
Submitted:
26 December 2025
Posted:
26 December 2025
You are already at the latest version
Abstract
Cryptococcal meningitis diagnosis at 62% is the leading cause of meningitis among adults with advanced HIV disease in areas with a high burden of infection. Despite attempts to improve treatment, in-hospital mortality remains unprecedentedly high. Disease complications associated with unmasking symptoms and relapse of fungal infections, delay in treatment increase the risk of individuals succumbing to cryptococcal meningitis. In this narrative review, we highlight published clinical trials evaluating the treatment of HIV-associated cryptococcal meningitis with survival as the primary endpoint. Aggregated clinical trial data show a significant decrease in survival from diagnosis to 88.5% at 2 weeks of treatment to 74% at 10 weeks of observation (p=0.001). The WHO standard of care was used as the control arm. Survival rates were similar between the control and trial arms. High in-hospital mortality remains a challenge for new survival-modifying treatments for cryptococcal meningitis. We provide evidence-based updates on cryptococcal meningitis treatment to inform new antifungal formulations or research approaches for improved outcomes. The consistency and generalizability of fungal clearance in the cerebrospinal fluid and the efficacy of antifungal drugs to clear fungi in the brain parenchyma remain unclear.
Keywords:
cryptococcal meningitis
; clinical trials
; antifungal therapy
; human immunodeficiency virus
; mortality improved regimen
; survival
1. Introduction
Cryptococcal meningitis (CM) is the leading cause of meningitis in people with advanced HIV disease, accounting for decreased hospital survival from admission to 85% (Interquartile range, (IQR); 76-%-87% survival) followed by tuberculous meningitis at 21% [1]. Though the highest burden of disease is reported in low- and middle-income countries [2], the cases in the developed world show high in-hospital mortality (~30%) compared to 19% global mortality estimates[3,4]. The global cryptococcal meningitis mortality rate of 19% is lower compared to 28%-33% mortality in the predominantly Caucasian (67%-73% of patient), young (age; 40 -70 years old), and male (79%-82%) patients with cryptococcal meningitis in the developed countries[3,4]. Unlike in low-income settings where HIV infection is the predominant risk factor for cryptococcosis (96%) [5], several studies in developed countries show multiple comorbidities contributing to cryptococcosis including: HIV infection (44.4%), exposure to corticosteroid therapy (28.3%), malignancy (25.5%), smoking (20.0%), transplant-related conditions (18.9%), and presence of lung disease (18.2%) [3,4].
Though multiple comorbidities are associated with cryptococcosis, the pathogenesis, the adverse outcome, and the degree of disease impairment among patients are similar across the globe. Frequently observed abnormalities include: hearing impairment (16%), muscle weakness (40%), cognitive deficits (33%), hydrocephalus (with need for a ventriculoperitoneal shunt) (7.4%), stroke (33%), and relapse occurring in 23% of patients[3]. The finding that 23% of patients with cryptococcal meningitis in the United States cohorts will experience relapse of infection/disease and the high mortality rates with treatment compared to the rest of the world [2,3,5,6], aligns with the hypothesis of possible limited antifungal drug bioavailability and persistence of disseminated fungal infection in deep tissue niches. Unfortunately, no human study has attempted to investigate whether fungal clearance in CSF correlates with clearance of disseminated fungal infection in tissues [7].
Despite attempts to improve treatment, high mortality rates remain a concern with mortality of up to 45% reported by 10 weeks of treatment [8,9]. Early diagnosis and treatment are complicated by disease presentation and high burden of concomitant comorbidities in the developed world and high burden of infections with similar symptoms in areas with high burden of advanced HIV disease [2,8,10]. Despite evidence of effective antifungal therapy, mortality remains high and unpredictable due to complications impacting survival [7]. The individuals at risk of death are those with significantly low systemic evoked immune response in peripheral and central nervous system (CNS) compartments [11].
2. Materials and Methods
We searched PubMed for primary peer-reviewed articles on cryptococcal meningitis clinical trials conducted between January 2000 and January 2024 using the search term “Cryptococcal meningitis Clinical Trials” (Figure 1). Our goal was to consolidate knowledge of survival using improved regimens and emerging therapies, and to determine how different regimens have impacted survival in clinical trials over the past 24 years.
3. Results
3.1. Modern Therapeutic Advances for Cryptococcal Meningitis
Therapeutic advances to improve survival have relied on the rapid killing of the fungus associated with higher early fungicidal activity based on fungal clearance from the CSF compartment. This infection and fungal clearance in the CSF compartment are used as an accessible means to monitor the kinetics of antifungal efficacy in the CNS [7]. The fungal killing and clearance from the CSF using antifungal drugs is reported as the early fungicidal activity (EFA) reported as x log10 colony forming units/ml of CSF/day[12]. Even better, is the early fungicidal activity reported with the use of a combination of antifungal drugs which surmount rapid and synergistic effects to fungal killing and fungal clearance compared to antifungal monotherapies [13]. Though the rate of fungal clearance in the CNS is determined by negative CSF fungal culture conversion,[14] the holistic view of the host can inform unmet host-directed needs for personalized therapy. Consistently, individuals with low evoked and poorer immune response experience the highest risk of succumbing to cryptococcal meningitis compared to their counterparts with elevated immune responses [15,16,17]. This group of patients with paucity of immune response present an opportunity for trials of adjunctive immune therapy to improve survival.
3.2. Evolution of Antifungal Clinical Trials to Improve Survival with Cryptococcal Meningitis
In attempts to improve the quality of life and survival following HIV associated cryptococcal meningitis, new antifungal regimens and patient-centered interventions emerged in the era of peak HIV-related deaths prior to increased availability of antiretroviral therapy (ART). Today, the persistently low survival rates among hospitalised patients even with WHO-recommend antifungal therapy still drive the need to do more trials [18]. HIV infection is prevalent in Africa, and the hotspots of the disease also have the highest burden of HIV-associated cryptococcal meningitis. Most global cryptococcal meningitis clinical trials are conducted in Africa, particularly in Uganda, Malawi, South Africa, Tanzania, and Botswana, with some in other parts of the world (Map: Figure 2). In Asia, most trials are in Thailand, Vietnam, and China. In North America, trials are in the US, Canada, Indonesia, and Laos.
Cryptococcal meningitis remains a significant problem for treatment and survival improvement in Africa, despite a 40-year HIV epidemic. Since clinical trials emerged, global public health participation has increased substantially, leading to improvements in survival (Figure 3). Trials compared trial regimens with the WHO-recommended standard of care for antifungal treatment of cryptococcal meningitis (Figure 3). The WHO recommended regimen includes Amphotericin B Liposomal (Ambisome) or deoxycholate formulations for induction therapy, Fluconazole consolidation combination therapy, and Fluconazole maintenance monotherapy. Despite variations in survival on trial regimens, 96% of randomized trial regimens used old antifungal molecules tested against the standard WHO regimen (Figure 4). Amphotericin B and Fluconazole were the standard regimen in 92% of trials (25/27 trials), while Amphotericin B and Fluconazole were the standard regimen in 4% of trials (1/27 trials) (Figure 4 and Table 1).
The published clinical trial literature in the last 24 years show the field has maintained the old antifungal formulations of Amphotericin B, (discovered in 1953) [37], Flucytosine (discovered in 1957) [38], and Fluconazole (discovered in 1978) [39], as the primary antifungal candidate models in cryptococcal meningitis clinical trials (Figure 4 and Supplementary Table S1). The new antifungals in cryptococcal meningitis clinical trials are reconfigured antifungal formulations of amphotericin B (e.g., intravenous liposomal amphotericin B, amphotericin B deoxycholate or the oral lipid nanocrystal formulation of amphotericin B at 0.7-1 mg/kg body weight). Fluconazole 800mg - 1200mg daily, or Flucytosine 100mg/kg four times daily administered in inductive phases (first 7 -14 days, depending on fungal clearance colony-forming units in CSF cultures. The consolidation phase with 800mg daily of 6-12mg per kg body weight of Fluconazole for 8 weeks after induction therapy. The maintenance phase is implemented with 200mg daily dose of Fluconazole for secondary prophylaxis [40,41].
