Submitted:
29 December 2025
Posted:
30 December 2025
You are already at the latest version
Abstract
Background/Objectives: Stable graft fixation is a key determinant for predictable guided bone regeneration (GBR) performed simultaneously with implant placement. Titanium tacks are commonly used for graft and membrane stabilization but require additional hardware and may necessitate removal at re-entry. Periosteal mattress sutures have been proposed as a hardware-free alternative; however, clinical evidence comparing both ap-proaches remains limited. The objective of this randomized clinical trial was to compare postoperative buccal bone dimensions following horizontal GBR in the aesthetic zone us-ing periosteal mattress sutures versus titanium tacks for graft stabilization. Methods: This pilot randomized controlled clinical trial included patients requiring horizontal GBR with simultaneous implant placement in the anterior maxilla. Participants were randomly al-located to graft stabilization using either periosteal mattress sutures (S) or titanium tacks (T). In all cases, a composite xenogeneic collagenated bovine block graft was applied and covered with a resorbable collagen membrane, followed by tension-free flap closure. Cone-beam computed tomography (CBCT) was obtained after 6 months. Buccal bone thickness was measured at 1, 3, and 6 mm apical to the implant platform. Mean buccal bone thickness and reconstructed buccal bone area between 1 and 6 mm were calculated and compared between groups. Results: Thirty implants were included in the final analy-sis (S, n = 16; T, n = 14). Mean buccal bone thickness was 1.16 ± 1.01 mm in the periosteal suture group and 1.23 ± 1.16 mm in the titanium tack group, with no statistically signifi-cant differences between groups. No significant intergroup differences were observed at any individual measurement level or in the reconstructed buccal bone area. Conclusions: Within the limitations of this pilot trial, periosteal mattress sutures provided buccal bone regeneration outcomes comparable to titanium tacks during GBR with simultaneous im-plant placement. Periosteal suturing may represent a reliable hardware-free alternative for graft stabilization in horizontal ridge augmentation.
Keywords:
guided bone regeneration
; graft stabilization
; periosteal mattress sutures
; titanium tacks
; buccal bone thickness
1. Introduction
Guided bone regeneration depends on two fundamental biological conditions: 1. the creation of a stable compartment that protects the graft during early healing, and 2. the achievement of a tension-free soft-tissue closure capable of preserving that compartment throughout the regenerative phase [1,2]. To address these requirements, several surgical refinements have been introduced. Periosteal-releasing approaches, for example, enable controlled coronal advancement of the buccal flap while preserving its vascular supply, thereby facilitating tension-free primary closure and reducing the risk of membrane exposure [3]. Our group has previously standardized and reported one such technique, offering a reproducible method for flap advancement in sites with significant buccolingual atrophy [4].
A second key determinant of predictable augmentation is graft stabilization. Preclinical studies have demonstrated that membrane fixation enhances GBR outcomes by improving space maintenance and limiting graft micromotion, thereby promoting more favorable conditions for new bone formation [5,6]. Traditional fixation using titanium tacks or screws provides rigid immobilization but requires additional surgical steps and often necessitates hardware removal at re-entry. As a less invasive alternative, periosteal mattress suturing has been proposed as a hardware-free fixation method that stabilizes particulate or block grafts beneath the membrane through apical and lateral anchorage [7]. This technique has been shown to integrate efficiently into the workflow of lateral ridge augmentation [8].
Beyond flap management and fixation strategies, the biological characteristics of the graft material also play a central role in treatment predictability. Composite bone grafts such as xenogeneic blocks composed of deproteinized bovine mineral integrated within a collagen matrix offer both structural and handling advantages. The mineralized component provides a stable three-dimensional scaffold for new bone formation, while the collagen matrix enhances adaptability and facilitates intimate contact with the recipient site. This combination generates a malleable yet volumetrically stable graft that can support the regenerative process in lateral defects [9,10,11].
Because these three elements, adequate soft-tissue release, hardware-free graft stabilization, and composite graft materials address complementary aspects of the regenerative environment, their combined application may provide a biologically coherent alternative to titanium-tack fixation. The objective of the present study was therefore to compare postoperative buccal bone dimensions after implant placement between sites stabilized with titanium tacks and those stabilized with periosteal sutures.
2. Materials and Methods
2.1. Participants
All study procedures were conducted under approval of the Scientific Ethics Committee of the Servicio de Salud Aconcagua (CEC-SSA 19/2021) and in accordance with national regulations. Patients were consecutively recruited from the Periodontics Clinic of Hospital San Camilo, where individuals seeking implant therapy in the anterior maxilla were screened for eligibility. Those requiring simultaneous guided bone regeneration at the time of implant placement were evaluated by the clinical team, and candidates meeting the inclusion criteria were invited to participate. A trained investigator not involved in the surgical treatment provided verbal and written information regarding the study objectives and procedures, obtained written informed consent in the presence of an authorized witness, and ensured that participation was voluntary and could be discontinued at any time.
