
Submitted:
31 December 2025
Posted:
01 January 2026
You are already at the latest version
Abstract
Bruton's tyrosine kinase (BTK) inhibitors have revolutionized the treatment landscape for patients with indolent lymphoid malignancies such as chronic lymphocytic leukaemia (CLL) and mantle cell lymphoma (MCL). The most common adverse events include cardiac arrhythmia, bleeding, infection, diarrhoea, arthralgias, hypertension and skin changes. Second-generation BTK inhibitors, e.g. acalabrutinib and zanubrutinib, and the non-covalent BTK inhibitor pirtobrutinib, are less toxic than the first-generation BTK inhibitor ibrutinib. The most common skin toxic symptoms related to BTKi treatment include haemorrhage, bleeding events, bruising, skin ecchymoses and contusion; these are particularly common in patients treated with ibrutinib. Other dermatologic symptoms include rash, cellulitis, skin infections, subcutaneous abscesses and peripheral oedema. This article discusses the development of skin symptoms in patients with ibrutinib and newer BTK inhibitors, and summarises their clinical and pathological characteristics. A literature search was performed using PubMed, Web of Science, and Google Scholar for articles published in English. Additional relevant publications were obtained by reviewing the references from the chosen articles.
Keywords:
acalabrutinib
; bleeding
; BTK inhibitors
; ibrutinib
; infections
; mucosal symptoms
; neutrophilic dermatoses
; rash
; skin toxicity
; vasculitis
; zanubrutinib
1. Introduction
Over the past decade, the treatment landscape for indolent B-cell lymphoid malignancies has shifted from chemotherapy and immunochemotherapy to targeted oral therapies [1], with the Bruton’s tyrosine kinase (BTK) inhibitors ibrutinib, acalabrutinib and zanubrutinib playing the key role [2,3]. These agents effectively inhibit B-cell receptor (BCR) signalling in neoplastic B-cells and they are most commonly used in slow-growing indolent non-Hodgkin lymphoma (NHL). According to the 5th Edition of the World Health Organization Classification and International Consensus Classification (ICC)indolent NHLs comprise chronic lymphocytic leukaemia/small lymphocytic lymphoma (CLL/SLL), follicular lymphoma (FL), marginal zone lymphoma (MZL), lymphoplasmacytic lymphoma, mantle cell lymphoma (MCL) and hairy cell leukaemia (HCL), together with various other rarer entities [4]. BTK inhibitors can also play active roles in treating autoimmune disorders like autoimmune haemolytic anaemia (AIHA), immune thrombocytopenia (IT), multiple sclerosis, pemphigus vulgaris, atopic dermatitis, rheumatoid arthritis, systemic lupus erythematosus and Sjögren’s disease [5].
BTK inhibitors are divided into covalent irreversible BTKis, such as ibrutinib, acalabrutinib and zanubrutinib, and non-covalent, reversible BTK inhibitors, such as pirtobrutinib and nemtabrutinib. Ibrutinib was the first-in-class covalent, irreversible BTK inhibitor, which was approved in 2013 for the treatment of CLL [1]. Since then, two other covalent, irreversible, second-generation BTK inhibitors, acalabrutinib and zanubrutinib, were developed. These next-generation BTK inhibitors present more selective binding to BTK than ibrutinib and hence possess a better safety profile [6]. However, they are still associated with similar dermatological toxicities.
Among the non-covalent, reversible BTK inhibitors, the most advanced forms tested in clinical trials are pirtobrutinib and nemtabrutinib. Neither act by binding to the C481 residue, and are hence effective in patients with BTK C481 mutation. Pirtobrutinib was highly selective for BTK, with greater than 100-fold selectivity over other tested kinases, thus minimizing off-target activity and potentially lowering the risk of bleeding and other toxicities [6,7]. This group of BTKis are designed to address some of the limitations of covalent BTK inhibitors, allowing them to overcome drug resistance and demonstrate greater safety.
While BTK inhibitors are relatively safe and well-tolerated drugs [8], their use has been associated with certain common adverse events (AEs). The most common include cardiac arrhythmia, bleeding, infection, diarrhoea, arthralgias, hypertension and skin changes [9]. Cutaneous toxicity has been reported as one of the most common non-haematological side effects of ibrutinib [9]. Dermatological AEs have been reported in 2–27% of patients treated with mostly mild to moderate intensity [10,11,12], and most commonly occur during the first year of treatment [12]. While dermatological AEs are generally scarce, their presence can lead to ibrutinib discontinuation in a small proportion of patients [12,13,14,15]. A retrospective analysis of 46 real-world acalabrutinib-treated CLL patients intolerant to ibrutinib found that rash led to discontinuation of acalabrutinib in 10 (22%) patients. During treatment with acalabrutinib, with a median follow-up of five months, a rash was noted in five (7%) patients [15]. The most common cutaneous AEs associated with BTK inhibitors include rash, bleeding and bruising, ecchymoses, neutrophilic panniculitis, hair and nail changes, skin infections bruising, petechiae and purpuric eruption [12,13,14,15,16,17].
Dermatological toxicities were reported in ≥10% patients treated with zanubrutinib [18]. Grade 4 dermatological toxicities developed within one month after treatment; these included bruising, maculopapular rash, ecchymosis, haemorrhagic blister, acne-like rash, papulopustular rash, and skin infections. Several clinical trials indicated that zanubrutinib-related skin side effects are well tolerated and can be managed with symptomatic treatment in most patients; however, in some patients, drug discontinuation is required [19].
The mechanism of skin toxicity in patients treated with BTK inhibitors is multifactorial and mostly related to the off-target activity of these agents. In addition to BTK inhibition, ibrutinib can inhibit other kinases, including Src (Rous sarcoma virus) kinase, tyrosine-protein kinase (TEC), and epidermal growth factor receptor (EGFR) [20]. In contrast, second-generation BTK inhibitors, e.g., acalabrutinib and zanubrutinib, have fewer off-target effects.
Some of these effects are associated with the epidermal growth factor receptor (EGFR) pathway, which stimulates epidermal growth by regulating the normal growth and differentiation process of the epidermis. EGFR receptors are expressed on keratinocytes, which are distributed in the basal and suprabasal layers of the epidermis. EGFR inhibition causes premature skin cell differentiation, inflammation, apoptosis, skin atrophy, telangiectasia, and photosensitivity [21]. In addition, in the first few weeks of BTKi therapy in patients with CLL and the leukemic form of non-Hodgkin lymphoma (NHL), the patients may demonstrate inhibition of c-kit and platelet-derived growth factor (PDGF) receptors resulting in increased lymphocytosis [10].
Dermatological toxicities associated with BTK inhibitors are mainly noted in the first year of treatment, and their incidence decreases gradually with time [9,12]. Treatment of BTKi-induced dermatologic toxicity depends on the grade of EAs. In patients with moderate to severe dermatological toxicities, topical steroid ointments used alone or in combination with topical emollients are recommended. In patients with grade 4 toxicities, systemic antibiotics or antibiotic ointments should be used in patients with infection; otherwise dose reduction or temporarily discontinuation should be considered [19,22].
This article presents the clinical and pathological characteristics of skin symptoms in patients treated with BTK inhibitors. The literature included in the review was identified through a search of PubMed, Web of Science, and Google Scholar; all articles were published in English. Additional relevant publications were obtained by reviewing the references from the chosen articles.
2. Hemoragic Symptoms in the Skin
A common hemorrhagic skin complications of BTK inhibitors are bruising, hematomas and petechiae (Figure 1 and Figure 2). An analysis of 15 ibrutinib clinical trials for lymphoid malignancies found any-grade bleeding to occur in 40% of patients [23], with only 4% of patients developing major haemorrhage, and 1% of all treated cases leading to ibrutinib discontinuation. In a pooled analysis of three pivotal studies encompassing 330 patients with CLL treated with ibrutinib, bleeding/bruising events were observed in 55% of patients, and 25 major haemorrhage events were reported in 21 patients (6%) [24].
The haemorrhagic skin complications of BTK inhibitors include bruising, skin hematomas, ecchymoses, haemorrhagic crusting or blisters and purpuric nodules/ eruption [24,25,26]. The risk of BTK inhibitor-associated bleeding peaks during the first year of treatment, and decreases over subsequent years.
The elevated risk of bleeding is mainly due to inhibition of platelet function by BTK inhibitors, largely attributed to interference with platelet glycoprotein (GP) VI signaling and TEC inhibition involved in platelet activation and aggregation [27]. Moreover, patients treated with BTKis show reduced collagen-mediated platelet aggregation, which correlates with the occurrence of clinical bleeding [28]. Moreover, patients treated with dual-antiplatelet therapy or systemic anticoagulants are at a ghier risk of bleeding following BTK inhibitor use [29,30].
The risk of bleeding has been found to be was 2.5-fold higher among patients treated with ibrutinib and anticoagulant compared with those treated with ibrutinib alone [31].
Acalabrutinib and zanubrutinib, i.e., more selective BTK inhibitors with less off-target activity than ibrutinib, also have lower antiplatelet activity [32]. A pooled analysis of 1040 patients with mature B-cell lymphoid malignancies treated with acalabrutinib monotherapy found haemorrhage to occur in 46% of cases, with 4% demonstrating a major haemorrhage (grade ≥3 AEs) [33]. Another pooled analysis of 779 patients treated with zanubrutinib monotherapy identified haemorrhage in 55% of patients, including 4% major haemorrhage [18].
