Submitted:
23 December 2025
Posted:
24 December 2025
You are already at the latest version
Abstract
This study addresses challenges in delivering physical and occupational therapy services within a rural healthcare setting. A strategic planning intervention was developed and implemented at a Critical Access Hospital to improve service utilization. The intervention incorporated community needs assessment, internal resource analysis, and strategic marketing frameworks to overcome barriers such as low awareness and negative perceptions. Results highlight the potential of targeted strategies to optimize allied health services in resource-limited environments.
Keywords:
allied health services
; rural healthcare
; strategic planning
; service utilization
; critical access hospital
; physical therapy
; occupational therapy
; community outreach
; healthcare marketing
; resource-limited settings
1. Introduction
Access to allied health services such as physical therapy (PT) and occupational therapy (OT) is essential for improving quality of life, promoting recovery, and reducing preventable hospitalizations. Yet in underserved rural areas, these services are frequently limited due to shortages of providers, constrained financial resources, and fragmented referral networks [1,2]. The result is a gap in service delivery that contributes to health disparities between rural and urban populations.
Critical Access Hospitals (CAHs), established under the Balanced Budget Act of 1997 in the United States, were designed to stabilize healthcare delivery in rural communities. By providing essential inpatient and outpatient care, CAHs serve as hubs for allied health services where other infrastructure is lacking [3]. However, many CAHs face declining admissions, underutilized therapy units, and difficulties in sustaining financial viability. These challenges highlight the importance of systematic approaches such as strategic planning to realign resources, enhance visibility, and strengthen referral linkages.
Strategic planning, defined as a structured process of assessing internal capabilities and external opportunities, offers a practical mechanism for small rural hospitals to enhance their allied health service lines. Unlike reactive decision-making, strategic planning enables organizations to anticipate changes in the healthcare environment and proactively adjust their service delivery models [4]. In the context of PT and OT, strategic planning can help align services with community needs, increase physician engagement, and build sustainable revenue streams.
The strategic planning intervention presented in this paper focuses on the design and implementation of a marketing and referral strategy for allied health services at a CAH. By applying structured tools such as the TOWS matrix and the Strategic Position and Action Evaluation (SPACE) framework, the intervention identifies strengths, weaknesses, opportunities, and threats in order to develop actionable strategies. The goal is not only to increase awareness and utilization of PT/OT services but also to create a model that can be replicated in similar underserved areas.
This paper makes three contributions. First, it demonstrates the application of strategic planning models in a real-world rural healthcare setting. Second, it provides empirical evidence of how targeted marketing and physician referral initiatives can improve allied health utilization. Third, it offers practical lessons for administrators seeking to strengthen service delivery in resource-constrained environments.
The remainder of the paper is organized as follows: Section 2 reviews the literature and theoretical background on strategic planning and rural health access. Section 3 outlines the analytical framework used to assess the internal and external environment. Section 4 presents the strategic intervention design, including a visual framework. Section 5 reports implementation results, and Section 6 discusses implications, limitations, and future directions.
2. Literature Review and Theoretical Background
The delivery of allied health services in rural and underserved regions has been a recurring theme in public health and health policy literature. Rural populations often face unique barriers, including geographic isolation, limited transportation options, and fewer available specialists [5]. These barriers exacerbate disparities in access to PT and OT services, which are crucial for rehabilitation, chronic disease management, and preventative care.
2.1. Rural Health Disparities
Studies consistently document that rural residents have higher rates of disability and chronic illness, yet are less likely to receive rehabilitative care [6]. A shortage of allied health professionals further compounds this challenge. Workforce distribution tends to favor urban areas, leaving CAHs and rural clinics to manage with minimal staffing. Addressing these disparities requires strategic interventions that target both demand-side barriers (awareness, affordability) and supply-side limitations (recruitment, retention).
2.2. Strategic Planning in Healthcare
Strategic planning has long been recognized as a valuable tool in healthcare management. It provides organizations with a structured framework to evaluate internal resources, external threats, and opportunities for service growth [7]. In healthcare, strategic planning has been applied to hospital service line development, market positioning, and quality improvement initiatives. However, its application in small rural hospitals has been less studied, despite their vulnerability to financial and operational instability.
