
Submitted:
31 December 2025
Posted:
02 January 2026
You are already at the latest version
Abstract
Unlike skeletal Class I and II patients, the application of maxillomandibular advancement (MMA) in skeletal Class III patients with obstructive sleep apnea (OSA) is not well documented. The aim of this scoping review was to explore the variations and outcomes of MMA techniques in this unique subgroup. A comprehensive search of PubMed, Embase, Cochrane and LILACS databases were conducted for articles published up to May 2025. Nine studies met the inclusion criteria. Three main variations of MMA were identified: (1) Bimaxillary advancement, which provides the most significant airway enlargement across all pharyngeal regions but carries the highest risk of facial aesthetic distortion; (2) Maxillary advancement with mandibular auto-rotation, a less invasive option suited for patients with isolated maxillary retrusion and symmetrical mandibular anatomy; (3) Maxillary advancement with mandibular setback, which addresses aesthetic concerns in patients with mandibular excess but may compromise oropharyngeal airway space. All variations were reported to be effective in treating OSA but with different considerations. Surgical planning for skeletal Class III patients with OSA should be individualized based on craniofacial morphology, anatomical site of airway obstruction, and aesthetic considerations. A decision flowchart was shared in this study.
Keywords:
apnea
; orthognathic surgery
; sleep apnea syndromes
; jaw
; Malocclusion Angle Class III
Introduction
Maxillomandibular advancement (MMA) is a well-established and effective surgical intervention for the treatment of obstructive sleep apnea (OSA). It is frequently recommended as a primary surgical option for patients with dentofacial deformities, severe OSA, lateral pharyngeal wall collapse, or concentric velar collapse [1]. The procedure has demonstrated particularly high success rates in individuals with skeletal Class II malocclusion, where it is well understood that simultaneous advancement of the maxilla and mandible results in significant airway enlargement [2]. This leads not only to improved respiratory function but also favorable changes to the facial profile [3].
Modifications of MMA—collectively referred to as modified maxillomandibular advancement (MMMA)—have been proposed to address potential aesthetic concerns associated with the standard procedure. Yong et al. described variations such as combining MMA with anterior segmental osteotomy to mitigate post-operative facial fullness [4]. These approaches are especially relevant for patients with bimaxillary protrusion, where additional skeletal advancement may lead to an unesthetic perioral profile. This consideration is particularly important in certain populations, such as East Asians, where bimaxillary protrusion is more prevalent, highlighting the need for individualized surgical planning [4,5,6,7].
In contrast, the literature on the surgical management of OSA in patients with skeletal Class III patterns remains limited, and there remains uncertainty regarding the most effective approaches. These patients typically present with a hypoplastic maxilla and hyperplastic mandible. There is a with a higher prevalence of Class III malocclusion among East Asian populations compared to Whites [8]. Kaewja et al. reported that 11.22% of skeletal Class III orthognathic surgery patients were diagnosed with obstructive sleep apnea (OSA) preoperatively [9]. Similarly, Kim et al. analyzed the skeletal profiles of 1,226 patients diagnosed with OSA and found that 10.5% exhibited a skeletal Class III relationship [10]. These patients were frequently noted to have a narrower nasopharyngeal airway space compared to individuals with other dentofacial patterns [10].
Orthognathic surgery in this group of patients often involves mandibular setback procedures with the goal of addressing occlusion and/or facial profile concerns. This is seemingly counterintuitive to the goal of OSA surgery, which is to enlarge the airway. While existing studies suggest that bimaxillary surgery—maxillary advancement combined with mandibular setback—does not elevate the risk of developing OSA postoperatively, there is a paucity of data focusing specifically on patients diagnosed with OSA prior to surgery [11]. This gap in knowledge underscores the need for further research into tailored surgical approaches for managing OSA in skeletal Class III individuals.
In the revised Stanford protocol proposed by Liu et al. in 2019, it was recommended that patients with skeletal Class III deformities should not routinely undergo standard maxillomandibular advancement (MMA) [1]. Instead, they advocated for counterclockwise rotation and advancement of the maxilla, paired with rotational repositioning of the mandible, thereby eliminating the need for mandibular setback. This highlights a key clinical dilemma: while straightforward maxillary advancement can enhance airway patency and function, it may adversely affect facial aesthetics in Class III patients. Conversely, mandibular setback may preserve facial harmony but risks compromising airway volume and exacerbating OSA symptoms.
Given these unique anatomical and aesthetic challenges in Skeletal Class III patients, careful surgical planning is essential. A integration of current knowledge is thus warranted to evaluate the effectiveness, safety, and most appropriate surgical approaches of MMA in OSA among this unique patient population. This study aims to systematically identify and synthesize existing primary research on the use of MMA, including its various modifications, in treating skeletal Class III patients diagnosed with OSA.
Materials and Methods
A scoping review was performed in this study, as the surgical procedures, methodologies, and outcomes of the studies on MMMA are heterogeneous. The protocol for this review was created according to the Joanna Briggs Institute scoping review protocol guidelines, and was performed using the five steps proposed by Arksey and O’Malley [12,13]. PRISMA-ScR guidelines were used to guide the reporting of this review [14]. The protocol of this review is available in the INPLASY Register (INPLASY20256006). Ethical approval was not required for the study.
Research Question
The primary research question was: "How is maxillomandibular advancement (MMA) performed in skeletal Class III patients diagnosed with obstructive sleep apnea (OSA)?"
Based on this, the objectives of the study were to:
- Identify the surgical techniques and approaches used in MMA for this patient group.
- Examine the clinical considerations influencing treatment selection.
Search Strategy
A systematic search was conducted in PubMed, Embase, Cochrane Library and LILACS using a comprehensive set of keywords, including: maxillomandibular advancement (MMA), maxillary advancement, modified maxillomandibular advancement (MMMA), bimaxillary advancement, telegnathic surgery, bimaxillary rotation, counterclockwise rotation (CCWR), sub-apical osteotomy, prognathism, progenia, Class III, Class 3, mandibular hyperplasia, obstructive sleep apnea (OSA), sleep-disordered breathing, apnea-hypopnea index (AHI), respiratory disturbance index (RDI), oxygen desaturation index (ODI), and lowest oxygen saturation (LSAT) (Supplementary Material 1). References of relevant review articles were also screened to identify additional eligible studies. The final search was completed on 1 May 2025.
Study Selection
Two independent reviewers (CWY and CLKJ) screened the titles and abstracts based on relevance to the research question. Full-text articles were then assessed for eligibility.Inclusion criteria were:
- Primary research articles
- Patients with skeletal Class III deformities
- Use of MMA or skeletal advancement surgery specifically for the treatment of OSA
- Patients diagnosed with OSA
Exclusion Criteria Were:
- Review articles
- Absence of skeletal Class III patients with OSA
- Inability to isolate data specific to Class III patients
- No skeletal advancement or MMA performed
- Lack of full-text availability
- Presence of craniofacial syndromes
A third reviewer was involved if there were differing opinions between the two main reviewers (HKLJ).
