Submitted:
02 January 2026
Posted:
06 January 2026
You are already at the latest version
Abstract
Background: Dementia and Type 2 diabetes (T2D) represent two of the most pressing global public health challenges of our time, both exacerbated by physical inactivity. These conditions disproportionately affect Global Majority populations, who experience earlier onset, higher prevalence, and poorer access to culturally appropriate preventive care. However, conventional research and interventions often overlook the sociocultural and structural factors that underpin this disparity. This study synthesises current evidence to understand how these three conditions intersect and to identify equitable pathways for prevention and support. Methods: A meta-narrative review approach was employed, guided by the framework of Greenhalgh et al. (2005), to integrate evidence from diverse research traditions. Databases including MEDLINE, CINAHL, PsycINFO, and Web of Science were searched. Five meta-narratives were identified: biomedical and epidemiological, public health, health disparities, sociocultural and behavioural, and intervention science. Cross-narrative synthesis produced a conceptual framework linking upstream determinants, lifestyle factors, and disease outcomes. Results: The review revealed that structural inequities such as deprivation, environmental barriers and sociocultural factors including stigma, gendered norms, limited access to culturally appropriate facilities that restrict physical activity (PA) opportunities within Global Majority communities. These constraints elevate T2D and dementia risk through biological pathways involving insulin resistance, vascular injury, and neuroinflammation. Community-based participatory research (CBPR) interventions particularly those delivered in trusted cultural, or faith settings emerged as effective strategies to improve PA, glycaemic control, and cognitive wellbeing. Conclusion: This synthesis reframes dementia and diabetes as interlinked within a wider syndemic driven by structural and sociocultural inequities. The proposed framework underscores the importance of culturally grounded, community-led approaches to promote brain health, reduce risk, and achieve equitable healthy ageing among Global Majority populations.
Keywords:
dementia
; diabetes
; physical inactivity
; global majority populations
; community-based participatory research
Introduction
The world is undergoing a profound demographic shift. Global populations are experiencing an unprecedented ageing trend, a phenomenon marked by a substantial rise in proportion of older individuals within society. It is projected that by 2030, one-sixth of the world’s population will be 60 years of age or older, a figure expected to grow from 1 billion in 2020 to 2.1 billion by 2050 (World Health Organization, 2022). While increased longevity is a testament to public health successes, these gains are often marred by a longer period spent in poor health. For instance, in the United Kingdom (UK) an average man lives around 16 years and women nearly 22 years with disability (Nursing Times, 2023). This extension of morbidity is largely driven by a global epidemic of non-communicable diseases (NCDs), which places an immense and growing burden on healthcare systems, economies, and societies at large.
Among the most challenging of these NCDs are dementia and diabetes. These are not merely parallel crises but are deeply interconnected, creating a complex public health challenge that demands a nuanced and integrated response. The task of tackling the difficulties presented by the simultaneous presence of ageing and chronic illnesses has therefore emerged as a crucial area of interest for healthcare professionals, policymakers, and scholars on a global scale (Jones et al., 2024).
Dementia and Diabetes
Dementia is a rapidly growing public health concern with devastating social and economic implications. Characterised by a progressive decline in cognitive function beyond what might be expected from normal ageing, it compromises memory, thinking, orientation, comprehension, and judgment. Currently estimated to affect 50 million people globally, this figure is projected to triple to 150 million by 2050 (Alzheimer’s Association, 2023). The urgency of this crisis is profoundly amplified by a stark clinical reality: there are currently no medical or pharmaceutical interventions that can halt or reverse the progression of common dementias such as Alzheimer’s disease (Annear et al., 2015). This therapeutic impasse places an enormous emphasis on prevention and risk reduction as the most powerful tools available.
Concurrently, diabetes, particularly Type 2 Diabetes (T2D), has reached epidemic. The global prevalence of diabetes in 2017 was estimated at 451 million individuals and is projected to rise to 693 million by 2045 without effective preventive action (Cho et al., 2018). The condition is a major driver of mortality and morbidity, linked to elevated rates of cardiovascular disease (CVD), stroke, kidney disease, and cancer (Dixon et al., 2024; He et al., 2025). A compelling and concerning body of evidence established a detrimental synergy between these two conditions. A meta-analysis by Cole et al. (2007) found that T2D confers a two- to three-fold higher risk of developing dementia. This is further attested by recent research suggesting that diabetes is linked with an enhanced risk of dementia (Olesen et al., 2025). This neurometabolic link creates a “double dilemma” for patients and clinicians (Hill, 2019). Not only does diabetes elevate dementia risk, but the cognitive impairments associated with dementia can severely compromise a patient’s ability to self-manage their diabetes. This can lead to missed medications, poor glucose monitoring, dietary indiscretions, and an increased risk of dangerous hypoglycemic or hyperglycemic events, further accelerating a downward spiral of health (Hill, 2019; Meneilly et al., 2016).
Dementia, Diabetes and Physical Activity (DDPA)
Amidst this complex interplay of chronic diseases, a third factor emerges as critically important: physical inactivity. Ranked by the World Health Organization as the fourth leading risk factor for global mortality costing five million lives annually (WHO, 2024), physical inactivity is a powerful driver of NCDs. Its role in the context of dementia and diabetes is particularly significant. Previous research has identified physical inactivity as one of the key modifiable risk factors for Alzheimer’s disease (Tang et al., 2025; Jones et al., 2024; Norton et al., 2014). These findings underscore the huge potential for prevention.