A total of 46 patients seeking implant therapy in the anterior maxilla were assessed for eligibility. Of these, 6 patients were excluded prior to enrollment due to uncontrolled diabetes (n = 4) or ongoing bisphosphonate therapy (n = 2). The remaining 40 patients met the inclusion criteria, provided informed consent, and were randomized. Nineteen patients were allocated to the suture fixation group, of whom 17 received the allocated intervention, while 2 declined treatment. Twenty-one patients were allocated to the titanium tack fixation group, of whom 20 received the allocated intervention and 1 declined treatment. During the follow-up period, in the tack fixation group, 3 patients were lost to follow-up after declining continued participation and abandoning treatment, and 1 implant failure was recorded, resulting in 16 patients completing the six-month follow-up. In the suture fixation group, 1 patient was lost to follow-up after declining continued participation, and 16 patients completed follow-up. For radiographic analysis, 2 cases in the tack fixation group were excluded due to radiographic artifacts, resulting in 14 implants analyzed in this group, whereas all 16 cases in the suture fixation group were included in the final analysis. The overall flow of participants through enrollment, allocation, follow-up, and analysis is summarized in the CONSORT diagram shown in Figure 1.
A full clinical and radiographic baseline examination was performed following consent. This included a cone-beam computed tomography scan (CBCT) obtained at an external radiology facility, as well as digital impressions.
Implant surgeries were performed by an experienced periodontist using a standardized approach, and guided bone regeneration was carried out simultaneously with implant placement. The postoperative course was uneventful for all participants, with no adverse events observed during early healing. Follow-up visits were scheduled at 7 and 14 days to assess soft tissue healing and remove sutures as appropriate, and an additional evaluation was performed at approximately four weeks, consistent with the institutional protocol for implant patients. Long-term healing was assessed at six months, at which time a second CBCT scan and digital impressions were obtained to allow quantitative and qualitative evaluation of the regenerated tissues.
All clinical data were collected by a calibrated periodontist who was not involved in the surgical procedures.
2.2. Study Design and Surgical Procedures
This study evaluated the dimensional characteristics of the buccal bone contour following implant placement and guided bone regeneration (GBR). All implants were placed in healed ridges following standard surgical protocols. Buccal augmentation was performed using a xenogeneic composite block graft of bovine origin, consisting of deproteinized bone particles embedded in a collagen matrix (InterOss® Collagen Block, Sigmagraft). The block graft was shaped to the recipient site and positioned to restore the buccolingual contour and then covered by a resorbable collagen membrane (InterCollagen® Guide, Sigmagraft).
Two different graft-stabilization approaches were compared following horizontal guided bone regeneration. In one group (T), the composite bovine block graft was secured using titanium tacks (Titan pin set®, Botiss). In the second group (S), the graft was stabilized using the periosteal mattress suture technique as described in detail elsewhere [8]. Briefly, this method employs vertically oriented periosteal sutures placed to immobilize the graft laterally, supplemented by a horizontal mattress suture extending between the flap edges to prevent apical displacement. A schematic illustration of both stabilization approaches is shown in Figure 2. The soft tissues were advanced and closed without tension. A healing period of six months was allowed before further evaluation.
2.3. Radiographic Acquisition and Measurement Protocol
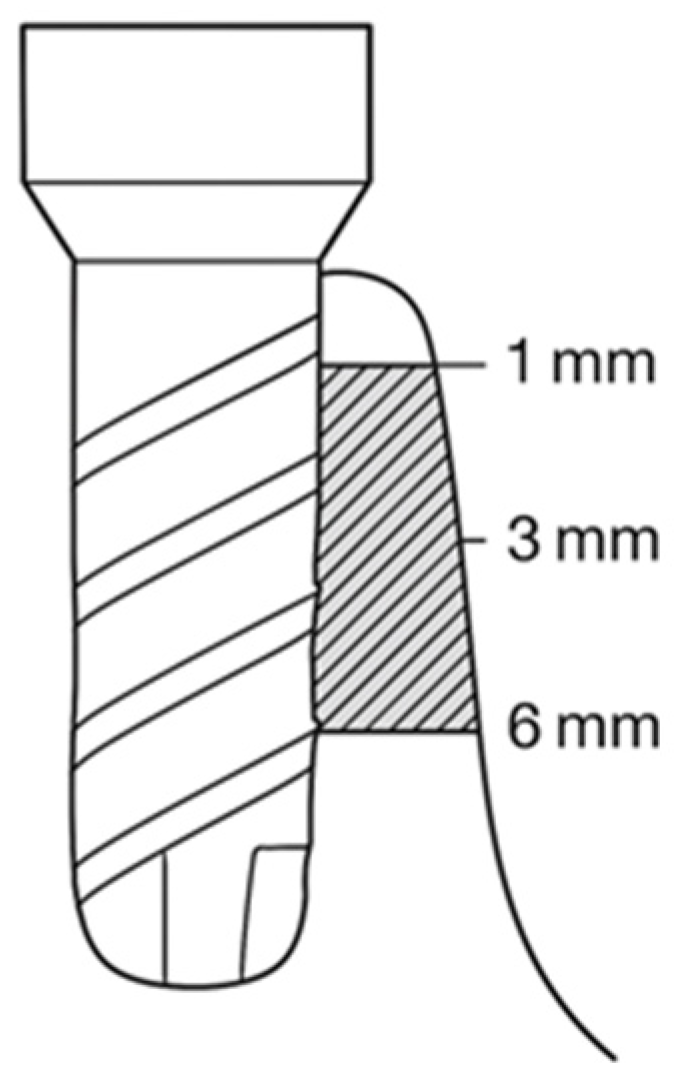
After six months, all participants underwent cone beam computed tomography (CBCT) using a standardized acquisition protocol. For each implant, three reference levels were identified: 1 mm, 3 mm, and 6 mm apical to the implant platform. At each of these levels, a perpendicular linear measurement was taken from the implant surface to the outer contour of the buccal bone. These measurements represented the horizontal bone thickness at each depth.
