
Submitted:
27 December 2025
Posted:
29 December 2025
You are already at the latest version
Abstract
Background:
We present our experience with the endovascular therapy (EVT) of a pseudo-aneurysm of the posterior tibial artery (PTA) with an associated arteriovenous fistula (AVF) and a systematic review was carried out to put a light on the EVT.
Methods:
A 31-year-old patient presented with pain in the lower leg with increasing severity and a history of war trauma. A CT-Angiogram confirmed an aneurysm of the PTA with an AVF. With a bidirectional endovascular approach, the aneurysm was occluded with Coils and excluded with a Viabahn Endoprosthesis. Aspirin and Clopidogrel were recommended postoperatively. After 18 months of follow-up, the patient is free of symptoms with patent endoprosthesis. Multiple databases (Scopus, Pubmed, Medline, OVID) were systematically searched with MeSH terms. The studies were scrutinized and data on demographics, procedural details, and follow-up was collected and pooled.
Results:
A total of 44 studies (56 patients) were eligible and included. Average age was 50 (15-87 years). The most common etiology was trauma (iatrogenic 29/56;51.7% and non-iatrogenic 15/56;26.7%). EVT strategies included coil-embolization (n=29), stent-implantation (n=25), and a combination of both (n= 2). Median stent diameter was 3mm (2.5–6). The follow-up period ranged from 1week-60 months. Primary Patency was 18/27 (66.6%) with no reported complications.
Conclusion:
EVT offers a feasible and safe alternative to simple ligation or occlusion of crural aneurysms to preserve distal flow to the foot. Dedicated stents for crural arteries are not available. Studies with long-term follow-up are lacking.
Keywords:
endovascular treatment
; crural aneurysms
; pseudoaneurysms
; anterior tibial artery
; posterior tibial artery
; tibioperoneal trunk
; peroneal artery
Introduction
Aneurysms of the crural arteries are a rare entity. The current literature reports a diverse etiology, with trauma being the most common inciting factor [1]. Trauma can be iatrogenic, e.g., following orthopedic surgery [2,3], vascular interventions such as balloon angioplasty, embolectomy [4], or after blunt [5] or penetrating non-iatrogenic trauma [6]. These aneurysms have also been reported in patients with connective tissue disorders like panarteritis nodosa [7], Ehlers-Danlos syndrome [8], and Behçet's disease [9], without any history of trauma. Infected mycotic aneurysms in patients with endocarditis have also been reported [10,11].
The characteristic symptomatology of crural aneurysms is pain, swelling, and/or a pulsatile mass in the lower leg [11,12]. Rarely, neurological symptoms such as paresthesia or foot drop caused by nerve compression [13], or rupture of the aneurysm with or without compartment syndrome [14,15], can be the presenting feature. In a few cases, the course of crural aneurysms is completely asymptomatic, and the diagnosis appears to be incidental [16,17].
The spectrum of treatment modalities encompasses conservative management, open surgical treatment [17], minimally invasive treatment with thrombin injection, and endovascular treatment [18]. EVT includes coiling of the aneurysm and/or the feeding vessel to occlude the aneurysm [19–22]. Alternatively, exclusion of the aneurysm with a stent graft offers the opportunity to preserve blood flow distal to the aneurysm [23–26].
Apart from reporting our experience with EVT of an aneurysm of the posterior tibial artery (PTA), the aim of this study was to systematically summarize the current literature regarding the EVT of crural aneurysms, focusing on the type of EVT, stent characteristics, patency, and reintervention rates.
Materials and Methods
Case Report
A 31-year-old man presented with calf pain in the right limb, which had gradually increased in severity over the past few months. The pain was throbbing in nature and not associated with walking. There was a history of war injury to his lower leg in the region of the pain. The patient reported being hit in the lower leg region with a bomb shrapnel. Physical examination revealed a pulsatile, tender mass in the mid-calf region. Duplex ultrasound revealed an aneurysm in the mid-calf region of the posterior tibial artery. To define the morphology of the aneurysm and the anatomy of the crural vessels, a CT angiogram was obtained. This confirmed the presence of an aneurysm of the PTA associated with an AV fistula to the deep posterior tibial veins (Fig. 1).
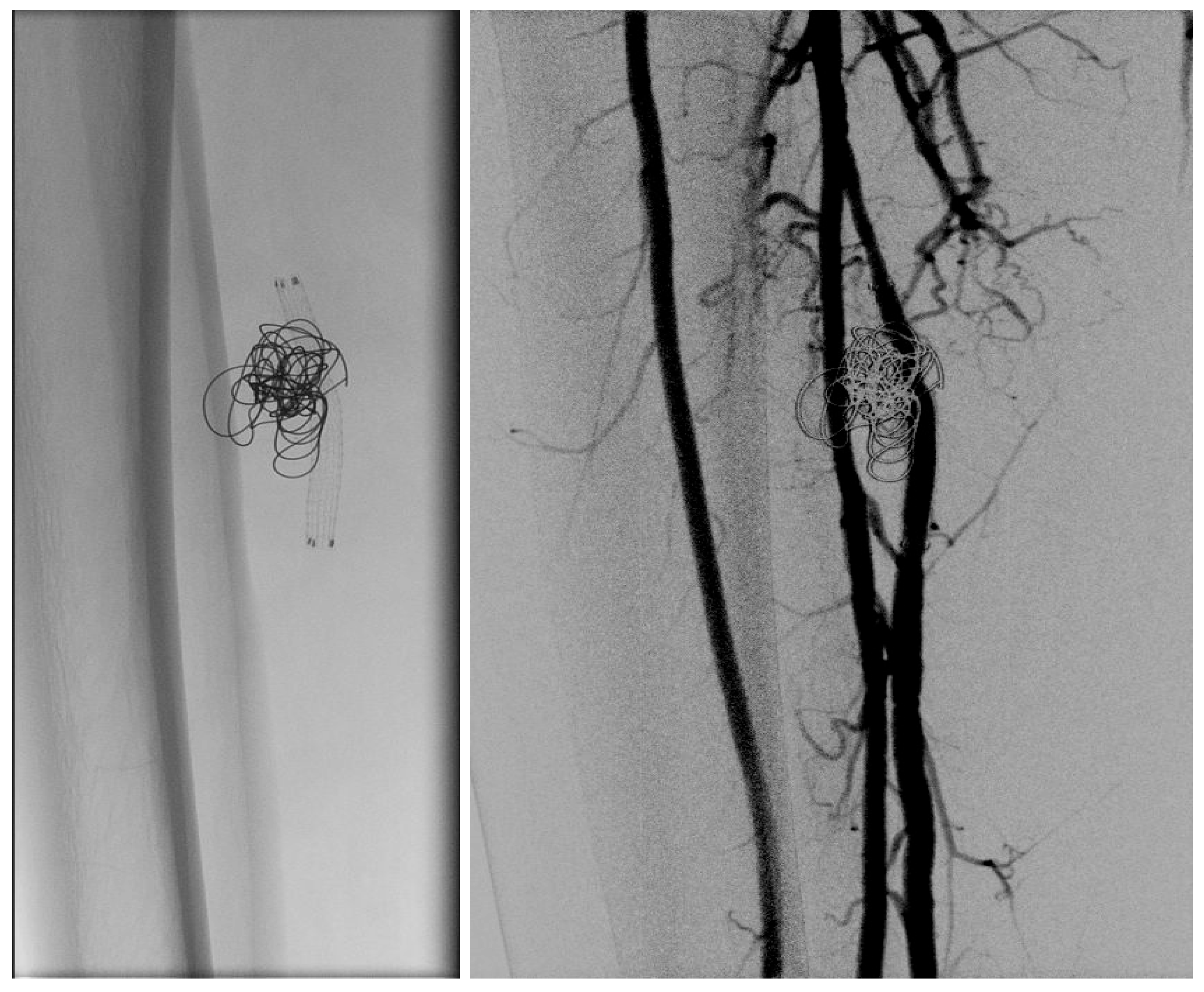
In light of a symptomatic aneurysm, treatment was offered to the patient. After discussing the risks of open and endovascular treatment options with the patient, an endovascular approach was opted for. The presence of a large aneurysm with an AV fistula and venous congestion posed an increased risk of significant bleeding complications associated with open surgery. An antegrade femoral access was obtained via a 5F sheath. After obtaining an angiogram, two coils were deployed in the aneurysm sac (Concerto PGLA helical PV-20-50-Helix and Concerto PGLA 3D PV-18-40-3D, Medtronic, Minneapolis, United States of America), with the aim to cause sac thrombosis and obliterate the flow from multiple AV fistulas. As anticipated, this did not lead to complete occlusion of the aneurysm and AV fistula. A retrograde pedal access was obtained, and cannulation of the PTA was successfully performed with a V14 guidewire (Fig. 2, 3). After obtaining guidewire access, the aneurysm was excluded with a stent graft (Viabahn Endoprosthesis 5 mm × 50 mm, WL Gore, Flagstaff, AZ, USA). Immediately after the procedure, angiography control visualized complete exclusion of the pseudoaneurysm, occlusion of the sac, and absence of any AVF (Fig. 4). Postoperatively, the patient reported pain reduction. Both pedal pulses were palpable. Postoperative antithrombotic therapy included Aspirin 100 mg and Clopidogrel 75 mg daily for 6 months. Additionally, Class 2 compression stockings were recommended for 1 month. After 18 months of follow-up, the patient was free of symptoms, and the stent graft was patent.
