
Submitted:
31 December 2025
Posted:
01 January 2026
You are already at the latest version
Abstract
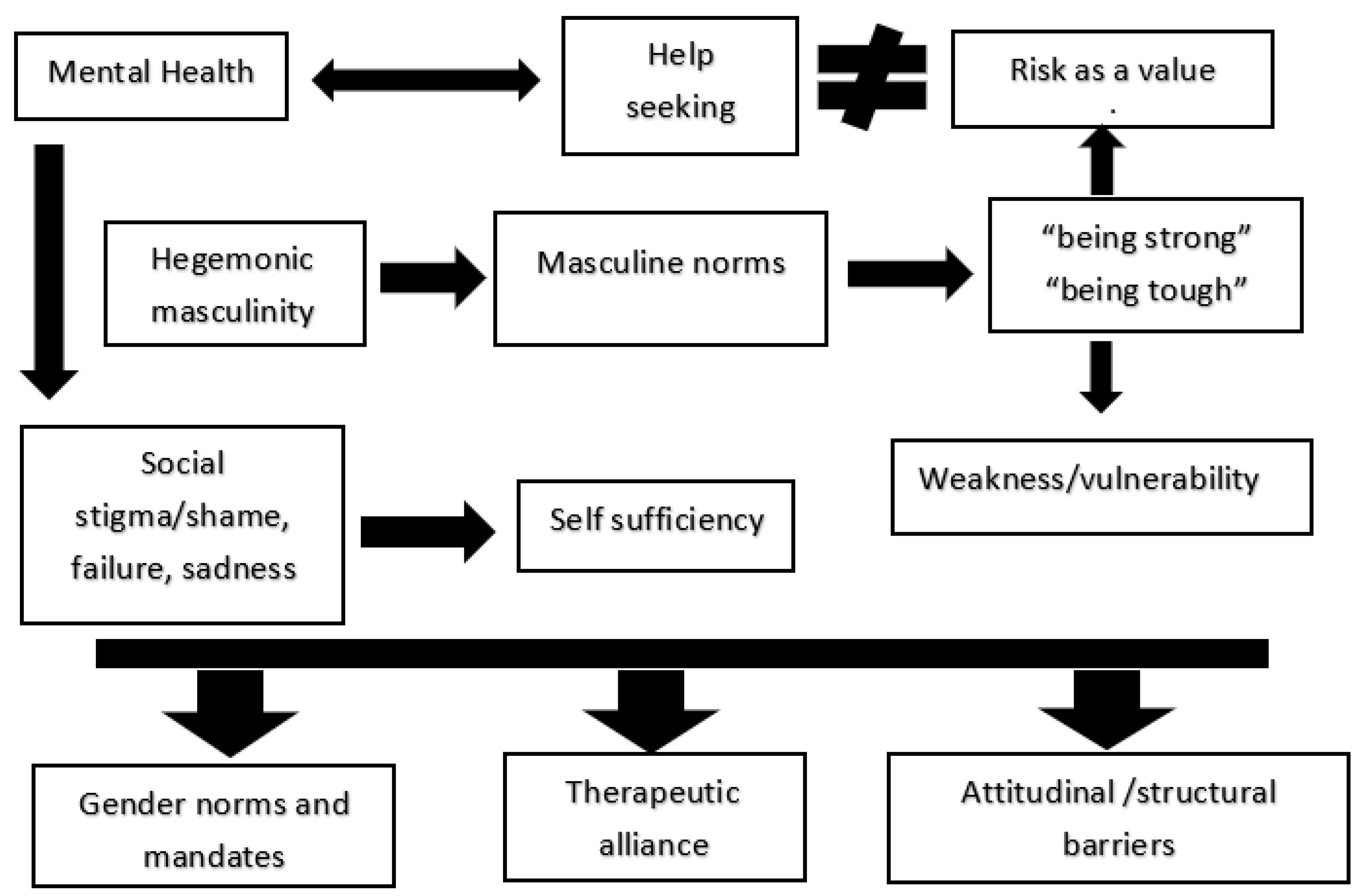
Background: Research on men’s mental health points out gender differences in help-seeking and access to care. Traditional masculine norms (i.e., emotional repression, self-reliance, “being strong”) and gender bias might conceal distress, delay treatment, and help to explain higher burdens of addiction, violence, and suicide alongside lower recorded affective/anxiety diagnoses. Methods: An exploratory narrative review with scoping aims was conducted. PubMed, Scopus, and Web of Science were searched for 2015–2025 studies using MeSH and terms on men’s mental health, masculinities, and stigma. Results: Eleven studies identified attitudinal barriers (i.e., self-stigma, shame, symptom minimization, mistrust, etc.) and structural barriers (i.e., limited tailored services, navigation difficulties, costs, bureaucracy, etc.) that contribute late presentation, weaken therapeutic alliance, and increase dropout; especially when therapy is perceived as impersonal or ineffective. Intersectional factors (i.e., class, age, ethnicity) further contribute with access and they need to be included in the field of men’s mental health. Gender-sensitive approaches and alternative masculinity role models have the potential to enhance engagement and legitimize emotional experience. Conclusions: Hegemonic masculinity–related gender norms, acquired through gender-differentiated socialization, are associated with adverse mental health outcomes among men. A lack of gender-sensitive awareness campaigns to reduce stigma around men’s mental health may hinder prevention, delaying early identification and timely intervention. Therefore, men’s mental health care should integrate gender and intersectionality transversally to improve prevention, access, diagnosis, treatment, adherence, and outcomes, supported by professional training and tailored therapeutic tools in clinical routine practice. These findings underscore the need to promote healthier, more egalitarian masculinities and to deconstruct stigmas associated with help-seeking and mental health service.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Data Sources and Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Selection and Evaluation Process
3. Results
3.1. Traditional Masculinity Norms as Barriers to Men’s Mental Health Help-Seeking
3.2. Hegemonic Masculinity and Structural Constraints Limiting Men’s Access to Mental Health Resources
3.3. Weak Therapeutic Alliance and Perceived Ineffectiveness as Drivers of Treatment Dropout Among Men
3.4. Study Limitations of the Analyzed Studies

| Authors/Year | Objective | Sample (gender and age) | Main findings | Main limitations |
|---|---|---|---|---|
| Lynch et al. (2016) [44]. | To explore the barriers faced by young men aged 18 to 24 in seeking professional help for mental health problems, and to analyze the solutions they propose that are relevant to their lived realities. This aims to improve the mental health of this demographic group, enhance meaningful interventions, and contribute to suicide prevention measures. | The study sample consisted of 17 young men aged between 18 and 24 years, residing in County Donegal, in northwestern Ireland. | The main findings of the study identify seven key barriers to young men’s help-seeking professional support: peer acceptance, personal challenges, cultural and environmental influences, self-medication with alcohol, negative perceptions of professional help, fear of homophobic responses, and traditional masculine ideals. | Recruitment difficulties: The sensitive nature of the topic limited participant availability. Specific sample: Most participants were involved in a youth center, thereby excluding the voices of young men less willing to discuss mental health issues and of groups such as young men from the Irish Traveller community. Limited generalizability: The findings are not applicable to other countries, although parallels may be drawn with contexts characterized by a strong Catholic heritage. Potential bias: Despite measures such as member checking and reflexivity, latent biases on the part of the lead researcher may remain. |
