1. Introduction
For over a century, root resection has been used as a treatment approach. This technique was initially introduced by Farrar in 1884 and subsequently adopted and developed by many other clinicians [
1]. Today, there is a distinction between the procedures included in the resective techniques. The definitions of which are as follows: Root separation involves the sectioning of the root complex and the maintenance of all roots [
2]. Root resection involves the sectioning and the removal of one or two roots of a multi-rooted tooth [
2,
3]. Bicuspidization refers to sectioning a mandibular molar and treating the two sections like two premolars [
4]. Hemisection is defined as the removal of half of a tooth performed by sectioning the tooth, removing one root and it is frequently used with reference to lower molars [
3,
4].
These techniques are treatment approaches meant to extend the survival of compromised molars [
5,
6,
7,
8].
The main indications for resective root therapy include endodontic, periodontal, restorative considerations and combined Endo-Perio lesions, primarily of periodontic origin that cannot be managed otherwise [
7,
8,
9,
10,
11,
12,
13,
14,
15].
Table A1 presents a detailed overview of the indications.
In the past several decades, many studies have demonstrated successful outcomes in preserving teeth with root resection and hemisection [
5,
6,
7,
10,
16,
17,
18,
19,
20,
21,
22,
23]. However, the success of these procedures depend on multiple prognostic factors, including the amount of remaining bone support, the position of the tooth within the arch, the presence of parafunctional habits, and the overall periodontal status [
2,
5,
8,
13,
19].
Long term clinical success is achieved through the application of precise surgical technique followed by an appropriate prosthetic rehabilitation [
8,
13,
19,
20,
24,
25]. Prosthetic management of teeth treated with resective techniques is pivotal to longevity and success. The use of full-coverage crowns, single or splinted, aids in the even distribution of occlusal forces, protects the remaining tooth structure and provides oral hygiene. This minimizes the risk of fracture, secondary caries and periodontal disease resulting from plaque accumulation in the treated area [
7,
8,
13,
19,
20].
Nowadays, tooth extraction followed by dental implant placement has often become the preferred and chosen treatment in many cases [
26]. However, the high incidence of peri-implant complications, particularly in patients with a history of periodontitis, and the difficulty and unpredictable outcomes of managing these complications have renewed interest in resective therapy [
6,
10,
27,
28,
29,
30,
31,
32,
33].
This case series presents clinical situations in a private dental practice in which hemisection and bicuspidization were selected as treatment options to preserve compromised molars, also it shows the achievement of long-term functional outcomes by maintaining these teeth for several years.
2.1. Clinical Case No 1
A 45-year-old male patient non-smoker with non-contributory medical history came to our clinic the year 2009 complaining about a slight pain during eating at the right side of his mouth.
Clinical examination confirmed a localised gum inflammation on the lower right side of the mouth despite the good oral hygiene conditions of the patient. A 10mm narrow periodontal pocket was evidenced in the mesial root of the lower right second molar (#47) upon clinical examination and mobility was not present.
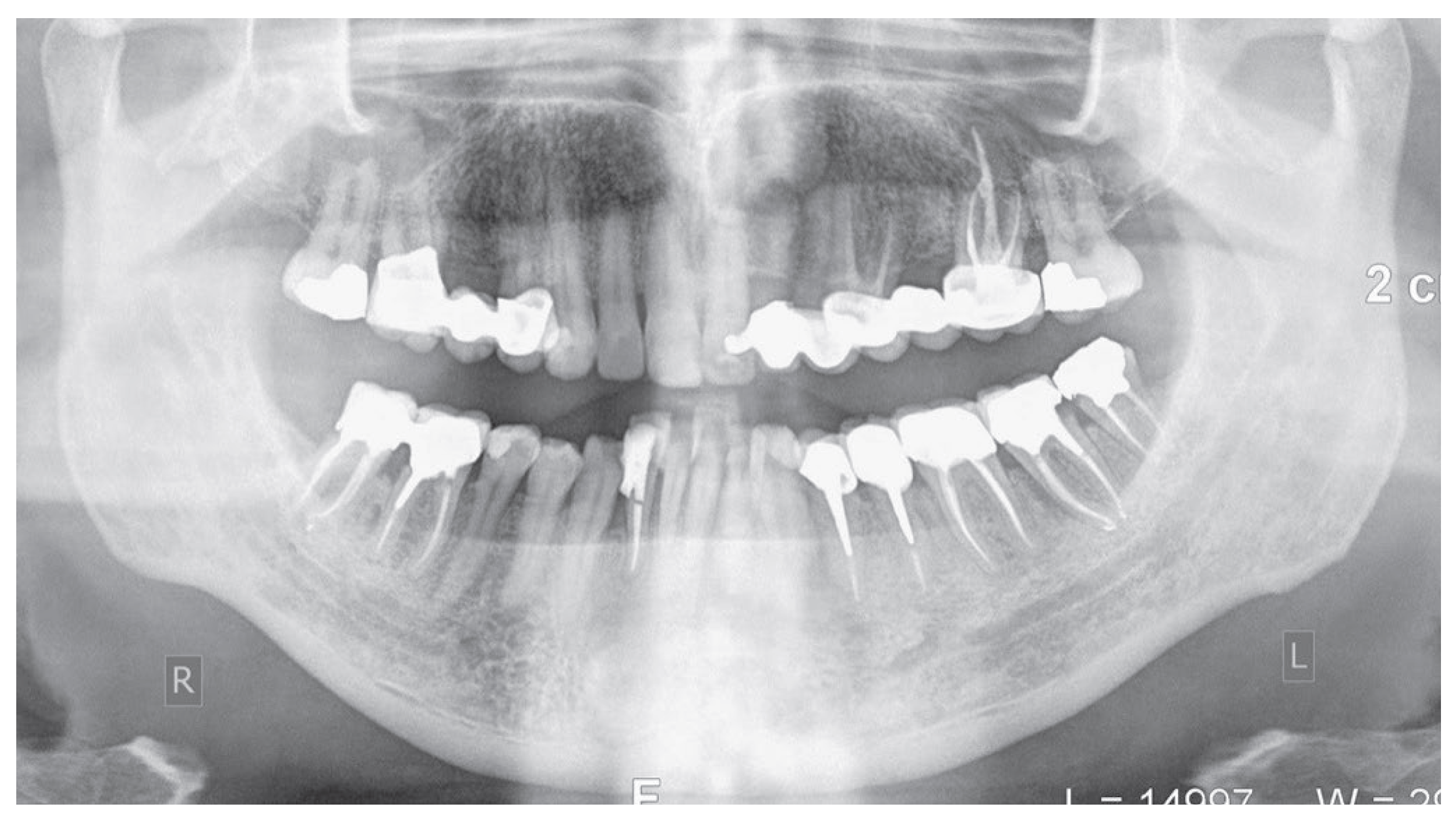
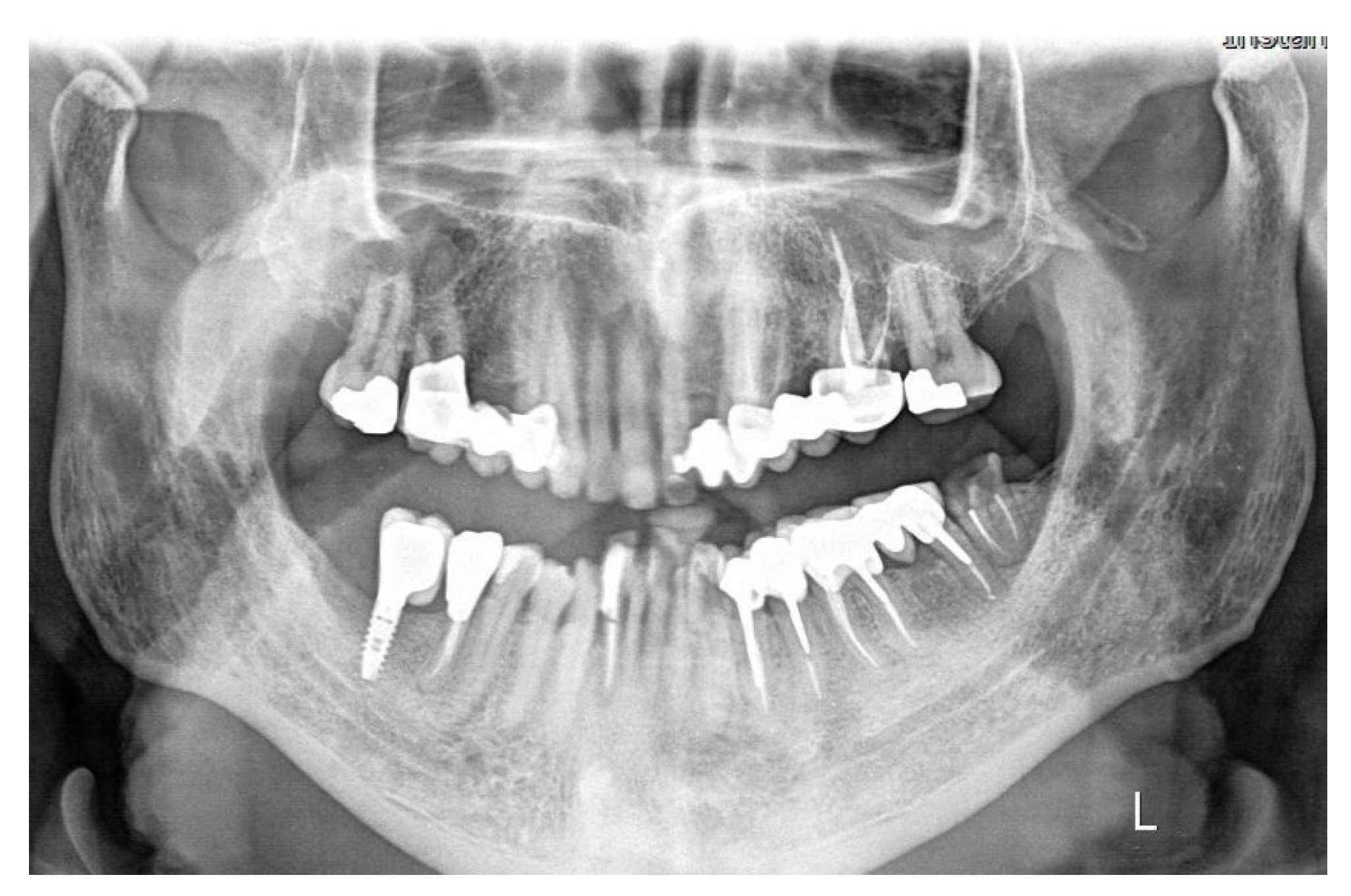
From radiographic examination with OPT (
Figure 1) a moderate periodontal bone loss on the lower right side of the patient was observed.
