a basal oval nucleus with stippled chromatin and, occasionally, a prominent nucleolus (Figure 2f - inset). The mitotic count was 11 per 10 HPF, with occasional bizarre mitoses. Multifocally, moderate areas of necrosis were present, associated with dystrophic calcification and cholesterol cleft formation, as well as mild peritumoral lymphoplasmacytic infiltrates. This lesion was diagnosed as a pulmonary adenosquamous carcinoma.
The other masses exhibited similar microscopic characteristics. In general, there was disruption of the normal tissue architecture, which was replaced by round to oval structures or sheets of neoplastic epithelial and polygonal cells (Figure 2e, Figure 2g and Figure 2h), showing marked nuclear pleomorphism and frequent mitotic figures. A presumptive diagnosis of a primary pulmonary adenosquamous carcinoma, with metastasis to the lung, parietal pleura, left hemiface, right scapula, spleen, popliteal and sublumbar lymph nodes, left femoral quadriceps and right gastrocnemius was considered.
4.3. Immunohistochemistry
The immunohistochemical panel was performed on slides representative of the first biopsy taken from the fourth digit of the left forelimb, as well as on lesions subsequently identified during necropsy, located in the lung, scapular region and left hemiface.
In all the lesions tested, the great majority of the neoplastic population (>95%) showed a moderate to strong, both membranous and cytoplasmatic AE1/AE3 immunopositivity, confirming the epithelial histogenesis of the lesions.
In addition, approximately 90% of the neoplastic cells constituting the papillary portion of the pulmonary lesion, exhibited moderate nuclear to paranuclear TTF-1 immunoreactivity (Figure 2j - inset). In the squamous counterpart, only about 5% of the cells exhibited mild to moderate nuclear TTF-1 immunopositivity. In all the other lesions, 0-10% of the neoplastic cells displayed weak to moderate nuclear positivity against the same antibody (Figure 2i – inset, 2k – inset, 2l – inset).
Regarding c-kit immunoexpression, no immunoreactivity was observed in the neoplastic cells present in the digit, lung, or facial lesion. (Figure 2i-2k). However, approximately 90% of the neoplastic cells in the scapular lesion exhibited weak cytoplasmic c-kit immunopositivity (Figure 2l).
The immunopositivity against TTF-1 in the lung lesion allowed diagnosing of carcinoma of pulmonary origin. Although more less common, the presence of this antigenic marking in other lesions permitted connecting them to the one found in the lungs, classifying them as metastases arising from a primary pulmonary carcinoma.
5. Discussion
Pulmonary carcinomas in cats are rare and have a poor prognosis therefore, there is limited data regarding treatment options and response [2]. Amputation of the affected digit can be recommended as a palliative measure to enhance the cat’s comfort and overall quality of life. Indeed, Gottfried et al. (2000) compiled clinicopathological findings from a group of cats with metastatic digital carcinoma originating from primary pulmonary carcinoma [3]. Among the 19 cases with complete clinical records, the median survival time from onset of clinical signs was only 58 days [3]. Digit amputation was occasionally performed as a palliative measure, but disease progression, often involving additional digits and systemic decline, was common, limiting its benefit and survival typically less than two months after diagnosis [3].
Regarding treatment, one study reported pneumonectomy performed in a cat with a well differentiated adenocarcinoma of pulmonary origin, with posterior mitoxantrone chemotherapy, resulting in survival of the animal for at least 34 months, but there was no evidence of metastatic disease [15]. The usage of tyrosine receptors inhibitors has been suggested as a possible palliative treatment for this disease, as it has been successfully used for other feline carcinomas, but it has never been specifically reported in FLDS [2]. A recent study on cats with oral squamous cell carcinoma treated with TOC reported that patients responding to this therapy experienced longer progression-free survival and overall survival times [5].
Recently, a case report described a dog with primary pulmonary adenocarcinoma that developed lung metastases three months after lobectomy [16]. TOC therapy was initiated at month ten and continued long-term, with dose adjustments due to adverse effects such as gastrointestinal signs and neutropenia [16]. The dog survived for 33 months post-diagnosis, suggesting that TOC may offer a valuable therapeutic option for metastatic pulmonary adenocarcinoma [16].
