
Submitted:
03 January 2026
Posted:
06 January 2026
You are already at the latest version
Abstract
This study aims to characterizing both the pre-existing conditions that increase susceptibility and the long-term, post-acute sequelae ("long flu") following influenza. A longitudinal cohort study was conducted using data from the FinnGen cohort of 429,209 individuals including 9,204 influenza cases. A disease-wide association study (DWAS) framework was employed, using Cox proportional hazards models adjusted for age and sex to analyze 110 influenza-comorbid clinical endpoints. Pre-existing conditions, most notably cardiovascular diseases such as heart failure, coronary atherosclerosis, atrial fibrillation, and stroke, were significantly associated with an increased likelihood of a subsequent influenza diagnosis. Following influenza, individuals had a substantially elevated risk for a durable, multi-system "long flu" syndrome. The most robust and persistent risks were for new-onset cardiovascular and neurological diseases. Risks for thromboembolic events, heart failure, atrial fibrillation, stroke, and myocardial infarction remained significantly elevated for one to five years following influenza. Similarly, influenza was associated with a long-term increased incidence of neurodegenerative disorders, including migraine (with and without aura), Alzheimer's disease, and dementia. These findings underscore the urgent need to intensify preventive strategies, particularly through targeted vaccination of at-risk individuals, and to develop integrated care pathways to manage the multi-organ sequelae of long flu.
Keywords:
influenza
; long flu
; disease-wide association study
; post-acute sequelae
; cardiovascular disease
; atrial fibrillation and flutter
; heart failure
; myocardial infarction
; stroke
1. Introduction
Influenza, a viral pathogen responsible for recurrent seasonal epidemics and devastating pandemics for over a century, has historically been conceptualized primarily as an acute respiratory illness.[1] This paradigm, however, requires a fundamental re-evaluation, according to the World Health Organization (WHO) that endorsed the Pandemic Influenza Preparedness (PIP) Framework incorporating lessons from COVID-19.[2,3,4] The recent COVID-19 pandemic cast a stark light on the profound and persistent multi-organ sequelae that can follow an acute viral infection, a phenomenon now widely recognized as long COVID or Post-Acute Sequelae of SARS-CoV-2 (PASC).[5,6] This has catalyzed a critical re-examination of other respiratory viruses, prompting the hypothesis that influenza may also precipitate a parallel, yet under-characterized, post-acute infection syndrome (PAIS)—a “long flu”.[7,8]
Long flu has been recognized for many years, particularly within the cardiovascular system. The association between influenza and cardiac dysfunction is not a modern observation; severe cardiac damage was documented in nearly all fatalities of the 1918 Spanish flu pandemic,[9] and has been a consistent finding in autopsies of fatal seasonal influenza cases since.[10,11] Modern epidemiological analyses have quantified this burden, estimating that influenza infection is significantly attributable to cardiovascular diseases (CVDs), such as myocarditis,[12] ischemic heart disease,[13] stroke,[14] heart failure,[15] atrial fibrillation,[16,17] and acute myocardial infarction.[18,19,20,21,22] Crucially, recent experimental evidence has transcended correlation, providing mechanistic underpinnings for these observations. Studies using heart- influenza virus models have demonstrated that robust viral replication within cardiomyocytes is a requisite driver of cardiac fibrosis and electrical dysfunction, a pathogenic effect that is not solely attributable to systemic inflammation from severe lung infection.[23] Beyond the heart, emerging evidence also links influenza to adverse neurological outcomes of Alzheimer’s Disease and dementia,[24,25,26] further supporting its potential for systemic, long-term pathology.
Despite this growing body of evidence, our understanding of the long-term, multi-system consequences of influenza remains fragmented. Prior research has often been confined to shorter follow-up periods, a narrow spectrum of outcomes, or a singular focus on either cardiovascular or respiratory complications. Consequently, a comprehensive, longitudinal cartography of the risks preceding and following influenza infection is conspicuously absent. Comparative analyses with COVID-19 have revealed that while both viruses impose a significant post-acute burden, they exhibit distinct organ-specific risk profiles.[8] This finding underscores the necessity of characterizing long flu not merely as an analogue of long COVID, but as a distinct clinical entity with its own unique landscape of risk and morbidity. Key knowledge gaps persist regarding the long-term persistence of multi-organ sequelae, the pre-existing conditions that confer susceptibility, and the pathophysiology of extrapulmonary complications independent of acute pneumonia.
To address these critical gaps, this study leveraged a large-scale cohort to conduct a disease-wide association study (DWAS), systematically mapping the landscape of health outcomes following influenza. This DWAS approach was chosen due to its ability to capture the broad spectrum of disease associations and its previous successful application in investigating systemic conditions such as stroke, depression, and Alzheimer’s disease.[27,28,29,30,31] This DWAS of influenza aims to provide a comprehensive, temporally resolved portrait of both pre-existing risks before influenza and the subsequent risk of multi-organ sequelae, with a particular focus on their persistence over one, five, and fifteen years. By situating these findings within a multi-system framework, this effort seeks to redefine the true, long-term burden of this ubiquitous pathogen. This comprehensive landscape is essential for refining preventive strategies—including vaccination prioritization and risk stratification—and for generating precise hypotheses to guide future mechanistic and interventional research.
2. Materials and Methods
2.1. Study Design and Data Source
This investigation was designed as a nationwide, registry-based cohort study, leveraging the comprehensive, longitudinal data architecture of the FinnGen project.[32] The FinnGen infrastructure provides a unique opportunity for high-fidelity epidemiological research by linking data from multiple national Finnish registries, which collectively offer cradle-to-grave tracking of the entire population. Core data sources for this study included: 1) the Care Register for Health Care (HILMO), which captures all inpatient and outpatient specialist care encounters nationwide; 2) the Population Register Centre (DVV) and the National Death Registry, providing demographic information and date and cause of death; and 3) the Social Insurance Institution (Kela) registry, which contains records of all prescription medication purchases and reimbursements. The deterministic linkage of these registries using unique personal identity codes creates a robust, population-scale dataset that enables the detailed characterization of disease trajectories over several decades.
