1. Introduction
Lamotrigine is a widely used anticonvulsant and mood stabilizer, primarily prescribed for epilepsy and the long-term management of bipolar disorder [
1,
2]. Its strength lies in preventing depressive relapse, and its generally favorable tolerability profile makes it an attractive therapeutic option. Nonetheless, careful dose titration is essential to minimize the risk of severe rash, a rare but serious adverse effect [
3,
4].
Therapeutic drug monitoring (TDM) plays a central role in optimizing lamotrigine therapy [
5,
6,
7]. Target plasma concentrations typically range between 5–60 µmol/L, balancing efficacy in seizure control with the avoidance of toxicity. The substantial interindividual variability in lamotrigine pharmacokinetics—driven by factors such as hepatic function, age, pregnancy, and concomitant enzyme-inducing or -inhibiting medications—necessitates TDM and individualized dose adjustments [
8,
9,
10]). Recent pharmacokinetic modeling and simulation studies highlight how patient-specific characteristics can markedly influence exposure, underscoring the need for robust and adaptable measurement strategies in clinical laboratories. Retrospective real-world TDM data further illustrate the complexity of dose–concentration relationships, particularly in heterogeneous epilepsy populations undergoing polytherapy, reinforcing the importance of reliable longitudinal assay performance [
11].
Traditional quality assurance in TDM relies on internal quality control and external proficiency testing. While indispensable, these approaches may not fully capture subtle, practice-level shifts that accumulate over time. Patient-based quality control (PBQC) strategies—especially those leveraging aggregated patient statistics—offer a complementary framework for continuous surveillance [
12,
13]. For lamotrigine, PBQC is particularly advantageous because specimens are often collected in stable clinical rhythms and across well-defined care pathways. This consistency can be harnessed to detect analytical drift in near real time, without additional costs or workflow disruption.
Tracking patient median concentrations over defined intervals represents a pragmatic PBQC approach [
14,
15]. Medians are inherently robust to outliers and skewed distributions, making them well suited to identify small biases or shifts that might elude conventional controls. In lamotrigine TDM, monitoring patient medians across time windows and stratified cohorts (e.g., monotherapy vs. polytherapy, plasma vs. saliva) can provide early warning signals of drift, bias, or imprecision. Such surveillance strengthens confidence in clinical interpretation and supports safer, more effective dose adjustments.
In this study, we evaluate the use of patient median values as a tool for monitoring the analytical performance of lamotrigine assays in routine TDM practice.
2. Materials and Methods
2.1. Samples
Blood samples submitted for routine lamotrigine monitoring at the Departments of Clinical Chemistry and Pharmacology, Uppsala University Hospital were collected in serum tubes (BD Vacutainer Systems, Plymouth, UK). The study period spanned from 2008 through December 1, 2025, comprising 16,495 samples. Data extraction was performed in accordance with ethical approval, ensuring patient anonymity. Only sampling date, age (in years), sex, and lamotrigine concentrations were retained. Ethical clearance was granted by the Uppsala University Ethics Committee (Dnr 01-367).
2.2. Instruments
Lamotrigine measurements were initially analyzed on Beckman Coulter DxI 9000 at department of clinical pharmacology, Karolinska University Hospital, Stockholm from 2008 to 2011. In February 2011 the method was transferred to the Architect platform (Abbott Laboratories, Abbott Park, IL, USA) in Uppsala using QMS® Lamotrigine reagent no. 0373795 (Microgenics, Fremont, CA, USA), together with calibrator no. 0373787 and control no. 0374090 (Microgenics). The overall coefficient of variation (CV) was 3.6% at 7.4 µmol/L and 6.0% at 54.4 µmol/L.
In January 2021, the assay was transferred to the Cobas Pro c 503 platform, employing ARK Lamotrigine reagent no. 5023-0001-00 (ARK Diagnostics, Fremont, CA, USA) along with ARK calibrators and controls. External quality controls were provided monthly by LGC Standards (Wesel, Germany). The CV was 5.3% at 7.3 µmol/L and 4.7% at 45 µmol/L. The therapeutic reference range was 5–60 µmol/L.
2.3. Statistical calculations
Yearly median lamotrigine values were calculated. Statistical evaluations were conducted using Excel 365 (Microsoft Corp., Seattle, WA, USA) and Statistica 10 (Tibco Software, Palo Alto, CA, USA). A non parametric comparison of lamotrigine concentrations between males and females was performed using the Mann–Whitney U test. The null hypothesis (H₀) stated that the distributions did not differ by sex.In this section, where applicable, authors are required to disclose details of how generative artificial intelligence (GenAI) has been used in this paper (e.g., to generate text, data, or graphics, or to assist in study design, data collection, analysis, or interpretation). The use of GenAI for superficial text editing (e.g., grammar, spelling, punctuation, and formatting) does not need to be declared.
