
Submitted:
31 December 2025
Posted:
31 December 2025
You are already at the latest version
Abstract
Background: Intraductal papillary mucinous neoplasms (IPMN) are the most common pancreatic cystic lesions and are established precancerous entities. Side-branch IPMN (SB-IPMN) are the most prevalent subtype and generally carry a low risk of malignant transformation. The revised 2024 Kyoto guidelines define management and surveillance strategies based on high-risk stigmata and worrisome features; however, real-life adherence to these recommendations remains variable.
Aim: To compare real-world management of SB-IPMN at a tertiary medical center with Kyoto guideline–based recommendations using an algorithm-based decision-support tool.
Methods: SB-IPMN cases were retrospectively analyzed. An algorithm implementing the Kyoto guidelines was used to generate recommended management strategies based on imaging, clinical, and laboratory data, and these recommendations were compared with actual clinical decisions. Long-term clinical and radiological follow-up data were collected, including development of pancreatic ductal adenocarcinoma (PDAC).
Results: A total of 368 patients (69% male; median age 69.5 years) were followed for a median of 48.5 months radiologically and 64 months clinically. Mean cyst size at presentation was 11 ± 6.5 mm. Only 58 patients (15.8%) were managed in accordance with Kyoto guidelines; most underwent more intensive surveillance (60.3%), while 23.9% received less intensive monitoring (p = 0.04). Larger cyst size (>2 cm) was associated with higher guideline adherence. Younger patients, including all patients under 50 years of age, were more frequently over-surveilled. Over-surveillance resulted in an excess of 0.42 MRI/MRCP examinations per patient-year. Only one PDAC case occurred, arising after more than five years of cyst stability.
Conclusion: Fewer than 20% of patients with SB-IPMN were managed according to Kyoto guidelines. Over-surveillance was common, particularly in younger patients, without apparent oncologic benefit. Algorithm-based decision-support tools may help standardize care and optimize resource utilization.
Keywords:
intraductal papillary mucinous neoplasm
; pancreatic cyst surveillance
; Kyoto guidelines
; clinical decision‐support systems
1. Background
Intraductal papillary mucinous neoplasms (IPMN) are the most common type of cystic pancreatic lesions. Having equal sex distribution, they arise from ductal cells and are classified by anatomical location (main duct, side branch, or mixed), histologic subtype, and degree of dysplasia. These cysts have established malignant potential, depending on histologic and anatomic characteristics, previously estimated as high as 85% for main-duct IPMN (MD-IPMN) and 38% for side-branch IPMN (SB-IPMN), based on surgical specimens2,3. This risk, however, is much lower for small, asymptomatic surveyed cysts4-6. Being mostly asymptomatic, IPMN surveillance and management is therefore usually guided by risk stratification using imaging and clinical features1.
In many pancreaticobiliary tertiary center, current management strategies are primarily defined by the International Association of Pancreatology (IAP) Fukuoka guidelines (2017)7 and the revised Kyoto guidelines (2024)8. The Fukuoka guidelines stratify patients by "high-risk stigmata" (main pancreatic duct ≥10 mm, obstructive jaundice, enhancing mural nodule ≥5 mm) and "worrisome features" (cyst ≥3 cm, mural nodule <5 mm, thickened cyst wall, main duct 5–9 mm, abrupt duct change, lymphadenopathy, elevated CA 19-9, rapid growth >5 mm/2 years). Surgical resection is warranted for main duct IPMN or SB-IPMN with high-risk stigmata; Endoscopic ultrasonography (EUS) is recommended for surveillance of worrisome features, with surgery considered for surgically fit patients with additional risk factors. Otherwise, surveillance is recommended using cross sectional imaging modalities, such as contrast-enhanced magnetic resonance imaging/cholangiopancreatography (MRI/MRCP), and contrast-enhanced multi-detector computed tomography (MDCT). Surveillance intervals are tailored to cyst size and features, with more frequent imaging for higher-risk lesions9.
The revised Kyoto guidelines similarly stratify IPMN by high-risk stigmata and worrisome features, but emphasize the cumulative effect of multiple worrisome features. They provide validated hazard ratios for malignancy risk, increasing with larger numbers of worrisome features, and therefore support personalized management10,11. Necessity of long-term surveillance is not well defined in the guidelines, suggesting its duration to be decided based on local health economics and individual patient characteristics8.