Figure 1.
The CT-Angiogram shows the aneurysm of the posterior tibial artery with AV-Fistula (Contrast uptake by the deep and the superficial veins).
Figure 1.
The CT-Angiogram shows the aneurysm of the posterior tibial artery with AV-Fistula (Contrast uptake by the deep and the superficial veins).
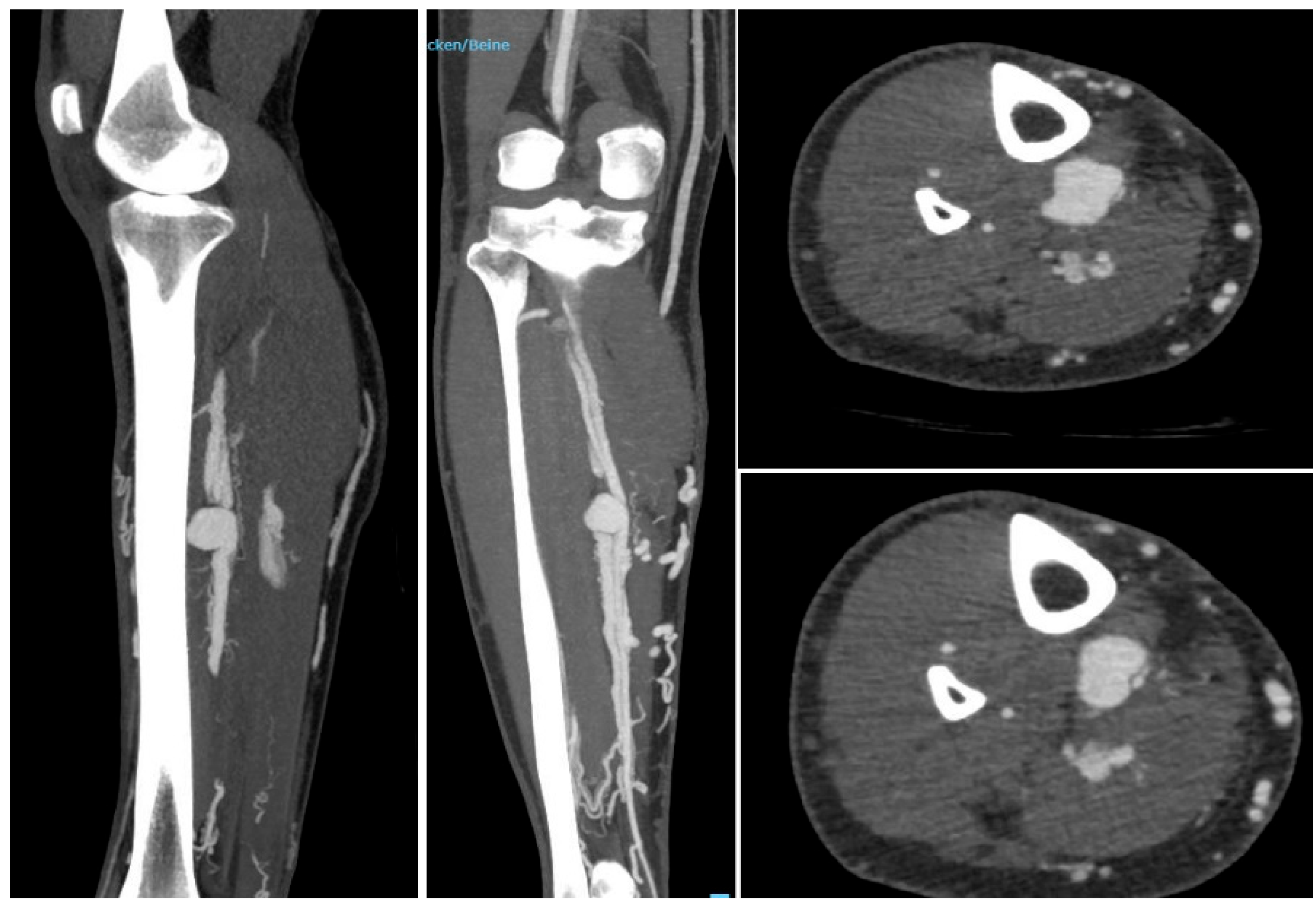
Figure 2.
Left to right. An angiogram was obtained, the aneurysm sack was coiled. Multiple attempts to cannulate the distal posterior tibial artery failed (Microcatheter is in the crural vein). After coiling the aneurysm sack and the AV-Fistula were still patent.
Figure 2.
Left to right. An angiogram was obtained, the aneurysm sack was coiled. Multiple attempts to cannulate the distal posterior tibial artery failed (Microcatheter is in the crural vein). After coiling the aneurysm sack and the AV-Fistula were still patent.
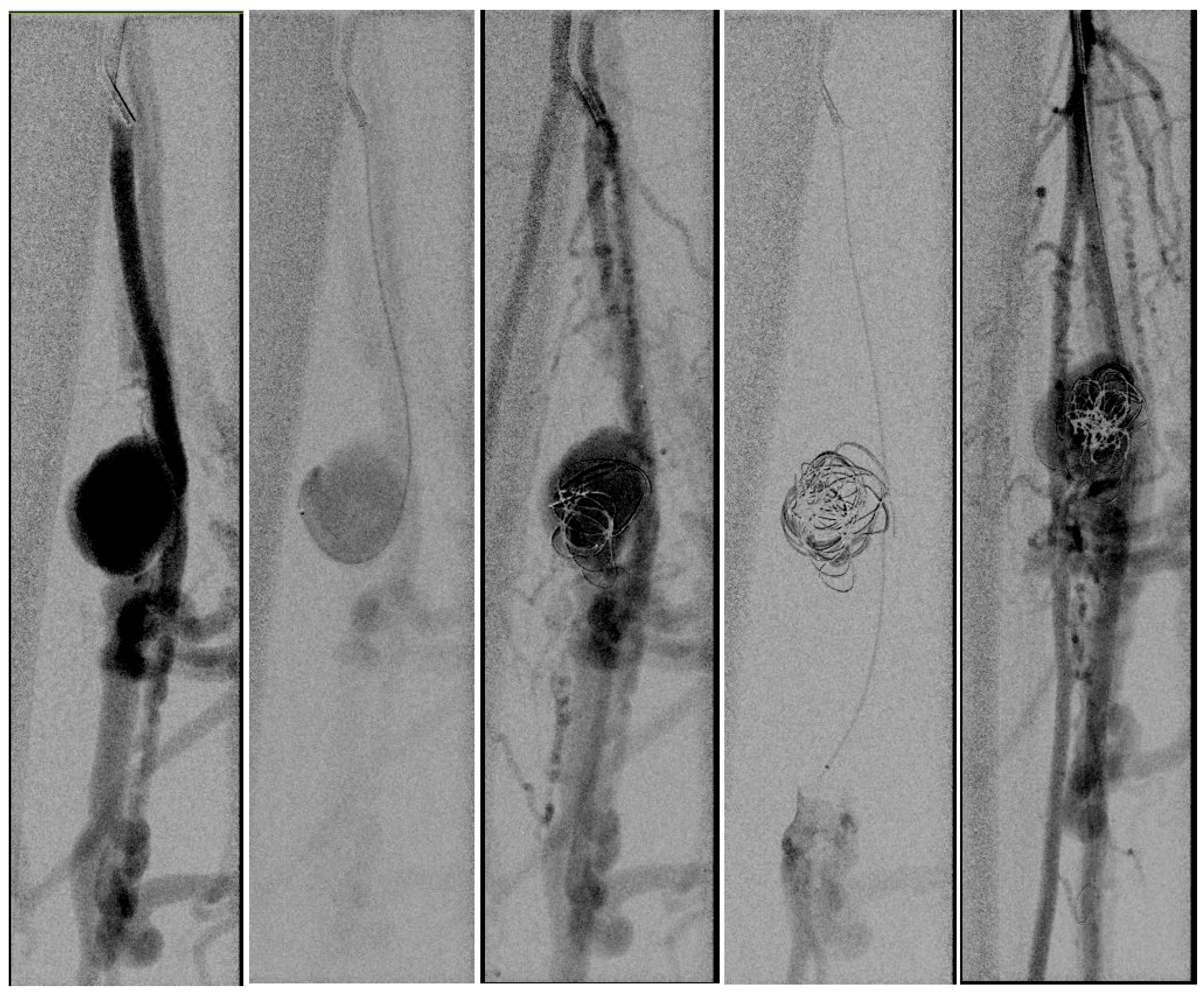
Figure 3.