The noncovalent reversible BTK inhibitor Pirtobrutinib demonstrates improved tolerability in comparison with covalent BTK inhibitors, and may provide patients with another opportunity to safely receive BTK inhibitor therapy. In a post hoc analysis of bleeding risk in patients with B-cell malignancies treated with pirtobrutinib, bleeding/bruising events were mostly low-grade, with Grade 3 events occurring in fewer than 3% of patients [34]. All grade bleeding/bruising were observed in 44.9% of patients and grade ≥3 in 2.8%; among these, bruising was observed in 27.8%, contusion in 22.7% and petechiae in 3.7%, Moreover, patients who received concomitant antithrombotic therapy were more likely to demonstrate bleeding/bruising events (44.9%) than those who did not (32.5%), although the antithrombotic therapy group did not experience any grade 4–5 bleeding/bruising events.
Ecchymoses or bruises have been widely described with BTK inhibitors [12,35,36,37]. Ecchymoses are more common in older patients, particularly on skin exposed to the sun. Among patients receiving BTK inhibitors, ecchymoses and bruises should be managed with emollients and by preventing sun exposure. However, more severe dermatologic lesions require BTKi treatment cessation. Acalabrutinib-induced ecchymotic lesions have also been reported. Kucharik et al. describe an ecchymotic patch diagnosed as cutaneous collagenous vasculopathy (CCV) on the dorsal aspect of the left forearm in a CLL patient treated with acalabrutinib; the observed skin changes were probably due to endothelial proliferations, which may be the underlying cause of the associated vascular leakage [38]. Following acalabrutinib cessation, these skin changes improved and the patch began to resolve; however, the ecchymotic patch reappeared after restarting acalabrutinib.
Guenther et al. present another patient who developed an extensive ecchymotic patch following treatment with acalabrutinib [39]. Skin changes were characterized by superficial vascular ectasia and chronic thrombotic changes with partial occlusion of the vessels by proteinaceous debris; these were located on the dorsal aspect of the left forearm. Resolution was observed six weeks after treatment discontinuation. In another patient treated with acalabrutinib, Truong et al. described extensive, indurated, confluent purpuric eruption associated with subcutaneous swelling and pain confined to both upper limbs [40]. These changes were not reduced following acalabrutinib dose reduction to 100 mg daily.
Zanubrutinib, another second-generation BTK inhibitor, can also induce eccchymotic lesions [35,36,37]. In one case, skin lesions were located on the hands and forearms and arms; the changes were characterized as purpuric, purplish, non-infiltrated vascular patches located mainly on photo-exposed areas. Another case of zanubrutinib-induced petechial ecchymotic reaction was also noted in a patient with CLL [37]. The lesions were characterized as well-demarcated, yellow-brown macular discoloration over the right breast; they extended onto the intermammary skin and the upper abdomen with petechiae scattered throughout. Their location was restricted to a previously-irradiated area. In this region, histopathologic examination was consistent with ecchymosis, characterized by mild perivascular inflammation and focal erythrocyte extravasation in the papillary dermis. Skin changes were benign and did not require treatment discontinuation.
3. Skin Rash
BTKi-induced rashes present with a relatively non-specific and varied clinical presentation [10], ranging from asymptomatic ecchymosis, non-palpable petechial rash, to leukocytoclastic vasculitis-like palpable purpura (Figure 3) [10,41]. Rash has been reported in 13% to 27% of patients treated with ibrutinib and 13% to18% of patients treated with zanubrutinib [12,41,42,43]. Nocco et al. identified five different types of rash morphologies associated with ibrutinib therapy: non-palpable petechial rash, leukocytoclastic vasculitis-like pruritic palpable purpura, pityriasis roseae-like rash, papulopustular rash, and painless non-pruritic oedematous papules [22]. Among these, the most common clinical manifestation is acne-like rash with erythematous papules or pustules centred on the hair follicles.
The most likely mechanism of BTKi-induced skin rash is the inhibition of EGFR. However, it has also been proposed that ibrutinib-induced drug eruption may occur though the inhibition of c-kit and PDGF receptor [42].
Ibrutinib-induced rashes have been identified in the course of B-cell lymphoid malignancies, with some patients experiencing symptoms as late as 300-400 days after beginning treatment [44]. In a study of 33 ibrutinib-intolerant patients who were subsequently treated with acalabrutinib, eight (24%) reported the occurrence of a rash; of these, 6% were rash grade ≥ 3. Of the eight recorded rash events, after acalabrutinib treatment, the rash did not recur in five patients, returned at a lower grade in one patient, and returned with the same grade in two [45].
Petechial rash is believed to be caused by BTK-mediated platelet dysfunction, and usually develops several months after treatment initiation. Oedematous, or purpuric papular rashes, appear in the first few weeks of treatment and have been associated with an immune-mediated drug reaction; they are more common in patients with a history of drug hypersensitivity [22]. Patients with grade 3 rashes have also demonstrated severe allergic drug reactions, such as lip tingling and tongue swelling, following ibrutinib treatment [46].
A pityriasis rosacea-like rash can also develop as violaceous, scaly, pruritic plaques or papules, and is typically observed on the trunk. It is most likely caused by off-target inhibition of the c-Kit and PDGF receptor. In addition, off-target inhibition of EGFR can cause a papulopustular rash, which presents in the first few weeks of treatment, and can be associated with photosensitivity [17].
One case of zanubrutinib-induced petechial ecchymotic reaction has been reported in a patient with CLL [37]. Another case, presented by Zhou et al. [47], described the development of progressive rash after taking zanubrutinib for two months. The male patient developed scattered papules with mild itching in both lower limbs; these papules ruptured in multiple locations, and the ulcers gradually increased in size and depth. The ulcers were surrounded by erythema and exudate, with a scattered distribution and Cryptococcal infection. Zanubrutinib treatment was stopped and replaced with fluconazole for 10 months. The skin ulcers on both lower limbs disappeared.
Palpable rashes are commonly pruritic and associated with inhibition of EGF receptors and infiltration by inflammatory cells [42]. They have been observed in patients treated with second-generation BTK inhibitors, despite their higher selectivity [48]. Grade 4 skin rash was also reported in a patient treated with zanubtutinib [19].
Rash lesions attributable to BTK inhibitors usually resolve over a few weeks. In one study, rash resolution was observed after a median three-week course of topical corticosteroids and oral antihistamines, without the need for BTK-inhibitor cessation [42]. Elsewhere, resolution was achieved in two weeks in patients treated with oral steroids, antihistamines and temporary BTK-inhibitor cessation [43]. For more severe or persistent rash, temporary suspension of BTK-inhibitor therapy and use of topical or oral corticosteroids should be considered until resolution of cutaneous symptoms [10,42,49,50].
4. Vasculitis
Vasculitis is a group of diseases characterized by inflammation of the walls of blood vessels, which can lead to their narrowing, ischemia and even bleeding. Diagnosis of ibrutinib-induced vasculitis is challenging, as the clinical manifestation of a specific vasculitic disorder depends on various factors, including the size and location of the involved vessels, and the degree and pattern of extravascular inflammation [38].
Rodriguez-Baeza describe a patient with MCL receiving ibrutinib treatment who presented repeated episodes of lymphocytic vasculitis (LyV) [51]. Multiple erythematous papular lesions were observed to develop on the legs and arms several times, although each outbreak was followed by spontaneous resolution, without any need for treatment discontinuation. A biopsy of the lesion showed the presence of a dense infiltrate of lymphocytes, monocytes, and scattered eosinophils around small and medium-sized vessels on the superficial and deep dermis. Immunohistochemical staining confirmed the presence of a reactive CD3+ T cell infiltrate with a mixture of CD4+ and CD8+ lymphocytes and scattered CD20+ B lymphocytes; MCL was absent, as confirmed by CD5, SOX11, and cyclin D1 negativity.
Cutaneous leukocytoclastic vasculitis is clinically characterized by maculopapular skin rash caused by paraneoplastic dermatitis. The condition is characterised by the presence of perivascular inflammatory exudates with extravasation of red blood cells, together with elevated eosinophils consistent with drug eruption. The histopathology of the skin lesion includes evidence of vasculitis and vessel wall destruction, leukocytoclasis with extravasation of erythrocytes, and the presence of lymphocytic and granulocytic infiltration under the epithelium and in the subcutaneous tissue [52,53].
Leukocytoclastic vasculitis is a very rare adverse event of ibrutinib treatment [43,54]. Kaya et al. describe leukocytoclastic vasculitis, manifested as multiple skin lesions, in a patient with CLL 13 days after ibrutinib initiation [55]. Patients with low-grade leukocytoclastic vasculitis-like eruptions may improve with topical corticosteroids and oral antihistaminic drugs. In more advanced symptoms, patients can be treated with oral corticosteroids with either BTKi dose reduction or cessation [42].
5. Neutrophilic Dermatoses
Neutrophilic dermatoses comprise a wide spectrum of diseases characterized by a dense infiltration composed mainly of neutrophils [56]. They are manifested by constellation of clinical features, including fever, neutrophilic leucocytosis, raised painful plaques and skin infiltration by neutrophils and include Sweet syndrome (Figure 4A), neutrophilic panniculitis (Figure 4B) and pyoderma gangrenosum Figure 4 C and D).
5.1. Acute Febrile Neutrophilic Dermatosis
Acute febrile neutrophilic dermatosis (Sweet syndrome) (Figure 4A) is a rare skin condition characterised by a sudden onset of painful, inflamed skin lesions [57,58].