| Wilson et al. (2022). [45]. | The primary objective of the study is to examine parents’ and teachers’ perceptions of the development of masculinity within a private all-boys school context, as well as their views on priorities for school-based initiatives designed to support students toward positive trajectories of masculine identity development. In addition, the study seeks to identify potential links with the promotion of mental health through changes in masculine norms. | The study sample consisted of 16 participants, including 10 parents (6 women and 4 men, all with a child in Year 11) and 6 teachers (3 women and 3 men), recruited from a high-fee private all-boys school in Melbourne, Australia. | Students adjust their behavior according to the social context, adopting “masks” to conform to traditional masculine norms. Sporting culture and “blokey” humor reinforce traditional masculine norms. Such schools can both challenge and reinforce traditional masculine norms. The findings highlight the importance of engaging parents and teachers in school-based initiatives to promote healthy masculinities and improve students’ mental health. |
Limited sample: The study focused on a single high-fee private all-boys school, which restricts the generalizability of the findings to other contexts, such as lower-resourced or coeducational schools. Homogeneous participants: All participants identified as heterosexual, limiting the applicability of the findings to parents and teachers from sexual minority groups. Potential response bias: Participants with a particular interest in the topic may have been more likely to take part, and some may have censored their responses due to fear of judgment. Cis-heteronormative focus: The prevailing perspective may have limited the exploration of diverse masculinities, such as those of transgender or non-binary individuals. These limitations highlight the need for more inclusive and diverse research. |
| Kwon et al. (2023). [46]. | The primary objective of the study is to better understand the reasons men give for disengaging from mental health services and to identify factors that could facilitate their re-engagement with the care system. | The study sample included 73 men who participated in a national survey conducted by Lived Experience Australia (LEA). These participants were users of mental health services in Australia. | Reasons for men’s disengagement: These include a lack of autonomy, professionalism, and authenticity within services, as well as systemic barriers such as inconsistency, insufficient follow-up, and accessibility issues. Factors that may facilitate re-engagement: Key factors include clinician-initiated reconciliation, support from community workers and peers with lived experience, and the simplification of processes for re-entering services. |
Small sample size: Only 73 men participated. Limited survey period: The survey was open for only three weeks. Lack of diversity: Ethnic, cultural, and sexual minority groups were underrepresented. Absence of specific data: Diagnostic information was not collected, nor were data disaggregated for young men aged 18–24 years. Limited generalizability: The findings may not be applicable to other countries or contexts. |
| Stewart & Harmon. (2004). [47]. | The primary objective of the study is to challenge traditional beliefs about angry men, who are frequently diagnosed with antisocial personality disorder (ASPD) and often regarded as untreatable cases. The article seeks to explore similarities between ASPD and borderline personality disorder (BPD), highlighting their association with childhood trauma and proposing a re-evaluation of diagnosis and treatment approaches. | The study includes a detailed case study of a 31-year-old man referred to as “John” (a pseudonym), who presented with aggressive behaviors, a history of childhood