Left to right. Retrograde pedal access was obtained and the cannulation was successful with a V14 Guidewire.
Figure 3.
Left to right. Retrograde pedal access was obtained and the cannulation was successful with a V14 Guidewire.
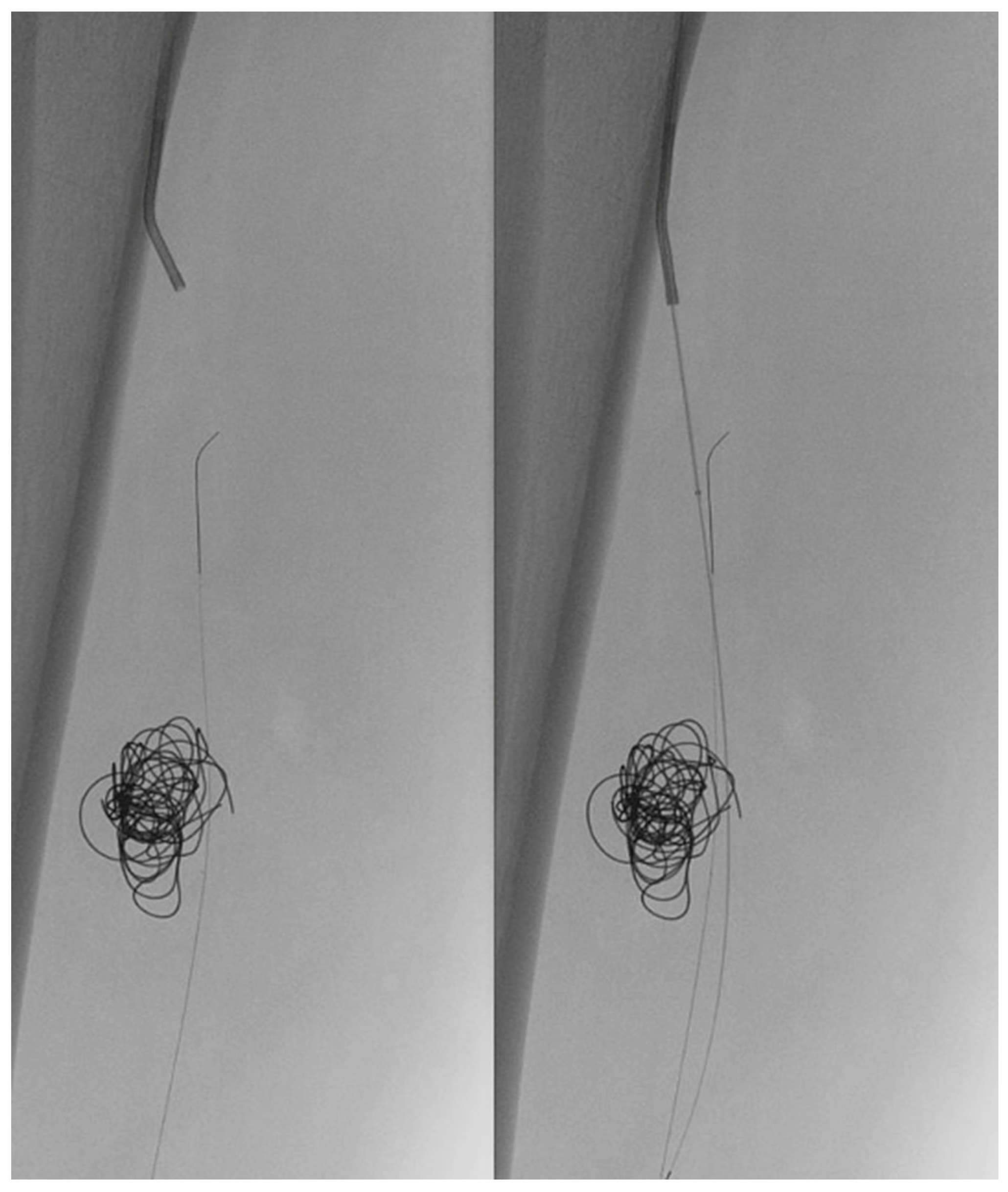
Figure 4.
Left to right. Coils and Viabahn Stent-Graft. Post-Stenting angiogram showing excluded aneurysm and fully deployed Viabahn.
Figure 4.
Left to right. Coils and Viabahn Stent-Graft. Post-Stenting angiogram showing excluded aneurysm and fully deployed Viabahn.
Systematic Review
A multiple database search (Scopus, PubMed, Medline, OVID) was carried out in accordance with PRISMA 2020 guidelines for publications between January 2000 and January 2024 (Fig. 5) [27]. MeSH terms for the search strategy were crural aneurysm, anterior tibial artery aneurysm, posterior tibial artery aneurysm, peroneal artery aneurysm, and tibio-peroneal trunk aneurysm. The studies were assessed, and data on demographics, procedural details, and follow-up were collected and pooled independently by two reviewers. Case series, trials, and retrospective studies with EVT of aneurysms were included. Concomitant treatment of aneurysms other than crural aneurysms, patients treated conservatively, surgically or with thrombin, and patients <15 years were excluded from the study.