Engaging in regular PA is a cornerstone of both preventing and managing T2D and its complications. Physiologically, engaging in regular PA/exercise can improve glycemic control by enhancing insulin sensitivity in muscle and liver tissues and promoting glucose uptake (Piras & Raffi, 2023). Beyond blood sugar regulation, the benefits include improved lipid profiles, lower blood pressure, and weight management, all of which mitigate CVD risk. In the context of brain health, PA is a potent non-pharmacological intervention. It is believed to protect the brain by reducing neuroinflammation, combating oxidative stress, maintaining good blood flow, and promoting neurogenesis the growth of new neurons (Gronek et al., 2019; Dementia Australia). Given the lack of curative treatments for dementia, PA represents one of the promising strategies for mitigating cognitive decline and preserving functional independence.
DDPA in Global Majority Groups
The burden of dementia, diabetes, and physical inactivity is not distributed equally across populations. In the UK and other Western nations, Global Majority populations often referred to as Black, Asian, and Minority Ethnic (BAME) communities experience a profound and disproportionate impact. In the UK, the number of people from these communities living with dementia is projected to increase by 600% between 2011 and 2051, a rate of growth far exceeding that of the White British population (All-Party Parliamentary Group on Dementia, 2013).
This disparity is driven by a convergence of risk factors. People of South Asian, Black African, and African Caribbean descent are at a significantly higher risk of developing T2D, and at a much younger age (e.g., from 25 years old) compared to 40 for the White population (Johnson, 2022). This heightened biological susceptibility, potentially linked to genetic predispositions and patterns of visceral fat storage (Gujral et al., 2013; Johnson, 2022), is dangerously amplified by behavioural and social factors. Data consistently shows that people from Asian and Black backgrounds are far more likely to be physically inactive than their White counterparts (Public Health Walsall, 2015; Smith, 2020).
These disparities are further compounded by systemic and cultural barriers to care. People from Global Majority communities are less likely to receive a timely dementia diagnosis and are less likely to engage with dementia support services (Alzheimer’s Society, 2023). This can be due to a range of factors, including stigma, lack of culturally or linguistically appropriate terminology for dementia, and cultural perceptions around caregiving that discourage seeking external help (Alzheimer’s Society, 2023). As highlighted by Kaufman and Perales-Puchalt (2023), this is not simply a collection of separate risk factors but a “syndemic” a clustering of interconnected diseases (dementia, diabetes) driven and exacerbated by the social, economic, and environmental inequities that shape people’s lives.
Rationale of this Narrative Review
Despite the clear evidence of a syndemic of dementia, diabetes, and physical inactivity in Global Majority populations, public health research and interventions have often failed to adequately address the issue. Much of the research on modifiable dementia risk factors has been conducted in predominantly White populations, and the unique risk profiles and sociocultural contexts of diverse communities remain poorly understood. While seven key modifiable risk factors for dementia have been identified—including physical inactivity, diabetes, midlife obesity, and hypertension but their specific impact and interplay within British South Asian and other minority communities have not been sufficiently investigated.
This review is predicated on the understanding that effective and equitable public health strategies cannot be developed without a deep appreciation of this complexity. A one-size-fits-all approach that ignores cultural norms, structural barriers, and the lived experiences of diverse communities is destined to fail. This suggests for urgent need to synthesise the existing, albeit fragmented, evidence from across disciplines including biomedicine, public health, sociology, and behavioural science to build a more holistic picture and approaches. By weaving together these different “storylines” of research, we can better understand the multifaceted nature of the problem and identify promising pathways for intervention. Therefore, the aim of this review is to address the gap by examining, intersection of dementia, diabetes, and PA through the lens of health, culture and care, with a specific focus on the disparities faced by Global Majority populations.
Research Aim
To narratively review and synthesise current literature exploring the intersections of dementia, diabetes, and physical inactivity, with a focus on understanding the health, cultural, and care perspectives that shape disparities across diverse populations.
Research Objective
To narratively analyse and integrate existing literature from multiple research traditions to gain insight into the biomedical links, behavioural drivers, sociocultural contexts, and systemic barriers surrounding dementia, diabetes, and physical inactivity, with a particular consideration for Global Majority populations.
Research Question
What are the key findings, theoretical frameworks, and evidence gaps across different research narratives regarding the intersectionality of dementia, diabetes, and physical inactivity, and how can this synthesised understanding inform the development of equitable and culturally competent public health recommendations?
Methodological Approach: Meta-Narrative Review
This study was conducted as a meta-narrative review, a method specifically designed for synthesising complex and heterogeneous bodies of evidence (Greenhalgh et al., 2005). This approach is distinct from a traditional systematic review, which typically seeks to aggregate findings from methodologically similar studies to answer a narrow question. Instead, a meta-narrative review aims to understand a broad topic by mapping the “storylines” of different research traditions, illuminating how each tradition has framed the problem, the theories it employs, and the evidence it has generated. This approach is particularly well-suited to the current research question, which requires integrating insights from fields as diverse as epidemiology, physiology, behavioural psychology, and medical sociology.
The review process was guided by the six key principles and phases outlined by Greenhalgh et al. (2005):
- Planning: Defining the research scope and assembling a multidisciplinary team to guide the review.
- Searching: An iterative process of searching electronic databases. An initial strategy focused narrowly on the intersection of all three topics within Global Majority groups. However, due to the limited literature, the search was broadened to capture key research within each “storyline” separately, which could then be synthesised. Key search terms included combinations of (“dementia” OR “Alzheimer’s disease”), (“diabetes” OR “type 2 diabetes”), and (“physical inactivity” OR “sedentary behaviour”). Databases included CINAHL, MEDLINE, PsycINFO, AMED, ASSIA, Cochrane Library, and Web of Science. Seminal works and grey literature (e.g., reports from public health bodies) were also included.
- Mapping: Identifying the key meta-narratives or research traditions apparent in the literature. For this review, these included: (a) the biomedical/epidemiological narrative, (b) the public health/preventive medicine narrative, (c) the health disparities/sociological narrative, (d) the behavioural science narrative, and (e) the intervention science narrative.