trauma, mental health difficulties, and challenges in his interpersonal relationships. This case is used to illustrate the challenges and therapeutic approaches involved in the treatment of men with aggressive behaviors and borderline personality disorder. | The main findings indicate that men with aggressive behaviors and antisocial personality disorder (ASPD) can benefit from structured therapeutic approaches that consider their traditional values and childhood trauma. The case study demonstrates that, with connection, clear boundaries, and ongoing support, significant improvements in mental health and behavior are achievable. | The main limitations include diagnostic bias between ASPD and BPD, a lack of differentiation between antisocial behaviors and antisocial personality traits, and the prevailing perception of ASPD as untreatable. In addition, traditional therapeutic approaches are often incompatible with traditional masculine values, which may hinder men’s engagement in treatment. |
| Boettcher et al. (2019). [48]. | The primary objective of the study is to contribute to the theoretical understanding of work-related mental health experiences among men and to explore opportunities for employers to provide gender-sensitive support for men’s mental health. Specifically, the study examines how masculine role norms influence work-related stress and mental health, using narratives from men employed in male-dominated occupations. | The study sample comprised 18 men employed in male-dominated occupations, selected from a larger pool of 37 participants. These men were working full-time, and the majority appeared to be Caucasian and based in Canada. | The main findings show that masculine role norms influence men’s work-related stress and mental health. These norms are divided into three types: Descriptive norms: Men adjust their work behavior according to that of their peers, which can normalize overwork and make help-seeking more difficult. Injunctive norms: Internal beliefs about what men “should” do at work, generating anxiety and questioning of personal worth during periods of low productivity. Cohesive norms: Leaders model and communicate performance expectations, often contradicting mental health support policies. These norms reinforce behaviors that may compromise men’s mental health in the workplace. |
Sample homogeneity: Most participants were Caucasian and from a middle-to-upper socioeconomic background, which limits the representation of men from diverse backgrounds. Participant self-selection: Men interested in discussing workplace mental health may have biased the results. Lack of occupational diversity: Only full-time employed men were included, excluding the perspectives of part-time or precariously employed workers. Overrepresented sector: A predominance of participants from the energy sector, which was affected by the economic recession. Secondary data: The analysis was based on responses to general questions about work-related stress, rather than specifically on masculine role norms. |
| Edwards et al. (2017). [49]. | The primary objective of the study is to analyze differences between male and female caregivers using data from the 2009 Behavioral Risk Factor Surveillance System (BRFSS). | The study sample was drawn from the 2009 Behavioral Risk Factor Surveillance System (BRFSS), which included 421,215 participants from all 50 U.S. states. | Gender distribution: Two-thirds of caregivers were women. Unhealthy days: Women reported more physically and mentally unhealthy days than men. Social support: Men were more likely to report rarely or never receiving social support, but the impact of social support on quality of life was stronger for men than for women. Associated factors: Age, education, and social support were associated with fewer unhealthy days, whereas smoking and physical inactivity were associated with more unhealthy days. |