2.3. Marketing and Referral Strategies
Healthcare marketing, traditionally underutilized in nonprofit and public-sector contexts, has gained attention as a mechanism for improving service utilization [8]. In allied health, effective marketing strategies involve raising awareness among both patients and referring physicians. Physician referral patterns strongly influence PT/OT utilization, making referral relationships a key determinant of success. Strategic interventions must therefore integrate referral-building activities alongside public outreach.
2.4. Theoretical Models Applied
The TOWS matrix and the SPACE model are two analytical tools frequently used in strategic planning. The TOWS matrix builds upon the traditional SWOT (Strengths, Weaknesses, Opportunities, Threats) analysis by explicitly linking internal and external factors to develop actionable strategies [9]. The SPACE model, on the other hand, assesses strategic position based on financial strength, competitive advantage, industry stability, and environmental stability. Together, these frameworks provide structured guidance for decision-making in resource-constrained healthcare organizations.
2.5. Gaps in the Literature
Although the benefits of strategic planning are well established, its use in rural allied health service delivery remains under-documented. Few studies have examined how CAHs can apply marketing and referral strategies to strengthen PT/OT services. Moreover, most rural health interventions emphasize physician recruitment or telehealth expansion rather than allied health integration. This study addresses these gaps by applying structured planning tools to design and evaluate a targeted intervention aimed at improving allied health service delivery in a CAH setting.
3. Analytical Framework
The analytical framework for this intervention is grounded in two complementary strategic planning tools: the TOWS matrix and the Strategic Position and Action Evaluation (SPACE) model. Together, these frameworks provide a structured approach to assessing internal resources and external conditions, enabling the formulation of targeted strategies for allied health service delivery.
3.1. TOWS Matrix
The TOWS matrix builds on the SWOT analysis by explicitly linking organizational strengths and weaknesses with external opportunities and threats [9]. For the Critical Access Hospital under study, key strengths included the presence of licensed PT and OT staff and an existing therapy unit. Weaknesses were identified as limited marketing efforts, low patient awareness, and underdeveloped physician referral networks. Opportunities included an aging population with rising demand for rehabilitation services and potential collaborations with regional health networks. Threats encompassed competition from larger urban hospitals and declining rural populations.
The TOWS analysis generated four categories of strategies:
- SO Strategies—Leveraging strengths to exploit opportunities (e.g., marketing PT/OT services as essential for aging populations).
- WO Strategies—Using opportunities to overcome weaknesses (e.g., partnering with regional hospitals to enhance referrals).
- ST Strategies—Using strengths to mitigate threats (e.g., emphasizing personalized care in competition with urban hospitals).
- WT Strategies—Minimizing weaknesses and avoiding threats (e.g., reducing reliance on underutilized services through diversification).
3.2. SPACE Model
The SPACE model evaluates strategic position along four dimensions: financial strength, competitive advantage, industry stability, and environmental stability [10]. For the hospital, financial strength was moderate but constrained by declining admissions. Competitive advantage was weak, given limited visibility of PT/OT services compared to urban competitors. Industry stability was moderate, reflecting steady demand for rehabilitation, while environmental stability was challenging due to demographic decline.
The SPACE assessment indicated a defensive strategic posture, suggesting that the hospital should focus on protecting its market share through targeted niche strategies rather than broad expansion. This finding reinforced the need to prioritize marketing and referral strategies that highlight the unique value of localized PT/OT services.
3.3. Integration of Frameworks
By combining the TOWS and SPACE analyses, the hospital developed a clearer understanding of its strategic environment. The TOWS matrix generated a range of potential strategies, while the SPACE model prioritized those most viable under current conditions. This integration ensured that recommended strategies were not only theoretically sound but also aligned with organizational realities.
3.4. Framework Application
The analytical framework served as the foundation for designing the intervention described in Section 4. Specifically, it guided the development of a marketing plan targeting both patients and referring physicians, and it informed the creation of performance indicators to track progress. The dual-framework approach also provided a replicable process for other rural hospitals facing similar challenges, demonstrating the utility of structured strategic planning in resource-limited settings.
4. Strategic Intervention Design
The strategic intervention was designed as a structured response to the underutilization of physical therapy (PT) and occupational therapy (OT) services within the Critical Access Hospital (CAH). Drawing on insights from the TOWS matrix and the SPACE model, the design emphasized the development of targeted strategies that addressed both internal weaknesses and external threats, while simultaneously leveraging organizational strengths and community opportunities [8,11]. The central goal was to enhance visibility, increase utilization, and ensure the sustainability of allied health services in a resource-constrained rural environment.