The lesions may be few or numerous and may persist from days to weeks. They commonly affect the face, neck, and upper extremities. Hammel et al. describe a male CLL patient receiving ibrutinib who presented several migratory ecchymotic 2- to 3-cm nodules on the lower extremities [59]. A biopsy of a right leg nodule showed a mixed inflammatory panniculitis with small-vessel vasculitis and concomitant involvement of the septa and fibrinoid necrosis of vascular endothelium with associated neutrophils. The skin lesions completely resolved when ibrutinib was stopped, but new lesions developed within a week of recommencement. El Halabi et al. present a patient with CLL who developed several erythematous, painful, and papulo-nodular skin lesions in the limbs, neck, and face [60]. Neutrophilic dermatosis was confirmed by skin biopsy and Sweet syndrome was diagnosed. Ibrutinib therapy was stopped and the lesions disappeared; however, they returned following rechallenge with ibrutinib at full dose, indicating a direct relationship between dose and symptoms [60]. Another case with atypical neutrophilic dermatosis induced by ibrutinib was recently reported by Renuy et al. [61].
5.2. Neutrophilic Panniculitis
Neutrophilic (lobular) panniculitis (Figure 4B) is a very rare neutrophilic dermatosis characterized by subcutaneous nodular eruption and neutrophilic inflammation in subcutaneous fat. A few cases of neutrophilic panniculitis have been noted as rare cutaneous side effects of ibrutinib therapy [41].
In patients treated with ibrutinib, panniculitis has been described as painful erythematous nodules primarily involving the lower extremities, and occurring within one to 90 days of starting treatment. They are characterised by septal and lobular inflammation. In most patients, ibrutinib discontinuation, or treatment with low-dose prednisone, was found to be effective.
Stewart et al. report a case with painful erythematous nodules on lower extremities which developed one month after initiating ibrutinib therapy for CLL [62]. Histological evaluation revealed lobular panniculitis with fat necrosis and infiltrates consisting predominantly of neutrophils. A diagnosis of neutrophilic panniculitis was rendered, which the patient opted not to treat. The lesions resolved spontaneously despite continued ibrutinib therapy [62].
Fabbro et al. reported five patients who developed panniculitis during ibrutinib therapy for lymphoid leukaemia [41]. The patients presented with painful erythematous nodules at the extremities after initiation of ibrutinib therapy. Histopathological evaluation confirmed lymphohistiocytic, lobular panniculitis with prominent leukocytoclasis. Complete resolution of cutaneous lesions was observed when low-dose systemic corticosteroids were introduced, and nonsteroidal anti-inflammatory drugs in some patients.
5.3. Pyoderma Gangrenosum
Pyoderma gangrenosum (PG) is a rare, inflammatory, ulcerative dermatosis affecting mostly people between 20 and 50 years of age [64]. It may be caused by some drugs, including small molecules like tyrosine kinase inhibitors (TKIs) or BTK inhibitors [65,66]. It most commonly manifests as pustules or nodules, developing into a painful ulcer with undermined violaceous borders and a fibropurulent base (Figure 4C,D) [67,68]. The lesions may be single or multiple, and the most prevalent locations are the lower limbs, followed by the trunk; it can also manifest as arthritis or a hematologic disorder.
Sławińska et al. describe the case of a patient with CLL who developed PG six months after initiation of ibrutinib therapy (3×140 mg/d) [65]. Ibrutinib was discontinued, and the patient treated with prednisone and cyclosporin A. The patient recovered with healing being almost complete after six weeks. Similarly, Giovanni et al. report the case of another patient with CLL who developed PG after five months of ibrutinib treatment [67]. Subsequent steroid treatment resulted in visible improvement; while remission could only be maintained with continued low-dose prednisone, the lesions disappeared completely when ibrutinib was switched to venetoclax. Finally, Pinato et al. report 15 cases of PG, including eight cases associated with sunitinib, two with imatinib, two with ibrutinib, one with gefitinib, one with pazopanib, and one with dabrafenib and trametinib. [69].
6. Skin Infections
Treatment with BTK inhibitors weakens the immune system; as such, patients are at an increased risk of various infectious complications, including skin infections [70,71]. Skin infections by bacteria, fungi, viruses or parasites can cause cutaneous symptoms such as rashes, swelling, itching and pain (Figure 5) [72]. The most common bacterial infections are associated with Staphylococcus aureus, typically as moderate folliculitis [12,17,73]. A systematic review of 48 prospective trials of hematologic malignancies by Tillman et al. classified the occurrence of infectious AEs [74]. Infections of any grade were noted in 56% of patients treated with single-agent ibrutinib and 52% of those receiving combination therapy. Grade 3-4 infectious AEs occurred in 26% (single-agent ibrutinib) and 20% (combination). In both groups, the rate of grade 5 infectious AEs was 2% [74].
In another study of 378 patients treated with ibrutinib over a 5-year period, serious infections were observed in 11%, with most arising during the first year of ibrutinib therapy [75]. Importantly, an increased risk of opportunistic infections was noted, especially by fungal infections, most commonly Aspergillus spp. [76,77]. Singh et al. describe a patient with CLL who developed skin toxicity in the perianal area during ibrutinib treatment, leading to a superimposed bacterial infection and perianal cellulitis. As a result, ibrutinib was discontinued and antibiotic treatment initiated [70].
Opportunistic skin infections, mainly due to non-tuberculous mycobacteria or mucormycosis, have also been associated with inibrutinib treatment [78,79]. An increased risk of herpes virus infection was also reported in patients treated with ibrutinib and acalabrutinib [80,81,82,83]. Prophylactic use of valaciclovir or Herpes zoster vaccination should be considered in patients with common Herpes infection before treatment with BTK inhibitors.
7. Mucosal Symptoms
Mucosal symptoms have been described in around 10% of patients treated with ibrutinib, but only 1-3% were grade 3 or higher [12]. In a pivotal study performed in treatment-naïve CLL patients, all-grade mucositis was reported in 11% of patients and high-grade stomatitis in 1%; however, the clinical aspects were not described [84]. Clinically, mucosal changes manifest as painful oral necrotic ulcers mimicking aphthous stomatitis. Ibrutinib can also induce severe impairing stomatitis (Figure 6).
Vigarios et al. describe three patients treated with ibrutinib who developed a grade ≥3 stomatitis [85]. Two patients reported painful necrotic aphthous-like ulcers that developed within four weeks or even 16 months from the beginning of treatment. In three patients, the resulting skin changes required treatment interruption. in all three patients, the mucosal lesions resolved within a week of treatment discontinuation combined with supportive care including basic oral or steroid care. Reintroduction of treatment at a lower dose did not result in any recurrence of the lesions [86]. In general, for patients with BTKi, oral care prevention of infection and pain control, improve quality of life, and manage concomitant oral complications [87].
8. Nail Lesions and Hair Abnormalities
Hair and nail abnormalities are commonly associated with ibrutinib treatment, and usually appear several months after treatment initiation (Figure 7) [88,89].
8.1. Nail Changes
Patients treated with ibrutinib often demonstrate nail changes, such as brittleness onycholysis, onychorrhexis, onychoschizia, koilonychia, trachyonychia, paronychia, and subungual splinter haemorrhages (Figure 7A–C). The most common symptoms are mild to moderate nail cracking and detachment, onychoschizia and onychorrhexis; however, these are mainly Grade 1 or 2 severity, and do not require treatment [22.90]. Nail changes are typically located on the fingers, develop gradually and are diagnosed after several months of treatment [88,89,91].
Ibrutinib-induced pyogenic granuloma, a benign vascular tumor also known as lobular capillary hemangioma, has also been observed [91]. It manifests as a solitary and rapidly-growing papule or nodule. In some patients, fragile and brittle nails with trachyonychia, linear splitting, horizontal splitting, and shedding of proximal nails (onychomadesis) have been reported, mainly on the fingers [88,89,91].
Farooqui et al. report nail ridging in 22 of 51 (43%) CLL patients treated with ibrutinib [92]. Another study of 66 patients with CLL treated with ibrutinib found 44 (67%) to develop brittle finger nails after a median of 6.5 months and 15 (23%) brittle toe nails after a median of nine months [88]. The mechanism of drug-induced alterations in nail texture is multifactorial and may be related to its influence on cysteines, which are critical for nail hardness: ibrutinib may increase nail brittleness by disrupting the disulphide bonds between cysteine residues. Ibrutinib-related nail plate abnormality is not a drug-limiting toxicity in most patients [89].
A study of 66 patients undergoing long-term treatment with ibrutinib found 67% to have experienced finger nail brittleness and 22.7% toe nail brittleness. These changes manifested over the course of six to nine months of treatment [88].
In most patients, nail changes do not represent a dose-limiting toxicity and no treatment is needed. Nevertheless, patients with nail changes should keep their nails short and polish then once a week. Daily biotin can be also useful [89].
8.2. Hair Changes
Around 20%-30% of patients treated with ibrutinib demonstrate hair changes [88,92] such as straightening and softening, increased curliness and alopecia, with the hair follicle changing from curly to straight (Figure 7D) [88]. Ibrutinib may have a similar influence on the disulphide bonds in hair as those in nails: a scanning electron microscopy study confirmed changes in the hair shaft, similar to those following EGF inhibitors [93]. In some patients, hair changes can be minimized by minoxidil treatment [86].
9. Conclusions
The cutaneous side effects of BTK inhibitor therapy include bruising, rashes, hair changes and nail plate abnormalities, and less commonly, purpuric painful nodules and pyoderma gangrenosum. They occur mainly in patients treated with ibrutinib but also result from acalabrutinib or zanubrutinib treatment. For most patients, the skin changes are self-limiting, they can be relieved with local symptomatic treatment or be managed with local or systemic steroids. However, BTKi dose reduction, treatment interruption or even complete cessation is recommended.
Author Contributions
Both authors contributed equally to writing, reviewing the manuscript and provided their approval of the final version of the manuscript.