- Appraisal: Critically appraising the literature within each tradition, not to exclude studies based on a rigid quality hierarchy, but to understand the strengths, limitations, and underlying assumptions of each body of work.
- Synthesis: The core of the review, involving the construction of a coherent overarching narrative that explains the findings of the different traditions. This involved identifying points of convergence, explaining points of tension or conflict, and building a rich, integrated account of the topic.
- Recommendations: Drawing conclusions and formulating recommendations for policy, practice, and future research based on the synthesised narrative.
By adopting this pluralistic and historically sensitive approach, this review aimed to produce a rich, contextually grounded synthesis that illuminates the key storylines, paradigms, and contestations within the field, providing a robust foundation for public health action.
Results
The meta-narrative synthesis of the literature revealed five distinct but overlapping storylines that, when woven together, provide a comprehensive picture of the intersection of dementia, diabetes, and physical inactivity, particularly within the context of Global Majority populations.
Meta-Narrative 1: The Biomedical and Epidemiological Narrative – A Triad of Risk
This foundational narrative, rooted in epidemiology and clinical medicine, establishes the quantitative and mechanistic links between the three conditions. The central finding from this body of work is the robust, causal relationship between T2D and an elevated risk of dementia. Large-scale cohort studies and meta-analyses consistently demonstrate that individuals with T2D have a two- to three-fold increased risk of developing both Alzheimer’s disease and vascular dementia (Cole et al., 2007; Stewart & Liolitsa, 1999).
This storyline further elaborates on the concept of the “double dilemma” (Hill, 2019). The link is bidirectional: not only does diabetes damage the brain, but the resulting cognitive decline makes managing diabetes exponentially difficult. This is particularly extreme for older adults with diabetes, who already carry a high burden of comorbidities such as cardiovascular disease, stroke, and nephropathy (Meneilly et al., 2016). The cognitive deficits of dementia impaired memory, executive dysfunction, and poor judgment can lead to critical errors in self-management, including missed medication doses, incorrect insulin administration, poor glucose monitoring, and failure to recognise and treat hypoglycaemic episodes. This creates a vicious cycle where poor glycaemic control worsens cognitive decline, and cognitive decline leads to even worse glycaemic control, accelerating the progression of both diseases and placing an immense strain on patients and their caregivers.
Meta-Narrative 2: The Public Health Narrative – Physical Inactivity as a Central, Modifiable Factor
This narrative, emerging from public health and preventive medicine, positions PA as a powerful, non-pharmacological tool for risk reduction. The landmark finding from this tradition is the identification of physical inactivity as the single largest modifiable risk factor for Alzheimer’s disease in Western populations (Norton et al., 2014). This reframes the dementia crisis not as an inevitability of ageing but, in a significant portion of cases, as a potentially preventable condition.
This storyline delves into the physiological mechanisms through which PA exerts its protective effects. In the context of brain health, exercise is understood to work through multiple pathways. It improves cerebral blood flow, reduces systemic and neuroinflammation, combats oxidative stress, and stimulates the production of neurotrophic factors like Brain-Derived Neurotrophic Factor (BDNF), which promotes neurogenesis (the growth of new neurons) and synaptic plasticity (Gronek et al., 2019; Dementia Australia).
In the context of diabetes management, the mechanisms are clear. For instance, a combination of aerobic and resistance training is highly effective at improving glycaemic control by enhancing insulin sensitivity and increasing glucose uptake by muscles (Piras & Raffi, 2023). Based on this evidence, international guidelines have converged on a clear recommendation: at least 150 minutes of moderate-intensity aerobic PA per week, supplemented with muscle-strengthening activities (Annear et al., 2015; WHO, 2025). However, researchers in this tradition also acknowledge the complexity of real-world application, noticing the scientific difficulty of isolating the “net effect” of exercise in clinical studies, as most patients with T2D present with a cluster of related conditions known as metabolic syndrome (Bertram et al., 2016). This complexity points toward the need for a broader, more systemic understanding of risk.
Meta-Narrative 3: The Health Disparities Narrative – A Syndemic of Inequity
This critical narrative, drawing from medical sociology and social epidemiology, reframes the intersection of dementia, diabetes, and inactivity not as a simple co-occurrence of diseases but as a “syndemic” (Kaufman & Perales-Puchalt, 2023). A syndemic is a conceptual framework that describes the synergistic clustering of two or more diseases within a population, where the clustering is driven and sustained by adverse social, economic, and environmental conditions. This lens shifts the focus from individual biology and behaviour to the upstream “causes of the causes”—the social determinants of health.
This storyline is supported by a wealth of quantitative data demonstrating profound disparities at every stage of the disease pathway:
- Heightened Initial Risk: Populations of South Asian descent exhibit a unique biological susceptibility to T2D, developing the condition at a lower BMI and a younger age (Gujral et al., 2013).
- Amplified Behavioural Risk: This biological vulnerability is dangerously amplified by higher rates of physical inactivity. For example, a UK public health assessment in Walsall found that only 36% of Asian adults met PA guidelines, compared to 57% of their White British counterparts (Public Health Walsall, 2015). Furthermore, Safi et al. (2023) condcuted a cross-sectional study exploring the PA levels of British South Asian specifically focusing on youth from Afghan, Pakistani, Bangladeshi, and Indian groups and found that 88.5% Afghans, 80% Bangladeshi, 78.6% Indians and 63% Pakistani reported engaging in less than 30 minutes of PA per day. Furthermore, Safi et al. (2025A) condcuted a cross-sectional study exploring the sitting time of the same population and found that Afghan heritage had a median of sitting time of 150 minutes (MAD =222.390), Bangladeshi heritage 300 minutes (MAD =333.585), Indian heritage 465 minutes (MAD =229.803), and Pakistani heritage 390 minutes (MAD =400.302). While the group with Indian heritage had the highest median sitting time duration and Afghans the lowest. This aligns with previous findings suggesting lower activity levels among many Global Majority groups (Yates et al., 2010).