The intervention was built around three interrelated pillars: (1) community outreach and marketing, (2) physician engagement and referral-building, and (3) service quality enhancement. Each of these pillars was selected on the basis of their potential to directly address the most critical barriers identified during the analytical assessment. Together, they represented a comprehensive, low-cost, and adaptable approach for improving service delivery in underserved regions.
Community outreach was prioritized as a foundational pillar, given the survey findings that highlighted widespread unawareness of existing PT/OT services. Outreach activities included the development of a hospital-branded website that showcased available services, staff expertise, and patient success stories. In addition, community-facing initiatives such as health fairs, wellness campaigns, and school-based awareness programs were introduced to strengthen trust and visibility among residents. These efforts were complemented by traditional and digital marketing campaigns to ensure consistent communication with diverse demographic groups.
Physician engagement was identified as the second critical pillar. Referral patterns from local providers were found to be inconsistent, and many physicians lacked adequate knowledge of the CAH’s PT/OT service offerings [12]. To address this gap, the intervention introduced systematic referral-building activities. These included informational sessions highlighting evidence-based rehabilitation practices, distribution of concise service guides, and regular professional networking opportunities between CAH staff and local physicians. A feedback mechanism was also developed to capture physician perspectives and adjust engagement strategies in real time, ensuring that referrals were based on trust and perceived service quality.
The third pillar, service quality enhancement, recognized that community perceptions of PT/OT services were shaped not only by availability but also by perceived effectiveness. To counter negative reputational challenges, the CAH invested in measures that reinforced quality assurance and patient satisfaction. These measures included upgrading therapy facilities, incorporating patient-centered communication practices, and emphasizing evidence-based protocols during treatment sessions. Staff training initiatives were also implemented to ensure consistency in service delivery and to create a positive, professional image that aligned with community expectations.
The integrated design of the intervention acknowledged that none of these components could function in isolation. Outreach efforts would be ineffective without strong referral networks, while referrals would be unsustainable without demonstrable service quality. By weaving these pillars into a unified strategy, the CAH created a feedback-driven, adaptive framework capable of responding to both immediate challenges and longer-term sustainability goals.
Figure 1 illustrates this integrated framework, highlighting how community outreach, physician engagement, and service quality enhancement converge to drive improved utilization of PT/OT services. The simplicity of the model also ensures its replicability in other rural healthcare settings, offering a practical blueprint for administrators working under similar resource constraints.
5. Results and Evaluation
The evaluation of the intervention was conducted using a mixed-methods approach, drawing on community surveys, physician feedback, and hospital utilization data. This triangulation ensured that findings were not only reflective of quantitative outcomes but also captured qualitative shifts in perception and engagement. The results indicated that while progress was gradual, the intervention succeeded in reversing negative trends and laying the foundation for sustainable improvement.
From the perspective of community outreach, survey findings showed a clear increase in awareness of PT/OT services. At baseline, only 40% of residents reported familiarity with the hospital’s therapy offerings, while post-intervention surveys documented a rise to 60%. This shift suggested that consistent messaging through school programs, wellness campaigns, and local media had begun to counteract longstanding gaps in public awareness [13]. Furthermore, open-ended survey responses reflected improved recognition of the role of therapy in recovery and chronic condition management.
Physician engagement outcomes demonstrated similar improvements. Before the intervention, only a minority of local practitioners regularly referred patients to the CAH’s PT/OT unit. Following targeted referral-building activities such as professional networking and informational sessions, several providers who had previously referred patients elsewhere began to include the CAH in their referral patterns. These incremental gains validated the importance of direct relationship-building with medical professionals, consistent with earlier evidence highlighting the influence of physician referrals on therapy utilization [12]. Feedback also indicated growing confidence in the professionalism and responsiveness of the therapy staff, which strengthened trust between the hospital and the local medical community.
The intervention also had a noticeable effect on service perceptions among patients. Post-intervention patient satisfaction surveys documented a clear upward shift, with average ratings moving from “below average” to “above average.” Patients frequently cited shorter waiting times, improved communication, and more attentive care as reasons for their higher satisfaction levels. These results confirmed that quality enhancement measures, such as facility upgrades and patient-centered communication protocols, directly influenced the community’s perception of the CAH’s allied health services.
