01. Introduction
Over the past two decades, major respiratory viral outbreaks, including severe acute respiratory syndrome in 2002, influenza A(H1N1) in 2009, Middle East respiratory syndrome in 2012, and coronavirus disease 2019, have adversely affected the health and well-being of healthcare workers (HCWs). HCWs, given the inherent characteristics of their profession, are at substantial risk of contracting these viruses and have been prioritized for protection against these fatal diseases (1). Initial reports of SARS-CoV-2 exposure in HCWs indicated clear evidence of infection risks (2) and psychological consequences (3, 4). A systematic review studying the prevalence of COVID-19 among HCWs reported that the adjusted pooled prevalence of real-time reverse-transcriptase polymerase chain reaction (rRT-PCR)-confirmed COVID-19 among HCWs was 11% (95% CI: 7–16%) (5).
The World Health Organization (WHO) estimates that at least 115,500 HCWs worldwide have lost their lives due to COVID-19 (6). In Bangladesh, approximately 9402 HCWs were reported to be infected with the SARS-CoV-2 virus, along with 186 physician deaths among them in 2021 (7, 8). The mortality rate among physicians was 4% in Bangladesh, which was above the global average standard mortality rate of 2.5% (9). However, Bangladesh had the lowest rate of SARS-CoV-2 testing in Asia, while ranking 16th globally in the April 2020 infection rate (10-13). This low number of sample tests was also linked to the asymptomatic positive COVID-19 cases, who would unknowingly transmit the infection to others. According to several systematic reviews, it has been estimated that 21.7 to 64.3 percent of individuals infected with SARS-CoV-2 do not exhibit any symptoms during their infection phase (14-16). The efficient transmission of the virus by asymptomatic patients thus poses a significant challenge in effectively controlling the pandemic (17). To generate evidence on the true proportion of infected individuals with the virus regardless of presenting symptoms, testing methods alternative to RT-PCR, such as antibody testing, have been considered crucial by experts to cover large populations, including Bangladesh (18). Furthermore, it was deemed essential to monitor changes in SARS-CoV-2 seroprevalence and antibody protection conferred by COVID-19 vaccines over time to predict their patterns and to develop an appropriate public health strategy to address future pandemics (19).
The COVID-19 pandemic has had a profound impact on the mental health of frontline HCWs. Multiple studies have documented high rates of persistent psychological distress among HCWs, including anxiety, depression, burnout, post-traumatic stress disorder (PTSD), and insomnia (20-22). The intense pressure of heavy workloads, extended working hours, fear of infection, and exposure to high patient mortality placed immense psychological strain on HCWs (20). These challenges were further exacerbated by inadequate protective equipment, moral distress, and social isolation. In Bangladesh, studies have reported that the prevalence of anxiety among HCWs ranged from 69.5% to 78%, while depression affected approximately 39.5% to 44% of HCWs (23, 24).
Implementing robust Infection Prevention and Control (IPC) measures has been instrumental in reducing COVID-19 infections among HCWs. Strict adherence to IPC protocols, including proper use of personal protective equipment (PPE), hand hygiene, surface disinfection, and patient isolation, was crucial in minimizing transmission. Studies have shown that HCWs who consistently followed IPC guidelines had lower infection rates than those with inadequate protection (25-29). Hospitals with comprehensive IPC training, adequate PPE supply, and strict compliance monitoring reported fewer COVID-19 cases among staff (28). A study conducted in Singapore demonstrated that enhanced IPC strategies, including improved patient segregation, universal masking, and heightened adherence to standard precautions, led to a significant decrease in healthcare-associated respiratory viral infections, with the cumulative incidence dropping from 9.69 to 0.83 cases per 10,000 patient-days (30).
Therefore, we established a unique prospective cohort of HCWs providing patient care in Bangladesh during the early phase of the pandemic, when there was an inadequate understanding of the full extent of COVID-19’s impact on HCWs in an LMIC. Our cohort was the largest and first HCW cohort in Bangladesh, comprising 3697 participants, and was designed to assess their physical and mental health status during the pandemic. The primary aim of establishing this cohort was also to document COVID-19 illness and to identify risk factors that could be mitigated to reduce the likelihood of infection among participants. Other areas of interest included determining primary series vaccine coverage and assessing IPC undertaken by HCWs during this time.
As this cohort was established with many HCWs from all levels and types of existing healthcare facilities across Bangladesh, the substantial volume of data generated facilitated the establishment of an additional study within this cohort. The second phase of the study focused on identifying breakthrough infections, monitoring emerging SARS-CoV-2 strains, assessing the barriers and enablers to booster vaccination, and investigating immune responses during the COVID-19 peri-infection period among HCWs. It was considered essential to examine how infection and vaccination affect an individual’s ability to cope with the psychological demands of work during a later phase of the pandemic, particularly in an LMIC context. In this paper, we present the HCW cohort by describing the study design, data, and specimen-collection procedures across the study phases, the follow-up protocol, and preliminary findings to date.