Survival significantly decreased from admission to 2 weeks and 10 weeks of therapy, regardless of the trial regimen (Figure 3). Aggregated data from 14 studies before and 12 studies following ART optimization showed similar survival rates, with or without ART initiation after cryptococcal meningitis diagnosis [26]. Other factors, besides antifungals, could contribute to the significant difference in survival among patients with cryptococcal meningitis on antifungal therapy. Reasons for persistent mortality after initial hospital discharge include immune reconstitution inflammatory syndrome (IRIS) [42], fungal infection relapse [43,44], delayed return to hospital [45], or other opportunistic infections [1], and low CD4 T cell counts [45,46]. These factors negatively impact survival after CM diagnosis or initial hospital admission. The extra social support needed to improve outcomes after hospital discharge explains why clinical care engagement rates were better in a cohort of people living with HIV who received community follow-up care after hospital discharge compared to those who did not [47].
3.3. Trials of Antifungal Dosage Formulations to Improve Cryptococcal Meningitis Survival
Evidence from clinical trials has improved clinical practice and infrastructure, but funding gaps can limit the transfer of knowledge from clinical trials to lower public healthcare settings, hindering patient benefits [8,10]. Differences in the funding scope and standard of care contribute to the differences in survival between patients receiving treatment in the tertiary hospital setting at 85 - 90% 2-week survival [2] compared to 51- 61% 2-week survival observed in the lower public healthcare facilities [8]. The factors influencing poor survival in public healthcare settings include limited capabilities to perform and provide extensive diagnostic packages of care critical to inform clinical decisions for patient-centered care in areas of high burden of co-infections [10]. The varied diagnostic algorithms are important given the diversity of alternative co-infections among patients with cryptococcal meningitis [1]. Improving survival following HIV associated cryptococcal meningitis remains a daunting challenge.
In response to the research and development needs for discovering new antifungal molecules and drug formulations to improve treatment, a few new antifungal formulations have joined the market for the treatment of invasive fungal infections. Adjunctive therapies including dexamethasone [48,49], sertraline [19,50], interferon gamma [20], tamoxifen [24], acetazolamide [21,51] have been tested as adjuncts to current antifungal regimens for the treatment of CM. However, these adjunctive therapies have yielded either none or limited additive efficacy. Unfortunately, with all efforts to model antifungal drug formulations in clinical trials, 2- and 10-week survival remains staggeringly low (Figure 5). The 2-week survival in 17 studies was 88.5% (IQR; 82.1-93.15%) compared to the 10-week median 74.0% survival (IQR; 62.13-85.0% survival) in 18 studies (p=0.001) (Figure 5). The collective clinical trial observations show a significant drop in survival from 100% to 2-week survival rates ranging between (60 - 99% survival) and 10 week survival dropping down to between (49% - 90% survival) (Figure 5). The majority of trials did not exceed 10-weeks of follow-up, which limits the interpretation of cryptococcal meningitis-related survival to no more than10 weeks.
3.4. Evolution of Promising Cryptococcal Meningitis Optimal Antifungal Therapy
Four seminal studies demonstrated superior efficacy of antifungal regimens used for the treatment of cryptococcal meningitis(Figure 5). The antifungal regimen with the lowest frequency of cryptococcal-related mortality had 1% mortality at 2 weeks and 10% mortality at 10 weeks of observation [41]. The regimen included 2-loading doses of intravenous Liposomal Amphotericin B Deoxycholate, an oral lipid nanocrystal formulation of Amphotericin B Deoxycholate and Flucytosine (Boulware et al., 2023) [41] (Figure 5) tested against WHO-recommended standard antifungal regimen (0.7-1mg per kg Amphotericin B deoxycholate and 800mg Fluconazole). This antifungal drug formulation was modeled in the phase II cryptococcal meningitis clinical trial in three tertiary hospitals in Uganda [41]. Phase III trials are needed to demonstrate the survival benefit of the oral formulation. This could improve the management of cryptococcal meningitis patients by reducing the need for intravenous drug administration and intensive nursing care for monitoring antifungal drug toxicity.
Among the seminal antifungal regimens for treatment of cryptococcal meningitis and the two WHO-recommended antifungal regimens for treatment of cryptococcal meningitis (Figure 4). 1) Liposomal Amphotericin B deoxycholate and Flucytosine inductive therapy [28], with 3% attrition after 2-weeks and 10% at 10-weeks using the WHO standard of care antifungal regimen (0.5 -0-7mg per kg Amphotericin B deoxycholate and 100mg per kg per day Flucytosine). 2) Liposomal Amphotericin B and Fluconazole inductive regimen [56], resulted in 3% mortality at 2-weeks and 15% mortality at 10-weeks of observations. Both outcomes were reported on the WHO standard antifungal regimen (0-7 1mg per kg Amphotericin B deoxycholate and 800mg Fluconazole).
The inclusion of at least two therapeutic lumbar punctures to monitor and manage persistently elevated intracranial pressure or for the alternative diagnosis of co-infections or demonstration of fungal clearance improve survival. These clinical and treatment-modifying attempts yielded the significant increase in 2-week survival by 18% from (76 -87% ) compared to 94 -99% at 2-weeks and 80-90% at 10-weeks during cryptococcal meningitis clinical trials (Figure 5).
4. Conclusion
In summary, persistent high mortality among hospitalized individuals with CM at 19% overall, means more efficacious antifungal regimens are needed for host-directed therapies to improve survival. Continued collaborative engagement is required with the public health enterprises, pharmaceuticals, governments, and donor agencies to support cryptococcal meningitis treatment and the package of care with essential medicines, diagnostics, technical expertise, and continued research to move the field forward to scale up care to improve survival.
5. Limitations
The primary literature was from peer-reviewed articles published in PubMed-indexed Journal where most funding agencies for clinical trials require data to be deposited for public access and immediate use. We might have left out important articles published elsewhere on funding agencies' websites or authors' preferred archives. Based on the search criteria and interest in follow-up survival outcomes, we did not include articles with no traceable survival outcomes during clinical trials' implementation.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Both SO and DBM equally contributed to study conceptualization, data curation, formal analysis, data interpretation, validation, visualization, writing the original draft, review, and editing of the final manuscript.
Funding
Not applicable except for salary support during writing of the manuscript.
Ethics Approval and Consent to Participate
Not applicable.
Availability of Data and Material
The data generating the manuscript is presented on tables, figures, and intext
citations. The meta-data is available if requested.
Acknowledgments
We would like to thank Edward N. Janoff from the University of Colorado, Denver Anschutz Medical Campus, Aurora Colorado USA, David R. Boulware, and Nathan C. Bahr, from the Division of Infectious Diseases and International Medicine, Department of Medicine, University of Minnesota, Minneapolis, USA, and Lillian Tugume from Infectious Diseases Institute, Makerere University for providing the extensive review of the initial draft.
Competing Interests
No competing interests.
Clinical Trial Number
Not applicable.
Consent for Publication
Authors consented to have the manuscript published.
References
- Ellis J, Bangdiwala AS, Cresswell FV, et al. The Changing Epidemiology of HIV-Associated Adult Meningitis, Uganda 2015–2017. Open Forum Infectious Diseases [Internet]. 2019 [cited 2024 Feb 6]; 6(10):ofz419. Available from: https://academic.oup.com/ofid/article/doi/10.1093/ofid/ofz419/5575986. [CrossRef]
- Rajasingham R, Smith RM, Park BJ, et al. Global burden of disease of HIV-associated cryptococcal meningitis: an updated analysis. The Lancet Infectious Diseases [Internet]. 2017 [cited 2023 Oct 23]; 17(8):873–881. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1473309917302438.
- Kashef Hamadani BH, Franco-Paredes C, McCollister B, Shapiro L, Beckham JD, Henao-Martínez AF. Cryptococcosis and cryptococcal meningitis: New predictors and clinical outcomes at a United States academic medical centre. Mycoses. 2018; 61(5):314–320. [CrossRef]
- Henao-Martínez AF, Gross L, Mcnair B, et al. Risk Factors for Cryptococcal Meningitis: A Single United States Center Experience. Mycopathologia [Internet]. 2016 [cited 2025 Sept 13]; 181(11–12):807–814. Available from: http://link.springer.com/10.1007/s11046-016-0048-x. [CrossRef]
- Mugabi T, Namombwe S, Dai B, et al. Etiology and Outcomes of Meningitis among Adults in Three Ugandan Referral Hospitals, 2018–2023: A Prospective Cohort Study in a High-HIV Endemic Setting.