Similarly, the cat of the present report showed a longer survival time than the mean previously described [3]. Additionally, the disease seemed to progress rapidly after stopping TOC administration, suggesting that it may have held the progression of the disease during its intake.
The owner was provided with a “Pet Quality of Life Scale and Daily Diary” to monitor the cat’s well-being throughout TOC treatment. This instrument evaluates key parameters such as appetite, mobility, social interaction, and overall comfort, offering a structured approach to assess daily quality of life. During therapy, the cat achieved a mean score of 10.5 out of 12, indicating a very good level of comfort despite the underlying disease and ongoing treatment. Notably, no adverse effects were observed during treatment, and the cat appeared to maintain a good appetite even when medicated with a higher dose. This finding is clinically relevant as it suggests that TOC not only prolonged survival but also helped maintain a high quality of life, which is a fundamental objective in veterinary oncology. Nevertheless, it should be acknowledged that the assessment was performed by the owner and may therefore be subject to bias, as subjective perceptions can influence scoring accuracy.
In the present case, the cat was treated with TOC at an initial dose of 2.3 mg/kg administered on a Monday–Wednesday–Friday schedule, which was increased to 3.1 mg/kg after two weeks. The cat also received meloxicam (0.1 mg/kg once daily) concurrently, and no adverse effects were observed throughout treatment, even after the dose escalation. This contrasts with the findings of Harper and Blackwood (2017), who evaluated cats with various neoplastic conditions and reported a median toceranib dose of 2.78 mg/kg (range: 2.38–3.25 mg/kg), with 71% of cats experiencing some degree of toxicity, primarily mild gastrointestinal signs and myelosuppression, and two cases of severe hepatotoxicity requiring drug discontinuation [17]. Notably, cats with squamous cell carcinoma did not respond to treatment in their study [17]. Despite these toxicities, these authors observed a biological response rate of 57.1%, with a median response duration of 90 days [17]. In comparison, the absence of side effects in our case, even at a dose near the upper limit of the reported range (3.1 mg/kg vs. 3.25 mg/kg), suggests individual variability in drug tolerance and highlights the importance of close monitoring during therapy.
Although other studies have reported toxicities associated with toceranib phosphate administration in cats—such as gastrointestinal signs, hematologic changes, and biochemical alterations—the drug is generally considered well tolerated [5,11,13,18]. Other authors consistently describe adverse events as predominantly mild (VCOG grade I–II), resolving with supportive care, dose adjustment, or temporary discontinuation of therapy [5,13,18]. In most cases, permanent cessation of treatment was rarely required, underscoring the manageable nature of these toxicities. In the present case, no adverse effects were observed despite dose escalation, and the decision to suspend treatment was not due to toxicity but rather a clinical choice guided by established protocols and literature recommendations, prioritizing patient welfare and quality of life.
Although feline pulmonary carcinomas are classically associated with FLDS, characterized by digital metastases, atypical metastatic patterns have been increasingly recognized [1,2,19,20]. Previous reports describe dissemination to skeletal muscle, skin, and other distant sites, highlighting the aggressive biological behaviour of these tumours [1,2]. In the present case, metastases were identified not only in a digit but also in the lung, parietal pleura, mandible, scapula, spleen, skeletal muscle, and popliteal and sublumbar lymph nodes, further supporting the adoption of the broader “MODAL syndrome” terminology proposed to encompass multi-organ and distant anatomical involvement. Although regional lymph node involvement has recently been documented by Santos et al. (2023), this report appears to be the first to describe metastasis to distant lymph nodes (popliteal and sublumbar) in conjunction with such extensive multi-organ involvement [19]. These observations underscore the need for comprehensive staging and monitoring in affected cats, as metastatic spread may extend well beyond the classic digit involvement traditionally associated with FLDS.