2. Materials and Methods
2.1. Study site
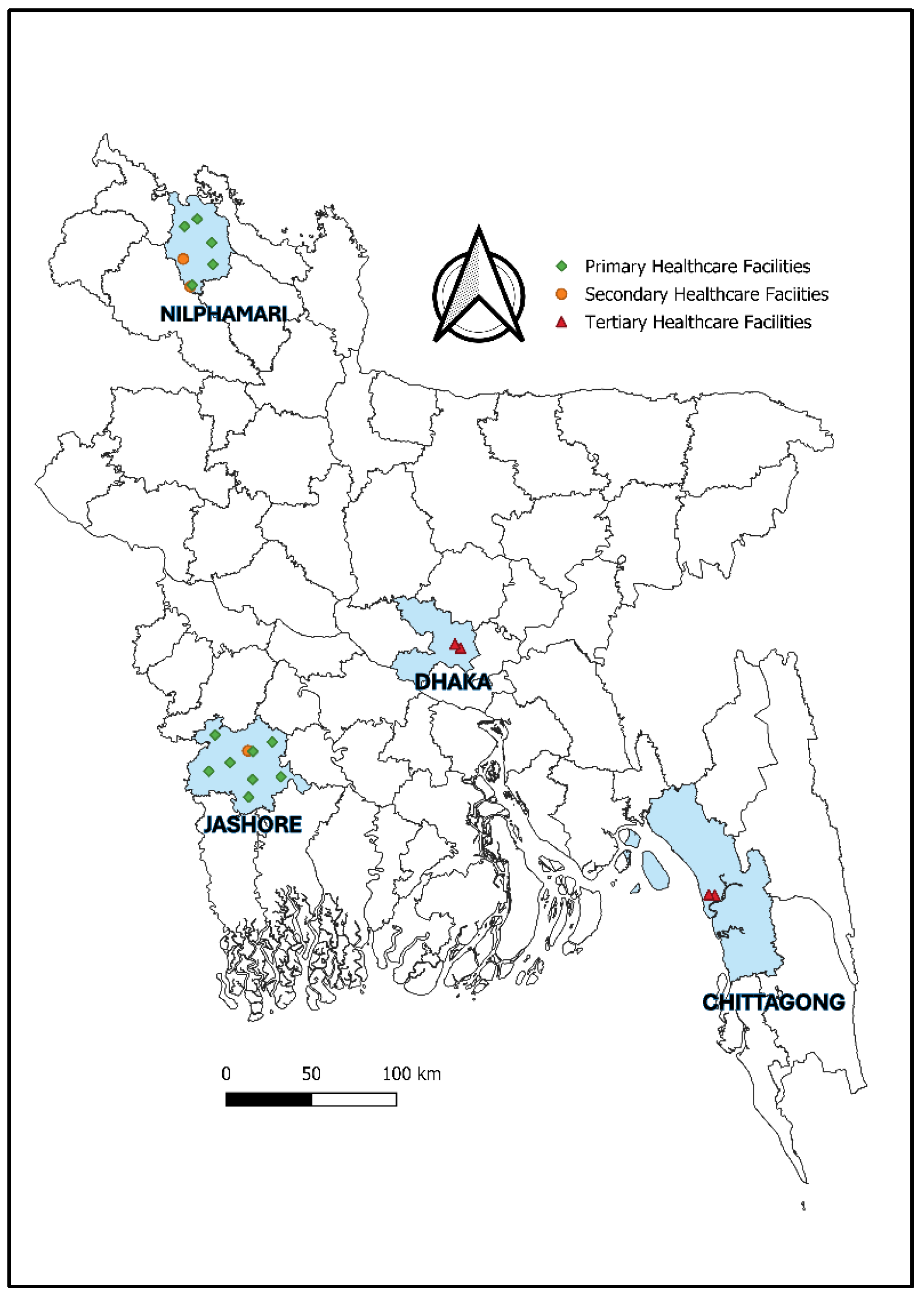
The cohort included HCWs from four purposively selected administrative divisions of Bangladesh: Dhaka, Chittagong, Khulna, and Rangpur. To establish a geographically diverse and representative cohort of HCWs, HCWs were recruited from 20 health facilities across Bangladesh. The locations of the facilities are shown in
Figure 1, and
Table 1 lists each facility’s name, type, and number of beds.
2.2. Participant enrollment
The study population comprised HCWs who provided direct or indirect patient care during the pandemic, working in either COVID-19 or non-COVID-19 wards. At the start of the study, approximately 5,000 HCWs were employed at the participating facilities according to the Directorate General of Health Services (DGHS) Facility Registry. Recruitment followed an open, rolling enrolment approach from February 2021, whereby eligible HCWs could enrol at any time upon providing informed consent, regardless of prior SARS-CoV-2 infection or intentions to be vaccinated against COVID-19. A total of 3,697 HCWs were enrolled till December 2022.
For this cohort, HCWs were defined as facility-employed staff involved in patient care or patient-facing support activities, with potential exposure to patients, body fluids, contaminated materials, or the clinical environment. This definition included healthcare professionals, allied and auxiliary health workers, and support staff such as nurses, physicians, laboratory and diagnostic personnel, radiology physicians and technicians, phlebotomists, respiratory therapists, nutritionists, social workers, physical and rehabilitation therapists, cleaners and laundry personnel, patient transporters, clerical staff, and catering staff. Staff from basic medical science faculties and administrative personnel without clinical or patient-facing responsibilities were excluded.
All participants were contacted by a research physician and a research nurse assigned to each study site during the study period. The physician and nurse collected and maintained a list of HCWs from the selected health facility, including their names, designations, contact numbers, and posting wards, provided by the hospital administration. The research physician and nurse then contacted HCWs who met the inclusion criteria, explained the study’s aims and objectives, and obtained written informed consent from participants who wished to participate. The HCWs who consented to participate were then asked to visit the study room assigned to each hospital for data collection.