- Rajasingham R, Govender NP, Jordan A, et al. The global burden of HIV-associated cryptococcal infection in adults in 2020: a modelling analysis. The Lancet Infectious Diseases [Internet]. 2022 [cited 2025 Sept 13]; 22(12):1748–1755. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1473309922004996.
- Perfect JR. Efficiently Killing a Sugar-Coated Yeast. N Engl J Med [Internet]. 2013 [cited 2025 Feb 12]; 368(14):1354–1356. Available from: http://www.nejm.org/doi/10.1056/NEJMe1302038. [CrossRef]
- Tenforde MW, Gertz AM, Lawrence DS, et al. Mortality from HIV-associated meningitis in sub-Saharan Africa: a systematic review and meta-analysis. J Intern AIDS Soc [Internet]. 2020 [cited 2024 Feb 13]; 23(1):e25416. Available from: https://onlinelibrary.wiley.com/doi/10.1002/jia2.25416. [CrossRef]
- Ellis J, Nsangi L, Bangdiwala A, et al. advanced HIV disease: a randomised strategy trial. Wellcome Open Research. 2024; .
- Okwir M, Link A, Rhein J, et al. High Burden of Cryptococcal Meningitis Among Antiretroviral Therapy–Experienced Human Immunodeficiency Virus–Infected Patients in Northern Uganda in the Era of “Test and Treat”: Implications for Cryptococcal Screening Programs. Open Forum Infectious Diseases [Internet]. 2022 [cited 2024 Feb 6]; 9(2):ofac004. Available from: https://academic.oup.com/ofid/article/doi/10.1093/ofid/ofac004/6501505. [CrossRef]
- Okurut, S. (2023) B cell responses, immune modulation and survival among patients with HIV-associated cryptococcal meningitis. [PhD. Thesis]. [Kampala, Uganda]: Makerere University.
- Kimuda S, Kwizera R, Dai B, et al. Comparison of Early Fungicidal Activity and Mortality Between Daily Liposomal Amphotericin B and Daily Amphotericin B Deoxycholate for Cryptococcal Meningitis. Clinical Infectious Diseases [Internet]. 2025 [cited 2025 Feb 12]; 80(1):153–159. Available from: https://doi.org/10.1093/cid/ciae326. [CrossRef]
- Bennett JE, Dismukes WE, Duma RJ, et al. A Comparison of Amphotericin B Alone and Combined with Flucytosine in the Treatment of Cryptoccal Meningitis. N Engl J Med [Internet]. 1979 [cited 2025 Feb 12]; 301(3):126–131. Available from: http://www.nejm.org/doi/abs/10.1056/NEJM197907193010303. [CrossRef]
- Perfect JR. The antifungal pipeline: a reality check. Nat Rev Drug Discov [Internet]. 2017 [cited 2025 Feb 12]; 16(9):603–616. Available from: https://www.nature.com/articles/nrd.2017.46. [CrossRef]
- Okurut S, Boulware DR, Manabe YC, et al. Impact of cerebrospinal fluid leukocyte infiltration and activated neuroimmune mediators on survival with HIV-associated cryptococcal meningitis. Rodrigues ML, editor. PLoS Negl Trop Dis [Internet]. 2025 [cited 2025 Feb 12]; 19(2):e0012873. Available from: https://dx.plos.org/10.1371/journal.pntd.0012873.
- Okurut S, Boulware DR, Okafor E, et al. Divergent neuroimmune signatures in the cerebrospinal fluid predict differential gender-specific survival among patients with HIV-associated cryptococcal meningitis. Frontiers in Immunology. [CrossRef]
- Han X, Liu H, Wang Y, et al. A nomogram for predicting paradoxical immune reconstitution inflammatory syndrome associated with cryptococcal meningitis among HIV-infected individuals in China. AIDS Res Ther [Internet]. 2022 [cited 2025 Feb 12]; 19(1):20. Available from: https://aidsrestherapy.biomedcentral.com/articles/10.1186/s12981-022-00444-5. [CrossRef]
- Kambugu A, Meya DB, Rhein J, et al. Outcomes of cryptococcal meningitis in Uganda before and after the availability of highly active antiretroviral therapy. Clinical Infectious Diseases. 2008; 46(11):1694–1701. [CrossRef]
- Rhein J, Huppler Hullsiek K, Tugume L, et al. Adjunctive sertraline for HIV-associated cryptococcal meningitis: a randomised, placebo-controlled, double-blind phase 3 trial. The Lancet Infectious Diseases [Internet]. 2019 [cited 2024 Jan 20]; 19(8):843–851. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1473309919301276. [CrossRef]
- Jarvis JN, Meintjes G, Rebe K, et al. Adjunctive interferon-γ immunotherapy for the treatment of HIV-associated cryptococcal meningitis: a randomized controlled trial. AIDS [Internet]. 2012 [cited 2024 Jan 20]; 26(9):1105–1113. Available from: https://journals.lww.com/00002030-201206010-00006. [CrossRef]
- Orem J, Tindyebwa L, Twinoweitu O, Mukasa B, Tomberland M, Mbidde EK. Feasibility study of serial lumbar puncture and acetazolamide combination in the management of elevated cerebrospinal fluid pressure in AIDS patients with cryptococcal meningitis in Uganda. Trop Doct [Internet]. 2005 [cited 2024 Jan 20]; 35(1):19–21. Available from: http://journals.sagepub.com/doi/10.1258/0049475053001967. [CrossRef]
- Jackson AT, Nussbaum JC, Phulusa J, et al. A phase II randomized controlled trial adding oral flucytosine to high-dose fluconazole, with short-course amphotericin B, for cryptococcal meningitis. AIDS [Internet]. 2012 [cited 2024 Jan 20]; 26(11):1363–1370. Available from: https://journals.lww.com/00002030-201207170-00006. [CrossRef]
- Pappas PG, Chetchotisakd P, Larsen RA, et al. A Phase II Randomized Trial of Amphotericin B Alone or Combined with Fluconazole in the Treatment of HIV-Associated Cryptococcal Meningitis. CLIN INFECT DIS [Internet]. 2009 [cited 2024 Jan 20]; 48(12):1775–1783. Available from: https://academic.oup.com/cid/article-lookup/doi/10.1086/599112. [CrossRef]
- Ngan NTT, Thanh Hoang Le N, Vi Vi NN, et al. An open label randomized controlled trial of tamoxifen combined with amphotericin B and fluconazole for cryptococcal meningitis. eLife [Internet]. 2021 [cited 2024 Jan 20]; 10:e68929. Available from: https://elifesciences.org/articles/68929.
- Day JN, Chau TTH, Wolbers M, et al. Combination Antifungal Therapy for Cryptococcal Meningitis. N Engl J Med [Internet]. 2013 [cited 2024 Jan 20]; 368(14):1291–1302. Available from: http://www.nejm.org/doi/10.1056/NEJMoa1110404. [CrossRef]
- Nussbaum JC, Jackson A, Namarika D, et al. Combination Flucytosine and High-Dose Fluconazole Compared with Fluconazole Monotherapy for the Treatment of Cryptococcal Meningitis: A Randomized Trial in Malawi. CLIN INFECT DIS [Internet]. 2010 [cited 2024 Jan 20]; 50(3):338–344. Available from: https://academic.oup.com/cid/article-lookup/doi/10.1086/649861.
