
Submitted:
01 January 2026
Posted:
02 January 2026
You are already at the latest version
Abstract
In people with dementia, malnutrition and dehydration are strongly associated with declines in physical function, increased susceptibility to infection, delirium, worsening behavioral and psychological symptoms of dementia (BPSD), and earlier hospitalization and institutionalization. Epidemiological and clinical studies in older adults and people with dementia consistently demonstrate that adequate intake of energy, protein, and fluids does not treat dementia itself, but plays a critical role in suppressing reversible factors that can rapidly exacerbate disease progression.However, many conventional nutrition education and dietary interventions implicitly assume cognitive abilities such as self-management of food intake, understanding of nutrients, and judgment in food selection. For people with dementia, these assumptions often render implementation and continuation difficult. As a result, an “implementation gap” emerges in which theoretically valid nutritional interventions fail to function effectively in real-world clinical and caregiving settings.The purpose of this paper is to reconceptualize dietary and nutritional interventions for people with dementia by systematically separating (1) core active ingredients from (2) elements that generate excessive cognitive and operational burden. By integrating existing guidelines, intervention studies, and clinical epidemiological research, we propose an implementation-adapted minimal model consisting of: (1) ensuring one protein item at each meal, (2) daily fluid intake of 1.2–1.5 liters, and (3) meal environment design that does not require choice or judgment.This model does not aim to directly modify the neurodegenerative pathology of dementia. However, by suppressing “progression accelerators” such as malnutrition, dehydration, infection, delirium, and BPSD, it offers high practical utility for both clinical practice and long-term care policy.
Keywords:
dementia
; dietary intervention
; nutrition
; malnutrition
; dehydration
; non-pharmacological intervention
; implementation-adapted intervention
; behavioral and psychological symptoms of dementia (BPSD)
; caregiving burden
1. Introduction
1.1. Malnutrition, Dehydration, and Outcomes in Dementia
In people with dementia, malnutrition and dehydration frequently occur due to reduced appetite, impaired swallowing, attentional deficits, changes in eating behavior, and difficulties adapting to the environment. These conditions are not merely accompanying symptoms; they are independent prognostic factors associated with functional decline, impaired immune function, delirium, worsening BPSD, increased risk of hospitalization, and mortality.
International guidelines for older adults consistently indicate that malnutrition and dehydration significantly increase the risk of functional decline and mortality (Volkert et al., 2019). More recently, guidelines specifically addressing nutrition and hydration management in people with dementia have been developed, clearly positioning nutritional care not as “supplementary care” but as “basic medical and caregiving intervention” in dementia (Volkert et al., 2024).
A critical point is that these findings do not claim that specific nutrients treat dementia. Rather, they demonstrate that malnutrition and dehydration act as conditions that discontinuously worsen the course of dementia through infection, delirium, falls, and BPSD. This relationship is schematically illustrated in Figure 1.
1.2. Limitations of Conventional Nutrition Education and Dietary Interventions
Against this background, various interventions—such as nutrition education, supplementation, and dietary planning—have been proposed. However, their reproducibility in real-world clinical and caregiving settings has not been consistently high.
The main reason is that conventional nutritional interventions rely on the following assumptions:
First, that individuals can self-manage food content and quantity.Second, that individuals can understand the importance of nutrients and adjust their choices accordingly.Third, that individuals can continuously make judgments at each meal.
All of these abilities strongly depend on attention, memory, and executive function, which are often compromised from the mild to moderate stages of dementia. As a result, nutritional interventions tend to become “correct but unworkable.”
This paper does not propose a new nutritional therapy. Rather, it aims to reorganize existing knowledge in a way that aligns with the cognitive realities of dementia and reconstructs it into a form that can actually function in practice.
2. Constraints in Dietary and Nutritional Interventions
2.1. Cognitive Constraints: Difficulties in Judgment, Choice, and Self-Management
In dementia, adjusting food intake, understanding nutritional balance, and making decisions among multiple options become increasingly difficult. In particular, decisions regarding “what and how much to eat” rely heavily on executive function and are therefore prone to early breakdown in dementia.
