
Submitted:
01 January 2026
Posted:
04 January 2026
You are already at the latest version
Abstract
In people with dementia, cognitive stimulation, learning, and meaningful activities do not constitute disease-modifying therapies that directly alter neurodegenerative pathology such as brain atrophy or amyloid/tau accumulation. However, reduced daytime activity, disengagement, apathy, and social withdrawal are consistently associated with cognitive decline, deterioration in activities of daily living (ADL), behavioral and psychological symptoms of dementia (BPSD; e.g., depression, irritability, agitation), increased caregiver burden, and a higher likelihood of hospitalization or institutionalization. Therefore, learning and leisure activities should be positioned not as “brain-training interventions” but as foundational interventions aimed at suppressing inactivity and disengagement, which function as “progression-accelerating factors” (Robert et al., 2009; Brodaty & Burns, 2012).Many conventional cognitive training and learning interventions implicitly assume preserved comprehension, memory, task performance, and tolerance for evaluation, making them difficult to implement in real-world dementia care settings. This paper decomposes existing evidence (including Cognitive Stimulation Therapy, CST) into “active ingredients” and “excessive burdens,” and proposes an implementation-adaptive minimal model consisting of: (1) 10–20 minutes per day of meaningful activity (including leisure activities); (2) a level of difficulty that ensures successful experiences; (3) interpersonal elements when feasible; and (4) the removal of evaluation, correct-answer demands, and self-management requirements.The value of learning should be assessed not by maximizing cognitive test scores, but by outcomes such as suppression of apathy, depression, and BPSD, maintenance of daytime activity and ADL, and prevention of caregiving breakdown and hospitalization.
Keywords:
dementia
; learning and leisure activities
; non-pharmacological intervention
; apathy
; disengagement
; implementation adaptation
; BPSD
1. Introduction
1.1. Redefining “Learning and Leisure Activities” in Dementia
Cognitive stimulation, learning, and leisure activities do not “cure” dementia; however, they play an important role in suppressing progression-accelerating factors such as disengagement, apathy, and social withdrawal (Robert et al., 2009). Apathy is one of the most prevalent core symptoms of dementia and, while overlapping with depression, can be clinically distinguished as reduced activity and goal-directed behavior (Robert et al., 2009). Reviews of non-pharmacological interventions suggest that individualized therapeutic activities may alleviate apathy (Brodaty & Burns, 2012).
This positioning of learning and leisure activities in dementia—not as disease-modifying interventions but as foundational interventions to suppress progression-accelerating factors—is schematically illustrated in Figure 1.
1.2. Limitations of Conventional Cognitive Training and Learning Interventions
Many learning programs are designed on the implicit assumptions of:
- (i)
- comprehension and memory;
- (ii)
- accurate task performance;
- (iii)
- continuous self-management; and
- (iv)
- tolerance for evaluation.
In dementia, these assumptions often break down early, resulting in interventions that are theoretically valid but difficult to implement. This mismatch creates failure experiences that reinforce apathy and refusal, leading to a vicious cycle.
2. Constraints in Learning and Leisure Activity Interventions
2.1. Cognitive Constraints: Difficulties in Comprehension, Memory, and Self-Regulation
Understanding task meaning, retaining procedures, making choices among multiple options, and self-evaluation rely heavily on executive function and attention, which are easily compromised in dementia.
2.2. Emotional Constraints: Failure Experiences Trigger BPSD
Learning that emphasizes “mistakes” or “inability” can induce anxiety, anger, and refusal, ultimately promoting withdrawal from activities.
2.3. Implementation Constraints: Care Burden and Daily Care Pathways
Interventions that require extensive preparation, long durations, specialized tools, or relocation are less likely to be sustained.