2.2. Cohort Assembly and Definition
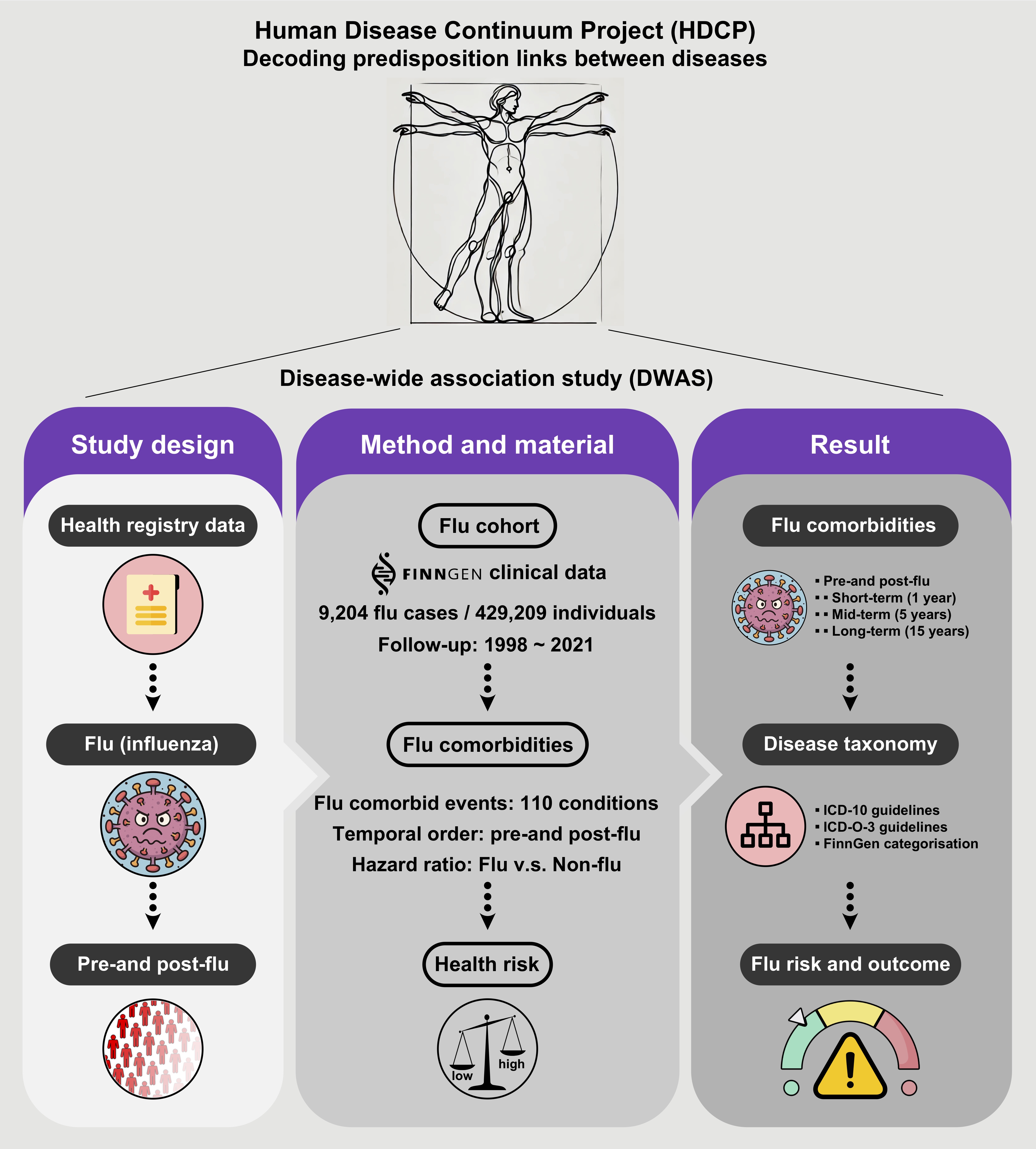
From the total FinnGen cohort, this study constructed two distinct study groups. The influenza-exposed cohort was defined as all individuals with at least one recorded clinical diagnosis of influenza from inpatient or outpatient specialist care between January 1, 1998, and December 31, 2021. Influenza cases were identified using International Classification of Diseases, 10th Revision (ICD-10) codes: J09 (influenza due to identified zoonotic or pandemic influenza virus), J10 (influenza due to other identified influenza virus), and J11 (influenza, virus not identified), resulting in an initial cohort of 9,204 individuals. For the unexposed comparator cohort, this study identified 420,005 individuals from the same source population who had no recorded diagnosis of either influenza or pneumonia (ICD-10 codes: J09-J18) throughout their entire available medical history. The follow-up for all participants commenced on January 1, 1998, and continued until the date of death or the end of the study period on December 31, 2021 (Figure 1).
2.3. Disease Endpoint Ascertainment
To construct a comprehensive, multi-system landscape of clinical conditions, this analysis evaluated a broad range of 110 influenza-comorbid clinical endpoints (Table S1). These endpoints were defined and harmonized within the FinnGen project, utilizing established algorithms that map diagnoses from the ICD-10 and the International Classification of Diseases for Oncology, Third Edition (ICD-O-3) to specific disease categories. This standardized disease taxonomy ensures consistent endpoint definition across the cohort and facilitates a systematic, high-throughput analysis of multi-organ morbidity.
2.4. Statistical Analysis
This study employed a temporally-stratified, disease-wide association study (DWAS)[27,28,29,30] framework to systematically map the landscape of diseases associated with influenza. This analysis was bidirectional, designed to assess both pre-existing conditions that may confer susceptibility to influenza and the long-term incident outcomes that manifest as post-acute sequelae.
For each of the 110 clinical endpoints, this analysis fitted separate Cox proportional hazards models, adjusted for age and sex, to estimate hazard ratios (HRs) and 95% confidence intervals (CIs).[33] The proportional hazards assumption was assessed for all models. To account for the large number of hypotheses tested, this study controlled the false discovery rate (FDR), with an FDR-adjusted p-value < 0.001 considered the threshold for robust statistical significance.
The temporal dynamics of disease association were dissected by stratifying the analysis into distinct time windows relative to the influenza index date. To identify pre-existing risk factors, this analysis assessed the prevalence of different endpoints diagnosed at any point before the index date in the influenza cohort compared to the unexposed group. Additionally, to characterize the longitudinal burden of long flu, this analysis evaluated the incidence of new-onset diseases diagnosed after the index date. This post-infection follow-up period was further segmented into 1-year, 5-year, and 15-year time windows to assess the persistence and evolution of risk over time.
To prioritize the most clinically impactful findings, this study further highlighted “high-risk” associations that satisfied three stringent criteria: a robust statistical association (FDR-adjusted p-value < 0.001), a substantial effect size (HR > 2.0 or < 0.5), and a minimum clinical prevalence (>0.5% in the exposed cohort). This filtering approach ensures that the identified associations are both statistically sound and clinically relevant.
3. Results
3.1. Overview of Disease-Wide Association of Influenza
The DWAS of 110 distinct clinical endpoints revealed a complex landscape of influenza-related disorders. After stringent correction for multiple hypothesis testing (FDR-adjusted p-value < 0.001), this analysis identified numerous significant associations spanning a wide array of organ systems. These included not only the expected respiratory conditions but also robust links to diseases of the circulatory system (I9), musculoskeletal system and connective tissue (M13), nervous system (G6), cancer (CD2; ICD−O−3), digestive system (K11), endocrine, nutritional and metabolic diseases (E4), mental and behavioral disorders (F5), eye and adnexa (H7), and respiratory system (J10), as well as specific rheumatoid and autoimmune diseases (Figure 2).
This broad pattern of associations underscores that the clinical impact of influenza extends far beyond the acute respiratory tract, implicating it as a significant systemic stressor. The subsequent analyses dissect the temporal nature of these associations, distinguishing between pre-existing conditions that predispose individuals to influenza and the long-term sequelae that define the “long flu” syndrome.
3.2. Pre-Existing Risks of Increased Influenza Predisposition
This study first investigated the pre-influenza health status of individuals who subsequently received a clinical diagnosis of influenza. This analysis of the predisposition window revealed that a significant burden of chronic disease was associated with a higher likelihood of future influenza diagnosis. Notably, pre-existing cardiovascular diseases (CVDs) constituted the most prominent risk category. Individuals with established diagnoses of heart failure, hypertension, coronary atherosclerosis, atrial fibrillation and flutter, pulmonary embolism, major coronary heart disease, stroke, myocardial infarction, and venous thromboembolism all demonstrated a significantly higher probability of a subsequent influenza diagnosis compared to the unexposed cohort (Figure 3 and Figure 4).
Beyond the cardiovascular system, other chronic conditions also emerged as significant predisposing factors. These included chronic respiratory diseases such as chronic obstructive pulmonary disease (COPD), metabolic disorders like type 2 diabetes, and chronic inflammatory conditions, including rheumatoid arthritis. This pattern suggests that the risk of progressing to clinically significant influenza is not random but is concentrated in individuals with a higher burden of pre-existing, non-communicable diseases, likely reflecting a state of heightened vulnerability or compromised physiological reserve.
3.3. Long-Term, Multi-System Sequelae Following Influenza
The central objective of this study was to characterize the post-acute landscape of incident disease following influenza. This analysis of the post-infection period identified a substantial burden of new-onset morbidity across multiple organ systems, with many risks persisting for years after the acute infection. The temporal dynamics of these sequelae were heterogeneous; some risks were concentrated in the immediate post-infection period, while others remained significantly elevated for up to one-to-fifteen years, defining a clear “long flu” phenotype (FDR-adjusted p-value < 0.001; Figure 4).
The most striking and persistent signals were observed within the cardiovascular and neurological domains. While long COVID has been associated with neurological symptoms, neurological complications in long flu are less well-studied and require more rigorous investigation to establish clear patterns and mechanisms. Moreover, significant long-term risks were also identified for metabolic, musculoskeletal, and renal disorders, including new-onset type 2 diabetes, osteoporosis, and chronic kidney disease. These findings collectively establish that influenza can act as an initiating or accelerating event for a wide spectrum of chronic conditions, contributing to a substantial long-term burden of health loss.