Funding
No funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Medical University of Lodz (No RNN/227/23/KE and No RNN/103/16/KE) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
Not applicable.
Acknowledgments
We thank Edward Lowczowski, a native English speaker from the Medical University of Lodz, Poland, for language assistance.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Robak, T.; Iskierka-Jażdżewska, E.; Puła, A.; Robak, P.; Puła, B. The Development of Novel Therapies for Chronic Lymphocytic Leukaemia in the Era of Targeted Drugs. J. Clin. Med. 2025, 14, 8247. [Google Scholar] [CrossRef] [PubMed]
- Wen, T.; Wang, J.; Shi, Y.; Qian, H.; Liu, P. Inhibitors targeting Bruton’s tyrosine kinase in cancers: drug development advances. Leukemia 2020, 35, 312–332. [Google Scholar] [CrossRef]
- Robak, T.; Witkowska, M.; Smolewski, P. The Role of Bruton’s Kinase Inhibitors in Chronic Lymphocytic Leukemia: Current Status and Future Directions. Cancers 2022, 14, 771. [Google Scholar] [CrossRef]
- Falini, B.; Martino, G.; Lazzi, S. A comparison of the International Consensus and 5th World Health Organization classifications of mature B-cell lymphomas. Leukemia 2022, 37, 18–34. [Google Scholar] [CrossRef]
- Robak, E.; Robak, T. Bruton’s Kinase Inhibitors for the Treatment of Immunological Diseases: Current Status and Perspectives. J. Clin. Med. 2022, 11, 2807. [Google Scholar] [CrossRef] [PubMed]
- Robak, T.; Witkowska, M.; Wolska-Washer, A.; Robak, P. BCL-2 and BTK inhibitors for chronic lymphocytic leukemia: current treatments and overcoming resistance. Expert Rev. Hematol. 2024, 17, 781–796. [Google Scholar] [CrossRef]
- Gomez, E.B.; Ebata, K.; Randeria, H.S.; Rosendahl, M.S.; Cedervall, E.P.; Morales, T.H.; Hanson, L.M.; E Brown, N.; Gong, X.; Stephens, J.R.; et al. Pirtobrutinib preclinical characterization: a highly selective, non-covalent (reversible) BTK inhibitor. Blood 2023, 142, 62–72. [Google Scholar] [CrossRef]
- Puła, A.; Stawiski, K.; Braun, M.; Iskierka-Jażdżewska, E.; Robak, T. Efficacy and safety of B-cell receptor signaling pathway inhibitors in relapsed/refractory chronic lymphocytic leukemia: a systematic review and meta-analysis of randomized clinical trials. Leuk. Lymphoma 2017, 59, 1084–1094. [Google Scholar] [CrossRef] [PubMed]
- O’brien, S.M.; Brown, J.R.; Byrd, J.C.; Furman, R.R.; Ghia, P.; Sharman, J.P.; Wierda, W.G. Monitoring and Managing BTK Inhibitor Treatment-Related Adverse Events in Clinical Practice. Front. Oncol. 2021, 11. [Google Scholar] [CrossRef]
- Iberri, D.J.; Kwong, B.Y.; Stevens, L.A.; Coutre, S.E.; Kim, J.; Sabile, J.M.; Advani, R.H. Ibrutinib-associated rash: a single-centre experience of clinicopathological features and management. Br. J. Haematol. 2016, 180, 164–166. [Google Scholar] [CrossRef]
- Ransohoff, J.D.; Kwong, B.Y. Cutaneous Adverse Events of Targeted Therapies for Hematolymphoid Malignancies. Clin. Lymphoma Myeloma Leuk. 2017, 17, 834–851. [Google Scholar] [CrossRef]
- Sibaud, V.; Beylot-Barry, M.; Protin, C.; Vigarios, E.; Recher, C.; Ysebaert, L. Dermatological Toxicities of Bruton’s Tyrosine Kinase Inhibitors. Am. J. Clin. Dermatol. 2020, 21, 799–812. [Google Scholar] [CrossRef]
- Sharman, JP; Black-Shinn, JL; Clark, J; Bojena, B. Understanding ibrutinib treatment discontinuation patterns for chronic lymphocytic leukaemia. Blood 2017, 130, 4060. [Google Scholar] [CrossRef]
- Mato, A.R.; Nabhan, C.; Thompson, M.C.; Lamanna, N.; Brander, D.M.; Hill, B.; Howlett, C.; Skarbnik, A.; Cheson, B.D.; Zent, C.; et al. Toxicities and outcomes of 616 ibrutinib-treated patients in the United States: a real-world analysis. Haematologica 2018, 103, 874–879. [Google Scholar] [CrossRef]
- Yazdy, M.S.; Mato, A.R.; Roeker, L.E.; Jarral, U.; Ujjani, C.S.; Shadman, M.; Skarbnik, A.; Whitaker, K.J.; Deonarine, I.; Kabel, C.C.; et al. Toxicities and Outcomes of Acalabrutinib-Treated Patients with Chronic Lymphocytic Leukemia: A Retrospective Analysis of Real World Patients. Blood 2019, 134, 4311–4311. [Google Scholar] [CrossRef]
- Heymann, W.R. Cutaneous adverse reactions to Bruton tyrosine kinase inhibitors: Banal to brutal. J. Am. Acad. Dermatol. 2023, 88, 1263–1264. [Google Scholar] [CrossRef]
- Singer, S.; Tan, S.Y.; Dewan, A.K.; Davids, M.; LaCasce, A.S.; Treon, S.P.; LeBoeuf, N.R. Cutaneous eruptions from ibrutinib resembling epidermal growth factor receptor inhibitor–induced dermatologic adverse events. J. Am. Acad. Dermatol. 2023, 88, 1271–1281. [Google Scholar] [CrossRef] [PubMed]
- Tam, C.S.; Dimopoulos, M.A.; Garcia-Sanz, R.; Trotman, J.; Opat, S.; Roberts, A.W.; Owen, R.G.; Song, Y.; Xu, W.; Zhu, J.; et al. Pooled safety analysis of zanubrutinib monotherapy in patients with B-cell malignancies. Blood Adv. 2022, 6, 1296–1308. [Google Scholar] [CrossRef]
- Wang, L.; Tang, J.; Feng, J.; Huang, Y.; Cheng, Y.; Xu, H.; Miao, Y. Case report: Zanubrutinib-induced dermatological toxicities: A single-center experience and review. Front. Oncol. 2022, 12. [Google Scholar] [CrossRef]
- Estupiñán, H.Y.; Berglöf, A.; Zain, R.; Smith, C.I.E. Comparative Analysis of BTK Inhibitors and Mechanisms Underlying Adverse Effects. Front. Cell Dev. Biol. 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Lacouture, M.E. Mechanisms of cutaneous toxicities to EGFR inhibitors. Nat. Rev. Cancer 2006, 6, 803–812. [Google Scholar] [CrossRef]
- Nocco, S.; Andriano, T.M.; Bose, A.; Chilov, M.; Godwin, K.; Dranitsaris, G.; Wu, S.; Lacouture, M.E.; Roeker, L.E.; Mato, A.R.; et al. Ibrutinib-associated dermatologic toxicities: A systematic review and meta-analysis. Crit. Rev. Oncol. 2022, 174, 103696. [Google Scholar] [CrossRef]
- Brown, J.R.; Moslehi, J.; Ewer, M.S.; O’BRien, S.M.; Ghia, P.; Cymbalista, F.; Shanafelt, T.D.; Fraser, G.; Rule, S.; Coutre, S.E.; et al. Incidence of and risk factors for major haemorrhage in patients treated with ibrutinib: An integrated analysis. Br. J. Haematol. 2018, 184, 558–569. [Google Scholar] [CrossRef]
- Coutre, S.E.; Byrd, J.C.; Hillmen, P.; Barrientos, J.C.; Barr, P.M.; Devereux, S.; Robak, T.; Kipps, T.J.; Schuh, A.; Moreno, C.; et al. Long-term safety of single-agent ibrutinib in patients with chronic lymphocytic leukemia in 3 pivotal studies. Blood Adv. 2019, 3, 1799–1807. [Google Scholar] [CrossRef]
- Li, X.; Shang, N.; Yan, Q.; Yue, X.; Liu, Y.; Zheng, X. Investigating bleeding adverse events associated with BTK inhibitors in the food and drug administration adverse event reporting system (FAERS). Expert Opin. Drug Saf. 2024, 24, 183–192. [Google Scholar] [CrossRef]
- Shatzel, JJ; Olson, SR; Tao, DL; McCarty, OJT; Danilov, AV; DeLoughery, TG. Ibrutinib-associated bleeding: pathogenesis, management and risk reduction strategies. J Thromb Haemost. 2017, 15(5), 835–847. [Google Scholar] [CrossRef] [PubMed]
- Levade, M.; David, E.; Garcia, C.; Laurent, P.-A.; Cadot, S.; Michallet, A.-S.; Bordet, J.-C.; Tam, C.; Sié, P.; Ysebaert, L.; et al. Ibrutinib treatment affects collagen and von Willebrand factor-dependent platelet functions. Blood 2014, 124, 3991–3995. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, A.H.; Farooqui, M.Z.; Tian, X.; Martyr, S.; Cullinane, A.M.; Nghiem, K.; Sun, C.; Valdez, J.; Niemann, C.U.; Herman, S.E.M.; et al. Incidence and risk factors of bleeding-related adverse events in patients with chronic lymphocytic leukemia treated with ibrutinib. Haematologica 2015, 100, 1571–1578. [Google Scholar] [CrossRef] [PubMed]
- Mock, J.; Kunk, P.R.; Palkimas, S.; Sen, J.M.; Devitt, M.; Horton, B.; Portell, C.A.; Williams, M.E.; Maitland, H. Risk of Major Bleeding with Ibrutinib. Clin. Lymphoma Myeloma Leuk. 2018, 18, 755–761. [Google Scholar] [CrossRef]
