
Submitted:
10 September 2024
Posted:
10 September 2024
You are already at the latest version
Abstract
Background/Objectives: Caregivers play an important role in supporting care recipients to navigate their health needs including adherence to dietary recommendations which are complex and multifaceted. The study aimed to i) describe the nutrition knowledge of caregivers of people with chronic kidney disease (CKD), and ii) explore caregivers’ perception of their role in providing healthy meals and nutrition support for care recipients. Methods: Caregivers (n=78) of people with stage 1-5 CKD or post-transplant were recruited from a single centre. A sequential mixed-methods approach was used. Nutrition knowledge was assessed with the revised General Nutrition Knowledge questionnaire. Theory informed semi-structured interviews in a sub-sample (n=12) explored caregiver perception. Results: Most caregivers were female (75.6%) caring for a male care recipient (87%; aged 74 (66;80) yrs.). Caregivers (75.6%) provided a meal ≥6 times/week to their care recipient and had moderate nutrition knowledge (66.1 (60.5; 73.9) %). Four themes emerged describing caregivers’ perception on meal provision and nutrition support including i) food literacy skills are valued, ii) social support is important, iii) caregivers’ sense of social responsibility, and iv) meal provision is complex and dynamic. Conclusions: Caregivers have moderate nutrition knowledge; they want to provide healthy meals and support to care recipients to adhere to dietary recommendations. Targeted, co-designed nutrition education programs for caregivers may enhance nutrition care delivery to people with CKD.
Keywords:
diet therapy
; family caregiver
; food literacy
; nutrition knowledge
; meal provision
; dietary adherence
1. Introduction
Chronic kidney disease (CKD) affects more than 10% of the Australian population and is the 12th leading cause of mortality globally [1,2]. CKD not only diminishes quality of life and life expectancy but is also exacerbated by the complex interplay of comorbidities that influence disease onset, management, and progression [3]. These comorbidities, such as hypertension, diabetes, and cardiovascular disease, not only increase the risk of developing CKD but also accelerate its progression [4]. Addressing comorbidities through lifestyle modifications, including a focus on diet, is a crucial component in the management of CKD [5,6]. Literature reports that low diet quality is frequently observed in people with CKD [7,8,9] and improved diet quality can achieve better disease control [10]. Furthermore, longitudinal cohort studies have found that high quality diets can also prevent the progression of CKD [11,12]. In such cases the management of an individual’s health is achieved through promoting healthy dietary patterns and eating in line with general healthy eating principles [13]. However, in many cases, healthy eating may not only be a clinical challenge, but also a behavioural challenge involving not just the person with CKD, but those involved in their health care, namely their caregivers and family [14,15].
The cognitive and physical decline associated with CKD, often means individuals will require the support of a caregiver [16]. A caregiver is an unpaid and untrained individual that is primarily responsible for helping a patient cope with and manage their disease [17]. Within this role, a caregiver often assumes responsibility for an individual’s health care, including diet [16]. The provision of food that aligns with recommendations to manage disease is often a task that caregivers fulfill and can pose significant challenges, necessitating increased support and resources [18]. The renal diet is perceived by caregivers to be overwhelming, frustrating and emotionally demanding [19]. To enable caregivers to provide the required dietary support, a foundation of knowledge on healthy eating and food choices is beneficial. The nutrition knowledge of caregivers of people with CKD is unclear and remains to be elucidated.
Higher levels of nutrition knowledge have been associated with healthier food choices, particularly fruit and vegetable intake in adults [20]. A study involving Australian caregivers of individuals with intellectual disabilities revealed that these caregivers possess lower nutrition knowledge when compared to the general public, potentially affecting their ability to plan and provide nutritious meals for their care recipients [21]. To better understand caregivers’ ability to provide dietary support, it is crucial to gain an understanding of their existing nutrition knowledge, as well as their perceptions on their role in supporting their care recipient to adhere to dietary recommendations. Therefore, this study aimed to examine the nutrition knowledge of caregivers for individuals with CKD, as well as explore caregivers’ perceptions of their role to provide healthy meals and nutrition support to their care recipients.
2. Materials and Methods
2.1. Study Design
This study had a mixed-method sequential study design (quantitative data collection preceded interviews) and recruited caregivers of people with CKD attending renal outpatient clinics within the Sunshine Coast Hospital and Health Service (SCHHS). Ethics was obtained from the Human Research and Ethics Committee of The Prince Charles Hospital (LNR/2018/QPCH/47886) and the Ethics Committee of The University of Sunshine Coast (A191219).
2.2. Participants and Procedure
Individuals with CKD, not requiring dialysis, stages G3a to G5 and post-kidney transplant, were approached for recruitment via convenience sampling from two renal units in a regional health service between May and December 2021. Eligible patients were identified and provided with written information on the study to provide to their caregivers. The caregivers of those patients that provided written consent were approached to participate in the study. Written consent was obtained from caregivers prior to inclusion to the study. Exclusion criteria included patients receiving dialysis, <18 year of age, caregivers who were non-English speaking or those with cognitive impairment. Patients were screened for eligibility and a final sample of 78 participants were included, see Figure 1.
After inclusion, caregivers were asked to complete a survey comprised of sociodemographic characteristics, caregiving relationship, and nutrition knowledge questionnaire. Care recipient information was collected from hospital medical records including age, gender, cause of CKD, transplant date, eGFR, comorbidity status and smoking status.
2.3. Nutrition Knowledge
Nutrition knowledge was measured with the revised Australian general nutrition knowledge questionnaire (GNKQ). The GNKQ is a validated nutrition knowledge questionnaire for adults [22] which has been revised and validated to an Australian population based on the Australian dietary guidelines [23]. It is a self-administered, 117-item questionnaire comprised of four sub-sections assessing different areas of nutrition knowledge namely; i) the Australian Dietary Guidelines (19 items scoring 19 points, ii) food groups and food sources of nutrients (9 items, 53 points), ii) knowledge of food healthy choices (10 items, 10 points), and iv) the relationship between diet and disease (9 items, 35 points) with an overall maximum score of 117 [23]. In the current study, a percentage of less than 50% for the full questionnaire or any sub-section were deemed low or inadequate nutrition knowledge, a percentage of 50 to 74% as moderate nutrition knowledge, and a percentage of 75% or higher as a high level of nutrition knowledge.