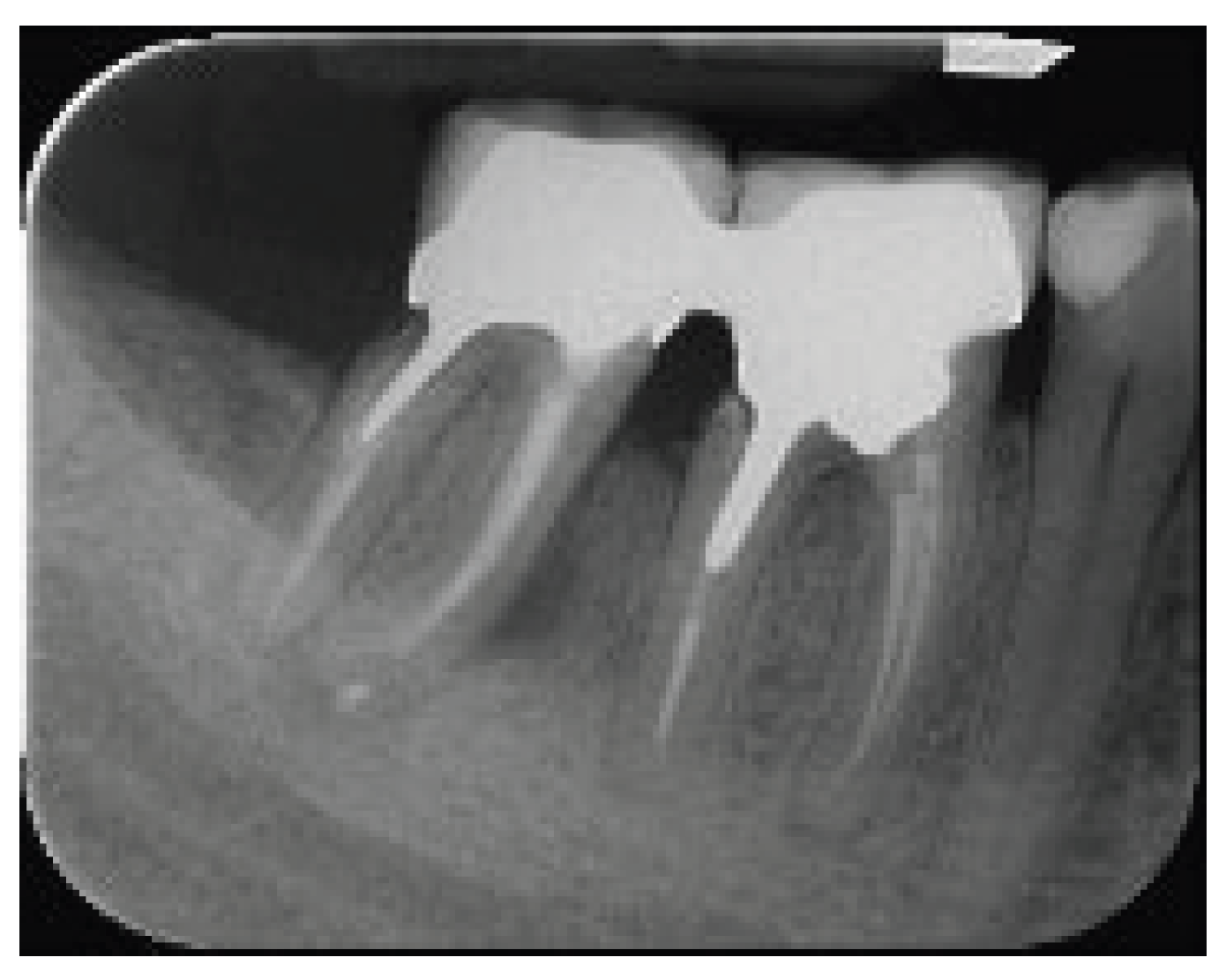
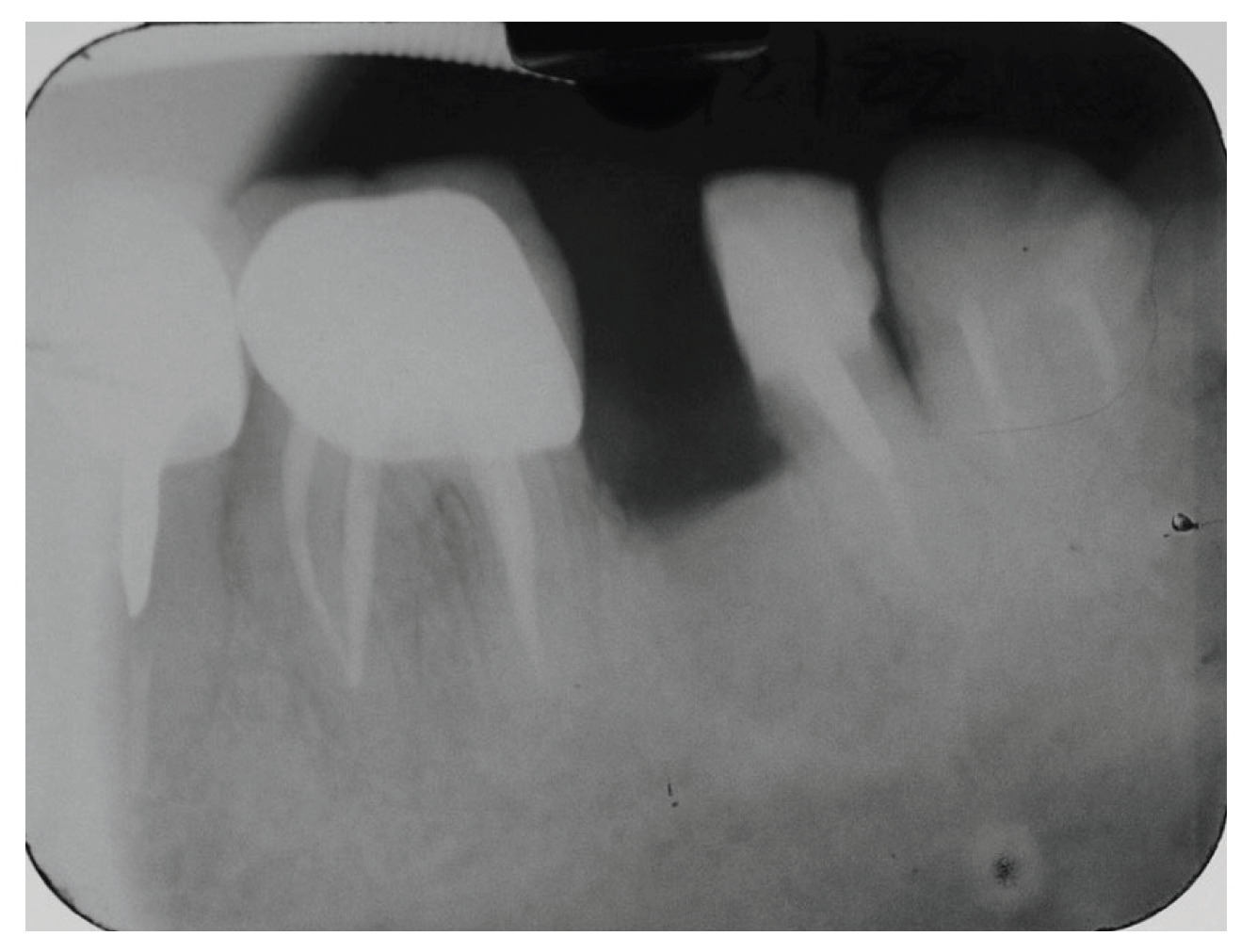
A periapical radiograph in the molar region of #46-47 teeth revealed that there was a radiolucent area in the middle third of the mesial root of tooth #47. This lesion was located mesially and it seems to be rather well defined in this area but coronally the bone loss had a J-shape appearance. In addition, subgingival carries in the distal roots of #47 and #46 were also detected (
Figure 2). Both teeth had been restored with cast posts and splinted fused to metal ceramic crowns. Crestal bone between the two teeth appeared to be moderately resorbed.
