
Submitted:
19 December 2025
Posted:
23 December 2025
You are already at the latest version
Abstract
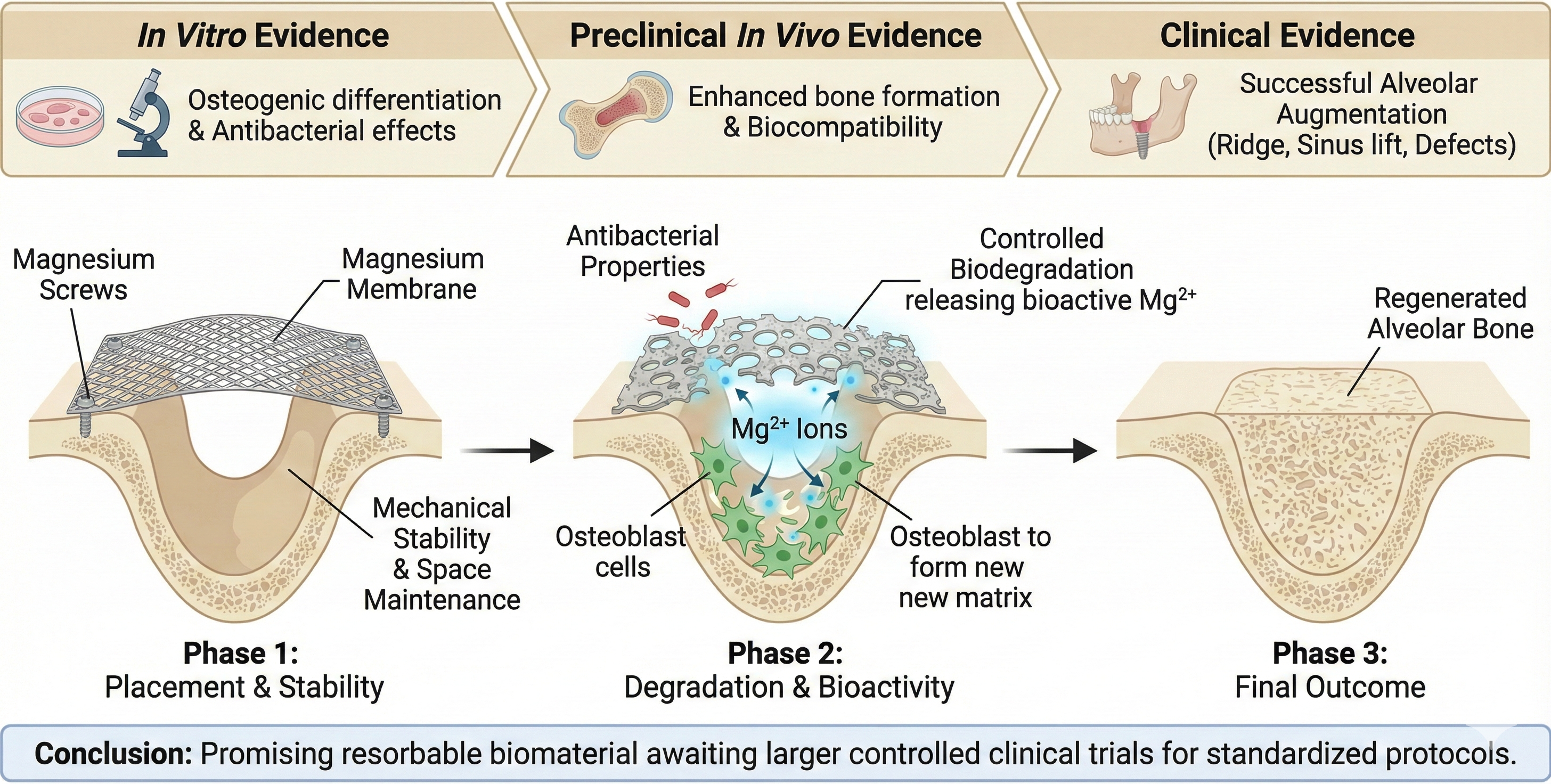
Magnesium-based membranes are promising biomaterials for guided bone regeneration due to their unique properties of mechanical strength, biocompatibility, and controlled biodegradation. This scoping review aims to map and synthesize the available clinical, preclinical, and in vitro evidence on the use of magnesium membranes and fixation screws in alveolar bone augmentation. A PubMed search was conducted in November 2025 following the Preferred Reporting Items for Systematic reviews and Me-ta-Analyses extension for Scoping Reviews guidelines. Twenty-five studies met the in-clusion criteria, including clinical case reports and series, preclinical in vivo experi-ments, in vitro studies, and narrative or systematic reviews. Across the included stud-ies, magnesium membranes demonstrated favorable handling, reliable space mainte-nance, and predictable resorption, maintaining barrier function during early healing while slowly degrading into biologically active Mg²⁺ ions. Clinically, magnesium membranes supported successful bone regeneration in horizontal and vertical ridge augmentation, immediate dentoalveolar regeneration, sinus lift procedures, cystic le-sion management, and intrabony periodontal defects. Preclinical evidence confirmed their osteogenic stimulation, biocompatible tissue response, and enhanced bone for-mation compared with conventional materials. Complications were generally minor and self-limiting; even in cases of membrane exposure, regenerated bone volume was preserved. In vitro research demonstrated their concentration-dependent enhancement of osteogenic differentiation and antibacterial effects associated with magnesium deg-radation. Overall, the current evidence supports magnesium membranes as a promising class of resorbable barrier materials offering mechanical stability, bioactivity, and fa-vorable clinical performance. However, most available studies are small case series or pre-clinical investigations, underscoring the need for larger, controlled clinical trials to establish long-term outcomes and standardized protocols. The review’s findings could help researchers advance the understanding of bone regeneration and help develop new strategies to improve bone regeneration.