2.3. Phases and timelines of the cohort
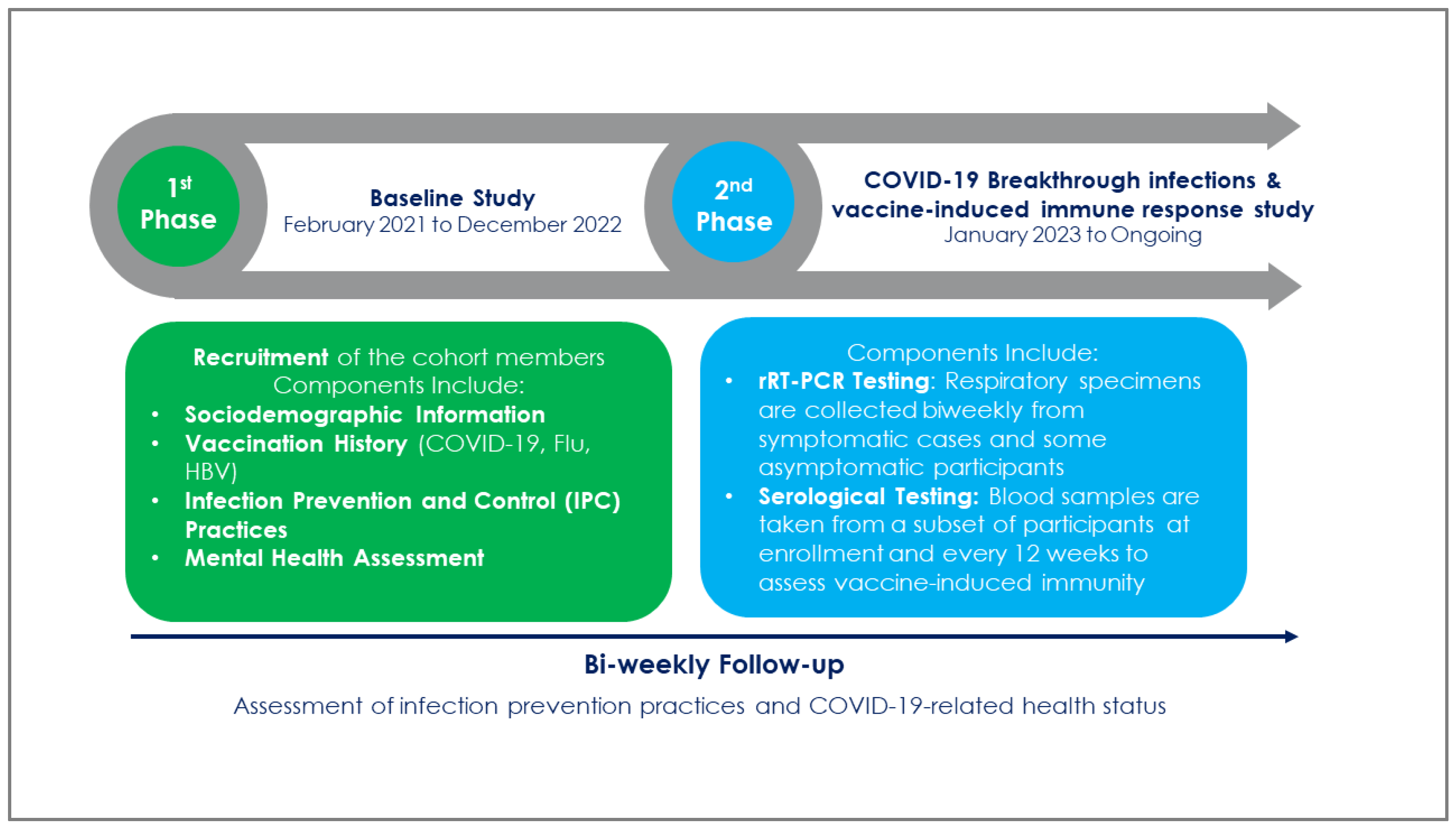
Recruitment of members into this open longitudinal cohort in the first phase of the study began in February 2021 and ended in December 2022. Each member was followed biweekly, starting on the 14th day of enrolment. Phase 2 of the study was introduced in January 2023, when each HCW had received their primary series of COVID-19 vaccine (
Figure 2). Respiratory specimens were collected from suspected COVID-19 cases to determine the incidence of breakthrough infection by rRT-PCR among cohort members. A study of vaccine-induced immune responses was also conducted during this period to assess antibody levels induced by various brands of anti-SARS-CoV-2 vaccines among 1000 HCWs randomly selected from the cohort.
2.4. Baseline information collection
The study physician conducted face-to-face interviews to collect baseline data on HCWs during enrolment. These included information on their socio-demographic characteristics, history of any preexisting or current medical condition, history of having any respiratory illness since the beginning of the epidemic in the country, history of SARS-CoV-2 exposure (which included contact with COVID-19 patients, use of personal protective equipment, adherence to infection prevention and control measures, and participation in aerosol-generating procedures), history of being confirmed for COVID-19 through RT-PCR tests, their self-reported COVID-19 vaccination status (confirmed by a vaccination card provided by the Government of Bangladesh), other vaccination histories (e.g., influenza and Hepatitis B vaccination), and any adverse events following COVID-19 vaccination series. All the information was collected on a handheld computer programmed with a standardized questionnaire by the designated physician. The study physician also collected participants’ anthropometric measurements, including height, weight, and waist circumference (
Table 2).
To assess the mental health status of the enrolled HCWs, at baseline, the questionnaire included questions on the history of having any mental illness, such as depression, mood disorders, anxiety disorders, and sleep and health-related quality of life during the pandemic. Psychometric scales that are validated in Bangladesh, such as the Patient Health Questionnaire (PHQ-9) for depression, Generalised Anxiety Disorder (GAD-7) for anxiety, Perceived Stress Scale (PSS) for stress, Pittsburgh Sleep Quality Index (PSQI) to assess sleep quality, and 12-Item Short Form Survey (SF-12) to assess health-related quality of life were used in the evaluation. Additionally, study instruments for IPC assessment included the WHO Facility Assessment Tool (IPCAF) (31), WHO hand hygiene observation tools (32), a contextualized observational checklist, and structured questionnaires assessing IPC knowledge, attitudes, and practices among HCWs. The mean interview duration was approximately 30 minutes at baseline and 20 minutes at follow-up.