Based on the clinical and the radiographic findings, a root fracture of the mesial root of tooth #47 was suspected while the prognosis of both teeth were evaluated as unfavourable due to the presence of caries, the extensive restorations and the minimal remaining tooth structure.
After informing the patient with these findings, treatment options were presented. The tooth #47 had to be extracted while the prognosis of tooth #46 was poor due to extensive carious lesion. Thus, the first treatment option was extraction of both teeth #47 and #46 and placement of two implants supporting fixed crowns and the second treatment option was a more conservative approach namely extraction of tooth #47, hemisection and extraction of distal root of #46 and after healing, placement of an implant supported crown in the area of #47, retreatment of the mesial root of # 46, build-up of the remaining mesial root and a restoration with a zirconia crown. Patient mentioned that he was sceptical about implants, and he preferred to keep his natural teeth, therefore he decided to proceed with the second treatment option.
Endodontic retreatment of the mesial root of #46 was performed and extractions of the right second lower molar and the distal root of the first lower molar followed, which were done uneventfully and no attempt was made for socket preservation since the buccal and lingual bone plates were intact. Few days later, the retained mesial root was built-up with resin and fiberglass post and finally a zirconia crown restoration was inserted after 4 weeks. The patient was informed that the post extraction site must be left to heal for at least 5-6 months before placing an implant in the region of the missing tooth #47 and the distal root of #46. However, the patient did not return to office for implant placement in due time despite the recall notifications, but he appeared five years (2014) later complaining about a pain occurring upon chewing in the lower left side.
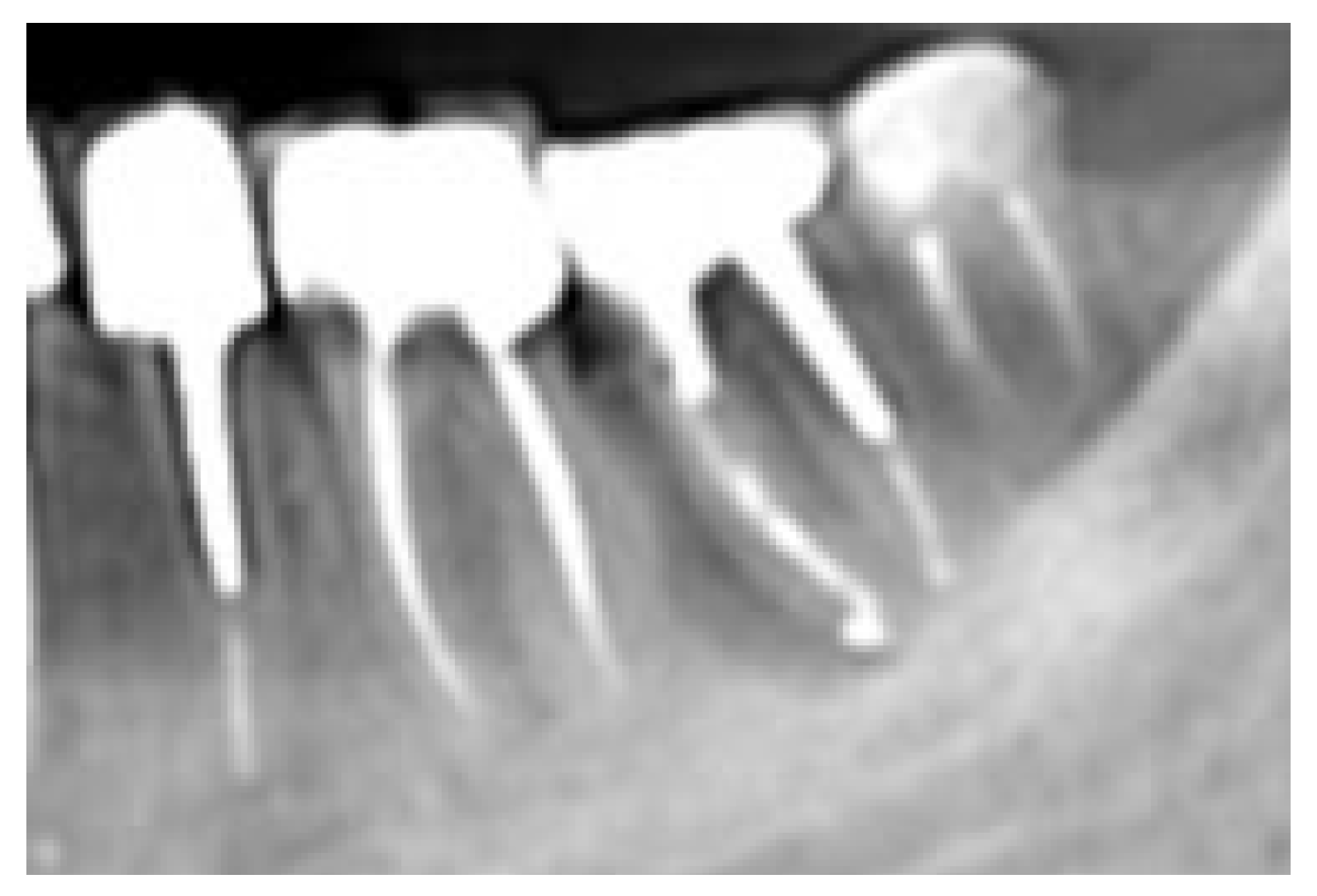
The clinical examination in this area revealed that the gingiva in the molar region was moderately inflamed, percussion of the molars elicited a slight sensitive reaction on tooth #37 and no mobility was present. However, a deep narrow pocket (16mm) in the buccal aspect of the mesial root of the second molar (#37) was found upon probing. A periapical radiograph in this area showed a J- shaped radiolucent area in the mesial root of the #37 tooth extending from crest of the alveolar ridge to the apex of the tooth (