Results
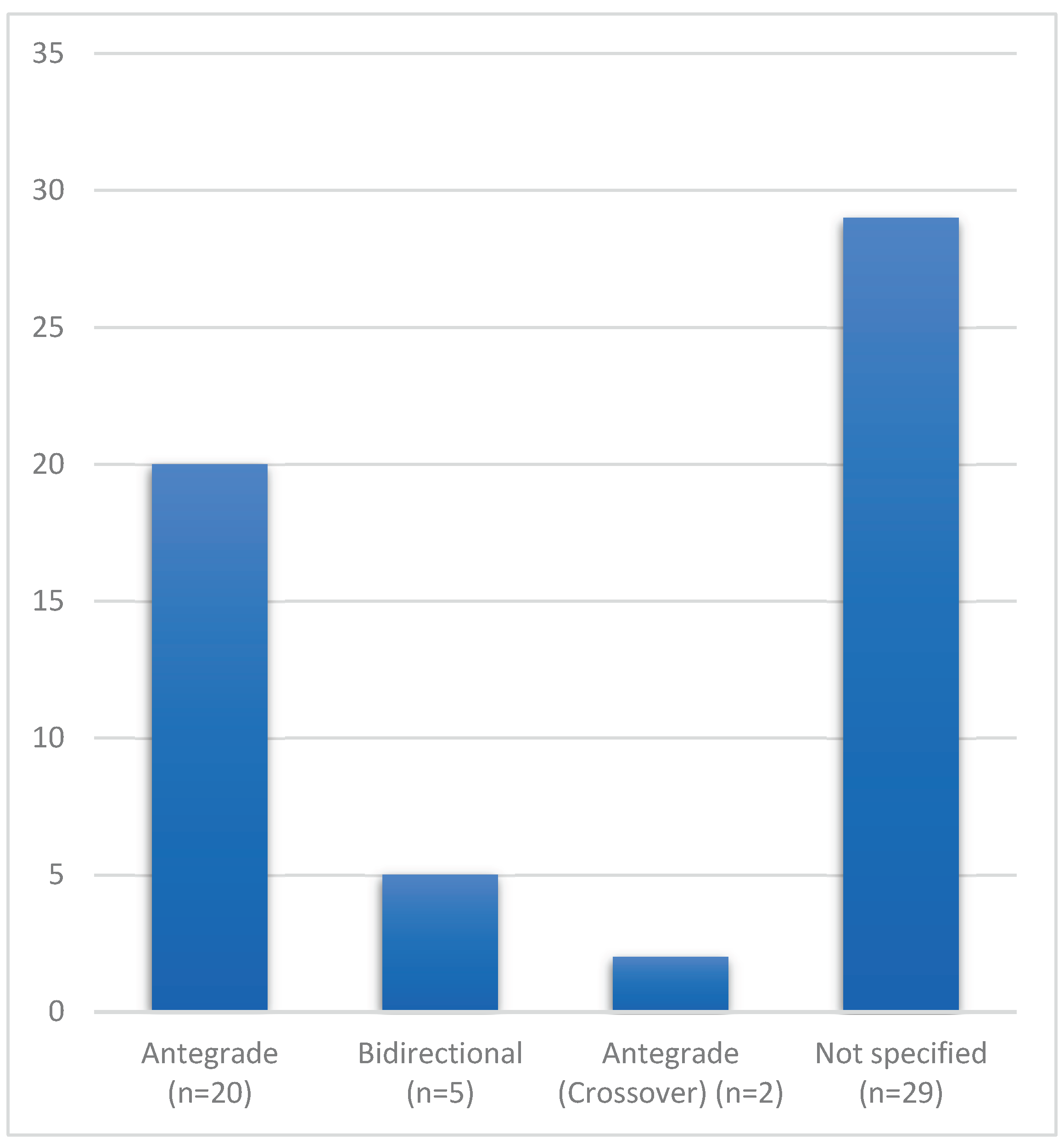
A total of 790 records were identified (Fig. 5). After initial screening of the titles and abstracts and removing duplicates, a total of 75 studies were sought for retrieval. A total of 44 studies were eligible to be included in the current review [1,5–12,14,16,18–26,28–51]. This included 43 case reports, one case series, and a total of 56 treated patients/limbs (Table 1). The average age of the patients was 50 years (range 15–87). The peroneal artery was the most frequently affected crural vessel (Fig. 6). The most common etiology was iatrogenic trauma 29/56 (51.7%), followed by outside-hospital trauma 15/56 (26.7%), connective tissue disorders like Behçet’s disease and Ehlers-Danlos syndrome in 6/56 (10.7%), mycotic in 1/56 (1.7%), and idiopathic in 5/56 (8.9%). The type of endovascular procedure and access are depicted in Fig. 7a and 7b. Various stents and stent grafts were used for the endovascular exclusion of the crural aneurysms. The most commonly used type of stent graft was balloon-expandable, followed by self-expanding stent grafts (Table 2). The median stent diameter was 3 mm (range 2.5 mm–6 mm), and the Graftmaster™ RX Coronary Stent Graft (Abbott, Chicago, Illinois, United States) was the most commonly used stent graft system. The average follow-up was 9.5 months (one week–60 months). Eighteen of 27 (18/27) patients had patent stents at follow-up, with a pooled primary patency rate of 66.6%. No studies reported any reinterventions or complications.
Figure 5.
Flow diagram of systematic review including searched databases and study selection.
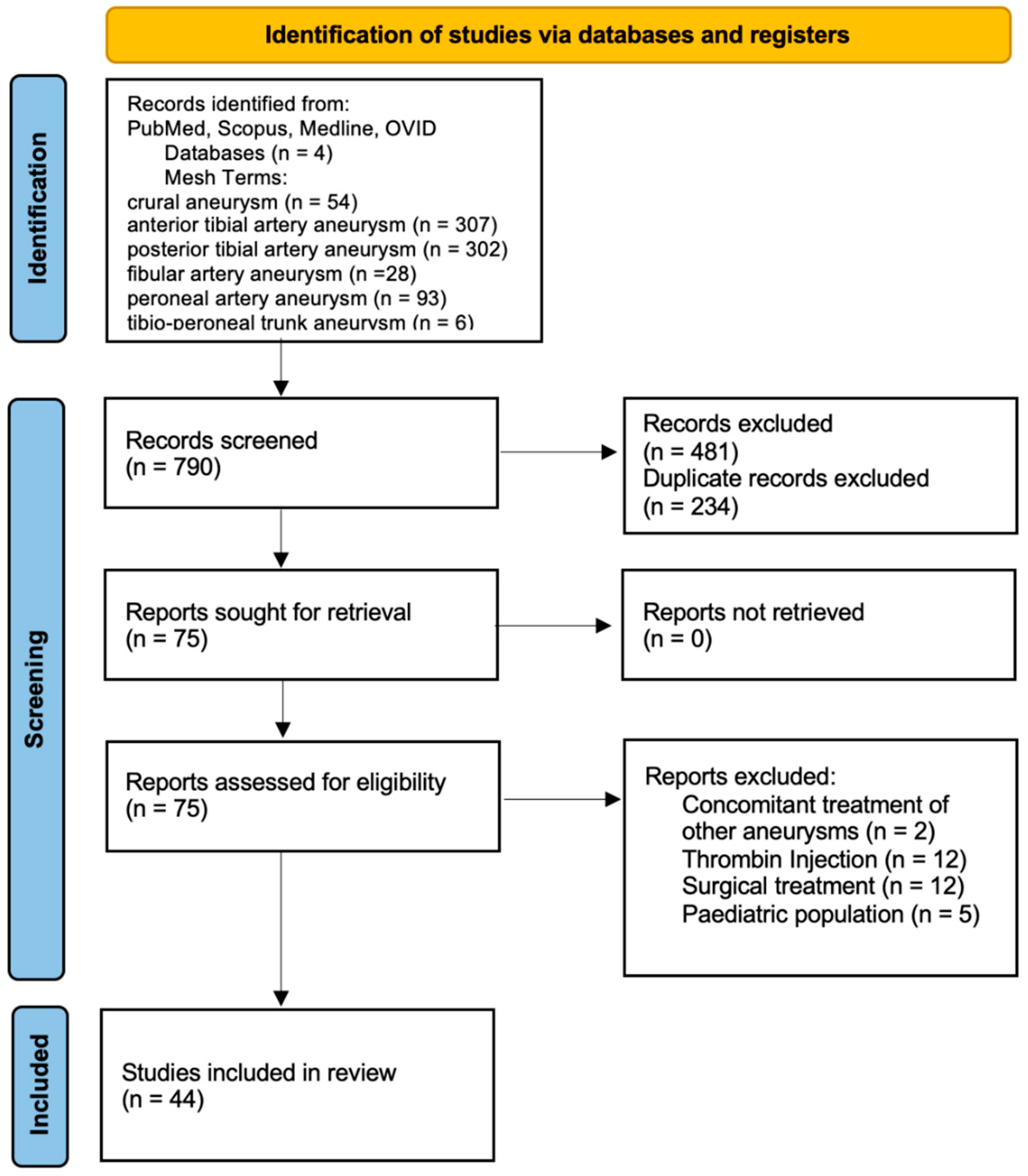
Figure 6.
Involvement of arteries in the pooled data of patients from the studies included in the review. Anterior tibial artery (ATA), posterior tibial artery (PTA), peroneal artery (A. fib.), tibioperoneal trunk (TPT).
Figure 6.
Involvement of arteries in the pooled data of patients from the studies included in the review. Anterior tibial artery (ATA), posterior tibial artery (PTA), peroneal artery (A. fib.), tibioperoneal trunk (TPT).