2.2. Behavioral and Environmental Constraints: Instability of Eating Behavior
Environmental changes, excessive stimulation, and experiences of failure during meals can easily trigger food refusal, selective eating, and BPSD. Excessive verbal prompting or instruction—even when well-intentioned—may amplify anxiety and confusion.
2.3. Nutritional Interventions as Implementation Failure
Thus, failures of nutritional interventions should be understood not as a lack of nutritional validity, but as a mismatch between design assumptions and patient characteristics.
3. Separating Active Ingredients from Excessive Burden
3.1. Core Active Ingredients in Dietary and Nutritional Interventions
Integrating the literature, the active ingredients of nutritional interventions for people with dementia can be summarized as follows:
- Securing adequate energy and protein
- Sustained fluid intake
- Prevention of acute deterioration due to malnutrition and dehydration
Figure 2 presents these active ingredients organized into a minimal, implementable model. Multinutrient interventions (e.g., LipiDiDiet) have demonstrated some suppression of functional decline in the prodromal stage of dementia (Soininen et al., 2017; 2021). One interpretation is that avoiding nutritional deficiency itself may be more important than specific components.
3.2. Excessive Implementation Burdens to Be Removed
In contrast, the following elements unnecessarily increase implementation burden:
- Detailed management at the level of individual nutrients
- Judgment and choice at every meal
- Self-recording of food intake
- Evaluation of achievement or intake levels
These elements should be intentionally removed.
4. Dementia-Adapted Dietary and Nutrition Intervention Model
4.1. Minimal Component ①: One Protein Item at Each Meal
At each meal, include one protein source (meat, fish, eggs, legumes, or dairy products) as the main dish. Quantity and nutritional calculation are not required. This is not intended to achieve a specific intake target, but rather to serve as an implementation guideline to avoid malnutrition.
Theoretical basis:
ESPEN guidelines indicate that protein deficiency in older adults and people with dementia is associated with functional decline (Volkert et al., 2019; 2024).
4.2. Minimal Component ②: Daily Fluid Intake of 1.2–1.5 L
Using water, tea, soup, etc., aim for a daily intake of 1.2–1.5 liters, divided across the day. Awareness of thirst is not assumed (medical judgment should take priority in cases such as heart failure or renal impairment).
Theoretical basis:
Dehydration is associated with delirium, hospitalization, and mortality risk (El-Sharkawy et al., 2015; Parkinson et al., 2023).
4.3. Minimal Component ③: A Decision-Free Eating Environment
Standardize menus, reduce choices, and maintain consistent meal times and locations. Meals are framed not as an individual management task, but as an environmental design task.
5. Implementation Protocol (Summary)
- Duration: Continuous
- Decision-maker: Caregivers and environment
- Recording: Simple checklist only
- Progression: Do not increase complexity
6. Implications for Research, Practice, and Policy
The novelty of this paper lies not in proposing new nutrients or therapeutic diets, but in reconstructing existing knowledge in a manner adapted to the cognitive and emotional constraints of dementia. Figure 3 illustrates the differences between conventional nutritional support and the dementia-adapted approach proposed here. In particular, it visualizes that implementation failure arises from design assumptions rather than nutritional content. The value of nutritional interventions should be evaluated not by cognitive outcomes, but by cost-related outcomes such as delirium, BPSD, hospitalization, and caregiving breakdown.
7. Conclusion
Dietary and nutritional interventions for people with dementia should be redefined not as treatment, but as control of conditions that accelerate deterioration. This paper presents a minimal, implementation-adapted model that can function sustainably in real-world care settings.
Appendix
Dietary and Nutritional Support
Implementation Manual for People with Dementia
(Implementation Guide for Care and Support Settings)
————————————————————————————————————
- Purpose and Positioning
This manual aims to provide implementation guidelines for delivering dietary and nutritional support to people with dementia in a safe and sustainable manner in both home-based and caregiving settings.
This program does not aim to provide nutrition education or to enhance self-management abilities.
Rather, it is an implementation-adapted non-pharmacological intervention whose primary objective is to suppress the following “progression accelerators”:
- Malnutrition
- Dehydration
- Delirium and BPSD
- Infection, falls, and hospitalization
This manual is intended for use by:
- Care staff working in long-term care facilities or home care settings
- Family caregivers supporting people with dementia
- Medical and welfare professionals who wish to integrate dietary and hydration management into daily care
Note:
- This manual is not a clinical trial protocol, but an implementation guide for routine care.