3.4. Persistent Cardiovascular and Neurological Risk Signatures
Among the diverse sequelae, cardiovascular and neurological outcomes represented the most robust and durable risk signatures. Following an influenza infection, individuals exhibited a significantly elevated risk for a wide range of incident CVDs. The risk for thromboembolic events, including pulmonary embolism and venous thromboembolism, was acutely elevated in the first year post-infection before gradually attenuating over time. Additionally, the risks for other major cardiovascular events, such as heart failure, atrial fibrillation and flutter, stroke, and myocardial infarction, also remained statistically significant and clinically relevant across the one-to-five year follow-up windows (Figure 4). This long-term, persistent elevation in cardiovascular risk highlights influenza as a potent trigger for durable adverse cardiac and vascular remodeling.
A parallel signature of persistent risk was observed for neurological and psychiatric conditions. Influenza was associated with a long-term increased incidence of neurodegenerative disorders, including migraine (with and without aura), Alzheimer’s disease and dementia, as well as common mental health conditions such as depression. The risk for these conditions was evident within the first year and persisted throughout the one-to-five-year follow-up period (Figure 3 and Figure 4). These findings suggest that the systemic inflammation or potential neurotropic effects of influenza may contribute to the initiation or acceleration of neuropathological processes.
In summary, this longitudinal analysis reveals that an influenza infection is not an isolated event but is embedded in a continuum of chronic disease. It is both preceded by a state of heightened vulnerability, particularly in patients with existing cardiometabolic disease, and is followed by a durable, multi-system legacy of heightened risk for new-onset chronic conditions, with cardiovascular and neurological diseases being the most prominent long-term sequelae.
4. Discussion
This nationwide, disease-wide investigation fundamentally reframes our understanding of influenza, moving beyond its conceptualization as a self-limited respiratory illness to redefine it as a potent systemic catalyst for a broad spectrum of chronic, non-communicable diseases. By analyzing the longitudinal health trajectories of an entire population, this study demonstrates that a clinical diagnosis of influenza is not a stochastic event but is deeply embedded within a continuum of multi-morbidity. These findings establish a clear bidirectional relationship: a substantial burden of pre-existing chronic disease, particularly cardiometabolic conditions, markedly increases susceptibility to clinically significant influenza, which in turn precipitates a durable, multi-system legacy of incident morbidity that persists for up to five-to-fifteen years. This “long flu” syndrome, characterized by significantly elevated risks of cardiovascular, neurological, and metabolic sequelae, represents a previously underappreciated public health burden.
The findings from this study underscore the long-term, multi-organ sequelae associated with influenza infection, particularly highlighting the sustained cardiovascular and neurological risks that persist for years after recovery from acute infection. While these results align with previous research documenting the broader systemic effects of influenza, they also emphasize the need for a clearer conceptualization of “long flu.” As we have discussed, “long flu” is not a single syndrome but rather a constellation of independent post-viral sequelae that may include cardiovascular, neurological, and other systemic complications. This understanding is crucial as it helps to guide future research and inform clinical practices related to post-influenza care. It is important to note, however, that due to limitations in the available data, such as the lack of information on vaccination status, socio-economic factors, and behavioral variables, the study’s findings may be subject to residual confounding. While adjustments for major pre-existing conditions were made, further research incorporating these additional variables is needed to refine our understanding of long flu and its clinical implications. Moving forward, a more rigorous investigation into the construct validity of long flu, including potential latent class or factor analyses, is essential to further define its clinical significance and distinguish it from other post-viral syndromes, such as long COVID.
A central finding of this study is the profound and enduring interplay between influenza and cardiovascular disease. This analysis demonstrates that influenza effectively functions as a systemic “stress test,” unmasking latent cardiovascular vulnerability and actively promoting new-onset pathology. The observation that individuals with pre-existing heart failure, coronary atherosclerosis, and atrial fibrillation are predisposed to influenza aligns with a model where compromised physiological reserve lowers the threshold for severe infection. More striking, however, is the clear evidence of influenza as a causative or accelerating factor for long-term cardiovascular risk, independent of acute pneumonia. The persistent, multi-year elevation in risk for heart failure, stroke, and myocardial infarction post-infection points towards mechanisms that transcend the acute inflammatory phase. This aligns with experimental data showing direct influenza virus replication in cardiomyocytes drives cardiac fibrosis and dysfunction, and with large-scale observational studies estimating that influenza is attributable for a substantial fraction of ischemic heart disease mortality globally. Plausible mechanisms likely involve a concert of pathways, including sustained endothelial dysfunction, a persistent pro-thrombotic state, and chronic, low-grade inflammation that accelerates underlying atherosclerotic processes.[15,23,34]
The discovery of a durable risk signature for neurological and psychiatric sequelae, including migraine (with and without aura), Alzheimer’s disease, dementia, and depression, is a critical and sobering finding. This observation positions influenza alongside other systemic inflammatory triggers implicated in neuro-inflammation and the acceleration of neurodegenerative processes. While the observational design cannot elucidate the precise pathophysiology, these associations lend strong support to hypotheses involving viral-induced breakdown of the blood-brain barrier, activation of central nervous system microglia, or persistent systemic inflammation promoting protein misfolding and neuronal injury. The prolonged risk horizon, extending over a decade, suggests that the initial viral insult can initiate a cascade of pathological events that unfolds over many years, contributing significantly to the population burden of cognitive decline and mental illness.
The broader landscape of post-acute sequelae, including new-onset type 2 diabetes and chronic kidney disease, solidifies the characterization of long flu as a multi-system disorder. This pattern of extrapulmonary organ injury is a defining feature of post-acute infection syndromes (PAIS), as established most prominently during the COVID-19 pandemic. Previous studies has shown that while both SARS-CoV-2 and influenza can lead to long-term health loss, they exhibit distinct organotrophic profiles, and SARS-CoV-2 exerts a more pronounced and widespread extrapulmonary toll.[8,35,36] Additionally, Type 2 diabetes were observed both in long flu and long COVID, which may be driven by mechanisms linked to chronic inflammation, insulin resistance, and other metabolic disruptions that are common to both post-infectious syndromes.[37] Comparatively, this study for influenza confirmed that its systemic impact is significant and warrants a holistic, multi-organ approach to post-infection surveillance and care.
The relationship between infectious and chronic diseases is increasingly recognized as being deeply interconnected, with infections playing a pivotal role in the onset and exacerbation of chronic conditions. Acute infections can act as triggers for long-term health problems, either by directly inducing organ damage or by initiating chronic inflammatory processes that persist long after the infection has resolved. Furthermore, individuals with pre-existing chronic conditions are often more susceptible to severe infections, creating a vicious cycle where chronic diseases exacerbate the severity of infections, while infections further impair long-term health. This bidirectional relationship underscores the need for a holistic approach to healthcare that considers the long-term implications of infections on chronic disease progression, emphasizing the importance of preventive measures such as vaccination and early interventions to break the cycle of disease exacerbation. Addressing this intersection could significantly reduce the global burden of both infectious and chronic diseases, improving long-term health outcomes across diverse populations.
4.1. Clinical and Public Health Implications
This study carries immediate and actionable implications for clinical practice and public health strategy. The identification of patients with pre-existing cardiometabolic and inflammatory conditions as a high-risk group for influenza provides a clear, evidence-based rationale for prioritizing and intensifying preventive measures. Chief among these is vaccination. Overwhelming evidence demonstrates that influenza vaccination significantly mitigates the risk of major adverse cardiovascular events, reduces hospitalizations for heart failure, and lowers mortality, particularly during periods of peak viral circulation.[38,39,40,41,42,43] Despite this, vaccine uptake remains distressingly suboptimal, even in high-risk populations within well-resourced health systems.[44] While vaccination reduces the risk of acute cardiovascular complications, the impact on long-term sequelae, particularly in the context of long flu or long COVID, requires further investigation.[5,45] Influenza vaccination may reduce the risk of myocardial infarction, stroke, and cardiovascular-related mortality, particularly among high-risk populations. A study involving approximately 9,000 adults revealed that individuals who received the influenza vaccine had a 34% lower likelihood of experiencing major cardiovascular events in the following year compared to those who did not receive the vaccine.[46] For individuals with recent cardiac events, the protective effect was even more pronounced, with a 45% reduction in the risk of severe cardiovascular outcomes.[46]
Accurately framing the influenza vaccine as a preventive tool for heart attacks and strokes may be pivotal in addressing the persistently low global vaccination rates. The World Health Organization has set a target of achieving 75% vaccination coverage among older adults and individuals with chronic health conditions. However, as of 2023, only 13 of 194 member states have met this target. This represents a critical, actionable gap in secondary prevention that must be addressed through targeted patient education, system-level interventions, and proactive engagement by cardiologists and primary care physicians alike, who must champion vaccination as a fundamental component of cardiovascular risk management.[47,48] By emphasizing the role of long flu, healthcare professionals can better communicate the substantial benefits of vaccination to the public.