- Compounded Risk Post-Diagnosis: The disparity continues even after a diabetes diagnosis. A large, 10-year study of over 22,000 older adults with T2D found that, even after adjusting for numerous clinical and demographic factors, African Americans and Native Americans had a 40-60% higher risk of subsequently developing dementia compared to Asian Americans, who had the lowest risk (Whitmer et al., 2012). This reveals a compounded disadvantage, where the progression from one chronic disease to the next is itself shaped by factors linked to race and ethnicity.
- Exacerbated Future Burden: Projections indicate a dramatic future escalation of this disparity, with the number of people from ethnic minority communities in the UK living with dementia expected to increase seven-fold by 2051 (All-Party Parliamentary Group on Dementia, 2013).
Meta-Narrative 4: The Sociocultural and Behavioural Narrative – Understanding Inaction
This storyline, rooted in behavioural psychology and qualitative research, seeks to answer the crucial question: why do these disparities in PA exist? It moves beyond simply documenting the problem to exploring its underlying drivers. The Theory of Planned Behaviour (TPB) provides a useful framework for organizing these findings, positing that behavioural intention is shaped by attitudes, subjective norms, and perceived behavioural control (Ajzen, 1991).
Qualitative research, particularly with South Asian older adults, has provided rich insights into these constructs:
- Attitudes: Negative attitudes toward PA are often shaped by experiences of chronic pain, fatigue, and a perception that exercise is inappropriate or unsafe for older people (Horne & Tierney, 2012). Furthermore, Safi and Myers (2021) condcuted explored the barriers to PA of Afghans in the UK compared to those living in Afghanistan and found that Lack of time and being too tired were barriers for both populations but were rated higher by those living in Afghanistan as was a lack of confidence and being uncomfortable with exercise clothing.
- Subjective Norms: Powerful social and cultural pressures can discourage PA. For women, this may include expectations to prioritize domestic duties and caregiving roles over self-care. For both men and women, community norms around food and hospitality can conflict with healthy lifestyle advice (Begum et al., 2009; Horne & Tierney, 2012).
-
Perceived Behavioural Control: This is arguably the most significant area of barriers. For instance, Safi and Myers (2021) found that Afghan females perceived a lack of single-sex facilities, not being able to participate in PA with males, and having to be fully covered outside of the home as important barriers to their PA, but these were more of a barrier for those residing in the UK compared to those in Afghanistan. Furthermore, some other barriers include:
- Systemic Barriers: Lack of access to safe, affordable, and culturally appropriate facilities (e.g., women-only gym sessions, prayer facilities).
- Environmental Barriers: Living in deprived areas with poorly maintained green spaces or concerns about personal safety.
- Communication Barriers: Language barriers with healthcare providers, leading to a poor understanding of health advice (Yeowell, 2010).
- Cultural Barriers: A sense of fatalism or the belief that health outcomes are predetermined (“in God’s hands”), reducing self-efficacy. Stigma surrounding dementia can also prevent families from seeking help or engaging with preventive health services (Alzheimer’s Society, 2023; Hossain & Khan, 2019).
This narrative demonstrates that physical inactivity is not simply a matter of poor individual choice but is deeply embedded in a complex web of cultural beliefs, social structures, and environmental constraints.
Meta-Narrative 5: The Intervention Science Narrative – Pathways to Equity
The final storyline addresses the question of “what is to be done?” It moves from problem analysis to solution design. This narrative begins with the optimistic finding that pragmatic, real-world lifestyle interventions are effective in reducing the incidence of T2D (Ashra et al., 2015) and can be critical for secondary prevention—managing existing conditions to prevent further complications like dementia (Bailey, 2020). However, the central challenge identified in this storyline is how to adapt these interventions to be effective, equitable, and sustainable within diverse communities.
The key paradigm that emerges from this narrative is Community-Based Participatory Research (CBPR). CBPR is defined as a collaborative research model that “harnesses community wisdom” by equitably involving community members, researchers, and organisations in all aspects of the research process (Shalowitz et al., 2009). This collaborative approach fundamentally shifts the power dynamic in research, moving away from a top-down model where experts “intervene” on a community, to a bottom-up partnership where solutions are co-created. The rationale is that interventions designed with a community are far more likely to be trusted, culturally resonant, relevant to their lived experiences, and ultimately, sustainable if dedicated sessions made available in the UK and across the world (Safi and Myers, 2021). Furthermore, a prime example of this approach in action is a pilot study of a mosque-based PA programme for South Asian Muslim men and women, which demonstrated high feasibility and acceptability (Safi et al., 2025b; Banerjee et al., 2016). By delivering the intervention in a trusted, accessible, and culturally safe space, the programme successfully overcame many of the barriers identified in the sociocultural narrative. This storyline concludes that to address intractable health disparities, public health must move beyond simply disseminating information and instead invest in building authentic community partnerships to co-design solutions.
Discussion
This meta-narrative review has synthesised evidence from five distinct but complementary research traditions to construct a holistic understanding of the intersection between dementia, diabetes, and physical inactivity, with a critical focus on the disparities experienced by Global Majority populations. The synthesis reveals that these are not separate issues to be tackled in silos, but a complex, interconnected syndemic rooted in a combination of biological vulnerability, behavioural patterns, sociocultural context, and systemic inequity.