Caregiving period: The BRFSS question only covered the previous month, excluding caregivers outside that period. Telephone coverage: Only individuals with landline telephones were included, which may have underrepresented younger adults and those with fewer resources. Measurement of social support: A single item was used, which is less precise than a full scale. Marital relationship: The quality of marital relationships was not assessed, which may have influenced the results. |
| Seidler et al. (2019). [50]. | The primary objective of the study is to examine perceived barriers—both attitudinal and structural—that hinder men’s access to mental health services. In addition, the study seeks to analyze the associations between these barriers and men’s intentions to seek or not seek treatment for their mental health concerns. | The study sample consisted of 778 men who reported experiencing a mental health concern and were not receiving treatment at the time. |
Common barriers: The most frequent barriers were attitudinal, such as “many people feel sad and depressed” (80%) and “I need to solve my own problems” (73%), and structural, such as “I do not know what to look for in a psychotherapist” (80%) and “I cannot afford psychotherapy” (72%). Differences by treatment intention: Men who did not want treatment were more likely to doubt the effectiveness of psychotherapy, not disclose their emotional state to their physician, and prefer to solve their problems on their own. Predictive factors: Attitudinal barriers, such as the need to solve problems independently, were significant predictors of not wanting treatment. |
Cross-sectional design: The data were based on a single survey, which limits the ability to examine changes over time. Predefined barriers: Not all possible barriers were included, which may have led to the omission of important factors. Specific sample: Participants had already recognized a mental health concern and were recruited through an online resource, limiting generalizability to men who do not seek help or lack awareness of their mental health. Prior interaction: It is unclear whether use of the HeadsUpGuys website influenced participants’ responses. |
| Tibubos et al. (2022). [51]. | The primary objective of the study is to develop and validate a brief measure to assess gender expression using a shortened version of the Personal Attributes Questionnaire (PAQ-8), and to examine its associations with mental distress in the German population in 2006 and 2018. In addition, the study aims to explore how expressions of femininity and masculinity contribute to the mental health gap between men and women. | The study sample includes data from two representative studies conducted in Germany in 2006 and 2018. Participant information is detailed below: Year 2006: Total participants: 2,507 individuals. Mean age: 48 years (standard deviation: 18.1). Representativeness: The sample was representative of the general German population in terms of age, sex, and educational level. Year 2018: Total participants: 2,516 individuals. Mean age: 48 years (standard deviation: 17.6). Representativeness: Similar to the 2006 study, with comparisons made using census data from the German Federal Statistical Office. |
PAQ-8 validity: The brief version of the questionnaire (PAQ-8) is a valid measure for assessing gender expression, with good internal consistency and the ability to distinguish between masculinity and femininity. Changes in gender expression: Between 2006 and 2018, femininity increased among women and decreased among men, while masculinity remained stable. Association with mental distress: Higher levels of femininity and masculinity were associated with lower mental distress. Gender expression was a better predictor of mental health than biological sex. Impact of time: An increase in gender differences in the expression of femininity between men and women was observed over time. |