3. Distinguishing Active Ingredients from Excessive Burden
3.1. Core Active Ingredients
Integrating the literature with implementation realities, the effective elements of learning and leisure activities can be summarized as follows:
- Maintenance of engagement: Prevents fixation of disengagement and apathy
- Securing successful experiences (achievement/pleasure): Preserves reward systems and self-efficacy
- Addition of social context (interpersonal elements when feasible): Simultaneously promotes stimulation, arousal, and emotional stability
- Minimal repeatable units: Even short activities that can be performed “every day”
Cognitive Stimulation Therapy (CST) has been shown to improve cognitive function, quality of life, and depression in people with mild to moderate dementia (Desai et al., 2024). This paper does not deny the effectiveness of CST itself; rather, it emphasizes that in home care and later stages of dementia, the key is to translate the active ingredients (active engagement, successful experiences, and social context) into minimal daily units. Figure 2 reorganizes these core ingredients into a minimal model compatible with dementia care realities.
3.2. Excessive Implementation Burdens to Be Removed
- Evaluation of correct answers or achievement levels (test-like formats)
- Requiring motivation or sustained willingness from the person
- Complex rules or tasks requiring memory
- Decision-making burdens caused by offering multiple choices
- Obligatory recording, scoring, or reflection
4. Dementia-Adaptive Minimal Model of Learning and Leisure Activities
4.1. Minimal Component ①: 10–20 Minutes per Day of “Meaningful Activity” (Including Leisure)
The 10–20-minute duration does not represent an optimal dose, but rather the minimum amount that can realistically be sustained daily.
Examples (fixed according to individual preferences):
- Leisure: coloring, origami, gardening, partial sewing tasks, arranging a shogi board, simple musical instruments, singing
- Roles: assisting with meal setup, folding towels, sorting, wiping, arranging
- Language: reading aloud, short read-aloud sessions, reminiscence using old photographs
- Sensory: keeping rhythm, hand and finger movements (focus on process rather than completion)
4.2. Minimal Component ②: Difficulty Set to Ensure Successful Experiences (“Leaning Toward Can-Do”)
- Early termination is acceptable; completion is not required
- Demonstrate and perform together rather than explaining verbally
- Do not correct mistakes; do not evaluate outcomes based on product quality
4.3. Minimal Component ③: Interpersonal Elements When Possible (One-to-One Is Sufficient)
Social isolation and reduced social relationships are associated with cognitive decline (Kuiper et al., 2015). Therefore, rather than group participation, doing activities together one-to-one should be prioritized.
4.4. Minimal Component ④: Removal of Evaluation and Self-Management Demands (Shifting Responsibility to the Environment)
Instead of relying on the person’s effort or self-management, caregivers and the environment should create pathways that allow activities to begin naturally with minimal steps.
5. Implementation Protocol (Summary)
- Frequency: Daily (short duration)
- Format: Same time, same place, same tools (predictability)
- Leader: Caregiver-led (does not assume user initiative)
- Recording: Simple ○/× check only (no evaluation)
6. Implications for Research, Practice, and Policy
The implementation-adaptive model proposed here differs fundamentally from conventional learning interventions in its assumed cognitive demands. This contrast is illustrated in Figure 3. The novelty of this paper lies not in proposing new cognitive training, but in redefining learning and leisure activities as control mechanisms for progression-accelerating factors and reconstructing them into an implementable minimal unit. Evaluation metrics should extend beyond cognitive test improvements to include apathy, depression, BPSD, daytime activity, ADL decline, caregiver burden, and hospitalization or institutionalization—outcomes directly linked to societal costs (Brodaty & Burns, 2012).
7. Conclusion
Learning and leisure activity support for people with dementia should be reconstructed not as “brain-training interventions,” but as foundational interventions to prevent disengagement, apathy, and social withdrawal. By preserving core active ingredients—engagement, successful experiences, and social context—while removing evaluation, judgment, and self-management demands, a model that functions in home and care settings can be established.
Appendix
Implementation Manual for Learning and Leisure Activity Support for People with Dementia
(Implementation Guide for Care and Support Settings)
1. Purpose and Positioning
This manual aims to provide practical implementation guidelines for safely and sustainably delivering learning and leisure activity support for people with dementia in home and care settings.
