Submitted:
23 December 2025
Posted:
24 December 2025
You are already at the latest version
Abstract
In Africa, the load of diarrheal and respiratory diseases is amplified by limited surveillance capacity, diagnostic limitations, and socioeconomic inequalities. In rapidly urbanizing settings such as Kigali (Rwanda), integrating wastewater-based epidemiology (WBE) into existing surveillance systems gives a promising strategy for generating real-time epidemiological intelligence, identifying community-level hotspots, and addressing gaps in traditional reporting systems. Gastrointestinal and respiratory infections remain major causes of morbidity and mortality globally, mainly in low- and middle-income countries (LMICs), where traditional clinical surveillance systems frequently underreport true disease burden. This review synthesizes present evidence on the detection of gastrointestinal and respiratory pathogens in wastewater and evaluates the utility of WBE for early warning and public health action. A narrative review approach was used to identify peer-reviewed literature, global health reports, and surveillance studies focusing on wastewater detection of gastrointestinal and respiratory pathogens. Databases including PubMed, Scopus, and Google Scholar were searched for studies published between 2000–2024. The search yielded 1,247 records, of which 312 duplicates were removed. After title/abstract screening, 228 full texts were assessed for eligibility. Ultimately, 96 studies met the inclusion criteria and were included in the final review. Reasons for exclusion included: lack of pathogen data (n=58), industrial focus (n=27), or insufficient methodological detail (n=47). WBE provides a non-invasive, cost-effective approach for monitoring symptomatic and asymptomatic infections. Challenges involve variability in sampling, environmental factors affecting viral decay, and differences in laboratory workflows. WBE is a powerful complement to traditional infectious disease surveillance, suggesting early warning capabilities, population-level coverage, and real-time insights into pathogen circulation. Integrating WBE into surveillance programs especially in LMICs such as Rwanda can significantly strengthen epidemic preparedness, guide resource allocation, and improve outbreak response. Sustained investment in laboratory capacity, standardized protocols, and multisector collaboration is essential to fully leverage WBE for public health protection.
Keywords:
wastewater-based epidemiology
; gastrointestinal and respiratory pathogens
; early warning
; public health surveillance
1. Introduction
Wastewater-based epidemiology (WBE) has emerged as a powerful, non-invasive tool for monitoring infectious diseases at the community level, suggesting timely and cost-effective insights into pathogen circulation [1,2,3] Globally, gastrointestinal and respiratory infections remain among the most meaningful public health threats, extremely affecting populations in low- and middle-income countries (LMICs) due to prompt rapid population growth, urbanization, climate change, stressed sanitation systems, and rising antimicrobial resistance [4,5,6,7]. These factors contribute to the spread and re-emergence of enteric and respiratory pathogens, generating an urgent need for advanced surveillance systems capable of detecting both symptomatic and asymptomatic infections. Traditional clinical surveillance reliant on healthcare-seeking performance, laboratory diagnostics, and broadcasting systems captures only a portion of true cases, particularly in resource-limited situations where diagnostic coverage is uneven and health-seeking patterns vary widely [8,9,10]. Throughout the COVID-19 pandemic, adjournments in detecting community transmission and reliance on clinical testing critically damaged response efforts and intensified transmission in many regions [11,12,13]. These limits have led to increasing global interest in environmental surveillance approaches, particularly WBE, as complementary tools for considerate pathogen transmission dynamics and strengthening epidemic preparedness such as in Rwanda. WBE includes analyzing sewage for genetic material or biomarkers shed by infected individuals, allowing the detection of both symptomatic and asymptomatic infections at a population level [1,3,14]. This approach has validated strong performance in tracking a wide range of pathogens, including SARS-CoV-2, norovirus, rotavirus, hepatitis A virus, Campylobacter spp., Salmonella spp., and protozoan parasites such as Giardia and Cryptosporidium [15,16,17,18,19,20] to mention but a few. Numerous studies have exhibited strong correlations between pathogen concentrations in wastewater and clinical case trends, with wastewater signals often preceding clinical waves by several days to weeks highlighting the value of WBE as an early warning system [12,17,21,22,23]. Gastrointestinal pathogens including Escherichia coli, Salmonella, Vibrio cholerae, norovirus, rotavirus, and hepatitis A virus remain major contributors to global morbidity and mortality, mostly among children under five in LMICs [6,18,19,24]. In addition, Also, respiratory pathogens, especially SARS-CoV-2 and influenza viruses, have been identified in wastewater, supporting the use of WBE for respiratory disease surveillance [12,22,25]. Wastewater monitoring consequently offers a critical opportunity to notice outbreaks, display endemic disease patterns, and value the effectiveness of public health interventions such as vaccination programs and increases in water and sanitation infrastructure [17,24,26]. In Africa, the load of diarrheal and respiratory diseases is amplified by limited surveillance capacity, diagnostic limitations, and socioeconomic inequalities [7,27,28]. In rapidly urbanizing settings such as Kigali (Rwanda), integrating WBE into existing surveillance systems gives a promising strategy for generating real-time epidemiological intelligence, identifying community-level hotspots, and addressing gaps in traditional reporting systems [28,29,30]. Evidence from the COVID-19 pandemic revealed that WBE can detect emerging variants, identify resurgences even when clinical testing failures, and support data-driven decision-making in resource-limited environments [12,21,30,31,32]. Given these advantages, understanding in what way WBE can be leveraged for multi-pathogen detection in Kigali and similar urban centers is vital for strengthening public health preparedness and response. This review synthesizes up-to-date evidence on the finding of gastrointestinal and respiratory pathogens in wastewater, evaluates relationships between wastewater pathogen strengths and clinical case patterns, and emphasizes the role of WBE as an early warning tool. Furthermore, we discuss methodological considerations, challenges, and opportunities for integrating WBE into national disease surveillance frameworks in Rwanda and within Africa.
2. Materials and Methods
2.1. Why the Africa Context Matters?
In Africa with over 50 countries and rapidly expanding cities, The African context, particularly urbanizing cities such as Kigali is critically important for advancing wastewater-based epidemiology (WBE). Many African countries experience an uneven burden of infectious diseases and frequent outbreaks, while investigation systems often face diagnostic delays due to reduced laboratory capacity and under-reporting of clinical cases [33,34]. Fast population growth, dense settlements, and uneven health infrastructure additional increase the risk of silent transmission, making early detection essential [35]. Kigali, Rwanda’s capital and largest city with about two million population (2022 Rwandan Census) exemplifies a rapidly developing urban environment where expanding wastewater networks and high population mobility generate both challenges and opportunities for implementing WBE as a cost-effective surveillance tool [36,37]. Besides providing population-level, near–real-time pathogen insights, WBE can strengthen early-warning systems, complement traditional surveillance, and support more equitable outbreak readiness across African settings [14,38,39]. This systematic review was led following PRISMA principles to safeguard transparency and reproducibility. Five electronic databases were searched: PubMed/MEDLINE, Scopus, Web of Science, and the African Journals Online (AJOL) platform. The search covered studies published between January 2000 and October 2024 October 2025. A comprehensive Boolean search strategy combining Medical Subject Headings (MeSH) and free-text terms was applied. The core search series included combinations of: wastewater-based epidemiology, wastewater surveillance, environmental surveillance, pathogen detection, Africa, Rwanda, Kigali, SARS-CoV-2, enteric pathogens, AMR, virus detection, and public health surveillance [14,16,38]. This assessment aims to synthesize current suggestion on wastewater-based epidemiology for early pathogen detection, with emphasis stress on its applicability in African frameworks. Latest studies reveal that WBE can reliably detect viral, bacterial, and antimicrobial-resistant pathogens and bring actionable public-health insights before clinical data become available [14,38,39,40]. Nonetheless, research coverage across Africa remains limited, despite demonstrated feasibility in countries such as South Africa, Nigeria, Rwanda, and Senegal [36,41,42,43]. In consolidating global and Africa-specific results, this review identifies methodological advances, data gaps, and integration opportunities for strengthening public-health surveillance. Eventually, it highlights the potential for WBE to serve as a scalable and sustainable early-warning system capable of refining disease preparedness in resource-limited sets such as Kigali.
2.2. Inclusion Criteria
Studies were considered eligible for inclusion in this review if they reported either primary or secondary data on the detection of pathogens in wastewater. Eligible studies were essential to present microbiological, genomic, molecular or epidemiological outcomes significant to wastewater-based epidemiology (WBE). In addition, studies conducted in African settings were selected, as well as those specifying methodological understandings applicable to low-resource or resource-limited frameworks. Peer-reviewed articles, preprints, technical reports, and governmental or institutional surveillance documents published in either English or French were incorporated to ensure comprehensive coverage of both scientific and policy-oriented evidence.