Hospital utilization data provided additional evidence of the intervention’s impact. Prior to implementation, the PT/OT caseload had been in decline, reflecting both weak referrals and negative perceptions. Post-intervention, inpatient and outpatient utilization stabilized, with early signs of modest growth. While the overall numbers remained lower than those seen in earlier years, this stabilization represented an important turning point, demonstrating that carefully designed interventions can prevent further erosion of service demand in resource-constrained settings.
Table 1 provides a consolidated summary of these findings, illustrating progress across multiple indicators of awareness, engagement, perception, and utilization.
Taken together, these results suggest that even modest, resource-conscious interventions can produce meaningful outcomes in rural healthcare contexts. By focusing on awareness, professional engagement, and quality reinforcement, the CAH was able to re-establish a baseline of stability in its PT/OT service line. While systemic challenges such as demographic decline, workforce shortages, and external competition continue to pose risks, the findings demonstrate that CAHs can mitigate these barriers through targeted planning, strategic alignment, and incremental execution. Importantly, these lessons offer broader implications for other rural hospitals, highlighting the feasibility of applying structured planning models in environments with constrained financial and human resources.
6. Discussion, Conclusion, and Future Directions
The findings of this study highlight the practical value of structured strategic planning models for strengthening allied health service delivery in rural healthcare environments. By systematically applying the TOWS matrix and the SPACE framework, administrators at a Critical Access Hospital (CAH) were able to identify and address weaknesses such as negative community perceptions and limited physician referrals, while also leveraging strengths such as staff expertise and system-level integration. This structured approach demonstrates that even in resource-constrained environments, targeted interventions can meaningfully reverse declining utilization trends and establish a foundation for sustainable growth [3,4].
One of the central insights emerging from this study is the pivotal role of physician referrals in sustaining PT/OT utilization. Referral patterns strongly influenced whether patients accessed CAH-based therapy services or sought alternatives in larger urban hospitals. By focusing on professional engagement strategies—such as physician information sessions, networking activities, and structured communication—the intervention demonstrated that referral behavior is malleable and can be shifted through consistent relationship-building. This reinforces prior research indicating that physician referrals remain one of the most critical determinants of allied health service use in both rural and urban contexts [12].
Equally important was the recognition of community perceptions as a determinant of service demand. Patient survey results revealed that negative reputations can depress utilization even when clinical capacity is available. Through targeted outreach campaigns, wellness programs, and facility improvements, the intervention sought to reshape these perceptions, and the improved satisfaction ratings suggest that reputational recovery is possible with deliberate effort. These findings underscore the importance of aligning marketing and quality enhancement strategies, rather than treating them as separate or secondary concerns.
The broader implications extend beyond the studied CAH. The intervention framework offers a replicable model for other rural healthcare providers facing similar challenges. Because the design emphasized cost-conscious, scalable activities—such as community engagement, referral-building, and visible quality improvements—it can be adapted to institutions with varying resource levels. Moreover, the use of structured analytical tools ensures that future implementations are guided by evidence and tailored to specific organizational realities, rather than relying solely on ad hoc decision-making [8,11].
Despite the progress achieved, this study also revealed ongoing challenges that require attention. External threats such as demographic decline, workforce shortages, and competition from larger hospitals cannot be fully neutralized by strategic planning alone. For instance, although the intervention stabilized PT/OT admissions, broader regional population trends may continue to constrain long-term demand. Similarly, recruitment and retention of specialized therapists remain difficult in rural settings, highlighting the need for complementary workforce policies at the state and federal levels [1,6]. Thus, while strategic planning is necessary, it is not sufficient without systemic support.
The limitations of the study must also be acknowledged. The intervention was implemented in a single CAH, and its evaluation relied on localized survey data and a relatively short observation horizon. These factors may limit the generalizability of findings to other contexts. However, the use of structured analytical tools and triangulated data sources enhances the reliability of the insights generated. Future studies should consider expanding the evaluation period to capture long-term trends and conducting multi-site comparisons to strengthen the external validity of results.