4.2. Policy Attention and Prioritization of Long Flu
The advent of Long COVID has propelled a significant expansion in our understanding of the long-term sequelae of viral infections, prompting analogous investigations into the post-acute effects of influenza. Like Long COVID, long flu represents a multi-system disorder that manifests in a wide range of chronic health conditions, often extending far beyond the initial respiratory illness. These insights provide a crucial framework for understanding how influenza, like SARS-CoV-2, may trigger or accelerate the progression of chronic diseases such as heart failure, stroke, and neurodegenerative conditions. As with Long COVID, these complications are often under-recognized and poorly understood, leaving patients with a prolonged burden of disease that significantly impairs quality of life.
Moreover, the absence of a unified diagnostic and treatment framework for long flu, akin to the challenges observed in Long COVID care, underscores the need for urgent policy attention and research prioritization. Specifically, there is a pressing need for the development of robust diagnostic tools, effective therapeutic interventions, and comprehensive care pathways that address the multifaceted impacts of influenza beyond the acute phase. This call to action is further supported by the intersection of long flu and broader public health priorities, including vaccination strategies, healthcare infrastructure, and equitable access to care, which were similarly highlighted in the policy recommendations for Long COVID. Public health initiatives are needed to raise awareness about the potential long-term impacts of influenza, especially among healthcare providers and at-risk populations. Educating the public about the risk factors for long flu and the importance of vaccination can help reduce its prevalence and severity.
4.3. Limitations of This Study
While this study provides a comprehensive analysis of the long-term sequelae of influenza using the extensive FinnGen dataset, the strengths of this study—its population-scale, longitudinal design, and disease-wide scope—must be weighed against its inherent limitations. The observational framework precludes definitive causal inference; residual confounding from factors such as healthcare-seeking behaviors, socioeconomic status, or unmeasured lifestyle variables may influence the observed associations. While the analysis was adjusted for age and sex, the lack of data on additional important confounders—such as baseline comorbidities, vaccination status, socio-economic indicators, and behavioral factors (e.g., smoking, physical activity)—is a notable limitation. These variables could influence both the likelihood of influenza infection and the severity of post-influenza sequelae. Unfortunately, these data were not considered in this study. Therefore, while our findings provide valuable insights, they may be subject to residual confounding, and the conclusions drawn may not fully account for these unmeasured factors. We highlight this limitation and suggest that future studies should aim to incorporate these additional variables for more comprehensive risk assessments. Additionally, the reliance on clinical diagnosis codes from specialist care may not capture milder influenza cases managed in primary care, potentially selecting for a population with a higher baseline burden of disease.
Another limitation pertains to the observational nature of the study and the use of Cox proportional hazards models to assess the associations between influenza and long-term health outcomes. While these models are robust, they do not fully address potential biases inherent in the data, such as immortal-time bias or competing risks, which could affect the accuracy of the associations observed. Although we recognize the value of sensitivity analyses such as propensity score matching, competing risks models, and landmark analyses, these methods were not implemented due to the complexity of the cohort and the focus on maintaining statistical power.
5. Conclusions
In summary, this study provides a comprehensive, temporally resolved map of the multisystem disorders associated with influenza. The findings suggest that influenza is linked to a range of chronic diseases, with evidence of both pre-existing vulnerabilities and long-term post-acute effects, particularly in cardiovascular and neurological domains. While these associations are compelling, it is important to emphasize that the observational nature of the study does not allow for definitive causal conclusions. Nonetheless, the results highlight the potential for influenza to act as a trigger or exacerbating factor for long-term health consequences in susceptible individuals. This underscores the need for continued focus on preventive strategies, particularly through targeted vaccination of at-risk populations, and the development of integrated care pathways to address the multi-organ sequelae of influenza. Further research, including experimental studies, is needed to better understand the underlying mechanisms and to refine approaches for managing long-term outcomes associated with influenza.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Table S1: Comorbid conditions of influenza in this study.
Author Contributions
Conceptualization, M.Z.; methodology, M.Z.; software, M.Z.; validation, M.Z.; formal analysis, M.Z.; investigation, M.Z.; resources, M.Z.; data curation, M.Z.; writing—original draft preparation, M.Z.; writing—review and editing, M.Z.; visualization, M.Z.; supervision, M.Z.; project administration, M.Z.; funding acquisition, M.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This work is primarily supported by the Human Disease Continuum Project (HDCP) from M.Z.’s funds and resources, as well as the National Natural Science Foundation of China (grant number: 32100739). All funding sources have been disclosed, and no additional financial support was received for this study.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
No human subjects were directly involved in this study. This study was conducted using de-identified, summary-level data, which precluded any direct interaction with study participants. The overarching FinnGen study protocol has received ethical approval from the Coordinating Ethics Committee of the Hospital District of Helsinki and Uusimaa, Finland (statement number HUS/990/2017; 30 August 2017). All research activities were performed in strict accordance with national regulations and the ethical principles outlined in the Declaration of Helsinki. Due to the fully anonymized nature of the data, the requirement for individual informed consent was waived by the ethics committee.
Data Availability Statement
The data that support the findings of this study will be available from the corresponding author upon reasonable request.
Acknowledgments
I want to acknowledge the participants and investigators of the FinnGen study.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| DWAS | Disease-wide association study |
| WHO | World Health Organization |
| PIP | Pandemic Influenza Preparedness |
| CVD | Cardiovascular disease |
| HDCP | Human Disease Continuum Project |
References
- Palese, P. Influenza: old and new threats. Nat Med 2004, 10, S82–87. [Google Scholar] [CrossRef]
- WHO. Pandemic Influenza Preparedness Framework for the Sharing of Influenza Viruses and Access to Vaccines and Other Benefits. 2011. Available online: https://www.who.int/europe/groups/pandemic-influenza-preparedness-(pip)-framework.
- WHO. Pandemic influenza preparedness framework: partnership contribution high-level implementation plan III 2024-2030. Available online: https://www.who.int/publications/i/item/9789240070141.