2.5. Protocol for follow-up
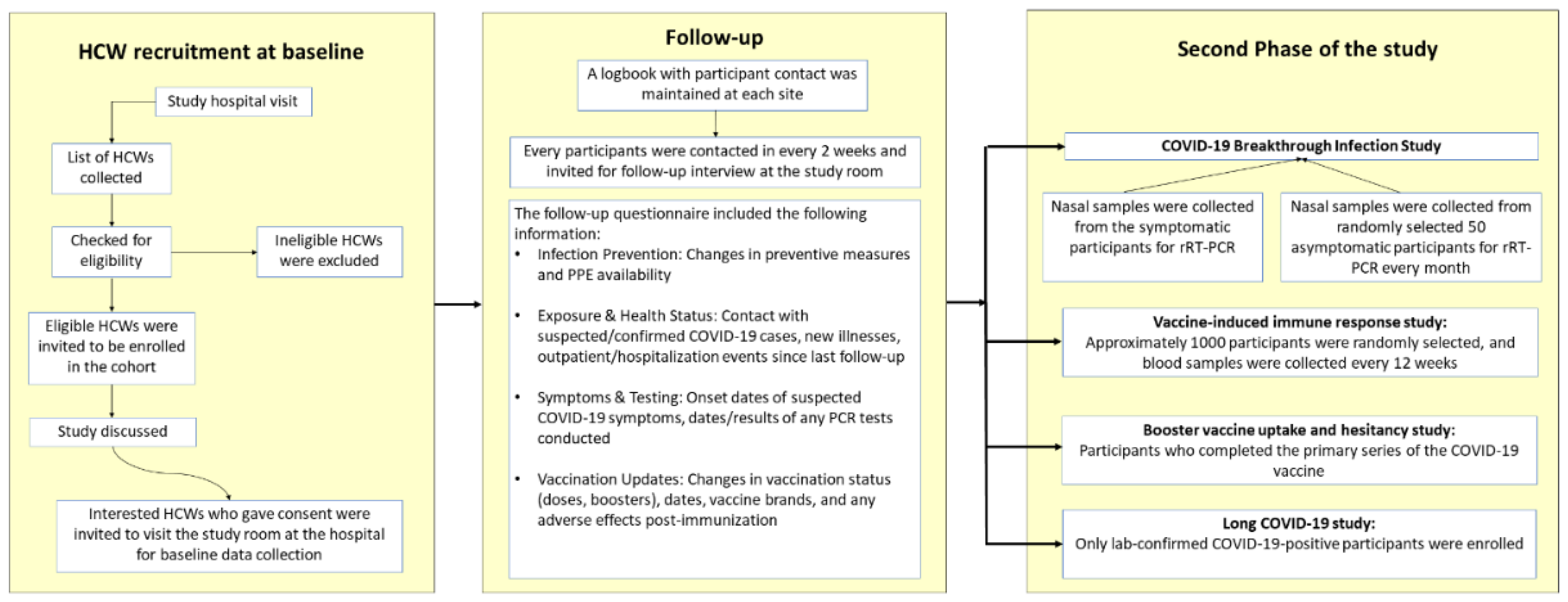
To mitigate the risk of participant attrition during the follow-up phase, a logbook listing the names and contact details of recruited participants was maintained at each study site (
Figure 3).
Follow-up assessments were planned at bi-weekly intervals, with a predefined allowable window around each scheduled contact. When a scheduled follow-up was missed, study staff attempted to contact the participant by telephone on three consecutive days. If contact was unsuccessful, the participant was approached again at the subsequent scheduled follow-up, 14 days later. During each follow-up, the questionnaire had much information in familiar. Participants were asked about any changes in their infection prevention measures, availability of personal protective equipment, contact with individuals suspected or confirmed to have COVID-19, information on any illness, outpatient visits, or hospitalization since the last follow-up, suspected COVID-19 symptoms and date of onset of symptoms, date of PCR testing and if any, PCR results, change in COVID-19 vaccination status, number of doses including booster dose, date of vaccination and brand and any adverse event following immunization (
Table 3).
2.6. Second phase of the study
In January 2023, a breakthrough infection study was initiated within the cohort following the completion of the primary COVID-19 vaccination series. HCWs who met the WHO’s suspected COVID-19 clinical case definition (31) were identified during prospective follow-ups. Nasopharyngeal swabs were collected from these individuals to confirm breakthrough infections. Moreover, to detect asymptomatic COVID-19 cases within the cohort, HCWs were stratified proportionally by role in patient care (e.g., doctors, nurses, and support staff), and respiratory swabs were collected every two weeks from a randomly selected subset of 50 asymptomatic HCWs within these strata. Respiratory specimens collected from HCWs were tested for SARS-CoV-2 using real-time reverse transcriptase PCR (rRT-PCR). All PCR products were analyzed through agarose gel electrophoresis and Sanger sequencing, using separate forward and reverse primers. Additionally, a plan is in place to conduct whole-genome sequencing on a subset of 104–140 respiratory samples (assuming that 20% of positive cases have a CT value ≤30), which will be used to track the emergence of new SARS-CoV-2 variants.
Approximately 1,000 randomly selected HCWs from the baseline cohort were also subjected to a study assessing vaccine-induced immune responses in this phase. A trained study nurse, skilled in safe handling and spill decontamination, collected 10 ml of blood from each participant’s mid-cubital vein. The samples were processed on-site and labeled with unique HCW codes. Specimens were stored at -20 °C at field sites and transported biweekly to the immunology laboratory at the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) for IgG antibody testing against SARS-CoV-2 and analysis of the immune response. The same follow-up strategy was used, with HCWs in this sub-cohort contacted every 12 weeks to provide serum samples at the study site.
A validated tool was used during routine follow-ups in this phase to evaluate HCWs’ acceptance of additional COVID-19 vaccine doses. This included their vaccination status, booster uptake and date, future vaccination intentions, access to booster doses, and scores on the Protection Motivation Theory (PMT) and Vaccine Hesitancy (VH) scales. Furthermore, the long-term effects of COVID-19 on HCWs who reported being infected with SARS-CoV-2 were assessed using WHO’s Global COVID-19 Clinical Platform Case Report Form (CRF) for Post COVID condition (Post COVID-19 CRF) (32). This assessment collected data on the persistence of symptoms following acute COVID-19 infection, including fatigue, cognitive impairment, and respiratory symptoms.