Data Extraction
Data were extracted independently by two reviewers (CWY and LKJC) using a standardized template. A third reviewer (JKLH) resolved any discrepancies between the two primary extractors. Extracted data included author, year of publication, journal, population studied, sample size, sex, mean age, mean body mass index (BMI), MMMA surgical technique, surgical movements, and outcome measures. The outcome measures included the apnea-hypopnea index (AHI), Epworth sleepiness scale (ESS) score, radiographic changes to airway dimensions, aesthetics, complications, or any other quality of life measures.
Analysis and Synthesis of Results
Cohen’s kappa statistic was used to assess inter-rater agreement. A descriptive synthesis of the included studies was performed due to heterogeneity in study design, surgical techniques, and outcome measures.
Results
The search of these three databases yielded 4307 articles. 1584 articles were eliminated because they were duplicates. A total of 111 full-length articles were reviewed. Nine articles were included in this scoping review (Figure 1). The inter-rating agreement was high (κ =0.9). The extracted data are summarized in Table 1 and Table 2.
Patient Demographics
The nine included studies reported on a total of 27 patients with a Class III skeletal relationship. The cohort was predominantly male (92.6%), with a mean age of 38.2 ± 13.4 years and a mean body mass index (BMI) of 28.8 ± 7.5 kg/m². The mean apnea–hypopnea index (AHI) or respiratory disturbance index (RDI) was 42.7 ± 31.7 events/hour. Among the subset of patients with available data, the mean Epworth Sleepiness Scale (ESS) score was 10.9 ± 3.9 (n=20), the mean oxygen desaturation index (ODI) was 17.3 ± 20.3 events/hour (n=16), and the average posterior airway space (PAS) was 6.5 ± 2.1 mm, as measured by cephalometric analysis (n=9).
Description of the Variations of MMA
Across the included studies, three variations of MMA or skeletal advancement surgery were reported in the management of skeletal Class III patients with OSA (Table 2).
Variation 1: Maxillary and mandibular advancement
Five studies (Rossi et al., 2019; Brevi et al., 2011; Alsaty et al., 2020; Li et al., 2000; Ronchi et al., 2010) described the use of conventional MMA in skeletal Class III OSA patients (Figure 2) [15,16,17,18,19]. However, data isolating outcomes specifically for Class III patients were available for only 10 individuals, all from predominantly White populations.
The baseline cephalometric values were: Sella-Nasion-A point (SNA) = 80.04 ± 5.26°, and Sella-Nasion-B point (SNB) = 81.01 ± 2.14°. Among the included studies, only Alsaty et al. reported the extent of maxillary advancement (9 mm) [17]. Across the pooled data, the mean changes in SNA and SNB were 9.09 ± 4.04° and 5.11 ± 2.27°, respectively. The average reduction in apnea-hypopnea index (AHI) or respiratory disturbance index (RDI) was 85.24 ± 10.84%.
Within-study comparisons indicated mixed outcomes. Brevi et al. reported a slightly lower AHI reduction in Class III patients (78.52 ± 7.61%, n=2) compared to Class I and II patients (81.45 ± 9.81%, n=30) [16]. In contrast, Ronchi et al. found similar AHI reductions in Class III (86.50 ± 9.63%, n=3) and Class I/II patients (86.03 ± 8.33%, n=19) [19]. Li et al. observed greater efficacy in Class III patients (91.58 ± 5.53%, n=3) versus Class I/II patients (87.12 ± 14.37%, n=20) [18].
ESS scores were reported in six patients, with a mean reduction of 10 ± 5. Notably, one patient showed no change (ESS 8 to 8), while the remaining patients exhibited significant improvement. PAS enlargement was noted in 6 patients, with an average increase of 79.68 ± 52.16% [15,16,18,19]. Data on ODI were reported only by Brevi et al. (n=2), which decreased from 32 to 4 and 84 to 9, respectively [16].
Complications were reported in three patients: one required reoperation due to skeletal instability from inadequate fixation; another had mandibular fixation implants removed due to localized irritation; and one patient self-reported worsening of facial aesthetics postoperatively [18,19].
Variation 2: Maxillary advancement with mandible auto-rotation
Two case reports described the use of isolated maxillary advancement with mandible auto-rotation in the management of Class III patients with OSA [20,21]. Ishida et al. (2019) described a Japanese patient treated with isolated maxillary advancement (4.5 mm at the anterior nasal spine), resulting in mandibular auto-rotation due to superior repositioning of the maxilla (Figure 3) [20]. Postoperative SNA increased from 74.6° to 77.8°, while SNB remained unchanged at 77.1°. AHI was reduced from 15.3 to 2.8 events/h, reflecting an 81.7% improvement. The authors suggested this approach may be preferable for patients with Class III deformities due to maxillary retrusion, but was not suitable for those with severe mandibular asymmetry or canting. Hiroshjkima et al (2015) describe the same approach for another Japanese patient. Similarly, the maxillary advancement was modest, with only 3.5mm at the anterior nasal spine. Both the postoperative SNA and SNB increased from 80.5° to 84.5° and 80.5° to 82.0° respectively. AHI was reduced from 18.8 to 7.6 events/h (59.6%). No complications were reported for both patients.
Variation 3: Maxillary advancement and mandibular setback
Lu et al reported the treatment of a class III patient with moderate OSA (AHI 22.8 events/h) with maxillary advancement and mandibular setback [22]. The maxillary anterior and mandibular posterior movements were equal at 4mm. In addition, counterclockwise rotation of the maxillomandibular complex and genioplasty advancement may have further facilitated the improvement in AHI (55.7% reduction).
A retrospective study by Abdelwahab et al. (2023) reported outcomes from 14 skeletal Class III patients (10 White, 4 non-White) treated with maxillary advancement combined with mandibular setback (Figure 4) [23]. Preoperative SNA and SNB were not defined, and only mean postoperative values were reported: SNA = 80.69°, SNB = 82.72°. The extent of surgical movements was similarly not detailed, but a surgical simulation figure suggested an 8.3 mm overlap between proximal and distal mandibular segments at the inferior border. The utilisation of advancement genioplasty and rotation of the maxillomandibular complex were mentioned but not well described.
Mean AHI decreased from 37.17 to 11.81 events/h, reflecting a 68.23% reduction in OSA severity. Surgical success (defined as >50% AHI reduction and postoperative AHI <20) was achieved in 78.6% of patients, and surgical cure (defined as postoperative AHI <5) in 35.7%. For comparison, the Class II cohort in the same study had a success rate of 92.8% and a cure rate of 21.4%. The authors concluded that the surgical outcomes for skeletal Class III patients were comparable to those achieved with MMA in skeletal Class II patients.
The authors looked at outcomes in the skeletal class III OSA patients with pre-operative SNB < 80° versus SNB > 80°, and found that there was no statistical differences in the preoperative AHI and change in AHI. There was similarly no statistical difference in preoperative AHI and change in AHI between patients with preoperative SNA < 82° versus SNA > 82°.
Additional reported outcomes included reductions in ESS (from 10.23 ± 4.38 to 4.22 ± 3.07) and ODI (from 11.43 ± 11.40 to 5.44 ± 7.96). No surgical complications were reported.