- Jani, C.; Pandit, Z.; Singh, H.; Al Omari, O.; Caughey, T.; Shapiro, D.S.; Lam, P. Imbruvica (Ibrutinib) induced subcutaneous hematoma: A case report. Curr. Probl. Cancer: Case Rep. 2021, 3. [Google Scholar] [CrossRef]
- Allouchery, M.; Tomowiak, C.; Singier, A.; Puyade, M.; Dari, L.; Pambrun, E.; Pariente, A.; Bezin, J.; Pérault-Pochat, M.; Salvo, F. Bleeding risk with concurrent use of anticoagulants and ibrutinib: A population-based nested case-control study. Br. J. Haematol. 2023. [Google Scholar] [CrossRef] [PubMed]
- von Hundelshausen, P.; Siess, W. Bleeding by Bruton Tyrosine Kinase-Inhibitors: Dependency on Drug Type and Disease. Cancers 2021, 13, 1103. [Google Scholar] [CrossRef]
- Furman, R.R.; Byrd, J.C.; Owen, R.G.; O’bRien, S.M.; Brown, J.R.; Hillmen, P.; Stephens, D.M.; Chernyukhin, N.; Lezhava, T.; Hamdy, A.M.; et al. Pooled analysis of safety data from clinical trials evaluating acalabrutinib monotherapy in mature B-cell malignancies. Leukemia 2021, 35, 3201–3211. [Google Scholar] [CrossRef]
- Lamanna, N.; Tam, C.S.; Woyach, J.A.; Alencar, A.J.; Palomba, M.L.; Zinzani, P.L.; Flinn, I.W.; Fakhri, B.; Cohen, J.B.; Kontos, A.; et al. Evaluation of bleeding risk in patients who received pirtobrutinib in the presence or absence of antithrombotic therapy. eJHaem 2024, 5, 929–939. [Google Scholar] [CrossRef]
- Belkaïd, S.; Amini-Adle, M. Zanubrutinib-associated ecchymotic lesions. Lancet Haematol. 2024, 11, e708–e708. [Google Scholar] [CrossRef]
- Samperio, V.M.; Ghonge, A.; Dasanu, C.A.; Dasanu, C. Zanubrutinib-Induced Symmetrical Soft Tissue Forearm Swelling in a Patient With Waldenström Macroglobulinemia. Cureus 2025, 17. [Google Scholar] [CrossRef] [PubMed]
- Vilasi, S.M.; Luu, L.A.; Noland, M.M. Zanubrutinib-induced petechial ecchymotic reaction in a previously irradiated area in a patient with chronic lymphocytic leukemia. JAAD Case Rep. 2024, 46, 70–72. [Google Scholar] [CrossRef]
- Kucharik, A.H.; Curkovic, N.B.; Chavez, J.C.; Tsai, K.Y.; Brohl, A.S.; Grichnik, J.M. Pseudoangiosarcoma and cutaneous collagenous vasculopathy in a patient on a Bruton’s tyrosine kinase inhibitor. JAAD Case Rep. 2024, 51, 17–21. [Google Scholar] [CrossRef]
- Guenther, J.; Vecerek, N.; Worswick, S. Extensive ecchymotic patch in a patient with chronic lymphocytic leukemia. Int. J. Dermatol. 2023, 63, 313–315. [Google Scholar] [CrossRef] [PubMed]
- Truong, K.; Bhattacharyya, A.; Kim, J.; Wells, J. A uniquely distributed purpuric drug eruption from acalabrutinib. Australas. J. Dermatol. 2022, 63, E142–E144. [Google Scholar] [CrossRef]
- Fabbro, S.K.; Smith, S.M.; Dubovsky, J.A.; Gru, A.A.; Jones, J.A. Panniculitis in Patients Undergoing Treatment With the Bruton Tyrosine Kinase Inhibitor Ibrutinib for Lymphoid Leukemias. JAMA Oncol. 2015, 1, 684–686. [Google Scholar] [CrossRef]
- Iberri, D.J.; Kwong, B.Y.; Stevens, L.A.; Coutre, S.E.; Kim, J.; Sabile, J.M.; Advani, R.H. Ibrutinib-associated rash: a single-centre experience of clinicopathological features and management. Br. J. Haematol. 2016, 180, 164–166. [Google Scholar] [CrossRef]
- Kirar, S.; Gogia, A.; Gupta, R.; Mallick, S. Ibrutinib-Induced Skin Rash. Turk. J. Hematol. 2021, 38, 81–83. [Google Scholar] [CrossRef]
- Jensen, A.B.; Stausbøl-Grøn, B.; Riber-Hansen, R.; D’aMore, F. Ibrutinib-associated skin toxicity: a case of maculopapular rash in a 79-year old Caucasian male patient with relapsed Waldenstrom’s macroglobulinemia and review of the literature. Dermatol. Rep. 2017, 9, 6976. [Google Scholar] [CrossRef] [PubMed]
- Awan, F.T.; Schuh, A.; Brown, J.R.; Furman, R.R.; Pagel, J.M.; Hillmen, P.; Stephens, D.M.; Woyach, J.; Bibikova, E.; Charuworn, P.; et al. Acalabrutinib monotherapy in patients with chronic lymphocytic leukemia who are intolerant to ibrutinib. Blood Adv. 2019, 3, 1553–1562. [Google Scholar] [CrossRef]
- Paydas, S. Management of adverse effects/toxicity of ibrutinib. Crit. Rev. Oncol. 2019, 136, 56–63. [Google Scholar] [CrossRef]
- Zhou, J.; Ma, W.; Hu, N.; Ma, Y.; Zhu, H.; Gao, L. Severe atypical skin disease in two patients with CLL/SLL after BTKi treatment—a case report and literature review. Front. Oncol. 2024, 14, 1467891. [Google Scholar] [CrossRef]
- Portillo, T.M.P.; Dhaliwal, D.; Krishnan, B. Acalabrutinib-Related Dermal Toxicities: A Next-Generation Diagnostic Challenge. Am. J. Clin. Pathol. 2023, 160, S26–S26. [Google Scholar] [CrossRef]
- Lasica, M.; Tam, C.S. Management of Ibrutinib Toxicities: a Practical Guide. Curr. Hematol. Malign- Rep. 2020, 15, 177–186. [Google Scholar] [CrossRef]
- Bitar, C.; Sadeghian, A.; Sullivan, L.; Murina, A. Ibrutinib-associated pityriasis rosea–like rash. JAAD Case Rep. 2018, 4, 55–57. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Baeza, D.; Pérez-López, E.; Román-Curto, C.; Santos-Briz, A. Cutaneous Lymphocytic Vasculitis Due to Ibrutinib Therapy. Actas Dermo-Sifiliograficas 2024, 115, 1073–1074. [Google Scholar] [CrossRef]
- Moyers, J.T.; Liu, L.W.; Ossowski, S.; Goddard, L.; Kamal, M.O.; Cao, H. A rash in a hairy situation: Leukocytoclastic vasculitis at presentation of hairy cell Leukemia. Am. J. Hematol. 2019, 94, 1433–1434. [Google Scholar] [CrossRef]
- Robak, E.; Jesionek-Kupnicka, D.; Iskierka-Jazdzewska, E.; Janus, A.; Robak, T. Cutaneous leukocytoclastic vasculitis at diagnosis of hairy cell leukemia successfully treated with vemurafenib and rituximab. Leuk. Res. 2021, 104, 106571. [Google Scholar] [CrossRef]
- Mannis, G.; Wu, D.; Dea, T.; Mauro, T.; Hsu, G. Ibrutinib rash in a patient with 17p del chronic lymphocytic leukemia. Am. J. Hematol. 2014, 90, 179–179. [Google Scholar] [CrossRef]
- Kaya, A.; Aras, I.; Kurtgöz, P.Ö.; Çakıroğlu, U. Ibrutinib-Associated Leukocytoclastic Vasculitis in a Patient with Chronic Lymphocytic Leukemia. Turk. J. Hematol. 2024, 41, 57–58. [Google Scholar] [CrossRef]
- Álvarez-Salafranca, M.; García-García, M.; Yangüela, B.d.E. Neutrophilic dermatosis of the dorsal hands related to cocaine abuse. An. Bras. de Dermatol. 2021, 96, 574–577. [Google Scholar] [CrossRef]
- Cohen, P.R. Sweet’s syndrome—a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J. Rare Dis. 2007, 2, 34–34. [Google Scholar] [CrossRef]
- Khan, U.; Rizvi, H.; Ali, F.; Lebovic, D. Sweet syndrome: a painful reality. BMJ Case Rep. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Hammel, J.A.; Roth, G.M.; Ferguson, N.; Fairley, J.A. Lower extremity ecchymotic nodules in a patient being treated with ibrutinib for chronic lymphocytic leukemia. JAAD Case Rep. 2017, 3, 178–179. [Google Scholar] [CrossRef] [PubMed]
- El Halabi, L.; Cherif-Rebai, K.; Michot, J.-M.; Ghez, D. Ibrutinib-Induced Neutrophilic Dermatosis. Am. J. Dermatopathol. 2018, 40, 198–200. [Google Scholar] [CrossRef] [PubMed]
- Renuy, J.; Fizazi, A.; Girard, C.; Dereure, O. Atypical Neutrophilic Dermatosis Induced by Ibrutinib: A Dose-Dependent Cutaneous Adverse Reaction. Int. J. Dermatol. 2025, 65, 160–162. [Google Scholar] [CrossRef]
- Stewart, J.; Bayers, S.; Vandergriff, T. Self-limiting Ibrutinib-Induced Neutrophilic Panniculitis. Am. J. Dermatopathol. 2018, 40, e28–e29. [Google Scholar] [CrossRef]
- Mulvey, J.J.; Nuovo, G.J.; Magro, C.M. Cutaneous, Purpuric Painful Nodules Upon Addition of Ibrutinib to RCVP Therapy in a CLL Patient: A Distinctive Reaction Pattern Reflecting Iatrogenic Th2 to Th1 Milieu Reversal. Am. J. Dermatopathol. 2016, 38, 492–498. [Google Scholar] [CrossRef]
- Bhat, R. Pyoderma gangrenosum: An update. Indian Dermatol. Online J. 2012, 3, 7–13. [Google Scholar] [CrossRef]