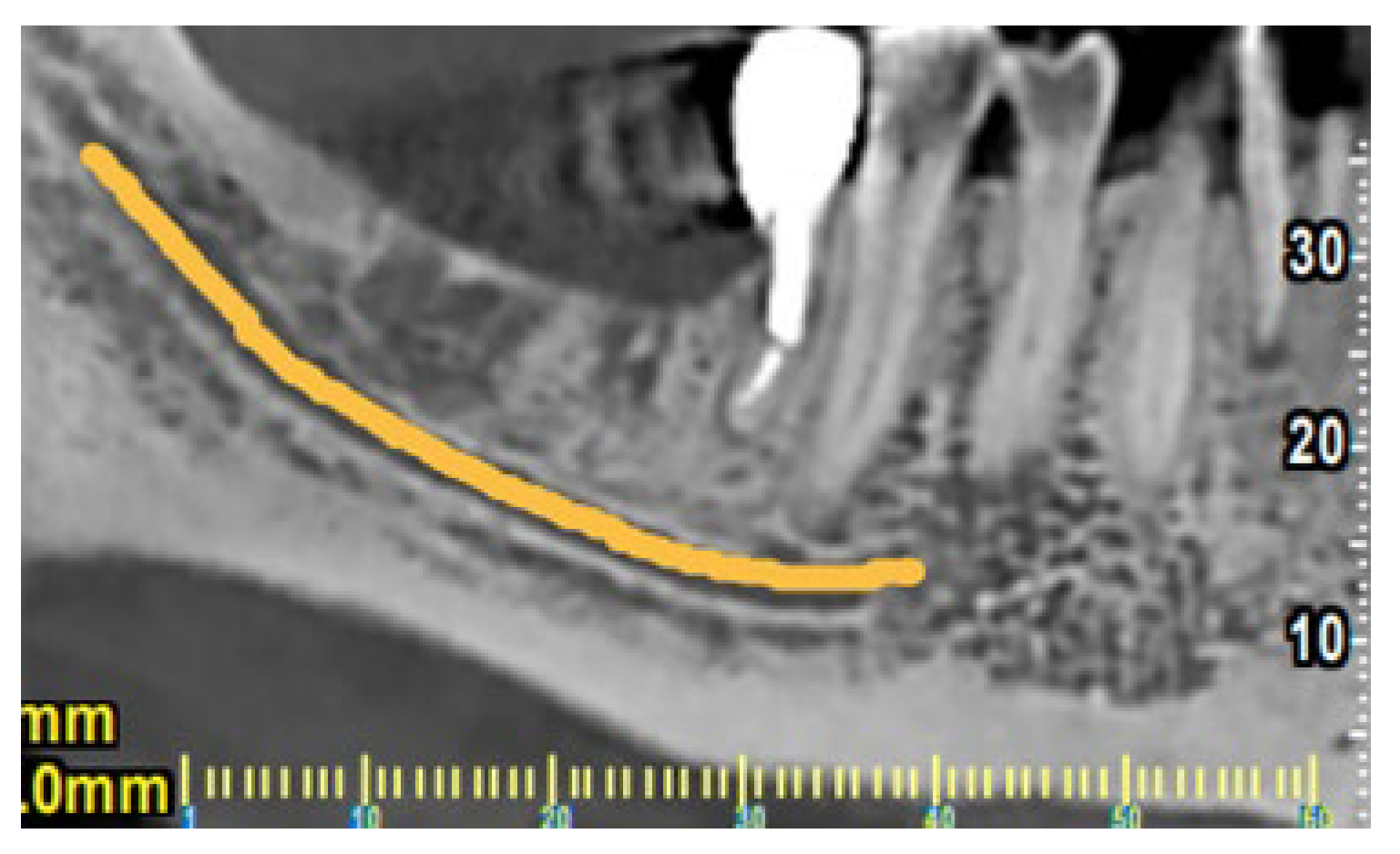
Figure 3). Based on these clinical and radiographic findings a CBCT examination of the lower jaw was suggested to evaluate firstly if there is a vertical fracture on mesial root of tooth #37 and secondly to verify the consistency and dimensions of the bone for implant placement in the region of #46-#47. (
Figure 4 and
Figure 5). From the CBCT evaluation the suspected vertical root fracture in the mesial root and the suitability for implant placement were confirmed [
34] (
Figure 4).
According to these findings the following treatment plan was proposed: a) placement of an implant in the region of the missing second molar in the right side as planned five years before and b) resection of the mesial tooth of the #37 followed by a bridge restoration supported on teeth #36 -distal root of the #37 and mesial root of #37 as a pontic. Since endodontic treatments of the teeth were acceptable without any periapical lesion and no caries were detected after removing the crowns, it was decided to proceed with the proposed treatment plan without retreatment. Hemisection was performed using the vertical cut method, without flap elevation. The vertical cut was made with a long diamond bur to divide the two roots and then the mesial portion of the tooth including the mesial root and the equivalent portion of the crown were extracted with premolar forceps [
4,
12,
13]. Postsurgical radiograph was taken to verify that no undercuts and ledges were left [
13,
25](
Figure 6). No attempt for socket preservation was made and the extraction site was left to heal normally.
The patient was advised to return to the referring GP for the placement of the prosthetic reconstruction [
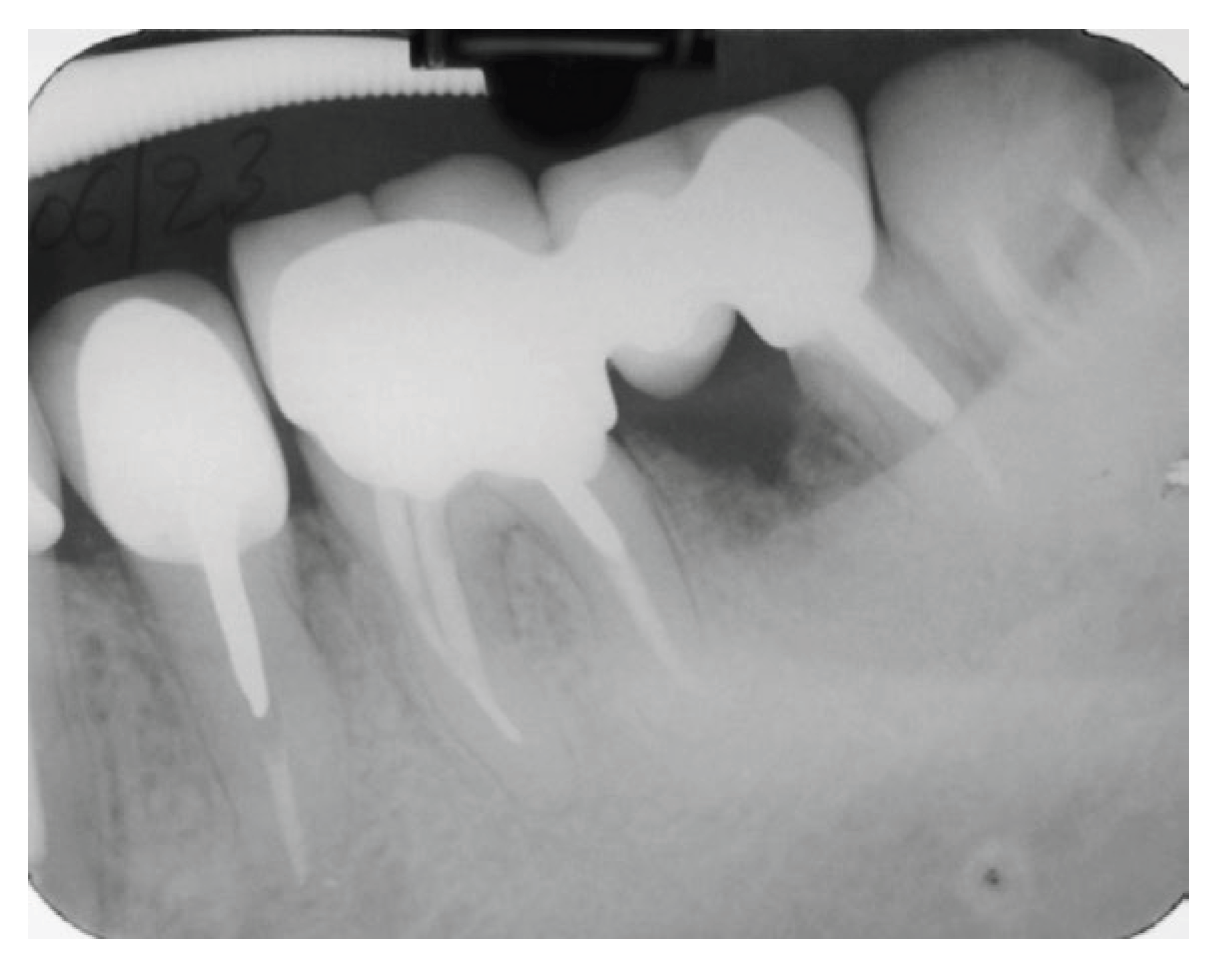
10]. The prosthetic rehabilitation was fitted after the healing of the extraction socket and special care was given to minimize the occlusal forces especially on the distal root of #37 tooth. A follow up X-ray taken one year after restoration revealed an uneventful ongoing healing of the extraction socket (2016) (
Figure 7).