3. Results
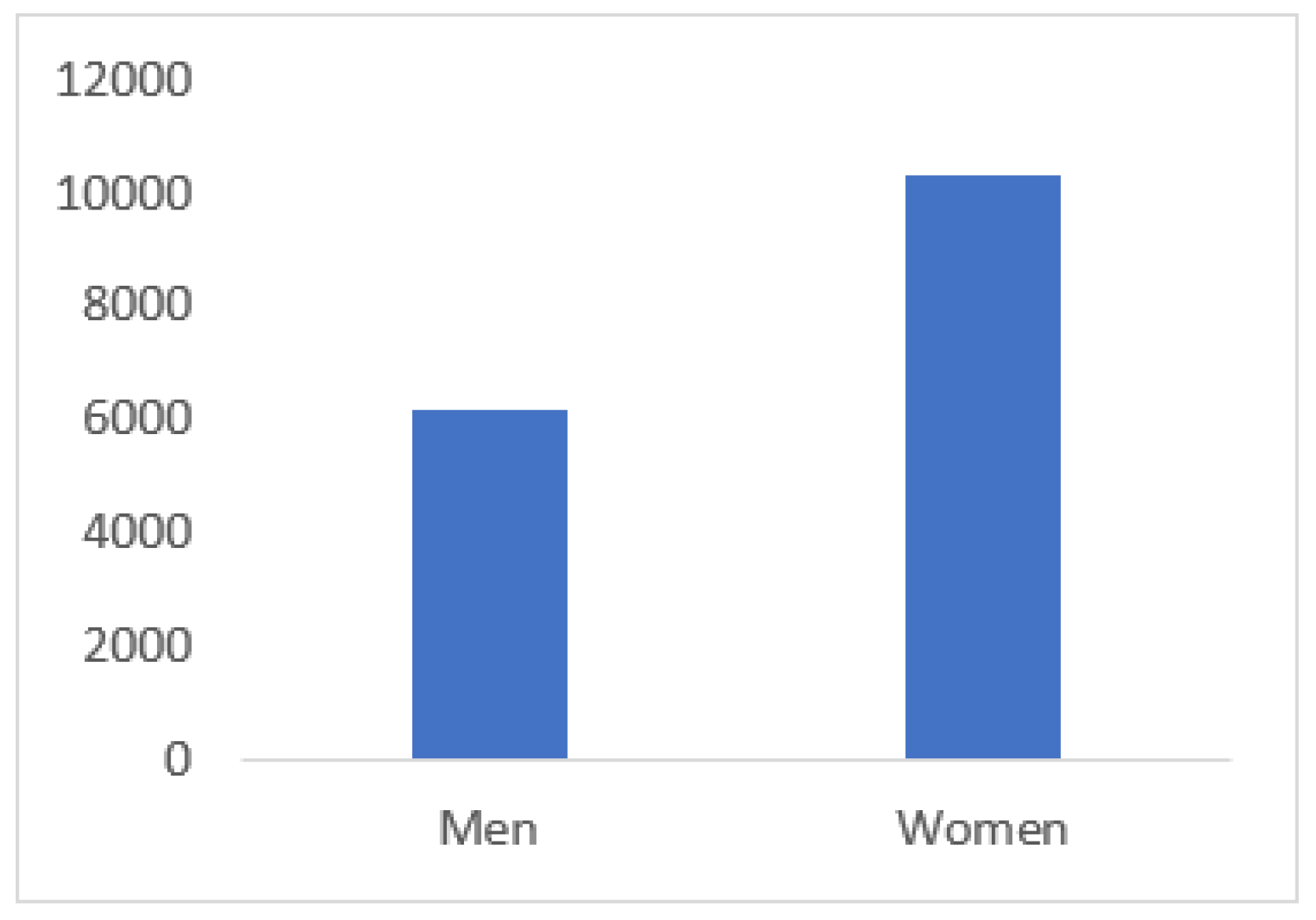
3.1. Number of lamotrigine results and sex distribution
Between 2008 and 2025 a total of 16495 lamotrigine results were reported. Of these, 6164 were from males and 10331 from females (χ² = 534.8559; p << 0.0001); (
Figure 1).
The median lamotrigine concentration was 13.71 µmol/L in females and 15.20 µmol/L in males (
Table 1). This difference was highly significant according to the Mann-Whitney (Z= 6.162; p-value 7.2 × 10⁻¹¹).
The simulated medians closely matched the reported values, supporting the use of the fitted distributions for this purpose. Under the assumptions of the log normal approximation, these results suggest that the underlying distributions differ between sexes, with males having higher values than females.