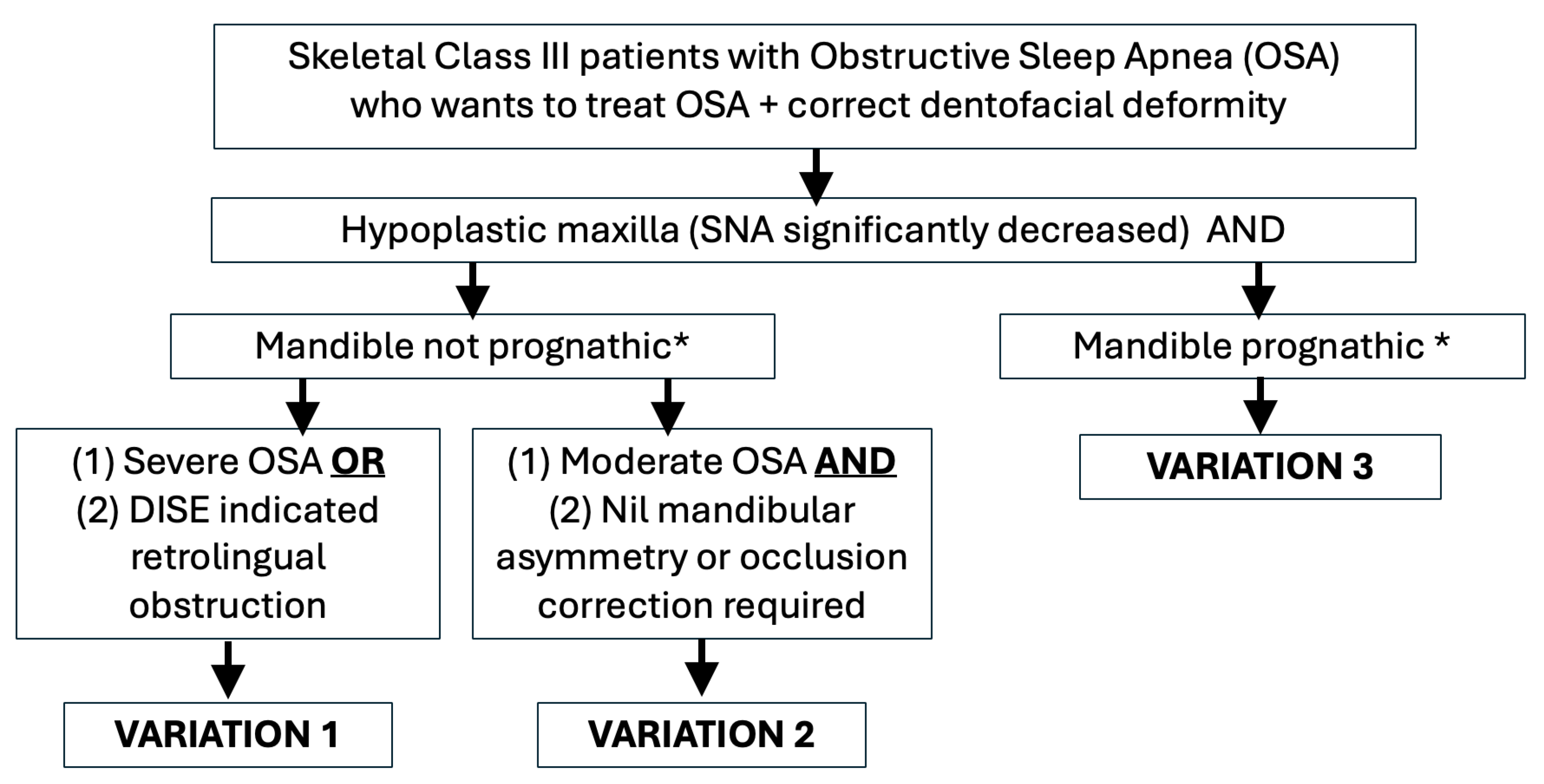
Figure 5.
Flowchart on decision process. * Prognathism is determined by SNB values on cephalometric analysis or if prognathism has affected aesthetics..
Figure 5.
Flowchart on decision process. * Prognathism is determined by SNB values on cephalometric analysis or if prognathism has affected aesthetics..
Discussion
Maxillomandibular advancement (MMA) is a well-established surgical treatment for obstructive sleep apnea (OSA) in patients with skeletal Class I and II relationships. However, its efficacy in skeletal Class III OSA patients remains less clear. This scoping review identified and analyzed nine studies involving 27 skeletal Class III OSA patients, revealing three distinct surgical variations of MMA utilized in this subgroup. The findings underscore the necessity of individualized surgical planning to optimize both functional and aesthetic outcomes. Based on the results from the studies, a decision making flowchart was generated.
Variation 1: Bimaxillary Advancement
While the forward projection of the chin in skeletal Class III patients could potentially compromise facial aesthetics, no such concerns were reported. Several factors may explain this: (1) the average pre-treatment SNB angle was not significantly high (81.3 ± 2.36°), indicating maxillary retrusion rather than mandibular prognathism as the dominant deformity; (2) although bimaxillary advancement was done, the SNA change (8.70 ± 3.74°) exceeded that of SNB (5.01 ± 2.64°), supporting the notion that maxillary advancement played a larger role in the correction; and (3) the patient population was predominantly White, a group known to tolerate or aesthetically accommodate bimaxillary advancement due to baseline retrusive profiles [24]. Furthermore, this population may be more culturally accepting of stronger lower facial projection, further mitigating concerns about aesthetic compromise [25,26]. All the patients included in the studies had severe pre-treatment OSA. While retrolingual obstruction was also reported for 1 patient (endoscopy findings not reported for other patients), the need to further expand the mandibular framework should also be considered for patients retrolingual obstruction.
Therefore, based on the results, the authors recommend that for Class III patients with OSA, variation 1 is recommended for those with mandible that are not prognathic, severe OSA or with retrolingual obstruction.
Variation 2: Isolated Maxillary Advancement with Mandibular Auto-Rotation
The second variation features isolated maxillary advancement and impaction. This induces a counter-clockwise rotation of the mandible, leading to an automatic enlargement of the upper airway. This technique is particularly beneficial for patients with maxillary retrusion and no significant cants or mandibular asymmetry.
Before selecting this surgical variation, it is essential to accurately identify the primary site of airway obstruction. This approach may be particularly beneficial for patients with retropalatal or nasopharyngeal narrowing. Studies have shown that maxillary advancement alone can significantly increase upper airway volume, including both the nasopharyngeal and oropharyngeal regions. For instance, a study by Rosário et al. showed that isolated maxillary advancement performed in 14 patients with skeletal Class III deformities resulted in a significant increase in upper airway volume [27]. Similarly, a systematic review by Steegman et al. reported volumetric airway expansion following maxillary advancement procedures, with increases noted not only in the nasopharynx but also extending into the oropharyngeal region [28]. However, the degree of airway enlargement is generally less than that achieved with bimaxillary advancement, which produced more substantial changes particularly in the oropharyngeal space. While the findings from the above two studies are informative, it is important to recognize that both studies were conducted in non-OSA populations, thereby limiting their direct applicability. It must also be noted that anatomical dimensions alone does not fully account for the complexity of OSA pathophysiology—factors such as airway collapsibility and neuromuscular tone must also be considered [29].
Based on the findings of the study, the authors recommend to limit variation 2 to patients with moderate OSA and do not require mandibular surgery for facial asymmetry or occlusion purposes. However, case selection for isolated maxillary advancement in the management of OSA still requires further validation, especially given the small sample sizes and lack of data specific to this population.