- It does not claim therapeutic effects of specific nutritional therapies or foods.
————————————————————————————————————
- 2.
- Target Population
Eligible Individuals
- People with mild to moderate dementia
- Individuals capable of oral intake
- Individuals for whom eating and drinking support can be provided in daily life
Exclusion / Cautionary Cases
- Severe dysphagia requiring specialized nutritional management
- Medically unstable acute conditions (e.g., severe infection, acute delirium)
- Cases in which specific food-related stimuli provoke marked refusal or agitation
Note:
- Final decisions should always prioritize clinical judgment.
- Even in advanced dementia, this approach may be flexibly applied as supportive eating care that respects the individual’s presence, without evaluating intake volume or reactions.
————————————————————————————————————
- 3.
- Fundamental Design Principles
This program is designed based on the following four principles.
1. Minimization of Cognitive Load
- Do not require nutritional knowledge or understanding
- Do not ask the individual to judge intake quantity or nutritional balance
- Do not require food selection by the individual
2. Ensuring Emotional Safety
- Do not evaluate meal quantity or eating behavior
- Do not reprimand, correct, or persuade
- If anxiety, confusion, or refusal is observed, immediately pause or scale down support
3. Predictability and Repetition
- Fix meal content, timing, and provision method as much as possible
- Avoid making meals “special events”
- Reduce statements such as “Today is special”
4. Caregiver- and Environment-Led Support
- Do not assume motivation, judgment, or self-management by the individual
- Value support that “remains valid even if the person cannot eat”
————————————————————————————————————
- 4.
- Overall Structure of Implementation
Recommended Frequency and Targets
- Meals: Three meals per day (frequency may be adjusted according to lifestyle)
- Fluid intake: Approximately 1.2–1.5 L per day, divided across time
- Verbal prompting and monitoring: As needed at each meal
Implementation Environment
- Familiar daily living environment
- Calm locations (avoid excessive stimulation and noise)
- Minimize movement, preparation, and choice requirements
————————————————————————————————————
- 5.
- Core Support Components (Three Mandatory Elements)
5.1 Ensuring One Protein Item at Each Meal
Purpose
- Prevention of malnutrition
- Suppression of muscle weakness and susceptibility to infection
Method
At each meal, include one of the following as the main dish:
- Meat or fish
- Eggs
- Legumes or soy products
- Dairy products
Note:
- Quantity, cooking method, and nutritional calculations are not required.
- Failure to finish the meal is not considered failure.
Example Verbal Prompts
- “I’ll just leave a little here for you.”
- “It’s okay to eat as much as you can.”
————————————————————————————————————
5.2 Distributed Daily Fluid Intake of 1.2–1.5 L
Purpose
- Prevention of dehydration
- Suppression of delirium, constipation, and infection
Method
- Use water, tea, soup, jelly drinks, etc.
- Do not request large volumes at once
- Provide fluids divided across meals and between meals
Note:
- Do not assume awareness of thirst.
- Accurate recording of intake volume is not mandatory.
Example Verbal Prompts
- “Shall we take just a little sip?”
- “I’ll leave this here for you.”
————————————————————————————————————
5.3 Designing a Decision-Free Eating Environment
Purpose
- Prevention of food refusal and confusion
- Prevention of BPSD triggers
Method
- Standardize menus
- Do not present choices
- Keep meal time and location as consistent as possible
Practices to Avoid
- Asking “Which would you like?”
- Presenting intake targets
- Instructing how to eat
————————————————————————————————————
- 6.
- Explicitly Excluded Interventions
The following are not included in this program:
- Nutrition education or explanatory guidance
- Interventions aimed at evaluating intake volume or nutritional balance
- Treating meals as “rehabilitation tasks”
- Engagement aimed at achieving meal completion or independent eating
Note:
This is not an exclusion of nutritional support itself, but a restructuring of its format.
This manual is not an intervention study designed to quantitatively verify the effects of specific dietary or nutritional interventions.Rather, it integrates existing guidelines, epidemiological evidence, and implementation research to present an implementation-adapted framework compatible with the cognitive and emotional constraints of dementia.