- Maggi, S.; Andrew, M.K.; de Boer, A. Podcast: Influenza-Associated Complications and the Impact of Vaccination on Public Health. Infect Dis Ther 2024, 13, 413–420. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Sivan, M.; Perlowski, A.; Nikolich, J.Z. Long COVID: a clinical update. Lancet 2024, 404, 707–724. [Google Scholar] [CrossRef]
- Cai, M.; Xie, Y.; Topol, E.J.; Al-Aly, Z. Three-year outcomes of post-acute sequelae of COVID-19. Nat Med 2024, 30, 1564–1573. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Bowe, B.; Maddukuri, G.; Al-Aly, Z. Comparative evaluation of clinical manifestations and risk of death in patients admitted to hospital with covid-19 and seasonal influenza: cohort study. BMJ 2020, 371, m4677. [Google Scholar] [CrossRef]
- Xie, Y.; Choi, T.; Al-Aly, Z. Long-term outcomes following hospital admission for COVID-19 versus seasonal influenza: a cohort study. Lancet Infect Dis 2024, 24, 239–255. [Google Scholar] [CrossRef]
- LUCKE, B.; WIGHT, T.; KIME, E. Pathologic anatomy and bacteriology of influenza: Epidemic of autumn, 1918. Archives of Internal Medicine 1919, 24, 154–237. [Google Scholar] [CrossRef]
- Oseasohn, R.; Adelson, L.; Kaji, M. Clinicopathologic Study of Thirty-Three Fatal Cases of Asian Influenza. New England Journal of Medicine 1959, 260, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Paddock, C.D.; Liu, L.; Denison, A.M.; Bartlett, J.H.; Holman, R.C.; Deleon-Carnes, M.; Emery, S.L.; Drew, C.P.; Shieh, W.J.; Uyeki, T.M.; et al. Myocardial injury and bacterial pneumonia contribute to the pathogenesis of fatal influenza B virus infection. J Infect Dis 2012, 205, 895–905. [Google Scholar] [CrossRef]
- Kodama, M. Influenza myocarditis. Circ J 2010, 74, 2060–2061. [Google Scholar] [CrossRef] [PubMed]
- Chaves, S.S.; Nealon, J.; Burkart, K.G.; Modin, D.; Biering-Sorensen, T.; Ortiz, J.R.; Vilchis-Tella, V.M.; Wallace, L.E.; Roth, G.; Mahe, C.; et al. Global, regional and national estimates of influenza-attributable ischemic heart disease mortality. EClinicalMedicine 2023, 55, 101740. [Google Scholar] [CrossRef]
- Boehme, A.K.; Luna, J.; Kulick, E.R.; Kamel, H.; Elkind, M.S.V. Influenza-like illness as a trigger for ischemic stroke. Ann Clin Transl Neurol 2018, 5, 456–463. [Google Scholar] [CrossRef]
- Skaarup, K.G.; Modin, D.; Nielsen, L.; Jensen, J.U.S.; Biering-Sorensen, T. Influenza and cardiovascular disease pathophysiology: strings attached. Eur Heart J Suppl 2023, 25, A5–A11. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.J.; Rolfes, M.A.; O’Halloran, A.; Anderson, E.J.; Bennett, N.M.; Billing, L.; Chai, S.; Dufort, E.; Herlihy, R.; Kim, S.; et al. Acute Cardiovascular Events Associated With Influenza in Hospitalized Adults: A Cross-sectional Study. Ann Intern Med 2020, 173, 605–613. [Google Scholar] [CrossRef]
- Bolton, A.; Thyagaturu, H.; Ashraf, M.; Carnahan, R.; Hodgson-Zingman, D. Effects of atrial fibrillation on outcomes of influenza hospitalization. Int J Cardiol Heart Vasc 2022, 42, 101106. [Google Scholar] [CrossRef]
- Clayton, T.C.; Thompson, M.; Meade, T.W. Recent respiratory infection and risk of cardiovascular disease: case-control study through a general practice database. Eur Heart J 2008, 29, 96–103. [Google Scholar] [CrossRef]
- Warren-Gash, C.; Smeeth, L.; Hayward, A.C. Influenza as a trigger for acute myocardial infarction or death from cardiovascular disease: a systematic review. Lancet Infect Dis 2009, 9, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Guan, X.; Yang, W.; Sun, X.; Wang, L.; Ma, B.; Li, H.; Zhou, J. Association of influenza virus infection and inflammatory cytokines with acute myocardial infarction. Inflamm Res 2012, 61, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Kwong, J.C.; Schwartz, K.L.; Campitelli, M.A.; Chung, H.; Crowcroft, N.S.; Karnauchow, T.; Katz, K.; Ko, D.T.; McGeer, A.J.; McNally, D.; et al. Acute Myocardial Infarction after Laboratory-Confirmed Influenza Infection. N Engl J Med 2018, 378, 345–353. [Google Scholar] [CrossRef]
- de Boer, A.R.; Riezebos-Brilman, A.; van Hout, D.; van Mourik, M.S.M.; Rumke, L.W.; de Hoog, M.L.A.; Vaartjes, I.; Bruijning-Verhagen, P. Influenza Infection and Acute Myocardial Infarction. NEJM Evid 2024, 3, EVIDoa2300361. [Google Scholar] [CrossRef]
- Kenney, A.D.; Aron, S.L.; Gilbert, C.; Kumar, N.; Chen, P.; Eddy, A.; Zhang, L.; Zani, A.; Vargas-Maldonado, N.; Speaks, S.; et al. Influenza virus replication in cardiomyocytes drives heart dysfunction and fibrosis. Sci Adv 2022, 8, eabm5371. [Google Scholar] [CrossRef]
- Veronese, N.; Demurtas, J.; Smith, L.; Michel, J.P.; Barbagallo, M.; Bolzetta, F.; Noale, M.; Maggi, S. Influenza vaccination reduces dementia risk: A systematic review and meta-analysis. Ageing Res Rev 2022, 73, 101534. [Google Scholar] [CrossRef]
- Zhao, H.; Zhou, X.; Fu, K.; Duan, Y.; Wen, Q.; Wang, S.; Zhan, S. Prospective cohort study evaluating the association between influenza vaccination and neurodegenerative diseases. NPJ Vaccines 2024, 9, 51. [Google Scholar] [CrossRef]
- Bukhbinder, A.S.; Ling, Y.; Hasan, O.; Jiang, X.; Kim, Y.; Phelps, K.N.; Schmandt, R.E.; Amran, A.; Coburn, R.; Ramesh, S.; et al. Risk of Alzheimer’s Disease Following Influenza Vaccination: A Claims-Based Cohort Study Using Propensity Score Matching. J Alzheimers Dis 2022, 88, 1061–1074. [Google Scholar] [CrossRef]
- Zheng, M.; Lavie, C.J. Landscape of stroke comorbidities: A disease-wide association study. Prog Cardiovasc Dis 2024, 86, 96–99. [Google Scholar] [CrossRef]
- Zheng, M. Disease-wide association study uncovers disease continuum network of unipolar depression. European Neuropsychopharmacology 2025, 92, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M. Disease continuum centered on Parkinson’s disease. European Neuropsychopharmacology 2025, 93, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M. Snapshot of disease continuum centered on Alzheimer’s disease: Exploring modifiable risk factors. Prog Neuropsychopharmacol Biol Psychiatry 2025, 138, 111316. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M. Thinking bipolar disorder as a symptom rather than a disease. Asian journal of psychiatry 2025, 109, 104540. [Google Scholar] [CrossRef]