Implants were oriented in cross-sectional views to ensure a true buccolingual slice perpendicular to the long axis. All measurements were performed by a calibrated examiner using radiographic analysis software with a known spatial resolution (Blue Sky Plan® version 4.7.55, BlueSky Bio).
To integrate information across depths, the buccal bone contour between 1 mm and 6 mm was reconstructed using three coordinate pairs corresponding to the horizontal bone thickness at 1 mm, 3 mm, and 6 mm below the platform. These values were treated as points along the long axis of the implant. Between these points, linear interpolation was used to construct a piecewise linear approximation of the buccal bone surface. The bone area covering the implant between 1 and 6 mm was then computed as the sum of two trapezoidal regions bounded by the implant surface (vertical reference line), the interpolated bone contour, and the perpendicular lines at 1 mm, 3 mm, and 6 mm. This generated a reproducible quantitative metric representing the buccal bone envelope in the augmented region (Figure 3).
Figure 3.
Buccal bone profile and calculated bone area derived from CBCT measurements at 1, 3, and 6 mm.
Figure 3.
Buccal bone profile and calculated bone area derived from CBCT measurements at 1, 3, and 6 mm.
2.4. Statistical Analysis
All statistical procedures were carried out using Python 3.11. Data organization and preliminary processing were conducted with the pandas library, numerical computations with numpy, and inferential testing with the scipy.stats module. Graphical evaluations of distributional patterns and internal verification steps were performed with matplotlib.
For each subject, horizontal bone measurements obtained at 1 mm, 3 mm, and 6 mm below the implant platform were treated as independent quantitative variables. In addition, a derived metric representing the total buccal bone area between 1 mm and 6 mm — calculated through the geometric combination of two trapezoidal regions based on the measured thicknesses — was included as an outcome of interest. To complement these values, the mean bone thickness across the three reference depths was also computed for each implant, and this mean value was compared between the two groups.
The normality of each variable in group T and group S was evaluated through the Shapiro–Wilk test. When both groups met the assumptions of normality, intergroup comparisons were performed using an independent-samples t-test with Welch’s correction. When the assumption of normality was violated in either group, the Mann–Whitney U test was used instead. This analytical approach was applied to the measurements at 1 mm, 3 mm, and 6 mm, to the reconstructed bone area, and to the mean of the three linear measurements, allowing a comprehensive evaluation of potential differences in buccal bone morphology between the two groups. A two-tailed significance threshold of p < 0.05 was adopted for all analyses.
3. Results
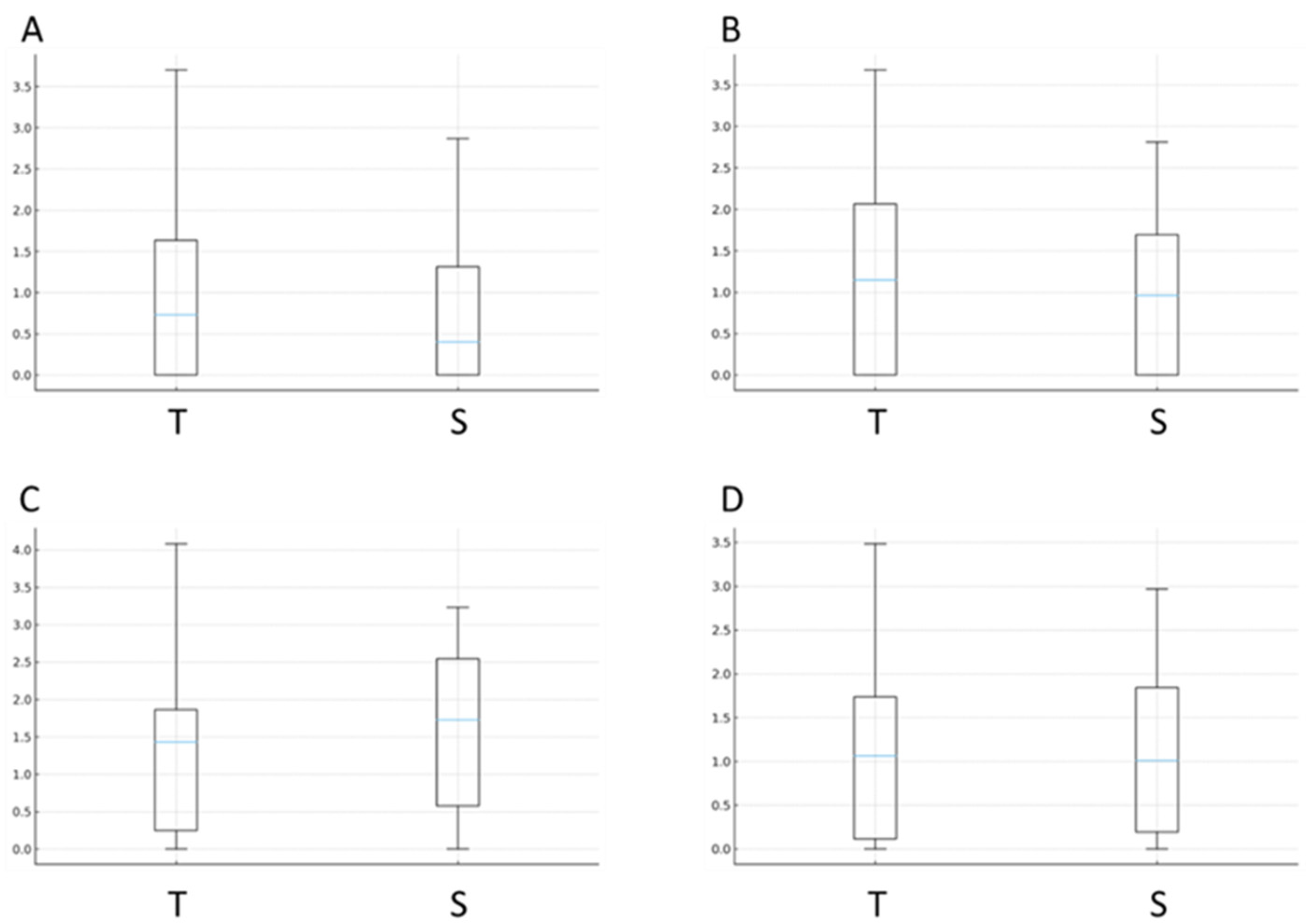
Descriptive statistics for all linear measurements, including horizontal bone thickness at 1 mm, 3 mm, and 6 mm below the implant platform as well as the mean thickness across these reference points, are presented in Table 1. The comparative analysis showed no statistically significant differences between group T and group S for any of the linear measurements. Both groups demonstrated similar central tendencies and overlapping dispersion ranges across all three depths, and the same pattern was observed when the combined mean thickness was evaluated (Figure 3).