Variation 3: Maxillary Advancement with Mandibular Setback
The third variation entailed a combination of maxillary advancement and mandibular setback, a strategy traditionally used in non-OSA Class III patients for facial balance. Despite concerns that mandibular setback could reduce the oropharyngeal airway and exacerbate OSA, surgical success rates remained high. This suggests that maxillary advancement may offset the airway narrowing effect of the mandibular setback, possibly by advancing the velopharyngeal musculature and soft tissue. Some studies propose that reductions in airway volume following mandibular setback are transient, with subsequent remodelling and rebound over time [11,30,31]. Additionally, skeletal Class III patients may possess an enlarged posterior airway pre-operatively, allowing a margin of reduction without significant physiological consequence [11,30,31]. However, none of the reviewed studies included precise data on pre-treatment airway volumes or obstruction sites, limiting the ability to predict outcomes. The heterogeneity of skeletal Class III deformities—whether due to maxillary retrusion or mandibular prognathism—did not appear to significantly affect surgical outcomes, though further investigation is warranted to clarify this relationship. As with variation 2, it remains unclear whether airway changes in non-OSA patients respond similarly to those in OSA patients. Therefore, identifying the pre-treatment site of obstruction and assessing airway volume are important for determining the appropriateness of this surgical approach. While variation is most appropriate who patients with a truly prognathic mandible, other adjunctive movements such as counter-clockwise rotation or genioglossus advancement should still be considered.
Previous reviews have reported lower apnea–hypopnea index (AHI) reductions in Class III patients undergoing MMA compared to Class I and II patients, hypothesizing that less mandibular advancement may underlie this trend [32]. However, our review did not corroborate this, as MMA outcomes ranged from superior to comparable or inferior. This suggests that factors beyond the extent of mandibular advancement, such as individual craniofacial morphology and surgical technique, play critical roles. Thus, results of this review highlights that MMA in Class III patients cannot be standardized but should instead be tailored to the individual’s anatomical and functional needs.
Surgeons often target 10 mm of maxillary and mandibular advancement based on earlier reports3. While this benchmark may serve as a guideline, the degree, direction, and type of skeletal movement must consider disease severity, anatomical site(s) of obstruction, and the patient’s baseline craniofacial structure. The decision-making process in Class III patients is particularly complex, as it may involve trade-offs between airway patency and aesthetic balance—particularly in cases where mandibular setback is contemplated.
Beyond jaw repositioning, mandibular plane angle is a relevant cephalometric variable linked to OSA severity and treatment response. High-angle mandibles are associated with narrower oropharyngeal airways and reduced response to therapy [33,34]. Ma et al reported that patients with a high mandibular angle have a smaller baseline dimension of the oropharyngeal airway and required a greater protrusion to achieve an effective treatment [34]. While this factor was not consistently reported in the included studies, it should be integrated into pre-operative assessment and planning.
The future of MMA planning may benefit from predictive simulations of airway response. Computational fluid dynamics (CFD) has demonstrated promise in modelling airway behaviour post-surgery and may help optimize surgical planning by quantifying expected changes in airflow dynamics [35]. A target of 70% airway enlargement has been suggested, but tools to accurately simulate these changes preoperatively are still in development and not widely accessible [36].
This review has several limitations. First, the small sample size and heterogeneous methodologies across the included studies precluded formal meta-analysis. Second, most studies lacked detailed assessment and description of the specific sites of upper airway obstruction, which limits personalized surgical recommendations. Only 1 study (Rossi et al 2019) described the patient to have both retropalatal and retrolingual obstruction. Third, while SNA and SNB changes were consistently reported, linear advancement in millimetres and rotational movements were less frequently documented—metrics that many clinicians find more practical for surgical planning. Finally, the studies reviewed primarily included White populations, limiting generalizability to other ethnic groups who may have different aesthetic thresholds and craniofacial morphology.
This scoping review consolidates available evidence on MMA variations in skeletal Class III patients with OSA. Although no universal protocol can be recommended, the findings support a nuanced, individualized approach to surgical planning. Importantly, this review also highlights the relative paucity of research in this specific population—one that may be underrepresented in the current OSA surgical literature. Further prospective studies with standardized reporting on anatomical, functional, and aesthetic outcomes are urgently needed to guide evidence-based surgical management in this subgroup.
In conclusion, this scoping review highlights that while MMA is effective for OSA, its use in skeletal Class III patients requires individualized planning. Three surgical variations—bimaxillary advancement, isolated maxillary advancement, and maxillary advancement with mandibular setback—were identified. Each variation offers differing benefits depending on facial structure, obstruction site, and aesthetic goals. Variation 1 (Bimaxillary advancement) may be more suitable for patients with obstructions in the oropharyngeal or hypopharyngeal area, and mild pre-surgical mandibular prognathism. Variation 2 (Maxillary advancement with mandibular auto-rotation) is more suitable for patients with obstructions mainly in the nasopharyngeal region secondary to a maxillary retrusion. Variation 3 (Maxillary advancement with mandibular setback) can be considered in patients with mandibular prognathism requiring setback for aesthetic reasons. There is a need to rule out pre-treatment obstructions in the oropharyngeal regions as there is potential that it may be worsened. The findings emphasize that treatment cannot rely on standardized protocols but must instead be tailored to patient-specific anatomy and functional needs. Further research with larger samples and detailed reporting is needed to guide evidence-based practice in this underrepresented subgroup.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
Nil.
Conflicts of Interest
Nil to declare.
Ethical Approval and Patient Consent
Not required.
References
- Liu, SY; Awad, M; Riley, R; Capasso, R. The Role of the Revised Stanford Protocol in Today's Precision Medicine. Sleep Med Clin. 2019, 14, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Quah, B; Sng, TJH; Yong, CW; Wen Wong, RC. Orthognathic Surgery for Obstructive Sleep Apnea. Oral Maxillofac Surg Clin North Am. 2023, 35, 49–59. [Google Scholar] [CrossRef]
- Zaghi, S; Holty, JE; Certal, V; et al. Maxillomandibular Advancement for Treatment of Obstructive Sleep Apnea: A Meta-analysis. JAMA Otolaryngol Head Neck Surg. 2016, 142, 58–66. [Google Scholar] [CrossRef]
- Yong, CW; Ng, WH; Quah, B; Sng, TJH; Loy, RCH; Wong, RCW. Modified maxillomandibular advancement surgery for the treatment of obstructive sleep apnoea: a scoping review. Int J Oral Maxillofac Surg. 2024, 53, 36–44. [Google Scholar] [CrossRef]
- Yong, CW; Quah, B; Colpani, JT; Lee, FKF; Loh, EE; Wong, RCW. Effectiveness of mandibular advancement devices in obstructive sleep apnea therapy for East Asian patients: a systematic review and meta-analysis. J Clin Sleep Med 2025. [Google Scholar] [CrossRef]
- Leung, YY; Leung, JKC; Li, ATC; et al. Accuracy and safety of in-house surgeon-designed three-dimensional-printed patient-specific implants for wafer-less Le Fort I osteotomy. Clin Oral Investig. 2023, 27, 705–713. [Google Scholar] [CrossRef]
- Leung, YY; Wan, JCC; Fu, HL; Chen, WC; Chung, JHZ. Segmental mandibular advancement for moderate-to-severe obstructive sleep apnoea: a pilot study. Int J Oral Maxillofac Surg. 2023, 52, 956–963. [Google Scholar] [CrossRef] [PubMed]
- Lee, CKJ; Yong, CW; Saigo, L; Ren, YJ; Chew, MT. Virtual surgical planning in orthognathic surgery: a dental hospital's 10-year experience. Oral Maxillofac Surg. 2024, 28, 729–738. [Google Scholar] [CrossRef]
- Thanakorn Kaewja NS, Kanich Tripuwabhrut. Obstructive Sleep Apnea Prevalence, Upper Airway Dimensions, and Sleep Parameters in Skeletal Class III Malocclusion Patients Undergoing Orthognathic Surgery with Different Vertical Skeletal Patterns. Thai Journal of Orthodontics. 2024:14:6-16.