With IPMN prevalence increasing with age, reaching 11% over the age of 50 and over 20% by the age of 8012,13, and given the fact side-branch lesions are estimated to comprise 70% of all IPMN5, surveillance of these lesions has significant implications, from both the individual patient and healthcare systems perspectives. However, the additive effect of several worrisome features on suggested management according to the revised Kyoto guidelines makes clinical decision making even more complex and prone to variability between physicians.
This study aimed to use a specially-designed AIgo-based decision-support tool to compare real-life clinical practice at a single tertiary medical center with guideline-based management according to the Kyoto criteria, and to evaluate its clinical implications.
2. Methods
2.1. Study Population
A total of 368 patients with known SB-IPMN from our center were followed up retrospectively for 17 years, between 2007-2024. All patients were over the age of 18 and had undergone at least one initial MRI/MRCP at our institution, marking the beginning of follow-up. Following the index MRI/MRCP, all patients were either followed up radiologically at our center (with at least one other MRI/MRCP or EUS), or were referred to surgery.
Excluded from the study were individuals under the age of 18, patients diagnosed simultaneously with MD-IPMN or mixed-type IPMN, patients with pancreatic cysts other than IPMN and patients who were lost to follow up at our center after the index MRI/MRCP.
The decision-support tool (AIgo) was developed to operationalize the revised Kyoto guidelines8 in a standardized and reproducible manner. Development was based on a detailed review of the original guideline publications and the underlying decision tree logic describing risk stratification according to high-risk stigmata and cumulative worrisome features. The guideline decision framework was then provided as structured input to a large language model (LLM)-based artificial intelligence (AI) system, which translated the clinical decision tree into a rule-based, code-driven calculator.
The tool was implemented on a web-based platform, enabling structured data entry of patient demographics, clinical characteristics, and imaging findings, and generating guideline-concordant management recommendations, including surveillance modality and interval or referral for surgery. All outputs generated by the AI model were manually reviewed and validated by the study investigators to ensure strict fidelity to the original Kyoto decision tree and to avoid deviations introduced by automated interpretation. Discrepancies were iteratively corrected until full concordance with guideline logic was achieved. The finalized version of the AIgo tool was then used retrospectively for all study participants to generate standardized recommendations, which were subsequently compared with real-life clinical decisions. The tool is accessible at sher-ai.com.
Data on all 368 patients were collected from medical records and into the decision-making tool, including relevant demographic and clinical parameters. These parameters included age, expected life expectancy, IPMN type, general performance status, prior recurrent events of pancreatitis and the presence of cumulative worrisome features. Specific worrisome features or high-risk stigmata were also documented from MRI/MRCP reports. The Algo-based tool then provided specific recommendations regarding mode of treatment or surveillance for each case, with the recommended interval to the next imaging. That recommendation was compared to real-life clinical decisions made. In addition, medical records were reviewed for prior medical history and relevant conditions (presence of diabetes mellitus, BMI, smoking or alcohol abuse history, pancreatitis or other hepatobiliary diseases, prior malignancies or their development during follow-up).
2.2. Statistical Analysis
Categorical variables were presented as frequencies and percentages. Continuous variables distribution was evaluated using histograms. Since the continuous variables did not follow a normal distribution, they were reported as medians and interquartile ranges (IQRs). Accordance between clinical management and the Kyoto guidelines was examined using the Chi-square test and Fisher's exact test for categorical variables, while the association for continuous and ordinal variables was investigated using the Mann-Whitney test. Similarly, the choice to manage a patient in a more stringent or liberal way than the guidelines was associated with categorical variables using the Chi-square test and Fisher's exact test, while the association with continuous and ordinal variables was investigated using the Kruskal-Wallis test. SPSS software was used for all statistical analyses (IBM SPSS Statistics for Windows, Version 29, IBM Corp., Armonk, NY, USA, 2023)
3. Results
Three hundred and sixty-eight patients (69% male, 31% female) with a median age of 69.5 (IQR 63.2-75.2) years were included in the study. They were followed up radiologically and clinically for median durations of 48.5 (IQR 28-75) and 64 (IQR 46-88) months, respectively, between the years 2007-2014. All had SB-IPMN, with an average leading cyst size at presentation of 11±6.5 mm. thirty-nine patients (10.5%) had more than one cyst at the beginning of follow-up, and in their case, progression data was collected on the main cyst. Baseline demographic and clinical data are presented in Table 1.