- Hamill RJ, Sobel JD, El-Sadr W, et al. Comparison of 2 Doses of Liposomal Amphotericin B and Conventional Amphotericin B Deoxycholate for Treatment of AIDS-Associated Acute Cryptococcal Meningitis: A Randomized, Double-Blind Clinical Trial of Efficacy and Safety. CLIN INFECT DIS [Internet]. 2010 [cited 2024 Jan 20]; 51(2):225–232. Available from: https://academic.oup.com/cid/article-lookup/doi/10.1086/653606. [CrossRef]
- Zhao T, Xu X, Wu Y, et al. Comparison of amphotericin B deoxycholate in combination with either flucytosine or fluconazole, and voriconazole plus flucytosine for the treatment of HIV-associated cryptococcal meningitis: a prospective multicenter study in China. BMC Infect Dis [Internet]. 2022 [cited 2024 Jan 20]; 22(1):677. Available from: https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-022-07665-z. [CrossRef]
- Loyse A, Wilson D, Meintjes G, et al. Comparison of the Early Fungicidal Activity of High-Dose Fluconazole, Voriconazole, and Flucytosine as Second-Line Drugs Given in Combination With Amphotericin B for the Treatment of HIV-Associated Cryptococcal Meningitis. Clinical Infectious Diseases [Internet]. 2012 [cited 2024 Jan 20]; 54(1):121–128. Available from: https://academic.oup.com/cid/article-lookup/doi/10.1093/cid/cir745. [CrossRef]
- Muzoora CK, Kabanda T, Ortu G, et al. Short course amphotericin B with high dose fluconazole for HIV-associated cryptococcal meningitis. Journal of Infection [Internet]. 2012 [cited 2024 Jan 20]; 64(1):76–81. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0163445311005330. [CrossRef]
- Jarvis JN, Leeme TB, Molefi M, et al. Short-course High-dose Liposomal Amphotericin B for Human Immunodeficiency Virus–associated Cryptococcal Meningitis: A Phase 2 Randomized Controlled Trial. Clinical Infectious Diseases [Internet]. 2019 [cited 2024 Jan 20]; 68(3):393–401. Available from: https://academic.oup.com/cid/article/68/3/393/5045212. [CrossRef]
- Katende A, Mbwanji G, Faini D, et al. Short-course amphotericin B in addition to sertraline and fluconazole for treatment of HIV-associated cryptococcal meningitis in rural Tanzania. Mycoses [Internet]. 2019 [cited 2024 Jan 20]; 62(12):1127–1132. Available from: https://onlinelibrary.wiley.com/doi/10.1111/myc.12995. [CrossRef]
- Jarvis JN, Lawrence DS, Meya DB, et al. Single-Dose Liposomal Amphotericin B Treatment for Cryptococcal Meningitis. N Engl J Med [Internet]. 2022 [cited 2024 Jan 20]; 386(12):1109–1120. Available from: http://www.nejm.org/doi/10.1056/NEJMoa2111904. [CrossRef]
- Zhao T, Xu XL, Lu YQ, et al. The Effect of Early vs. Deferred Antiretroviral Therapy Initiation in HIV-Infected Patients With Cryptococcal Meningitis: A Multicenter Prospective Randomized Controlled Analysis in China. Frontiers in Medicine. 2021; 8(November):1–12. [CrossRef]
- Xu X, Lu Y, Harypursat V, et al. The Optimal Timing of Antiretroviral Therapy Initiation in HIV-Infected Patients with Cryptococcal Meningitis: A Multicenter Prospective Randomized Controlled Trial. Acta Med Okayama. 2021; 75(1).
- Molloy SF, Kanyama C, Heyderman RS, et al. Antifungal Combinations for Treatment of Cryptococcal Meningitis in Africa. N Engl J Med [Internet]. 2018 [cited 2024 Jan 20]; 378(11):1004–1017. Available from: http://www.nejm.org/doi/10.1056/NEJMoa1710922.
- Dutcher JD. The Discovery and Development of Amphotericin B. Diseases of the Chest [Internet]. 1968 [cited 2024 Feb 12]; 54:296–298. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0096021716319185.
- Sigera LSM, Denning DW. Flucytosine and its clinical usage. Therapeutic Advances in Infection [Internet]. 2023 [cited 2025 Mar 31]; 10:20499361231161387. Available from: https://journals.sagepub.com/doi/10.1177/20499361231161387. [CrossRef]
- Richardson K, Cooper K, Marriott MS, Tarbit MH, Troke F, Whittle PJ. Discovery of Fluconazole, a Novel Antifungal Agent. Clinical Infectious Diseases [Internet]. 1990 [cited 2024 Feb 12]; 12(Supplement_3):S267–S271. Available from: http://academic.oup.com/cid/article/12/Supplement_3/S267/300773/Discovery-of-Fluconazole-a-Novel-Antifungal-Agent.
- Boulware DR, Meya DB, Muzoora C, et al. Timing of Antiretroviral Therapy after Diagnosis of Cryptococcal Meningitis. N Engl J Med [Internet]. 2014 [cited 2024 Jan 20]; 370(26):2487–2498. Available from: http://www.nejm.org/doi/10.1056/NEJMoa1312884.
- Boulware DR, Atukunda M, Kagimu E, et al. Oral Lipid Nanocrystal Amphotericin B for Cryptococcal Meningitis: A Randomized Clinical Trial. Clinical Infectious Diseases [Internet]. 2023 [cited 2024 Jan 20]; 77(12):1659–1667. Available from: https://academic.oup.com/cid/article/77/12/1659/7246927.
- Meya DB, Manabe YC, Boulware DR, Janoff EN. The immunopathogenesis of cryptococcal immune reconstitution inflammatory syndrome: understanding a conundrum. Current opinion in infectious diseases. 2016; 29(1):10–22. [CrossRef]
- Van Wyk M, Govender NP, Mitchell TG, Litvintseva AP. Multilocus sequence typing of serially collected isolates of cryptococcus from HIV-infected patients in South Africa. Journal of Clinical Microbiology. 2014; 52(6):1921–1931.
- Hakyemez IN, Erdem H, Beraud G, et al. Prediction of unfavorable outcomes in cryptococcal meningitis: results of the multicenter Infectious Diseases International Research Initiative (ID-IRI) cryptococcal meningitis study. European Journal of Clinical Microbiology and Infectious Diseases. European Journal of Clinical Microbiology & Infectious Diseases; 2018; 37(7):1231–1240.
- Ding Y, Li P, He Q, et al. The CD4+ T-lymphocyte count is an important predictor for the prognosis of cryptococcosis. European Journal of Clinical Microbiology and Infectious Diseases. 2017; 36(5):897–904.
- Bahr NC, Skipper CP, Huppler-Hullsiek K, et al. Recurrence of Symptoms Following Cryptococcal Meningitis: Characterizing a Diagnostic Conundrum With Multiple Etiologies. Clinical Infectious Diseases [Internet]. 2023 [cited 2024 Mar 13]; 76(6):1080–1087. Available from: https://academic.oup.com/cid/article/76/6/1080/6776123. [CrossRef]
- Khawcharoenporn T, Damronglerd P, Chunloy K, Sha BE. Enhanced inpatient rounds, appointment reminders, and patient education improved HIV care engagement following hospital discharge. Int J STD AIDS [Internet]. 2018 [cited 2025 Dec 6]; 29(7):641–649. Available from: https://journals.sagepub.com/doi/10.1177/0956462417749420. [CrossRef]
- Beardsley J, Wolbers M, Kibengo FM, et al. Adjunctive Dexamethasone in HIV-Associated Cryptococcal Meningitis. N Engl J Med [Internet]. 2016 [cited 2024 Jan 20]; 374(6):542–554. Available from: http://www.nejm.org/doi/10.1056/NEJMoa1509024. [CrossRef]
- Day J, Imran D, Ganiem AR, et al. CryptoDex: A randomised, double-blind, placebo-controlled phase III trial of adjunctive dexamethasone in HIV-infected adults with cryptococcal meningitis: study protocol for a randomised control trial. Trials [Internet]. 2014 [cited 2023 Oct 20]; 15(1):441. Available from: https://trialsjournal.biomedcentral.com/articles/10.1186/1745-6215-15-441.
- Rhein J, Morawski BM, Hullsiek KH, et al. Efficacy of adjunctive sertraline for the treatment of HIV-associated cryptococcal meningitis: an open-label dose-ranging study. The Lancet Infectious Diseases [Internet]. 2016 [cited 2024 Jan 20]; 16(7):809–818. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1473309916000748. [CrossRef]
- Newton PN, Short JM, Chierakul W, et al. A Randomized, Double-Blind, Placebo- Controlled Trial of Acetazolamide for the Treatment of Elevated Intracranial Pressure in Cryptococcal Meningitis. [CrossRef]
- Newton PN, Thai LH, Tip NQ, et al. A Randomized, Double-Blind, Placebo-Controlled Trial of Acetazolamide for the Treatment of Elevated Intracranial Pressure in Cryptococcal Meningitis. CLIN INFECT DIS [Internet]. 2002 [cited 2024 Jan 20]; 35(6):769–772. Available from: https://academic.oup.com/cid/article-lookup/doi/10.1086/342299. [CrossRef]
- Bicanic T, Wood R, Meintjes G, et al. High-Dose Amphotericin B with Flucytosine for the Treatment of Cryptococcal Meningitis in HIV-Infected Patients: A Randomized Trial. CLIN INFECT DIS [Internet]. 2008 [cited 2024 Jan 20]; 47(1):123–130. Available from: https://academic.oup.com/cid/article-lookup/doi/10.1086/588792.