This program is not intended to restore cognitive function or to provide cognitive training effects. Rather, it is an implementation-adaptive non-pharmacological intervention whose primary objective is to suppress so-called progression-accelerating factors, including:
- disengagement
- apathy
- activity avoidance
- emotional instability
- behavioral and psychological symptoms of dementia (BPSD)
This manual is intended for use by:
- care staff working in residential care facilities or home-care settings
- family caregivers supporting people with dementia
- medical and welfare professionals seeking to integrate learning and leisure activities into daily care without excessive burden
Notes:
- This manual is not a clinical trial protocol, but an implementation guide for routine care.
- It does not claim therapeutic efficacy or cognitive improvement from learning or leisure activities.
2. Target Population
Eligible Individuals
- People with mild to moderate dementia
- Individuals who respond to simple verbal cues, imitation, or non-verbal guidance
- Individuals capable of engaging in short-duration activities in daily life
Exclusion and Caution Criteria
- Persistent severe agitation, refusal, or irritability that prevents safe implementation
- Marked exacerbation of BPSD triggered by activity-related stimulation
- Medically unstable conditions such as acute delirium, severe pain, or significant physical illness
Notes:
- Final decisions should always prioritize clinical judgment.
- Even in advanced dementia, this program may be adaptively applied as presence-affirming activities when outcomes or responses are not demanded.
3. Basic Design Principles
This program is designed according to the following four principles:
1. Minimization of Cognitive Load
- Do not require comprehension, memory retention, or learning outcomes
- Do not evaluate correctness, completeness, or improvement
2. Emotional Safety
- Do not correct, instruct, compare, or reprimand
- Immediately reduce or stop the activity if anxiety, confusion, or refusal is observed
3. Predictability and Repetition
- Fix activity content, timing, and procedures as much as possible
- Avoid framing activities as special events
4. Caregiver- or Environment-Led Implementation
- Do not assume motivation, judgment, or self-management by the person
- Consider support successful even if the person does not actively “participate”
4. Overall Program Structure
Recommended Frequency and Duration
- Learning and leisure activities: daily, 10–20 minutes
- Interpersonal interaction (when feasible): short one-to-one engagement
- Verbal prompting and initiation: embedded within routine daily care
Implementation Environment
- Familiar living environments
- Quiet settings that avoid excessive stimulation
- Minimal preparation, movement, and choice requirements
5. Core Support Components (Three Mandatory Elements)
5.1. Daily 10–20 Minutes of “Meaningful Activity” (Learning or Leisure)
Objectives
- Prevent fixation of disengagement and apathy
- Maintain daytime activity levels and emotional stability
Methods
- Fix activities that the individual has previously enjoyed or resists least
- Do not require completion, understanding, or measurable outcomes
Examples
- Leisure: coloring, origami, knitting, gardening (watering only), singing
- Learning-like activities: reading aloud, short read-aloud sessions, simple calculation-like tasks
- Role-based activities: folding towels, sorting, arranging, wiping
Example Phrases
- “Let’s try this together for a little while.”
- “It’s okay to stop at any time.”
5.2. Difficulty Adjustment to Ensure Successful Experiences
Objective
- Prevent refusal or BPSD triggered by failure experiences
Methods
- Reduce difficulty to a clearly achievable level
- Treat incomplete or partial engagement as success
Practices to Avoid
- Correcting mistakes
- Referring to improvement or performance outcomes
5.3. Interpersonal Elements Within Feasible Limits
Objective
- Support attention, arousal, and emotional stability
Methods
- Engage together in a one-to-one format
- Emphasize parallel or supportive presence
Cautions
- Do not force group participation
- Do not check whether the person remembers or understands
6. Explicitly Excluded Practices
The following are not included in this program:
- Cognitive training or test-like learning formats
- Interventions that evaluate correctness, achievement, or outcomes
- Persuasive approaches aimed at eliciting motivation or willingness
- Interactions requiring decision-making through choice presentation
Notes:
- This is not an exclusion of learning stimuli per se, but a restructuring of format.
- This manual does not constitute an intervention study designed to quantitatively verify the effectiveness of a specific learning program.
- Its primary aim is to present an implementation framework adapted to the cognitive and emotional constraints of dementia, based on existing theoretical, review, and implementation studies.