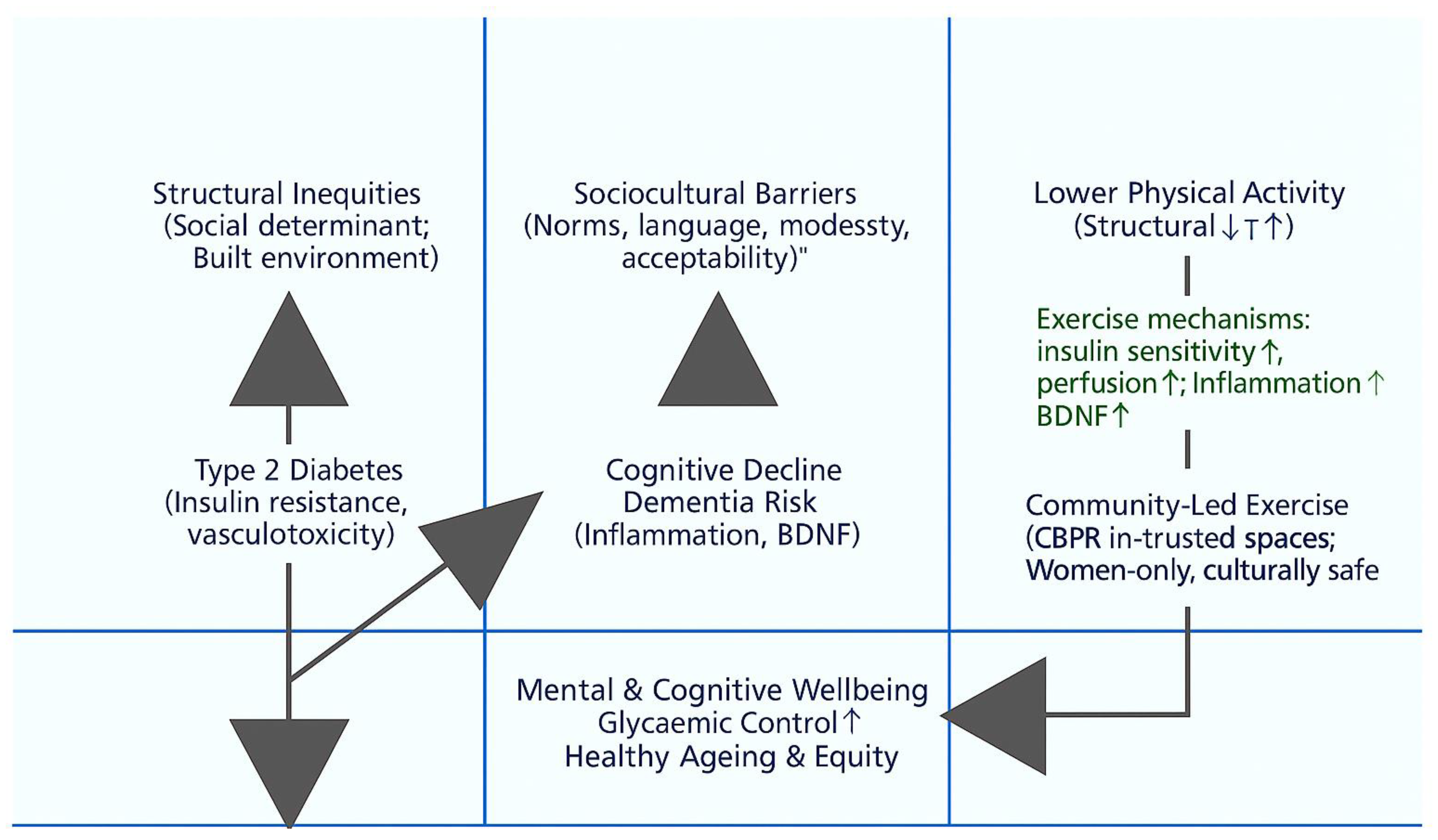
Figure 1 provides a visual synthesis of the five meta-narratives identified in this review, offering an integrative conceptual framework that explains how dementia, diabetes, and physical inactivity intersect within Global Majority populations. The framework positions structural inequities such as poverty, deprivation, environmental barriers, and institutional bias as the fundamental upstream determinants shaping exposure to unhealthy environments. These structural forces interact with sociocultural barriers, including community norms, stigma, and gendered expectations, to constrain opportunities for PA and hinder engagement with preventive health services.
This reduced PA engagement contributes to T2D through mechanisms of insulin resistance, obesity, and vascular dysfunction, while diabetes-related metabolic and vascular changes particularly neuroinflammation and reduced Brain-Derived Neurotrophic Factor (BDNF) increase the risk of cognitive decline and dementia. The diagram also depicts the positive moderating role of community-led PA/exercise interventions, particularly those grounded in Community-Based Participatory Research (CBPR) principles. Such interventions, delivered in culturally trusted and gender-sensitive spaces, enhance glycaemic control, stimulate neurogenesis, improve mental wellbeing, and promote healthy ageing and health equity.
In synthesising the biological, behavioural, and sociocultural dimensions of the evidence, this conceptual model makes clear that the intersection of dementia and diabetes is not simply a biomedical phenomenon but a syndemic rooted in structural and cultural determinants. The framework therefore advances a public-health perspective that situates individual health behaviours within their broader social context and highlights the need for community-driven, culturally safe strategies as a pathway toward equitable healthy ageing.
The overarching framework for understanding this issue is that of the syndemic (Narrative 3). This concept provides the essential context for interpreting the findings from the other narratives. The stark biomedical link between T2D and dementia (Narrative 1) is not a universal constant; its real-world impact is dramatically amplified in populations already burdened by social and economic disadvantage. The powerful preventive potential of PA (Narrative 2) remains unrealized for many because of the formidable sociocultural and systemic barriers that constrain individual choice (Narrative 4). The failure of traditional, one-size-fits all public health messaging is a predictable outcome when the deep-seated “causes of the root-causes” are ignored. This integrated understanding points unequivocally toward a new paradigm for intervention, one grounded in community partnership and cultural competence (Narrative 5).