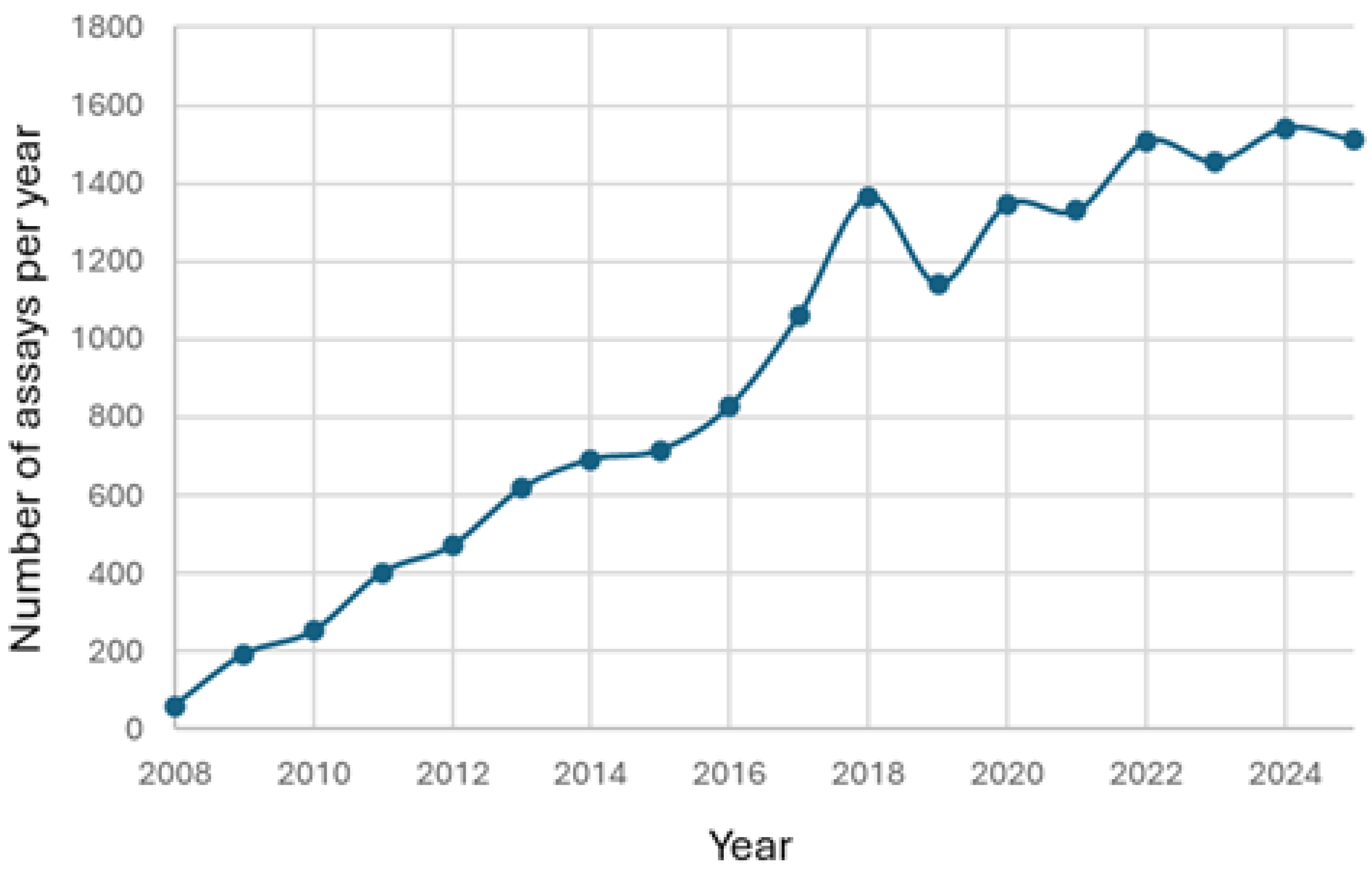
3.2. Changes in the number of reported lamotrigine results over time
The number of reported results increased from 60 in 2008 to 1543 in 2024 (
Figure 2). During the first eleven months of 2025 the number of reported results were 1510, indicating that the total for 2025 will exceed the value for 2024.The decrease observed in 2019 is most likely due to the COVID-19 pandemic.