2.3. Exclusion Criteria
Studies were excluded from the review if they dedicated exclusively on industrial discharge or environmental monitoring without direct relevance to public health. Publications lacking empirical laboratory records or epidemiological evidence were also excluded, as were studies that did not report specific pathogen finding outcomes in wastewater. Moreover, duplicate records, editorials, opinion pieces, interpretations, and conference abstracts without full methodological descriptions were rejected to preserve methodological rigor and data reliability.
2.4. Screening Process
All recovered records were imported into Zotero for de-duplication, after which two independent reviewers selected titles and abstracts. Full texts of potentially eligible studies occurred then assessed for inclusion. Any differences were resolved through consensus or adjudication by a third reviewer. Data extraction focused on key study types and outcomes, including the country, study setting, the specific pathogens targeted, the sampling and analytical methods employed. Extracted outcomes involved pathogen detection rates, assessable measurements, and any reported relationships between wastewater signals and corresponding clinical or epidemiological data. Furthermore, information on the public-health applications of wastewater-based epidemiology, such as early warning, surveillance integration, or outbreak response, was methodically collected.
2.5. Technical Workflow Overview
This section provides a high-level overview of the biological and analytical workflows commonly used in wastewater-based epidemiology studies included in this review.
2.6. Sampling Workflow
Most studies conducted in Africa and generally employed one of three primary wastewater-sampling strategies. Grab sampling was usually used, mostly at influent points of wastewater treatment plants or at sewer junctions, due to its effective simplicity. Composite sampling, frequently implemented using automated samplers, integrated flow-proportional or time-proportional samples over a 24-hour period to better apprehend temporal variability in pathogen shedding. Passive sampling approaches, involving Moore swabs and other absorbent materials, have gained increasing responsiveness, especially in low-resource settings such as Rwanda, where they offer a cost-effective and logistically feasible alternative while maintaining analytical sensitivity [36,44,45]. Sample preservation normally involved cooling at 4 °C during transport, with laboratory processing performed within 6–24 hours to minimize nucleic acid degradation and ensure data quality.
2.7. Concentration and Extraction Workflow
Viral and bacterial targets in wastewater samples were concentrated prior to analysis exploiting a range of conventional methods. Normally applied approaches involved polyethylene glycol (PEG) precipitation, ultrafiltration, electronegative membrane adsorption–elution techniques, and flocculation-based protocols. The concentration method varied according to target pathogen type, available laboratory infrastructure, sample matrix and resource settings, with each methodology offer distinct advantages in terms of recovery efficiency, scalability, and operational feasibility. RNA and DNA extractions were performed using commercial kits (e.g., Qiagen, Promega Maxwell, ThermoFisher) or phenol-chloroform-based protocols, depending on laboratory capacity. Internal process controls such as murine hepatitis virus (MHV), pepper mild mottle virus (PMMoV), and MS2 bacteriophage were often used to gauge recovery efficiency and normalization [40,46].
2.8. Biological and Molecular Detection Workflow
Following nucleic acid extraction, pathogen detection and quantification were primarily performed by reverse transcription quantitative PCR (RT-qPCR) or quantitative PCR (qPCR) for viral and bacterial targets. Droplet digital PCR (ddPCR) was also used in several studies to reach higher analytical sensitivity and enhanced absolute quantification, particularly for low-abundance targets. In addition, amplicon-based or whole-genome sequencing approaches were used to sustain variant tracking, antimicrobial resistance profiling, and phylogenetic inference. To increase data quality and comparability across sampling sites and time facts, normalization and quality control strategies were applied, including the use of fecal indicators such as pepper mild mottle virus (PMMoV) and crAssphage, as well as adjustments based on wastewater flow rates [40,79]. This workflow reflects the methodologies used both globally and in emerging African studies, including Rwanda’s SARS-CoV-2 wastewater surveillance pilot in Kigali, which demonstrated strong concordance between wastewater viral concentrations and reported clinical trends [4,36].
3. Results
3.1. Prisma Layout Flow Summary
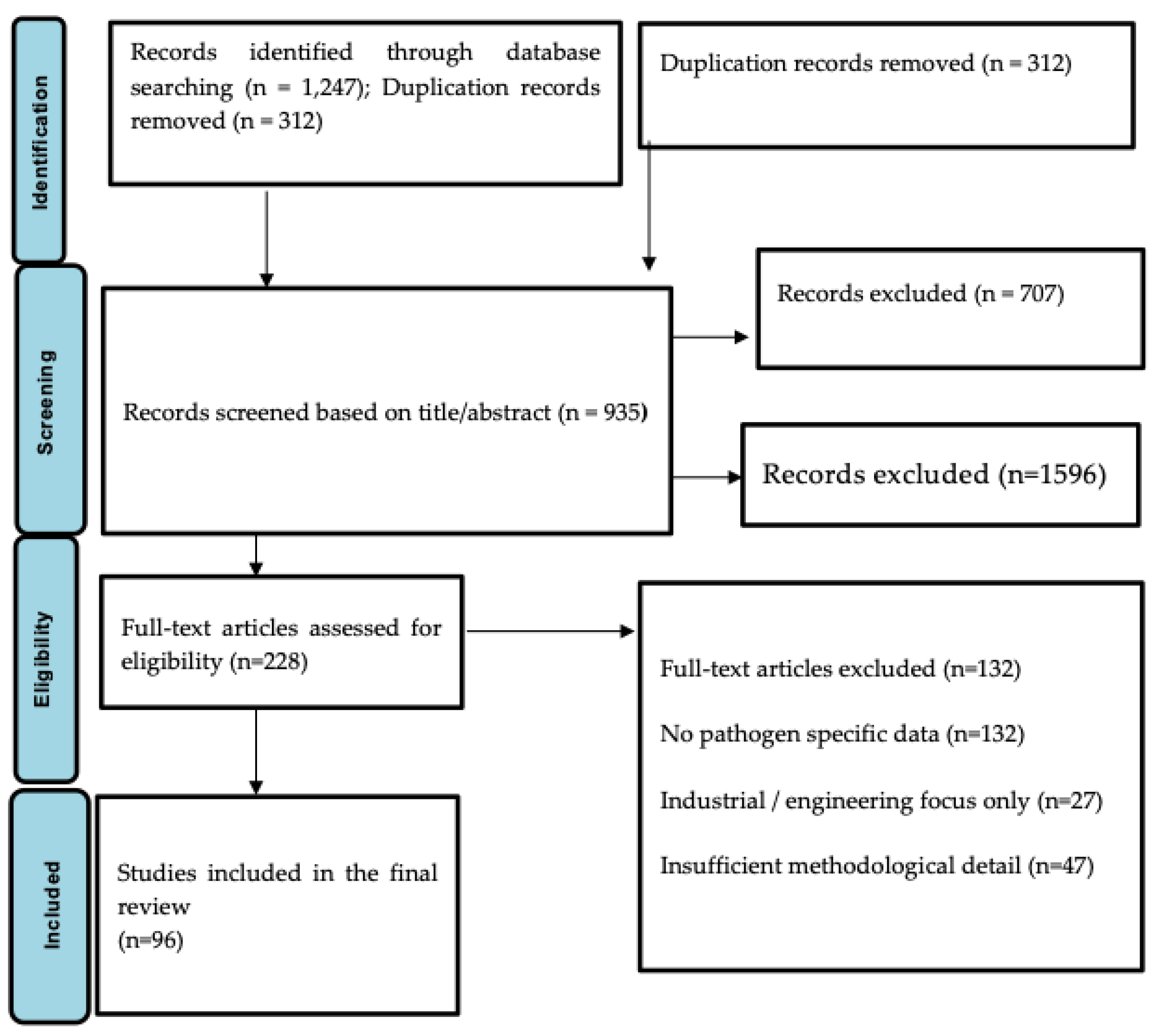
The search yielded 1,247 records, of which 312 duplicates were removed. After title/abstract screening, 228 full texts were assessed for eligibility. Ultimately, 96 studies met the inclusion criteria and were included in the final review. Reasons for exclusion included: lack of pathogen data (n=58), industrial focus (n=27), or insufficient methodological detail (n=47).
Figure 1.
PRISMA Flow Chart: Details of Screening Procedure.