————————————————————————————————————
- 7.
- Adjustment and Discontinuation Criteria
Adjustable Elements
- Meal quantity (reduction is acceptable)
- Number of meals
- Provision method (texture, temperature, etc.)
Discontinuation Criteria
- Clear anxiety, refusal, or agitation
- Worsening of BPSD during meal situations
- Increased risk of aspiration
————————————————————————————————————
- 8.
- Safety and Burden Management
- Physical risks are relatively low
- The greatest risk is over-intervention
- Minimize caregiver guilt
- A day without eating is not considered failure
————————————————————————————————————
- 9.
- Consistency with Existing Evidence
This manual is based on existing evidence regarding:
- Associations between malnutrition/dehydration and mortality, hospitalization, and functional decline
- Nutrition and hydration management guidelines for people with dementia
- Evidence that dehydration triggers delirium and BPSD
These findings are reorganized to align with the implementation realities of dementia care.
————————————————————————————————————
- 10.
- Use in Research and Practice
Research Applications
- Supplementary materials describing intervention content
- Clarification of implementation methods and fidelity
Practical Applications
- Simplified manuals for care staff
- Handout materials for family caregivers
- Shared policy documents for dietary support
————————————————————————————————————
End of Appendix Manual
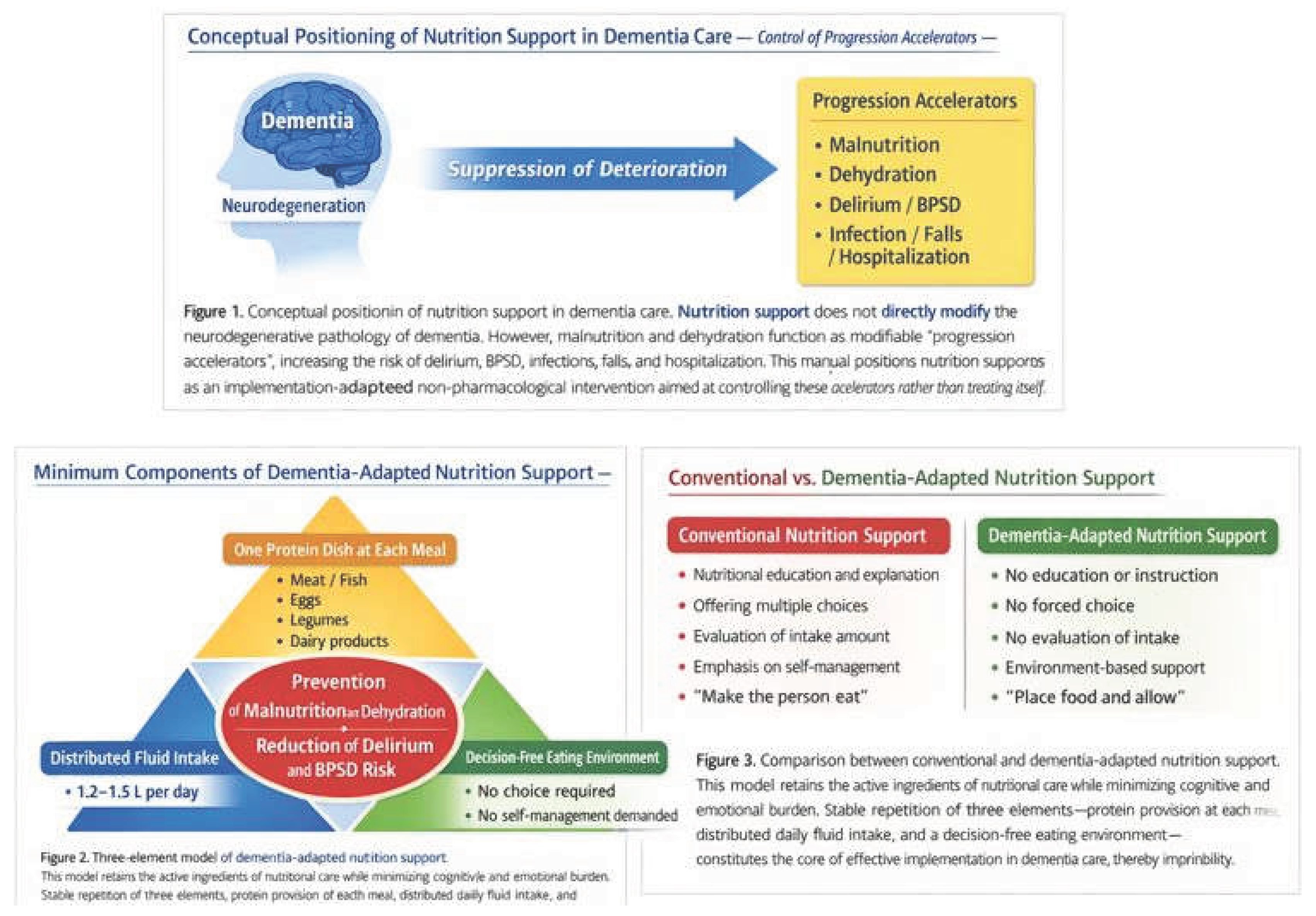
Figure 1. Conceptual positioning of nutrition support in dementia care. Nutrition support does not directly modify the neurodegenerative pathology of dementia. However, malnutrition and dehydration function as modifiable “progression accelerators,” increasing the risk of delirium, BPSD, infections, falls, and hospitalization. This manual positions nutrition support as an implementation-adapted non-pharmacological intervention aimed at controlling these accelerators rather than treating dementia itself.
Figure 2. Three-element model of dementia-adapted nutrition support. This model retains the active ingredients of nutritional care while minimizing cognitive and emotional burden. Stable repetition of three elements—protein provision at each meal, distributed daily fluid intake, and a decision-free eating environment—constitutes the core of effective implementation in dementia care.