- Kim, SJ; Ahn, HW; Hwang, KJ; Kim, SW. Respiratory and sleep characteristics based on frequency distribution of craniofacial skeletal patterns in Korean adult patients with obstructive sleep apnea. PLoS One 2020, 15, e0236284. [Google Scholar] [CrossRef] [PubMed]
- Chen, F; Terada, K; Hua, Y; Saito, I. Effects of bimaxillary surgery and mandibular setback surgery on pharyngeal airway measurements in patients with Class III skeletal deformities. Am J Orthod Dentofacial Orthop. 2007, 131, 372–377. [Google Scholar] [CrossRef]
- Arksey, H; O'Malley, L. Scoping studies: towards a methodological framework. International journal of social research methodology 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Peters, MD; Godfrey, CM; McInerney, P; Soares, CB; Khalil, H; Parker, D. The Joanna Briggs Institute reviewers' manual 2015: methodology for JBI scoping reviews. 2015. [Google Scholar]
- Tricco, AC; Lillie, E; Zarin, W; et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Annals of internal medicine 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Rossi, DS; Romano, M; Sweed, AH; Baj, A; Gianni, AB; Beltramini, GA. Use of CAD-CAM technology to improve orthognathic surgery outcomes in patients with severe obstructive sleep apnoea syndrome. J Craniomaxillofac Surg. 2019, 47, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Brevi, BC; Toma, L; Pau, M; Sesenna, E. Counterclockwise rotation of the occlusal plane in the treatment of obstructive sleep apnea syndrome. J Oral Maxillofac Surg. 2011, 69, 917–923. [Google Scholar] [CrossRef] [PubMed]
- AlSaty, G; Burns, M; Ngan, P. Effects of maxillomandibular advancement surgery on a skeletal Class III patient with obstructive sleep apnea: A case report. APOS Trends Orthod. 2021, 11(2), 161–168. [Google Scholar] [CrossRef]
- Li, KK; Powell, NB; Riley, RW; Zonato, A; Gervacio, L; Guilleminault, C. Morbidly obese patients with severe obstructive sleep apnea: is airway reconstructive surgery a viable treatment option? Laryngoscope 2000, 110, 982–987. [Google Scholar] [CrossRef] [PubMed]
- Ronchi, P; Novelli, G; Colombo, L; et al. Effectiveness of maxillo-mandibular advancement in obstructive sleep apnea patients with and without skeletal anomalies. Int J Oral Maxillofac Surg. 2010, 39, 541–547. [Google Scholar] [CrossRef]
- Ishida, T; Manabe, A; Yang, SS; Watakabe, K; Abe, Y; Ono, T. An orthodontic-orthognathic patient with obstructive sleep apnea treated with Le Fort I osteotomy advancement and alar cinch suture combined with a muco-musculo-periosteal V-Y closure to minimize nose deformity. Angle Orthod. 2019, 89, 946–952. [Google Scholar] [CrossRef]
- Hoshijima, M; Honjo, T; Moritani, N; Iida, S; Yamashiro, T; Kamioka, H. Maxillary Advancement for Unilateral Crossbite in a Patient with Sleep Apnea Syndrome. Acta Med Okayama 2015, 69, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Lu, C; Chen, Y; Tseng, Y. A Case of Class III Malocclusion with Obstructive Sleep Apnea Treated by Orthodontic Treatment Combined Two-jaw Orthognathic Surgery. Taiwanese Journal of Orthodontics 2024, 35, 193–203. [Google Scholar] [CrossRef]
- Abdelwahab, M; Taheri, N; Eltahir, L; Erdogan, C; Lee, K; Liu, SY. Maxillomandibular Advancement Efficacy in Obstructive Sleep Apnea Patients With Class 2 Versus 3 Dentofacial Deformity. Otolaryngol Head Neck Surg. 2023, 169, 1366–1373. [Google Scholar] [CrossRef] [PubMed]
- Ngan, P; Hägg, U; Yiu, C; Merwin, D; Wei, SH. Cephalometric comparisons of Chinese and Caucasian surgical Class III patients. Int J Adult Orthodon Orthognath Surg. Published. 1997, 12, 177–188. [Google Scholar]
- Gao, Y; Niddam, J; Noel, W; Hersant, B; Meningaud, JP. Comparison of aesthetic facial criteria between Caucasian and East Asian female populations: An esthetic surgeon's perspective. Asian J Surg. 2018, 41, 4–11. [Google Scholar] [CrossRef]
- Chen, T; Yang, X; Xue, C; Bai, D; Xu, H. Harmonizing soft tissue subnasale and chin position in a forehead-based framework: interracial commonalities and differences between Asian and Caucasian females. Angle Orthod. 2025, 95, 86–95. [Google Scholar] [CrossRef]
- Rosário, HD; de Oliveira, BG; Pompeo, DD; de Freitas, PH; Paranhos, LR. Surgical Maxillary Advancement Increases Upper Airway Volume in Skeletal Class III Patients: A Cone Beam Computed Tomography-Based Study. J Clin Sleep Med. 2016, 12, 1527–1533. [Google Scholar] [CrossRef]
- Steegman, R; Hogeveen, F; Schoeman, A; Ren, Y. Cone beam computed tomography volumetric airway changes after orthognathic surgery: a systematic review. Int J Oral Maxillofac Surg. 2023, 52, 60–71. [Google Scholar] [CrossRef]
- Eckert, DJ; White, DP; Jordan, AS; Malhotra, A; Wellman, A. Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets. Am J Respir Crit Care Med. 2013, 188, 996–1004. [Google Scholar] [CrossRef]
- Gandedkar, NH; Chng, CK; Por, YC; Yeow, VKL; Ow, ATC; Seah, TE. Influence of Bimaxillary Surgery on Pharyngeal Airway in Class III Deformities and Effect on Sleep Apnea: A STOP-BANG Questionnaire and Cone-Beam Computed Tomography Study. J Oral Maxillofac Surg. 2017, 75, 2411–2421. [Google Scholar] [CrossRef]
- Hassing GJ, The V, Shaheen E, Politis C, de Llano-Pérula MC. Long-term three-dimensional effects of orthognathic surgery on the pharyngeal airways: a prospective study in 128 healthy patients. Clin Oral Investig. 2022:26:3131-3139. [CrossRef]
- Khan, S; Sutton, SR; Nguyen, SA; et al. Outcomes of maxillomandibular advancement (MMA) by dentofacial class: A systematic review and meta-analysis. Br J Oral Maxillofac Surg. 2025, 63, 83–90. [Google Scholar] [CrossRef]
- Sutherland, K; Lee, RWW; Chan, TO; Ng, S; Hui, DS; Cistulli, PA. Craniofacial Phenotyping in Chinese and Caucasian Patients With Sleep Apnea: Influence of Ethnicity and Sex. J Clin Sleep Med. 2018, 14, 1143–1151. [Google Scholar] [CrossRef]
- Ma, Y; Yu, M; Gao, X. Role of craniofacial phenotypes in the response to oral appliance therapy for obstructive sleep apnea. J Oral Rehabil. 2023, 50, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Ogisawa, S; Shinozuka, K; Aoki, J; et al. Computational fluid dynamics analysis for the preoperative prediction of airway changes after maxillomandibular advancement surgery. J Oral Sci. 2019, 61, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Kongsong, W; Waite, PD; Sittitavornwong, S; Schibler, M; Alshahrani, F. The correlation of maxillomandibular advancement and airway volume change in obstructive sleep apnea using cone beam computed tomography. Int J Oral Maxillofac Surg. 2021, 50, 940–947. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA-Scr Flowchart.