3.2. Detection of Gastrointestinal Pathogens in Wastewater
Multiple studies have revealed that wastewater is a reliable and informative matrix for the detection of gastrointestinal pathogens circulating within communities. Viral agents frequently include norovirus, a leading global cause of acute gastroenteritis, rotavirus, which is mainly prevalent among children under five years of age, and hepatitis A virus, especially during community-level outbreaks. In addition to viral pathogens, wastewater surveillance has constantly detected a range of enteric bacteria such as Escherichia coli, Campylobacter spp., Salmonella spp., and Vibrio cholerae. Protozoan pathogens, including Cryptosporidium and Giardia, have also been identified, further highlighting the capacity of wastewater-based epidemiology to apprehend diverse gastrointestinal pathogens of public health importance. Discovery rates vary by pathogen type, environmental conditions, and sampling approach, but wastewater monitoring consistently classifies pathogen circulation even when clinical reporting is low.
Table 1 provides a consolidated outline of wastewater-based epidemiology (WBE) initiatives conducted across the African continent. These studies vary extensively in scope from SARS-CoV-2 surveillance and poliovirus environmental monitoring to antimicrobial resistance (AMR) recognition and enteric virus tracking. The table highlights the variety of pathogens monitored, methodological platforms used, and the uneven distribution of WBE activities across countries. It also highlights the growing role of WBE as a complementary surveillance tool in resource-limited settings.
Table 2 summarizes peer-reviewed studies that applied wastewater-based epidemiology methods across African countries, including study focus, pathogens detected, analytical platforms, and reference sources. It synthesizes key gastrointestinal pathogens detected in wastewater and the rational platforms commonly used for their identification. Enteric viruses such as norovirus, rotavirus, and adenovirus remain the most reported organisms due to their high shedding rates and environmental stability. Bacterial and protozoan pathogens need more specialized methods, including culture, PCR, and immunofluorescence assays. This table provides a technical foundation for understanding how wastewater reflects community-level circulation of GI diseases.
3.3. Detection of Respiratory Pathogens in Wastewater
Respiratory virus detection in wastewater has increased rapidly since the COVID-19 pandemic, providing critical insights into community-level transmission dynamics. Several studies have showed that SARS-CoV-2 RNA is highly detectable in wastewater and demonstrates strong correlations with reported clinical case trends. Importantly, wastewater viral signals have normally been observed to precede clinical case surges by approximately 4 to 10 days, underscoring the early-warning potential of wastewater-based epidemiology. In addition to SARS-CoV-2, influenza viruses (A and B) have also been effectively identified in untreated wastewater, further supporting the feasibility of wastewater surveillance for monitoring respiratory virus circulation beyond pandemic settings. These findings underscore the relevance of WBE beyond gastrointestinal pathogens, supporting integrated multi-pathogen surveillance systems.
3.4. Correlations Between Wastewater Signals and Clinical Case Data
Strong correlations between pathogen concentrations measured in wastewater and reported clinical cases have been known across diverse geographic regions. Wastewater signals of SARS-CoV-2 have been shown to closely track, and frequently forecast, community infection trends. Likewise, increases in norovirus RNA concentrations in wastewater coincide with gastroenteritis outbreaks, while rotavirus detection patterns align with seasonal trends in pediatric disease. Detection of hepatitis A virus in sewage has also been reported to precede clinical case spikes, enabling early outbreak identification. These correlations reinforce the value of wastewater-based epidemiology as a sensitive and timely population-level surveillance tool for infectious disease monitoring.
The respiratory pathogens identified in wastewater globally and in Africa, including methods used and representative studies.
The Table 3 summarizes respiratory pathogens that have been effectively identified in wastewater and stresses the rationale for their environmental detectability. SARS-CoV-2 remains the most documented respiratory virus in wastewater systems, but emerging evidence shows that influenza viruses, RSV, and adenoviruses can also be perceived. This demonstrates the expanding utility of WBE beyond enteric diseases, offering potential for integrated respiratory pathogen surveillance, especially during outbreaks or seasonal peaks. Also, a summary comparison of RT-qPCR and sequencing approaches is presented in Table 3.
3.5. Technical and Operational Considerations
The quality and reliability of wastewater-based epidemiology data are influenced by several interrelated methodological factors. These involve the choice of sampling strategy, such as grab versus composite sampling and the use of raw sewage linked with sludge, which can affect pathogen recovery and temporal representativeness. RNA preservation practices and viral decay dynamics throughout collection, transport, and storage further influence detection sensitivity. Also, variations in extraction and concentration workflows can considerably impact nucleic acid yield and analytical performance. The selection of molecular detection methods, including RT-qPCR, droplet digital PCR (ddPCR), and metagenomic sequencing, Finally, normalization approaches, such as the use of fecal indicators (e.g., PMMoV), wastewater flow data, or chemical tracers, are critical for improving comparability across sampling sites and over time.
Examples of studies demonstrating the strength of correlation between wastewater pathogen concentrations and reported clinical cases. This table presents examples of strong correlations between wastewater pathogen concentrations and reported clinical cases within different settings. Several studies consistently show that wastewater signals can lead increases in clinical incidence by days or weeks, highlighting the value of WBE as an early warning system. This correlation strengthens the case for integrating WBE into national disease surveillance frameworks, particularly in settings where diagnostic access is limited (Table 4).
Comparison of major advantages and limitations of wastewater-based epidemiology in public-health surveillance. This table strengths and Limitations of WBE. Table 5 outlines the major strengths and limitations of WBE as reported in the scientific literature. While wastewater surveillance offers early detection, population-wide coverage, and the capability to capture asymptomatic infections, it also faces methodological and operational challenges. These include viral decay, infrastructure variability, and limitations in quantification methods. Understanding these advantages and constraints is essential for designing feasible and impactful WBE programs in low-resource contexts
This Table 6 highlights key opportunities for advancing wastewater-based epidemiology in low-resource African settings. These opportunities involve the adoption of passive sampling technologies, integration with Africa CDC genomic networks, improved urban sanitation systems, and enhanced laboratory and workforce capacity. Together, these dynamics create a pathway for sustainable WBE expansion and its incorporation into routine public health decision-making.
3.6. Regional WBE Evidence in Africa Compared with Findings from Rwanda
To position the findings of this study within the broader African context, Table 7 (Summary Table Wastewater-Based Epidemiology Studies in Africa) provides a consolidated overview of WBE initiatives conducted across the continent. These studies demonstrate how wastewater surveillance has been applied to detect a wide range of pathogens, including SARS-CoV-2, poliovirus, enteric viruses, antimicrobial-resistant bacteria, and viral hepatitis, using diverse analytical platforms such as RT-qPCR, cell culture, PEG precipitation, metagenomic sequencing, and passive environmental sampling. The regional indication highlights numerous trends relevant to considerate Rwanda’s progress. Countries with long-standing environmental surveillance systems such as South Africa, Nigeria, and Senegal have leveraged their existing laboratory networks to rapidly integrate SARS-CoV-2 wastewater monitoring, accomplishing strong correlations with clinical case trends and generating real-time public health insights. In contrast, countries such as Ghana, Kenya, Uganda, and Ethiopia have applied WBE to target specific public health priorities, including enteric viruses, antimicrobial resistance, and bacterial pollution in wastewater systems.
Alongside this background, Rwanda’s recent expansion of WBE activities aligns with wider regional improvements while also demonstrating notable innovation. Rwanda’s community wastewater surveillance, joined with the development of WBE frameworks for early outbreak detection and the combination of airport-based genomic surveillance using aircraft wastewater, places the country among Africa’s emerging leaders in leveraging wastewater as a strategic public health tool. These initiatives are particularly significant in a situation where conventional clinical surveillance may face constraints related to access, testing coverage, and resource limitations.
Largely, the evidence summarized in Table 7 shows that WBE is gradually recognized across Africa as a complementary and cost-effective surveillance approach. Comparing Rwanda’s experience with other countries stresses both combined challenges such as laboratory capability, infrastructure variability, and resource constraints and substantial opportunities for strengthening national and regional disease early-warning systems through consistent WBE practices, integrated genomic surveillance, and cross-country knowledge exchange.