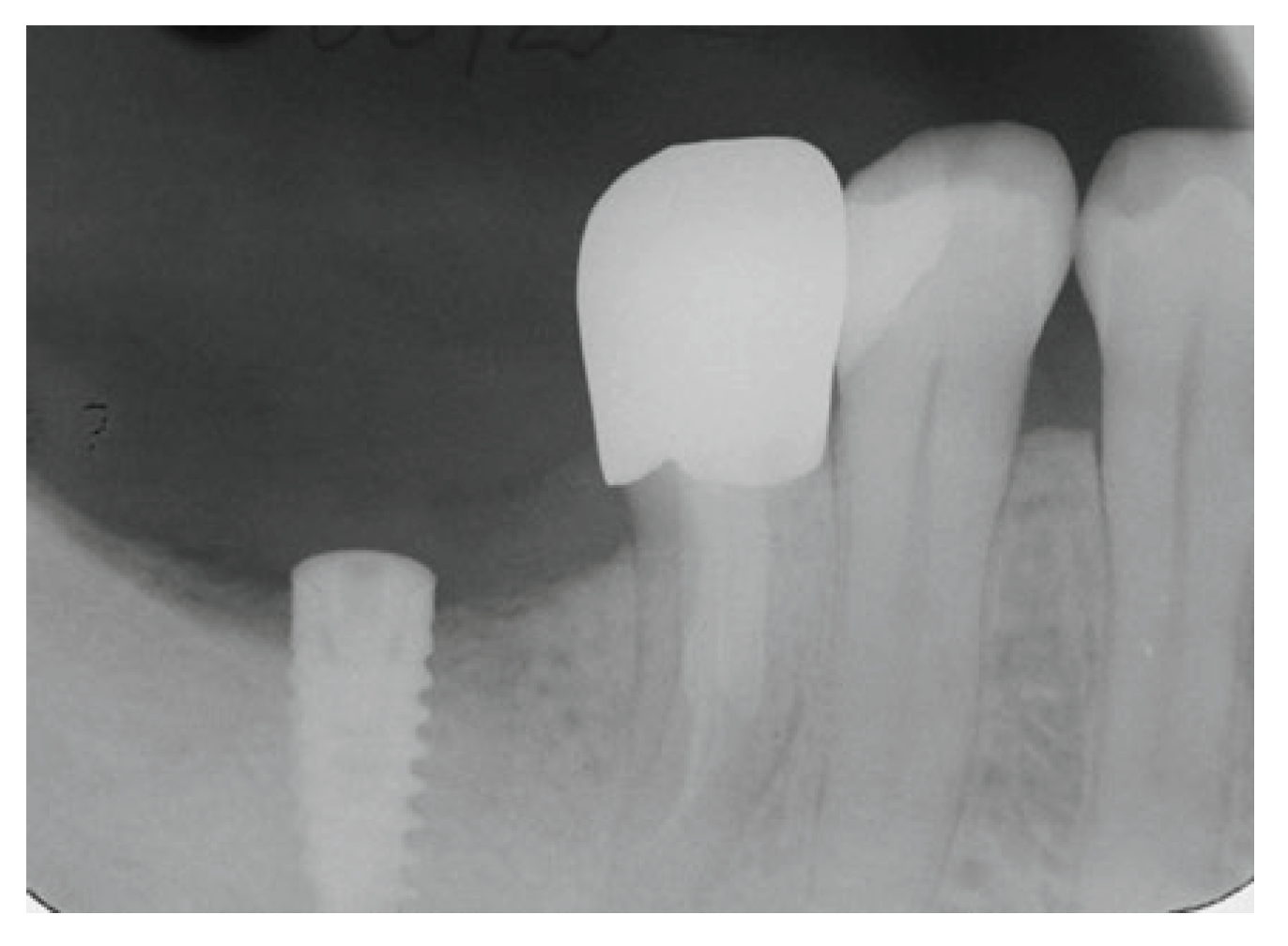
On the other site, namely in the area of #46-#47, according to CBCT measurements, it was decided to place only one MIS SEVEN implant having a 10 mm length and 4.20 mm diameter for replacement of missing teeth #47 and distal root of #46. Implant placement was done routinely, radiograph taken 4 months after placement showed an excellent healing and the patient referred to GP for the final placement of implant supported restoration (
Figure 8)
Follow up examination five years after completion of the treatment (2021) (
Figure 9) (
Figure 10), revealed that both right and left sides were functioning and having healed properly. The patient had no complaints, and no radiographic lesions were present.
2.2. Clinical Case No 2
A 50-year-old female patient referred to our clinic the year 2017 complaining of a recent growing pain and discomfort in the lower left posterior region. Clinical examination revealed a deep and narrow periodontal pocket around the mesial root of the tooth #36, moderate local inflammation on the buccal gingiva with overall good oral hygiene in the mouth. No mobility was present. Initial radiographic examination showed a periapical radiolucency associated with the mesial root of endodontically treated tooth #36 (
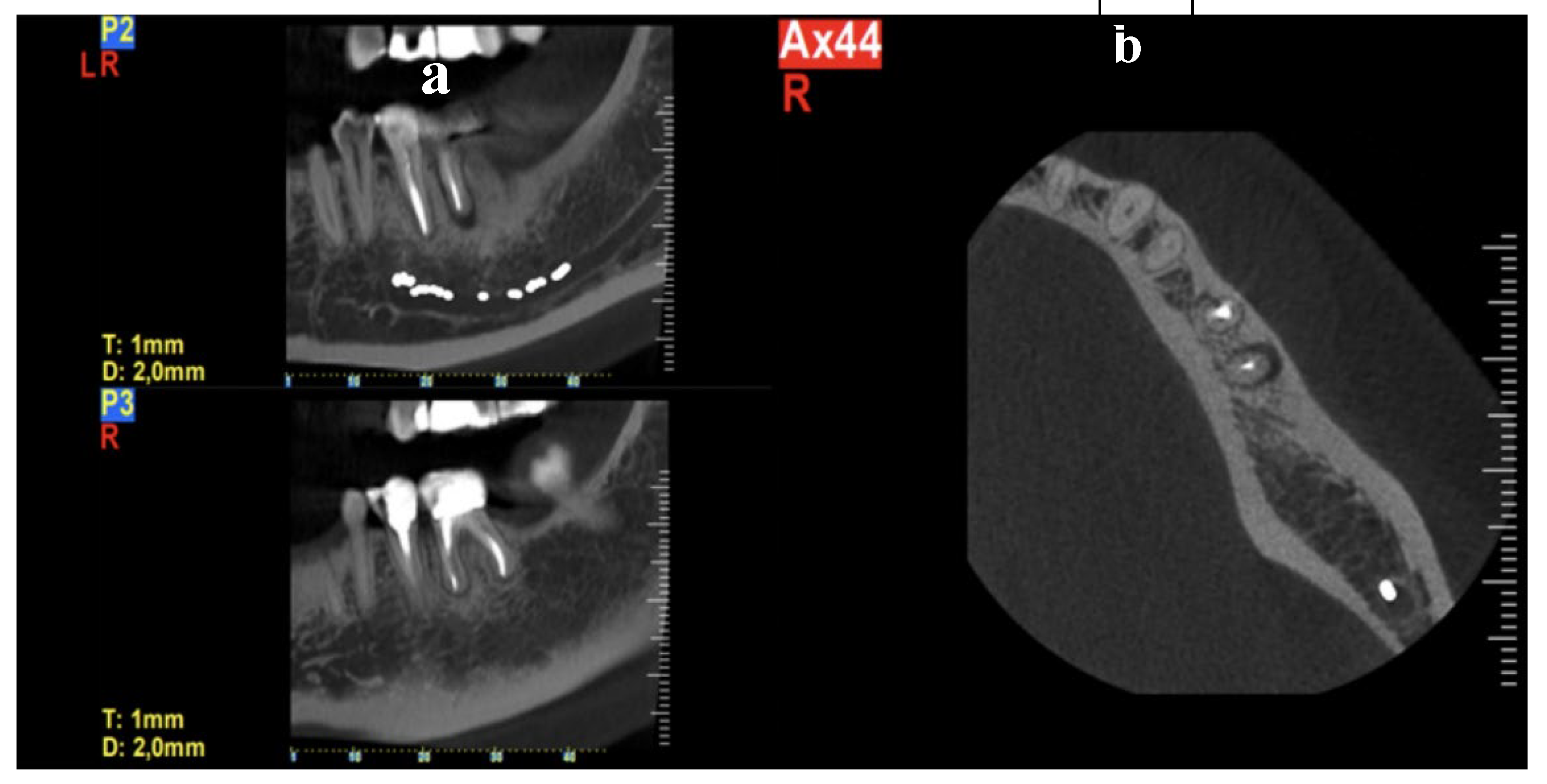
Figure 11). Based on patient symptoms and the clinical findings, an indication of a vertical root fracture of the mesial root was established and the patient was referred for a CBCT examination in order to confirm the diagnosis if possible. CBCT demonstrated a localized lesion extending along the buccal surface of the mesial root confirming the presence of a vertical root fracture in this root (
Figure 12).