Figure 3. Comparison between conventional and dementia-adapted nutrition support. Conventional nutrition interventions implicitly rely on cognitive abilities such as understanding, decision-making, and self-management, which are frequently impaired in dementia. Dementia-adapted nutrition support removes these assumptions and shifts responsibility from the individual to the care environment, thereby improving feasibility and sustainability.
References
- El-Sharkawy, A. M.; Watson, P.; Neal, K. R.; Ljungqvist, O.; Maughan, R. J.; Lobo, D. N. Hydration and outcome in older patients admitted to hospital (The HOOP study). Age and Ageing 2015, 44(6), 943–947. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Huntley, J.; Sommerlad, A.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. The Lancet 2020, 396(10248), 413–446. [Google Scholar] [CrossRef] [PubMed]
- Oh, E. S.; Fong, T. G. Delirium in older persons: Advances in diagnosis and treatment. JAMA 2017, 318(12), 1161–1174. [Google Scholar] [CrossRef] [PubMed]
- Parkinson, E.; Crichton, M.; Horne, R.; et al. Low-intake dehydration and clinical outcomes in older adults: A systematic review and meta-analysis. Clinical Nutrition 2023, 42(4), 728–738. [Google Scholar] [CrossRef]
- Soininen, H.; Solomon, A.; Visser, P. J.; Hendrix, S. B.; Blennow, K.; Kivipelto, M.; LipiDiDiet Clinical Study Group. 24-month intervention with a specific multinutrient in people with prodromal Alzheimer’s disease (LipiDiDiet): A randomised, double-blind, controlled trial. The Lancet Neurology 2017, 16(12), 965–975. [Google Scholar] [CrossRef] [PubMed]
- Soininen, H.; Kivipelto, M.; Solomon, A.; et al. Long-term effects of the LipiDiDiet intervention in people with prodromal Alzheimer’s disease. Alzheimer’s & Dementia 2021, 17(4), 1–11. [Google Scholar] [CrossRef]
- Volkert, D.; Beck, A. M.; Cederholm, T.; Cereda, E.; Cruz-Jentoft, A.; Goisser, S.; Bischoff, S. C. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clinical Nutrition 2019, 38(1), 10–47. [Google Scholar] [CrossRef] [PubMed]
- Volkert, D.; Chourdakis, M.; Faxen-Irving, G.; Frühwald, T.; Landi, F.; Suominen, M. H.; ESPEN. ESPEN guideline on nutrition and hydration in dementia. Clinical Nutrition 2024, 43(2), 159–190. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