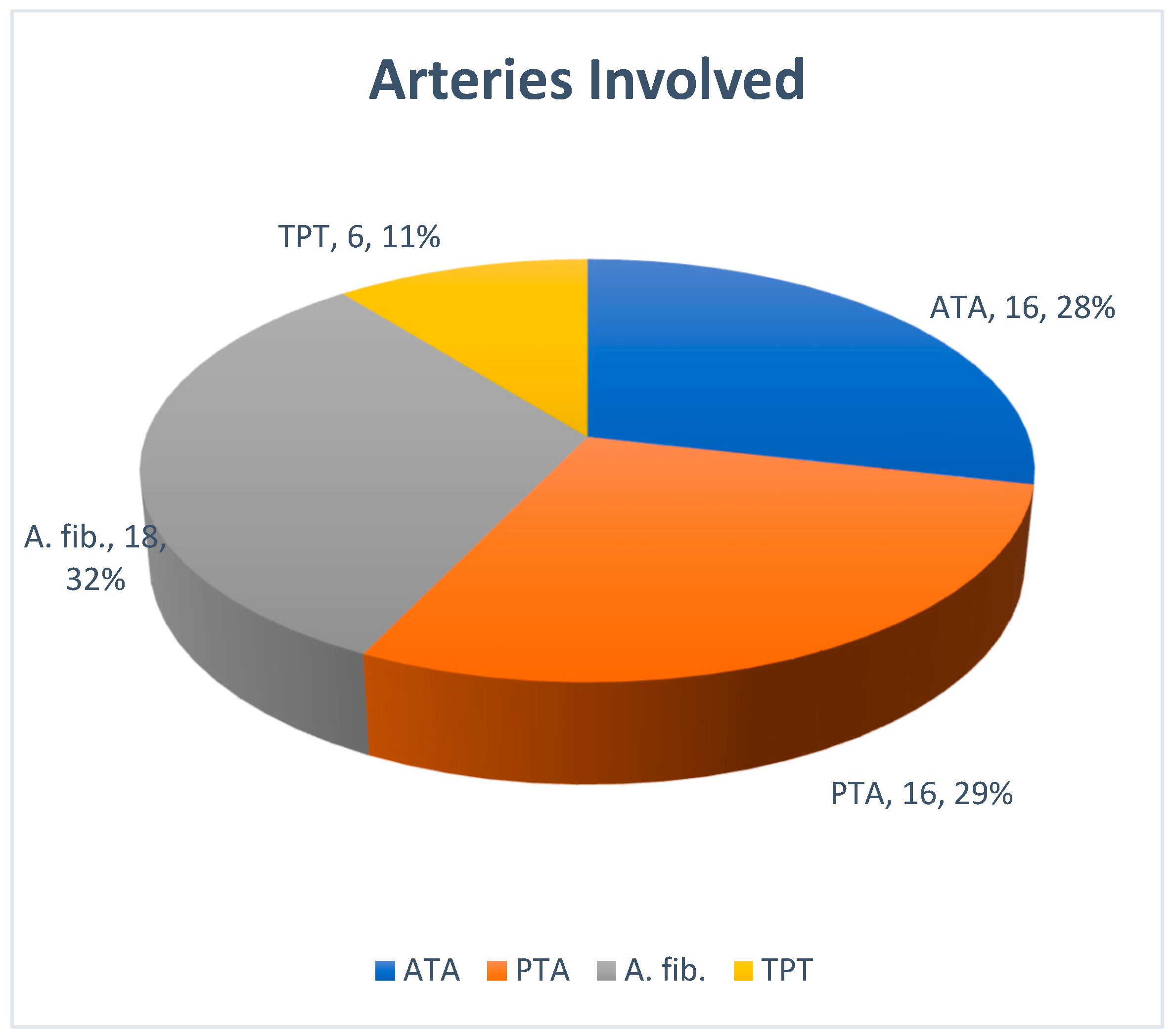
Figure 7.
a Endovascular treatment strategy opted for the treatment of crural aneurysms in the studies included in the review.
Figure 7.
a Endovascular treatment strategy opted for the treatment of crural aneurysms in the studies included in the review.
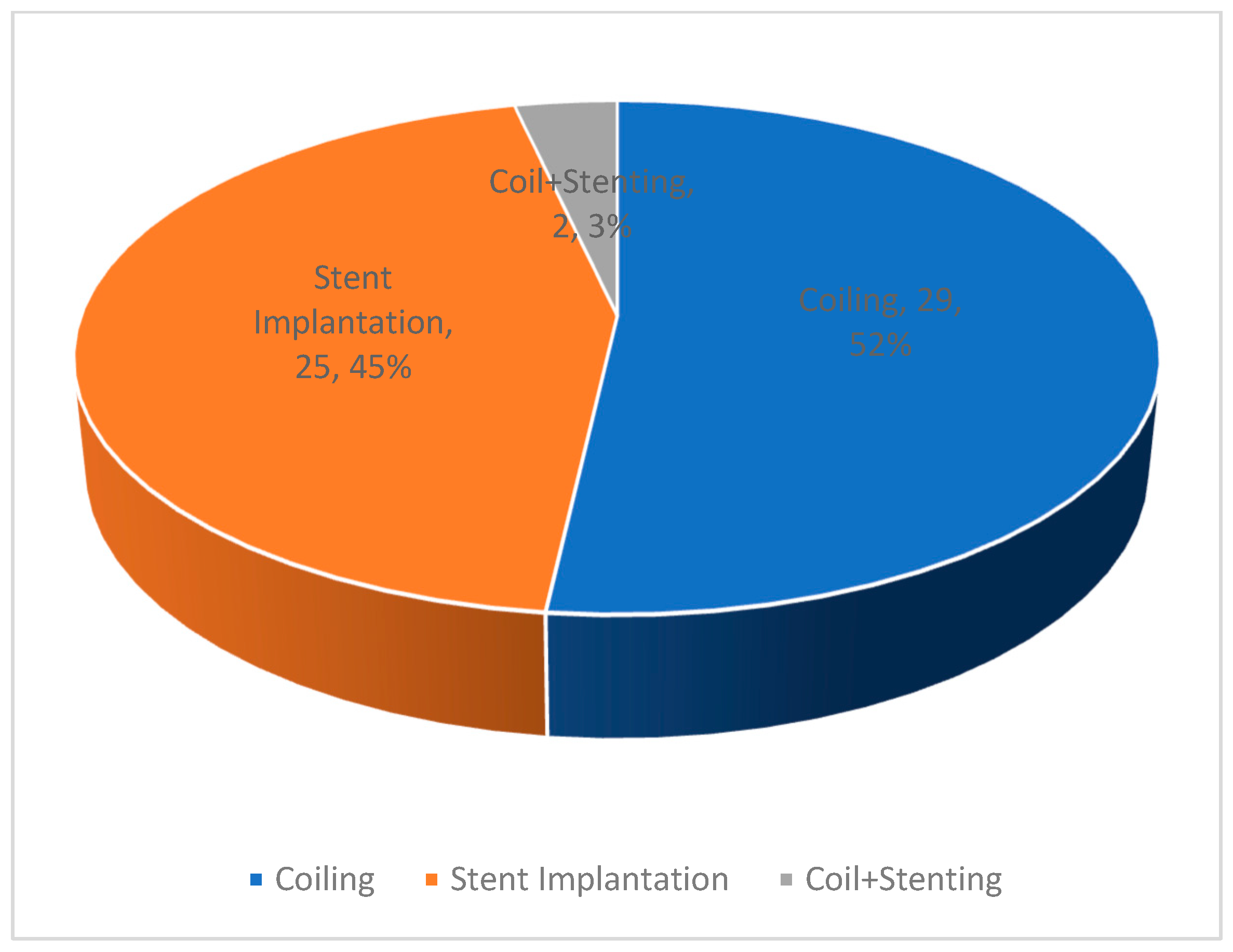
Figure 7.
b Choice of access for the endovascular treatment strategy opted for the treatment of crural aneurysms in the studies included in the review.
Figure 7.
b Choice of access for the endovascular treatment strategy opted for the treatment of crural aneurysms in the studies included in the review.
Discussion
Aneurysms of the crural arteries are a rare entity with unknown incidence. As encountered in the presented case in this study, the association of these aneurysms with an AV fistula to the deep veins is even rarer. An associated AV fistula was found in 5/56 (8.9%) patients in the current review. All of these patients had a history of trauma. Two of these were treated with coil occlusion [12,30] of the pseudoaneurysm and the affected vessel, and three were treated with stent-graft implantation [31,47,49]. In our case, we started the procedure with an antegrade approach and coil occlusion of the pseudoaneurysm. This was done to cause thrombosis of the aneurysm and prevent flow in the aneurysm from the multiple venous fistula tracts. Since the following angiogram demonstrated persistent but reduced contrast uptake by the aneurysm and associated deep veins, we decided to proceed with stent-graft implantation. The rationale for this was sealing the inflow to the aneurysm, preserving the vessel and its distal outflow, and avoiding coiling of the whole vessel. This approach is unlike the current review, where the most common treatment strategy was coil occlusion of the aneurysm and the vessel (52%). A prerequisite to this approach is the presence of distal flow to the foot through the non-affected arteries. Stent grafts, on the other hand, offer an opportunity to preserve distal blood flow in the affected artery. A combination of both coiling and stent-graft implantation is rarely described (3% in the current review).