Following index MRI/MRCP, only 58 patients (15.8%) were managed in accordance with the Kyoto guidelines. The rest were mostly subjected to more rigorous follow-up (n=222, 60.3% of the total cohort), while only 88 patients (23.9%) underwent less intensive monitoring (p=0.04). Cyst size>2 cm was associated with higher rates of follow-up according to guidelines compared to patients with cysts smaller than 2 cm (16.8% vs 32.5%, p=0.008). Similarly, median cyst size was significantly larger in patients managed in accordance with guidelines (12 mm, IQR 10-19 mm vs. 10 mm, IQR 10-14 mm, p=0.006). No other demographic or clinical parameters were associated with guideline adherence. Data are presented in Table 2.
Median age was not different among patients managed according to recommendations compared with those who were not (69.5 years, IQR 62.9-75.4 vs. 70.4 years, IQR 64.8-74.4 respectively, p=0.756). However, among patients not managed in accordance with clinical recommendations, the more conservatively-managed subgroup had a younger median age than the liberally-managed one (67.2 years, IQR 62.0-74.4 vs. 72.9 years, IQR 66.3-77.8, respectively, p=0.007). This stringent tendency among younger patients is further emphasized when analyzing a subgroup of patients under 50 years of age: of the 19 patients (5% of the cohort) who were under the age of 50 at the beginning of follow up, 17 were managed over-conservatively. Two other patients, who had high risk stigmata, were referred to surgery in accordance with guidelines.
Over-rigorous follow-up resulted in an average excess of 0.42 MRI/MRCPs per patient-year. During follow-up, pancreatic ductal adenocarcinoma (PDAC) developed in only one patient. However, this patient was from the conservatively managed group, with the PDAC occurring after over five years of cyst stability.
4. Discussion
This retrospective, single-center, decision-support tool–based study compared real-life clinical decision-making in the management of side-branch intraductal papillary mucinous neoplasms (SB-IPMN) with the revised Kyoto guidelines. We found that fewer than 20% of patients were managed in alignment with guideline recommendations, with the majority undergoing more intensive surveillance. These findings are consistent with prior reports showing that surveillance intervals and imaging modalities are frequently individualized based on physician preference, institutional policy, and patient-related factors, rather than strict adherence to standardized protocols recommended by the International Association of Pancreatology, the European Study Group on Cystic Tumors of the Pancreas, or the American Gastroenterological Association (AGA) guideline14.
A recent systematic review by Kazmi et al., demonstrated that over-surveillance is particularly common in small, low-risk cysts (<2 cm without worrisome features), and suggested that less frequent imaging would be appropriate in these cases15. Our findings are in accordance with this observation, as guideline adherence was more frequent in patients with cysts larger than 2 cm, while smaller, stable cysts were more often over-surveilled. Conversely, Han et al., reported that under-surveillance may occur in patients with higher-risk features, often due to comorbidities, non-adherence, or limited healthcare resources14, although this pattern was less prominent in our cohort.
Several prior studies have attempted to address the variability and complexity of IPMN management through algorithmic, nomogram-based, or decision-support approaches aimed at improving risk stratification and standardizing clinical decision-making. Early efforts primarily focused on malignancy risk prediction rather than guiding surveillance strategies. For example, Jang et al.,4 developed a nomogram incorporating cyst size, mural nodules, and ductal features to estimate individualized malignancy risk in branch-duct IPMN, demonstrating improved discrimination compared with guideline criteria alone. More recently, algorithmic frameworks have been proposed to translate guideline logic into structured clinical pathways. Fong et al., emphasized the need for a graded, algorithm-based approach to reconcile discrepancies between existing guidelines and reduce inter-physician variability, particularly in borderline case16.
In this context, our study differs from previous algorithm-based work in several important ways. Rather than developing a new predictive model, we implemented an AIgo-based decision-support tool that faithfully operationalizes the Kyoto guideline decision tree, ensuring strict concordance with published recommendations. This enabled direct comparison between real-world clinical decisions and guideline-based outputs at the individual patient level and allowed quantification of both over- and under-surveillance. To our knowledge, this is the first study to use a validated algorithmic implementation of the Kyoto guidelines to systematically assess guideline adherence, resource utilization, and oncologic outcomes in a large SB-IPMN surveillance cohort.