TTF-1 is a nuclear protein expressed in human and canine type II alveolar pneumocytes as well as in bronchiolar and thyroid epithelial cells, and its diagnostic utility in feline pulmonary carcinoma, including FLDS, has been demonstrated [21,22]. Interestingly, in the present case, some cells within the papillary component of the primary tumour exhibited paranuclear staining. In human pathology, cytoplasmic immunoreactivity for TTF-1 is rarely observed and should be disregarded, with only nuclear positivity considered diagnostically relevant [23]. A recent study evaluating the immunophenotypic profile of feline pulmonary carcinomas reported an absence of TTF-1 immunoreactivity in areas of squamous differentiation [19]. In contrast, our findings revealed markedly reduced but detectable nuclear immunopositivity for TTF-1 in some squamous cells, suggesting that a subset of these cells retained expression of this transcription factor despite phenotypic divergence. This observation may be clinically relevant, as TTF-1 expression can assist in determining the primary origin of metastatic lesions, particularly in cases with complex or atypical dissemination patterns.
C-kit is a receptor tyrosine kinase involved in the differentiation and survival of immature cells, and its expression is considered physiological in several cell types. However, neoplastic cells, including those of carcinomas and mast cell tumours, may also express this marker [24,25]. In canine mast cell tumours, a well-established correlation exists between c-kit expression patterns and prognosis, with diffuse immunoreactivity associated with poorer outcomes; however, similar prognostic associations have not been demonstrated in feline mast cell tumours [25,26]. In the present case, c-kit was specifically assessed because it represents one of the primary molecular targets of TOC, the tyrosine kinase inhibitor administered to this patient. Interestingly, the primary pulmonary carcinoma lacked c-kit immunoreactivity, whereas one metastatic lesion exhibited positive staining. This finding raises important considerations regarding tumour heterogeneity and therapeutic response. The absence of c-kit immunoexpression in most metastatic sites does not imply that toceranib suppressed its expression, as the drug inhibits receptor activity rather than gene expression. Instead, it suggests that only a subset of tumour cells relied on c-kit signalling, and these may have been controlled during treatment, while c-kit-negative clones continued to proliferate. Alternatively, the clinical benefit observed could have resulted from inhibition of other relevant targets, such as VEGFR2 and PDGFR, which regulate angiogenesis and tumour progression. These observations highlight the complexity of targeted therapy in feline oncology and reinforce the need for comprehensive immunohistochemical profiling to guide personalised treatment strategies.
6. Conclusions
To the authors’ knowledge, this appears to be the first report describing the use of toceranib phosphate for the treatment of a pulmonary carcinoma in a feline patient, particularly in an adjuvant setting. Remarkably, the cat presented in this case achieved a survival time that exceeded the mean values previously reported for similar conditions, suggesting a potential therapeutic benefit. Furthermore, the rapid progression of disease observed following discontinuation of toceranib strongly implies that the drug may have contributed to delaying tumour advancement during its administration, underscoring its possible role in disease control.
Although c-kit immunoexpression was identified in one metastatic lesion, its absence in the primary tumour and other metastases suggests that the therapeutic benefit observed may not be exclusively related to c-kit inhibition. Instead, it likely reflects the multi-target activity of toceranib phosphate, which also inhibits VEGFR2 and PDGFR, thereby impacting angiogenesis and tumour progression. This finding underscores the complexity of targeted therapy in feline oncology and highlights the importance of comprehensive immunohistochemical profiling to guide treatment decisions. Future studies should evaluate the efficacy of toceranib in a larger population of cats with FLDS and further investigate its role in inhibiting multiple receptor pathways, clarifying its broader therapeutic potential in this particular condition.
Author Contributions
Conceptualization, I.C. and I.A.; methodology, I.C.; validation, I.A.; investigation, I.C., G.M., G.F.S. and I.A.; resources, F.C.; writing—original draft preparation, I.C and G.M; writing—review and editing, I.C., I.A.; supervision, I.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent was obtained from the owner of the animals, who authorized the publication of this article.