The natural history of these aneurysms is unknown, and size does not seem to play a role in the symptomatology or as a causative factor for complications. Madison et al. describe a case with a 7–9 mm aneurysm of the anterior tibial artery associated with Ehlers-Danlos syndrome, with acute onset of calf pain, massive tenderness, and impending rupture. Similarly, Parry et al. describe a case of a pseudoaneurysm of the posterior tibial artery presenting as acute arterial hemorrhage from a chronic venous ulcer in a patient with deep-vein thrombosis and post-thrombotic syndrome. Singh et al. and Nwilati et al. describe urgent repair of a ruptured crural pseudoaneurysm with local compartment syndrome [15]. Case studies including Spronk et al. [53] describe a risk of distal embolisation and blue-toe syndrome as initial presentation. The rarity of this entity makes it difficult to give recommendations regarding diameter cut-off values to guide treatment. Analogous to popliteal artery aneurysms, we recommend treating symptomatic crural aneurysms on an urgent basis. Asymptomatic aneurysms without any signs of compression can be followed up regularly. Since, rupture rate in patients with connective tissue disorders are high, these patients can be monitored closely [15].
Various treatment strategies have been described in the literature. A recent publication including the treatment of 38 patients with peripheral artery pseudoaneurysms (traumatic and/or iatrogenic) compared three modalities (open repair, endovascular approach, and ultrasound-guided thrombin injection). Open repair was associated with higher amounts of blood loss requiring more blood transfusion, significantly longer operative time, and longer hospital stay [54]. A large aneurysm with an AV fistula, as in the described cases, carries a potential risk of profuse hemorrhage with open reconstruction. In our case, the size of the defect in the artery and the number of AV fistula connections could not be determined preoperatively. Additionally, due to the potential severe trauma associated with exploration during open reconstruction, we opted for an endovascular approach. An open approach appears feasible for aneurysms that have a small defect and where delineation of the AV fistula tract is possible. The options include patch reconstruction of the defect or a venous interposition graft [54].
The current literature review also provides information regarding the type and size of stents that are being used worldwide for this indication. The rare nature of this clinical entity explains the absence of dedicated stents and the lack of consensus on which stent can or should be used in the crural arteries for aneurysm exclusion. The most commonly used stent was a balloon-expandable stent (coronary stent, Graftmaster from Abbott). The pooled data showed that the median diameter of the stents used was 3 mm. We used a self-expanding stent graft (Viabahn 5 mm diameter), which one would think might be large for crural vessels. However, in this young patient, the vessels had a diameter of 4 mm as measured in the preoperative CT angiogram. The literature review revealed one more study group using a 5 mm Viabahn to exclude a crural aneurysm, without any complications and with a patent stent at 12 months of follow-up [11]. Surprisingly, Yamamoto et al. reported the use of a self-expanding bare-metal stent (Innova, Boston Scientific) as a barrier to trap coils in the aneurysm sac to cause sac thrombosis [19]. A recent study reported the use of a flow diverter pipeline embolization device (PED) with a diameter of 3.5 mm for crural aneurysm exclusion [48]. These devices are being used for the exclusion of intracranial aneurysms or dissections.
The average follow-up of the pooled patients was 9.5 months (one week–60 months). Eighteen of 27 (18/27) patients had patent stents at follow-up with a pooled patency rate of 66.6%. In the reported case, after 18 months of follow-up, the patient was free of symptoms, and the endoprosthesis was patent. This review highlights a key limitation of the available literature: long-term follow-up data, including information on reinterventions and secondary patency rates, are largely missing.
Conclusions
The endovascular approach to crural aneurysms offers an additional management modality with the advantages of low blood loss and early ambulation. The disadvantages include the necessity of postoperative antithrombotic therapy, with insufficient data regarding its duration. Moreover, the long-term results regarding stent patency are lacking. Open repair is associated with higher amounts of blood loss requiring more blood transfusion, significantly longer operative time, and longer hospital stay [54]. The superiority of one modality over the other cannot be answered with the currently available literature. However, the endovascular approach offers an additional quiver in the armamentarium of a vascular surgeon for flow preservation and is indeed a feasible alternative to open ligation or coil occlusion of the affected vessels.
Funding
This research received no external funding.
Authors’ Contributions
Conceiving and designing the study: AS, RS, MF, SK, FA; Collecting the data: AS, RS; Analysing and interpretating the data: AS, RS, MF, SK, FA; Writing the manuscript: AS, RS, FA; Critical Revisions of the article: AS, RS, MF, SK, FAFinal approval of the article: AS, RS, MF, SK, FA; Overall responsibility: AS, RS, MF, SK, FA. All authors have read and agreed to the published version of the manuscript.
Ethics Statement
This study does not disclose the identity of the patient. The Images were used with prior signed consent of the patient.
Data Availability Statement
Data can be made available on request.
Conflict of Interests
The authors declare no conflict of interests.
References
- Sadat U. et al. Peroneal artery pseudoaneurysm- a case report and literature review. BMC surgery 2007;7:4.
- Griffith JF, Cheng JC, Lung TK, Chan M (1998) Pseudoaneurysm after high tibial osteotomy and limb lengthening. Clin Orthop Relat Res 354:175–179.
- Han KJ, Won YY, Khang SY (2004) Pseudoaneurysm after tibial nailing. Clin Orthop Relat Res 418:209–212.
- Oehlert WH. A complication of the Fogarty arterial embolectomy catheter. Am Heart J 1972; 84 (4): 484 – 486.
- Chrencik, M. T. et al. Infrapopliteal Arterial Pseudoaneurysm Development Secondary to Blunt Trauma: Case Series and Literature Review Vasc endovascular surg 2020 vol. 54 (4) 367-374.
- Brunoro M. et al. Endovascular Treatment of an Anterior Tibial Artery Pseudoaneurysm Secondary to Penetrating Trauma in a Young Patient: Case Report and Literature Review 2019 Ann Vasc Surg Volume 60, 479.e5-479.e9.
- Maga P. et al. Unusual presentation of polyarteritis nodosa with unilateral pseudoaneurysm of the posterior tibial artery. Pol Arch Med Wewn. 2015; 125 (4): 301-302.
- Hagspiel, K. D. Metachronous bilateral posterior tibial artery aneurysms in Ehlers-Danlos syndrome type IV. 2011 Cardiovasc Intervent Radiol vol. 34 (2) 413-8.
- Rico, J. V. et al. Urgent endovascular treatment of a ruptured tibioperoneal pseudoaneurysm in Behçet's disease. 2011 Ann Vasc Surg vol. 25 (3) 385.e11-4.
- Ferrero, E. Et al. Endovascular treatment of a symptomatic mycotic aneurysm of the peroneal artery 2011 Ann Vasc Surg vol.25 (7) 982.e11-4.
- Domenick N, et al. Endovascular repair of multiple infrageniculate aneurysms in a patient with vascular type Ehlers-Danlos syndrome. J Vasc Surg. 2011 Sep;54(3):848-50. Epub 2011 Mar 31. [CrossRef] [PubMed]
- Singh D, Ferero A. Traumatic pseudoaneurysm of the posterior tibial artery treated by endovascular coil embolization. Foot Ankle Spec. 2013 Feb;6(1):54-8. Epub 2012 Oct 16. [CrossRef] [PubMed]
- Kars HZ, Topaktas S, Dogan K. Aneurysmal peroneal nerve compression. Neurosurgery. 1992;30(6):930-931.
- Madison MK, Wang SK, King JR, Motaganahalli RL, Sawchuk AP. Urgent Endovascular Repair of an Anterior Tibial Artery Aneurysm: Case Report and Literature Review. Vascular and Endovascular Surgery. 2020;54(8):760-764. [CrossRef]
- Nwilati AE, AlQedra D, Shafiei M, AlSaleh FM. True anterior tibial artery aneurysm with rupture and compartment syndrome. J Vasc Surg. 2019;70(5):e198-e199.
- Ono S, Shimogawara T, Yamazoe S, Matsui J. Successful endovascular isolation of a huge true anterior tibial artery aneurysm by the bi-directional approach in a young patient. Catheter Cardiovasc Interv. 2020;95(6):E175-E178.
- Musio D, Perfumo MC, Gazzola V, Pane B, Spinella G, Palombo D. A true giant aneurysm of the anterior tibial artery. Ann Vasc Surg. 2015;29(6):1319 e1315-e1319.
- Gratl A. et al., Treatment options of crural pseudoaneurysms Vasa 2014; 43: 209 – 215.