Treatment options were presented to the patient included: a) Extraction of the tooth and placement of an implant b) Extraction followed by bridge restoration of the region using the teeth #35 and #38 as abutments and C) Hemisection of #36 and a crown restoration. For the patient the placement of an implant was not an option. The bridge restoration between #35 and #38 presented some technical difficulties since the tooth #38 was mesially merged due to the fact that there was no restoration after the early extraction of tooth #37 rendering endodontic treatment a possible option. In addition, a gingivectomy around the tooth was needed for crown lengthening. The patient considered this scenario as an overtreatment. So, the only remaining option was to maintain as much as possible of the substance of tooth #36 and try to restore it in the most minimal and long-lasting way possible. Having this in mind and for better masticatory load distribution and stability [
8,
19,
35,
36], the alternative of a bridge between #35 and distal root #36 was proposed to the patient but she refused to proceed in this option. In order to come along with the patients requests and produce a stable and long-lasting restoration, a solution of restoring the distal root of tooth #36 with a crown having a mesial wing extension was selected. The wing extension would be bonded in the distal occlusal part of tooth #35.
The treatment proceeded with hemisection of the first molar (#36), a full thickness mucoperiosteal flap was elevated and since the fracture was visible buccally, hemisection was performed using the vertical cut method, using a long-fissured diamond bur. The mesial root along with the equivalent part of the crown extracted using premolar forceps [
4,
12,
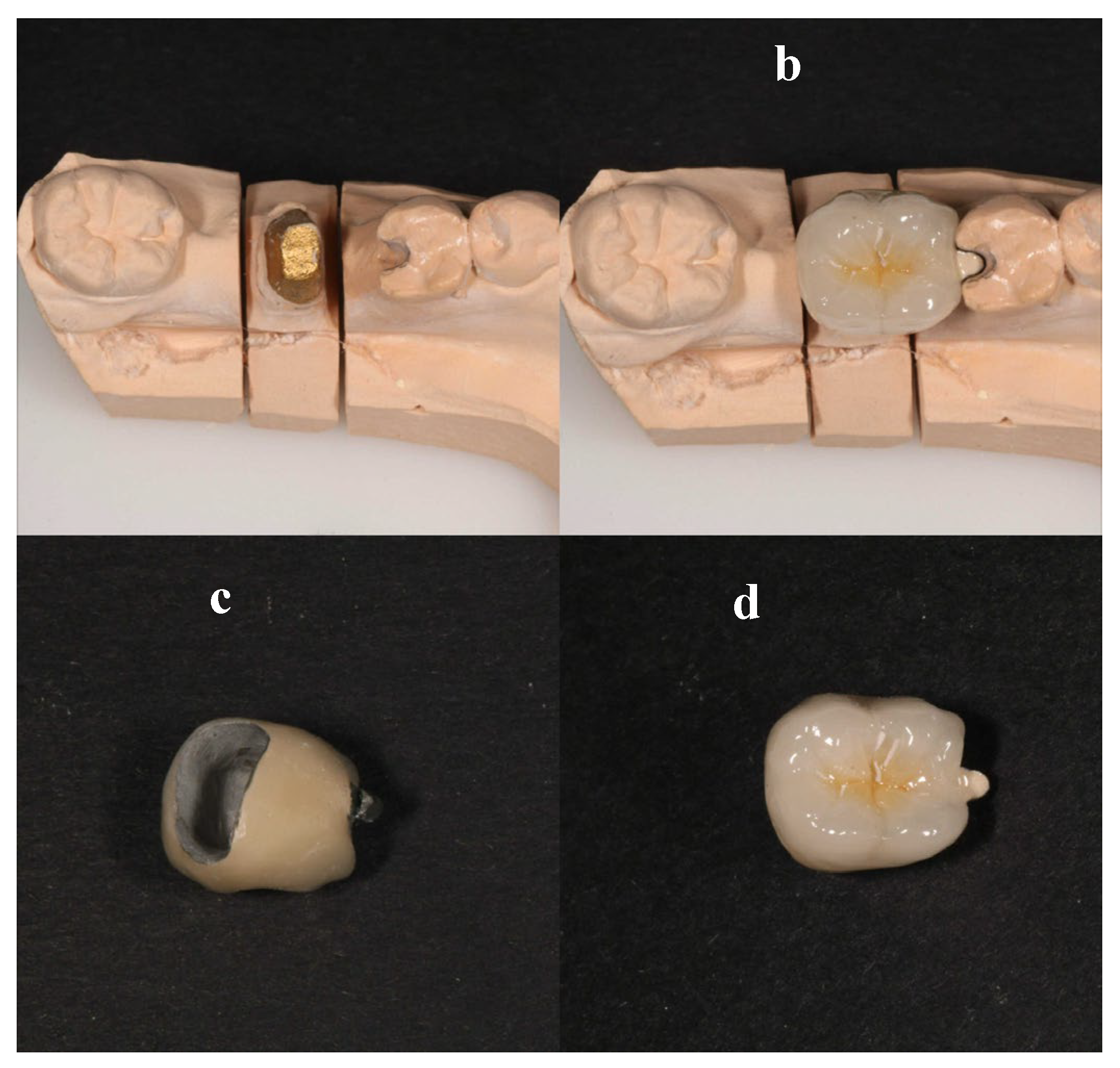
13]. Sutures were places using 4-0 vicryl sutures. The patient was given verbally and written post-op instructions. After 10 days a recall appointment was scheduled. At the recall appointment normal socket and soft tissue healing was noted and the sutures were removed. After 15 days of sutures removal, the patient returned to office, the remaining abutment was shaped, and a provisional crown was manufactured chairside and cemented until proper healing of the socket occur. When healing was completed, preparation of the remaining tooth crown was finished, a special notch on distal occlusal surface on tooth #35 was made, an impression was done and a porcelain crown fused to metal having a mesial wing was manufactured. The mesial metal wing was designed to be bonded on the prepared notch on tooth #35. (
Figure 13)
Figure 14.
Six months follow-up, after cementation of the crown.
Figure 14.
Six months follow-up, after cementation of the crown.
2.3. Clinical Case No 3
A 55-year-old female patient with no contributory medical history and non-smoker referred by a periodontologist to our clinic for endodontic evaluation and if possible, retreatment of the mesial root of the lower left first molar. According to referring records and as it was indicated in the accompanying periapical radiograph (
Figure 15), the initial treatment plan included removal of the distal root of tooth #36. Study of the periapical radiograph showed a furcal involvement in the tooth #36 and a periapical lesion of the untreated distal root. Clinical investigation revealed a type III furcation involvement, first grade mobility combined with deep periodontal pocket in the furcation area while the presence of initial caries was detected at the distal margins of the porcelain fused to metal crown. Based on these findings, removal of the crown was a necessity in order to examine if the tooth crown was restorable. As shown in
Figure 16, a periapical radiograph taken after removal of the crown revealed the presence of caries in the disto-buccal part of the tooth and the existence of two distal roots having a furcal involvement in between them.
The patient was informed about these findings, and the treatment options were as follows: a) Extraction of the tooth and an implant placement. This option was immediately excluded by the patient since she had a previous experience of a failing implant placement on the right side of her mouth. b) The second option offered was to perform a classical root resection, to maintain the mesial roots and to remove the distal buccal root which had a poor periodontal status and finally, after endodontic treatment, to restore the two separated roots as premolars with splinted crowns. Another alternative was to replace also the crown of tooth #35 and to splint it with the restoration of tooth #36, but this was excluded by the periodontologist, since it would render daily oral hygiene more difficult.