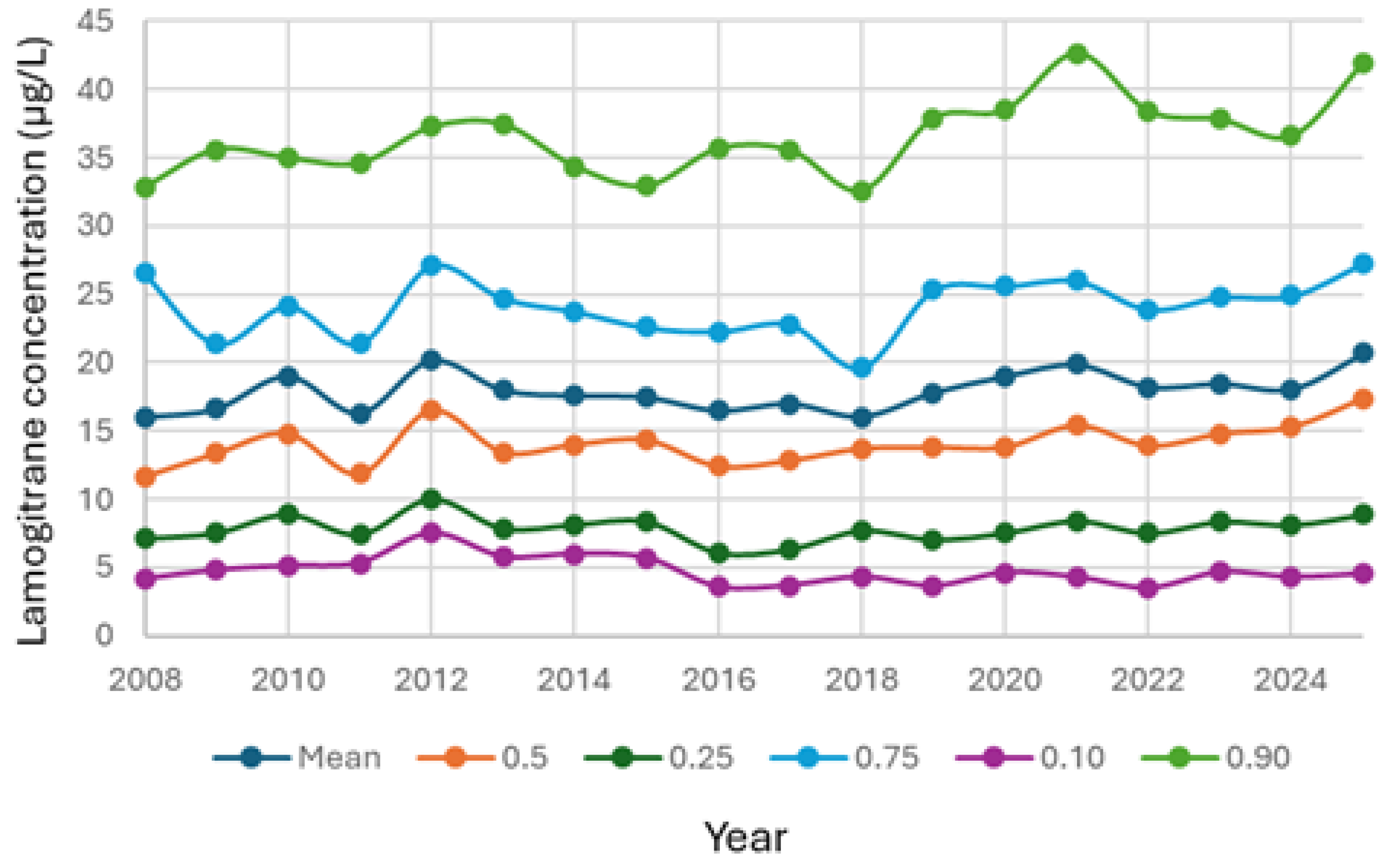
3.3. Changes in median lamotrigine concentrations over time
The median lamotrigine concentrations increased over time from 11.65 µmol/L in 2008 to 17.40 µmol/L in 20025 (
Figure 3). This trend represented a weak but highly significant change according to Spearman´s rank test (R = 0.047; p < 1 x 10-9).
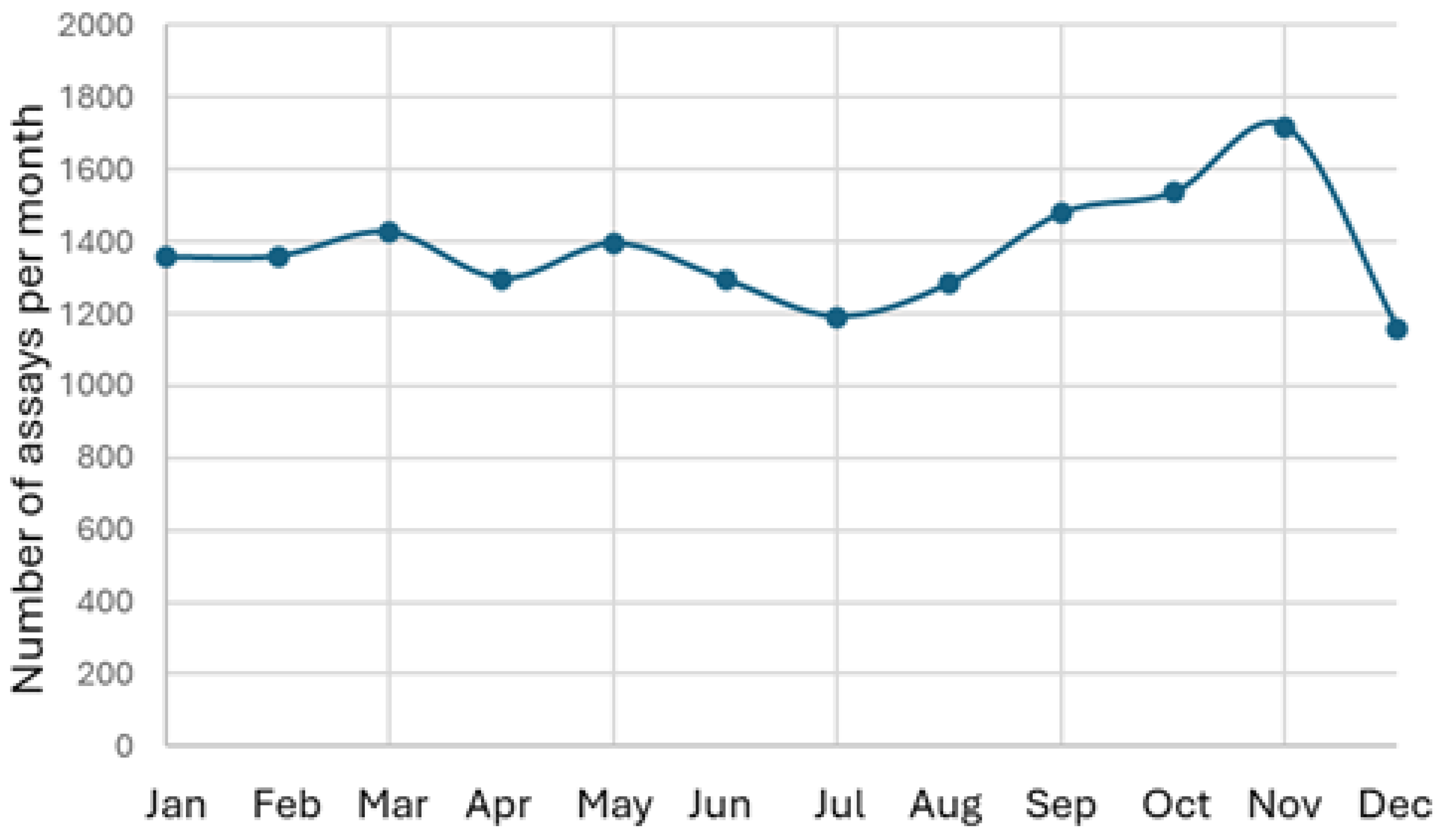
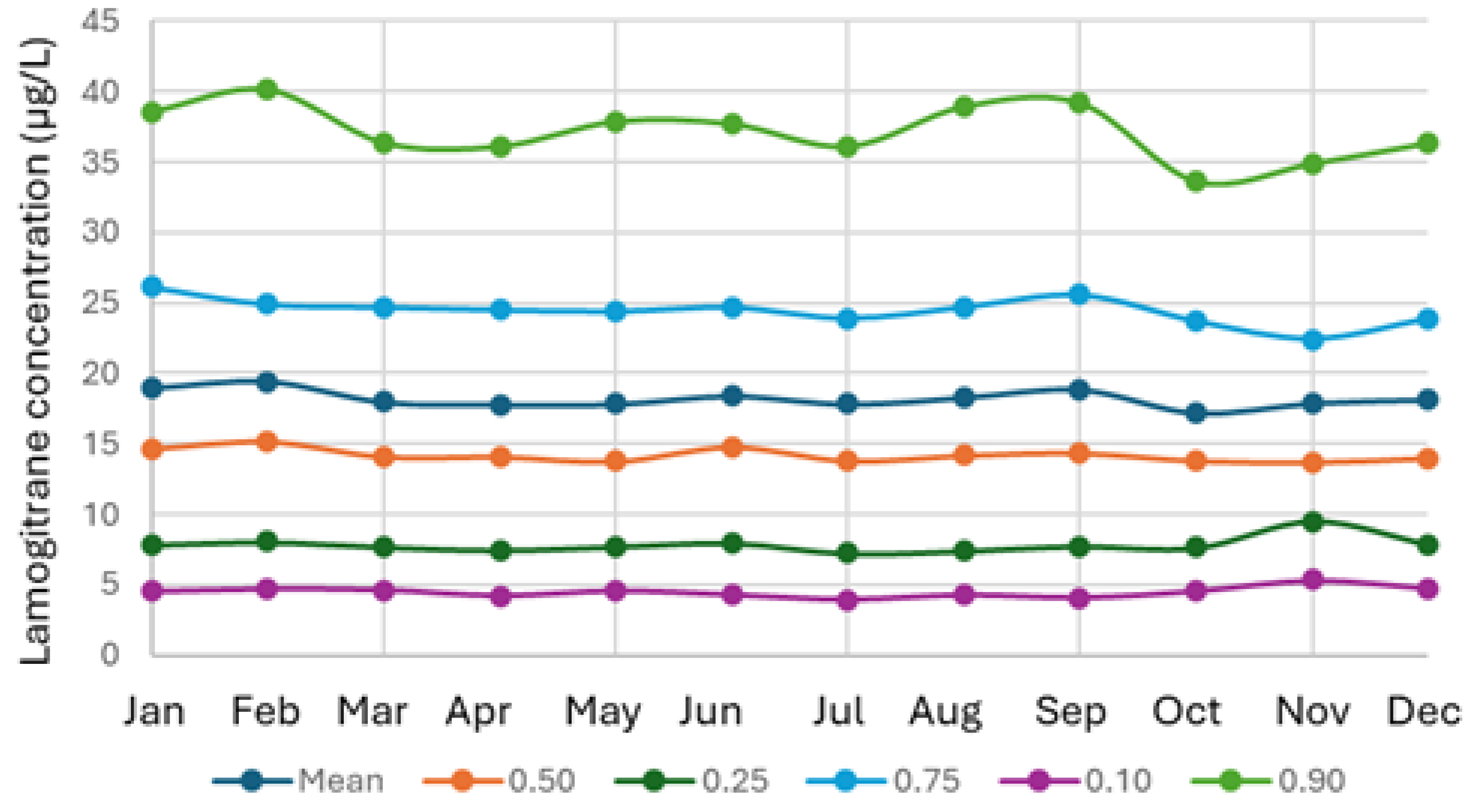
3.4. Seasonal variation in lamotrigine results
The number of reported lamotrigine results was highest in November and lowest in July and December (
Figure 4). July is the main vacation month in Sweden and December is also a holiday month. Despite these variations in the number of reported test results across months, the median lamotrigine concentrations remained stable, with a coefficient of variation for the monthly medians of 3.15% (
Figure 5).