Several studies have addressed the question of surveillance de-escalation or cessation. A multicenter analysis by Marchegiani et al., demonstrated that patients aged ≥65 years with SB-IPMN ≤15 mm that remained morphologically stable and free of worrisome features or high-risk stigmata for at least five years were most likely to benefit from reduced or discontinued surveillance. For patients aged ≥75 years, this threshold could be extended to cysts <30 mm, provided stability was maintained over five years3. These cysts were associated with malignant conversion rates of approximately 0.2% and time to progression often exceeding ten years14. McGuigan et al,. further reinforced these findings, showing that patients with stable cysts had standardized incidence ratios for pancreatic ductal adenocarcinoma (PDAC) comparable to those of the general population17.
Patients with a high comorbidity burden, particularly those with elevated age-adjusted Charlson Comorbidity Index scores, appear to derive limited benefit from intensive surveillance strategies. In these individuals, non–IPMN-related mortality substantially exceeds the risk of IPMN progression, thereby diminishing the likelihood of benefit from continued surveillance or surgical intervention18,19.
In contrast, our study identified a clear association between younger age and over-surveillance. A recently published systematic review showed that surveillance is often continued in younger individuals even when the risk of progression is low, whereas discontinuation is more frequently considered in older patients with stable, low-risk cysts20. This likely reflects a tendency to maintain intensive surveillance in younger cohorts due to perceived benefit from early cancer detection and longer life expectancy. However, this approach contrasts with data suggesting that age alone is not a significant predictor of malignant progression. Indeed, Ideno et al., concluded that age was not independently associated with progression to PDAC 20.
Although the retrospective design of our study precluded formal assessment of optimal surveillance duration, it nonetheless demonstrates a tendency toward intensified surveillance in younger patients. This practice stands in contradiction to current consensus guidelines, including those of the American College of Gastroenterology, the International Association of Pancreatology, and recent systematic reviews, which recommend surveillance intervals based on cyst size, the presence of worrisome features, and overall life expectancy, without specific interval modification based solely on younger age3,5,14,21.
Over-surveillance in our cohort resulted in an average excess of 0.42 MRI/MRCP examinations per patient-year. Comparable quantitative data from other cohorts are limited. For example, Girometti et al., reported an average of 1.12 MRI/MRCP examinations per patient-year in a smaller cohort of SB-IPMN patients22. However, that study included patients referred for initial evaluation of suspected SB-IPMN, including individuals subsequently excluded from follow-up after IPMN was ruled out, likely underestimating the true long-term surveillance burden in patients with established diagnoses.
Excess imaging inevitably leads to increased healthcare utilization, with over-surveillance previously estimated to cost approximately $2,600–$8,100 per patient-year15,17. These costs are expected to rise further with increasing life expectancy and the growing incidence of incidentally detected IPMN resulting from more widespread use of cross-sectional imaging.
Beyond economic implications, excessive surveillance imposes a psychological burden. Overactive management exposes patients to repeated testing without clear medical benefit14,15,23. Prospective studies have shown that patients undergoing long-term surveillance for stable, low-risk IPMN may experience increased somatization, depression, and anxiety, despite minimal objective risk of malignant progression, and in some cases greater psychological distress than patients who undergo surgical resection24.
During a total of 1,661 patient-years of radiological surveillance, only one case of PDAC was observed, corresponding to an incidence of 0.06% per patient-year. This rate is lower than those reported in some previous studies, such as Ideno et al.,20, and Han et al.,14, and is similar to rates described by McGuigan et al.,17. Possible explanations include differences in cohort composition, case selection, and ethnic variability between Asian and Western populations14.
This study is limited by its retrospective design and single-center setting, which may affect generalizability. However, its strengths include a large, well-characterized cohort, extended follow-up, and direct comparison between real-life clinical decisions and guideline-based recommendations.
In conclusion, this real-world analysis demonstrates that the majority of patients with SB-IPMN are managed more aggressively than recommended by current Kyoto guidelines, without clear clinical benefit. Over-surveillance is particularly common among younger patients and those with small, stable cysts, contributing to unnecessary healthcare utilization and patient distress. Given the increasing complexity of IPMN guidelines, particularly the cumulative weighting of worrisome features in the Kyoto framework, validated algorithm-based decision-support tools may help standardize care, reduce unnecessary imaging, improve cost-effectiveness, and support clinicians in navigating increasingly nuanced surveillance algorithms.