Figure 2, in combination with Table 7, show the geographic distribution, thematic focus, and methodological diversity of wastewater-based epidemiology (WBE) studies conducted across Africa. The figure highlights that WBE activities have been concentrated in a limited number of countries, with South Africa, Nigeria, and Rwanda emerging as regional leaders in the implementation of wastewater surveillance. South Africa demonstrates the most expanded WBE portfolio, including SARS-CoV-2 surveillance, long-standing poliovirus environmental surveillance, and antimicrobial resistance (AMR) monitoring using advanced molecular platforms, with RT-qPCR, metagenomic sequencing, and PEG-based concentration methods [50,51,52,53,54,55]. Several countries, including Nigeria, Senegal, and Ghana, have leveraged WBE mainly for enteric virus surveillance, particularly poliovirus and other gastrointestinal pathogens, reflecting alignment with global polio eradication and diarrheal disease control initiatives [56,57,69,70,71,72]. In contrast, North African countries such as Egypt, Tunisia, and Morocco have focused predominantly on SARS-CoV-2 and hepatitis virus detection in wastewater, largely adopting RT-qPCR-based approaches through the COVID-19 pandemic [59,60,61,62,63,64]. East African countries, including Kenya, Uganda, Ethiopia, and Rwanda, demonstrate an increasing integration of WBE into antimicrobial resistance surveillance and pandemic awareness. Kenya and Uganda have applied culture-based approaches combined with PCR to reveal resistant Escherichia coli, Enterococcus, and other clinically significant bacteria [65,66,67,68], while Ethiopia has focused on quantifying resistance genes using qPCR [78]. Rwanda presents a particularly notable case, with several complementary WBE initiatives ranging from municipal SARS-CoV-2 surveillance to the development of national wastewater surveillance frameworks and innovative airport-based wastewater and genomic surveillance targeting imported variants at Kigali International Airport [74,75,76,77].
4. Discussion
4.1. Overview of Wastewater-Based Epidemiology (WBE) for GI and Respiratory Pathogens
Wastewater-based epidemiology (WBE) has appeared as a powerful population-level surveillance tool capable of detecting a broad spectrum of gastrointestinal (GI) and respiratory pathogens shed in human excretion. Pathogens excreted in feces, urine, saliva, sputum, and mucus enters sewage networks, allowing the aggregation of biological signals from large communities regardless of healthcare-seeking behavior or testing access [14,35,38]. WBE complements traditional surveillance by providing near–real-time data on pathogen flows, including viruses (e.g., norovirus, rotavirus, adenovirus, SARS-CoV-2), bacteria (e.g., Salmonella, Shigella, Vibrio), and antimicrobial resistance (AMR) markers [44,80,81]. Its application expanded substantially during the COVID-19 pandemic and is currently recognized as a scalable early-warning approach, particularly valuable for resource-limited settings where routine clinical surveillance remains fragmented [36,37,79].
4.2. Detection of Gastrointestinal Pathogens in Wastewater
Various studies have demonstrated successful detection of GI pathogens in wastewater using RT-qPCR, ddPCR, culture-based assays, and sequencing. Enteric viruses such as norovirus, rotavirus, hepatitis A virus (HAV), and enteroviruses are within the most frequently monitored and consistently detected at high concentrations due to robust fecal shedding dynamics [18,19,36,48,50]. Bacterial pathogens including Salmonella enterica, Vibrio cholerae, Shigella spp., Campylobacter spp., and diarrheagenic Escherichia coli have been identified across various wastewater systems globally, including in African settings such as South Africa, Nigeria, Senegal, and Rwanda [43,44,83,84]. Wastewater has also proven valuable for identifying AMR genes (e.g., blaCTX-M, carbapenemases, macrolide resistance markers), offering insights into community-level resistance pressures [49]. These findings highlight WBE’s strong potential to track GI diseases that represent a major burden across Africa.
4.3. Detection of Respiratory Pathogens in Wastewater
Although respiratory pathogens are not naturally associated with fecal-oral transmission, several respiratory viruses, including SARS-CoV-2, influenza A/B, respiratory syncytial virus (RSV), and human metapneumovirus have been consistently detected in wastewater due to mucosal shedding and enteric replication pathways [14,37,86]. SARS-CoV-2 surveillance via WBE has been broadly validated, including in low-resource settings such as Kigali, where viral RNA trends strongly revealed clinical case patterns during multiple pandemic waves [36,86]. Emerging studies also exhibit wastewater detection of influenza viruses and RSV, enabling population-level monitoring even when clinical testing readiness decreases or asymptomatic infections dominates transmission [85,87]. These advances swell the scope of WBE from traditional GI pathogens toward broader respiratory disease surveillance.
4.4. Correlation Between Wastewater Signals and Clinical Data
A reliable finding across global literature is the strong correlation between wastewater pathogen concentrations and reported clinical case data. For SARS-CoV-2, multiple studies demonstrated that growths in wastewater RNA concentrations precede rises in clinical cases by 4 to14 days, making WBE a dependable early-warning indicator [31,36,37,86]. Similar correlations have been observed for norovirus, rotavirus, poliovirus, hepatitis A, and Salmonella outbreaks, where wastewater detection also predicted or reflected community transmission dynamics [18,82]. In Rwanda, wastewater SARS-CoV-2 concentrations measured at major treatment facilities in Kigali showed high concordance with PCR-confirmed case data throughout the pandemic [86]. This alignment emphasizes WBE’s utility in settings with limited diagnostic coverage, asymptomatic infections, or delays in clinical reporting.
4.5. Strengths and Limitations of WBE in Public Health Surveillance
Wastewater-based epidemiology (WBE) offers several strengths that make it a valuable tool for communicable disease surveillance. It is a cost-effective surveillance approach, particularly in low-resource settings where widespread individual testing is not feasible [44,87]. In addition, WBE allows the simultaneous monitoring of multiple pathogens, including antimicrobial resistance markers, and offers a noninvasive, community-wide surveillance mechanism that supports equity in public-health responses [81]. It also provides population-level coverage that is independent of healthcare-seeking behavior, acknowledging more comprehensive monitoring of community infection dynamics [35,38]. WBE can detect pathogen circulation early, often before symptomatic cases peak, thereby supporting suitable public-health interventions [31,37]. Despite these benefits, WBE also presents several limitations. Variability in sewage infrastructure can affect the representativeness of samples, particularly in informal or underserved settlements [35,44]. Environmental factors such as temperature, pH, flow rate, and hydraulic retention time influence the decay of RNA and DNA in wastewater, potentially decreasing detection sensitivity [37,80]. Further challenges include difficulties in accurate quantification, normalization, and establishing direct links between wastewater signals and precise case numbers [88,89]. Furthermore, limited laboratory capacity for molecular analysis and sequencing in many African regions constrains large-scale implementation [44,83]. However, when integrated with environmental, clinical, and genomic data, WBE remains a powerful and complementary approach to traditional surveillance systems, particularly for strengthening early warning and public health awareness.
4.6. Implications for Early Warning Systems
WBE’s capacity to identify pathogens before clinical increases occur makes it a cornerstone for early-warning systems. Through detecting pre-symptomatic and asymptomatic shedding, WBE can guide rapid interventions such as targeted assessment, vaccination campaigns, public-risk communication, and resource allocation [18,31,37]. During COVID-19, WBE allowed early detection of emerging variants and informed public-health decision-making even when clinical-testing capacity was overwhelmed [14,86]. Similar frameworks are now being applied to other pathogens such as cholera, norovirus, and AMR genes to support outbreak prediction and response strategies in Africa and other resource-limited regions [43,49,56]. Its integration into national surveillance systems can significantly increase resilience against future rises.
4.7. Opportunities for Implementation in Low-Resource African Settings
African settings present a unique opening for scaling WBE due to the disproportionate burden of infectious diseases, under-resourced clinical surveillance systems, and increasing wastewater infrastructure in urban centers such as Kigali, Nairobi, Johannesburg, Dakar, and Lagos [43,44,83]. Passive samplers (e.g., Moore swabs) have demonstrated particularly effective and low-cost for wastewater monitoring in Rwanda and other low-resource environments [86,89]. Regional initiatives such as the Africa CDC’s Pathogen Genomics Initiative and national early-warning agendas provide platforms for integrating WBE into routine disease surveillance and outbreak response frameworks [14,84,90]. Strengthening laboratory capacity, normalizing methods, and establishing cross-country data-sharing networks will be crucial to expanding WBE’s role in pathogen surveillance across Africa. With suitable investment, WBE can become a sustainable and equitable surveillance tool supporting epidemic preparedness in diverse urban and peri-urban African communities.