Figure 3.
Boxplots illustrate horizontal buccal bone thickness (mm) at different reference levels around implants augmented with a bovine composite block graft and stabilized either with titanium tacks (T) or periosteal sutures (S). (A) Thickness measured 1 mm apical to the implant platform. (B) Thickness measured 3 mm apical to the platform. (C) Thickness measured 6 mm apical to the platform. (D) Mean buccal bone thickness calculated from the measurements at 1-, 3- and 6-mm. T = tacks group; S = sutures group.
Figure 3.
Boxplots illustrate horizontal buccal bone thickness (mm) at different reference levels around implants augmented with a bovine composite block graft and stabilized either with titanium tacks (T) or periosteal sutures (S). (A) Thickness measured 1 mm apical to the implant platform. (B) Thickness measured 3 mm apical to the platform. (C) Thickness measured 6 mm apical to the platform. (D) Mean buccal bone thickness calculated from the measurements at 1-, 3- and 6-mm. T = tacks group; S = sutures group.
The reconstructed buccal bone area calculated between 1 mm and 6 mm, derived from the trapezoidal integration of the horizontal measurements, also showed no significant differences between groups. The distributions of area values were broadly comparable, reflecting similar postoperative buccal bone envelopes regardless of stabilization method. These results are presented in Figure 4, which displays the boxplot of the total area for the two groups.
4. Discussion
The present RCT showed that periosteal mattress sutures achieved buccal bone regeneration outcomes similar to titanium tacks when used to stabilize a composite xenogeneic block graft during simultaneous implant placement. Horizontal bone thickness at 1 mm, 3 mm, and 6 mm below the implant platform, as well as the reconstructed buccal bone area between these levels, showed no significant differences between groups.
These findings indicate that, under controlled surgical conditions and when combined with appropriate flap management, suture-based stabilization may maintain the regenerative compartment as effectively as conventional hardware fixation. This observation is consistent with previous reports suggesting that the mechanical stability required for guided bone regeneration can be achieved without rigid fixation devices [12].
The present findings might be explained by the following reasons. Titanium tacks are traditionally used to immobilize grafts and membranes, reducing micromotion and preserving the augmented space during early healing. However, stable flap closure and adequate soft-tissue adaptation are also critical contributors to compartment maintenance. Periosteal mattress suturing aims to reproduce the stabilizing effect of rigid fixation by anchoring the graft and membrane apically and laterally, thereby restricting displacement while avoiding the need for a second surgical intervention for hardware removal. Previous descriptions of periosteal sutures have highlighted their potential to provide hardware-free stabilization in lateral ridge augmentation, and the present results add quantitative radiographic evidence supporting their clinical utility.
The use of a composite xenogeneic block graft, consisting of deproteinized bovine mineral integrated within a collagen matrix, may also have contributed to the comparable outcomes observed in both groups. Composite grafts possess inherent structural cohesiveness, allowing them to better maintain volumetric stability even in the absence of rigid fixation [13]. Their collagen component enhances adaptability to the defect morphology and facilitates early clot stabilization, which may reduce the mechanical demands placed on the fixation method itself. Previous studies have reported that such composite materials may withstand functional and soft-tissue pressures more predictably than particulate grafts [9,10], suggesting that when using this type of biomaterial, the difference between fixation techniques may be less pronounced.
From a clinical perspective, these findings have several important implications. First, hardware-free stabilization simplifies the surgical procedure, avoids potential complications associated with tack placement, and eliminates the need for retrieval at re-entry. These advantages may be particularly relevant in settings where patient factors, anatomical constraints or surgical expertise limit the feasibility of using fixation devices. Second, the ability to achieve comparable outcomes with sutures alone may lower the cost of care and improve accessibility to regenerative procedures in resource-limited environments.
An additional observation was that buccal bone thickness at 1 mm below the implant platform tended to be lower than at deeper levels. This pattern is consistent with previous reports describing remodeling in the crestal region following augmentation. This phenomenon is commonly attributed to early remodeling dynamics and to the mechanical influence from the peri-implant soft tissues. Because this crestal zone is critical for long-term stability, insufficient buccal bone thickness in this area may increase susceptibility to surface remodeling potentially resulting in mucosal recessions [14] and biological complications such as bleeding on probing [15].