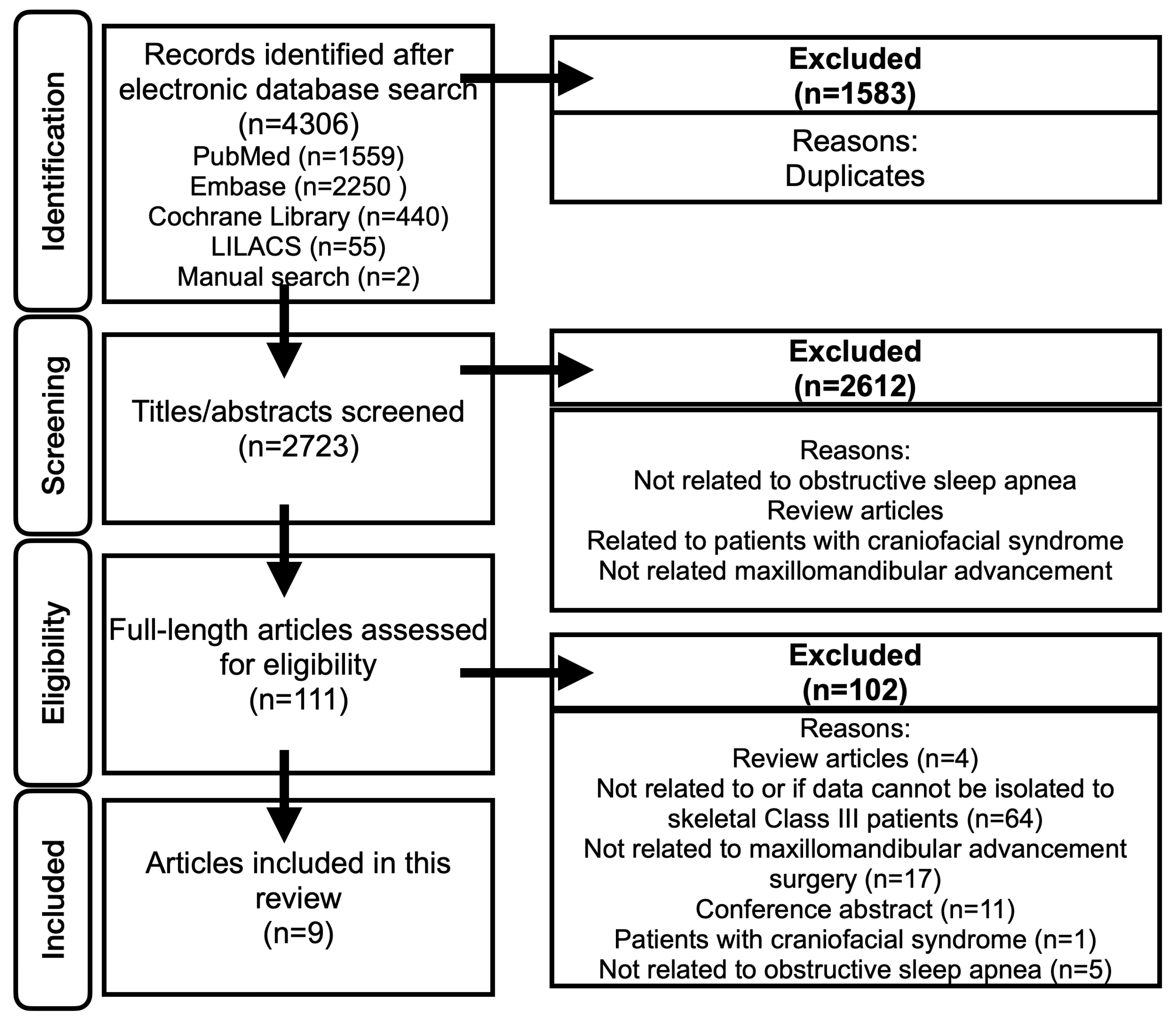
Figure 2.
Variation 1 before and after the surgery.
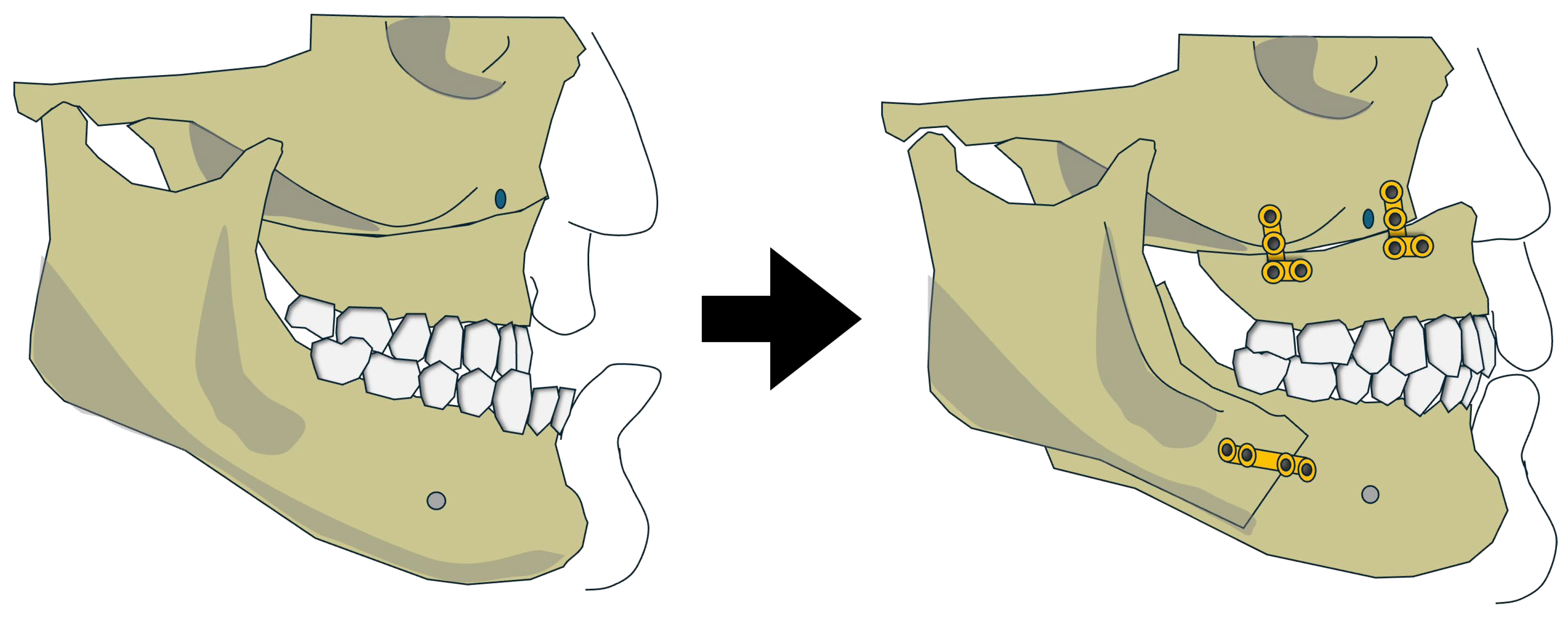
Figure 3.