- Boulware DR, Meya DB, Muzoora C, et al. Timing of Antiretroviral Therapy after Diagnosis of Cryptococcal Meningitis. N Engl J Med [Internet]. 2014 [cited 2024 Jan 20]; 370(26):2487–2498. Available from: http://www.nejm.org/doi/10.1056/NEJMoa1312884. [CrossRef]
- Molloy SF, Kanyama C, Heyderman RS, et al. Antifungal combinations for treatment of cryptococcal meningitis in Africa. New England Journal of Medicine. 2018; 378(11):1004–1017. [CrossRef]
- Pappas PG, Chetchotisakd P, Larsen RA, et al. A Phase II Randomized Trial of Amphotericin B Alone or Combined with Fluconazole in the Treatment of HIV-Associated Cryptococcal Meningitis. CLIN INFECT DIS [Internet]. 2009 [cited 2024 Jan 20]; 48(12):1775–1783. Available from: https://academic.oup.com/cid/article-lookup/doi/10.1086/599112. [CrossRef]
Figure 1.
Inclusion and exclusion approach for studies which contributed metadata. A- all articles published or indexed in PubMed by “Cryptococcal meningitis Clinical Trials free word search customized to a period between January 2000 to January 2024”. B - (i-ii) - articles that underwent primary selection for follow-up reported survival. C - (i-ii) – articles that underwent secondary selection for the best modeled antifungal regimen. N- total article collection. n- number of articles by subcategories. Included were CM clinical trials reporting findings in adults (sex - male and female) >18 years of age and follow-up survival after diagnosis or enrolment into the randomized antifungal clinical trials.
Figure 1.
Inclusion and exclusion approach for studies which contributed metadata. A- all articles published or indexed in PubMed by “Cryptococcal meningitis Clinical Trials free word search customized to a period between January 2000 to January 2024”. B - (i-ii) - articles that underwent primary selection for follow-up reported survival. C - (i-ii) – articles that underwent secondary selection for the best modeled antifungal regimen. N- total article collection. n- number of articles by subcategories. Included were CM clinical trials reporting findings in adults (sex - male and female) >18 years of age and follow-up survival after diagnosis or enrolment into the randomized antifungal clinical trials.
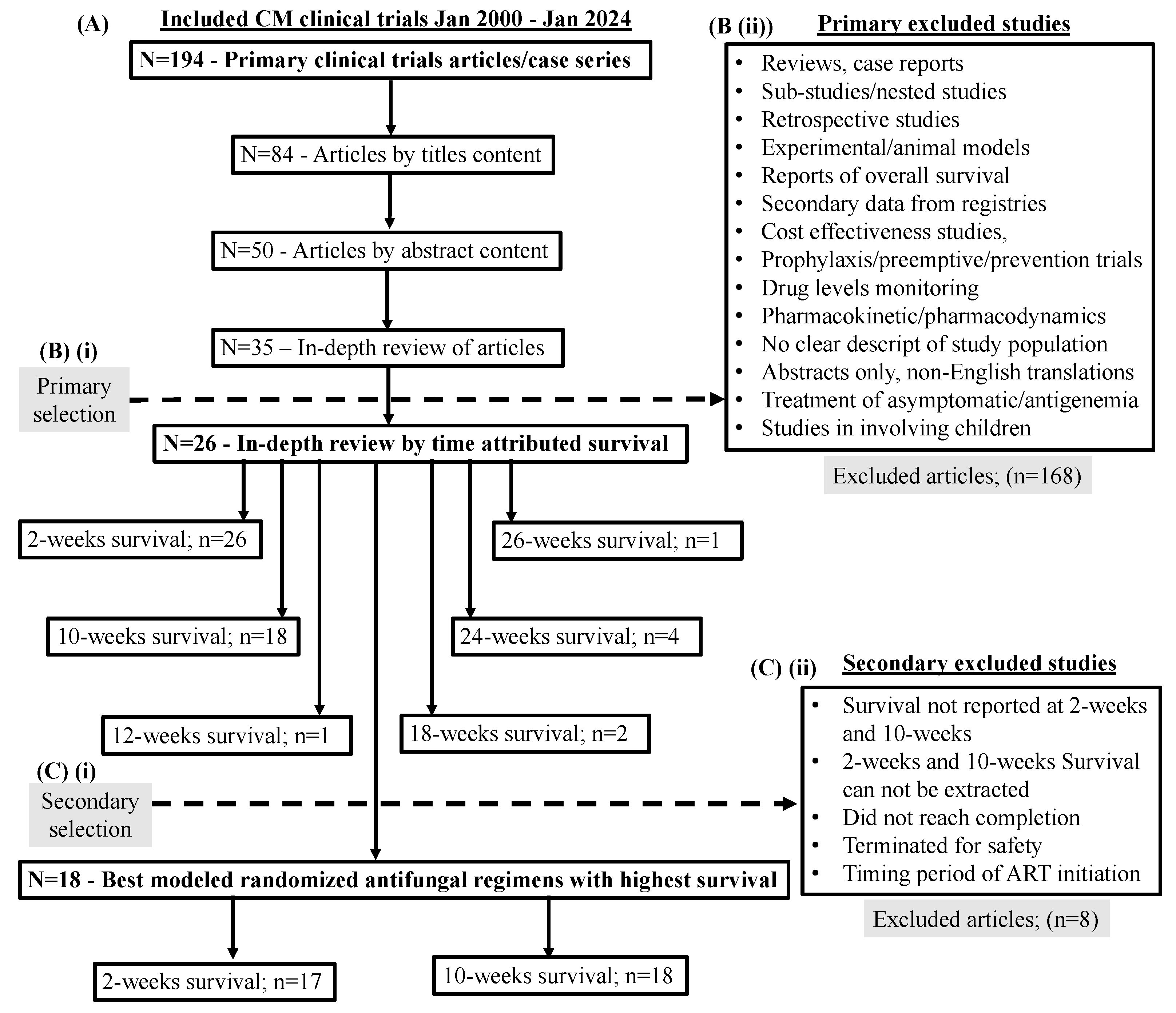
Figure 2.
Global distribution of cryptococcal meningitis clinical trials sites among peer-reviewed published case series reporting follow-up survival outcomes between January 2000 to January 2024. Included were 18 studies that reported survival with a specified follow-up period that was of interest for data comparison [19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36]. Excluded were studies that reported overall survival with no specific timeframe of follow-up and follow-up sub-studies exploiting parent clinical trials generated data. The rationale for exclusion was to avoid repetition, duplication, and compounding of location data by follow-up sub-studies’ reports.
Figure 2.
Global distribution of cryptococcal meningitis clinical trials sites among peer-reviewed published case series reporting follow-up survival outcomes between January 2000 to January 2024. Included were 18 studies that reported survival with a specified follow-up period that was of interest for data comparison [19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36]. Excluded were studies that reported overall survival with no specific timeframe of follow-up and follow-up sub-studies exploiting parent clinical trials generated data. The rationale for exclusion was to avoid repetition, duplication, and compounding of location data by follow-up sub-studies’ reports.