Data Availability Statement
Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| FLDS | Feline lung-digit syndrome |
| H&E | Haematoxylin and Eosin |
| HPF | High power-fields |
| MODAL | Muscle/ocular/digit/aorta/lung |
| PDGFR | Platelet derived growth factor receptor |
| TOC | Toceranib phosphate |
| TTF-1 | Thyroid transcription factor-1 |
| VEGFR2 | Vascular endothelial growth factor receptor 2 |
References
- Goldfinch, N.; Argyle, D. FELINE LUNG-DIGIT SYNDROME Unusual Metastatic Patterns of Primary Lung Tumours in Cats. JFMS CLINICAL PRACTICE Journal of Feline Medicine and Surgery 2012, 14, 202–208. [Google Scholar] [CrossRef]
- Thrift, E.; Greenwell, C.; Turner, A.L.; Harvey, A.M.; Maher, D.; Malik, R. Metastatic Pulmonary Carcinomas in Cats (‘Feline Lung–Digit Syndrome’): Further Variations on a Theme. JFMS Open Rep 2017, 3, 2055116917691069. [Google Scholar] [CrossRef] [PubMed]
- Gottfried, S.D.; Popovitch, C.A.; Goldschmidt, M.H.; Schelling, C. Metastatic Digital Carcinoma in the Cat: A Retrospective Study of 36 Cats. J Am Anim Hosp Assoc 2000, 36, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Bernabe, L.F.; Portela, R.; Nguyen, S.; Kisseberth, W.C.; Pennell, M.; Yancey, M.F.; London, C.A. Evaluation of the Adverse Event Profile and Pharmacodynamics of Toceranib Phosphate Administered to Dogs with Solid Tumors at Doses below the Maximum Tolerated Dose. BMC Vet Res 2013, 9. [Google Scholar] [CrossRef]
- Wiles, V.; Hohenhaus, A.; Lamb, K.; Zaidi, B.; Camps-Palau, M.; Leibman, N. Retrospective Evaluation of Toceranib Phosphate (Palladia) in Cats with Oral Squamous Cell Carcinoma. J Feline Med Surg 2017, 19, 185–193. [Google Scholar] [CrossRef]
- Fonseca-Alves, C.E.; Massimini, M.; Gentilini, F.; Nascimento, Y.; Coelho, B. Tyrosine Kinase Inhibitors as an Alternative Treatment in Canine Mast Cell Tumor. 2023. [Google Scholar] [CrossRef]
- Dedeaux, A.M.; Langohr, I.M.; Boudreaux, B.B. Long-Term Clinical Control of Feline Pancreatic Carcinoma with Toceranib Phosphate. Can Vet J 2018, 59, 751–754. [Google Scholar] [PubMed]
- Todd, J.E.; Nguyen, S.M. Long-Term Survival in a Cat with Pancreatic Adenocarcinoma Treated with Surgical Resection and Toceranib Phosphate. Journal of Feline Medicine and Surgery Open Reports 2020, 6. [Google Scholar] [CrossRef]
- Keepman, S.J.; Pellin, M.A. Low Dose Meloxicam Is Safe and Tolerable When Combined with Toceranib Phosphate in Cancer-Bearing Cats. J Feline Med Surg 2022, 24, 1187–1194. [Google Scholar] [CrossRef]
- Kopke, M.A.; Gal, A.; Piripi, S.A.; Poirier, V.J. Squamous Cell Carcinoma of the Anal Sac in Two Cats. Journal of Small Animal Practice 2021, 62, 704–708. [Google Scholar] [CrossRef]
- Olmsted, G.A.; Farrelly, J.; Post, G.S.; Smith, J. Tolerability of Toceranib Phosphate (Palladia) When Used in Conjunction with Other Therapies in 35 Cats with Feline Oral Squamous Cell Carcinoma: 2009–2013. J Feline Med Surg 2017, 19, 568–575. [Google Scholar] [CrossRef]
- Del Portillo Miguel, I.; Blackwood, L.; Maiques, E.; Pérez Roger, I.; Poch Jiménez, E.; Borrego, J. Evaluation of the Efficacy and Safety of Toceranib Phosphate in Cats with Macroscopic Mammary Adenocarcinoma. J Feline Med Surg 2024, 26. [Google Scholar] [CrossRef]
- Merrick, C.H.; Pierro, J.; Schleis, S.E.; Sones, E.A.; Wright, Z.M.; Regan, R.C.; Siedlecki, C.T.; Bergman, P.J. Retrospective Evaluation of Toceranib Phosphate (Palladia®) Toxicity in Cats. Vet Comp Oncol 2017, 15, 710–717. [Google Scholar] [CrossRef]
- Lap of Love Pet Quality-of-Life Scale. Available online: https://www.lapoflove.com/how-will-i-know-it-is-time/lap-of-love-quality-of-life-scale.pdf (accessed on 1 May 2022).