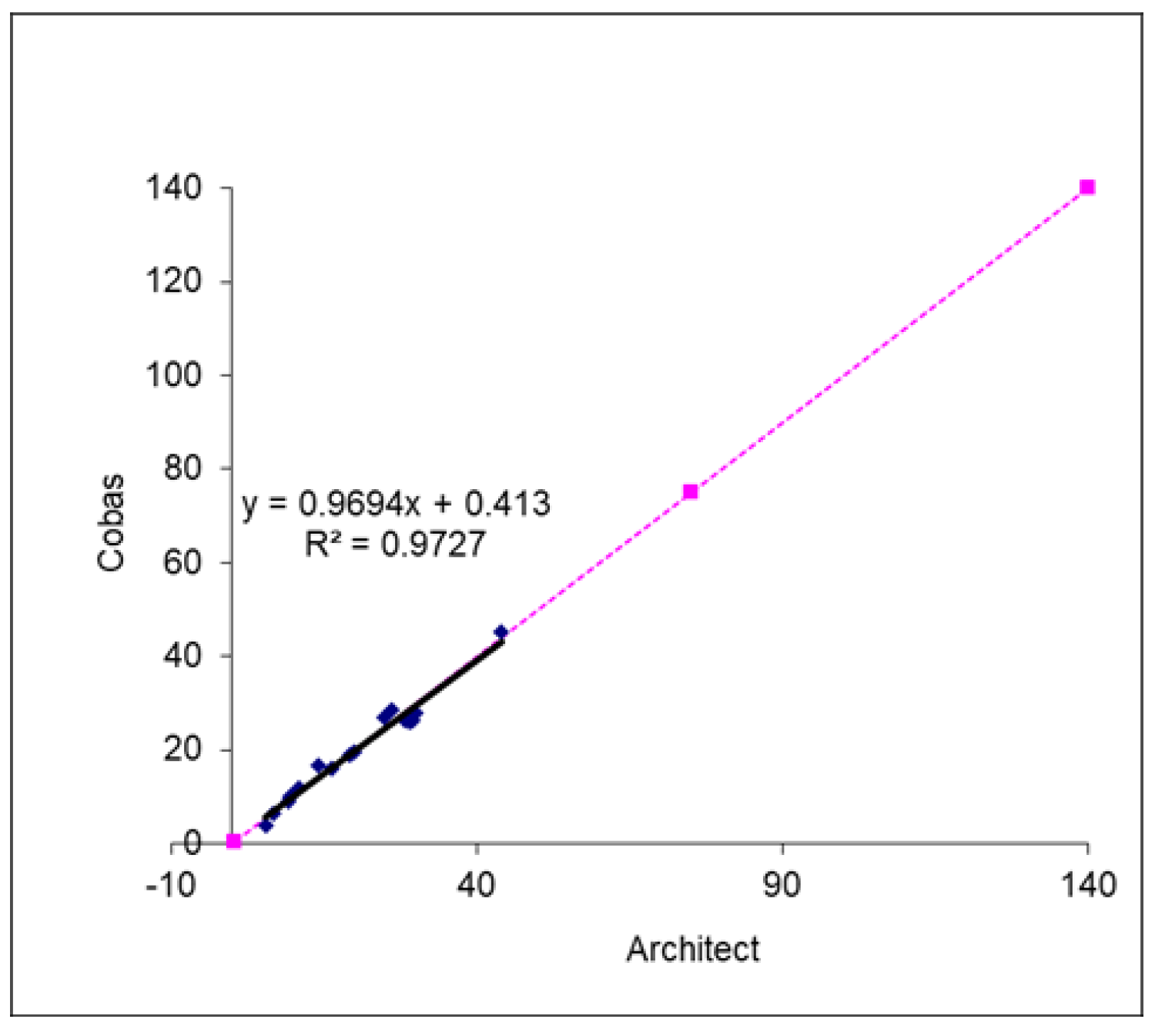
3.5. Method comparison between the Architect and Cobas lamotrigine methods
The comparison between the Architect and Cobas lamotrigine methods during the validation process of the Cobas method showed good agreement for patient samples (y=0.97x + 0.413; R2= 0.97) (
Figure 6).
4. Discussion
This large-scale retrospective study demonstrates the utility of patient median values as a pragmatic PBQC strategy for lamotrigine monitoring. Over 17 years, we observed consistent trends in assay performance, with rising median concentrations and increasing test volumes reflecting both clinical uptake and evolving therapeutic practices. The weak but statistically significant sex-related differences in median concentrations align with known pharmacokinetic variability, though the magnitude of difference is unlikely to warrant sex-specific reference ranges.