2.5. Caregiver Perception on Food Provision and Delivery of Nutrition Support
Semi-structured telephone interviews consisting of a series of open-ended questions, informed by the theory of planned behaviour [24], explored caregivers’ perceptions on their role in supporting their care recipients to follow dietary recommendations, and the provision of healthy meals to their care recipients. Questions were developed through a collaborative process involving dietitian clinicians with expertise in providing nutrition care to people living with CKD (GL and CM, over 40 years clinical experience as renal dietitians) and nutrition researcher with expertise in development of theory-informed interview questions (HHW), see supplementary materials Table S1 for interview questions.
2.6. Analysis
2.6.1. Quantitative Analysis
Statistical analysis was performed using IBM SPSS statistics package for Windows version 25 (Chicago, USA). Data was analysed for normality and appropriate descriptive statistics were used. Continuous data is presented as means and standard deviations for parametric variables or median and interquartile ranges for non-parametric variables. Categorical variables are presented as percentage of total group and frequencies.
Associations between sociodemographic information (gender, age, education level) and nutrition knowledge were explored using Spearman rank correlations. Relationships between care recipient comorbidities and caregiver nutrition knowledge were explored with chi-squared tests. Wilcoxon signed ranks test explored differences between nutrition knowledge sub-section scores. Student’s t-tests were used to explore differences in nutrition knowledge scores between caregivers that have received dietary advice from a dietitian compared to those that haven’t received dietary advice from a dietitian. Significance was set at p<0.05.
2.6.2. Qualitative Analysis
Individual telephone interviews were conducted at a predetermined mutually convenient time by one researcher (GL) in October 2022 and lasted between 9 and 24 minutes. Interviews were audio-recorded and transcribed verbatim.
Transcripts were inductively analysed thematically according to the six-phase process of Braun and Clarke [25], namely familiarization with the data, initial coding, identifying themes, reviewing themes, defining and naming themes, and writing up the findings.
Data analysis employed a comprehensive and iterative approach. Following each interview, the interviewer (GL) reflected and recorded reflexive interview notes. Two researchers (CM, HHW) immersed themselves in the data by repeatedly listening to and transcribing the recordings. Three researchers (GL, CM, & HHW) independently coded two transcripts, compared, and reconciled their codes to reach consensus. Using Microsoft Excel, coding continued with GL and CM independently analysing the remaining transcripts. Codes were organised into sub-themes which were identified and defined based on their combined analysis. Finally, GL and CM (qualitative analysis expertise) engaged in an iterative process to refine sub-themes into final themes. Triangulation of analysis through review of final themes by HHW (qualitative analysis expertise) further strengthened the analysis. Additionally, reflexive interview notes informed the finalisation of themes and sub-themes, with all researchers reaching agreement on the final themes.
3. Results
3.1. Participant Characteristics
Caregiver characteristics are summarised in Table 1. A typical caregiver was female, aged 65 years or older caring for a spouse or partner. The majority always (64.1%) or usually (30.8%) bought groceries for their care recipient.
Food preparation was completed by 75.6% of caregivers ≥6 times a week for their care recipient and 3-5 times a week by 19.2%. Caregivers’ perceptions of their own health were varied, with 37.7% viewing it as very good or excellent, 36.4% as good, and 26% as fair or poor.
The typical care recipient was a 74-year-old male presenting with multimorbidity, see Table 2. The most common self-reported cause of CKD was type 2 diabetes mellitus followed by cardiovascular disease.
3.2. Nutrition Knowledge
Less than half of caregivers (44.9%) reported to have received dietary advice on renal nutrition to support the management of their care recipient’s kidney disease. The top four sources of dietary advice were a dietitian (32.1%), nephrologist (15.4%), general practitioner (14.1%), and nurse practitioner (10%).
Caregivers’ overall nutrition knowledge was moderate with significant (p<0.05) differences in nutrition knowledge on sub-sections relating to knowledge on food choices as well as the relationship between diet and disease versus knowledge on the Australian dietary guidelines and food groups and nutrients, Table 3.
No difference was found in nutrition knowledge between caregivers who reported to have received dietary advice versus those who have not received dietary advice from a health professional (66.2% vs 64.1%, p=0.273).

Table 3.
Caregiver overall nutrition knowledge and sub-section nutrition knowledge(n=78).
| Variable | Raw score | Percentage |
|---|---|---|
| Overall nutrition knowledge 1 | ||
| Sub-section 1. Australian dietary guidelines | 12 (11; 13.25) | 63.2 (57.9; 69.7) a |
| Sub-section 2. Food groups and nutrients | 33.5 (28; 39) | 63.3 (52.8; 73.6) b |
| Sub-section 3. Knowledge on food choices | 7 (6; 8) | 87.5 (75.0; 100.0) c |
| Sub-section 4. Relationship between diet and disease |
25 (23; 28.0) | 71.4 (65.7; 80.0) d |
Data are expressed as median and interquartile ranges (25th; 75th). 1 Total score out of 115 due to omission of two questions in sub-section 3, sub-section 1 scored out of 19 points, sub-section 2 scored out of 53 points, sub-section 3 scored out of 8, and sub-section 4 scored out of 35 points. a and b Z=-2.000, p=0.046; a and c Z=-6.480, p=0.000, a and d Z =-3.205, p=0.001, b and c Z=-6.640, p=0.000, b and d Z=-5.192, p=0.000, c and d Z=-5.965, p=0.000.
3.2.1. Correlations
Positive associations were found between female gender and overall nutrition knowledge (r=0.317, p=0.005), knowledge on the relationship between diet and disease (r=0.382, p<0.001), was well as knowledge on food groups and nutrients (r=0.225 p=0.048). Age was positively associated with knowledge on the relationship between diet and disease (r=0.273, p=0.016), and level of education was associated with knowledge on food groups and nutrients (r=0.298, p=0.01).