To address these possible complications, alternative augmentation strategies have been proposed, including the so-called L-shape grafting approach [11]. In this technique a composite block is intentionally shaped to extend coronally over the implant platform, thereby reinforcing the most vulnerable portion of the buccal aspect [11,13,16]. This design aims to compensate for anticipated crestal remodeling and to provide a more protective envelope for the peri-implant soft tissues. Given that the present findings showed similar regenerative outcomes between periosteal sutures and titanium tacks, future studies should explore whether the L-shape technique could be combined suture-based stabilization, while preserving the advantages of a hardware-free approach.
The present study has limitations. The sample size was modest and while sufficient to detect large differences between groups, it may not have captured more subtle effects. All procedures were performed by a single experienced operator; nevertheless, an inherent learning curve related to the surgical technique may exist and should be considered when interpreting the results. All the measurements were limited to six months. Although this time-point reflects early functional stability of the regenerated bone, longer-term follow-up is necessary to assess remodeling behavior under functional loading.
5. Conclusions
Periosteal mattress sutures used for graft stabilization during guided bone regeneration with simultaneous implant placement resulted in radiographic buccal bone dimensions at 6 months comparable to those achieved with titanium tacks. Periosteal mattress sutures represent a viable alternative to titanium tacks that may simplify GBR procedures.
Author Contributions
Conceptualization, P.N. and F.C.; methodology, P.N., X.M., Y.C., F.M. and F.C.; software, F.M. and F.C.; validation, F.S.; formal analysis, F.M., F.S. and F.C.; investigation, P.N., X.M., Y.C. and F.C.; resources, F.C.; data curation, F.C.; writing—original draft preparation, F.C.; writing—review and editing, F.S. and F.C.; visualization, F.C.; supervision, F.C.; project administration, F.C.; funding acquisition, F.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Scientific Ethics Committee of the Servicio de Salud Aconcagua (CEC-SSA 19/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data supporting the findings of this study are not publicly available due to patient confidentiality and legal and ethical restrictions. However, the datasets generated and analyzed during the current study are available from the corresponding author (F.C.) upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Jepsen, S; Schwarz, F; Cordaro, L; Derks, J; Hämmerle, CHF; Heitz-Mayfield, LJ; Hernández-Alfaro, F; Meijer, HJA; Naenni, N; Ortiz Vigón, A; Pjetursson, B; Raghoebar, GM; Renvert, S; Rocchietta, I; Roccuzzo, M; Sanz-Sánchez, I; Simion, M; Tomasi, C; Trombelli, L; Urban, I. Regeneration of alveolar ridge defects. Consensus report of group 4 of the 15th European Workshop on Periodontology on Bone Regeneration. J Clin Periodontol 2019, 46 Suppl 21, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Cucchi, A; Chierico, A; Fontana, F; Mazzocco, F; Cinquegrana, C; Belleggia, F; Rossetti, P; Soardi, CM; Todisco, M; Luongo, R; Signorini, L; Ronda, M; Pistilli, R. Statements and Recommendations for Guided Bone Regeneration: Consensus Report of the Guided Bone Regeneration Symposium Held in Bologna, October 15 to 16, 2016. Implant Dent. 2019, 28(4), 388–399. [Google Scholar] [CrossRef] [PubMed]
- Urban, IA; Montero, E; Amerio, E; Palombo, D; Monje, A. Techniques on vertical ridge augmentation: Indications and effectiveness. Periodontol 2000 2023, 93(1), 153–182. [Google Scholar] [CrossRef] [PubMed]