- Kurki, M.I.; Karjalainen, J.; Palta, P.; Sipila, T.P.; Kristiansson, K.; Donner, K.M.; Reeve, M.P.; Laivuori, H.; Aavikko, M.; Kaunisto, M.A.; et al. FinnGen provides genetic insights from a well-phenotyped isolated population. Nature 2023, 613, 508–518. [Google Scholar] [CrossRef]
- Plana-Ripoll, O.; Pedersen, C.B.; Holtz, Y.; Benros, M.E.; Dalsgaard, S.; de Jonge, P.; Fan, C.C.; Degenhardt, L.; Ganna, A.; Greve, A.N.; et al. Exploring Comorbidity Within Mental Disorders Among a Danish National Population. JAMA Psychiatry 2019, 76, 259–270. [Google Scholar] [CrossRef]
- Frobert, O.; Pedersen, I.B.; Hjelholt, A.J.; Erikstrup, C.; Cajander, S. The flu shot and cardiovascular Protection: Rethinking inflammation in ischemic heart disease. Atherosclerosis 2025, 120405. [Google Scholar] [CrossRef]
- Zheng, M.; Lavie, C.J. COVID-19 susceptibility causally related to stroke risk: Using SARS-CoV-2 infection as a natural test of disease predisposition? Prog Cardiovasc Dis 2024, 86, 89–92. [Google Scholar] [CrossRef]
- Zheng, M. COVID-19 Predisposition Inherently Increases Cardiovascular Risk Before SARS-CoV-2 Infection. Cardiovasc Toxicol 2025, 25, 821–829. [Google Scholar] [CrossRef]
- Miller, M.G.; Terebuh, P.; Kaelber, D.C.; Xu, R.; Davis, P.B. SARS-CoV-2 Infection and New-Onset Type 2 Diabetes Among Pediatric Patients, 2020 to 2022. JAMA Netw Open 2024, 7, e2439444. [Google Scholar] [CrossRef] [PubMed]
- DiazGranados, C.A.; Robertson, C.A.; Talbot, H.K.; Landolfi, V.; Dunning, A.J.; Greenberg, D.P. Prevention of serious events in adults 65 years of age or older: A comparison between high-dose and standard-dose inactivated influenza vaccines. Vaccine 2015, 33, 4988–4993. [Google Scholar] [CrossRef]
- Frobert, O.; Gotberg, M.; Angeras, O.; Jonasson, L.; Erlinge, D.; Engstrom, T.; Persson, J.; Jensen, S.E.; Omerovic, E.; James, S.K.; et al. Design and rationale for the Influenza vaccination After Myocardial Infarction (IAMI) trial. A registry-based randomized clinical trial. Am Heart J 2017, 189, 94–102. [Google Scholar] [CrossRef]
- Lee, J.K.H.; Lam, G.K.L.; Shin, T.; Kim, J.; Krishnan, A.; Greenberg, D.P.; Chit, A. Efficacy and effectiveness of high-dose versus standard-dose influenza vaccination for older adults: a systematic review and meta-analysis. Expert Rev Vaccines 2018, 17, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Loeb, M.; Dokainish, H.; Dans, A.; Palileo-Villanueva, L.M.; Roy, A.; Karaye, K.; Zhu, J.; Liang, Y.; Goma, F.; Damasceno, A.; et al. Randomized controlled trial of influenza vaccine in patients with heart failure to reduce adverse vascular events (IVVE): Rationale and design. Am Heart J 2019, 212, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Gonuguntla, K.; Patil, S.P.; Rojulpote, C. Impact of influenza and pneumococcal vaccines upon in-hospital mortality in patients with heart failure: a retrospective cohort study in the United States. European Heart Journal 2020, 41. [Google Scholar] [CrossRef]
- Loeb, M.; Roy, A.; Dokainish, H.; Dans, A.; Palileo-Villanueva, L.M.; Karaye, K.; Zhu, J.; Liang, Y.; Goma, F.; Damasceno, A.; et al. Influenza vaccine to reduce adverse vascular events in patients with heart failure: a multinational randomised, double-blind, placebo-controlled trial. Lancet Glob Health 2022, 10, e1835–e1844. [Google Scholar] [CrossRef] [PubMed]
- Dermenchyan, A.; Choi, K.R.; Bokhoor, P.R.; Cho, D.J.; Delavin, N.L.A.; Chima-Melton, C.; Han, M.A.; Fonarow, G.C. Receipt of respiratory vaccines among patients with heart failure in a multicenter health system registry. Vaccine 2025, 46, 126682. [Google Scholar] [CrossRef]
- Xie, Y.; Choi, T.; Al-Aly, Z. Postacute Sequelae of SARS-CoV-2 Infection in the Pre-Delta, Delta, and Omicron Eras. N Engl J Med 2024, 391, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Behrouzi, B.; Bhatt, D.L.; Cannon, C.P.; Vardeny, O.; Lee, D.S.; Solomon, S.D.; Udell, J.A. Association of Influenza Vaccination With Cardiovascular Risk: A Meta-analysis. JAMA Netw Open 2022, 5, e228873. [Google Scholar] [CrossRef] [PubMed]
- Belongia, E.A.; Simpson, M.D.; King, J.P.; Sundaram, M.E.; Kelley, N.S.; Osterholm, M.T.; McLean, H.Q. Variable influenza vaccine effectiveness by subtype: a systematic review and meta-analysis of test-negative design studies. Lancet Infect Dis 2016, 16, 942–951. [Google Scholar] [CrossRef]
- Infections, G.B.D.L.R.; Antimicrobial Resistance, C. Global, regional, and national incidence and mortality burden of non-COVID-19 lower respiratory infections and aetiologies, 1990-2021: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Infect Dis 2024, 24, 974–1002. [Google Scholar] [CrossRef]
Figure 1.
Framework Overview of the Disease-Wide Association Study (DWAS) Approach. This diagram illustrates the methodological framework used to investigate the longitudinal associations of influenza across the Human Disease Continuum (HDC). The Disease-Wide Association Study (DWAS) approach systematically analyzes the entire spectrum of disease diagnoses (pre- and post-influenza) to identify statistically significant disease-disease relationships. The framework explicitly links the large-scale data sources, the time-stratified cohort definitions, and the statistical modeling pipeline (Cox proportional hazards regression) essential for distinguishing pre-existing risk factors from potential sequelae of acute influenza infection. This approach provides a rigorous platform for mapping the complete clinical trajectory of patients with a history of influenza.
Figure 1.
Framework Overview of the Disease-Wide Association Study (DWAS) Approach. This diagram illustrates the methodological framework used to investigate the longitudinal associations of influenza across the Human Disease Continuum (HDC). The Disease-Wide Association Study (DWAS) approach systematically analyzes the entire spectrum of disease diagnoses (pre- and post-influenza) to identify statistically significant disease-disease relationships. The framework explicitly links the large-scale data sources, the time-stratified cohort definitions, and the statistical modeling pipeline (Cox proportional hazards regression) essential for distinguishing pre-existing risk factors from potential sequelae of acute influenza infection. This approach provides a rigorous platform for mapping the complete clinical trajectory of patients with a history of influenza.
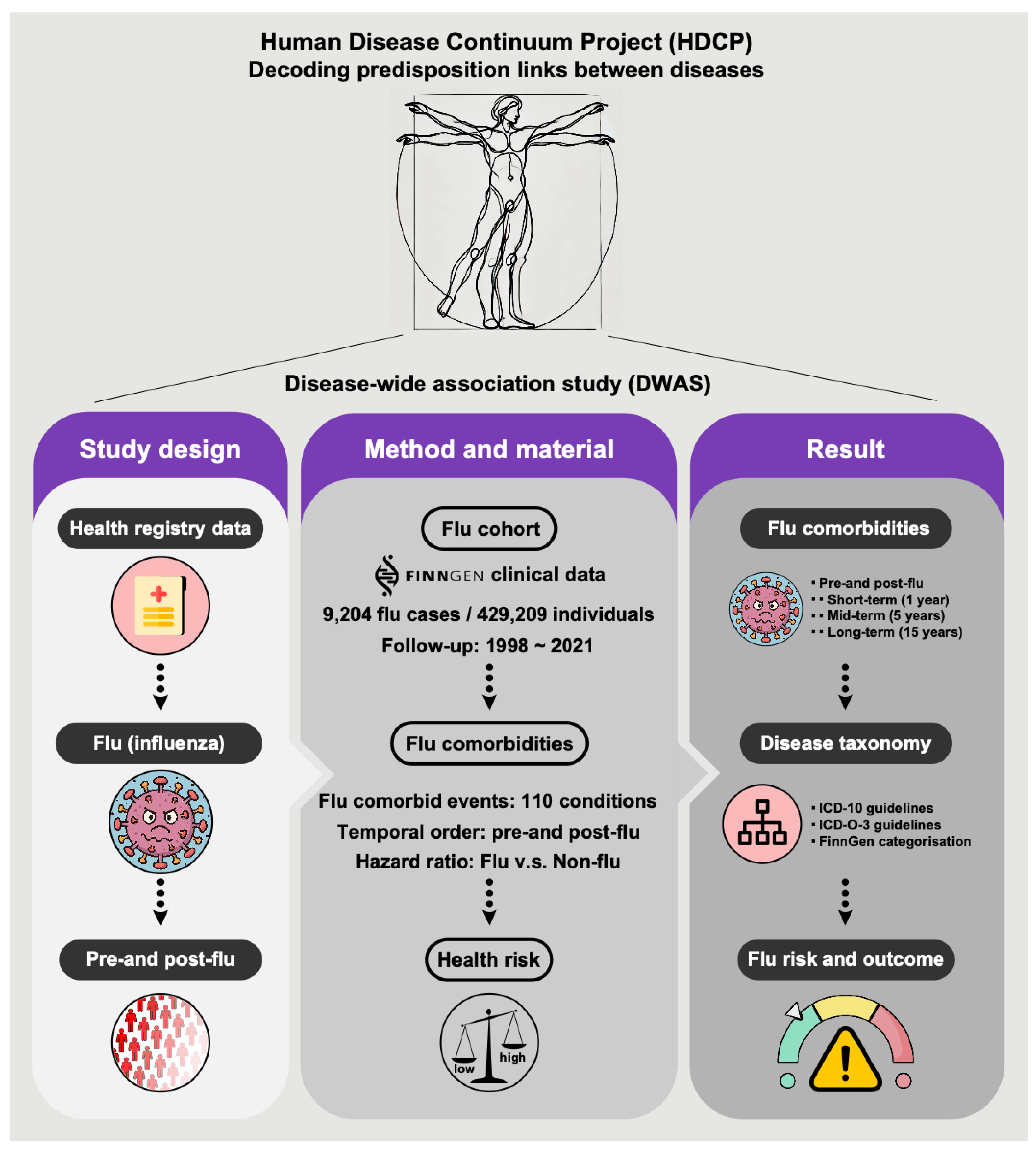
Figure 2.