Caregivers of individuals with type 2 diabetes mellitus had an adequate knowledge on carbohydrate containing foods whereas caregivers of CKD people without diabetes did not (c2=7.412, p=0.025). However, no relationship was found for adequacy of knowledge on fibre and sugar content between the same groups. Similarly, no relationship was found for adequacy of knowledge on salt content of food products in caregivers of care recipients with or without hypertension (c2=0.724, p=0.395).
3.2. Caregiver Perception on Meal Provision and Providing Nutrition Support.
Out of the n=23 caregivers who expressed interest in participating in the qualitative component of the study, n=12 was included (100% female, 67.5 (range 38-74) yrs.). Three caregivers declined to partake in semi-structured interviews when contacted by the research team and eight did not respond after three email invitations.
Four themes emerged describing caregivers’ perceptions on provision of healthy meals and support to adhere to dietary recommendations, namely i) food literacy skills are valued (meal planning and preparation, translating nutrition knowledge into mealtimes, access to credible nutrition information, practical advice and resources), ii) social support is important (timely and accessible health services, trusting relationships with health professionals, support from family, friends, and care recipient, community support programs), iii) caregivers’ sense of social responsibility (caring for self and family, responsible citizenship), and iv) meal provision is complex and dynamic (access and availability of healthy foods, creating an inclusive eating environment, budget constraints and life challenges, managing multifaceted dietary needs, personal beliefs about diet, health and wellbeing). Figure 2 illustrates the interaction between key factors which activates or hampers caregivers’ behaviour. Indicative quotes for each theme are illustrated in supplementary materials Table S2.
Food literacy skills was a key determinant of caregivers’ ability to provide healthy meals. These include ability to plan and prepare meals and translate nutrition knowledge into meal provision. In fact, those with strong food literacy were able to adapt recipes, utilise seasonal produce, and enable provision of nutritious meals despite budgetary constraints. Moreover, nutrition knowledge and access to credible information provided a theoretical knowledge base with regards to healthy eating for CKD. Access to written material, practical resources such as recipes or food lists, and cooking demonstrations were all mentioned important to inform meal provision. Advice and information provided from a renal specialist dietitian and other medical team members were highly valued.
Social support enabled caregivers to provide healthy meals. Caregivers found it easier to provide a healthy diet to their care recipient when the care recipient also valued this lifestyle choice, and they had the support of family and friends. Consistent and positive reinforcement of dietary recommendations by all health professionals was reported to enhance care recipient motivation for adherence. However, inconsistent advice on dietary management of CKD resulted in confusion and reduced confidence in meal provision. Timely access to health services was valued and forming trusting relationships with health professionals enabled care recipients to follow dietary recommendations and enhanced caregivers’ confidence in supporting adherence to these recommendations. The need for greater access to reliable nutrition information was expressed, as well as inclusion in nutrition education sessions, and flexibility in the mode of service delivery such home visits, telehealth and virtual education sessions to reduce travel time.
Caregivers exhibited a deep sense of social responsibility by consistently striving to provide nutritious meals for their care recipients and where relevant, the rest of their family members. This social responsibility was likely underpinned by the fact that most caregivers were caring for a spouse, partner, and/or children. Responsible citizenship was demonstrated by supporting farmers’ markets to purchase locally grown food and one care recipient expressed the importance to look after a new kidney post-transplant through supporting their care recipient to engage in health behaviours.
Meal provision by caregivers was recognized as a dynamic and intricate task due to the often complex and multifaceted dietary requirements of care recipients. These requirements extended beyond kidney disease management to encompass the nutritional needs associated with other chronic conditions. Additionally, caregivers discussed juggling the dietary requirements and food preferences of other household members, budgetary constraints, and time factors. The use of online meal delivery services and healthy preprepared meals helped to provide healthy meals when caregivers were time poor. Budget and financial constraints influenced the types of food purchased by care recipients, who emphasized the importance of strong food literacy, especially during times of financial hardship. In fact, budget constraints were viewed as a barrier to providing healthy meals. Caregivers were able to provide healthy diets for their care recipients by leveraging awareness of community food programs and access to affordable food sources. These resources included homegrown produce, affordable and fresh produce from local farmers markets and community food assistance programs.
Caregivers consistently emphasized the positive impact of following a healthy diet and adhering to dietary recommendations on overall health and well-being as well as disease management. Given that several care recipients presented with multimorbidity, caregivers often referred to the role of food in the management of other chronic disease such as type 2 diabetes. Specific ideas and beliefs on what constitute a healthy diet was expressed and the type of food provided to care recipients were influenced by caregivers’ personal food beliefs and preferences. The importance to balance food enjoyment with disease management was highlighted. An emotional burden of feelings of guilt when favourite foods were not allowed was expressed by caregivers. This was managed by being mindful of incorporating favourite foods into the diet to enhance quality of life and enjoyment for their care recipient.
4. Discussion
The aim of this study was to investigate the nutrition knowledge of caregivers of people with CKD and explore the perception of their role in providing healthy meals and nutrition support to their care recipients. Key findings include caregivers’ overall nutrition knowledge was moderate while knowledge on healthy food choices was high. Female gender, older age, and higher education level were all associated with greater nutrition knowledge. Key themes identified to influence caregivers’ meal provision and nutrition support behaviors highlighted food literacy, ability to manage complex and multifaceted dietary needs, and social support as important determinants.
The nutrition knowledge of this cohort of caregivers was moderate which is similar to other general population groups [23]. Knowledge on the Australian dietary guidelines (ADGs) as well as food groups and nutrients scored lower than other sub-sections on the nutrition knowledge survey in the current study. The ADGs are evidence-based population dietary guidelines promoting healthy eating patterns in order to reduce chronic disease risk [26] and manage non-communicable disease [27,28]. Adhering to healthy eating guidelines may reduce the risk of CKD and is promoted to manage early CKD to improve cardiometabolic health [8,29] and slow disease progression [30,31] amongst other health benefits [29,32]. Nutrition knowledge on food groups and nutrients provides insight into the ability of caregivers to identify key foods and nutrients for the management of not only CKD but also other chronic disease such as hypertension and diabetes [33,34]. Sociodemographic factors such as age, gender, education, and specialist dietary needs have been associated with nutrition knowledge [35] which is in agreement with the current study. Important to note was that male care recipients, younger age, and lower education level were associated with lower nutrition knowledge and highlights a need for targeted nutrition education programs for these caregivers.