3. Results
3.1. Characteristics of enrolled participants
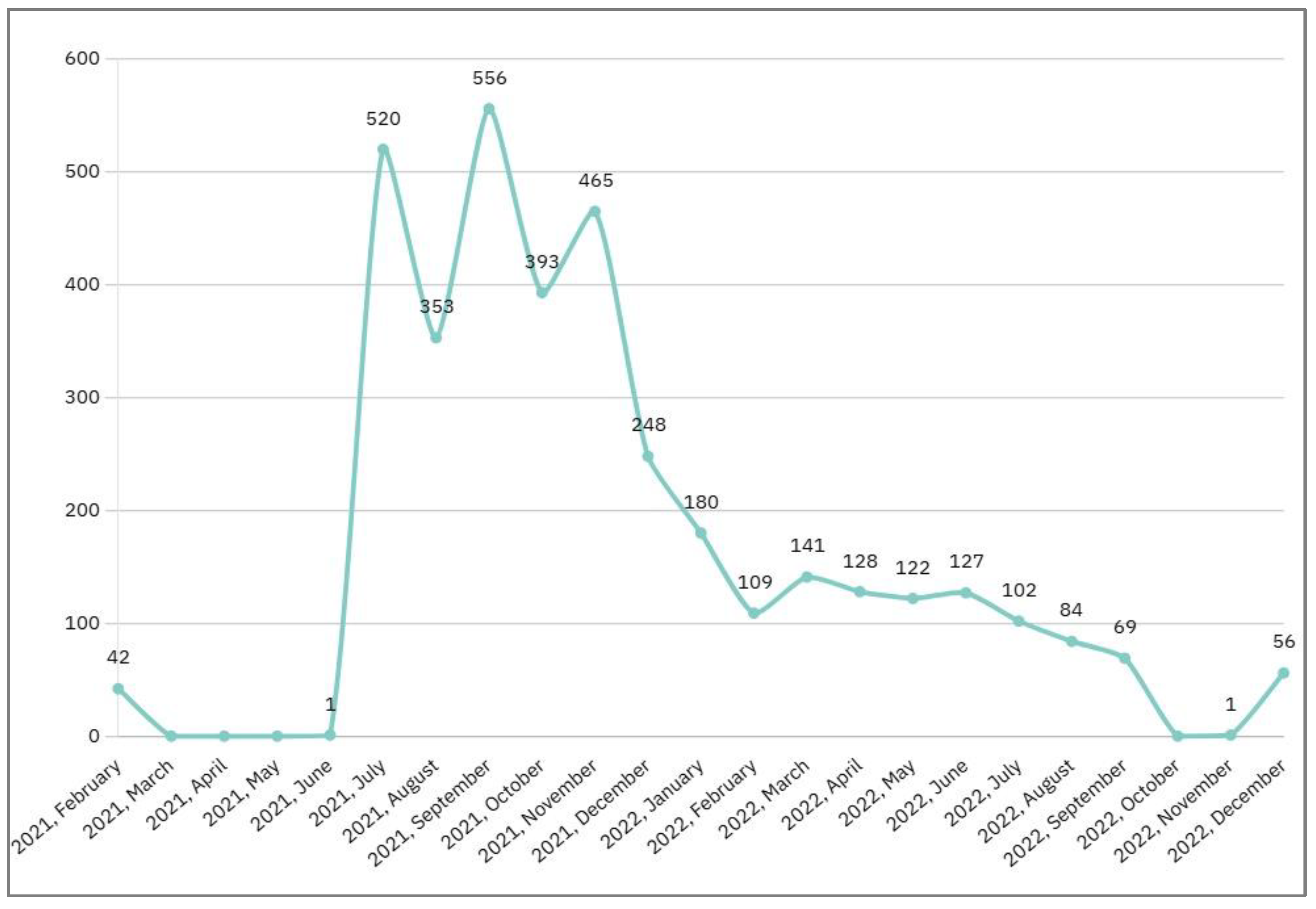
The cohort comprised 3697 participants with a median age of 36 years (IQR: 30-44). Monthly enrolment of HCWs was highest during mid-2021 and declined thereafter, with minimal enrolment observed from 2022 through late 2022 (
Figure 4).
The cohort consisted primarily of female HCWs (53.5%), with nurses accounting for 48% (1769) of the total participants (
Table 4). Support staff were the second most common occupational group (30%), followed by physicians (22%) in the cohort.
3.2. Follow-up implementation
Among the 3,697 enrolled HCWs, the median number of completed follow-up interviews was 27 (IQR: 13-43), and 31% of participants completed at least 40 follow-up interviews. When follow-up completeness was examined at the visit level, 38.9% of all completed follow-up interviews were contributed by participants who completed 20 or fewer follow-ups during their time in the cohort, 32.2% by those who completed 21–40 follow-ups, 24.2% by those who completed 41–60 follow-ups, and 4.7% by participants who completed more than 60 follow-up interviews. This distribution reflects rolling enrolment and variable follow-up duration inherent to the open cohort design.
3.3. COVID-19 illness among HCWs
The highest number of COVID-19 infections was reported in 2020, based on retrospective recall at baseline among all enrolled HCWs. From 2021 onwards, infections were captured prospectively through scheduled follow-up interviews. HCWs faced a second surge of SARS-CoV-2 infections in 2021, mirroring national trends. From 2022 onward, infections among HCWs became infrequent, with only minor fluctuations observed in 2023 and early 2024. These trends likely reflect the combined effects of public health interventions, including improved infection control measures and the rollout of COVID-19 vaccines beginning in early 2021 (35, 36).
According to the findings, 47% (1725) of HCWs experienced at least one symptomatic COVID-19 episode during the study period. Among cohort members, 30% (1117) of HCWs had lab-confirmed COVID-19 and were either PCR- or rapid antigen-positive (
Table 5). Among symptomatic episodes, fever was the most frequently reported symptom in 82% of the HCWs. This was followed by a cough in 56% of them. Among the lab-confirmed cases, 32% (356) also had a history of being hospitalized during this period due to symptoms and severity of COVID-19.
4. Discussion
The demographic and occupational composition of the cohort reflects the structure of the healthcare workforce in Bangladesh and similar low- and middle-income country settings. Among the enrolled HCWs, nurses, and support staff accounted for a substantial proportion of patient-facing roles. The predominance of female participants and nurses is consistent with national and international workforce patterns and reflects the gendered nature of healthcare delivery, particularly in nursing and allied professions (33). The inclusion of a large proportion of support staff in this cohort is also notable, as these groups are generally underrepresented in occupational health studies (34, 35). Capturing outcomes across diverse occupational categories enables a more comprehensive assessment of differential risk profiles within healthcare settings, a gap highlighted in earlier HCW studies during infectious disease outbreaks.