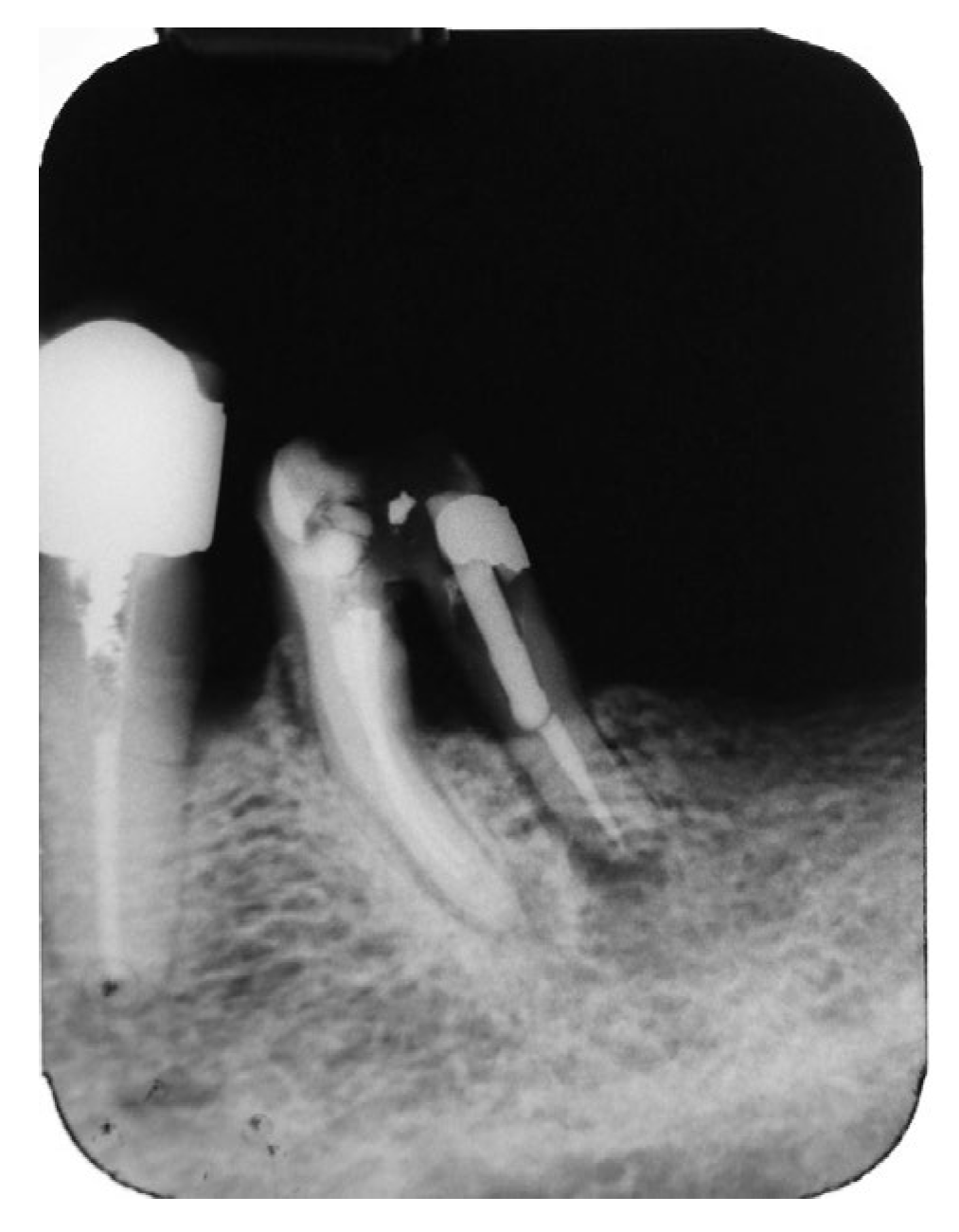
According to the second treatment plan, we proceeded with endodontic treatment and built-up restoration with composite resin and a prefabricated metal post of the disto-lingual root under dental dam isolation followed by initial separation of mesial and distal roots followed by separation of the two distal roots and extraction of the severely compromised disto-buccal root (
Figure 17).
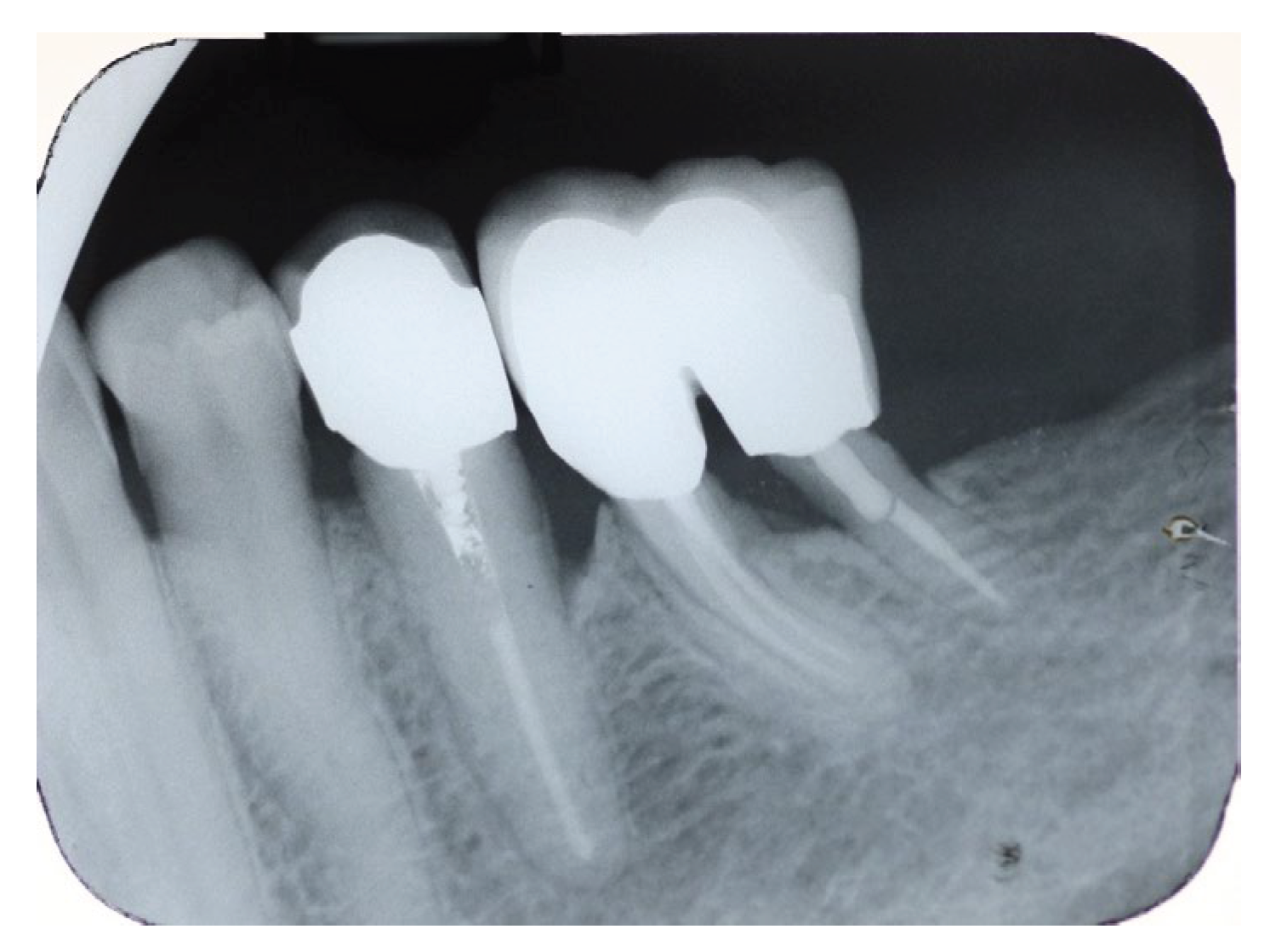
After socket healing, the patient returned for the final restoration which consisted of two splinted metal-ceramic crowns in the separated roots. Upon completion of restoration the patient referred to the periodontologist for further periodontal maintaining program. A six months recall examination revealed that the restoration was functioning well with no clinical signs of inflammation and only a slight mobility of the tooth was present. Patient was able to maintain oral hygiene properly according to instructions. Radiographically no lesions were evident and bone levels were stable (
Figure 18). The patient was advised to keep strictly the regular periodontal recall examination program.
Recall examination after 6 years showed that the tooth was fully functional and no signs of inflammation clinically or radiographically were present (
Figure 19).
3. Discussion
In recent years, the concept of tooth preservation has gained renewed attention as a biologically driven alternative to extraction and implant placement. While implant therapy has been considered for some decades the gold standard for tooth replacement in most situations [
37], the incidence of periimplantitis has risen steadily over the years [
27,
28,
29,
30,
31,
32,
33,
38]. Numerous studies have evaluated resective techniques such as root resection, hemisection and bicuspidization, over the past decades, and demonstrated that these clinical approaches can achieve successful clinical outcomes when case selection, periodontal stability and restorative planning are appropriately addressed [
4,
8,
19]. Recent case reports continue to document successful management of compromised molars that treated with resective techniques, highlighting the effectiveness of these minimally invasive procedures combined with an multidisciplinary approach [
39,
40]. In the presented clinical cases, the treated teeth were maintained in function following hemisection or bicuspidization, these outcomes emphasize the importance of careful case selection and the coordinated consideration of endodontic, periodontic and restorative factors within a multidisciplinary treatment approach.
It must be mentioned that in the presented clinical cases in our study, endodontic treatment or retreatment, was performed before the surgical resective procedures. This approach is supported by the literature which illustrates the predictability and overall success of this sequence of care [
2,
3,
12,
41]. However, cases in which resection can be performed on a tooth with a vital pulp (vital root resection), particularly in periodontally compromised multirooted teeth are also described in the literature [
42,
43,
44]. Several complications have been reported in association with this approach, some of them are difficulty achieving adequate anaesthesia due to chronic inflammation, challenges in performing proper endodontic treatment due to altered tooth morphology, potential pulp calcification, internal resorption resulting from chronic inflammation, pulp necrosis and severe postoperative pain [
12,
13,
42]. As a result, this approach remains controversial, as success rates vary widely and it is considered high-risk [
43,
44]. The prognosis of vital root resection is generally poorer compared to cases where endodontic treatment is performed before the root resection.