Variation 2 before and after the surgery.
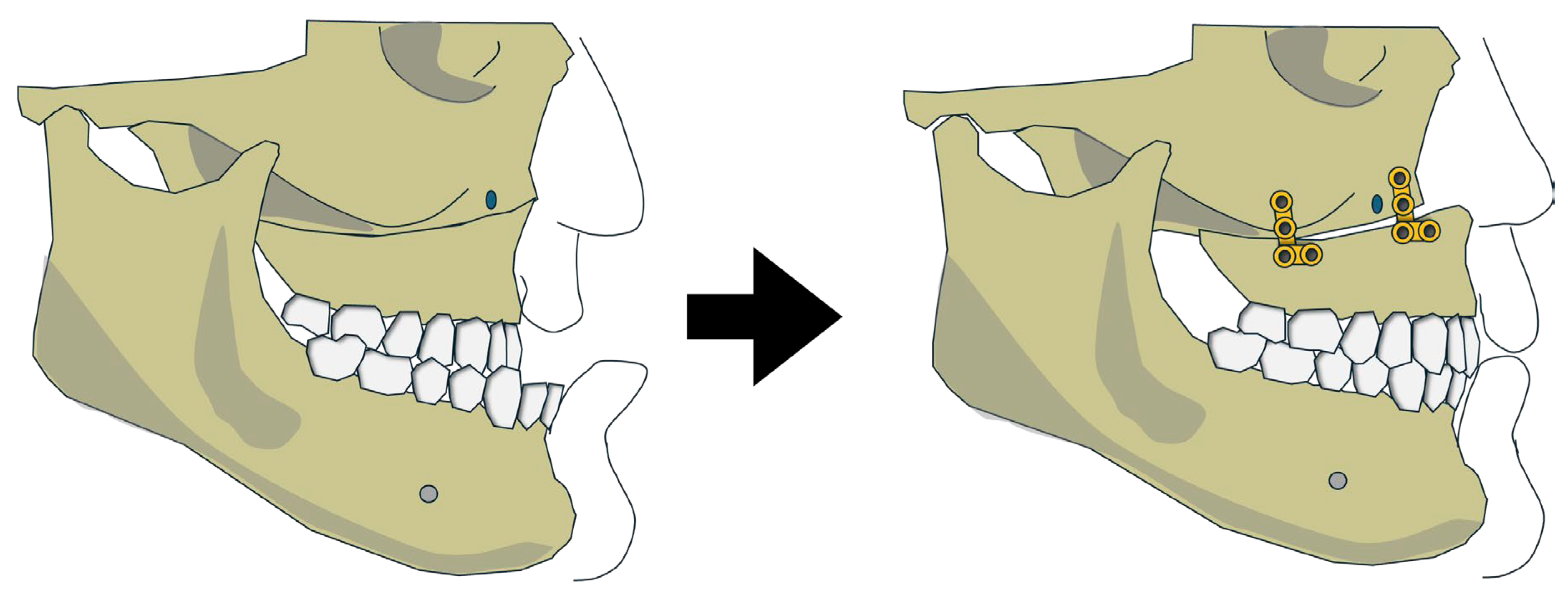
Figure 4.
Variation 3 before and after the surgery.
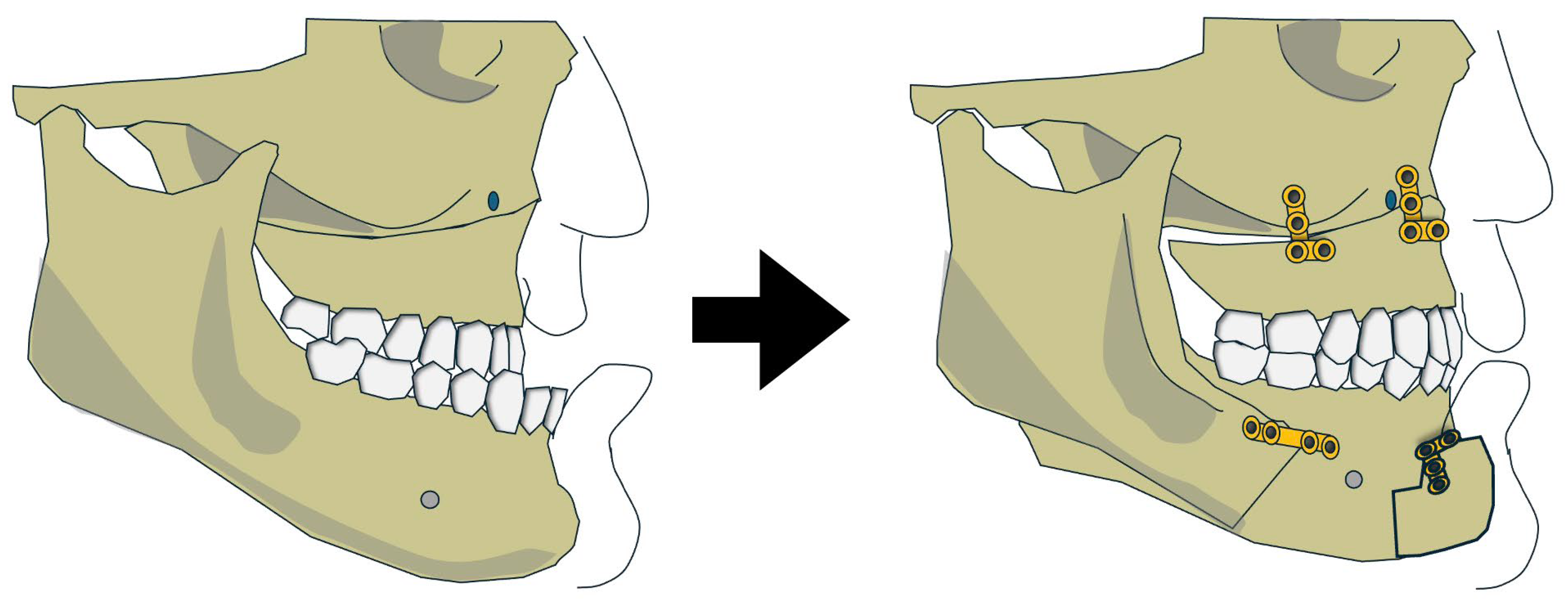

Table 1.