5. Conclusions
Wastewater-based epidemiology provides a dominant, non-invasive approach for monitoring community-level circulation of gastrointestinal and respiratory pathogens. Evidence displays that wastewater signals often precede clinical cases, suggesting valuable early warning for outbreaks. WBE is especially valuable in resource-limited surroundings where diagnostic access is constrained. Integrating WBE into national surveillance frameworks can enhance infectious disease monitoring, inform targeted interventions, and strengthen overall public health resilience. Continued investment in laboratory infrastructure, capacity building for early career researchers, standardized methodologies, and cross-sector collaboration will be essential to scaling WBE programs across Africa and globally.
Author Contributions
Conceptualization, S.B., T.T.A., L.M.; methodology, S.B., L.M., T.T.A.; literature search and study selection, S.B.; data curation, S.B.; formal analysis, S.B., T.T.A., L.M.; writing original draft preparation, S.B.; writing review and editing, S.B., T.T.A., L.M.; visualization, S.B.; supervision, L.M., T.T.A.; project administration, S.B.; Overall supervision, L.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable. This study is a systematic review of published literature and publicly available data and did not involve human participants, animal subjects, or identifiable personal data. However, it is noted that the authors have obtained ethical approval (Approval No. 743/CMHS IRB/2024) from the College of Medicine and Health Sciences (CMHS) Institutional Review Board for the primary research project entitled “Wastewater Surveillance: Community-Level Pathogen Monitoring for Rapid Response in Kigali, Rwanda.” The approval relates to the associated primary study and is independent of the present review.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
The authors would like to acknowledge the University of Rwanda, College of Medicine and Health Sciences, for providing an enabling academic environment for this work. The authors also thank the researchers and public health institutions whose published studies contributed to the evidence synthesized in this review.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| Abbreviation | Definition |
| AMR | Antimicrobial Resistance |
| AMS | Antimicrobial Stewardship |
| API20E | Analytical Profile Index 20 Enterobacterales |
| ARGs | Antimicrobial Resistance Genes |
| AST | Antimicrobial Susceptibility Testing |
| CLSI | Clinical and Laboratory Standards Institute |
| CSF | Cerebrospinal Fluid |
| CCN | Clinical Case Notification |
| |COVID-19 | Coronavirus Disease 2019 |
| ddPCR | Droplet Digital Polymerase Chain Reaction |
| DNA | Deoxyribonucleic Acid |
| DOAJ | Directory of open access journals |
| ESBL | Extended-Spectrum Beta-Lactamase |
| GI | Gastrointestinal |
| GLASS | Global Antimicrobial Resistance Surveillance System |
| HAI | Hospital-Acquired Infection |
| HAV | Hepatitis A Virus |
| HEV | Hepatitis E Virus |
| ICU | Intensive Care Unit |
| IPC | Infection Prevention and Control |
| IRB | Institutional Review Board |
| LMICs | Low- and Middle-Income Countries |
| MDRO | Multidrug-Resistant Organism |
| MDPI | Multidisciplinary Digital Publishing Institute |
| Mesh | Medical Subject Headings |
| MIC | Minimum Inhibitory Concentration |
| MDRO | Multidrug-Resistant Organism |
| MS2 | MS2 Bacteriophage |
| PMMoV | Pepper Mild Mottle Virus |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| qPCR | Quantitative Polymerase Chain Reaction |
| RNA | Ribonucleic Acid |
| RSV | Respiratory Syncytial Virus |
| RT-PCR | Reverse Transcription Polymerase Chain Reaction |
| RT-qPCR | Reverse Transcription Quantitative PCR |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| SSIs | Surgical Site Infections |
| UN DESA | United Nations Department of Economic and Social Affairs |
| WHO | World Health Organization |
| WBE | Wastewater-Based Epidemiology |
| WPV | Wild Poliovirus |
References
- Medema, G.; Been, F.; Heijnen, L.; Petterson, S. Implementation of environmental surveillance for SARS-CoV-2 virus to support public health decisions: Opportunities and challenges. Curr. Opin. Environ. Sci. Health 2021, 17, 49–71. [Google Scholar] [CrossRef]
- Bivins, A.; North, D.; Ahmad, A.; Ahmed, W.; Alm, E.; Been, F.; et al. Wastewater-based epidemiology: Global collaborative to maximize contributions in the fight against COVID-19. Environ. Sci. Technol. 2020, 54(13), 7754–7757. [Google Scholar] [CrossRef]
- Daughton, C.G. Wastewater surveillance for population-wide COVID-19: The present and future. SCI. Total Environ. 2020, 736, 139631. [Google Scholar] [CrossRef] [PubMed]
- Troeger, C.; Blacker, B.F.; Khalil, I.A.; et al. Global morbidity and mortality of diarrhea, 195 countries (GBD 2016). Lancet Infect. Dis. 2018, 18(11), 1211–1228. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. GLASS Report 2021; WHO: Geneva, 2021. [Google Scholar]
- Fischer Walker, C.L.; Perin, J.; Aryee, M.J.; et al. Diarrhea incidence in LMICs, 1990–2010. BMC Public Health 2012, 12, 220. [Google Scholar] [CrossRef]
- Fischer Walker, C.L.; Rudan, I.; Liu, L.; et al. Global burden of childhood pneumonia & diarrhea. Lancet 2013, 381(9875), 1405–1416. [Google Scholar] [CrossRef]
- Rees, C.A.; Luo, T.X.; Zhou, S.S.; et al. Barriers to surveillance in LMICs. BMJ Glob. Health 2021, 6, e004216. [Google Scholar]
- Amuquandoh, A.; Effah, E.; Ohene, S.A.; et al. Surveillance challenges in low-income settings. Pan Afr. Med. J. 2020, 36, 133. [Google Scholar]
- Mukhopadhyay, S.; et al. Limitations of clinical case reporting in resource-poor settings. Trop. Med. Int. Health 2019, 24(10), 1204–1214. [Google Scholar]
- Kupferschmidt, K.; Cohen, J. China’s COVID-19 strategy evaluation. Science 2020, 367(6482), 1061–1062. [Google Scholar] [CrossRef]
- Wu, F.; Zhang, J.; Xiao, A.; et al. High SARS-CoV-2 titers in wastewater. Nat. Biotechnol. 2020, 38, 1037–1043. [Google Scholar] [CrossRef]
- Peccia, J.; Zulli, A.; Brackney, D.E.; et al. Wastewater RNA tracks community infection dynamics. Nat. Biotechnol. 2020, 38, 1164–1167. [Google Scholar] [CrossRef] [PubMed]
- Kitajima, M.; Ahmed, W.; Bibby, K.; et al. SARS-CoV-2 in wastewater: Knowledge gaps. Sci. Total Environ. 2020, 739, 139076. [Google Scholar] [CrossRef] [PubMed]
- Norström, A.; et al. Wastewater-based pathogen surveillance: Global evidence. Environ. Int. 2022, 158, 106944. [Google Scholar]
- Ahmed, W.; Angel, N.; Edson, J.; et al. First confirmed SARS-CoV-2 detection in Australian wastewater. Sci. Total Environ. 2020, 728, 138764. [Google Scholar] [CrossRef]
- Rusiñol, M.; Martínez-Puchol, S.; Timoneda, N.; et al. Enteric virus monitoring in wastewater. Curr. Opin. Environ. Sci. Health 2020, 16, 1–12. [Google Scholar]
- Hellmér, M.; Paxéus, N.; Magnius, L.; et al. Early warning of HAV & norovirus from sewage. Appl. Environ. Microbiol. 2014, 80(21), 6771–6781. [Google Scholar] [CrossRef]
- La Rosa, G.; Bonadonna, L.; Lucentini, L.; et al. Emerging viral pathogens in wastewater. Sci. Total Environ. 2020, 734, 139435. [Google Scholar]
- Zhang, T.; Breitbart, M.; Lee, W.H.; et al. Systematic review of enteric viruses in wastewater. Water Res. 2021, 203, 117534. [Google Scholar] [CrossRef]
- Karthikeyan, S.; Levy, J.I.; De Hoff, P.; et al. Early detection of Omicron via wastewater sequencing. Nat. Biotechnol. 2022, 40, 367–370. [Google Scholar] [CrossRef]
- Bibby, K.; Bivins, A.; Wu, Z.; North, D. Wastewater surveillance of respiratory viruses. Science 2021, 371(6526), 1159–1160. [Google Scholar] [CrossRef]
- Betancourt, W.Q.; Schmitz, B.W.; Innes, G.K.; et al. COVID-19 wastewater surveillance for public health action. Emerg. Infect. Dis. 2021, 27(9), 2671–2674. [Google Scholar] [CrossRef]