- Neira, P; Moreno, X; Caric, Y; Strauss, FJ; Cavalla, F. Two-Step Periosteal Releasing Incision for Tension-Free Flap Closure After Implant Placement With Simultaneous Guided Bone Regeneration. J Oral Implantol 2024, 50(4), 317–321. [Google Scholar] [CrossRef] [PubMed]
- Park, JY; Song, YW; Ko, KA; Strauss, FJ; Thoma, DS; Lee, JS. Effect of collagen membrane fixation on ridge volume stability and new bone formation following guided bone regeneration. J Clin Periodontol 2022, 49(7), 684–693. [Google Scholar] [CrossRef] [PubMed]
- An, YZ; Strauss, FJ; Park, JY; Shen, YQ; Thoma, DS; Lee, JS. Membrane fixation enhances guided bone regeneration in standardized calvarial defects: A pre-clinical study. J Clin Periodontol 2022, 49(2), 177–187. [Google Scholar] [CrossRef] [PubMed]
- Urban, IA; Lozada, JL; Wessing, B; Suárez-López del Amo, F; Wang, HL. Vertical Bone Grafting and Periosteal Vertical Mattress Suture for the Fixation of Resorbable Membranes and Stabilization of Particulate Grafts in Horizontal Guided Bone Regeneration to Achieve More Predictable Results: A Technical Report. Int J Periodontics Restorative Dent 2016, 36(2), 153–9. [Google Scholar] [CrossRef] [PubMed]
- Moreno, X; Neira, P; Mandakovic, D; Strauss, FJ; Cavalla, F. Pilot Study: Periosteal Mattress Sutures as an Alternative to Pins and Screws in Guided Bone Regeneration in the Esthetic Zone. Int J Periodontics Restorative Dent. 2023, (7), s217–s226. [Google Scholar] [CrossRef] [PubMed]
- Romito, GA; Villar, CC; Sapata, VM; Soares, HH; Fonseca, MA; Conde, M; Hammerle, CHF; Schwarz, F. Autogenous bone block versus collagenated xenogeneic bone block in the reconstruction of the atrophic alveolar ridge: A non-inferiority randomized clinical trial. J Clin Periodontol 2022, 49(11), 1158–1168. [Google Scholar] [CrossRef] [PubMed]
- Romito, GA; Soares, HH; do Amaral, GCLS; Fonseca, MA; Sapata, VM; Conde, MC; Hammerle, CHF; Schwarz, F; Villar, CC. Radiographic outcomes of ridge reconstruction with autogenous bone block versus collagenated xenogeneic bone block: A randomized clinical trial. Clin Oral Implants Res. 2023, 34(8), 863–871. [Google Scholar] [CrossRef]
- Zuercher, AN; Mancini, L; Naenni, N; Thoma, DS; Strauss, FJ; Jung, RE. The L-shape technique in guided bone regeneration with simultaneous implant placement in the esthetic zone: A step-by-step protocol and a 2-14 year retrospective study. J Esthet Restor Dent. 2023, 35(1), 197–205. [Google Scholar] [CrossRef] [PubMed]
- Johnson, TM; Vargas, SM; Wagner, JC; Lincicum, AR; Stancoven, BW; Lancaster, DD. The Triangle Suture for Membrane Fixation in Guided Bone Regeneration Procedures: A Report of Two Cases. Clin Adv Periodontics 2022, 12(3), 186–193. [Google Scholar] [CrossRef] [PubMed]
- Jung, EH; Jeong, SN; Lee, JH. Augmentation stability and early wound healing outcomes of guided bone regeneration in peri-implant dehiscence defects with L- and I-shaped soft block bone substitutes: A clinical and radiographic study. Clin Oral Implants Res. 2021, 32(11), 1308–1317. [Google Scholar] [CrossRef] [PubMed]
- Monje, A; Roccuzzo, A; Buser, D; Wang, HL. Influence of buccal bone wall thickness on the peri-implant hard and soft tissue dimensional changes: A systematic review. Clin Oral Implants Res. 2023, 34(3), 157–176. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F; Sahm, N; Becker, J. Impact of the outcome of guided bone regeneration in dehiscence-type defects on the long-term stability of peri-implant health: clinical observations at 4 years. Clin Oral Implants Res 2012, 23(2), 191–196. [Google Scholar] [CrossRef] [PubMed]
- Lee, JH; Jung, EH; Jeong, SN. Augmentation Stability of Guided Bone Regeneration for Peri-Implant Dehiscence Defects with L-shaped Porcine-Derived Block Bone Substitute. Materials (Basel) 2021, 14(21), 6580. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Consort diagram.
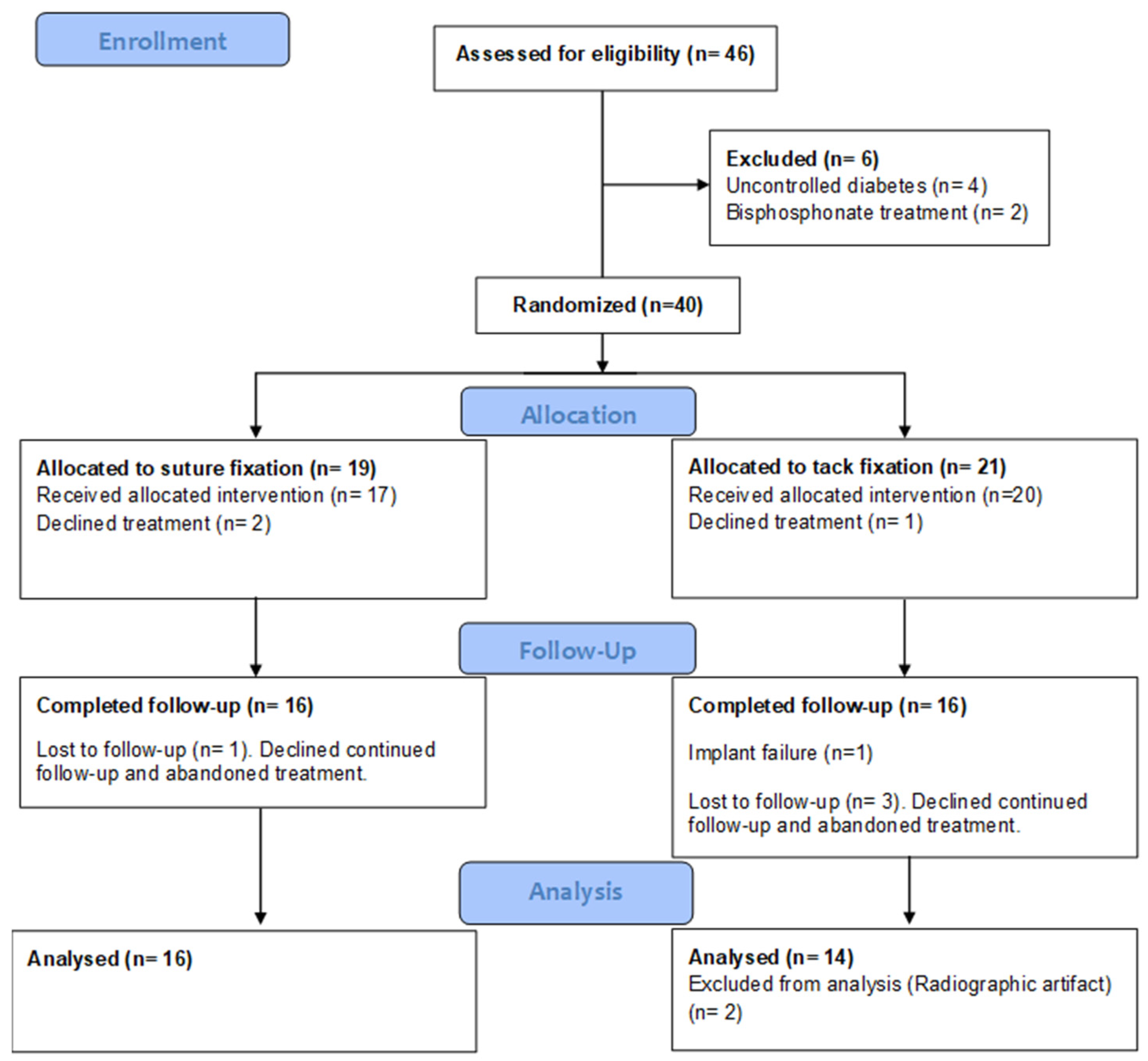
Figure 2.