The temporal pattern of SARS-CoV-2 infections observed in this cohort aligns closely with national epidemic trends in Bangladesh. The peak in reported infections in 2020 reflects retrospective baseline recall before cohort initiation, whereas the second surge in 2021 coincided with widespread community transmission during subsequent epidemic waves. The marked decline in infections from 2022 onward likely reflects the combined impact of COVID-19 vaccine rollout, increasing population immunity, and strengthened infection prevention and control measures within healthcare facilities. Similar declines in HCW infections following vaccination and improved IPC practices have been reported in other settings (36). The substantial proportion of HCWs reporting symptomatic infection and hospitalization highlights the occupational vulnerability of this workforce during the early pandemic phase. It reinforces evidence that HCWs experienced both elevated infection risk and more severe disease outcomes before widespread vaccine coverage was achieved (37, 38).
4.1. Patient and Public Involvement
This study was a collaborative effort between the Communicable Disease Control unit of the Ministry of Health and Family Welfare (MoHFW) and icddr,b. Following Institutional Review Board (IRB) approval, we adopted a participatory approach that embedded participant and public involvement throughout the study process. Initial consultations were held with healthcare facility directors to align the study objectives with on-the-ground feasibility and inform recruitment and communication strategies. Transparent and continuous communication with participants ensured they remained informed and supported during the study. Participants in the serology sub-study and those who provided nasal swabs received their results. They were encouraged to share feedback on their experience, which informed planning for subsequent study phases. Administrative officers, government officials, and participants were also provided with interim study updates and engaged in ongoing discussions, ensuring that their perspectives helped shape the cohort’s direction. This inclusive and responsive approach enhanced the study’s cultural relevance, acceptability, and alignment with the community.
4.2. Future research plans
With the long COVID data collected, the impact of long COVID on HCWs will be analyzed to understand its long-term effects on health and workforce capacity. By examining self-reported symptoms, the analysis aims to uncover patterns of prolonged post-COVID complications. Understanding the burden of long-COVID among Bangladeshi HCWs will provide valuable insights for LMICs with limited healthcare resources. It will shed light on the effects on healthcare systems and inform the development of targeted interventions, such as rehabilitation programs, workplace accommodations, and public health policies.
Additionally, serological analysis results, demographic information, and self-reported infection and immunization data will be used to examine the long-term effects of COVID-19 infection among subcohort participants. Furthermore, the results obtained from serology analysis during consecutive future follow-ups will also be used to assess the decrease in antibody titer levels in HCWs following vaccination. Biweekly follow-up and respiratory swab specimen collection from suspected COVID-19 cases within the cohort will continue to determine breakthrough infections following vaccination and to monitor emerging SARS-CoV-2 strains. Detecting emerging strains and monitoring immunogenicity against newer variants will help tailor effective preventive strategies in LMICs, including modifications to existing vaccines and the implementation of necessary public health measures. This can be achieved by sharing data among researchers and public health agencies worldwide. This collaborative effort will enable a swifter response to emerging variants and the development of more targeted vaccines and public health interventions.
4.3. Strengths and Limitations
This study is the first and largest cohort of HCWs in Bangladesh. It includes HCWs from all levels of healthcare facilities, including primary, secondary, and tertiary care, and represents all tiers of HCWs. Additionally, the study captures a diverse sample of HCWs across various roles, occupational settings, and geographic regions within an LMIC in the early stages of the pandemic, thereby ensuring a broad and inclusive perspective. The implementation and maintenance of biweekly follow-ups across the various stages of the pandemic mitigated the risk of data loss and enabled a comprehensive assessment of participants’ health status over the course of the study. The study additionally evaluates HCW’s physical and mental health dimensions, offering an extensive perspective on their overall well-being. The breakthrough infection study provides significant insights into vaccine efficacy and disease transmission mechanisms among HCWs exposed to SARS-CoV-2 through their occupation. The assessment of antibody levels elicited by various vaccine brands also plays a crucial role in enhancing comprehension of vaccination effectiveness and immunogenicity. This cohort, which has been regularly monitored throughout the pandemic, offers reliable data for analyzing workplace and personal factors associated with vaccination, infection with the SARS-CoV-2 virus, and adverse health effects of COVID-19 illness.
Despite its strengths, this study has several limitations too. HCWs were not randomly recruited into the cohort, which may limit the generalizability of the findings to the broader HCW community. Similarly, the subset of 1000 HCWs included in the immune response study may not accurately represent the entire cohort, which could limit the generalizability of the results. Additionally, the study evaluated serum antibody levels but may not capture other aspects of the immune response, such as cellular immunity.
4.4. Collaboration
To maintain the study participants’ confidentiality, the individual-level data is not publicly accessible. However, researchers interested in potential collaboration should contact the corresponding author. The research steering committee’s evaluation of data requests will adhere to established protocols for cohort studies to safeguard anonymity and ensure compliance with the terms outlined in the informed consent form used in this study.
5. Conclusions
The Bangladesh Healthcare Worker Cohort is the first large-scale HCW cohort that establishes a longitudinal framework for studying the short- and long-term impacts of COVID-19 on this risk group in Bangladesh. By combining repeated follow-up with clinical, occupational, mental health, and immunological data, the cohort provides an evidence base for examining evolving risks related to infection, vaccination, and recovery over time. Evidence generated from this cohort will inform occupational health policies, infection prevention strategies, and workforce support interventions in Bangladesh and similar resource-constrained settings.
Author Contributions
MZH conceptualized the original study design, obtained funding, and/or acted as principal investigator. HRS prepared the first draft and subsequent versions of the manuscript under MZH’s supervision. MZH, AKB, ASP, MAAJB, MR, FC, and AR reviewed and provided critical feedback on the manuscript. All authors read and approved the final manuscript.
Funding
This work has been supported by the US Centers for Disease Control and Prevention, Atlanta, GA, USA (Grant No GR-02312; Award ID: PO# 5263).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of icddr,b (PR: 22113).