Importantly, seasonal fluctuations in sample numbers did not translate into instability in median values, underscoring the robustness of medians as a quality-control metric. This resilience highlights their suitability for continuous monitoring, even in healthcare systems with predictable variations in patient flow due to holidays or staffing cycles.
The transition from the Architect to Cobas platform in 2021 provided a natural test of PBQC applicability. The strong agreement between methods (R² = 0.97) confirms analytical continuity, while patient medians offered an independent safeguard against unnoticed drift during implementation. Such real-world validation illustrates how PBQC can complement conventional internal and external quality controls, which may miss subtle practice-level shifts.
The gradual increase in median lamotrigine concentrations over time may reflect evolving prescribing practices, broader adoption of TDM, or changes in patient demographics. While the statistical correlation was weak, the significance suggests that longitudinal monitoring of medians can reveal subtle population-level trends that warrant further clinical investigation.
Taken together, these findings support the integration of patient median tracking into routine lamotrigine TDM workflows. By leveraging data already generated in clinical practice, laboratories can enhance surveillance without additional cost or burden. This approach not only strengthens analytical reliability but also improves confidence in therapeutic decision-making, ultimately contributing to patient safety.
Median plasma lamotrigine concentrations were slightly more than 10% higher in males compared with females. This difference should be interpreted with caution, because the analysis is based on approximate distributions derived from summary statistics rather than individual-level data. However, the very small p-value from the simulated Mann–Whitney U test indicates that the null hypothesis of identical distributions between males and females can be rejected.
Lamotrigine is metabolized primarily in the liver through UDP-glucuronosyltransferase-mediated glucuronidation, predominantly via UGT1A4, while cytochrome P450 enzymes play only a minimal and clinically negligible role in its metabolism [
16,
17]. Lamotrigine pharmacokinetics display clinically important interindividual variability driven by sex, age, pregnancy, and concomitant antiepileptic and hormonal therapy, necessitating therapeutic drug monitoring (TDM). This aligns with the high number of lamotrigine analyses in this study. Sex-related differences, age and exposure to exogenous estrogens (combined oral contraceptives and hormone-replacement therapy) substantially alter lamotrigine clearance and plasma concentrations, and to outline implications for monitoring. Combined oral contraceptives and other estrogen-containing preparations increase lamotrigine glucuronidation and reduce steady-state plasma concentrations, depending on the hormonal regimen [
18]. Pregnancy and rising estradiol levels markedly increase lamotrigine clearance, often necessitating dose escalation and close TDM to avoid seizure breakthrough [
19]. Hormone-replacement therapy may produce similar reductions in lamotrigine concentrations in postmenopausal women [
20]. While routine, universally applied TDM for lamotrigine is debated [
21], targeted monitoring is supported when factors known to alter clearance are present, or when clinical response changes [
20]. Evidence supports a pragmatic, individualized TDM approach for lamotrigine — prioritizing patients on polytherapy, women initiating or changing estrogenic therapies, pregnant patients, and those with age-related pharmacokinetic changes — to optimize efficacy and safety [
6].
Future work should explore stratified PBQC approaches, such as separating monotherapy and polytherapy cohorts, or comparing plasma and saliva workflows. Such refinements could further enhance sensitivity to analytical drift and provide richer insights into clinical pharmacokinetics.
Author Contributions
Anders Larsson: Writing – review & editing, Writing – original draft, Visualization, Validation, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Mats Eriksson: Writing – review & editing. Linda Steinholtz: review & editing. Anna-Karin Hamberg: Writing – review & editing, Supervision, Methodology.
Institutional Review Board Statement
The local ethical committee at Uppsala University approved the collection of samples (01-367). The ethical permit limited the patient information to age in years and sex.
Informed Consent Statement
Patient consent was waived because the data were extracted without patient identifiers, making it impossible to obtain informed consent from the study subjects. All testing was conducted as part of routine patient care, and no additional sampling was performed specifically for this study.