Lack of non-binary categories: Gender options beyond male and female were not included, excluding individuals with diverse gender identities. Limited aspects of gender: Only gender expression (masculinity and femininity) was assessed, leaving out other dimensions of gender. Cross-sectional nature: The data were derived from cross-sectional studies, preventing the establishment of causal relationships. Selection bias: Non-participation by some individuals may have introduced bias into the sample. Androgynous gender not assessed: Although mentioned in theory, androgynous gender was not included as a separate category in the analysis. |
| Sharp et al. (2023). [52]. | The primary objective of the study is to explore the influence of masculinities and Australian culture on men’s mental health. | The study sample included 43 men (mean age: 50.7 years, SD: 13.8) residing in the Greater Sydney and Blue Mountains regions of New South Wales, Australia. | History of strength and self-reliance: Traditional masculine norms in Australia, such as resilience and the “she’ll be right” attitude, make it difficult for men to seek help for their mental health. Social and geographical divisions: Although the culture of “mateship” promotes connection among men, it often limits emotional expression and genuine support. Masculine socialization and generational disconnection: Restrictive masculine norms, such as emotional repression, are transmitted across generations, but some men are renegotiating these norms to promote healthier behaviors. |
Contextuality of masculinities: The findings do not reflect the experiences of all men in Australia due to local and cultural specificities. Participant self-selection: Men less willing to discuss their mental health may have been excluded. Lack of linkage between quotations and demographic characteristics: Specific participant data were not recorded for the quoted excerpts. Intersection with social determinants: Factors such as economic hardship, racism, or discrimination against marginalized groups were not sufficiently explored. |
| Mesler et al. (2022). [53]. | The primary objective of the study is to clarify the relationships between masculine gender role discrepancy, discrepancy stress, and traditional masculinity ideology in men’s health-related behaviors. | The study sample consisted of 459 men with a mean age of 34.07 years (SD = 12.06). Participants were recruited via the Prolific Academic platform and came from three countries: 56.6% from the United Kingdom, 29.4% from the United States, and 14% from Canada. | The main findings indicate that discrepancy stress negatively mediates the relationship between masculine gender role discrepancy and health-promoting behaviors, such as proactive safety, healthy social relationships, and stress management. In addition, discrepancy stress is positively associated with negative mental health outcomes. These effects are stronger among men with greater adherence to traditional masculinity ideology. | The main limitations include the use of an online sample, which may introduce attentional biases, a single method design that may produce common method bias, and small, albeit statistically significant, effect sizes. In addition, the use of multiple subscales may have increased the risk of Type I error. |
| Mostoller et al. (2024). [54]. | To analyze the role of help seeking stigma as a mediating mechanism linking conformity to traditional masculine norms with men’s mental health status. To investigate how traditional masculine norms, internalized from an early age, influence perceptions of help seeking mental health problems and their impact on psychological well-being. |
In the study, 326 men residing in the United States participated, aged between 18 and 75 years (mean age of 33 years). Among them, 12 identified as transgender men, who were also included in the analyses, as conformity to masculine norms may affect both cisgender and transgender men. |
The main findings of the study indicate that conformity to masculine norms is associated with greater self-stigma related to help seeking, which in turn is linked to higher levels of perceived stress, but not to depression. In addition, specific aspects of masculinity, such as self-reliance, heterosexual presentation, and power over women, influence self-stigma and, in some cases, mental health. |