7. Adjustment and Discontinuation Criteria
Adjustable Elements
- Duration (shortening is acceptable)
- Activity content (simplification)
- Amount of interpersonal stimulation
Discontinuation Criteria
- Clear anxiety, refusal, or agitation
- Increased fatigue or confusion
- Signs of BPSD exacerbation
8. Safety and Burden Management
- Physical risks are extremely low
- The greatest risk is accumulation of failure experiences
- Do not demand perfect implementation or consistent success
- 9. Consistency with Existing Evidence
This manual is grounded in existing evidence concerning:
- Associations between apathy, reduced activity, and functional decline
- Findings on apathy reduction through non-pharmacological interventions
- Relationships between social engagement and cognitive or functional decline
and is reconstructed to align with real-world dementia care implementation.
10. Use in Research and Practice
Research Applications
- Supplementary material describing intervention content
- Documentation of implementation methods and fidelity
Practical Applications
- Simplified manuals for care staff
- Guides for family caregivers
- Shared reference materials for care policy discussions
End of Appendix Manual
Figure 1.
Conceptual Positioning of Learning and Leisure Activities in Dementia Care. Learning and leisure activities do not directly modify neurodegenerative pathology in dementia. However, reduced activity and apathy function as progression-accelerating factors that contribute to depression, BPSD, social withdrawal, ADL decline, and increased risks of hospitalization and institutionalization. This figure positions learning and leisure activities not as interventions aimed at cognitive recovery, but as foundational non-pharmacological interventions designed to suppress disengagement and apathy.
Figure 1.
Conceptual Positioning of Learning and Leisure Activities in Dementia Care. Learning and leisure activities do not directly modify neurodegenerative pathology in dementia. However, reduced activity and apathy function as progression-accelerating factors that contribute to depression, BPSD, social withdrawal, ADL decline, and increased risks of hospitalization and institutionalization. This figure positions learning and leisure activities not as interventions aimed at cognitive recovery, but as foundational non-pharmacological interventions designed to suppress disengagement and apathy.