Demographic details and surgical movements.
| Author & Year | Study Type | Sample Size | Mean Age (years) | Gender | BMI (kg/m2) | SNA, SNB and Surgical movements |
|---|---|---|---|---|---|---|
| Variation 1: Maxillary and mandibular advancement | ||||||
|
Rossi et al 2019 (Patient 6) |
Retrospective Cohort | 1 | 47 | M | 30 | SNA: 75.9° → 81.6°, (Dx + 5.7°) SNB 79.3° →84.9°, (Dx +5.6°) Maxilla advancement not noted in mm, Mandible advancement 13.2mm |
|
Ronchi et al 2010 (Patients No.5 from group 1, No.5 and 6 from group 2) |
Retrospective Cohort | 3 | 26 | M | 24 | SNA: 73° → 89°, (Dx + 16°) SNB 79° →85°, (Dx +6°) |
| 62 | M | 27.1 | SNA: 80° → 85°, (Dx + 5°) SNB 80° → 84°, (Dx +4°) |
|||
| 54 | M | 31 | SNA: 82° → 91°, (Dx + 9°) SNB 82 → 88, (Dx +6°) |
|||
|
Brevi et al 2011 (Patients No. 1,6) |
Retrospective Cohort | 2 | 67 | M | 25.7 | SNA 79° → 86°, (Dx +7°) SNB 84° → 88° (Dx +4°) Movements not recorded in mm |
| 45 | M | 30 | SNA 75° → 85°, (Dx +10°) SNB 78° → 82°, (Dx +4°) |
|||
| Alsaty et al 2020 | Case Report | 1 | 55 | M | 25.6 | SNA 78.5° → 83.7°,(Dx +5.2°) SNB 78.8° →81.3°, (Dx +2.5°) Maxilla advancement 9mm, Mandible advancement 5mm |
|
Li et al. 2000 (Patients No.7,13,21) |
Retrospective Cohort | 3 | 47 | F | 56.0 | SNA 83° → 96°, (Dx +13°) SNB 83° → 88° (Dx +5°) |
| 17 | M | 41.5 | SNA 83° → 88°, (Dx+5°) SNB 84° → 87°, (Dx +3°) |
|||
| 48 | M | 42.1 | SNA 81° → 96° (Dx +15°) SNB 82°→ 93° (Dx + 11°) |
|||
| Variation 2: Maxillary advancement with mandible auto-rotation | ||||||
| Hoshijima et al 2015 | Case Report | 1 | 44 | M | NA | SNA 80.5° → 84.5°, (Dx+4.0°) SNB 80.5° → 82.0°, (Dx +1.5°) 3.0mm forward at ANS |
| Ishida et al 2019 | Case Report | 1 | 23 | M | 18.6 | SNA 74.6° → 77.8° (Dx +3.2°), SNB 77.1° → 77.1° (Dx 0) 4.5mm forward at ANS |
| Variation 3: Maxillary advancement and mandibular setback | ||||||
| Abdelwahab et al 2023 | Retrospective Cohort | 14 | 33.9 ± 10.2 | 13M, 1F | 26.9 ± 3.7 | Post-op SNA 80.69° Post-op SNB 82.72° Surgical movements not defined |
| Lu et al 2025 | Case Report | 1 | 24 | 1 M | 21.7 | SNA 86.1° → 88.6°(Dx +2.5°), SNB 88.6° → 88.1°(Dx -0.5°), Maxilla advancement 4mm & counterclockwise rotation of 5°, mandible setback 4mm & counterclockwise rotation of 6.5°, genioplasty advancement 7mm |
Legend: BMI = Body mass Index, M= Male, F= Female, Dx = Difference of, SNA = Sella-Nasion-A Point Angle, SNB = Sella-Nasion-B Point Angle.
Table 2.
Outcomes.
| Author & Year | AHI/RDI (Events/hr) | ESS | ODI (Events/Hr) | PAS (mm) | Complications | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Dx | Pre | Post | Dx | Pre | Post | Dx | Pre | Post | Dx | |||
| Variation 1: Maxillary and mandibular advancement | ||||||||||||||
| Rossi et al 2019 | 33.5 | 11.9 | -21.6 (64.48%) | NA | NA | NA | NA | NA | NA | 9.21 | 16.5 | +7.29 | Nil | |
| Brevi et al 2011 | 24.2 | 7 | -17.7 (73.14%) |
8 | 8 | 0 | 32 | 5 | -28 | 7 | 10 | +3 | NA | |
| 87 | 14 | -73 (83.90%) |
13 | 0 | -13 | 84 | 9 | -75 | 8 | 15 | +7 | NA | ||
| Ronchi et al 2010 | 70 | 1 | -69 | 16 | 0 | -16 | NA | NA | NA | 8 | 14 | +6 | Worsened aesthetics | |
| 60 | 15 | -45 | 13 | 1 | -12 | NA | NA | NA | 4 | 10 | +6 | NA | ||
| 71 | 10 | -61 | 12 | 2 | -10 | NA | NA | NA | 5 | 12 | +7 | NA | ||
| Alsaty et al 2020 | 21.2 | 0.7 | -20.5 (96.70%) |
12 | 3 | -9 | NA | NA | NA | NA | NA | NA | Nil | |
|
Li et al 2000 |
44^ | 1^ | -43 (97.72%) |
NA | NA | NA | NA | NA | NA | 5 | 9 | +4 | Re-operation due to insufficient fixation | |
| 90^ | 9^ | -81 (90%) |
NA | NA | NA | NA | NA | NA | 3 | 8 | +5 | Nil | ||
| 77^ | 10^ | -67 (87.01%) |
NA | NA | NA | NA | NA | NA | 9 | 13 | +4 | Removal of mandibular implants due to localized irritation | ||
| Variation 2: Maxillary advancement with mandible auto-rotation | ||||||||||||||
| Hoshijima et al 2015 | 18.8 | 7.6 | 11.2 (59.6%) |
NA | NA | NA | NA | NA | NA | NA | NA | NA | ||
| Ishida et al 2019 | 15.3 | 2.8 | 12.5 (81.70%) |
NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| Variation 3: Maxillary advancement and mandibular setback | ||||||||||||||
| Abdelwahab et al 2023 | 37.17 ±35.77 |
11.81 ±15.74 | 25.36 (68.23%) p=0.41 |
10.23 ±4.38 | 4.22 ±3.07 | 6.01 P=0.006 |
11.43 ±11.40 | 5.44 ±7.96 | 5.99 P=0.828 |
NA | NA | NA | Nil | |
| Lu et al 2025 | 22.8 | 10.1 | 12.7 (55.7%) |
NA | NA | NA | NA | NA | NA | NA | NA | NA | Nil | |
Legend: AHI = Apnea-Hypopnea-Index, RDI or ^ = Respiratory Disturb Index, ODI= Oxygen Desaturation Index, PAS = Posterior Airway Space, NA = Not available, Dx = Difference Of, Nil = None reported.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