Informed Consent Statement
Written informed consent was obtained from all participants. The study team provided comprehensive oral and written explanations in the local language (Bangla) regarding the research aims, objectives, potential risks and benefits, confidentiality, voluntary participation, the right to withdraw at any time, conflicts of interest, and compensation. Participants were reminded that their participation was entirely voluntary and that all information would remain confidential before they were asked to sign the consent form.
Data Availability Statement
The authors assume responsibility for the data presented in this manuscript. The datasets produced and analysed in this study are available from the corresponding author upon request.
Acknowledgments
The authors gratefully acknowledge the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) for its organizational and institutional assistance in facilitating this research. icddr,b extends its sincere appreciation to the Governments of Bangladesh and Canada for their continued and unrestricted support to the institute, which made this study possible.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HCW |
Healthcare Worker |
| WHO |
World Health Organization |
| PPE |
Personal Protective Equipment |
| rRT-PCR |
Real-time Reverse Transcription-Polymerase Chain Reaction. |
References
- WHO SAGE ROADMAP FOR PRIORITIZING USES OF COVID-19 VACCINES IN THE CONTEXT OF LIMITED SUPPLY [Internet]. SAGE Working Group on COVID-19 vaccines. 2020. Available online: https://www.who.int/docs/default-source/immunization/sage/covid/sage-prioritization-roadmap-covid19-vaccines.pdf (accessed on 17 August 2025).
- Wei, XS; Wang, XR; Zhang, JC; Yang, WB; Ma, WL; Yang, BH; et al. A cluster of health care workers with COVID-19 pneumonia caused by SARS-CoV-2. J Microbiol Immunol Infect. 2021, 54(1), 54–60. [Google Scholar] [CrossRef]
- Chew, NWS; Lee, GKH; Tan, BYQ; Jing, M; Goh, Y; Ngiam, NJH; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav Immun. 2020, 88, 559–65. [Google Scholar] [CrossRef]
- Preti, E; Di Mattei, V; Perego, G; Ferrari, F; Mazzetti, M; Taranto, P; et al. The Psychological Impact of Epidemic and Pandemic Outbreaks on Healthcare Workers: Rapid Review of the Evidence. Curr Psychiatry Rep. 2020, 22(8), 43. [Google Scholar] [CrossRef]
- Dzinamarira, T; Nkambule, SJ; Hlongwa, M; Mhango, M; Iradukunda, PG; Chitungo, I; et al. Risk Factors for COVID-19 Infection Among Healthcare Workers. A First Report From a Living Systematic Review and meta-Analysis. Saf Health Work. 2022, 13(3), 263–8. [Google Scholar] [CrossRef]
- World Health Organization. Health and Care Worker Deaths during COVID-19 2021. Available online: https://www.who.int/news/item/20-10-2021-health-and-care-worker-deaths-during-covid-19#:~:text=WHO%20estimates%20that%20between%2080,in%20the%20world’s%20pandemic%20response (accessed on 17 August 2025).
- Rahman, A; Abdulla, F; Karimuzzaman, M; Hossain, MM. Burden of COVID-19 on health and wellbeing, education, and economy of Bangladesh. Clinical Case Reports 2022, 10(11), e6639. [Google Scholar] [CrossRef] [PubMed]
- Opu, MH. Over 180 doctors killed due to coronavirus in Bangladesh. Dhaka Tribune. 2021. Available online: https://www.dhakatribune.com/bangladesh/health/256664/over-180-doctors-killed-due-to-coronavirus-in (accessed on 17 August 2025).
- Rahman, MS; Farzana, M; Rahman, T. Occupational Challenges and Physician Deaths During COVID-19 Pandemic. International Journal of Travel Medicine and Global Health 2021, 9(2), 100–1. [Google Scholar] [CrossRef]
- Cousins, S. Bangladesh’s COVID-19 testing criticised. The Lancet 2020, 396(10251), 591. [Google Scholar] [CrossRef]
- Rahaman, KR; Mahmud, MS; Mallick, B. Challenges of Testing COVID-19 Cases in Bangladesh. International Journal of Environmental Research and Public Health 2020, 17(18), 6439. [Google Scholar] [CrossRef]
- Islam, MT; Talukder, AK; Siddiqui, MN; Islam, T. Tackling the COVID-19 pandemic: The Bangladesh perspective. J Public Health Res. 2020, 9(4), 1794. [Google Scholar] [CrossRef] [PubMed]
- Sakib, SN. Bangladesh: Low COVID-19 testing rate raises concerns. Anadolu Agency. 2020. Available online: https://www.aa.com.tr/en/asia-pacific/bangladesh-low-covid-19-testing-rate-raises-concerns/1810132 (accessed on 17 August 2025).
- Chen, X; Huang, Z; Wang, J; Zhao, S; Wong, MC; Chong, KC; et al. Ratio of asymptomatic COVID-19 cases among ascertained SARS-CoV-2 infections in different regions and population groups in 2020: a systematic review and meta-analysis including 130 123 infections from 241 studies. BMJ Open. 2021, 11(12), e049752. [Google Scholar] [PubMed]
- Sah, P; Fitzpatrick, MC; Zimmer, CF; Abdollahi, E; Juden-Kelly, L; Moghadas, SM; et al. Asymptomatic SARS-CoV-2 infection: A systematic review and meta-analysis. Proc Natl Acad Sci U S A 2021, 118(34). [Google Scholar]
- Ma, Q; Liu, J; Liu, Q; Kang, L; Liu, R; Jing, W; et al. Global Percentage of Asymptomatic SARS-CoV-2 Infections Among the Tested Population and Individuals With Confirmed COVID-19 Diagnosis: A Systematic Review and Meta-analysis. JAMA Netw Open. 2021, 4(12), e2137257. [Google Scholar] [CrossRef]
- Syangtan, G; Bista, S; Dawadi, P; Rayamajhee, B; Shrestha, LB; Tuladhar, R; et al. Asymptomatic SARS-CoV-2 Carriers: A Systematic Review and Meta-Analysis. Front Public Health 2020, 8, 587374. [Google Scholar] [CrossRef]
- World Health Organization. WHO SAGE roadmap for prioritizing uses of COVID-19 vaccines: an approach to optimize the global impact of COVID-19 vaccines, based on public health goals, global and national equity, and vaccine access and coverage scenarios, first issued 20 October 2020, updated: 13 November 2020, updated: 16 July 2021, latest update: 21 January 2022; World Health Organization: Geneva, 2022; Contract No.: WHO/2019-nCoV/Vaccines/SAGE/Prioritization/2022.1. [Google Scholar]
- Population-based age-stratified seroepidemiological investigation protocol for coronavirus 2019 (COVID-19) infection [Internet]. 2020. Available online: https://iris.who.int/bitstream/handle/10665/332188/WHO-2019-nCoV-Seroepidemiology-2020.2-eng.pdf?sequence=1 (accessed on 17 August 2025).