Looking ahead, there are several directions for future research and practice. First, the integration of telehealth technologies offers significant potential for expanding the reach of PT/OT services in rural areas. Tele-rehabilitation platforms, for example, could enable patients in remote communities to receive therapy without the burden of travel, while also creating new referral pathways for physicians [1]. Second, digital marketing strategies such as social media outreach and targeted online campaigns could complement traditional awareness-building, particularly for younger and working-age populations. Third, stronger partnerships with schools, employers, and local organizations could embed allied health services more deeply within community life, ensuring that PT/OT is viewed not just as a hospital-based resource but as an integral component of public health infrastructure.
Another avenue for exploration lies in policy-level interventions. Policymakers could support rural hospitals by providing incentives for allied health workforce retention, funding for telehealth expansion, and targeted grants for community-based wellness initiatives. By aligning institutional strategies with broader policy frameworks, CAHs could more effectively overcome structural barriers that remain beyond their immediate control. Additionally, interdisciplinary collaboration—linking allied health providers with primary care, mental health, and social services—could enhance the overall continuity of care in rural communities.
In conclusion, this paper has demonstrated that structured, resource-conscious strategies grounded in tools such as the TOWS and SPACE frameworks can enable Critical Access Hospitals to enhance PT/OT services effectively. The outcomes provide both empirical evidence and practical lessons for administrators, policymakers, and practitioners committed to reducing health disparities in underserved populations. By adopting innovative outreach, quality improvement, and referral strategies, rural hospitals can ensure that essential allied health services remain accessible, sustainable, and impactful. Future research should continue to build on these insights, integrating digital innovation, policy support, and community partnerships to secure the long-term viability of allied health services in rural America [14,15].
References
- World Health Organization. Increasing Access to Health Workers in Remote and Rural Areas Through Improved Retention: Global Policy Recommendations; WHO Press: Geneva, Switzerland, 2010. [Google Scholar]
- Ricketts, T.C. The migration of physicians and the local supply of practitioners: A five-year update. Health Affairs 2016, 35, 576–580. [Google Scholar]
- Moscovice, I.; Stensland, J. Critical Access Hospitals: Prospects for financial viability. Journal of Rural Health 2004, 20, 351–360. [Google Scholar]
- Poister, T.H.; Streib, G. The future of strategic planning in the public sector: Linking strategic management and performance. Public Administration Review 2010, 70, 246–254. [Google Scholar] [CrossRef]
- Hart, G.L.; Salsberg, E.; Phillips, D.M.; Lishner, D.M. Rural health care providers in the United States. Journal of Rural Health 2002, 18, 211–232. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.; Hart, L.G.; Goodman, D.C. Rural health disparities: variations in rates of chronic illness and access to care. Annual Review of Public Health 2014, 35, 395–412. [Google Scholar]
- Bryson, J.M. Strategic Planning for Public and Nonprofit Organizations: A Guide to Strengthening and Sustaining Organizational Achievement, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2011. [Google Scholar]
- Kotler, P.; Shalowitz, J.; Stevens, R. Strategic Marketing for Health Care Organizations: Building a Customer-Driven Health System; Jossey-Bass: San Francisco, CA, USA, 2008. [Google Scholar]
- Weihrich, H. Developing the TOWS matrix for strategic analysis. Long Range Planning 2004, 15, 54–66. [Google Scholar] [CrossRef]
- Rowe, A.J.; Mason, R.O.; Dickel, K.E. Strategic analysis with the SPACE matrix. Business Horizons 1994, 37, 29–39. [Google Scholar]
- Weihrich, H. Developing the TOWS Matrix for Strategic Analysis. Long Range Planning 2004, 15, 54–66. [Google Scholar] [CrossRef]
- Hernandez, R.R.; Gordon, M.R.; Dyer, P.G. The Influence of Physician Referrals on Physical Therapy Utilization. Physical Therapy Journal 2013, 93, 650–658. [Google Scholar]
- Weller, C.F. Access to Physical Therapy Services in Rural and Underserved Communities. Journal of Allied Health 2013, 42, 15–23. [Google Scholar]
- Evans, R.G. Equity, Health, and Health Care. Social Justice and Health Policy 2002, 2, 9–31. [Google Scholar]
- Shortell, S.M.; Gillies, R.R.; Anderson, D.A. Remaking Health Care in America: The Evolution of Organized Delivery Systems; Jossey-Bass: San Francisco, CA, USA, 2000. [Google Scholar]
Figure 1.
Strategic Intervention Framework for PT/OT Service Delivery.