- Sławińska, M.; Barańska-Rybak, W.; Sobjanek, M.; Wilkowska, A.; Mital, A.; Nowicki, R. Ibrutinib-induced pyoderma gangrenosum. Pol. Arch. Intern. Med. 2016, 126, 710–711. [Google Scholar] [CrossRef]
- Kridin, K.; Cohen, A.D.; Amber, K.T. Underlying Systemic Diseases in Pyoderma Gangrenosum: A Systematic Review and Meta-Analysis. Am. J. Clin. Dermatol. 2018, 19, 479–487. [Google Scholar] [CrossRef]
- Giovanni, B.; Ibatici, A.; Sola, S.; Brunasso, A.M.G.; Massone, C. Ibrutinib and Pyoderma Gangrenosum in a Patient With B-Cell Chronic Lymphocytic Leukemia. Am. J. Dermatopathol. 2020, 42, 148–150. [Google Scholar] [CrossRef]
- Khoshnam-Rad, N.; Gheymati, A.; Jahangard-Rafsanjani, Z. Tyrosine kinase inhibitors-associated pyoderma gangrenosum, a systematic review of published case reports. Anti-Cancer Drugs 2021, 33, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.; Sharma, R. Imatinib induced pyoderma gangrenosum. J. Postgrad. Med. 2013, 59, 244–245. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.; Gupta, P.; Vargas, J.; Kudelka, A.; Kobe, M.; Rocca, N. Ibrutinib-Induced Perianal Rash Complicated by Bacterial Infection in a Patient With Chronic Lymphocytic Leukemia: A Case Report and Literature Review. Cureus 2025, 17, e82952. [Google Scholar] [CrossRef] [PubMed]
- Estupiñán, H.Y.; Berglöf, A.; Zain, R.; Smith, C.I.E. Comparative Analysis of BTK Inhibitors and Mechanisms Underlying Adverse Effects. Front. Cell Dev. Biol. 2021, 9. [Google Scholar] [CrossRef]
- Anderson, B.J.; Wilz, L.; Peterson, A. The Identification and Treatment of Common Skin Infections. J. Athl. Train. 2023, 58, 502–510. [Google Scholar] [CrossRef]
- Ghasoub, R.; Albattah, A.; Elazzazy, S.; Alokka, R.; Nemir, A.; Alhijji, I.; Taha, R. Ibrutinib-associated sever skin toxicity: A case of multiple inflamed skin lesions and cellulitis in a 68-year-old male patient with relapsed chronic lymphocytic leukemia—Case report and literature review. J. Oncol. Pharm. Pr. 2019, 26, 487–491. [Google Scholar] [CrossRef]
- Tillman, B.F.; Pauff, J.M.; Satyanarayana, G.; Talbott, M.; Warner, J.L. Systematic review of infectious events with the Bruton tyrosine kinase inhibitor ibrutinib in the treatment of hematologic malignancies. Eur. J. Haematol. 2018, 100, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Varughese, T.; Taur, Y.; Cohen, N.; Palomba, M.L.; Seo, S.K.; Hohl, T.M.; Redelman-Sidi, G. Serious Infections in Patients Receiving Ibrutinib for Treatment of Lymphoid Cancer. Clin. Infect. Dis. 2018, 67, 687–692. [Google Scholar] [CrossRef]
- Rogers, K.A.; Mousa, L.; Zhao, Q.; Bhat, S.A.; Byrd, J.C.; El Boghdadly, Z.; Guerrero, T.; Levine, L.B.; Lucas, F.; Shindiapina, P.; et al. Incidence of opportunistic infections during ibrutinib treatment for B-cell malignancies. Leukemia 2019, 33, 2527–2530. [Google Scholar] [CrossRef] [PubMed]
- Ghez, D.; Calleja, A.; Protin, C.; Baron, M.; Ledoux, M.-P.; Damaj, G.; Dupont, M.; Dreyfus, B.; Ferrant, E.; Herbaux, C.; et al. Early-onset invasive aspergillosis and other fungal infections in patients treated with ibrutinib. Blood 2018, 131, 1955–1959. [Google Scholar] [CrossRef] [PubMed]
- Dousa, K.M.; Babiker, A.; Van Aartsen, D.; Shah, N.; A Bonomo, R.; Johnson, J.L.; Skalweit, M.J. Ibrutinib Therapy and Mycobacterium chelonae Skin and Soft Tissue Infection. Open Forum Infect. Dis. 2018, 5, ofy168. [Google Scholar] [CrossRef]
- Stein, M.K.; Karri, S.; Reynolds, J.; Owsley, J.; Wise, A.; Martin, M.G.; Zare, F. Cutaneous Mucormycosis Following a Bullous Pemphigoid Flare in a Chronic Lymphocytic Leukemia Patient on Ibrutinib. World J. Oncol. 2018, 9, 62–65. [Google Scholar] [CrossRef]
- Burger, J.A.; Tedeschi, A.; Barr, P.M.; Robak, T.; Owen, C.; Ghia, P.; Bairey, O.; Hillmen, P.; Bartlett, N.L.; Li, J.; et al. Ibrutinib as Initial Therapy for Patients with Chronic Lymphocytic Leukemia. New Engl. J. Med. 2015, 373, 2425–2437. [Google Scholar] [CrossRef]
- Treon, S.P.; Tripsas, C.K.; Meid, K.; Warren, D.; Varma, G.; Green, R.; Argyropoulos, K.V.; Yang, G.; Cao, Y.; Xu, L.; et al. Ibrutinib in Previously Treated Waldenström’s Macroglobulinemia. New Engl. J. Med. 2015, 372, 1430–1440. [Google Scholar] [CrossRef]
- Byrd, J.C.; Harrington, B.; O’brien, S.; Jones, J.A.; Schuh, A.; Devereux, S.; Chaves, J.; Wierda, W.G.; Awan, F.T.; Brown, J.R.; et al. Acalabrutinib (ACP-196) in Relapsed Chronic Lymphocytic Leukemia. New Engl. J. Med. 2016, 374, 323–332. [Google Scholar] [CrossRef]
- Ghasoub, R.; Albattah, A.; Elazzazy, S.; Alokka, R.; Nemir, A.; Alhijji, I.; Taha, R. Ibrutinib-associated sever skin toxicity: A case of multiple inflamed skin lesions and cellulitis in a 68-year-old male patient with relapsed chronic lymphocytic leukemia—Case report and literature review. J. Oncol. Pharm. Pr. 2019, 26, 487–491. [Google Scholar] [CrossRef]
- Byrd, J.C.; Brown, J.R.; O’Brien, S.; Barrientos, J.C.; Kay, N.E.; Reddy, N.M.; Coutre, S.; Tam, C.S.; Mulligan, S.P.; Jaeger, U.; et al. Ibrutinib versus Ofatumumab in Previously Treated Chronic Lymphoid Leukemia. N. Engl. J. Med. 2014, 371, 213–223. [Google Scholar] [CrossRef]
- Vigarios, E.; Beylot-Barry, M.; Jegou, M.; Oberic, L.; Ysebaert, L.; Sibaud, V. Dose-limiting stomatitis associated with ibrutinib therapy: a case series. Br. J. Haematol. 2018, 185, 784–788. [Google Scholar] [CrossRef]
- Vigarios, E.; Beylot-Barry, M.; Jegou, M.; Oberic, L.; Ysebaert, L.; Sibaud, V. Dose-limiting stomatitis associated with ibrutinib therapy: a case series. Br. J. Haematol. 2018, 185, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Elad, S.; Yarom, N.; Zadik, Y.; Kuten-Shorrer, M.; Sonis, S.T. The broadening scope of oral mucositis and oral ulcerative mucosal toxicities of anticancer therapies. CA: A Cancer J. Clin. 2021, 72, 57–77. [Google Scholar] [CrossRef]
- Bitar, C.; Farooqui, M.Z.H.; Valdez, J.; Saba, N.S.; Soto, S.; Bray, A.; Marti, G.; Wiestner, A.; Cowen, E.W. Hair and Nail Changes During Long-term Therapy With Ibrutinib for Chronic Lymphocytic Leukemia. JAMA Dermatol. 2016, 152, 698–701. [Google Scholar] [CrossRef] [PubMed]
- Manica, L.A.H.; Cohen, P.R. Ibrutinib-Associated Nail Plate Abnormalities: Case Reports and Review. Drug Saf.—Case Rep. 2017, 4, 15–15. [Google Scholar] [CrossRef] [PubMed]
- van de Kerkhof, P.C.; Pasch, M.C.; Scher, R.K.; Kerscher, M.; Gieler, U.; Haneke, E.; Fleckman, P. Brittle nail syndrome: A pathogenesis-based approach with a proposed grading system. J. Am. Acad. Dermatol. 2005, 53, 644–651. [Google Scholar] [CrossRef]
- Alamri, A.; Alghamdi, Y.; Alghamdi, A.; Albogami, D.B.; Shahada, O.; AlHarbi, A. Ibrutinib-Induced Paronychia and Periungual Pyogenic Granuloma. Cureus 2022, 14, e32943. [Google Scholar] [CrossRef] [PubMed]
- Farooqui, M.Z.H.; Valdez, J.; Martyr, S.; Aue, G.; Saba, N.; Niemann, C.U.; Herman, S.E.M.; Tian, X.; Marti, G.; Soto, S.; et al. Ibrutinib for previously untreated and relapsed or refractory chronic lymphocytic leukaemia with TP53 aberrations: a phase 2, single-arm trial. Lancet Oncol. 2015, 16, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Jr., H.L.d.A.; Sartori, D.S.; Malkoun, D.; Cunha, C.E.P. Scanning electron microscopy of ibrutinib-induced hair shaft changes. An. Bras. de Dermatol. 2023, 98, 520–523. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Hemorrhagic skin complications of BTK inhibitors. (A) Bruising in the neck of CLL patient treated with ibrutinib. (B) Bruisings in the the back of the hands of CLL patient treated with acalabrutinib.(C) Skin hemorages on the trunk and arm of MCL patient treated with ibrutinib. (D) Hematoma of the left eye in a patient on ibrutinib.