More than half of care recipients in the current study presented with multimorbidity, adequate understanding of healthy eating patterns, food groups and sources of key nutrients by caregivers is important as it may influence the types of food provided as well as adherence of care recipients [36]. In fact, caregivers who valued the role of nutrition in the management of CKD and overall health had a positive attitude towards providing healthy meals to care recipients. Additionally, understanding the link between nutrition and disease management empowered caregivers to support and motivate their care recipients to make healthy food choices. Caregivers consistently highlighted the belief that adhering to dietary recommendations would have a positive impact on overall health and wellbeing and non-adherence results in negative health outcomes for their care recipients. Our findings are in accordance with others [37,38] where caregivers and/or care recipients agree adjusting dietary behavior are more likely when there is a strong belief in the health consequences associated with dietary adherence [39,40,41]. Therefore, knowledge on general healthy eating principles and dietary recommendations for the management of CKD is vital to empower caregivers to plan and provide appropriate meals and enhance adherence to dietary recommendations of care recipients.
Acknowledging that diet-related behavior is influenced by more than just nutrition knowledge [35] the current study identified several factors influencing the meal provision and nutrition support behavior of caregivers. Food literacy and access to reliable nutrition information was reported to play an important role in caregivers’ perceived ability to adequately support care recipients to adhere to dietary recommendations for kidney health in the current study. Similarly, Rezaie [42] reported caregiver access to adequate nutrition information and dietetic services was vital to enable them to provide the required nutrition support for care recipients receiving hemodialysis treatment. The sentiment to involve caregivers in nutrition education sessions were echoed in people with early CKD. Carers were described as gatekeepers to change, playing a role in decision making on food choices, cooking and meal planning [37,43]. Cicolin et al. [44] found family carers improved dietary adherence in hemodialysis patients as carers provided patient support, filled knowledge gaps, and reminded them of dietary restrictions. In the current study, caregivers expressed the need for individualized and in-time access to credible nutrition information. The mode and format of delivery, as well as type of nutrition information required differed based on existing nutrition knowledge and skills. A systematic review evaluating educational interventions aimed at primary or secondary prevention of CKD found multifaceted educational interventions that are interactive and include individual as well as group participation was most promising to improve self-management of people living with CKD [45]. It can be argued that future interventions should include caregivers given their integral role in the translation of dietary recommendations at home. In fact, the need for caregiver inclusion in nutrition education session is not new [46] and seems to remain an unmet need. Donald et al. [18] identified key characteristics of desired self-management interventions through a qualitative exploration into the needs of people living with CKD and their caregivers. Timely access to credible, understandable, and meaningful information was highlighted as an unmet need and practical support from family carers was valued as key drivers of disease self-management. Of note is that caregivers in the current study spoke about the challenges faced to provide healthy meals in the face of rising living costs. Those reporting sound food literacy skills were able to overcome budgetary constraints as a hurdle to providing healthy meals. However, those reporting poor cooking skills and lacked confidence in translating nutrition information and recommendation to meal provision raised the need for practical nutrition resources and training sessions such as cooking demonstrations. Our findings highlight the need for nutrition programs co-designed by caregivers to enhance food literacy skills and ensure in-time access to individualized nutrition information, particularly in the current economic environment with rising food and living costs [40,47].
Most caregivers in our study were partners or spouses of their care recipients, positioning them not only as integral members of the care team but also as influential figures within the family dynamic, directly shaping social and subjective norms. Caregivers had significant involvement in grocery shopping and meal preparation highlighting their instrumental role in providing nutritional support to their care recipient. In fact, others have shown a positive attitude towards dietary change in people with CKD is associated with social expectations and social support [38,48]. Similar findings have been reported in other clinical populations. For example, an umbrella review on factors influencing diabetes self-management in adults, discussed the blanket success of social and cultural support in disease management in that positive social influences (roles and norms) were found to facilitate better diabetes self-management [48]. A study by Yehle et al. echoed the importance of social support to enhance dietary adherence when examining coronary heart disease patients’ views of dietary adherence and a supporting web-based tool [49]. A key theme that emerged in the care model was that social support makes dietary adherence easier for the patient [49]. Similarly, we found that social support in the form of caregivers can make dietary adherence easier for care recipients. In addition, caregivers play an important role in incorporate favorite foods while balancing dietary needs of care recipients, as well as considering the rest of the household’s dietary needs and preferences [37,40]. This approach ensures enjoyable mealtimes for all and contributes to a good quality of life, aligned with caregiver’s desire to balance dietary compliance with food enjoyment. Finally, consistent messages from health professionals regarding the role of nutrition in management of CKD was key to motivate care recipients to adhere to dietary recommendations, as well as enhance caregivers’ confidence in providing appropriate meals and nutrition support which is in agreement with the literature [18,38,46].
4.1. Strengths and Limitations
Strengths include using a validated tool to assess general nutrition knowledge and health literacy of caregivers. A robust qualitative analysis process was followed, and theory informed interview questions were used to describe caregivers’ perception on meal provision and nutrition support. The study was undertaken in a single health service which limits the generalizability of the findings. Due to the use of convenience sampling, selection bias may result, and results should be interpreted with care. Most participants were white female caregivers which limits generalizability to male caregivers or carers from minority groups. Confirmation bias may occur during interpretation of study data; however, research rigor was employed during qualitative analysis using an iterative process and researcher triangulation in finalizing qualitative themes. Two questions in the sub-section on knowledge on food choices of the general nutrition knowledge questionnaire were omitted by human error. One question was on interpretation of the health star rating, however there was another question on the same topic which captured caregivers’ ability to interpret the health star rating. One question was on label reading, asking to identify the product with the highest energy content per 100 grams. The relative percentage of the sub-section result, and overall nutrition knowledge result was adapted accordingly, however, findings need to be interpreted with care as knowledge on food choices may be positively skewed.