- Matthews, J.E.; Dickey, B.W.; Miller, R.D.; et al. Epidemiology of norovirus. Clin. Infect. Dis. 2012, 55 Suppl. 4, S120–S126. [Google Scholar] [CrossRef]
- Haramoto, E.; Kitajima, M.; Hata, A.; et al. Virus removal and fate in wastewater treatment. Water Res. 2018, 133, 195–214. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Wastewater-Based Disease Surveillance for Public Health Action. Washington DC: NASEM, 2023. [CrossRef]
- Gahamanyi, N.; et al. Surveillance challenges in Africa. Pan Afr. Med. J. 2022, 41, 52. [Google Scholar]
- Rwanda Biomedical Centre (RBC). Annual Epidemiological Bulletin; Ministry of Health: Kigali, 2023. [Google Scholar]
- Mutesa, L.; Ndishimye, P.; Butera, Y.; et al. Pooled testing strategy for SARS-CoV-2. Nature 2021, 589, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Orschler, L.; Lackner, S. Long-term wastewater SARS-CoV-2 monitoring. Water Res. 2021, 201, 117365. [Google Scholar] [CrossRef]
- Huisman, J.S.; Scire, J.; Caduff, L.; et al. Wastewater surveillance for reproduction number & variants. Nat. Biotechnol. 2023, 41, 528–536. [Google Scholar] [CrossRef]
- Naughton, C.C.; Roman, F.A.; Alvarado, A.G.F.; et al. Global wastewater surveillance needs transparency. Environ. Sci. Technol. 2021, 55(22), 14763–14772. [Google Scholar] [CrossRef]
- World Health Organization. World Health Statistics 2023; WHO: Geneva, 2023. [Google Scholar]
- Ihekweazu, C.; Agogo, E. Africa’s response to COVID-19. BMC Med. 2020, 18, 151. [Google Scholar] [CrossRef]
- United Nations Department of Economic and Social Affairs. World Urbanization Prospects 2022; UN DESA: New York, 2022. [Google Scholar]
- Edson, R.; Rutayisire, R.; El-Khatib, Z.; et al. SARS-CoV-2 detection via wastewater at Kigali International Airport. JMIR Public Health Surveill. 2025, 11, e71104. [Google Scholar] [CrossRef]
- Dzinamarira, T.; Gashema, P.; Iradukunda, P.G.; et al. Utilization of SARS-CoV-2 wastewater surveillance in Africa: A rapid review. Int. J. Environ. Res. Public Health 2022, 19, 969. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Gwee, S.X.W.; Ng, J.Q.X.; et al. Wastewater surveillance to infer COVID-19 transmission: A systematic review. [CrossRef] [PubMed]
- Sci. Total Environ. 2022, 804, 150060. [CrossRef]
- Fernandez-Cassi, X.; Scheidegger, A.; Bänziger, C.; et al. Wastewater monitoring outperforms case numbers when positivity rates are high. Water Res. 2021, 200, 117252. [Google Scholar] [CrossRef]
- Feng, S.; Roguet, A.; McClary-Gutierrez, J.S.; et al. Evaluation of sampling, analysis, and normalization methods for SARS-CoV-2 wastewater concentrations. Sci. Total Environ. 2021, 787, 147449. [Google Scholar] [CrossRef]
- Street, R.; Mathee, A.; Reddy, T.; et al. One year of wastewater surveillance in South Africa supporting COVID-19 clinical findings. Microorganisms 2024, 12, 2230. [Google Scholar] [CrossRef]
- Chukwu, E.E.; Lawal, R.A.; Igboanusi, C.J.; et al. Surveillance of public health pathogens using wastewater in Lagos, Nigeria.
- BMC Public Health 2024, 24, 21157. [CrossRef]
- Mendoza Grijalva, L.; Seck, A.; Roldan-Hernandez, L.; et al. Persistence of respiratory, enteric, and fecal indicator viruses in fecal sludge in Dakar, Senegal. J. Water Sanit. Hyg. Dev. 2024, 14(10), 916–928. [Google Scholar] [CrossRef]
- Van Zyl, WB; et al. Detection of pathogen bacteria in bacteria in wastewater in South Africa. Water SA 2017, 43(2), 239–248. [Google Scholar]
- Edson et al. — Correct Rwanda WBE reference (replacing incorrect Habiyaremye et al.). Edson, R.; Rutayisire, R.; El-Khatib, Z.; Nsekuye, O.; Mucunguzi, H.V.; Muvunyi, R.; et al. SARS-CoV-2 detection in international travelers through wastewater-based epidemiology at the Kigali International Airport: Genomic surveillance study. JMIR Public Health Surveil. 2025, 11, e71104. [CrossRef]
- Pecson; Pecson, B.M.; Darby, E.; Haas, C.N.; Amha, Y.M.; Bartolo, M.; Danielson, R.; et al. Reproducibility and sensitivity of 36 methods to quantify the SARS-CoV-2 genetic signal in raw wastewater: Findings from an interlaboratory evaluation. Environ. Sci.: Water Res. Technol. 2021, 7, 504–520. [Google Scholar] [CrossRef] [PubMed]
- Elmahdy, EM; Shaheen, MNF; Chawla-Sarkar, M; et al. Vertical distribution of enteric viruses in different layers of wastewater treatment plants in Egypt. Food Environ Virol. 2019, 11, 156–165. [Google Scholar] [CrossRef]
- World Health Organization. Polio Environmental Surveillance Expansion Guidelines: Surveillance of Polioviruses in Sewage and Wastewater; WHO: Geneva, 2022. [Google Scholar]
- United Nations – World Urbanization Prospects 2022.
- Johnson, R; et al. Wastewater SARS-CoV-2 trends correlate with clinical cases in South Africa. SCI Total Environ. 2021, 786, 147273. [Google Scholar] [CrossRef]
- Lester, R; et al. National wastewater surveillance for SARS-CoV-2 in South Africa. Water Res. 2022, 219, 118603. [Google Scholar] [CrossRef]
- Street, R; et al. One year of wastewater surveillance in South Africa. Microorganisms 2024, 12, 2230. [Google Scholar] [CrossRef]
- Mahlangu, P; et al. Environmental surveillance for polioviruses in South Africa. J Med Virol. 2019, 91, 144–152. [Google Scholar]
- Gumede, N; et al. Detection of polio in wastewater networks in SA. Commun Dis Surveill Bull 2020. [Google Scholar]
- Nkado, RM; et al. Wastewater as reservoir of AMR genes in South Africa. Sci Total Environ. 2020, 703, 135649. [Google Scholar] [CrossRef]
- Adeniji, JA; et al. Poliovirus detection in wastewater, Nigeria. Virus Res. 2017, 232, 36–44. [Google Scholar]
- Baba, M; et al. Environmental surveillance for poliovirus. J Med Virol. 2018, 90, 1027–1034. [Google Scholar]
- Awolusi, OO; et al. SARS-CoV-2 in wastewater in Nigeria. J Water Health 2023, 21(1), 67–78. [Google Scholar] [CrossRef]
- Elmahdy, EM; et al. HAV & HEV detection in wastewater. Food Environ Virol. 2019, 11, 156–165. [Google Scholar] [CrossRef]
- El-Said, A; et al. Hepatitis viruses in Egyptian sewage. Environ Sci Pollut Res. 2020, 27, 978–987. [Google Scholar]
- Shawky, S; et al. SARS-CoV-2 wastewater detection in Egypt. Sci Total Environ. 2021, 800, 149620. [Google Scholar]
- Barhoumi, M; et al. SARS-CoV-2 wastewater detection in Tunisia. Sci Total Environ. 2021, 760, 144044. [Google Scholar]
- Wurtzer, S; et al. SARS-CoV-2 viral load patterns in wastewater. Sci Total Environ. 2021, 757, 143738. [Google Scholar]
- Nasseri, S; et al. Wastewater surveillance for COVID-19 in Morocco. Sci Total Environ. 2021, 748, 141282. [Google Scholar]
- Kiiru, JN; et al. AMR bacteria in Kenyan wastewater. BMC Microbiol. 2018, 18, 22. [Google Scholar]
- Omwandho, CO; et al. Salmonella in Kenyan wastewater. East Afr Med J 2019. [Google Scholar]
- Oyaro, N; et al. SARS-CoV-2 wastewater detection. J Environ Health Sci Eng. 2021, 19, 865–872. [Google Scholar]
- Katongole, P; et al. AMR bacteria in wastewater. BMC Infect Dis. 2020, 20, 820. [Google Scholar]
- Armah, GE; et al. Norovirus & rotavirus detection in wastewater. J Med Virol. 2016, 88, 1692–1701. [Google Scholar]
- Aboagye, G; et al. Enteric viruses in wastewater. J Appl Microbiol. 2018, 125, 1130–1139. [Google Scholar]
- Diop, OM; et al. Poliovirus surveillance in Senegal. J Infect Dis. 2014, 210, S655–S665. [Google Scholar]
- Mendoza Grijalva, L; et al. Viral persistence in fecal sludge. J Water Sanit Hyg Dev. 2024, 14(10), 916–928. [Google Scholar] [CrossRef]
- Manangazira, P; et al. SARS-CoV-2 wastewater signal detection in Zimbabwe. Pan Afr Med J 2021, 39, 111. [Google Scholar]
- Uwimana, A; et al. SARS-CoV-2 wastewater surveillance in Kigali. Rwanda Public Health Bulletin 2022. [Google Scholar]
- RBC Wastewater Monitoring Report, 2021.