- Clements, D.N.; Hogan, A.M.; Cave, T.A. Treatment of a Well Differentiated Pulmonary Adenocarcinoma in a Cat by Pneumonectomy and Adjuvant Mitoxantrone Chemotherapy. J Feline Med Surg 2016, 6, 199. [Google Scholar] [CrossRef] [PubMed]
- TAMURA, Y.; NIWA, A.; MATSUDA, K.; ENDO, Y.; KADOSAWA, T. 原発性肺腺癌の肺転移病巣に対してリン酸トセラニブによる長期治療を行った犬の1例. 日本獣医師会雑誌 2017, 70, 52–55. [Google Scholar] [CrossRef]
- Harper, A.; Blackwood, L. Toxicity and Response in Cats with Neoplasia Treated with Toceranib Phosphate. J Feline Med Surg 2017, 19, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Berger, E.P.; Johannes, C.M.; Post, G.S.; Rothchild, G.; Shiu, K.B.; Wetzel, S.; Fox, L.E. Retrospective Evaluation of Toceranib Phosphate (Palladia) Use in Cats with Mast Cell Neoplasia. J Feline Med Surg 2018, 20, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Santos, I.R.; Raiter, J.; Lamego, É.C.; Bandinelli, M.B.; Dal Pont, T.P.; Siqueira, K.F.; Almeida, B.A.; Panzeira, W.; Sonne, L.; Driemeier, D.; et al. Feline Pulmonary Carcinoma: Gross, Histological, Metastatic, and Immunohistochemical Aspects. Vet Pathol 2023, 60, 8–20. [Google Scholar] [CrossRef]
- Sugiyama, H.; Maruo, T.; Shida, T.; Ishikawa, T.; Kanakubo, K.; Madarame, H.; Kayanuma, H.; Suganuma, T. Clinical Findings in Lung-Digit Syndrome in Five Cats. Journal of Japan Veterinary Cancer Society 2010, 1, 8–13. [Google Scholar] [CrossRef]
- Finotello, R.; Masserdotti, C.; Baroni, G.; Ressel, L. Role of Thyroid Transcription Factor-1 in the Diagnosis of Feline Lung–Digit Syndrome. J Feline Med Surg 2017, 19, 477–483. [Google Scholar] [CrossRef]
- D’Costa, S.; Yoon, B.I.; Kim, D.Y.; Motsinger-Reif, A.A.; Williams, M.; Kim, Y. Morphologic and Molecular Analysis of 39 Spontaneous Feline Pulmonary Carcinomas. Vet Pathol 2012, 49, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Bejarano, P.A.; Mousavi, F. Incidence and Significance of Cytoplasmic Thyroid Transcription Factor-1 Immunoreactivity. Arch Pathol Lab Med 2003, 127, 193–195. [Google Scholar] [CrossRef]
- Smith, A.J.; Njaa, B.L.; Lamm, C.G. Immunohistochemical Expression of C-KIT Protein in Feline Soft Tissue Fibrosarcomas. Vet Pathol 2009, 46, 934–939. [Google Scholar] [CrossRef]
- Rodriguez-Cariño, C.; Fondevila, D.; Segalés, J.; Rabanal, R.M. Expression of KIT Receptor in Feline Cutaneous Mast Cell Tumors. Vet Pathol 2009, 46, 878–883. [Google Scholar] [CrossRef] [PubMed]
- Kiupel, M.; Webster, J.D.; Kaneene, J.B.; Miller, R.; Yuzbasiyan-Gurkan, V. The Use of KIT and Tryptase Expression Patterns as Prognostic Tools for Canine Cutaneous Mast Cell Tumors. Vet Pathol 2004, 41, 371–377. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Anatomical distribution and gross features of metastatic masses identified at necropsy. Despite the variability in size, all lesions were irregular, multinodular and presented poorly defined margins. Created in BioRender.com, accessed on 21st November 2025.
Figure 1.
Anatomical distribution and gross features of metastatic masses identified at necropsy. Despite the variability in size, all lesions were irregular, multinodular and presented poorly defined margins. Created in BioRender.com, accessed on 21st November 2025.