A central theme emerging from the discussion is the concept of compounded risk. The “double dilemma” of managing co-occurring diabetes and dementia is a significant clinical challenge for any individual. However, for a person from a Global Majority community, this dilemma is compounded by multiple additional layers of disadvantage. They may have developed diabetes at a younger age, face language and cultural barriers when communicating with healthcare providers, live in an environment that is not conducive to PA, for instance people from communities where PA is regarded as important for health are more likely to perceive fewer barriers to PA, and therefore, engage in more regular PA compared to where PA is not a social norm (Safi and Myers, 2021) and belong to a community where dementia is highly stigmatised. The finding from Whitmer et al. (2012) highlight that even within a high-risk diabetic population, the progression to dementia is significantly higher for African Americans and Native Americans is a testament to this compounded risk. It demonstrates that race and ethnicity are not just demographic variables but representations for a lifetime of accumulated social and environmental exposures that shape disease trajectories.
The Theory of Planned Behaviour (TPB) proved to be more than just an abstract academic model; it serves as a practical diagnostic tool for deconstructing the complex reasons for physical inactivity. The qualitative evidence mapped onto the TPB’s constructs (attitudes, subjective norms, perceived behavioural control) provides a clear blueprint of the specific barriers that must be addressed. For example, an intervention that simply provides information about benefits of PA/exercise (targeting attitudes) will fail if it does not also address community norms around women’s roles (subjective norms) or the lack of women-only facilities (perceived behavioural control) as highlighted in the study by Safi and Myers (2021). This highlights the critical need for interventions to be multi-faceted, addressing not just individual knowledge but also the social and physical environment. The stark statistic from the Walsall public health report (2015), showing a 21-percentage-point gap in activity levels between Asian and White British adults, is a powerful real-world illustration of how these multifaceted barriers translate into inequitable health outcomes.
This review also underscores the pivotal role of healthcare professionals. The finding that physician advice is a key factor in promoting adherence to PA (Annear et al., 2015) and that GPs are a highly trusted source of information for South Asian older adults (Horne & Tierney, 2012) places a significant responsibility on the healthcare system. However, this potential is often unrealised. Clinicians may lack the time, training, or resources to provide specific, culturally competent advice. A 15-minute consultation is often insufficient to explore and address the complex sociocultural barriers a patient faces. This points to a systemic failure to equip the healthcare workforce with the skills and support needed to effectively promote lifestyle change in diverse populations.
Strengths and Limitations
The primary strength of this review lies in its meta-narrative methodology. By intentionally synthesising evidence from heterogeneous sources, it has been possible to construct a rich, multi-layered account of a complex problem that would not be visible through a narrower methodological lens. This approach has allowed for the integration of quantitative epidemiological data, qualitative sociological insights, and behavioural science theories into a single, cohesive argument, which is essential for addressing complex public health and policy questions. However, this approach also has inherent limitations. The process of identifying and interpreting the different “meta-narratives” is an interpretive act and is therefore subject to the researchers’ own perspectives and potential biases, despite efforts at reflexivity and peer discussion. Unlike a quantitative meta-analysis, this review does not produce a single, pooled statistical measure of effect. Its strength lies in its explanatory power, not in statistical aggregation. A significant challenge encountered during the search phase was the relative scarcity of literature that explicitly addressed dementia, diabetes, and physical inactivity simultaneously within specific Global Majority populations in the UK. This necessitated the broader meta-narrative approach but also highlights a critical gap in the primary research literature. Finally, while this review drew heavily on evidence concerning South Asian populations where a richer body of qualitative research exists the specific findings related to cultural barriers and facilitators may not be fully generalizable to all Global Majority groups, such as those of African Caribbean, Black African, or Eastern European heritage, each of whom possesses a unique cultural context, migration history, and experience with the healthcare system.
Research Implications and Recommendations for Future Study
The synthesis of evidence presented in this review leads to a series of urgent, actionable recommendations for researchers, public health bodies, healthcare systems, and policymakers. The overarching implication is that closing the profound health equity gap requires a fundamental shift away from individual-centric, culturally blind approaches toward systemic, community-grounded, and culturally competent strategies. The evidence strongly suggests that preventive strategies, including physical training, should begin as early as possible during the development of T2D to mitigate dementia risk (Bertram et al., 2016).
1. For Researchers and Funding Bodies: Prioritise and Mandate a Community-Based Participatory Research (CBPR) Paradigm
The evidence is clear that top-down interventions are insufficient. To develop solutions that are trusted, relevant, and sustainable, research itself must become a partnership.
- Implication: Future research on health interventions in Global Majority communities should be built on a CBPR framework. This involves equitably involving community members, leaders, and organizations in all phases of the research process, from defining the research question to designing the intervention and disseminating the findings (Shalowitz et al., 2009). This approach shifts power dynamics, builds trust, and ensures that interventions are grounded in the lived reality of the community.
- Recommendation: Funding bodies should create specific grant streams for CBPR projects and require evidence of genuine community partnership in applications for funding aimed at reducing health disparities. Research institutions should invest in training and supporting researchers to develop the skills needed for effective community engagement, moving beyond tokenistic consultation to true co-creation.
2. For Public Health Commissioners and Providers: Develop and Scale Culturally-Resonant Interventions in Trusted Spaces
Generic public health campaigns promoting physical activity are failing to reach those most at risk. Interventions must be delivered in a way that respects and integrates cultural norms and values.