From a clinical perspective, prosthetic rehabilitation is essential in the treatment, as even a successful root resection or hemisection will eventually lead to tooth loss within a certain period, if not followed by proper prosthetic rehabilitation. The most frequent failures were due to fracture, secondary caries, or recurrent periodontal disease resulting from plaque accumulation in the treated area [
45]. In our clinical cases, full coverage crowns were used to restored the preserved roots, as they improve the distribution and control of occlusal forces, protect the tooth from secondary caries and promote an environment that supports effective oral hygiene [
3,
4,
13,
15,
36,
45]. Special attention was given to the management of parafunctional habits [
19] and occlusal stresses to avoid possible fractures [
4,
11,
15,
19,
41,
46].
The decision about whether a crown restoration should be single, part of a prosthetic restoration, or splinted to an adjacent tooth was taken by factors including the remaining roots, the surrounding bone support, the tooth position in the arch, and the overall prosthetic treatment plan [
4,
8,
12,
20,
24]. In the first clinical case, on the lower right side the mesial root was retained and restored with a full coverage crown, while an implant was positioned and placed distally, resulting in favourable distribution of the occlusal stresses. In the same clinical case, a bridge on the lower left side was manufactured and not a single crown on distal root since the literature indicates that when a distal root serves as a last abutment it is preferable to splint it so as to enhance stability and load distribution forces [
12,
19,
22,
24]. In the second case, as the patient declined splinting the distal root with bridge or crowns, an alternative yet effective solution was provided to the patient using an occlusal rest to reduce the risk of root fracture [
8,
13,
19]. Lastly, in the third case, the two divided roots were splinted with two crowns, following the periodontologist recommendation to avoid including the premolar in the restoration. All three cases, were restored with attention to minimize excessive occlusal forces, allowing adequate oral hygiene while taking into consideration patient preferences.
These clinical decisions are also supported by the broader literature. Teeth functioning as terminal abutments demonstrates lower success rates because they are subject to greater occlusal forces [
5,
19,
22,
24], further reduction of the prognosis is observed when there is limited bone support around the retained root [
4,
7,
8]. For this reason, splinting or using the retained root as an intermediate bridge abutment when there is low bone support is generally recommended to improve force distribution and avoid fracture, especially in mandibular molars which is the main cause of failure [
4,
5,
8,
10,
19], when possible, these teeth should not be used as terminal abutments [
8,
20].
As mentioned above long-term survival and success of root resection and hemisection procedures has widely been examined. It has been found from clinical studies that the survival rates vary and depend upon careful case selection and well designed restorative management. Bergenholtz et al., Hamp et al., and Klavan et al. at early investigations reported high success rates of 91-94% on follow-up periods ranging from one to ten years, demonstrating under favourable periodontal and restorative conditions how reliable these procedures can be [
16,
17,
18]. However, studies with bigger observation period have revealed greater variability in rates, Langer et al. documented a success rate of 62% at ten years, while the success rate of 67,9% at the same timeframe was reported by Bühler et al., emphasizing the difficulties presented in preserving stability for long term period in more complex or less favourable cases [
5,
22]. Carnevale et al. reported survival rates approaching 99% at five years of observation and more that 93% at ten years, while Hou et al. observed perfect longevity in their cohort over a period ranging from six to thirteen years [
7,
21]. A comparison between root-resected molars and single molar implants, followed for thirteen to fifteen years, was conducted by Fugazzotto et al. and resulted that most resected molars had comparable results to single molar implants with survival rates of 95-100%, regarding distal roots of mandibular molars a notable difference was evidenced with a lower survival rate at approximately at 75% [
19]. Additional long-term information further support and confirm the durability of these treatment approaches, Megarbane et al., reported 94.8% survival after forty years of follow-up, and Schmitz et al. found a success rate of 93% after seven years of observation [
6,
20]. A progressive decline in survival was noted by Falabella et al. survival from 97.735 to 90.91% at ten years, indicative of the natural cumulative effects of long-term function [
10]. In a retrospective study Derks et al. found 90,6% survival rate after 10 years of observation [
23]. By comparison, the substantially lower survival rates of 58% at five years report by Oh et al. likely reflects a less advantageous interdisciplinary approach [
24].
In general, these findings prove that root resection and hemisection can also give satisfactory long-term outcomes, similar to those provided by treatment with implants. Lege artis endodontic treatment, controlled occlusal forces, stabilization of periodontal support as well as prosthetic restorations designed to limit biomechanical stress, remain essential components of success. Additionally, hemisection, bicuspidization and root resection, as illustrated in the clinical cases reported, allows the partial preservation of the natural tooth over a long period and contribute to the preservation and healing of the surrounding bone. Also, it can be noted that in the follow-up radiographs of the cases presented above the bone preservation is evident over the years, suggesting that this approach allows future implant placement if required under more favourable biological conditions.
Figure 1.
Initial OPT X-Ray.
Figure 1.
Initial OPT X-Ray.
Figure 2.
Periapical X-Ray of #46, #47.
Figure 2.
Periapical X-Ray of #46, #47.
Figure 3.
Periapical X-Ray of tooth #37 showing a J- shaped radiolucent area at the mesial root.
Figure 3.
Periapical X-Ray of tooth #37 showing a J- shaped radiolucent area at the mesial root.
Figure 4.
CBCT section of tooth #37 illustrating the pattern of bone resorption alongside the mesial root.
Figure 4.
CBCT section of tooth #37 illustrating the pattern of bone resorption alongside the mesial root.
Figure 5.
CBCT of the lower right region of the mandible for studying bone dimensions and anatomical elements for implant placement.
Figure 5.
CBCT of the lower right region of the mandible for studying bone dimensions and anatomical elements for implant placement.
Figure 6.
Postsurgical X-Ray following hemisection of tooth #37.
Figure 6.
Postsurgical X-Ray following hemisection of tooth #37.
Figure 7.
X-Ray at 1 year recall, after restoration. An ongoing bone formation on the extraction socket is evident.
Figure 7.
X-Ray at 1 year recall, after restoration. An ongoing bone formation on the extraction socket is evident.
Figure 8.
Periapical X-ray 4 months after implant placement showing excellent healing.
Figure 8.
Periapical X-ray 4 months after implant placement showing excellent healing.
Figure 9.
5 years follow up periapical X-Ray. Excellent bone regeneration is evident with proper crestal bone height.
Figure 9.
5 years follow up periapical X-Ray. Excellent bone regeneration is evident with proper crestal bone height.
Figure 10.
OPT at 5 years recall showed an excellent healing at both sites.
Figure 10.
OPT at 5 years recall showed an excellent healing at both sites.
Figure 11.
OPT of the patient with evident lesion in the mesial root of the #36.
Figure 11.
OPT of the patient with evident lesion in the mesial root of the #36.
Figure 12.
a) Coronal view, radiolucency around the mesial root b) Axial view, a very localized, angular, fissure-like pocket on the buccal surface of the mesial root of tooth 36 raises suspicion of a possible crack or fracture in the mesial root.
Figure 12.
a) Coronal view, radiolucency around the mesial root b) Axial view, a very localized, angular, fissure-like pocket on the buccal surface of the mesial root of tooth 36 raises suspicion of a possible crack or fracture in the mesial root.
Figure 13.
a) occlusal view of the dental cast b) dental crown placed on the cast c) dental crown with mesial wing d) occlusal view of the crown.
Figure 13.
a) occlusal view of the dental cast b) dental crown placed on the cast c) dental crown with mesial wing d) occlusal view of the crown.
Figure 15.
Initial Periapical X-Ray.
Figure 15.
Initial Periapical X-Ray.
Figure 16.
X-ray after crown removal showing the existence of the second distal root.
Figure 16.
X-ray after crown removal showing the existence of the second distal root.
Figure 17.
Postsurgical X-Ray after the built-up of the tooth and removal of the distal-buccal root of tooth #36.
Figure 17.
Postsurgical X-Ray after the built-up of the tooth and removal of the distal-buccal root of tooth #36.
Figure 18.
Recall X-ray after 6 months of the prosthetic rehabilitation.
Figure 18.
Recall X-ray after 6 months of the prosthetic rehabilitation.
Figure 19.
6 years recall X-Ray.
Figure 19.
6 years recall X-Ray.