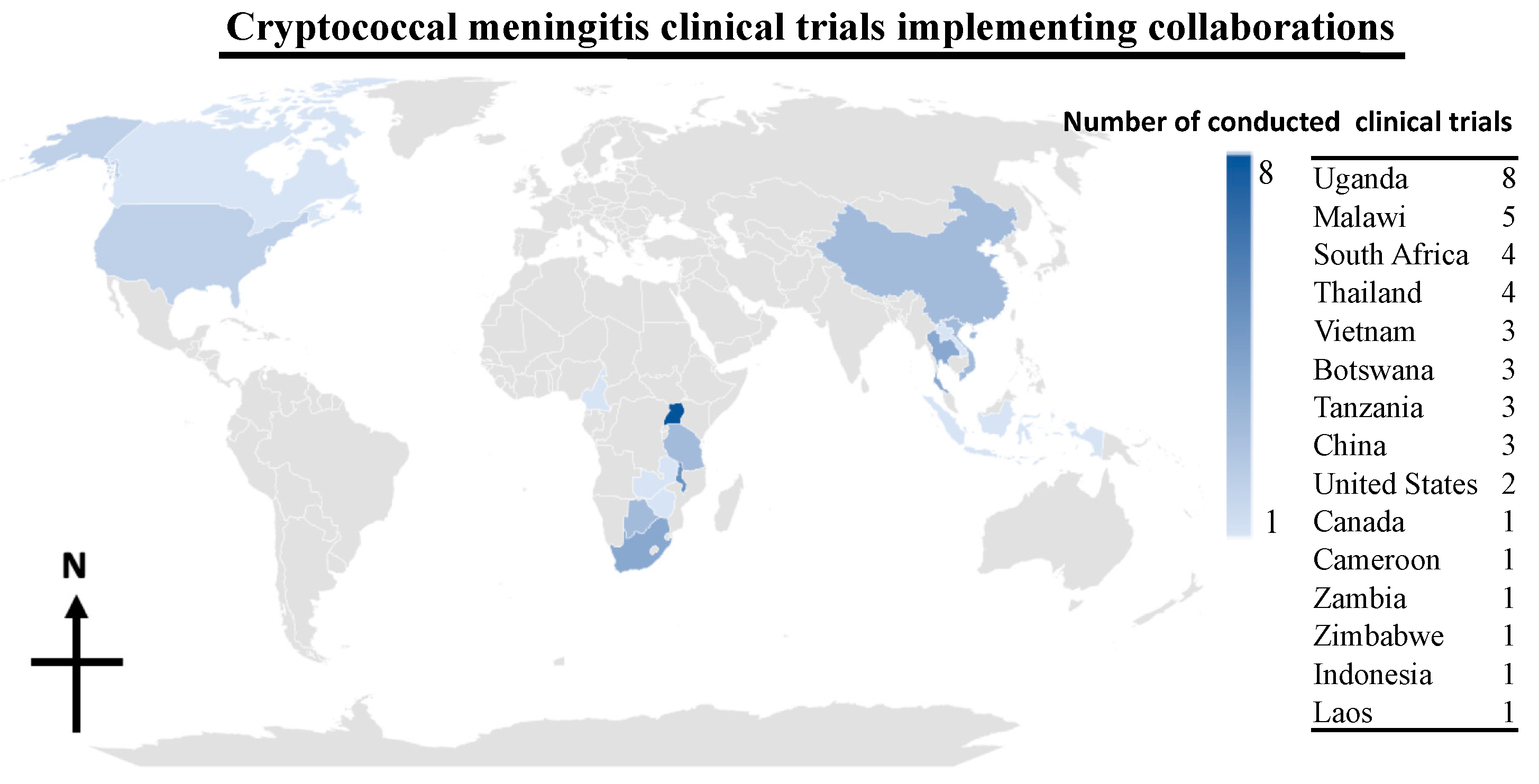
Figure 3.
Survival among participants enrolled in cryptococcal meningitis treatment and survival improvement clinical trials conducted between January 2000 to January 2024. Below the figure on the horizontal (-x-axis) are authors and the years the primary trials were published. Vertical dotted line and the opposite arrows show survival by clinical trials and year of publications before or after the period of timing of antiretroviral therapy among participants diagnosed with cryptococcal meningitis (CM). Values in the figure are percentages. The lines across the figure show survival per trial. ART – antiretroviral therapy. COAT – cryptococcal optimal antiretroviral therapy timing. ANOVA – analysis of variance across reported survival categories labelled above the figure. The comparative ANOVA p-value (p=0.029) was statistically significant.
Figure 3.
Survival among participants enrolled in cryptococcal meningitis treatment and survival improvement clinical trials conducted between January 2000 to January 2024. Below the figure on the horizontal (-x-axis) are authors and the years the primary trials were published. Vertical dotted line and the opposite arrows show survival by clinical trials and year of publications before or after the period of timing of antiretroviral therapy among participants diagnosed with cryptococcal meningitis (CM). Values in the figure are percentages. The lines across the figure show survival per trial. ART – antiretroviral therapy. COAT – cryptococcal optimal antiretroviral therapy timing. ANOVA – analysis of variance across reported survival categories labelled above the figure. The comparative ANOVA p-value (p=0.029) was statistically significant.
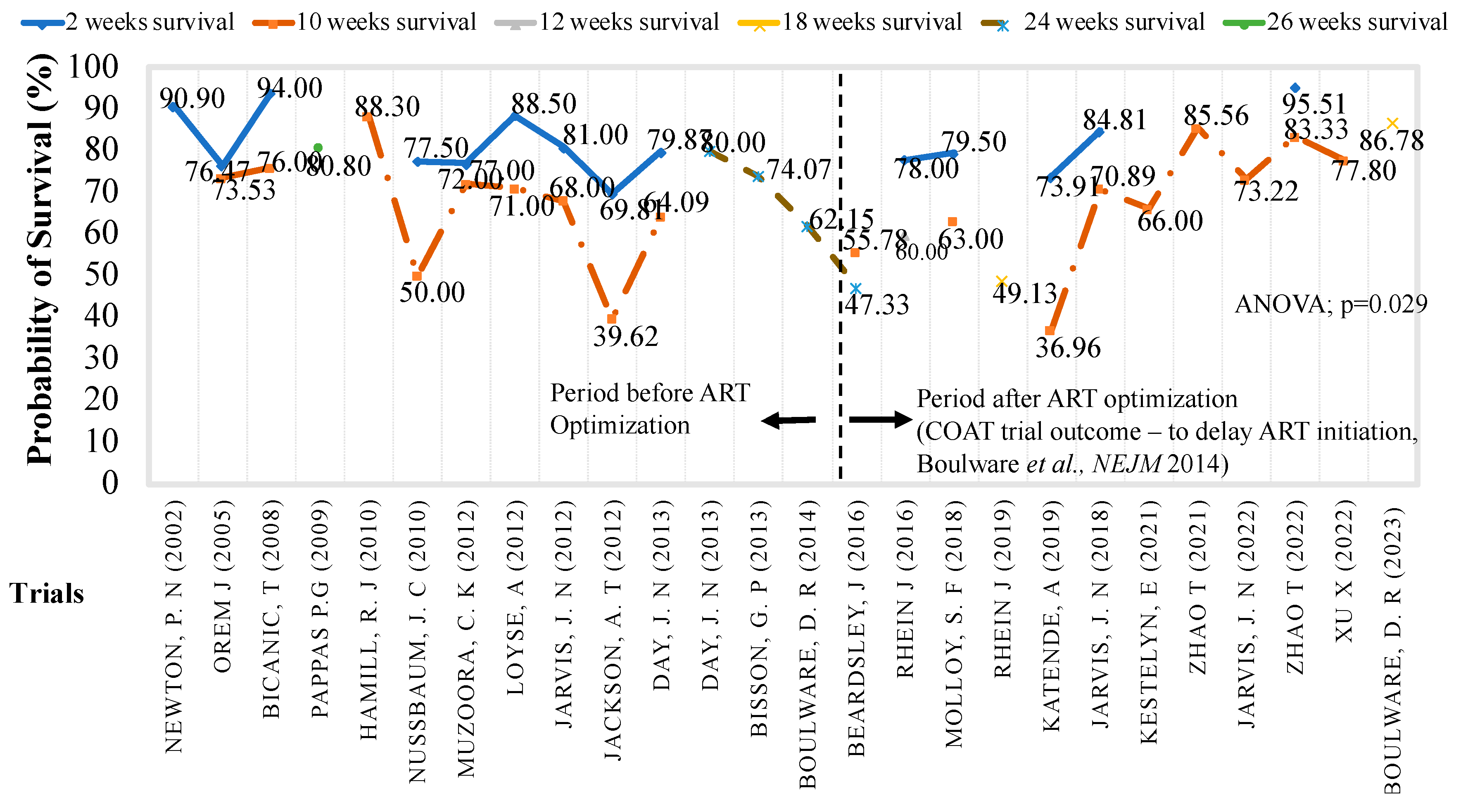
Figure 4.