5. Conclusions
This study revealed that caregivers of individuals with CKD or renal transplant recipients exhibit moderate overall general nutrition knowledge and report significant responsibility for meal provision to their care recipient. Nutrition knowledge formed the theoretical basis from which meals were provided while sound food literacy skills alongside adequate social support reduced caregiver burden to provide healthy meals. These findings present a valuable opportunity to leverage caregivers’ decision making, influence, and social support in helping care recipients to adhere to dietary recommendations. There is a need for targeted, co-designed nutrition intervention programs for caregivers of individuals with kidney disease to empower them with the knowledge and food literacy skills to effectively assist their loved ones in managing their condition through dietary change.
Supplementary Materials
The following supporting information can be downloaded at: preprints.org, Supplementary materials Table S1: Semi-structured interview questions; Table S2: Identified themes describing caregiver perception on meal provision and nutrition support to care recipients with indicative quotes..
Author Contributions
Paper conceptualization, H.H.W and N.G; methodology, H.H.W, C.M, G.L, L.D; formal analysis, H.H.W, L.D, C.M, G.L; investigation, G.L, L.D; resources, N.G, H.H.W; data curation, G.L, H.H.W; writing—original draft preparation, H.H.W, L.D and G.L; writing—review and editing, N.G, C.M; visualization, H.H.W and G.L; supervision, H.H.W, N.G; project administration, H.H.W, N.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of the Prince Charles Hospital (project code 47886, 11 March 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting reported results are available upon reasonable request and in accordance with the ethical principles.
Acknowledgments
The research team would like to acknowledge the contributions of Andrea Pollock, Pamela Gordon, and Yusuf Eqbal in participant recruitment and data curation. This article is a revised and expanded version of a paper entitled ‘Caregivers of people with chronic kidney disease: an untapped resource to improve person-centred care?’, which was presented at the Dietitians Australia annual conference, Brisbane, Queensland, Australia on 20 August 2024 [50].
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Collaboration, G.C.K. Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709-733. [CrossRef]
- Australian Institute of Health and Welfare. Chronic kidney disease: Australian facts; AIHW: Canberra, 2023.
- Tonelli, M.; Wiebe, N.; Guthrie, B.; James, M.T.; Quan, H.; Fortin, M.; Klarenbach, S.W.; Sargious, P.; Straus, S.; Lewanczuk, R.; et al. Comorbidity as a driver of adverse outcomes in people with chronic kidney disease. Kidney Int 2015, 88, 859-866. [CrossRef]
- Fraser, S.D.; Roderick, P.J.; May, C.R.; McIntyre, N.; McIntyre, C.; Fluck, R.J.; Shardlow, A.; Taal, M.W. The burden of comorbidity in people with chronic kidney disease stage 3: a cohort study. BMC nephrology 2015, 16, 193. [CrossRef]
- Kalantar-Zadeh, K.; Jafar, T.H.; Nitsch, D.; Neuen, B.L.; Perkovic, V. Chronic kidney disease. Lancet 2021, 398, 786-802. [CrossRef]
- Kaesler, N.; Baid-Agrawal, S.; Grams, S.; Nadal, J.; Schmid, M.; Schneider, M.P.; Eckardt, K.U.; Floege, J.; Bergmann, M.M.; Schlieper, G.; et al. Low adherence to CKD-specific dietary recommendations associates with impaired kidney function, dyslipidemia, and inflammation. Euro J Clin Nut 2021, 75, 1389-1397. [CrossRef]
- Fernandes, A.S.; Ramos, C.I.; Nerbass, F.B.; Cuppari, L. Diet Quality of Chronic Kidney Disease Patients and the Impact of Nutritional Counseling. J Renal Nut 2018, 28, 403-410. [CrossRef]
- Bowden, K.; Gray, N.A.; Swanepoel, E.; Wright, H.H. A Mediterranean lifestyle is associated with favourable cardiometabolic markers in people with non-dialysis dependent chronic kidney disease. J Nutr Sci 2021, 10, e42. [CrossRef]
- Chan, C.H.; Conley, M.; Reeves, M.M.; Campbell, K.L.; Kelly, J.T. Evaluating the Impact of Goal Setting on Improving Diet Quality in Chronic Kidney Disease. Frontiers Nut 2021, 8, 627753. [CrossRef]
- Chauveau, P.; Aparicio, M.; Bellizzi, V.; Campbell, K.; Hong, X.; Johansson, L.; Kolko, A.; Molina, P.; Sezer, S.; Wanner, C.; et al. Mediterranean diet as the diet of choice for patients with chronic kidney disease. Nephrol Dial Transplant 2018, 33, 725-735. [CrossRef]
- Dunkler, D.; Kohl, M.; Teo, K.K.; Heinze, G.; Dehghan, M.; Clase, C.M.; Gao, P.; Yusuf, S.; Mann, J.F.; Oberbauer, R. Dietary risk factors for incidence or progression of chronic kidney disease in individuals with type 2 diabetes in the European Union. Nephrol Dial Transplant 2015, 30 Suppl 4, iv76-85. [CrossRef]
- Hu, E.A.; Coresh, J.; Anderson, C.A.M.; Appel, L.J.; Grams, M.E.; Crews, D.C.; Mills, K.T.; He, J.; Scialla, J.; Rahman, M.; et al. Adherence to Healthy Dietary Patterns and Risk of CKD Progression and All-Cause Mortality: Findings From the CRIC (Chronic Renal Insufficiency Cohort) Study. American J Kidney Dis 2021, 77, 235-244. [CrossRef]
- Dunkler, D.; Dehghan, M.; Teo, K.K.; Heinze, G.; Gao, P.; Kohl, M.; Clase, C.M.; Mann, J.F.; Yusuf, S.; Oberbauer, R. Diet and kidney disease in high-risk individuals with type 2 diabetes mellitus. JAMA 2013, 173, 1682-1692. [CrossRef]
- Pereira, R.A.; Alvarenga, M.S.; Avesani, C.M.; Cuppari, L. Strategies designed to increase the motivation for and adherence to dietary recommendations in patients with chronic kidney disease. Nephrol Dial Transplant 2021, 36, 2173-2181. [CrossRef]
- Notaras, S.; Conti, J. A qualitative analysis of eating behaviour change for patients with diabetes and non-dialysis dependent chronic kidney disease stages 4-5. J Renal Care 2018, 44, 219-228. [CrossRef]
- Gayomali, C.; Sutherland, S.; Finkelstein, F.O. The challenge for the caregiver of the patient with chronic kidney disease. Nephrol Dial Transplant 2008, 23, 3749-3751. [CrossRef]
- Choi, S.; Seo, J. Analysis of caregiver burden in palliative care: An integrated review. Nurs Forum 2019, 54, 280-290. [CrossRef]