- Implication: The success of the pilot mosque-based programme (Banerjee et al., 2016) provides a model that should be adapted and expanded. Interventions need to be brought to where people are, both physically and culturally.
- Recommendation: Public health commissioners should work with community organizations to co-design and fund a diverse portfolio of PA programmes delivered in trusted community settings, such as gurdwaras, temples, churches, and community centres. These programmes should be tailored to address specific cultural needs, such as providing women-only sessions, ensuring modesty, incorporating culturally familiar activities (e.g., dance), and being sensitive to religious calendars and obligations. Employing “community health champions” or “cultural brokers” from within the community can further enhance trust and engagement.
3. For Health Systems and Professional Education Bodies: Equip Healthcare Professionals with Cultural Competency and Practical Tools
Healthcare professionals are a critical but underutilized resource in promoting lifestyle change. They must be better equipped to provide effective, culturally sensitive advice.
- Implication: The trust placed in GPs (Horne et al., 2012) represents a powerful opportunity. However, this trust can be eroded if patients feel their cultural context is not understood or respected.
- Recommendation: Medical and nursing school curricula, as well as continuing professional development programmes, must include mandatory training on cultural competency. This should go beyond superficial awareness to provide practical skills in: (a) understanding the syndemic of risk in diverse populations; (b) using tools like the Theory of Planned Behaviour to sensitively inquire about sociocultural barriers to health behaviours; and (c) “social prescribing,” where clinicians can connect patients to specific, culturally appropriate community-based programmes and resources. Health systems must also ensure adequate access to interpreters and support for longer consultation times when needed.
4. For Policymakers and Urban Planners: Advocate for Systemic Change to Address the Social Determinants of Health
Individual behaviour change is difficult, if not impossible, in an environment that is not conducive to health. Addressing the syndemic requires tackling the upstream drivers of disease.
- Implication: The high rates of physical inactivity in many Global Majority communities are linked to the socioeconomic and environmental conditions of the areas where they are more likely to live.
- Recommendation: Public health leaders must advocate for policies that address the social determinants of health. This includes equitable investment in safe, well-lit, and well-maintained public parks and green spaces in deprived neighbourhoods; policies that promote active transport (walking and cycling); and ensuring that new housing developments include accessible recreational facilities. This shifts the focus from solely blaming individuals for their inactivity to creating environments where the healthy choice is the easy choice for everyone.
5. For Future Research: Address Critical Evidence Gaps
While this review has synthesised existing knowledge, it has also highlighted several critical gaps that future research must address.
- Recommendation:
- Conduct large-scale, longitudinal cohort studies within specific UK-based Global Majority populations to more accurately quantify the population-attributable fraction of dementia risk from factors like diabetes and physical inactivity.
- Expand qualitative research beyond the South Asian community to better understand the unique barriers and facilitators to physical activity among Black African, African Caribbean, Eastern European, and other diverse groups.
- Conduct implementation science research to understand the best strategies for scaling up successful pilot interventions (like the mosque-based programme) to a regional or national level, while maintaining fidelity and community engagement.
- Develop and validate culturally-adapted assessment tools for dementia and cognitive decline, as existing tools may not be appropriate for linguistically and culturally diverse populations, leading to under-diagnosis.
In conclusion, the intersection of dementia, diabetes, and physical inactivity represents one of the most significant and inequitable public health challenges of our time. Moving forward requires a paradigm shift. By embracing community partnership, embedding cultural competence into our health systems, and tackling the systemic drivers of disease, we can begin to dismantle the syndemic of disparity and work toward a future of more equitable healthy ageing for all.
References
- Ajzen, I. The theory of planned behavior. Organizational behavior and human decision processes 1991, 50(2), 179–211. [Google Scholar]
- All-Party Parliamentary Group on Dementia. Dementia does not discriminate: The experiences of black, Asian and minority ethnic communities; The Alzheimer’s Society, 2013. [Google Scholar]
- Alzheimer’s Association. 2023 Alzheimer’s disease facts and figures. Alzheimer’s & Dementia 2023, 19(4), 1598–1695. [Google Scholar]
- Alzheimer’s Society. Left to Cope Alone: The unmet support needs of people with dementia from Black, Asian and minority ethnic communities; 2023. [Google Scholar]
- Annear, M. J.; Toye, C.; McInerney, F. What should we be recommending to older people in relation to the prevention of dementia? A narrative synthesis of the evidence from international guidelines. Geriatrics & Gerontology International 2015, 15(7), 811–819. [Google Scholar]
- Ashra, N. B.; Spong, R.; Carter, P.; Gujral, J. S. A systematic review and meta-analysis of the effectiveness of a real-world lifestyle intervention programme for the prevention of type 2 diabetes. BMJ Open 2015, 5(9), e007174. [Google Scholar]