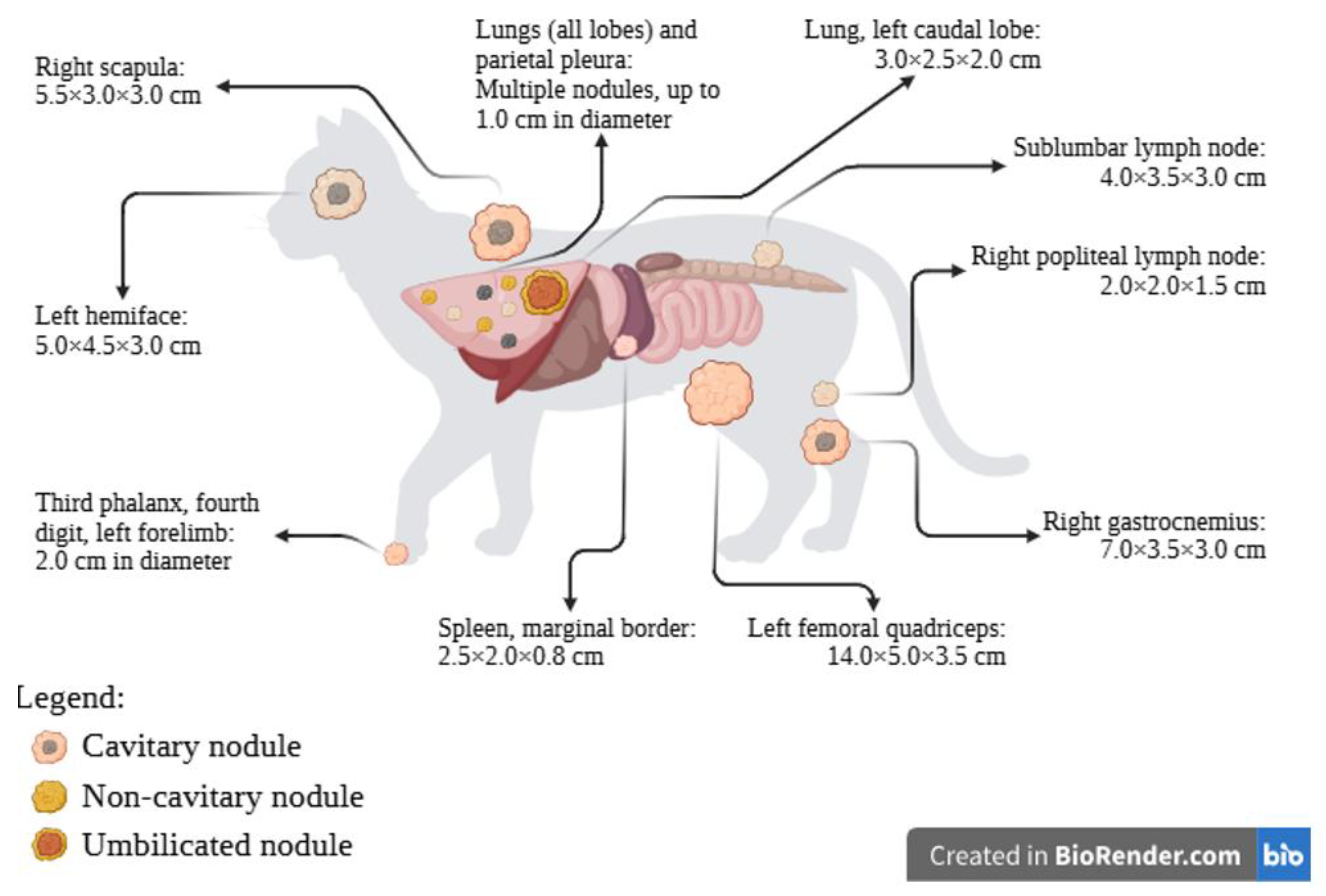
Figure 2.