Homogeneous sample: Predominance of White, cisgender, and heterosexual men, with low variability in the variables studied. Cross sectional design: This prevents establishing causality or examining changes over time. Lack of cultural diversity: Differences in masculine norms across ethnic and cultural contexts were not explored. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seidler, Z.E.; Wilson, M.J.; Walton, C.C.; Fisher, K.; Oliffe, J.L.; Kealy, D.; Rice, S.M. Australian men's initial pathways into mental health services. Health Promot J Austr 2021, 00, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Oliffe, J.L.; Han, C.S.E. Beyond workers’ compensation: Men’s mental health in and out of work. Am J Mens Health 2014, 8, 45–53. [Google Scholar] [CrossRef]
- Addis, M.E. Gender and depression in men. Clin Psychol Sci Pract 2008, 15, 153–168. [Google Scholar] [CrossRef]
- Connell, R.W.; Messerschmidt, J.W. Hegemonic masculinity: Rethinking the concept. Gend Soc 2005, 19, 829–859. [Google Scholar] [CrossRef]
- Courtenay, W. Constructions of masculinity and their influence on men’s well-being: A theory of gender and health. Soc Sci Med 2000, 50, 1385–1401. [Google Scholar] [CrossRef]
- Kimmel, M. Angry (White) Men: Masculinity at the End of an Era [Hombres (blancos) cabreados: La masculinidad al final de una era; Barlin Libros: Valencia, 2023. [Google Scholar]
- World Health Organization Regional Office for Europe. WHO Regional Committee for Europe resolution EUR/RC68/R4 on a strategy on the health and well-being of men in the WHO European Region; WHO Regional Office for Europe: Copenhagen, 2018. [Google Scholar]
- Scourfield, J.; Fincham, B.; Langer, S.; Shiner, M. Sociological autopsy: An integrated approach to the study of suicide in men. Soc. Sci. Med. 2012, 74, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Brownhill, S.; Wilhelm, K.; Barclay, L.; Schmied, V. ‘Big build’: Hidden depression in men. Aust. N. Z. J. Psychiatry 2005, 39, 921–931. [Google Scholar]
- Rice, S.M.; Purcell, R.; McGorry, P.D. Adolescent and young adult male mental health: Transforming system failures into proactive models of engagement. J Adolesc Health 2018, 62, S9–S17. [Google Scholar] [CrossRef] [PubMed]
- Walther, A. Gender-biased diagnosis and treatment of depression: considering our blind eye on men's depression. Int. J. Equity Health 2025, 24, 190. [Google Scholar] [CrossRef]
- Bacigalupe, A.; Martín, U.; Triolo, F.; Sjöberg, L.; Sterner, T.R.; Dekhtyar, S.; Fratiglioni, L.; Calderón-Larrañaga, A. Is the diagnosis and treatment of depression gender-biased? Evidence from a population-based aging cohort in Sweden. Int. J. Equity Health 2024, 23, 252. [Google Scholar] [CrossRef]
- Cavanagh, A.; Wilson, C.J.; Kavanagh, D.J.; Caputi, P. Differences in the Expression of Symptoms in Men Versus Women with Depression: A Systematic Review and Meta-analysis. Harv. Rev. Psychiatry 2017, 25, 29–38. [Google Scholar] [CrossRef]
- Sedlinská, T.; Mühle, C.; Richter-Schmidinger, T.; Weinland, C.; Kornhuber, J.; Lenz, B. Male depression syndrome is characterized by pronounced Cluster B personality traits. J. Affect. Disord. 2021, 292, 725–732. [Google Scholar] [CrossRef]
- Streb, J.; Ruppel, E.; Möller-Leimkühler, A.-M.; Büsselmann, M.; Franke, I.; Dudeck, M. Gender-Specific Differences in Depressive Behavior Among Forensic Psychiatric Patients. Front. Psychol. 2021, 12, 639191. [Google Scholar] [CrossRef]
- Camacho-Ruiz, J.A.; Galvez-Sánchez, C.M.; Galli, F.; Liminana-Gras, R.M. Patterns and Challenges in Help-Seeking for Addiction Among Men: A Systematic Review. J Clin Med 2024, 13, 6086. [Google Scholar] [CrossRef]
- Addis, M.E.; Mahalik, J. Men, masculinity, and the contexts of help seeking. Am Psychol 2003, 58, 5–14. [Google Scholar] [CrossRef]
- Levant, R.F.; Stefanov, D.G.; Rankin, T.J.; Halter, M.J.; Mellinger, C.; Williams, C.M. Moderated path analysis of the relationships between masculinity and men’s attitudes toward seeking psychological help. J Couns Psychol 2013, 60, 392–406. [Google Scholar] [CrossRef] [PubMed]