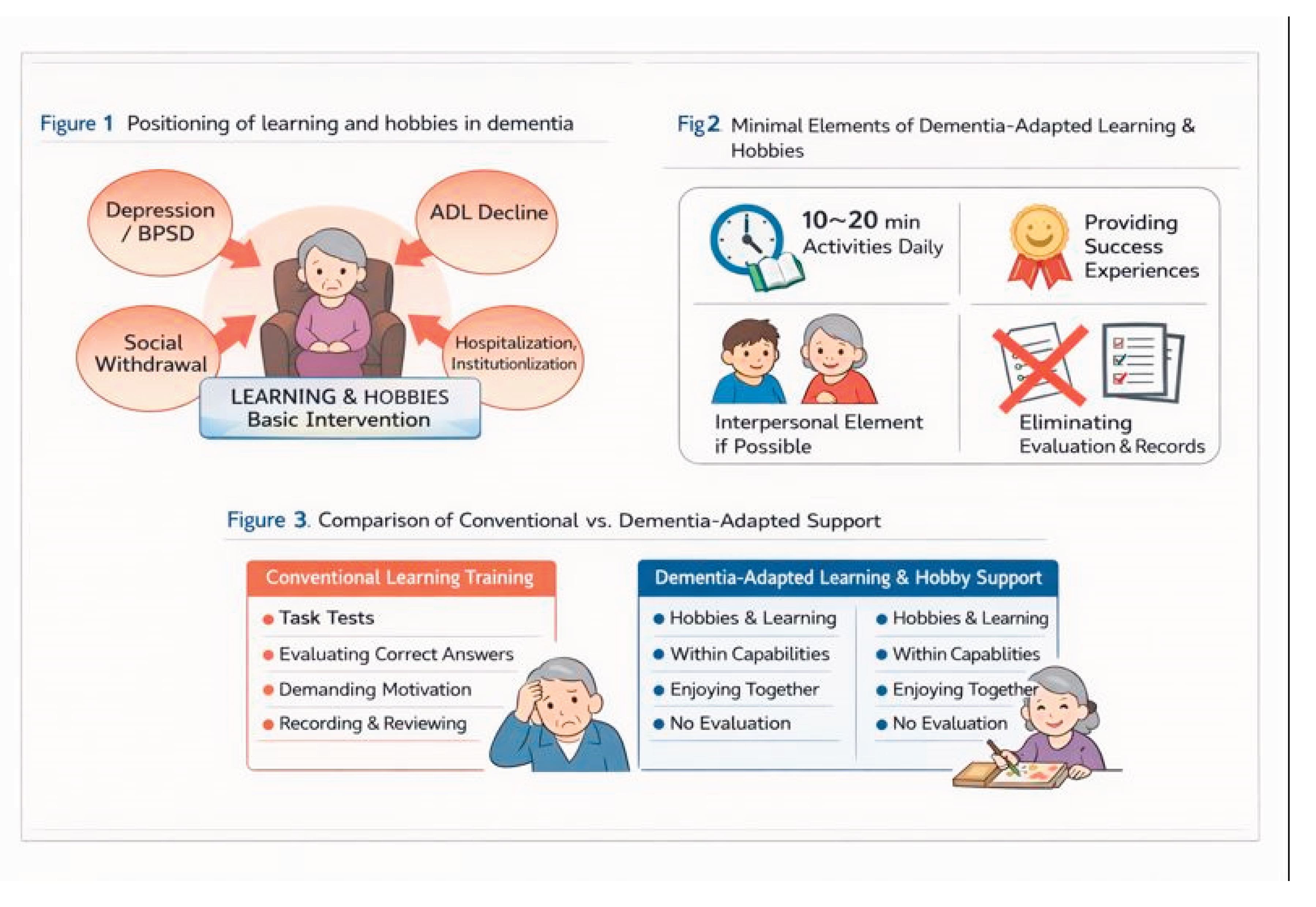
Figure 2. Dementia-Adaptive Minimal Model of Learning and Leisure Activities. This figure illustrates an implementation model of learning and leisure activities reconstructed to suit people with dementia. The model consists of four minimal elements: (1) short daily activities of 10–20 minutes; (2) emphasis on successful experiences rather than achievement or outcomes; (3) interpersonal engagement within feasible limits; and (4) explicit exclusion of evaluation, testing, and record-keeping. Through repeated and stable implementation of these elements, emotional safety and feasibility are ensured.
Figure 3. Comparison Between Conventional Learning Interventions and Dementia-Adaptive Learning and Leisure Support. Conventional learning interventions implicitly assume preserved comprehension, self-management, motivation, and performance evaluation. These assumptions often fail early in dementia, leading to failure experiences and activity avoidance. This figure demonstrates how dementia-adaptive learning and leisure support removes these assumptions and shifts responsibility from the individual to the care environment, thereby enhancing emotional safety and sustainability.
References
- Brodaty, H.; Burns, K. Nonpharmacological management of apathy in dementia: A systematic review. American Journal of Geriatric Psychiatry 2012, 20(7), 549–564. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.; Leung, W. G.; Fearn, C.; John, A.; Stott, J.; Spector, A. Effectiveness of cognitive stimulation therapy (CST) for mild to moderate dementia: A systematic review and meta-analysis. Ageing Research Reviews 97 2024, 102312. [Google Scholar] [CrossRef] [PubMed]
- Fratiglioni, L.; Paillard-Borg, S.; Winblad, B. An active and socially integrated lifestyle in late life might protect against dementia. The Lancet Neurology 2004, 3(6), 343–353. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, J. S.; Zuidersma, M.; Oude Voshaar, R. C.; et al. Social relationships and cognitive decline: A systematic review and meta-analysis. Ageing Research Reviews 22 2015, 39–57. [Google Scholar] [CrossRef] [PubMed]
- Robert, P.; Onyike, C. U.; Leentjens, A. F.; Dujardin, K.; Aalten, P.; Starkstein, S.; et al. Proposed diagnostic criteria for apathy in Alzheimer’s disease and other neuropsychiatric disorders. European Psychiatry 2009, 24(2), 98–104. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