Main lesions, histopathological and immunohistochemical investigations, before and after treatment with toceranib phosphate. (a) Radiography of the left forelimb, dorso-palmar projection. An extensive mass can be identified, causing osteolysis of the third phalanx of the fourth digit (White arrow). Furthermore, a smaller nodule can be discerned in the fifth digit (Blue arrow). (b) Cardiorespiratory system. A larger, yellow, umbilicated lesion is present in the left caudal lobe (arrow) and there are smaller, white, yellow or grey masses, multifocally and randomly distributed in all lobes. (c) Sagittal cuts of the head. An extensive mass occupies the left side of the head, extending from the ocular region into the ear canal (arrow). (d) Right scapula. Infiltrating the scapula, there is an extensive white, multinodular, irregularly shaped mass, with poorly defined borders and a central cavity. (e) Fourth digit lesion in the left front limb. There are nests of polygonal cells, surrounded by moderate amounts of fibrous tissue (H&E, 100x) (f) Lung, squamous portion of the neoplasm. Alveolar spaces are invaded by nests of polygonal neoplastic cells (H&E, 100x). Inset: Arborizing fronds of columnar cells, supported by scant fibrovascular stroma form the papillary portion of the neoplasm (H&E, 100x). (g) Left hemiface lesion. The presence of neoplastic cells triggers a noticeable desmoplastic reaction (H&E, 100x). (h) Right scapular lesion. Multifocally throughout the tissue, there is formation of round to oval structures containing neoplastic cells (H&E, 100x). (i) Fourth digit mass. There is no immunoreactivity against c-kit (200x). Inset: About 10 % of neoplastic cells have moderate nuclear marking against TTF-1 (200x). (j) Primary lesion in the lung. None of the cells show immunopositivity against c-kit (200x). Inset: The majority of cells that form the papillary portion of the tumour have marked nuclear immunoreactivity against TTF-1 (200x). (k) Metastatic hemifacial lesion. C-kit cannot be detected using immunohistochemistry. (200x). Inset: Few cells show moderate nuclear immunoreactivity against TTF1 (200x). (l) Right scapular lesion. A faint, diffuse cytoplasmatic immunoreactivity against c-kit can be seen in the majority of neoplastic cells (200x). Inset: There is rare immunopositivity against TTF-1 in the nucleus of neoplastic cells (200x).
Figure 2.
Main lesions, histopathological and immunohistochemical investigations, before and after treatment with toceranib phosphate. (a) Radiography of the left forelimb, dorso-palmar projection. An extensive mass can be identified, causing osteolysis of the third phalanx of the fourth digit (White arrow). Furthermore, a smaller nodule can be discerned in the fifth digit (Blue arrow). (b) Cardiorespiratory system. A larger, yellow, umbilicated lesion is present in the left caudal lobe (arrow) and there are smaller, white, yellow or grey masses, multifocally and randomly distributed in all lobes. (c) Sagittal cuts of the head. An extensive mass occupies the left side of the head, extending from the ocular region into the ear canal (arrow). (d) Right scapula. Infiltrating the scapula, there is an extensive white, multinodular, irregularly shaped mass, with poorly defined borders and a central cavity. (e) Fourth digit lesion in the left front limb. There are nests of polygonal cells, surrounded by moderate amounts of fibrous tissue (H&E, 100x) (f) Lung, squamous portion of the neoplasm. Alveolar spaces are invaded by nests of polygonal neoplastic cells (H&E, 100x). Inset: Arborizing fronds of columnar cells, supported by scant fibrovascular stroma form the papillary portion of the neoplasm (H&E, 100x). (g) Left hemiface lesion. The presence of neoplastic cells triggers a noticeable desmoplastic reaction (H&E, 100x). (h) Right scapular lesion. Multifocally throughout the tissue, there is formation of round to oval structures containing neoplastic cells (H&E, 100x). (i) Fourth digit mass. There is no immunoreactivity against c-kit (200x). Inset: About 10 % of neoplastic cells have moderate nuclear marking against TTF-1 (200x). (j) Primary lesion in the lung. None of the cells show immunopositivity against c-kit (200x). Inset: The majority of cells that form the papillary portion of the tumour have marked nuclear immunoreactivity against TTF-1 (200x). (k) Metastatic hemifacial lesion. C-kit cannot be detected using immunohistochemistry. (200x). Inset: Few cells show moderate nuclear immunoreactivity against TTF1 (200x). (l) Right scapular lesion. A faint, diffuse cytoplasmatic immunoreactivity against c-kit can be seen in the majority of neoplastic cells (200x). Inset: There is rare immunopositivity against TTF-1 in the nucleus of neoplastic cells (200x).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