Figure 1.
Hemorrhagic skin complications of BTK inhibitors. (A) Bruising in the neck of CLL patient treated with ibrutinib. (B) Bruisings in the the back of the hands of CLL patient treated with acalabrutinib.(C) Skin hemorages on the trunk and arm of MCL patient treated with ibrutinib. (D) Hematoma of the left eye in a patient on ibrutinib.

Figure 2.
Petechiae in a patient with MCL emerged two weeks post-initiation of ibrutinib treatment (A, B) and either vanished or considerably diminished two weeks after ceasing ibrutinib (C, D).
Figure 2.
Petechiae in a patient with MCL emerged two weeks post-initiation of ibrutinib treatment (A, B) and either vanished or considerably diminished two weeks after ceasing ibrutinib (C, D).
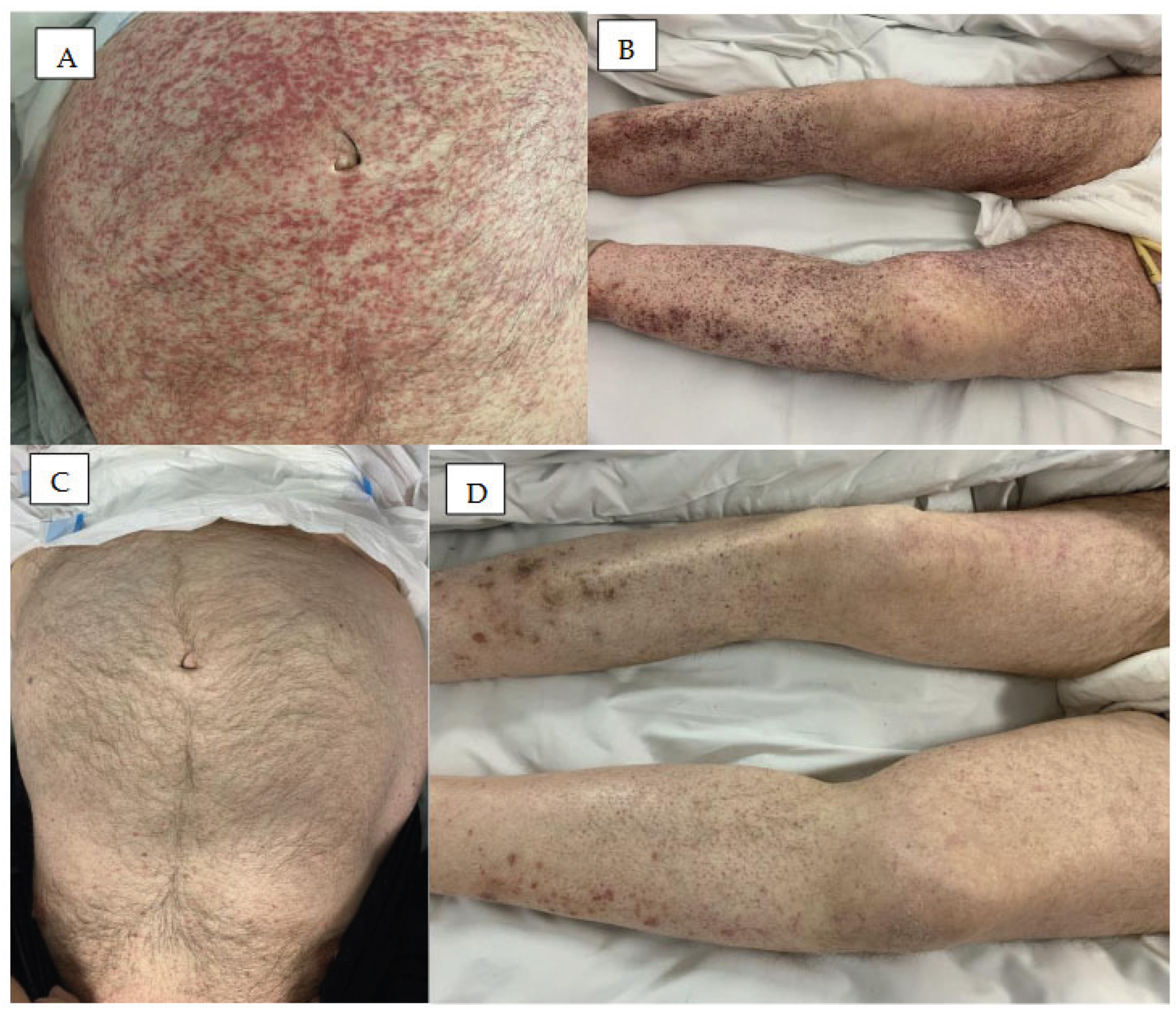
Figure 3.
Rash in patients treated with BTK inhibitors. (A) Erythema multiforme on the skin of the lower limbs in a patient treated with ibrutinib for five weeks.(B) Erythema with vascular reaction on the feets and lower legs after three months of treatment with zanubrutinib. (C) Acuteallergic-toxic erythema with a hemorrhagic component on the lower limbs after three weeks of treatment with ibrutinib. (D) Acute allergic erythema on the skin of the face and trunk in a patient treated for two weeks with ibrutinib.
Figure 3.
Rash in patients treated with BTK inhibitors. (A) Erythema multiforme on the skin of the lower limbs in a patient treated with ibrutinib for five weeks.(B) Erythema with vascular reaction on the feets and lower legs after three months of treatment with zanubrutinib. (C) Acuteallergic-toxic erythema with a hemorrhagic component on the lower limbs after three weeks of treatment with ibrutinib. (D) Acute allergic erythema on the skin of the face and trunk in a patient treated for two weeks with ibrutinib.

Figure 4.
Neutrhilic dermatoses in patients treated with BTK inhibitors. (A) Sweets syndrome diagnozed two months after ibrutinib treatment initiation in a patient with CLL. Painful papules, nodules and plaques acompanied by fiver on the skin of the back.(B)Panniculitis neutrofilica. Tender red nodules on the breast skin in a patient with CLL treated for two monhs with acalabrutinib. (C,D) Pyoderma gangenosum. Rapidly s[preading ulcers withraised edgeon the skin of the right hand and lower leg in a patient with CLL treated with ibrutinib (C) and in the patients with MCL treated with acalabrutinib (D).
Figure 4.
Neutrhilic dermatoses in patients treated with BTK inhibitors. (A) Sweets syndrome diagnozed two months after ibrutinib treatment initiation in a patient with CLL. Painful papules, nodules and plaques acompanied by fiver on the skin of the back.(B)Panniculitis neutrofilica. Tender red nodules on the breast skin in a patient with CLL treated for two monhs with acalabrutinib. (C,D) Pyoderma gangenosum. Rapidly s[preading ulcers withraised edgeon the skin of the right hand and lower leg in a patient with CLL treated with ibrutinib (C) and in the patients with MCL treated with acalabrutinib (D).