Schematic illustration of the two graft stabilization approaches used in guided bone regeneration: (A) titanium tacks and (B) periosteal mattress sutures.
Figure 2.
Schematic illustration of the two graft stabilization approaches used in guided bone regeneration: (A) titanium tacks and (B) periosteal mattress sutures.
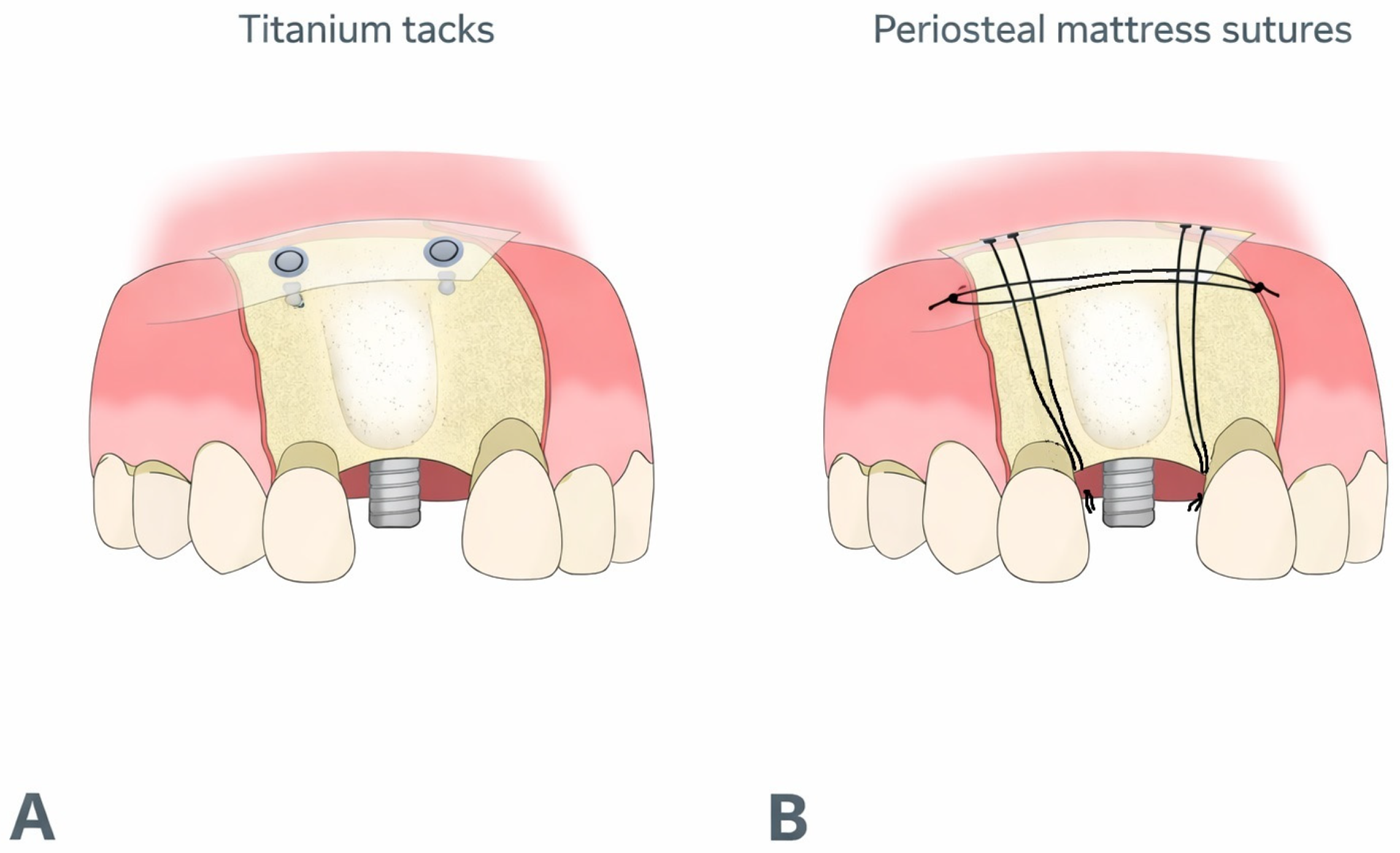
Figure 4.
Boxplot comparison of the reconstructed buccal bone area (1–6 mm) for implants augmented with a bovine composite block graft and stabilized either with titanium tacks (T) or periosteal sutures (S). The area represents the integrated bone contour derived from the horizontal measurements at 1, 3, and 6 mm below the implant platform.
Figure 4.