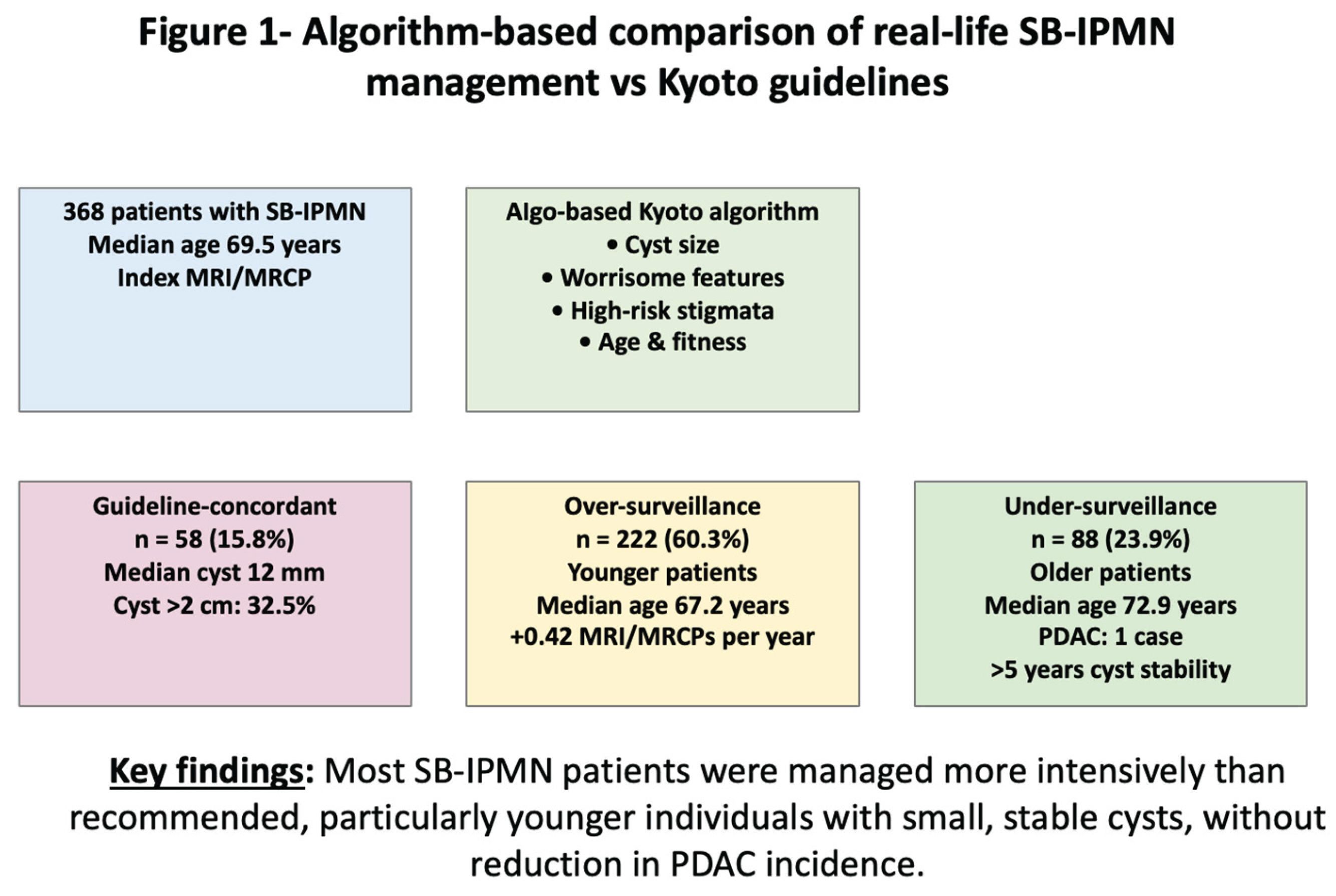
Figure 1.
Algorithm-based comparation of real.life SB-IPMN management vs. Kyoto guidelines.