10-weeks survival by randomization on inductive trial drugs arm or WHO recommended regimens that formed the standard therapy. Clinical trials randomizations among cases, those randomized to the trial drug and controls, those randomized to the WHO standard therapy. Included were (N=3,434 participants), (n=1710 trial arms randomized cases and n=1724 control randomized arm, randomized in a 1:1 ratio) among 18 studies with completed trial data. Excluded were studies that reported overall survival and all sub-studies among parent clinical trials. The rationale was to avoid repetition and compounding of clinical trial data by sub-studies reports. Further excluded were trials that were prematurely terminated or those that were in phase I efficacy trials or were setting the stage for subsequent trials e.g., studies that timed ART among participants with HIV-associated cryptococcal meningitis. Below the figure on horizontal (x-axis) are trial drugs randomization arms, authors and years the trial findings were published. WHO – World Health Organization. Flu – Fluconazole. 5FC -Flucytosine. AmB – Amphotericin B. L-AmB – Liposomal amphotericin B deoxycholate. LPs – Lumbar punctures. IFN-γ - interferon gamma. mg -milligram. Vori -Voriconazole. VCZ – Voriconazole. IV- intravenous. LNC -Liposomal Amphotericin B deoxycholate lipid encapsulated nanocrystals. Dexa – dexamethasone. x2 – two times. Comparative paired analysis p-value (p=0.715) was not statistically significant.
Figure 4.
10-weeks survival by randomization on inductive trial drugs arm or WHO recommended regimens that formed the standard therapy. Clinical trials randomizations among cases, those randomized to the trial drug and controls, those randomized to the WHO standard therapy. Included were (N=3,434 participants), (n=1710 trial arms randomized cases and n=1724 control randomized arm, randomized in a 1:1 ratio) among 18 studies with completed trial data. Excluded were studies that reported overall survival and all sub-studies among parent clinical trials. The rationale was to avoid repetition and compounding of clinical trial data by sub-studies reports. Further excluded were trials that were prematurely terminated or those that were in phase I efficacy trials or were setting the stage for subsequent trials e.g., studies that timed ART among participants with HIV-associated cryptococcal meningitis. Below the figure on horizontal (x-axis) are trial drugs randomization arms, authors and years the trial findings were published. WHO – World Health Organization. Flu – Fluconazole. 5FC -Flucytosine. AmB – Amphotericin B. L-AmB – Liposomal amphotericin B deoxycholate. LPs – Lumbar punctures. IFN-γ - interferon gamma. mg -milligram. Vori -Voriconazole. VCZ – Voriconazole. IV- intravenous. LNC -Liposomal Amphotericin B deoxycholate lipid encapsulated nanocrystals. Dexa – dexamethasone. x2 – two times. Comparative paired analysis p-value (p=0.715) was not statistically significant.
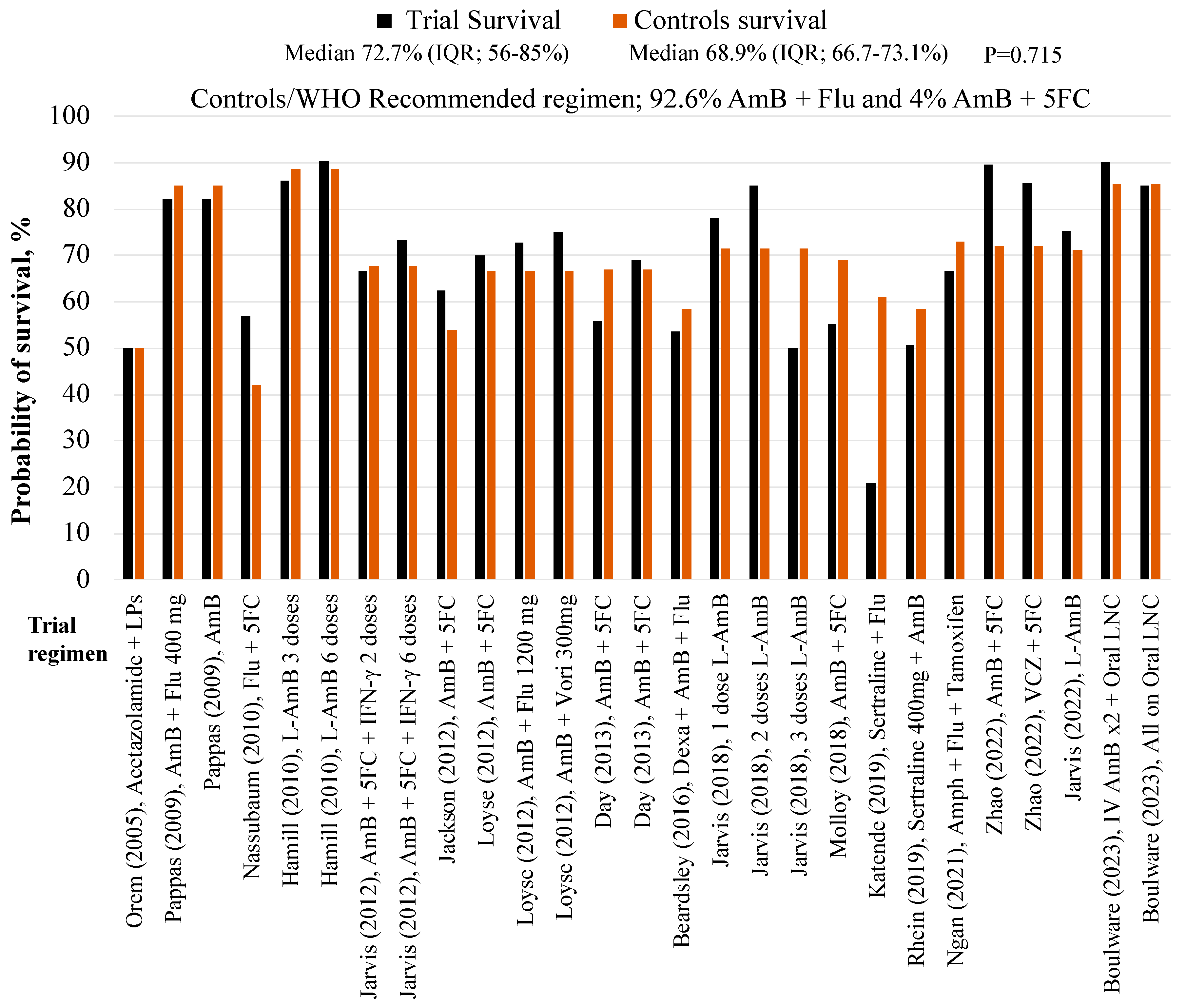
Figure 5.
Cryptococcal meningitis induction therapies to improve survival. Included were (N=4605 participants) enrolled in the parent clinical trials that reported survival with a specified follow-up which was of interest for comparison of outcomes [19,20,21,22,23,24,25,26,27,28,29,30,32,34,35,41,48,50,52,53,54,55]. Excluded were studies that reported overall survival with no follow-up period or whose survival data could not be traced and sub-studies among parent clinical trials. The rationale for excluding sub-studies was to avoid repetition and compounding of clinical trials data by sub-studies reports. Amp – amphotericin B deoxycholate. Flu - Fluconazole. 5FC – Flucytosine. L-Amp - Liposomal Amphotericin B deoxycholate. VCZ – voriconazole. Vori – Voriconazole. Crypto-Dexa – Cryptococcal – Dexamethasone. Adjunctive therapies include – dexamethasone, sertraline, tamoxifen, and acetazolamide. The comparative p valve p=0.001 was statistically significant.
Figure 5.
Cryptococcal meningitis induction therapies to improve survival. Included were (N=4605 participants) enrolled in the parent clinical trials that reported survival with a specified follow-up which was of interest for comparison of outcomes [19,20,21,22,23,24,25,26,27,28,29,30,32,34,35,41,48,50,52,53,54,55]. Excluded were studies that reported overall survival with no follow-up period or whose survival data could not be traced and sub-studies among parent clinical trials. The rationale for excluding sub-studies was to avoid repetition and compounding of clinical trials data by sub-studies reports. Amp – amphotericin B deoxycholate. Flu - Fluconazole. 5FC – Flucytosine. L-Amp - Liposomal Amphotericin B deoxycholate. VCZ – voriconazole. Vori – Voriconazole. Crypto-Dexa – Cryptococcal – Dexamethasone. Adjunctive therapies include – dexamethasone, sertraline, tamoxifen, and acetazolamide. The comparative p valve p=0.001 was statistically significant.