- Chen, H; Wang, B; Cheng, Y; Muhammad, B; Li, S; Miao, Z; et al. Prevalence of posttraumatic stress symptoms in health care workers after exposure to patients with COVID-19. Neurobiology of Stress. 2020, 13, 100261. [Google Scholar] [CrossRef]
- Giusti, EM; Pedroli, E; D’Aniello, GE; Stramba Badiale, C; Pietrabissa, G; Manna, C; et al. The Psychological Impact of the COVID-19 Outbreak on Health Professionals: A Cross-Sectional Study. In Frontiers in Psychology; 2020. [Google Scholar]
- Cheng, SKW; Wong, CW; Tsang, J; Wong, KC. Psychological distress and negative appraisals in survivors of severe acute respiratory syndrome (SARS). Psychological Medicine 2004, 34(7), 1187–95. [Google Scholar] [CrossRef]
- Repon, MAU; Pakhe, SA; Quaiyum, S; Das, R; Daria, S; Islam, MR. Effect of COVID-19 pandemic on mental health among Bangladeshi healthcare professionals: A cross-sectional study. Sci Prog. 2021, 104(2), 368504211026409. [Google Scholar] [CrossRef] [PubMed]
- Tasnim, R; Sujan, MSH; Islam, MS; Ritu, AH; Siddique, MAB; Toma, TY; et al. Prevalence and correlates of anxiety and depression in frontline healthcare workers treating people with COVID-19 in Bangladesh. BMC Psychiatry 2021, 21(1), 271. [Google Scholar] [CrossRef] [PubMed]
- Darboe, SMK; Darfour-Oduro, SA; Kpene, GE; Kebbeh, A; Fofana, N; Ndow, M; et al. Factors influencing healthcare workers’ perceived compliance with infection prevention and control standards, North Bank East region, The Gambia, a cross-sectional study. BMC Research Notes 2025, 18(1), 43. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, N; Elmahboub, R; Al-Qahtani, F; Qahtani, S; Eldeeb, S; Margan, A; et al. Assessment of Healthcare Workers’ Adherence to Infection Prevention and Control Measures in Najran City, Saudi Arabia, in the Post-COVID-19 Pandemic Era. Journal of Pure and Applied Microbiology 2024, 18. [Google Scholar] [CrossRef]
- El-Ghitany, E; Elrewany, E; Omran, E; Farghaly, A; Azzam, N. Self-reported adherence of healthcare workers to infection prevention and control practices during the early waves of the COVID-19 pandemic in Egypt. International Journal of Infection Control 2023. [Google Scholar] [CrossRef]
- Weldetinsae, A; Alemu, ZA; Tefaye, K; Gizaw, M; Alemahyehu, E; Tayachew, A; et al. Adherence to infection prevention and control measures and risk of exposure among health-care workers: A cross-sectional study from the early period of COVID-19 pandemic in Addis Ababa, Ethiopia. Health Sci Rep. 2023, 6(6), e1365. [Google Scholar] [CrossRef]
- Babore, GO; Eyesu, Y; Mengistu, D; Foga, S; Heliso, AZ; Ashine, TM. Adherence to Infection Prevention Practice Standard Protocol and Associated Factors Among Healthcare Workers. Glob J Qual Saf Healthc 2024, 7(2), 50–8. [Google Scholar] [CrossRef] [PubMed]
- Wee, LEI; Conceicao, EP; Tan, JY; Magesparan, KD; Amin, IBM; Ismail, BBS; et al. Unintended consequences of infection prevention and control measures during COVID-19 pandemic. American Journal of Infection Control 2021, 49(4), 469–77. [Google Scholar] [CrossRef]
- World Health Organization. WHO COVID-19 Case definition 2022. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Surveillance_Case_Definition-2022.1 (accessed on 17 December 2025).
- World Health Organization. Global COVID-19 Clinical Platform Case Report Form (CRF) for Post COVID condition (Post COVID-19 CRF). 2021. [Google Scholar]
- World Health Organization. Delivered by women, led by men: A gender and equity analysis of the global health and social workforce. Human Resources for Health Observer Series No. 24 2019. [Google Scholar]
- International Labour Organization. Care work and care jobs for the future of decent work. 2018. [Google Scholar]
- Lan, FY; Wei, CF; Hsu, YT; Christiani, DC; Kales, SN. Work-related COVID-19 transmission in six Asian countries/areas: A follow-up study. PLoS One 2020, 15(5), e0233588. [Google Scholar] [CrossRef]
- Nguyen, LH; Drew, DA; Graham, MS; Joshi, AD; Guo, CG; Ma, W; et al. Risk of COVID-19 among front-line health-care workers and the general community: a prospective cohort study. Lancet Public Health 2020, 5(9), e475–e83. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T; Ripp, J; Trockel, M. Understanding and Addressing Sources of Anxiety Among Health Care Professionals During the COVID-19 Pandemic. JAMA 2020, 323(21), 2133–4. [Google Scholar] [CrossRef] [PubMed]
- Brooks, SK; Webster, RK; Smith, LE; Woodland, L; Wessely, S; Greenberg, N; et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. The Lancet 2020, 395(10227), 912–20. [Google Scholar] [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).