Data Availability Statement
The dataset used and analyzed during the current study is available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Besag, F.M.C.; Vasey, M.J.; Sharma, A.N.; Lam, I.C.H. Efficacy and safety of lamotrigine in the treatment of bipolar disorder across the lifespan: a systematic review. Therapeutic advances in psychopharmacology 2021, 11, 20451253211045870. [CrossRef]
- Prabhavalkar, K.S.; Poovanpallil, N.B.; Bhatt, L.K. Management of bipolar depression with lamotrigine: an antiepileptic mood stabilizer. Frontiers in pharmacology 2015, 6, 242. [CrossRef]
- Zhang, L.; Yang, P.; Zhu, Y.; Liu, K.; Sun, Z. Toxic epidermal necrolysis following lamotrigine replacement therapy in a woman planning pregnancy: a case report and literature review. BMC women's health 2025, 25, 371. [CrossRef]
- De Bellis, M.; d'Orsi, G.; Rubino, E.M.; Arigliano, C.; Carella, M.; Sciruicchio, V.; Liantonio, A.; De Luca, A.; Imbrici, P. Adverse effects of antiseizure medications: a review of the impact of pharmacogenetics and drugs interactions in clinical practice. Frontiers in pharmacology 2025, 16, 1584566. [CrossRef]
- Rambeck, B.; Wolf, P. Lamotrigine clinical pharmacokinetics. Clinical pharmacokinetics 1993, 25, 433-443. [CrossRef]
- Goo, Y.; der Nederlanden, A.M.; Bleasel, A.; Alffenaar, J.W.; Kim, H.Y. Dose Monitoring of Lamotrigine Monotherapy in Pregnancy: Are Pregnant Women with Epilepsy Currently Optimally Managed? A Systematic Review. Therapeutic drug monitoring 2024, 46, 181-194. [CrossRef]
- Li, J.C.; Miao, C.F.; Lei, Y.; Liu, A.L. Physiologically Based Pharmacokinetic Modeling to Predict Lamotrigine Exposure in Special Populations to Facilitate Therapeutic Drug Monitoring and Guide Dosing Regimens. Pharmaceuticals (Basel, Switzerland) 2025, 18. [CrossRef]
- Reimers, A.; Skogvoll, E.; Sund, J.K.; Spigset, O. Lamotrigine in children and adolescents: the impact of age on its serum concentrations and on the extent of drug interactions. European journal of clinical pharmacology 2007, 63, 687-692. [CrossRef]
- Böttiger, Y.; Svensson, J.O.; Ståhle, L. Lamotrigine drug interactions in a TDM material. Therapeutic drug monitoring 1999, 21, 171-174. [CrossRef]
- Yamamoto, Y.; Usui, N.; Kagawa, Y.; Imai, K. Time-Course Changes in Lamotrigine Concentration after Addition of Valproate and the Safety and Long-Term Tolerability of Lamotrigine-Valproate Combination Therapy. Biological & pharmaceutical bulletin 2024, 47, 43-48. [CrossRef]
- Lee, Z.N.; van Nuland, M.; Bognàr, T.; Leijten, F.S.S.; van der Elst, K.C.M. Association of Lamotrigine Plasma Concentrations With Efficacy and Toxicity in Patients With Epilepsy: A Retrospective Study. Therapeutic drug monitoring 2024, 46, 642-648. [CrossRef]
- van Rossum, H.H. Technical quality assurance and quality control for medical laboratories: a review and proposal of a new concept to obtain integrated and validated QA/QC plans. Critical reviews in clinical laboratory sciences 2022, 59, 586-600. [CrossRef]
- Loh, T.P.; Cervinski, M.A.; Katayev, A.; Bietenbeck, A.; van Rossum, H.; Badrick, T. Recommendations for laboratory informatics specifications needed for the application of patient-based real time quality control. Clinica chimica acta; international journal of clinical chemistry 2019, 495, 625-629. [CrossRef]
- Larsson, A.; Hamberg, A.K.; Cedernaes, J.; Hallberg, P.; Karlqvist, J.H.; Karlsson, M. New Monitoring Recommendations for Digoxin During the Last Decade Are Associated With Decreased Serum Digoxin Concentrations in Patient Samples. Basic & clinical pharmacology & toxicology 2025, 137, e70083. [CrossRef]
- Larsson, A.; Saldeen, J.; Duell, F. Recent decline in patient serum folate test levels using Roche Diagnostics Folate III assay. Clinical chemistry and laboratory medicine 2025, 63, e275-e277. [CrossRef]
- Elwes, R.D.; Binnie, C.D. Clinical pharmacokinetics of newer antiepileptic drugs. Lamotrigine, vigabatrin, gabapentin and oxcarbazepine. Clinical pharmacokinetics 1996, 30, 403-415. [CrossRef]
- Gardner, I.; Heikkinen, A.T.; Tang, L.W.T.; Lapham, K.; Goosen, T.C. Development of a PBPK Model for Lamotrigine which Incorporates Metabolism by UGT2B10: Impact of UGT2B10 Poor Metabolizer Phenotype and Pregnancy. The AAPS journal 2025, 27, 40. [CrossRef]
- Sabers, A.; Ohman, I.; Christensen, J.; Tomson, T. Oral contraceptives reduce lamotrigine plasma levels. Neurology 2003, 61, 570-571. [CrossRef]
- Christensen, J.; Petrenaite, V.; Atterman, J.; Sidenius, P.; Ohman, I.; Tomson, T.; Sabers, A. Oral contraceptives induce lamotrigine metabolism: evidence from a double-blind, placebo-controlled trial. Epilepsia 2007, 48, 484-489. [CrossRef]
- Reimers, A. Hormone replacement therapy with estrogens may reduce lamotrigine serum concentrations: A matched case-control study. Epilepsia 2017, 58, e6-e9. [CrossRef]
- Chong, E.; Dupuis, L.L. Therapeutic drug monitoring of lamotrigine. The Annals of pharmacotherapy 2002, 36, 917-920. [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).