- Donald, M.; Beanlands, H.; Straus, S.; Ronksley, P.; Tam-Tham, H.; Finlay, J.; MacKay, J.; Elliott, M.; Herrington, G.; Harwood, L.; et al. Identifying Needs for Self-management Interventions for Adults With CKD and Their Caregivers: A Qualitative Study. American J Kidney Dis 2019, 74, 474-482. [CrossRef]
- Lambert, K.; Mansfield, K.; Mullan, J. How do patients and carers make sense of renal dietary advice? A qualitative exploration. J Renal Care 2018, 44, 238-250. [CrossRef]
- Wardle, J.; Parmenter, K.; Waller, J. Nutrition knowledge and food intake. Appetite 2000, 34, 269-275. [CrossRef]
- Hamzaid, N.H.; Flood, V.M.; Prvan, T.; O’Connor, H.T. General nutrition knowledge among carers at group homes for people with intellectual disability. JIDR 2018, 62, 422-430. [CrossRef]
- Parmenter, K.; Wardle, J. Development of a general nutrition knowledge questionnaire for adults. EJCN 1999, 53, 298-308. [CrossRef]
- Thompson, C.; Vidgen, H.A.; Gallegos, D.; Hannan-Jones, M. Validation of a revised General Nutrition Knowledge Questionnaire for Australia. Pub Health Nut 2021, 24, 1608-1618. [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ Behav Hum Dec Proc 1991, 50, 179-211. [CrossRef]
- Braun, V.; Clarke, V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual Res Psychol 2021, 18, 328-352. [CrossRef]
- NHMRC. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, 2013. Available online: https://www.nhmrc.gov.au/adg (accessed 1 August 2024).
- Nelson, M.R.; Banks, E.; Brown, A.; Chow, C.K.; Peiris, D.P.; Stocks, N.P.; Davies AO, R.; Raffoul, N.; Kalman, L.; Bradburn, E.; Jennings, G. 2023 Australian guideline for assessing and managing cardiovascular disease risk. Med J Aust 2024, 220, 482-490. [CrossRef]
- Royal Australian College of General Practitioners. Managment of type 2 diabetes: A handbook for general practice, 2020. Available online: https://www.racgp.org.au/clinical-resources/clinical-guidelines/key-racgp-guidelines/view-all-racgp-guidelines/diabetes/introduction (accessed 1 August 2024).
- Pérez-Torres, A.; Caverni-Muñoz, A.; González García, E. Mediterranean Diet and Chronic Kidney Disease (CKD): A Practical Approach. Nutrients 2023, 15(1), 97. [CrossRef]
- Khatri, M.; Moon, Y.P.; Scarmeas, N.; Gu, Y.; Gardener, H.; Cheung, K.; Wright, C.B.; Sacco, R.L.; Nickolas, T.L.; Elkind, M.S. The association between a Mediterranean-style diet and kidney function in the Northern Manhattan Study cohort. CJASN 2014, 9, 1868-1875. [CrossRef]
- Molina, P.; Gavela, E.; Vizcaíno, B.; Huarte, E.; Carrero, J.J. Optimizing Diet to Slow CKD Progression. Frontiers in medicine 2021, 8, 654250. [CrossRef]
- Campbell, K.L.; Carrero, J.J. Diet for the Management of Patients With Chronic Kidney Disease; It Is Not the Quantity, but the Quality That Matters. J Renal Nut 2016, 26, 279-281. [CrossRef]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report. Diabetes Care 2019, 42, 731-754. [CrossRef]
- Bazzano, L.A.; Green, T.; Harrison, T.N.; Reynolds, K. Dietary approaches to prevent hypertension. Curr Hypertension Rep 2013, 15, 694-702. [CrossRef]
- Worsley, A.; Wang, W.C.; Byrne, S.; Yeatman, H. Different patterns of Australian adults’ knowledge of foods and nutrients related to metabolic disease risk. J Nutr Sci 2014, 3, e14. [CrossRef]
- Wright, J.A.; Cavanaugh, K.L. Dietary sodium in chronic kidney disease: a comprehensive approach. Sem Dialysis 2010, 23, 415-421. [CrossRef]
- Okoyo Opiyo, R.; Nyawade, S.A.; McCaul, M.; Nyasulu, P.S.; Lango, D.B.; Were, A.J.O.; Nabakwe, E.C.; Bukania, Z.N.; Olenja, J.M. Perceptions on Adherence to Dietary Prescriptions for Adults with Chronic Kidney Disease on Hemodialysis: A Qualitative Study. Diseases 2020, 8. [CrossRef]
- Wright, H.H.; Kickbusch, H.; Swanepoel, E.; Gray, N. Factors Influencing Low Sodium Intake in People with Non-Dialysis Dependent Chronic Kidney Disease. J Renal Care 2020, 46, 95-105. [CrossRef]
- Hu, F.B.; Malik, V.S. Sugar-sweetened beverages and risk of obesity and type 2 diabetes: epidemiologic evidence. Physiol & Behavior 2010, 100, 47-54. [CrossRef]
- Chironda, G.; Bhengu, B. Contributing Factors to Non-Adherence among Chronic Kidney Disease (CKD) Patients: A Systematic Review of Literature. Med & Clin Rev 2016, 02. [CrossRef]
- Clarke, A.L.; Yates, T.; Smith, A.C.; Chilcot, J. Patient’s perceptions of chronic kidney disease and their association with psychosocial and clinical outcomes: a narrative review. Clin Kid J 2016, 9, 494-502. [CrossRef]
- Rezaie, M.A. The carer’s perception of dietitians’ advice and its impact on the management of patients receiving haemodialysis. JHND 2000, 13, 363-371. [CrossRef]
- Hollingdale, R.; Sutton, D.; Hart, K. Facilitating dietary change in renal disease: investigating patients’ perspectives. J Renal Care 2008, 34, 136-142. [CrossRef]
- Cicolini, G.; Palma, E.; Simonetta, C.; Di Nicola, M. Influence of family carers on haemodialyzed patients’ adherence to dietary and fluid restrictions: an observational study. J Advan Nurs 2012, 68, 2410-2417. [CrossRef]
- Lopez-Vargas, P.A.; Tong, A.; Howell, M.; Craig, J.C. Educational Interventions for Patients With CKD: A Systematic Review. American J Kidney Dis 2016, 68, 353-370. [CrossRef]
- Lambert, K.; Mansfield, K.; Mullan, J. How do patients and carers make sense of renal dietary advice? A qualitative exploration. J Renal Care 2018, 44, 238-250. [CrossRef]
- Drewnowski, A.; Darmon, N. Food Choices and Diet Costs: an Economic Analysis1,2. J Nut 2005, 135, 900-904. [CrossRef]
- Lambert, K.; Mullan, J.; Mansfield, K. An integrative review of the methodology and findings regarding dietary adherence in end stage kidney disease. BMC nephrology 2017, 18, 318. [CrossRef]
- Yehle, K.S.; Chen, A.M.; Plake, K.S.; Yi, J.S.; Mobley, A.R. A qualitative analysis of coronary heart disease patient views of dietary adherence and web-based and mobile-based nutrition tools. J Cardiopulmon Rehab Prev 2012, 32, 203-209. [CrossRef]
- Wright, H.H.; Lockwood G.; Davey L.; Eqbal Y.; McFarlane C.; Gray N. Caregivers of people with chronic kidney disease: an untapped resource to improve person-centred care? Nut & Diet 2024, 81(S1), 75. [CrossRef]
Figure 1.