Boxplot comparison of the reconstructed buccal bone area (1–6 mm) for implants augmented with a bovine composite block graft and stabilized either with titanium tacks (T) or periosteal sutures (S). The area represents the integrated bone contour derived from the horizontal measurements at 1, 3, and 6 mm below the implant platform.
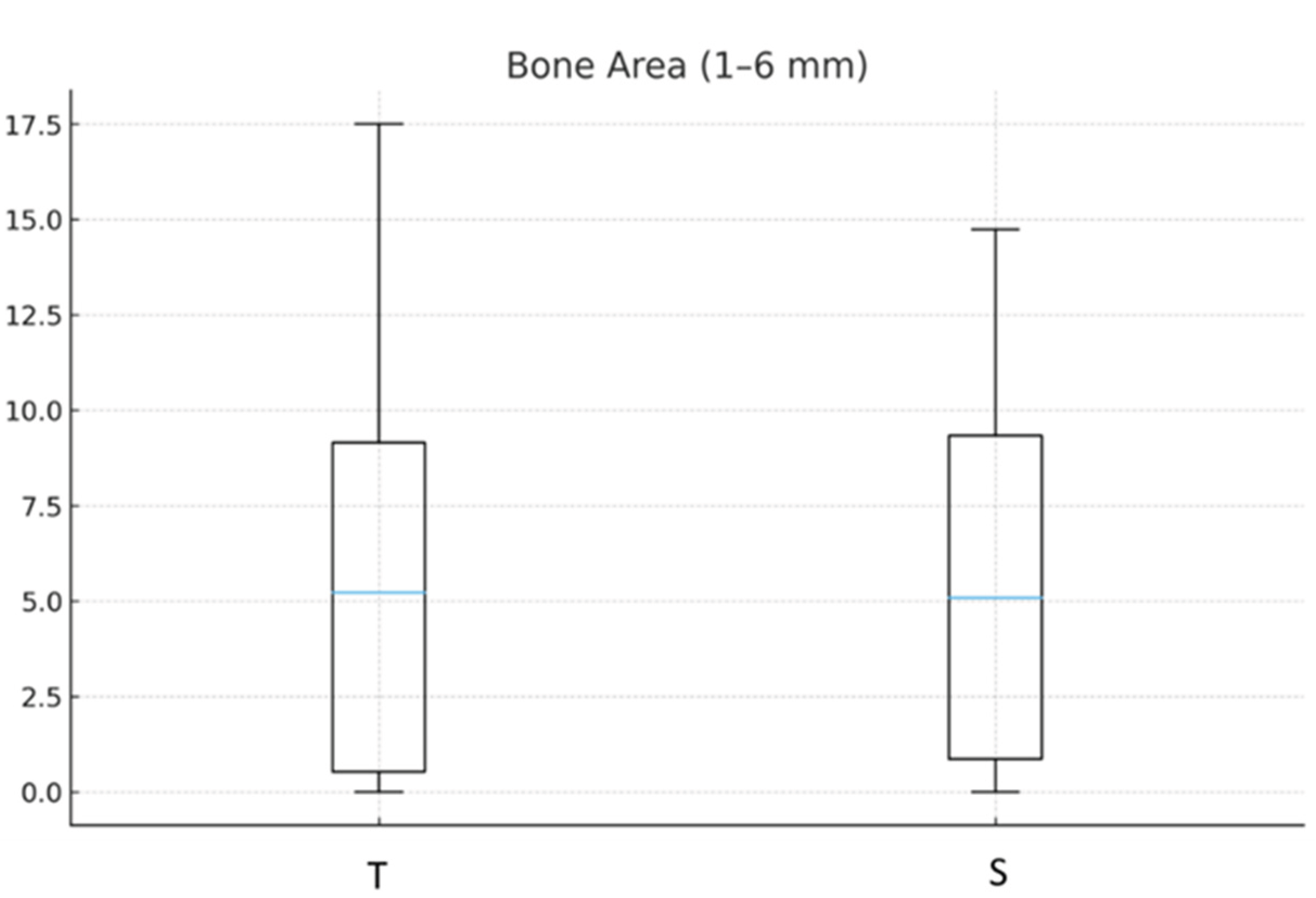

Table 1.
Descriptive statistics of horizontal buccal bone thickness at 1 mm, 3 mm, and 6 mm below the implant platform, and of the mean thickness across these levels, for both fixation groups. Values are presented as N, mean, standard deviation, median, and interquartile range (IQR).
Table 1.
Descriptive statistics of horizontal buccal bone thickness at 1 mm, 3 mm, and 6 mm below the implant platform, and of the mean thickness across these levels, for both fixation groups. Values are presented as N, mean, standard deviation, median, and interquartile range (IQR).
| Group | Variable | N | Mean (mm) | SD | Median (mm) | IQR |
|---|---|---|---|---|---|---|
| Sutures | 1 mm | 16 | 0.81 | 0.99 | 0.41 | 1.31 |
| 3 mm | 16 | 1.03 | 0.99 | 0.96 | 1.70 | |
| 6 mm | 16 | 1.62 | 1.20 | 1.73 | 1.97 | |
| Mean | 16 | 1.16 | 1.01 | 1.01 | 1.65 | |
| Tacks | 1 mm | 14 | 0.94 | 1.10 | 0.74 | 1.64 |
| 3 mm | 14 | 1.31 | 1.30 | 1.15 | 2.07 | |
| 6 mm | 14 | 1.45 | 1.26 | 1.43 | 1.62 | |
| Mean | 14 | 1.23 | 1.16 | 1.07 | 1.62 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