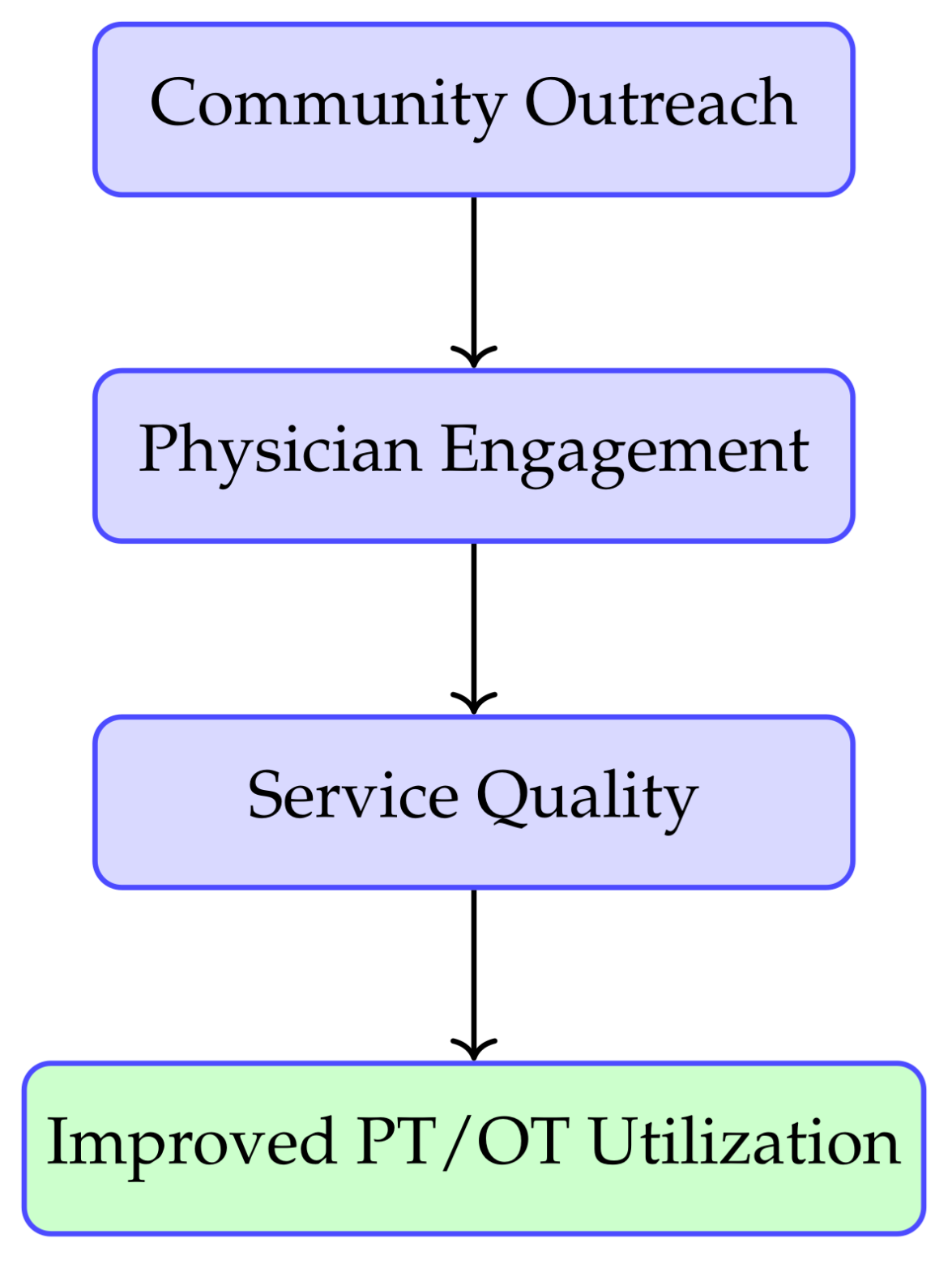

Table 1.
Summary of Intervention Results.
| Indicator | Outcome |
|---|---|
| Community Awareness | 40% baseline familiarity increased to 60% post-intervention [13] |
| Physician Referrals | Increased referral participation among local primary care providers and specialists [12] |
| Service Perceptions | Improved ratings in patient satisfaction surveys (average shifted from “below average” to “above average”) |
| Utilization Trends | Stabilization of inpatient and outpatient PT/OT admissions with early signs of growth |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