- Yamamoto Y. Et al. Endovascular coil embolization of a large tibioperoneal trunk pseudoaneurysm. Journal of Vascular Surgery Cases and Innovative Techniques 2020; Volume 6 number 3.
- Micari, A. et al. Tibioperoneal trunk pseudoaneurysm coil embolization 2010 Catheter Cardiovasc Interv vol.75 (2) 276-8.
- Miura, T. et al. Iatrogenic peroneal artery pseudoaneurysm treated by transluminal coil embolization 2013 Cardiovasc Interv Ther vol. 28 (1) 128-30.
- Okugi, S. et al. Endovascular Embolisation for Proximal Anterior Tibial Artery Aneurysm. 2021 Eur J Vasc Endovasc Surg vol. 61 (6) 979.
- de Troia A, Biasi L, Iazzolino L, Azzarone M, Tecchio T, Rossi C, Salcuni P. Endovascular stent grafting of a posterior tibial artery pseudoaneurysm secondary to penetrating trauma: case report and review of the literature. Ann Vasc Surg. 2014 Oct;28(7):1789.e13-7. Epub 2014 Feb 12. [CrossRef] [PubMed]
- Golledge, J et al. Use of a covered stent to treat two large false aneurysms of the anterior tibial artery 2008 J Vasc Surg vol. 47 (5) 1090.
- Joglar F, Kabutey NK, Maree A, Farber A. The role of stent grafts in the management of traumatic tibial artery pseudoaneurysms: case report and review of the literature. Vasc Endovascular Surg 2010; 44 (5): 407 – 409.
- De Roo, R. A. Et al. Exclusion of a crural pseudoaneurysm with a PTFE-covered stent-graft. 2004 J Endovasc Ther vol. 11 (3) 344-7.
- Page MJ, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. [CrossRef]
- Parry, D. J. et al. Arterial haemorrhage from a chronic venous ulcer--pseudoaneurysm formation of the posterior tibial artery 2000 Eur J Vasc Endovasc Surg vol. 20 (5) 489-491.
- Hebrang, A. et al. Successful closure of large pseudoaneurysm of peroneal artery using transluminal temporary occlusion of the neck with the catheter. 2001 Eur Radiol 11 (7) 1206-9.
- Rosa P, et al. Starnes B. Endovascular management of a peroneal artery injury due to a military fragment wound. Ann Vasc Surg. 2003 Nov;17(6):678-81. [CrossRef] [PubMed]
- Spirito R, et al. Endovascular treatment of a post-traumatic tibial pseudoaneurysm and arteriovenous fistula: case report and review of the literature. J Vasc Surg. 2007 May;45(5):1076-9. [CrossRef] [PubMed]
- van Hensbroek, P. B. et al. Endovascular treatment of anterior tibial artery pseudoaneurysm following locking compression plating of the tibia 2007 J Orthop Trauma vol. 21 (4) 279-82.
- Barbano B. et al. True posterior tibial artery aneurysm in a young patient: surgical or endovascular treatment? BMJ Case Rep 2009.
- Verma, R. et al. Endovascular coil embolization of pseudoaneurysm of a branch of the anterior tibial artery following total knee replacement 2009 vol. 22 (3) 269-71.
- Goltz, J. P. et al. Emergency and elective implantation of covered stent systems in iatrogenic arterial injuries. 2011 Rofo vol. 183 (7) 618-30.
- Jacobs, E et al. Pseudoaneurysm of the anterior tibial artery after ankle arthroscopy 2011 J Foot Ankle Surg 50 (3) 361-3.
- Chatterjee,S. et al. Coil migration through skin after posterior tibial artery pseudoaneurysm trapping. 2011 Cardiovasc Intervent Radiol vol. 34 suppl. 2 S315-7.
- Ferrero, E. et al. Symptomatic aneurysm of a perforating peroneal artery after a blunt trauma 2012 Ann Vasc Surg vol.26 (2) 277.e1-3.
- De Santis, F. et al. Endovascular exclusion coupled with operative anterior leg compartment decompression in a case of postthromboembolectomy tibialis anterior false aneurysm. 2013 Ann Vasc Surg vol. 27 (7) 973.e1-8.
- Gopal, A. et al. Recalcitrant peroneal artery pseudoaneurysm in a patient with Hemophilia B. 2013 Cardiovasc Revasc Med vol. 14 (6) 359-62.
- Sala F, Salerno CF, Albisetti W. Pseudoaneurysm of the peroneal artery: an unusual complication of open docking site procedure in bone transport with Taylor Spatial Frame. Musculoskelet Surg. 2013 Aug;97(2):183-6. Epub 2011 Aug 5. [CrossRef] [PubMed]
- Kaczynski J, Beveridge E, Holdsworth RJ. Iatrogenic pseudoaneurysm of the peroneal artery. BMJ Case Rep. 2016 Jul 18;2016:bcr2016215836. [CrossRef] [PubMed] [PubMed Central]
- Zhao, R. et al. Pseudoaneurysm of a high-division anterior tibial artery following primary TKA 2017 Orthopade 46 (3) 275-279.
- Yanaka, K. et al. Endovascular Therapy with a Covered Stent Graft for Pseudoaneurysm of the Peroneal Artery Complicating High Tibial Osteotomy-A Case Report 2019 Ann Vasc Surg vol. 58 380.e13-380.e16.
- Cvetic V, Lukic B. Endovascular Management of Tibioperoneal Trunk Pseudoaneurysm with Arteriovenous Fistula. Eur J Vasc Endovasc Surg. 2020 Sep;60(3):429. Epub 2020 Jul 25. [CrossRef] [PubMed]
- Cristiani-Winer, M. Distal peroneal artery pseudoaneurysm. 2021 Acta Ortop Mex vol.35 (3) 290-293.
- Scherer J, Schäfer FP, Kobe AR, Messmer F, Pape HC, Rauer T. Ordinary injury, big surprise - Traumatic false aneurysm and arteriovenous fistula of the posterior tibial artery after civilian trauma: A case report. Trauma Case Rep. 2021 Feb 18;32:100432. [CrossRef] [PubMed] [PubMed Central]
- Plotnik AN, Srinivasa RN, Szeder V, Moriarty J. Preservation of Posterior Tibial Artery Flow Following Dissection With Associated Aneurysmal Degeneration in Ehlers-Danlos Syndrome Type IV Treated With Flow-Diverting Stent. Ann Vasc Surg. 2021 May;73:521-524. Epub 2021 Jan 24. [CrossRef] [PubMed]
- Papageorgopoulou C, Nikolakopoulos K, Ntouvas I, Papadoulas S, Kritikos N. A rare combination of tibial artery aneurysm and traumatic arteriovenous fistula: a case report. Pan Afr Med J. 2022 Jun 15;42:122. [CrossRef] [PubMed] [PubMed Central]
- Park JJ, Perry LD, Tamburrini D, Kumar S. Successful Coil Embolization of a Large Anterior Tibial Artery Pseudoaneurysm After Open Reduction Internal Fixation of a Bi-condylar Tibial Plateau Fracture. Am Surg. 2023 Sep;89(9):3886-3888. Epub 2023 May 9. [CrossRef] [PubMed]
- Green RJ, Sellars J, Vennam S, Bhutia S. Off-label use of PK Papyrus coronary covered stent to treat traumatic pseudoaneurysm of posterior tibial artery. ANZ J Surg. 2023 May;93(5):1398-1399. Epub 2023 Feb 2. [CrossRef] [PubMed]
- Prasad K, Elefteriades JA. The Management of Peripheral Vascular Aneurysms: Present and Future Options. Int J Angiol. 2019 Mar;28(1):3-4. Epub 2019 Feb 22. [CrossRef] [PubMed] [PubMed Central]
- Spronk S, den Hoed PT, Veen HF. Case report: blue toe syndrome caused by a true crural aneurysm.Journal of Vascular Nursing. 2003;21(2):70-71. [CrossRef]
- Zhao, B., Zhang, J., Ma, J., Huang, M., Li, J. and Ma, X.. Comparison of three different treatment methods for traumatic and Iatrogenic peripheral artery pseudoaneurysms. Orthop Surg, 2022;14: 1404-1412. [CrossRef]

Table 1.
Details to investigators, years of study, age and sex of patients, etiology and localization of aneurysms; anterior tibial artery (ATA), posterior tibial artery (PTA), peroneal artery (A. fib.), tibioperoneal trunk (TPT), Polyarteritis nodosa (PAN), syndrome (sy.), not mentioned (NM).