Temporal and Taxonomic Distribution of Influenza-Associated Comorbidities. Temporal classification and taxonomic distribution of medical comorbidities significantly associated with influenza. This bar chart quantifies the number of distinct International Classification of Diseases (ICD)-based disease entities demonstrating a significant association with influenza across defined longitudinal windows. The data is stratified into panels based on the analysis window (e.g., 1, 5, or 15 years) and categorized as conditions diagnosed pre-influenza (potential risk factors) or post-influenza (potential long-term sequelae). Statistical significance for all associations was determined using Cox proportional hazards regression models, adjusted for key confounders including age and sex, with a stringent threshold set at an FDR-adjusted p-value <0.001. Comorbidity groups are categorized according to standardized classifications (ICD-10, ICD-O-3, and FinnGen), providing a standardized, multi-system perspective on the temporal relationship between influenza and subsequent or antecedent disease burden.
Figure 2.
Temporal and Taxonomic Distribution of Influenza-Associated Comorbidities. Temporal classification and taxonomic distribution of medical comorbidities significantly associated with influenza. This bar chart quantifies the number of distinct International Classification of Diseases (ICD)-based disease entities demonstrating a significant association with influenza across defined longitudinal windows. The data is stratified into panels based on the analysis window (e.g., 1, 5, or 15 years) and categorized as conditions diagnosed pre-influenza (potential risk factors) or post-influenza (potential long-term sequelae). Statistical significance for all associations was determined using Cox proportional hazards regression models, adjusted for key confounders including age and sex, with a stringent threshold set at an FDR-adjusted p-value <0.001. Comorbidity groups are categorized according to standardized classifications (ICD-10, ICD-O-3, and FinnGen), providing a standardized, multi-system perspective on the temporal relationship between influenza and subsequent or antecedent disease burden.
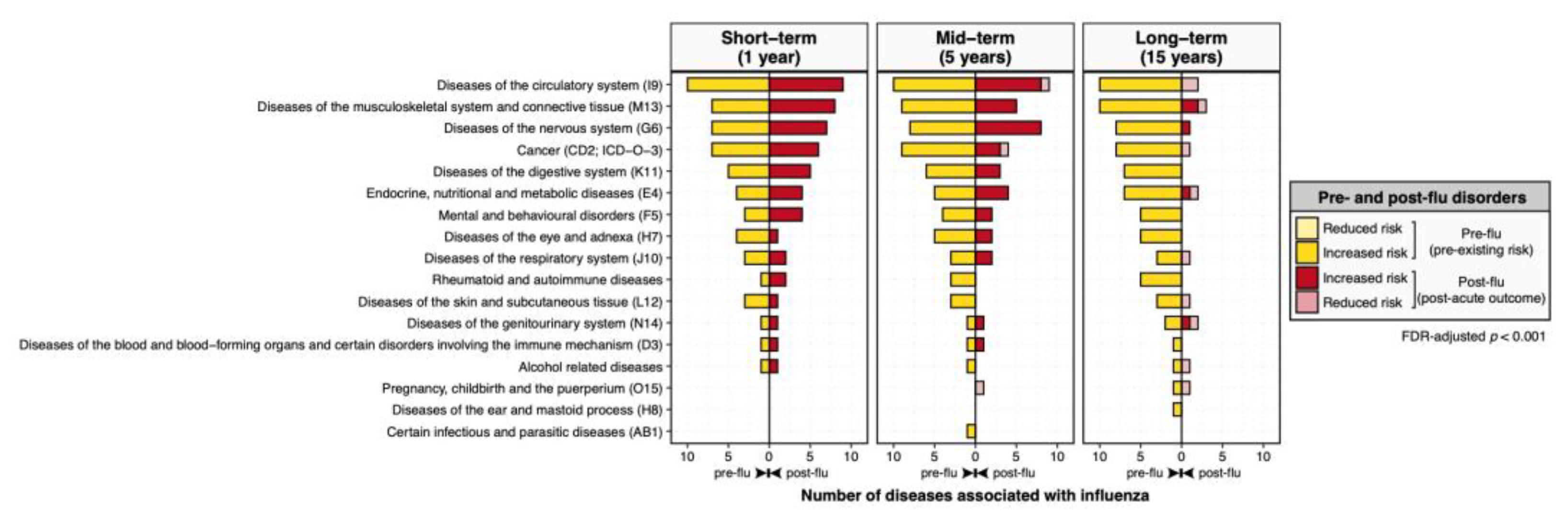
Figure 3.
Hazard Ratio Plot of the Disease-Wide Association of Influenza on Multi-organ Systems. Hazard ratio plot detailing the system-specific associations of influenza. This figure presents the Hazard Ratios (HRs), calculated via Cox proportional hazards regression models (adjusted for age and sex), for the full spectrum of disease associations identified in the DWAS. The plot visually ranks the magnitude and directionality of the association, with the HR>1 indicating an increased risk and HR<1 indicating a decreased risk. Error bars represent the 95% confidence intervals. This system-focused view exemplifies how the DWAS approach can precisely map which specific comorbidities are most strongly or weakly correlated with influenza.
Figure 3.
Hazard Ratio Plot of the Disease-Wide Association of Influenza on Multi-organ Systems. Hazard ratio plot detailing the system-specific associations of influenza. This figure presents the Hazard Ratios (HRs), calculated via Cox proportional hazards regression models (adjusted for age and sex), for the full spectrum of disease associations identified in the DWAS. The plot visually ranks the magnitude and directionality of the association, with the HR>1 indicating an increased risk and HR<1 indicating a decreased risk. Error bars represent the 95% confidence intervals. This system-focused view exemplifies how the DWAS approach can precisely map which specific comorbidities are most strongly or weakly correlated with influenza.