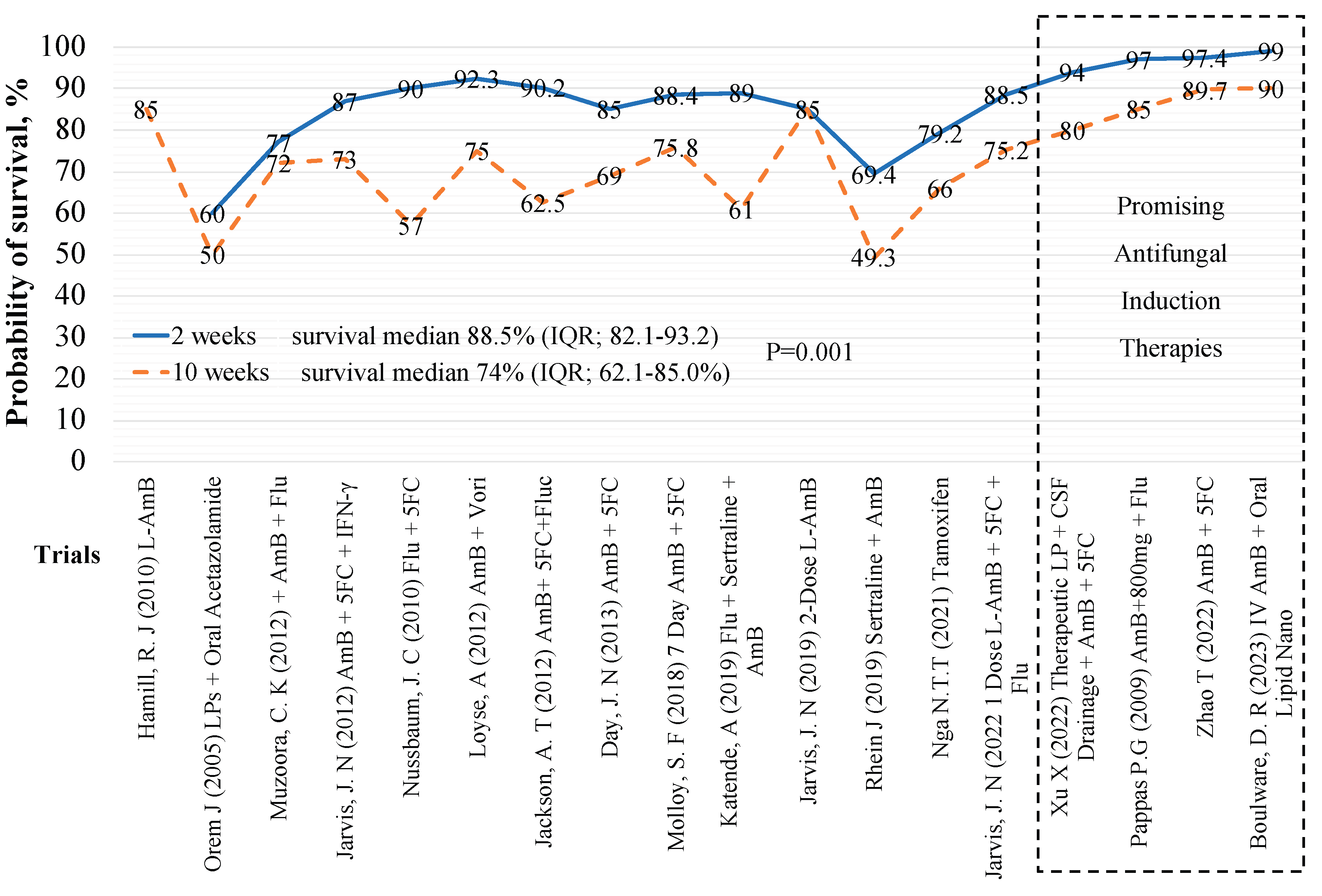

Table 1.
Summary of Trials by 10-Week Survival Included in Secondary Analyses/models.
| visualization, writing the original Author and publication year | Trial regimen | Trial arm, N=1710 |
10-week, survival, n (%) |
Control arm, N=1724; AmB + Flu or (*, **) |
10-week survival, n (%) |
|---|---|---|---|---|---|
| Boulware (2023) | IV AmB x2 + Oral AmB Nanocrystals | 40 | 35 (90%) | 41** | 35 (85.4%) |
| Boulware (2023) | All - Oral AmB Nanocrystals | 40 | 34 (85%) | 41** | 35 (85.4%) |
| Zhao (2022) | 10-week AmB + 5FC | 78 | 70 (89.7%) | 50 | 36 (72%) |
| Zhao (2022) | 10-week VCZ + 5FC | 28 | 24 (85.7%) | 50 | 36 (72%) |
| Jarvis (2022) | L-AmB 10 mg/kg x1 | 101 | 76 (75.2%) | 117** | 117 (71.3%) |
| Ngan NTT, (2021) | AmB + Flu + Tamoxifen | 24 | 16 (66.7%) | 26 | 19 (73.1%) |
| Rhein, (2019) | AmB + Fluconazole + Sertraline 400mg | 229 | 113 (50.7%) | 231 | 135 (58.4%) |
| Katende, (2019) | Sertraline + Fluconazole | 28 | 6 (21%) | 18 | 11 (61%) |
| Jarvis, (2018) | Single dose L-AmB + fluconazole | 18 | 14 (78%) | 21 | 15 (71.4%) |
| Jarvis, (2018) | 2 doses L-AmB + fluconazole | 20 | 17 (85%) | 21 | 15 (71.4%) |
| Jarvis, (2018) | 3 doses L-AmB + fluconazole | 20 | 10 (50%) | 21 | 15 (71.4%) |
| Molloy (2018) | AmB + 5FC | 225 | 124 (55%) | 228 | 157 (68.9%) |
| Beardsley (2016) | Dexa + AmB + Flu | 224 | 120 (53.6%) | 226 | 132 (58.4%) |
| Day J (2013) | AmB | 99 | 55 (56%) | 99 | 66 (67%) |
| Day J (2013) | AmB + 5FC | 100 | 70 (69%) | 99 | 66 (67%) |
| Jarvis (2012) | AmB + 5FC + IFN-γ | 57 | 40 (70.2%) | 62 | 42 (67.7%) |
| Jackson T (2012) | AmB + 5FC | 40 | 25 (62.5%) | 39 | 21 (53.8%) |
| Loyse (2012) | AmB + 5FC | 20 | 14 (70%) | 21 | 14 (66.7%) |
| Loyse (2012) | AmB + Flu 1200 mg | 22 | 16 (72.7%) | 21 | 14 (66.7%) |
| Loyse (2012) | AmB + Vori 300mg | 12 | 9 (75%) | 21 | 14 (66.7%) |
| Nussbaum, 2010 | Flu + 5FC | 21 | 12 (57%) | 19 | 8 (42%) |
| Hamill J.R, (2010) | L-AmB 3 mg/kg | 74 | 64 (86%) | 77 | 68 (88.5%) |
| Hamill J.R, (2010) | L-AmB 6 mg/kg | 85 | 77 (90.4%) | 77 | 68 (88.5%) |
| Pappas (2009) | AmB + Flu 400 mg | 48 | 41 (85%) | 45 | 44 (97%) |
| Pappas (2009) | AmB | 47 | 40 (85%) | 45 | 44 (97%) |
| Orem J (2005) | Acetazolamide + LPs | 10 | 5 (50%) | 8* | 4 (50%) |
AmB – Amphotericin B deoxycholate. Flu - Fluconazole. 5FC – Flucytosine. L-Amp - Liposomal amphotericin B deoxycholate. VCZ – voriconazole. Vori – Voriconazole. Dexa -Dexamethasone. IV – intravenous. 2x – twice. LPs -lumbar punctures. IFN-γ - interferon gamma. Kg – kilogram. mg -milligram. N – number of enrolled participants per trial randomization arm. * Acetazolamide. ** Flucytosine.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