Recruitment procedure of final sample of included caregivers.
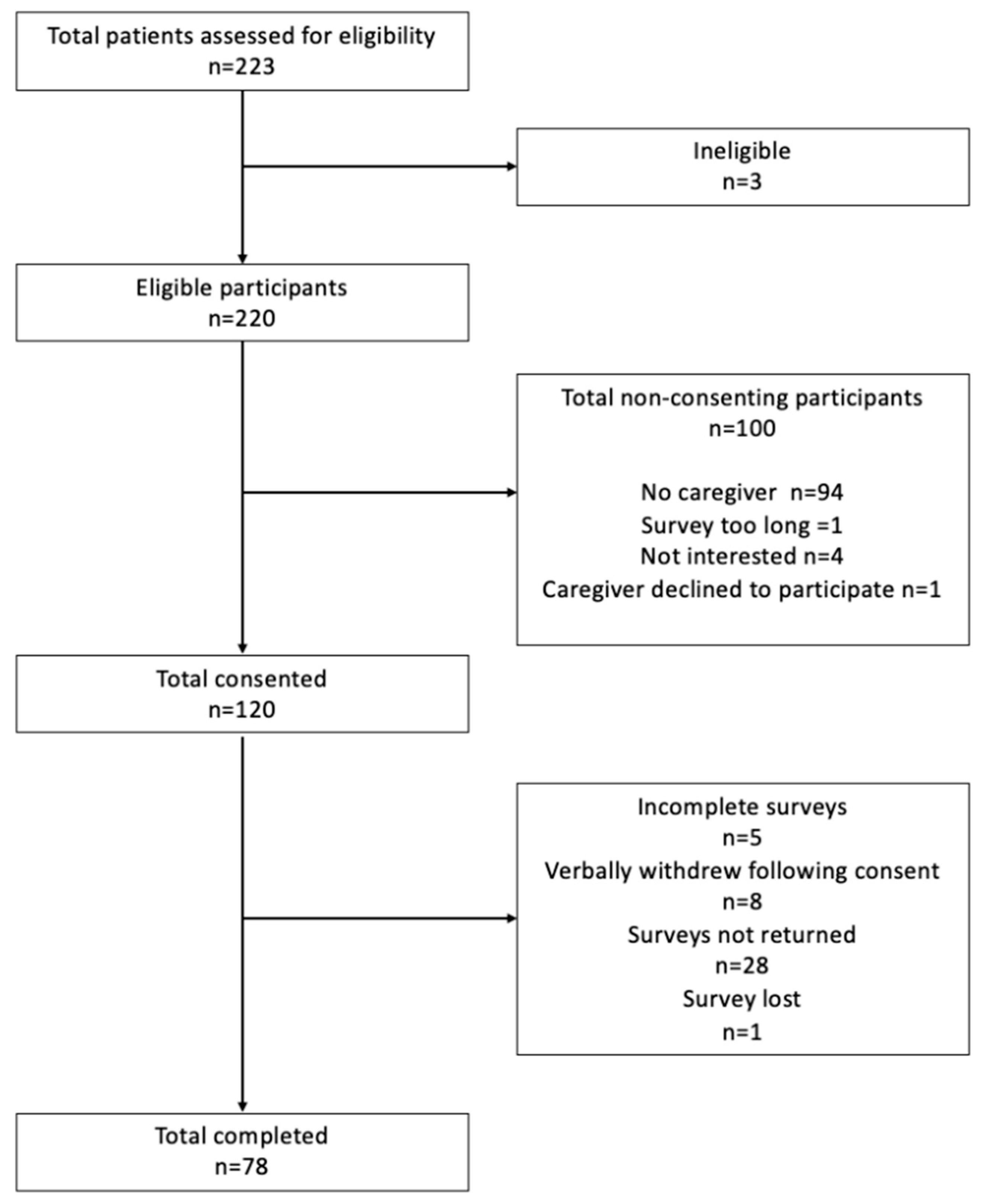
Figure 2.
Factors influencing caregiver’s meal provision and dietary support behavior.