- Ndayishimiye E, et al. Framework for wastewater surveillance in Rwanda. Rwanda J Med Health Sci. 2023.
- Misbah G, et al. Aircraft wastewater genomic surveillance in Rwanda. In press, 2025.
- Alemayehu, T; et al. AMR genes in Ethiopian wastewater. Antibiotics 2020, 9(7), 386. [Google Scholar]
- Wade, M.J.; Lo Jacomo, A.; Armenise, E.; Brown, M.R.; Bunce, J.T.; Cameron, G.; et al. Understanding and managing uncertainty and variability for wastewater monitoring beyond the pandemic: Lessons from the UK national surveillance programme. J. Hazard. Mater. 2022, 424(B), 127456. [Google Scholar] [CrossRef]
- Lodder, *!!! REPLACE !!!*; de Roda Husman Lodder, W; de Roda Husman, AM. SARS-CoV-2 in wastewater: Potential health risk, but also data source. Euro Surveill. 2020, 25(12), 2000302. [Google Scholar] [CrossRef] [PubMed]
- Hendriksen; CorrecHendriksen, RS; Munk, P; Njage, P; van Bunnik, B; McNally, L; Lukjancenko, O; et al. Global monitoring of antimicrobial resistance based on metagenomics analyses of urban sewage. Nat Commun. 2019, 10, 1124. [Google Scholar] [CrossRef] [PubMed]
- Kazama; Kazama, S; Miura, T; Masago, Y; et al. Environmental surveillance of norovirus genogroups I and II in Japan, 2012–2013. Food Environ Virol. 2017, 9, 245–253. [Google Scholar] [CrossRef]
- Awolusi; Awolusi, OO; Omeje, VO; Otunla, A; et al. Assessment of SARS-CoV-2 in wastewater in Nigeria: Implications for viral surveillance. J Water Health 2023, 21(1), 67–78. [Google Scholar]
- DOI: 10.2166/wh.2022.128.
- Africa CDC – Correct official citation. Africa Centres for Disease Control and Prevention. Pathogen Genomics Initiative Annual Reports, 2021–2024. Addis Ababa: Africa CDC; 2021–2024.
- Wolfe; Wolfe, MK; Topol, A; Knudson, A; Simpson, A; White, B; Vugia, DJ; et al. High-frequency, high-resolution wastewater SARS-CoV-2 surveillance for public health action. Environ Sci Technol Lett. 2022, 9(2), 127–132. [Google Scholar] [CrossRef]
- Deboosere et al. (Correct)Deboosere N, Horm SV, Delobel A, et al. Survival of viruses on fresh produce, using MS2 bacteriophage as surrogate. Appl Environ Microbiol. 2012; 78:3242–3248. [CrossRef]
- Bivins; Bibby Bivins, A; Bibby, K. Wastewater surveillance during and beyond COVID-19. Curr Opin Environ Sci Health 2021, 18, 100–108. [Google Scholar] [CrossRef]
- McClary-Gardner; McClary-Gardner, J; Chandra, F; Boehm, AB; et al. Quantifying uncertainty and variability in wastewater SARS-CoV-2 measurements: A multi-laboratory study. Sci Total Environ. 2023, 859, 160024. [Google Scholar] [CrossRef]
- Liu; Liu, P; Ibaraki, M; VanTassell, J; Geith, K; Cavallo, M; Kannayan, A; et al. Modeling spatial and temporal variation in wastewater SARS-CoV-2 concentrations. Sci Total Environ. 2022, 829, 154622. [Google Scholar] [CrossRef]
- Africa CDC – Correct institutional citation Africa Centres for Disease Control and Prevention. Early Warning and Surveillance Strategy 2023–2027. Addis Ababa: Africa CDC; 2023.
Figure 2.
Wastewater-based epidemiology studies in Africa.
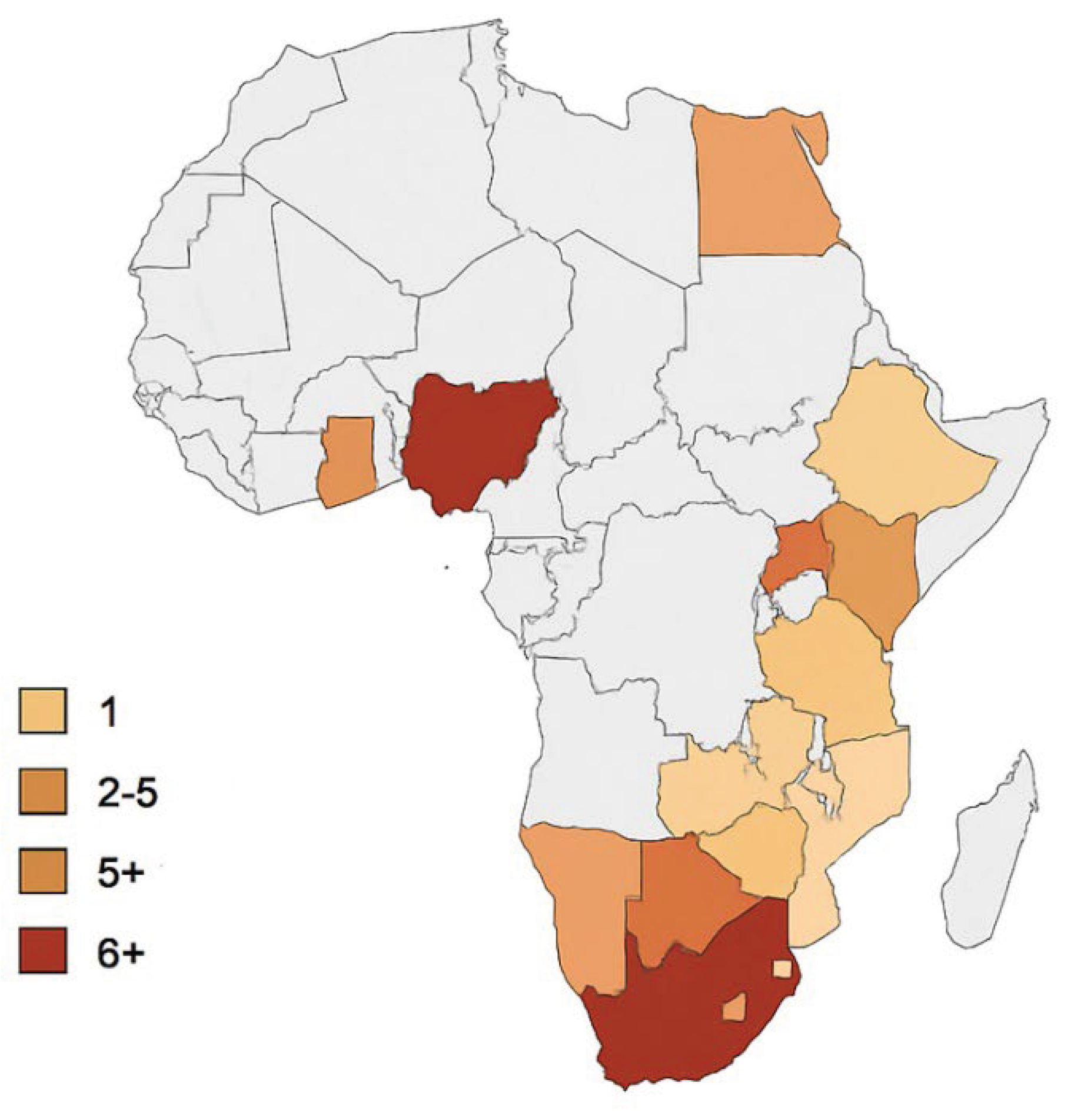

Table 1.