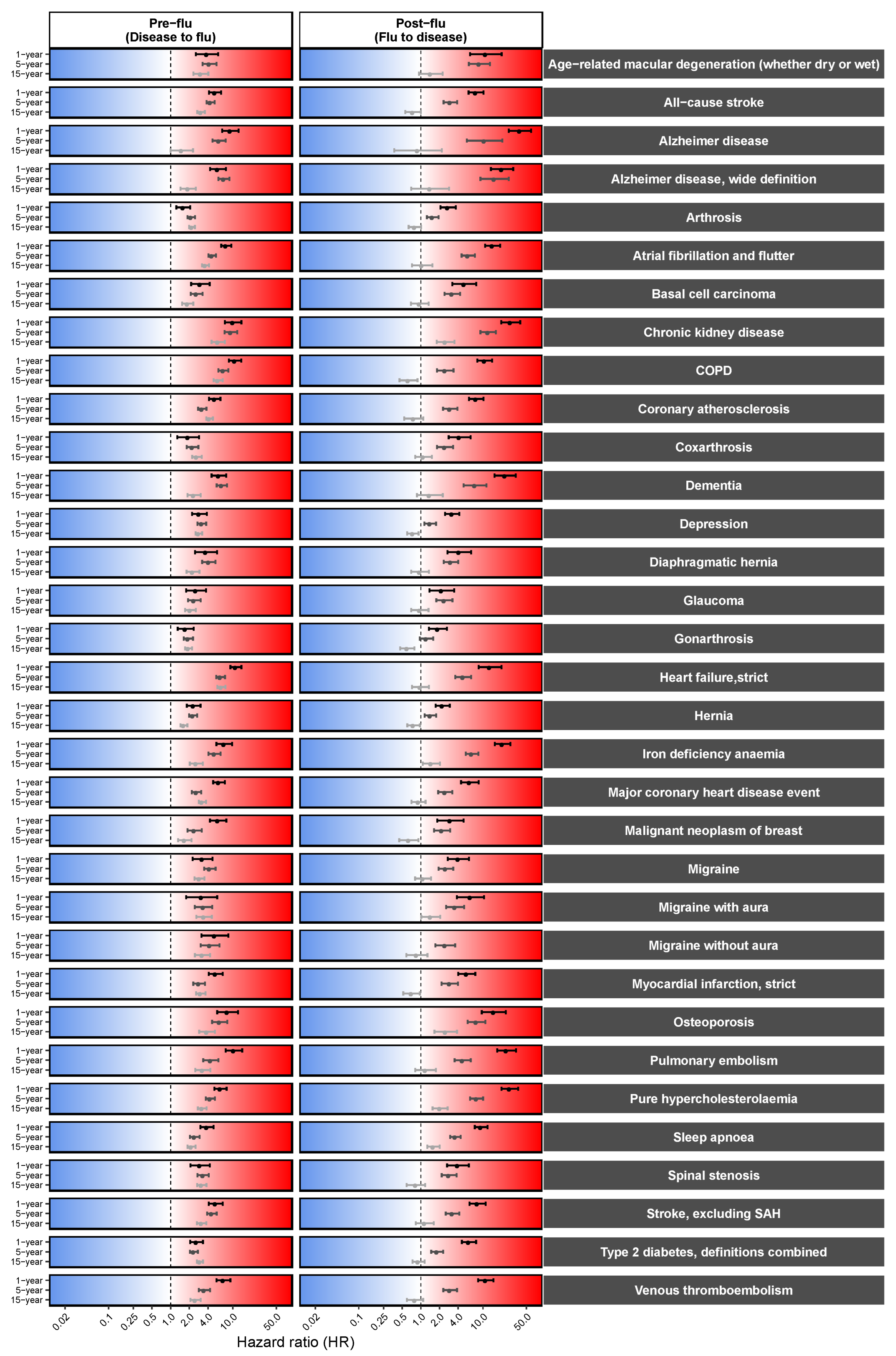
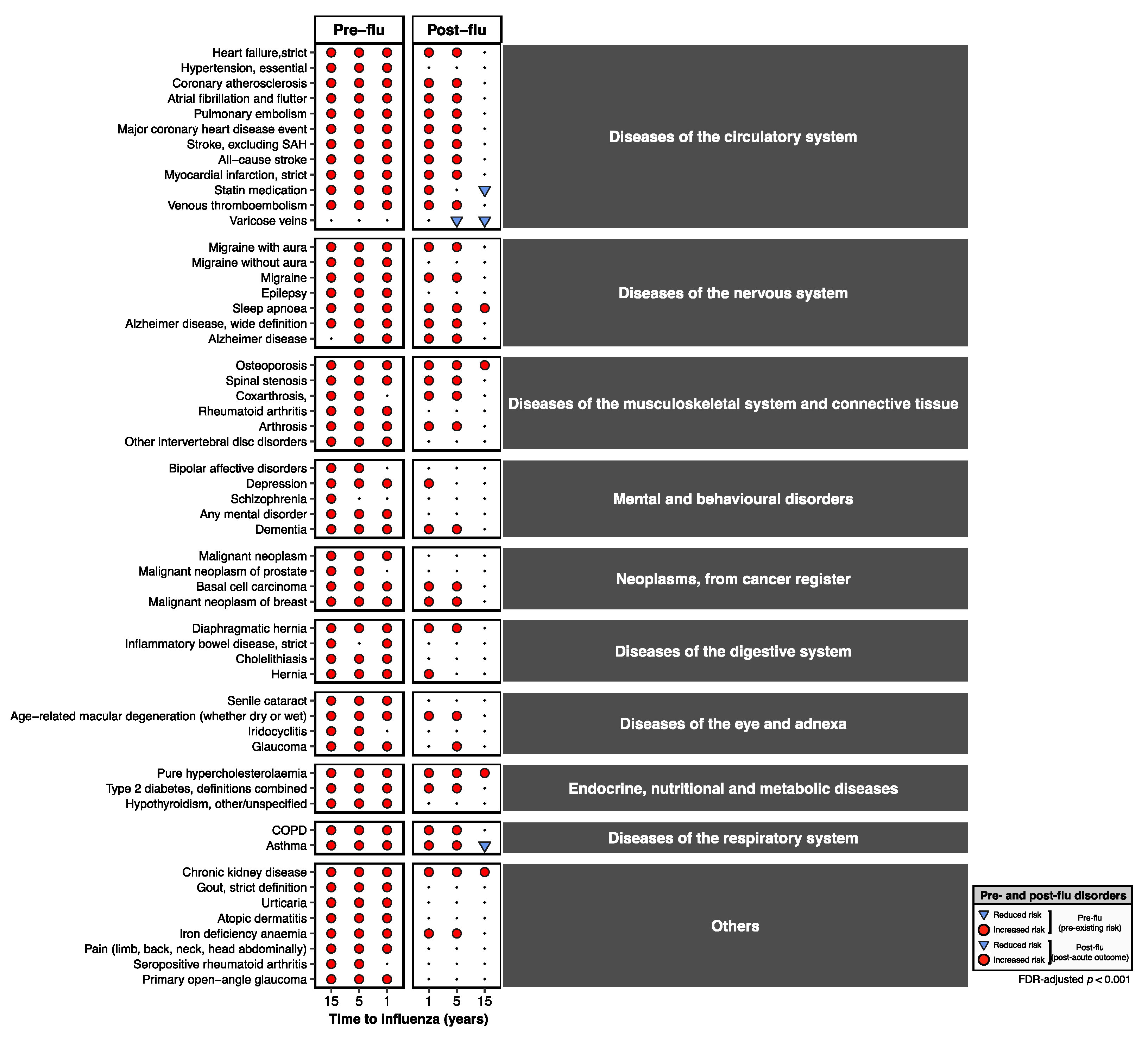
Figure 4.
Comprehensive Heatmap of Longitudinal Disease-Wide Associations (DWAS) with Influenza. Comprehensive heatmap summarizing the most significant longitudinal disease associations identified by the DWAS framework. The display is restricted to associations meeting stringent statistical and clinical criteria: FDR-adjusted p-value <0.001, a substantial magnitude (Hazard Ratio >2 or <0.5), and sufficient clinical relevance (disease prevalence >0.5%). The temporal categorization into pre-influenza (antecedent) and post-influenza (sequelae) comorbidities is highlighted along the vertical axis. The shape of each data point denotes the directionality of the association (e.g., circle for increased risk, triangle for reduced risk), while the color/intensity can represent the magnitude of the HR or the significance level. This heatmap underscores the central hypothesis that influenza is not an isolated event but rather a catalyst or marker within a broader disease predisposition continuum, impacting multiple organ systems as classified by ICD-10, ICD-O-3, and FinnGen taxonomies.
Figure 4.
Comprehensive Heatmap of Longitudinal Disease-Wide Associations (DWAS) with Influenza. Comprehensive heatmap summarizing the most significant longitudinal disease associations identified by the DWAS framework. The display is restricted to associations meeting stringent statistical and clinical criteria: FDR-adjusted p-value <0.001, a substantial magnitude (Hazard Ratio >2 or <0.5), and sufficient clinical relevance (disease prevalence >0.5%). The temporal categorization into pre-influenza (antecedent) and post-influenza (sequelae) comorbidities is highlighted along the vertical axis. The shape of each data point denotes the directionality of the association (e.g., circle for increased risk, triangle for reduced risk), while the color/intensity can represent the magnitude of the HR or the significance level. This heatmap underscores the central hypothesis that influenza is not an isolated event but rather a catalyst or marker within a broader disease predisposition continuum, impacting multiple organ systems as classified by ICD-10, ICD-O-3, and FinnGen taxonomies.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