Author Contributions
Roie Tzadok, MD- Conceptualization and study design, data collection, statistical analysis, interpretation of results, and manuscript drafting. Rivka Kessner, MD- Conceptual and scientific guidance, supervision of data collection, and final critical revision of the manuscript.Omer Ben-Ami Sher, PhD Decision-support tool (AIgo) development and implemented on a web-based platform. Hila Yashar, MD - Data collection and contribution to the results section. Sapir Lazar, MD- Data collection and critical revision of the manuscript. Yuval Katz, MD- Data collection and critical revision of the manuscript. Zur Ronen-Amsalem, MD- Data collection and critical revision of the manuscript. Arthur Chernomorets, MD- Data collection and critical revision of the manuscript.Dana Ben-Ami Shor, MD- Conceptualization and study design, data collection, statistical analysis, interpretation of results, and manuscript drafting. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
All authors have no conflicts of interest or financial disclosures to declare.
References
- Gonda, TA; Cahen, DL; Farrell, JJ. Pancreatic Cysts. N Engl J Med 2024, 391(9), 832–843. [Google Scholar] [CrossRef] [PubMed]
- Baiocchi, GL; Molfino, S; Frittoli, B; et al. Increased risk of second malignancy in pancreatic intraductal papillary mucinous tumors: Review of the literature. World J Gastroenterol 2015, 21(23), 7313–9. [Google Scholar] [CrossRef] [PubMed]
- Marchegiani, G; Pollini, T; Burelli, A; et al. Surveillance for Presumed BD-IPMN of the Pancreas: Stability, Size, and Age Identify Targets for Discontinuation. Gastroenterology 2023, 165(4), 1016–1024.e5. [Google Scholar] [CrossRef] [PubMed]
- Jang, JY; Park, T; Lee, S; et al. Proposed Nomogram Predicting the Individual Risk of Malignancy in the Patients With Branch Duct Type Intraductal Papillary Mucinous Neoplasms of the Pancreas. Ann Surg. 2017, 266(6), 1062–1068. [Google Scholar] [CrossRef]
- Elta, GH; Enestvedt, BK; Sauer, BG; Lennon, AM. ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts. Am J Gastroenterol 2018, 113(4), 464–479. [Google Scholar] [CrossRef]
- Chai, L; Zhu, N; Wang, Q; Wang, T; Chai, W. Assessment of Malignancy Potential in Intraductal Papillary Mucinous Neoplasms of the Pancreas on MDCT. Acad Radiol 2021, 28(5), 679–686. [Google Scholar] [CrossRef]
- Tanaka, M; Fernández-Del Castillo, C; Kamisawa, T; et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology 2017, 17(5), 738–753. [Google Scholar] [CrossRef]
- Ohtsuka, T; Fernandez-Del Castillo, C; Furukawa, T; et al. International evidence-based Kyoto guidelines for the management of intraductal papillary mucinous neoplasm of the pancreas. Pancreatology 2024, 24(2), 255–270. [Google Scholar] [CrossRef]
- Aziz, H; Acher, AW; Krishna, SG; Cloyd, JM; Pawlik, TM. Comparison of Society Guidelines for the Management and Surveillance of Pancreatic Cysts: A Review. JAMA Surg 2022, 157(8), 723–730. [Google Scholar] [CrossRef]
- Tashiro, Y; Kachi, M; Hashimoto, T; et al. Understanding intraductal papillary mucinous neoplasm from pathogenesis to risk assessment: a pictorial review based on the kyoto guidelines. In Abdom Radiol (NY); 16 Jun 2025. [Google Scholar] [CrossRef]
- Rahmatullah, ZF; Nia, IY; Afghani, E; Zaheer, A. Exploring the new Kyoto guidelines for managing pancreatic cysts: an overview and comparison with previous guidelines. Abdom Radiol (NY) 2025, 50(6), 2660–2675. [Google Scholar] [CrossRef]
- de la Fuente, J; Chatterjee, A; Lui, J; et al. Long-Term Outcomes and Risk of Pancreatic Cancer in Intraductal Papillary Mucinous Neoplasms. JAMA Network Open 2023, 6(10), e2337799–e2337799. [Google Scholar] [CrossRef] [PubMed]