Table 1.
Details to investigators, years of study, age and sex of patients, etiology and localization of aneurysms; anterior tibial artery (ATA), posterior tibial artery (PTA), peroneal artery (A. fib.), tibioperoneal trunk (TPT), Polyarteritis nodosa (PAN), syndrome (sy.), not mentioned (NM).
| Authors | Year | Age | Sex | Etiology | Involved artery | |
|---|---|---|---|---|---|---|
| 1 | Parry, D. J. et al. | 2000 | 44 | M | Idiopathic | PTA |
| 2 | Hebrang, A. et al. | 2001 | 51 | M | Iatrogenic | A. fib. |
| 3 | Rosa, P. et al. | 2003 | 19 | M | Post-traumatic | A. fib. |
| 4 | De Roo, R. A. et al. | 2004 | 58 | M | Iatrogenic | ATA |
| 5 | Sadat, U. et al. | 2007 | 68 | M | Iatrogenic | A. fib. |
| 6 | Spirito,R. et al. | 2007 | 74 | M | Post-traumatic | ATA |
| 7 | Van Hensbroek, P. B. et al. | 2007 | 55 | M | Iatrogenic | ATA |
| 8 | Golledge, J et al. | 2008 | 42 | M | Post-traumatic | ATA |
| 9 | Barbano B. et al. | 2009 | 28 | M | Idiopathic | PTA |
| 10 | Verma, R. et al. | 2009 | 79 | M | Iatrogenic | ATA |
| 11 | Joglar, F. et al. | 2010 | 39 | M | Post-traumatic | PTA |
| 12 | Micari, A. et al. | 2010 | 68 | M | Idiopathic | TPT |
| 13 | Domenick, N. et al. | 2011 | 33 | F | Ehler-Danlos sy. | PTA |
| 14 | Ferrero, E. et al. | 2011 | 69 | M | Mycotic | A. fib. |
| 15 | Goltz, J. P. et al. | 2011 | 87 | M | Iatrogenic | A. fib. |
| 16 | Hagspiel, K. D. et al. | 2011 | 24 | M | Ehler-Danlos sy. | PTA |
| 17 | Jacobs, E et al. | 2011 | 63 | F | Iatrogenic | ATA |
| 18 | Chatterjee,S. et al. | 2011 | 18 | M | Post-traumatic | PTA |
| 19 | Rico, J. V. et al. | 2011 | 41 | M | Behçet's disease | TPT |
| 20 | Ferrero, E. et al. | 2012 | 48 | M | Post-traumatic | A. fib. |
| 21 | De Santis, F. et al. | 2013 | 68 | M | Iatrogenic | ATA |
| 22 | Gopal, A. et al. | 2013 | 40 | M | Post-traumatic | A. fib. |
| 23 | Miura, T. et al. | 2013 | 82 | M | Iatrogenic | A. fib. |
| 24 | Sala, F. et al. | 2013 | 19 | M | Iatrogenic | A. fib. |
| 25 | Singh, D. et al. | 2013 | 23 | M | Post-traumatic | PTA |
| 26 | de Troia, A. et al. | 2014 | 34 | M | Post-traumatic | PTA |
| 27 | Gratl, A. et al. | 2014 | Range (15–84) | Iatrogenic | 6xA.fib, 3xPTA, 2xTPT, 2xATA | |
| 28 | Maga, P. et al. | 2015 | 32 | M | PAN | PTA |
| 29 | Kaczynski, J. et al. | 2016 | 78 | M | Iatrogenic | A. fib. |
| 30 | Zhao, R. et al. | 2017 | 72 | F | Iatrogenic | ATA |
| 31 | Brunoro M. et al. | 2019 | 18 | F | Post-traumatic | ATA |
| 32 | Yanaka, K. et al. | 2019 | 69 | F | Iatrogenic | A. fib. |
| 33 | Chrencik, M. T. et al. | 2020 | 60 | M | Post-traumatic | PTA |
| 34 | Cvetic, V. et al. | 2020 | 49 | M | Post-traumatic | TPT |
| 35 | Madison, M. K. et al. | 2020 | 26 | M | Ehler-Danlos sy. | ATA |
| 36 | Ono, S. et al. | 2020 | 33 | F | Idiopathic | ATA |
| 37 | Yamamoto, Y. et al. | 2020 | 70 | M | Iatrogenic | TPT |
| 38 | Cristiani-Winer, M. | 2021 | 60 | M | Iatrogenic | A. fib. |
| 39 | Okugi, S. et al. | 2021 | 72 | F | Idiopathic | ATA |
| 40 | Scherer,J. et al. | 2021 | 39 | F | Post-traumatic | PTA |
| 41 | Plotnik, A et al. | 2021 | 38 | M | Ehler-Danlos sy. | PTA |
| 42 | Papageorgopoulou, C et al. | 2022 | 60 | M | Post-traumatic | ATA |
| 43 | Park, J et al. | 2023 | NM | NM | Iatrogenic | ATA |
| 44 | Green, RJ et al. | 2023 | 18 | F | Post-traumatic | PTA |
Table 2.
Studies using stents or stent grafts for the exclusion of the crural aneurysms with size, type and number of stents deployed and their patency at the end of follow-up.
Table 2.
Studies using stents or stent grafts for the exclusion of the crural aneurysms with size, type and number of stents deployed and their patency at the end of follow-up.
| Authors | Stent Nr. / Size (mm) | Stent Type | Stent name, manufacturer | Follow-up (months) | Patent Stents | |
|---|---|---|---|---|---|---|
| 1 | De Roo, R. A. et al. | 1 / 4 x 31 | SESG | Symbiot, Boston Scientific | 12 | 1 |
| 2 | Spirito,R. et al. | 1 / 4 x 26 | BESG | Graftmaster, Abbott | 12 | 1 |
| 3 | Van Hensbroek, P. B. et al. | 1 / 3 x 20 | SESG | Symbiot, Boston Scientific | 6 | 1 |
| 4 | Golledge, J et al. | 1 /3 x 19, 1 / 3,5 x 19 |
BESG | Graftmaster, Abbott | 1,5 | 1 |
| 5 | Joglar, F. et al. | 1 / 3 x 19 | BESG | Graftmaster, Abbott | 8 | 1 |
| 6 | Domenick, N. et al. | 1 / 5 x 10 | SESG | Viabahn, WL. Gore | 12 | 1 |
| 7 | Ferrero, E. et al. | 1 / 3 x 26 | BESG | Graftmaster, Abbott | 60 | 1 |
| 8 | Goltz, J. P. et al. | 1 / 3 x 19 | BESG | Graftmaster, Abbott | 1 | 1 |
| 9 | De Santis, F. et al. | 1 / 4 x 19 | BESG | Direct-Stent, In-Situ Techn. | 10 | 1 |
| 10 | de Troia, A. et al. | 1 / 3 x 19 | BESG | Direct-Stent, In-Situ Techn. | 18 | 1 |
| 11 | Gratl, A. et al. | NM | BESG | Graftmaster, Abbott | 7 | 1 |
| 12 | Maga, P. et al. | 1 / 3.5 x 2.8 | BESG | AnuGraft, IGTI | 6 | 1 |
| 13 | Brunoro M. et al. | 1 / 3.5 x 16, 1 / 4 x 24 | BESG | B-Graft, Bentley | 13 | 1 |
| 14 | Yanaka, K. et al. | 1 / 2.8 x 16 | BESG | Graftmaster, Abbott | 4 | 1 |
| 15 | Yamamoto, Y. et al. | 1 / 6 x 40 | SESB | Innova, Boston scientific | 1 | 0 |
| 16 | Scherer,J. et al. | NM | SG | NM | 1 | 1 |
| 17 | Plotnik, A et al. | 1 / 3.5 x 30 | PED | Pipeline Embolization Device (PED), Medtronic | 2 | 1 |
| 18 | Papageorgopoulou,C et al. | NM | SG | NM | 6 | 1 |
| 19 | Green, RJ et al. | 1 / 2.5 x 20 | BESG | Coronary Covered Stent PK Papayrus | 1W | 1 |
Self-expanding stent graft (Covered) (SESG), Balloon-expanding stent graft (Covered) (BESG), Stent-graft (SG), Self-expanding stent bare metal (SESB), Pipeline Embolization Device (PED), not mentioned (NM), 1 Week (1W).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