- Vogel, D.L.; Heimerdinger-Edwards, S.R.; Hammer, J.H.; Hubbard, A. “Boys don’t cry”: Examination of the links between endorsement of masculine norms, self-stigma, and help-seeking attitudes for men from diverse backgrounds. J. Couns. Psychol. 2011, 58, 368–382. [Google Scholar] [CrossRef] [PubMed]
- Mahalik, J.R.; Good, G.E.; Englar-Carlson, M. Masculinity Scripts, Presenting Concerns, and Help Seeking: Implications for Practice and Training. Prof. Psychol. Res. Pract. 2003, 34, 123–131. [Google Scholar] [CrossRef]
- Real, T. How Can I Get Through to You? Closing the Intimacy Gap Between Men and Women; Scribner: New York, NY, USA, 2003. [Google Scholar]
- Galdas, P.M.; Cheater, F.; Marshall, P. Men and health help-seeking behaviour: literature review. J. Adv. Nurs. 2005, 49, 616–623. [Google Scholar] [CrossRef]
- Gough, B.; Robertson, S. Men, masculinities and health: Critical perspectives; Palgrave Macmillan: Basingstoke, 2010. [Google Scholar]
- Gough, B. Men’s depression talk online: A qualitative analysis of accountability and authenticity in help-seeking and support formulations. Psychol Men Masc 2016, 17, 156–164. [Google Scholar] [CrossRef]
- Englar-Carlson, M.; Kiselica, M.S. Affirming the strengths in men: A positive masculinity approach to assisting male clients. J. Couns. Dev. 2013, 91, 399–409. [Google Scholar] [CrossRef]
- Hooks, B. The Desire to Change: Men, Masculinity and Love [El Deseo de Cambiar: Hombres, Masculinidad y Amor]; Bellaterra Editions: Manresa, Spain, 2021. [Google Scholar]
- Crenshaw, K. Demarginalizing the Intersection of Race and Sex: A Black Feminist Critique of Antidiscrimination Doctrine, Feminist Theory and Antiracist Politics. Univ. Chic. Legal Forum 1989, 1, 139–167. [Google Scholar]
- Frosh, S. After Words: The Personal in Gender, Culture, and Psychotherapy; Palgrave Macmillan: New York, NY, USA, 2002. [Google Scholar]
- Jordan, J.; McKenna, H.; Keeney, S.; Cutcliffe, J. Providing Meaningful Care: Using the Experiences of Young Suicidal Men to Inform Mental Health Care Services: Research Report; Ulster University: Northern Ireland, 2012. [Google Scholar]
- Messner, M.A. Forks in the Road of Men’s Gender Politics: Men’s Rights vs Feminist Allies. Int. J. Crime Justice Soc. Democr. 2016, 5, 6–20. [Google Scholar] [CrossRef]
- Frosh, S.; Phoenix, A.; Pattman, R. Young Masculinities: Understanding Boys in Contemporary Society; Palgrave Macmillan: Basingstoke, UK, 2002. [Google Scholar]
- Seidler, Z.E.; Dawes, A.J.; Rice, S.M.; Oliffe, J.L.; Dhillon, H.M. The role of masculinity in men's help-seeking for depression: A systematic review. Clin Psychol Rev 2016, 49, 106–118. [Google Scholar] [CrossRef] [PubMed]
- Robertson, S.; Gough, B.; Hanna, E.; Raine, G.; Robinson, M.; Seims, A.; et al. Successful mental health promotion with men: Evidence from “tacit knowledge”. Health Promot Int 2018, 33, 334–344. [Google Scholar] [CrossRef]
- Mahalik, J.R.; Rochlen, A.B. Men’s Likely Responses to Clinical Depression: What Are They and Do Masculinity Norms Predict Them? Sex Roles 2006, 55, 659–667. [Google Scholar] [CrossRef]
- APA Handbook of Men and Masculinities; Wong, Y.J., Wester, S.R., Eds.; American Psychological Association: Washington, DC, USA, 2016. [Google Scholar]
- Seidler, Z.E.; Rice, S.M.; Kealy, D.; Oliffe, J.L.; Ogrodniczuk, J.S. What gets in the way? Men’s perspectives of barriers to mental health services. Int. J. Soc. Psychiatry 2020, 66, 105–110. [Google Scholar] [CrossRef]
- Seidler, Z.E.; Rice, S.M.; Ogrodniczuk, J.S.; Oliffe, J.L.; Dhillon, H.M. Engaging Men in Psychological Treatment: A Scoping Review. Am. J. Mens Health 2018, 12, 1882–1900. [Google Scholar] [CrossRef]
- Rice, S.M.; Telford, N.R.; Rickwood, D.J.; Parker, A.G. Young men’s access to community-based mental health care: Qualitative analysis of barriers and facilitators. J. Ment. Health 2018, 27, 59–65. [Google Scholar] [CrossRef]