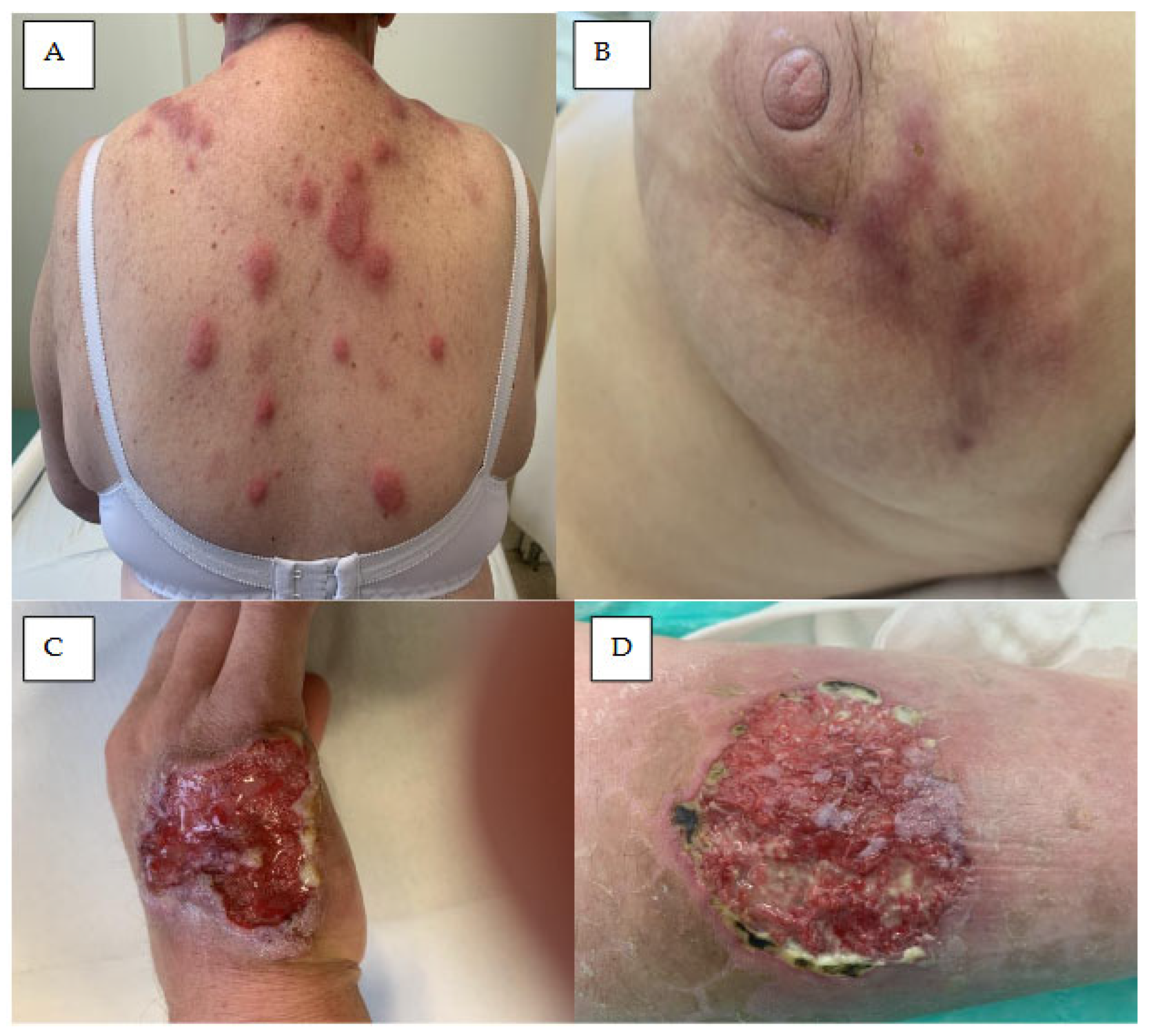
Figure 5.
Skin infections in patients treated with BTK inhibitors. (A) Erysipelas on the wright lower legs in a patient with CLL on the fifth week of treatment with ibrutinib. (B) Disseminated boils on both thighs in a patient with CLL in the second year of zanubrutinib treatment. (C) Fungal infection on the trunk of a patient with MCL six months afterf starting ibrutinib treatment. Peripherally spreading erythematous-scalylesions with the presence of exudative papules on periphery and accompanying itching. (D) Hepes zoster on the neck and left sideburn in a patient with CLL treated for six months with ibrutinib. Erythematous-vesicular lesions with a necrotic component.
Figure 5.
Skin infections in patients treated with BTK inhibitors. (A) Erysipelas on the wright lower legs in a patient with CLL on the fifth week of treatment with ibrutinib. (B) Disseminated boils on both thighs in a patient with CLL in the second year of zanubrutinib treatment. (C) Fungal infection on the trunk of a patient with MCL six months afterf starting ibrutinib treatment. Peripherally spreading erythematous-scalylesions with the presence of exudative papules on periphery and accompanying itching. (D) Hepes zoster on the neck and left sideburn in a patient with CLL treated for six months with ibrutinib. Erythematous-vesicular lesions with a necrotic component.
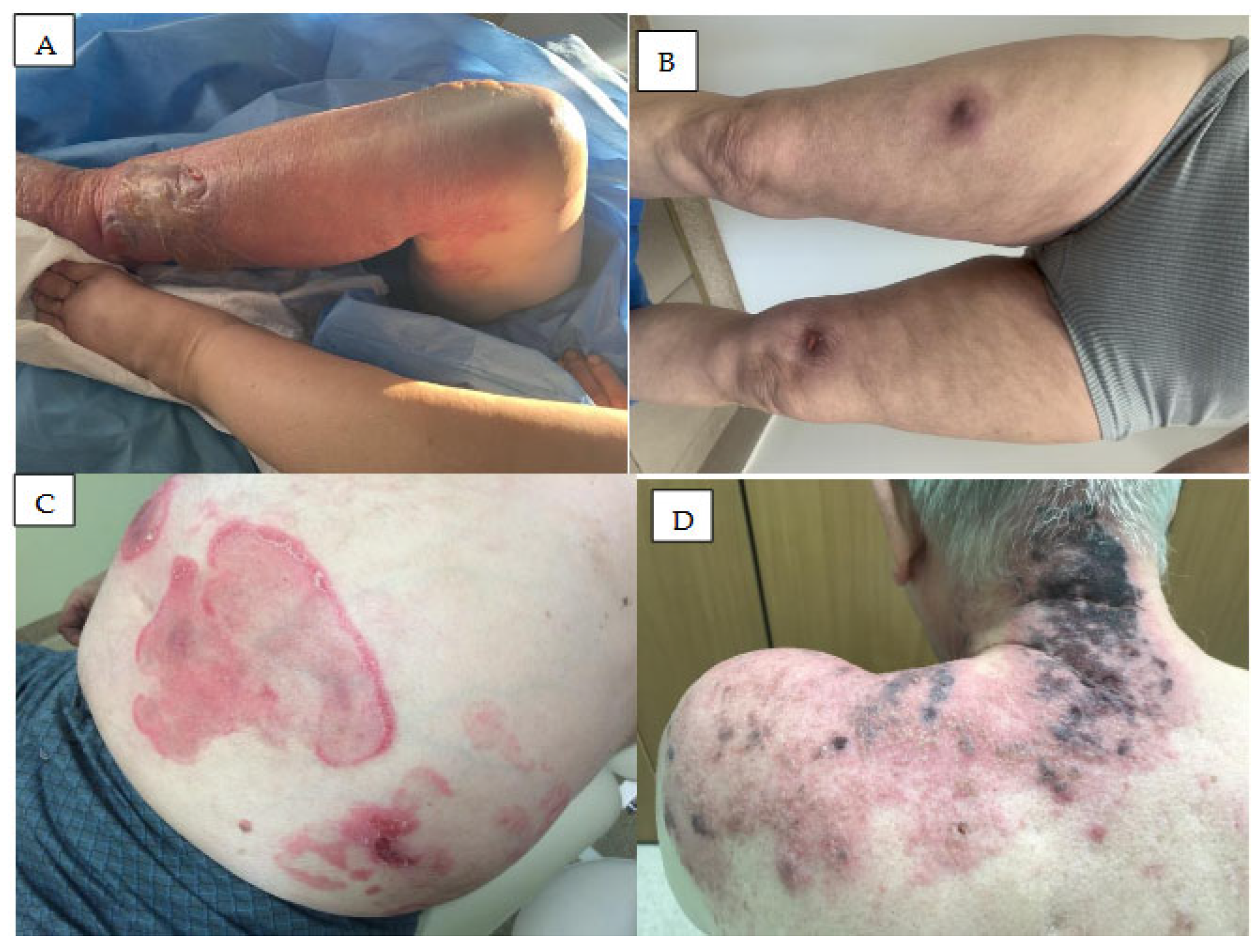
Figure 6.
Mucosal symptoms in a patient with MCL treated for two weeks with acalabrutinib. (A, B) Extensive oral mucositis with paiful, diffused erosions and necrotic ulcers with fibrin present. circumscribed necrotic ulcer with erythematous halo located on lip mucosa partly covered by a yellow fibrin. (C) Multiple hemorrhagic lesions located on mucosa of plate and lower lip. (D) Mucosal lesions located on tongue, mimicking major aphthous stomatitis in the same patient. .
Figure 6.
Mucosal symptoms in a patient with MCL treated for two weeks with acalabrutinib. (A, B) Extensive oral mucositis with paiful, diffused erosions and necrotic ulcers with fibrin present. circumscribed necrotic ulcer with erythematous halo located on lip mucosa partly covered by a yellow fibrin. (C) Multiple hemorrhagic lesions located on mucosa of plate and lower lip. (D) Mucosal lesions located on tongue, mimicking major aphthous stomatitis in the same patient. .

Figure 7.
Nail lesions and hair abnormalities in patients treated with ibrutinib. (A)Hemorrhagic and necrotic ulcers on the skin and nail plates of the right hand of a patient treated for two months with ibrutinib. (B) Excessive drying, delamination and chipping of fingernails in CLL patient six months after treatment with ibrutinib. (C) Onychodystrophy of the nails of the second and third fingers of the right hand in a patient with MCL, treated for six months with ibrutinib. (D) Diffuse hair loss with noticeable thinning on the topof the head in a CLL patient aftermone year treatment with ibrutinib.
Figure 7.
Nail lesions and hair abnormalities in patients treated with ibrutinib. (A)Hemorrhagic and necrotic ulcers on the skin and nail plates of the right hand of a patient treated for two months with ibrutinib. (B) Excessive drying, delamination and chipping of fingernails in CLL patient six months after treatment with ibrutinib. (C) Onychodystrophy of the nails of the second and third fingers of the right hand in a patient with MCL, treated for six months with ibrutinib. (D) Diffuse hair loss with noticeable thinning on the topof the head in a CLL patient aftermone year treatment with ibrutinib.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