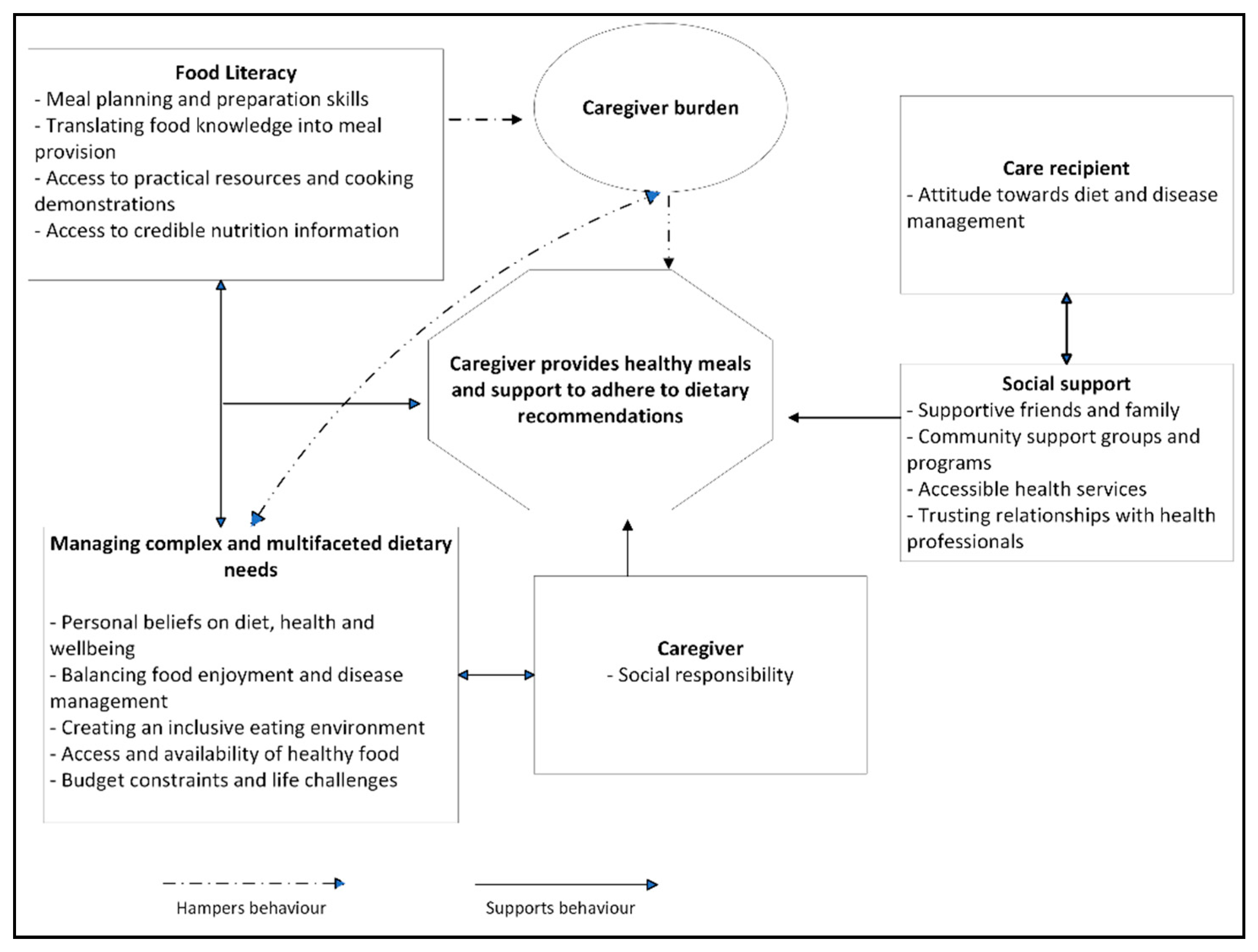
Table 1.
Sociodemographic characteristics of caregivers (n=78).
| Variable | Category | Findings 1 |
|---|---|---|
| Age (years) | 18-44 | 6.5 (5) |
| 45-64 | 27.3 (21) | |
| 65+ | 66.3 (51) | |
| Gender | Female Male |
75.6 (59) 24.4 (19) |
| Main language spoken | English Other |
98.7 (76) 1.3 (1) |
| Education Level | Primary School Secondary/High School Trade or certificate Diploma Degree Post-graduate degree |
4 (3) 37.3 (28) 21.3 (16) 24 (18) 12 (9) 1.3 (1) |
| Income per week |
$0 - $750 $751 - $1430 $1431 - $2430 Over $2430 Prefer not to say |
42.9 (33) 29.9 (23) 10.4 (8) 1.3 (1) 15.6 (12) |
| Relationship to care recipient | Spouse/partner Daughter/son Parent Other |
87 (67) 1.3 (1) 7.8 (6) 3.9 (3) |
| Marital Status | Married/partnered Separated/divorced Single |
89.6 (69) 6.5 (5) 3.9 (3) |
1 Data are expressed as percentage total group (frequency) for categorical data or median and interquartile range (25th;75th) for non-parametric variables.
Table 2.
Care recipient health information and characteristics (n=78).
| Variable | Category | Findings 1 |
|---|---|---|
| Age (yr.) | - | 74 (66; 80) |
| eGFR 2 (ml/min/1.73m2) | - | 27 (18; 42) |
| Gender | Male Female |
75.6 (59) 24.4 (19) |
| CKD Cause | Diabetes Hypertension or vascular disease Glomerulonephritis Other Polycystic kidney disease Reflux neuropathy Obstruction Hereditary |
25.6 (20) 24.4 (19) 21.8 (17) 14.1 (11) 6.4 (5) 3.8 (3) 2.6 (2) 1.3 (1) |
| Comorbidities | Hypertension Diabetes Ischaemic heart disease Cardiovascular disease Peripheral vascular disease |
76.9 (60) 42.3 (33) 29.5 (23) 16.7 (13) 11.5 (9) |
| Multimorbidity 3 | None | 10.3 (8) |
| One Two or more |
32.1 (25) 57.7 (45) |
|
| Smoking status | Smoker Non-smoker Unknown |
29.5 (23) 60.3 (47) 10.3 (8) |
| Kidney Transplant Recipient | Yes No |
15.4 (12) 84.6 (66) |
1 Data are expressed as percentage total group (frequency) for categorical data or median and interquartile range (25th;75th) for non-parametric variables. 2 eGFR, estimated glomerular filtration rate. 3 Multimorbidity refers to presence of two or more chronic conditions in a person at the same time.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