- Oliffe, J.L.; Seidler, Z.E.; Kelly, M.T.; Gonzalez Montaner, G.; Kealy, D.; Ogrodniczuk, J.S.; Rice, S.M. Mapping men’s mental health help-seeking after an intimate partner relationship break-up. Qual Health Res 2022, 32, 1464–1476. [Google Scholar] [CrossRef]
- Bailey, A.H.; LaFrance, M.; Dovidio, J.F. Implicit androcentrism: Men are human, women are gendered. J. Exp. Soc. Psychol. 2020, 89, 103980. [Google Scholar] [CrossRef]
- Verdonk, P.; Benschop, Y.W.M.; de Haes, H.C.J.M.; Lagro-Janssen, T.L.M. From gender bias to gender awareness in medical education. Adv. Health Sci. Educ. 2009, 14, 135–152. [Google Scholar] [CrossRef] [PubMed]
- Merone, L.; Tsey, K.; Russell, D.; Nagle, C. Sex inequalities in medical research: A systematic scoping review of the literature. Womens Health Rep. 2022, 3, 49–59. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Lynch, L.; Long, M.; Moorhead, A. Young men, help-seeking, and mental health services: Exploring barriers and solutions. Am J Mens Health 2016, 11, 1–12. [Google Scholar] [CrossRef]
- Wilson, M.J.; Gwyther, K.; Simmons, M.; Swann, R.; Oliffe, J.L.; Casey, K.; Rice, S.M. Exploring teacher and parent perspectives on school-based masculinities in relation to mental health promotion. Front Psychol 2022, 13, 864124. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.; Lawn, S.; Kaine, C. Understanding men’s engagement and disengagement when seeking support for mental health. Am J Mens Health 2023, 17, 1–15. [Google Scholar] [CrossRef]
- Stewart, D.; Harmon, K. Mental health services responding to men and their anger. Int J Ment Health Nurs 2004, 13, 249–254. [Google Scholar] [CrossRef]
- Boettcher, N.; Mitchell, J.; Lashewicz, B.; Jones, E.; Wang, J.; Gundu, S.; Marchand, A.; Michalak, E.; Lam, R. Men’s work-related stress and mental health: Illustrating the workings of masculine role norms. Am J Mens Health 2019, 13, 1–10. [Google Scholar] [CrossRef]
- Edwards, V.J.; Anderson, L.A.; Thompson, W.W.; Deokar, A.J. Mental health differences between men and women caregivers, BRFSS 2009. J Women Aging 2017, 29, 385–391. [Google Scholar] [CrossRef]
- Seidler, Z.E.; Wilson, M.J.; Kealy, D.; Oliffe, J.L.; Ogrodniczuk, J.S.; Rice, S.M. Men’s dropout from mental health services: Results from a survey of Australian men across the life span. Am J Mens Health 2021, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tibubos, A.N.; Otten, D.; Beutel, M.E.; Brähler, E. Validation of the Personal Attributes Questionnaire-8: Gender Expression and Mental Distress in the German Population in 2006 and 2018. Int J Public Health 2022, 67, 1604510. [Google Scholar] [CrossRef]
- Sharp, P.; Oliffe, J.L.; Bottorff, J.L.; Rice, S.M.; Schulenkorf, N.; Caperchione, C.M. Connecting Australian masculinities and culture to mental health: Men’s perspectives and experiences. Men Masc 2023, 26, 112–133. [Google Scholar] [CrossRef]
- Mesler, R.M.; Leary, R.B.; Montford, W.J. The relationships between masculine gender role discrepancy, discrepancy stress and men's health-related behavior. Pers Individ Dif 2022, 184, 111205. [Google Scholar] [CrossRef]
- Mostoller, A.M.; Mickelson, K.D. Masculinity and mental well-being: The role of stigma attached to help-seeking among men. Sex Roles 2024, 90, 353–362. [Google Scholar] [CrossRef]
- O’Neil, J.M. Summarizing 25 Years of Research on Men’s Gender Role Conflict Using the Gender Role Conflict Scale: New Research Paradigms and Clinical Implications. Couns. Psychol. 2008, 36, 358–445. [Google Scholar] [CrossRef]
- Oliffe, J.L.; Han, C.S.E.; Ogrodniczuk, J.S.; Phillips, J.C.; Roy, P. Suicide from the perspectives of older men who experience depression: A gender analysis. Am J Mens Health 2011, 5, 444–454. [Google Scholar] [CrossRef]
- Seidler, Z.E.; Wilson, M.J.; Trail, K.; Rice, S.M.; Kealy, D.; Ogrodniczuk, J.S.; Oliffe, J.L. Challenges working with men: Australian therapists’ perspectives. J. Clin. Psychol. 2021, 77, 2781–2797. [Google Scholar] [CrossRef]
- Gough, B. Try to Be Healthy, but Don’t Forgo Your Masculinity: Deconstructing Men’s Health Discourse in the Media. Soc. Sci. Med. 2006, 63, 2476–2488. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