Detection of Gastrointestinal Pathogens in Wastewater.
| Pathogen Group | Specific Pathogens | Preferred Detection Method(s) | Reference |
| Enteric viruses | Norovirus, Rotavirus, Enteroviruses, HAV | RT-qPCR, ddPCR | La Rosa et al., 2019 [19] ; Hellmér et al., 2014 [18] |
| Bacterial pathogens | AMR pathogens in sewage, Salmonella spp., Shigella spp., Vibrio cholera | Culture, qPCR, sequencing | Van Zyl et al., 2017 [44] Hendrick sen et al., 2019 [81] |
| Protozoa | Giardia, Cryptosporidium | Immunofluorescence, qPCR | Kitajima et al., 2020 [14] |
| AMR markers | blaCTX-M, blaNDM, macrolide-resistance genes | qPCR, metagenomic sequencing | Hendriksen et al., 2019 [81] |
Table 2.
Summarizes Major Pathogens Detectable in Wastewater.
| Country | Study Focus | Pathogens Detected | Analytical Platform | Reference |
| Rwanda | SARS-CoV-2 wastewater surveillance and feasibility | SARS-CoV-2 (RNA) | RT-qPCR, passive sampling | Edson et al., 2025 [36]; |
| South Africa | National WBE network for COVID-19 | SARS-CoV-2, PMMoV | RT-qPCR, normalization | Street et al., 2024 [41] |
| Nigeria | Enteric virus detection | Enteroviruses, adenovirus, norovirus | RT-PCR, cell culture | Awolusi et al., 2023 [58] |
| Senegal | Fecal sludge/ Viral persistence | Enteric and respiratory viruses | RT-qPCR | Mendoza Grijalya et al., 2024 [43] |
| Egypt | Detection of HAV and HEV viruses | HAV, HEV | RT-PCR | Elmahdy et al., 2019 [59] |
| South Africa | Bacterial pathogen tracking | Salmonella, Shigella, Vibrio | Culture + PCR | Van Zyl et al., 2017 [44] |
Table 3.
Detection of Respiratory Pathogens in Wastewater.
| Pathogen | Rationale for Wastewater Detection | Analytical Platform | Reference |
| SARS-CoV-2 | Fecal shedding; mucosal shedding | RT-qPCR, ddPCR, sequencing | Kitajima et al., 2020 [14]; Edson et al., 2025 [36] |
| Influenza A/B | Fecal shedding in infected individuals | RT-qPCR | Wolfe et al., 2022 [85] |
| RSV | Presence in stool and respiratory excretions | RT-qPCR | Wolfe et al., 2022 [53] |
| Human adenovirus | Dual GI and respiratory involvement | qPCR | La Rosa et al., 2019 [19] |
Table 4.
Correlation Between Wastewater Signals and Clinical Cases.
| Pathogen | Correlation Outcome | Setting | Reference |
| SARS-CoV-2 | Wastewater signal increases precede clinical cases by 4 to 14 days | Rwanda, Europe, USA | Huisman et al., 2022 [31]; Edson et al., 2025 [36] |
| Norovirus | Wastewater peaks reflect seasonal occurrences | Sweden | Hellmér et al., 2014 [18] |
| Polio | Strong correlation between wastewater and AFP surveillance | Global (WHO) | WHO poliovirus guidelines, 2022 [49] |
| Hepatitis A | Strong correlation between wastewater and AFP surveillance | Japan, Italy | La Rosa et al., 2019 [19] |
Table 5.
Strengths and Limitations of WBE.
| Category | Key Points | Reference |
| Strengths | Early detection, population-wide coverage, cost-effective, includes asymptomatic infections | Medema et al., 2021 [37] |
| Limitations | Infrastructure gaps, variable viral decay, quantification challenges, limited lab capacity | Wade et al., 2022 [79] |
Table 6.
Opportunities for WBE Implementation in Low-Resource African Settings.
| Opportunity Area | Description | Reference |
| Passive sampling | Low-cost, suitable for irregular sewage systems | Liu et al., 2022 [89] |
| Integration with Africa CDC networks | Strengthening surveillance through genomics initiatives | Africa CDC, 2023 [90] |
| Urban sanitation expansions | Improving coverage in cities such as Kigali, Nairobi | UN Urbanization Report 2022 [49] |
| Workforce and lab capacity-building | Training in PCR, sequencing, AMR monitoring | Hendriksen et al., 2019 [81] |
Table 7.
Wastewater-Based Epidemiology (WBE) Studies in Africa.
| Country | Research topic | Disease/Pathogen identified | Papers | Platform used |
Scientific References |
| South Africa | SARS-CoV-2 detection in municipal wastewater | COVID-19 | 6+ | RT-qPCR, Sequencing (illumine) PEG concentration | Johnson R. et al., 2021 [50]; Lester et al., 2022 [51]; Street et al., 2024 [52] |
| Poliovirus environmental surveillance | Polio (WPV, cVDPV) | 3 | Cell culture, RT-PCR | Mahlangu et al., 2019 [53]; Gumede et al., 2020 [54] | |
| AMR genes in wastewater | Antimicrobial resistance | 2 | Metagenomics, qPCR | Nkado R. et al., 2020 [55] | |
| Nigeria | Poliovirus environmental surveillance (national surveillance program) | Polio | 5+ | PCR, cell culture | Adeniji et al., 2017 [56]; Baba et al., 2018 [57]; |
| SARS-CoV-2 in wastewater | COVID-19 | 1 | RT-qPCR | Awolusi et al., 2023 [58] | |
| Egypt | Hepatitis A&E monitoring in wastewater | HAV, HEV | 2 | RT-PCR | El-Mahdy et al., 2019 [59]; El-Said et al., 2020 [60] |
| SARS-CoV-2 detection | COVID-19 | 1 | RT-qPCR | Shawky et al., 2021 [61] | |
| Tunisia | SARS-CoV-2 detection in wastewater | COVID-19 | 2 | RT-qPCR; | Barhoumi et al., 2021 [62]; Wurtzer et al., 2021 [63] |
| Morocco | Surveillance of SARS-CoV-2 in urban wastewater | COVID-19 | 1 | RT-qPCR | Nasseri et al., 2021 [64] |
| Kenya | Antibiotic resistance bacteria in wastewater | AMR bacteria (E. Coli, Klebsiella, Salmonella | 2 | Culture, AST, PCR | Kiiru et al., 2018 [65]; Omwandho et al., 2019 [66]; |
| SARS-CoV-2 wastewater surveillance | COVID-19 | 1 | RT-qPCR | Oyaro et al., 2021 [67] | |
| Uganda | AMR monitoring in wastewater | Resistance E. Coli & Enterococcus | 1 | Culture based, PCR | Katongole et al., 2020 [68] |
| Ghana | Environmental detection of enteric viruses | Norovirus, Rotavirus, Adenovirus | 2 | RT-PCR | Armah et al., 2016 [69]; Aboagye et al., 2018 [70] |
| Senegal | Polio environmental surveillance | Polioviruses | 2 | Cell culture, PCR | Diop et al., 2014 [71]; Mendoza et al., 2024 [72] |
| Zimbabwe | SARS-CoV-2 surveillance | COVID-19 | 1 | RT-qPCR | Manangazira et al., 2021 [73] |
| Rwanda | SARS-CoV-2 detection in municipal wastewater | COVID-19 | 2 | RT-qPCR, viral concentration (PEG) Sequencing support via regional labs | Uwimana A. et al., 2022 [74]; University of Rwanda - RBC wastewater monitoring report, 2021 [75] |
| Development of wastewater surveillance framework for early outbreak detection | Multi-pathogen (SARS-CoV-2) enteric viruses | 1 | RT-qPCR, environmental sampling protocol | Ndayishimiye et al., 2023 [76] | |
| Airport-based WBE and genomic surveillance using aircraft wastewater and pooled nasal swabs from international travelers at Kigali International Airport | SARS-CoV-2 and variants and other imported lineages | ≥2 peer-reviewed genomic surveillance studies using wastewater & swabs at the airport | Aircraft wastewater sampling + pooled nasal swabs; RT-qPCR and whole-genome sequencing to detect/imported variants; integration with national genomic surveillance | Edson R et al., 2025 [36]; (Misbah G et al., 2025 [77] | |
| Ethiopia | AMR genes | ARGs (blaCTX-M, mecA, etc.) |
1 | qPCR | Alemayehu et al., 2020 [78] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