- Ricci, C; Migliori, M; Imbrogno, A; et al. Prevalence of Asymptomatic Intraductal Papillary Mucinous Neoplasms in Healthy and Ill Populations Detected by Ultrasonography: A Single-Center Study of 6353 Outpatients. Pancreas 2019, 48(1), 113–120. [Google Scholar] [CrossRef] [PubMed]
- Han, Y; Kwon, W; Lee, M; et al. Optimal Surveillance Interval of Branch Duct Intraductal Papillary Mucinous Neoplasm of the Pancreas. JAMA Surg. 2024, 159(4), 389–396. [Google Scholar] [CrossRef] [PubMed]
- Kazmi, SZ; Jung, HS; Han, Y; et al. Systematic review on surveillance for non-resected branch-duct intraductal papillary mucinous neoplasms of the pancreas. Pancreatology 2024, 24(3), 463–488. [Google Scholar] [CrossRef]
- Fong, ZV; Hernandez-Barco, YG; Castillo, CF. A Clinical Guide to the Management of Intraductal Papillary Mucinous Neoplasms: the Need for a More Graded Approach in Clinical Decision-making. J Gastrointest Surg 2023, 27(9), 1988–1998. [Google Scholar] [CrossRef]
- McGuigan, MC; Hadjicosti, R; Cameron, AJ; et al. The Surveillance Strategy for Intraductal Pancreatic Mucinous Neoplasms: Criteria for Discontinuation. Ann Surg 2024. [Google Scholar] [CrossRef]
- Sahora, K; Ferrone, CR; Brugge, WR; et al. Effects of Comorbidities on Outcomes of Patients With Intraductal Papillary Mucinous Neoplasms. Clin Gastroenterol Hepatol 2015, 13(10), 1816–23. [Google Scholar] [CrossRef]
- Chhoda, A; Yousaf, MN; Madhani, K; et al. Comorbidities Drive the Majority of Overall Mortality in Low-Risk Mucinous Pancreatic Cysts Under Surveillance. Clin Gastroenterol Hepatol 2022, 20(3), 631–640.e1. [Google Scholar] [CrossRef]
- Ideno, N; Nakata, K; Abe, T; Watanabe, Y; Ikenaga, N; Nakamura, M. Systematic Review on Different Values of Surveillance by Age in Branch Duct Intraductal Papillary Mucinous Neoplasms of the Pancreas. J Hepatobiliary Pancreat Sci 2025. [Google Scholar] [CrossRef]
- Liu, Z; Pu, X; Cao, L. Assessing Follow-Up Duration in Intraductal Papillary Mucinous Neoplasm Patients. Med Sci Monit 2025, 31, e947810. [Google Scholar] [CrossRef]
- Girometti, R; Pravisani, R; Intini, SG; et al. Evolution of incidental branch-duct intraductal papillary mucinous neoplasms of the pancreas: A study with magnetic resonance imaging cholangiopancreatography. World J Gastroenterol 2016, 22(43), 9562–9570. [Google Scholar] [CrossRef]
- Petrov, MS. When to Stop Surveillance: Pancreatic Cysts. Am J Gastroenterol 2023, 118(3), 440–442. [Google Scholar] [CrossRef]
- Marinelli, V; Secchettin, E; Andrianello, S; et al. Psychological distress in patients under surveillance for intraductal papillary mucinous neoplasms of the pancreas: The "Sword of Damocles" effect calls for an integrated medical and psychological approach a prospective analysis. Pancreatology 2020, 20(3), 505–510. [Google Scholar] [CrossRef]

Table 1.
Baseline demographic and clinical characteristics of the study cohort.
| Characteristic | Overall Cohort (n = 368) |
|---|---|
| Age, years, median (IQR) | 69.5 (63.2–75.2) |
| Male sex, n (%) | 254 (69.0) |
| Radiological follow-up, months, median (IQR) | 48.5 (28–75) |
| Clinical follow-up, months, median (IQR) | 64 (46–88) |
| Side-branch IPMN, n (%) | 368 (100) |
| Leading cyst size, mm, mean ± SD | 11 ± 6.5 |
| Leading cyst size, mm, median (IQR) | 10 (10–14) |
| Multiple cysts at baseline, n (%) | 39 (10.5) |
Table 2.
Clinical management strategies and factors associated with guideline adherence.
| Variable | Guideline-Concordant | Non-Concordant | p Value |
|---|---|---|---|
| Number of patients, n (%) | 58 (15.8) | 310 (84.2) | |
| Cyst size >20 mm, % | 32.5 | 16.8 | 0.008 |
| Leading cyst size, mm, median (IQR) | 12 (10–19) | 10 (10–14) | 0.006 |
| Age, years, median (IQR) | 69.5 (62.9–75.4) | 70.4 (64.8–74.4) | 0.756 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