- Bailey, R. R. Promoting physical activity and nutrition in people with stroke. Stroke 2020, 51(2), 691–693. [Google Scholar]
- Banerjee, A. T.; Kin, C.; Strachan, P. H.; Boyle, M. H. A mosque-based physical activity intervention for South Asian Muslim women: a pilot and feasibility study. Women’s Health 2016, 12(4), 399–408. [Google Scholar]
- Begum, S.; Williams, J.; Adamson, A. J. ‘I want to be a little bit lighter but I don’t want to be skinny’: a qualitative study of the diet and physical activity views and preferences of Bangladeshi women living in Newcastle upon Tyne. Journal of Human Nutrition and Dietetics 2009, 22(6), 529–537. [Google Scholar]
- Bertram, S.; Brixius, K.; Brinkmann, C. “Physical exercise and dementia in patients with type 2 diabetes mellitus”. Authors’ reply. Endocrine 2016, 54, 840. [Google Scholar] [CrossRef]
- Cho, N. H.; Shaw, J. E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J. D.; Ohlrogge, A. W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Research and Clinical Practice 2018, 54, 271–281. [Google Scholar] [CrossRef]
- Cole, J. H.; Vinberg, M.; Fotopoulou, A. The impact of type 2 diabetes on the risk of dementia. Diabetologia 2007, 50(7), 1364–1375. [Google Scholar]
- Dementia Australia. Physical activity; Retrieved from Dementia Australia website; n.d. [Google Scholar]
- Greenhalgh, T.; Robert, G.; Macfarlane, F.; Bate, P.; Kyriakidou, O.; Peacock, R. Storylines of research in diffusion of innovation: a meta-narrative approach to systematic review. Social science & medicine 2005, 61(2), 417–430. [Google Scholar]
- Gronek, P.; Balko, S.; Gronek, J.; Zajac, A.; Maszczyk, A.; Celka, R.; Yu, F. Physical activity and Alzheimer’s disease: A narrative review. Aging and disease 2019, 10(6), 1282. [Google Scholar] [CrossRef] [PubMed]
- Gujral, U. P.; Pradeepa, R.; Weber, M. B.; Narayan, K. M.; Mohan, V. Type 2 diabetes in South Asians: similarities and differences with white Caucasian and other populations. Annals of the New York Academy of Sciences 2013, 1281(1), 51–63. [Google Scholar] [CrossRef] [PubMed]
- Hill, J. The double dilemma: the rising prevalence of diabetes and dementia. British Journal of Community Nursing 2019, 24(12), 586–591. [Google Scholar]
- Horne, M.; Tierney, S. What are the barriers and facilitators to exercise and physical activity uptake and adherence among South Asian older adults: a systematic review of qualitative studies. Preventive medicine 2012, 55(4), 276–284. [Google Scholar] [CrossRef]
- Hossain, M. Z.; Khan, H. T. A. Dementia in the Bangladeshi diaspora in England: A qualitative study of the myths and stigmas about dementia. Journal of evaluation in clinical practice, 2019.
- Johnson, A. Risk of type 2 diabetes for people from Black African, African Caribbean and South Asian backgrounds; Diabetes UK, 2022. [Google Scholar]
- Kaufman, M. R.; Perales-Puchalt, J. Applying a syndemic framework to understand and address health disparities. JAMA 2023, 329(17), 1455–1456. [Google Scholar]
- Lascar, N.; Brown, J.; Pattison, H.; Barnett, A. H.; Bailey, C. J.; Bellary, S. Type 2 diabetes in adolescents and young adults. The Lancet Diabetes & Endocrinology 2018, 6(1), 69–80. [Google Scholar] [CrossRef]
- Meneilly, G. S.; Tessier, D.; Knip, A. Diabetes in elderly adults. The Lancet 2016, 387(10028), 1677–1685. [Google Scholar] [CrossRef]
- Norton, S.; Matthews, F. E.; Barnes, D. E.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: an analysis of population-based data. The Lancet Neurology 2014, 13(8), 788–794. [Google Scholar] [CrossRef]
- Nursing, Times. Life expectancy rises but years in good health falls; Retrieved from Nursing Times website; 2023. [Google Scholar]
- Piras, A.; Raffi, M. A narrative literature review on the role of exercise training in managing type 1 and type 2 diabetes mellitus. Healthcare 2023, 11(22), 2947. [Google Scholar] [CrossRef]
- Walsall, Public Health. Healthy Weight and Physical Activity Needs Assessment; 2015. [Google Scholar]
- Safi, A.; Hossain, M.; Myers, T. Faith, health and well-being: a qualitative study exploring Islamic perspectives on physical activity and the role of Imams (scholars). Discover Social Science and Health 2025, 5(1), 1–12. [Google Scholar] [CrossRef]
- Shalowitz, M. U.; Isacco, A.; Barquin, N.; Clark-Kauffman, E.; Delger, P.; Nelson, D.; Wagenaar, K. Community-based participatory research: a review of the literature with strategies for community engagement. Journal of developmental and behavioral pediatrics: JDBP 2009, 30(4), 350. [Google Scholar] [CrossRef]
- Smith, L. Physical inactivity in Black and Asian people; Public Health England, 2020. [Google Scholar]
- Stewart, R.; Liolitsa, D. Type 2 diabetes mellitus, cognitive impairment and dementia. Diabetic Medicine 1999, 16(2), 93–112. [Google Scholar] [CrossRef]
- Whitmer, R. A.; Karter, A. J.; Yaffe, K.; Quesenberry, C. P., Jr.; Selby, J. V. Hypoglycemic episodes and risk of dementia in older patients with type 2 diabetes mellitus. JAMA 2009, 301(15), 1565–1572. [Google Scholar] [CrossRef]
- WHO. Physical Inactivity; World Health Organisation, 2024. [Google Scholar]
- World Health Organization. Ageing and health; 2022. [Google Scholar]
- Yates, T.; Davies, M. J.; Khunti, K. Physical activity and ethnic minorities. Postgraduate medical journal 2010, 86(1011), 42–47. [Google Scholar]
- Yeowell, G. The health-care experiences of British-Pakistani women with osteo-arthritis of the knee. Disability and rehabilitation 2010, 32(1), 31–39. [Google Scholar]
Figure 1.
Conceptual Framework Linking Structural Inequities, Sociocultural Barriers, and Physical Inactivity to Type 2 Diabetes, Cognitive Decline, and Dementia Risk in Global Majority Populations.
Figure 1.
Conceptual Framework Linking Structural Inequities, Sociocultural Barriers, and Physical Inactivity to Type 2 Diabetes, Cognitive Decline, and Dementia Risk in Global Majority Populations.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