Keywords:
Biomaterial
; Bone regeneration
; Magnesium screws
; NOVAMag membrane
; Regenerative dentistry
; Resorbable metal
1. Introduction
An alveolar bone defect is defined as a localized loss of the bone supporting the teeth and forming the dental arch, presenting as horizontal, vertical, or circumferential defects [1]. Bone resorption often arises from multiple causes, including the most frequent factors: tooth extraction [1,2], periodontal inflammation [3], tumors, cysts [4,5], and trauma [5]. To mitigate bone loss, reconstructive approaches, such as ridge expansion, distraction osteogenesis, sandwich osteotomy, and guided bone regeneration (GBR), are essential for modern implant and prosthetic rehabilitation [6]. GBR, the most widely documented and utilized technique, relies on key components, including a biocompatible barrier membrane to maintain space and prevent soft tissue invasion, a bone graft to facilitate new bone formation, and secure wound closure to protect the regenerative site from contamination or membrane exposure [7,8]. Ultimately, the success of this process depends on achieving tight contact between the graft and host bone, mechanical stability, and an adequate blood supply to support predictable bone augmentation [9]. The membrane used for GBR is an essential component of the treatment and is typically classified as either first-generation non-resorbable materials, such as expanded polytetrafluoroethylene (e-PTFE), or second-generation resorbable membranes, most commonly collagen [9,10]. While non-resorbable membranes provide good biocompatibility and stability, thereby maintaining good space maintenance, they require a second surgery for removal. Resorbable membranes were therefore introduced to eliminate the need for membrane retrieval and have since become widely used across many clinical applications [10]. Collagen membranes, while highly biocompatible and resorbable, exhibit limited mechanical strength and unpredictable degradation rate, which can compromise space maintenance and barrier function [11].
Given the limitations of resorbable membranes in mechanical strength and predictable degradation, magnesium has emerged as a promising alternative material [12]. Magnesium membranes maintain space and barrier function for several weeks to support bone regeneration and prevent soft-tissue collapse [13]. Additionally, magnesium metal degrades into Mg ions that promote cortical bone growth via periosteal stem cells and enhance soft-tissue adhesion [14,15]. Since the introduction of magnesium membranes, multiple clinical studies have reported their benefits and outcomes in bone augmentation procedures. Therefore, this scoping review aims to summarize the existing literature on the use of magnesium membranes and fixation screws in regenerative bone augmentation. The findings of this review could help researchers advance their knowledge in alveolar ridge regeneration and provide insight into developing new approaches to improve bone regeneration.
2. Materials and Methods
2.1. Protocol Development and Registration
This scoping review adhered to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines [16]. The protocol was prospectively registered with the Open Science Framework (OSF) public registry (Registration DOI: doi.org/10.17605/OSF.IO/CG9JK).
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
- Studies involving the use of magnesium membranes.
- Publications in English.
- Clinical studies, case reports, case series, or preclinical in vivo studies (animal models) relevant to bone regeneration.
2.2.2. Exclusion Criteria
- Studies not involving magnesium-based membranes.
- Studies focused solely on orthopedic, cardiovascular, or non-alveolar or cortical bone applications.
- Studies lacking relevant outcome measures for bone regeneration or clinical application.
2.3. Search Strategy
An electronic database (PubMed) was searched, and information was gathered in November 2025, as shown in Table 1. In order to identify articles in the topic of interest, several related terms were used: “Magnesium membrane for bone augmentation”, “NOVAMag membrane”, and “Magnesium”. Publications on the topic were gathered, duplicates were removed manually, and, subsequently, the titles and abstracts of the articles were screened independently against the predefined inclusion and exclusion criteria.
2.4. Selection Process
First, all relevant studies were retrieved from database searches, and duplicate records were eliminated. Titles and abstracts were then independently screened by two reviewers against the predefined eligibility criteria. Studies that met these initial criteria underwent full-text evaluation to confirm eligibility. Any conflicts or disagreements were resolved through discussion and agreement among all three reviewers.
2.5. Data Extraction
Relevant data were individually extracted from the selected articles by two reviewers using separate customized charts. Information such as authors' names, title, year of publication, study type, sample size, important findings, and conclusions was categorized and summarized.
2.6. Quality Assessment
The quality of evidence was assessed using the Oxford Center for Evidence-Based Medicine (CEBM) levels of evidence as follows [17]:
- Level 1: Systematic reviews, meta-analyses, randomized controlled trials.
- Level 2: Cohort studies, low-quality randomized controlled trials.
- Level 3: Case-control studies.
- Level 4: Case series, case reports, and poor-quality cohort/case-control studies.
- Level 5: Expert opinion, mechanism-based reasoning, and clinical guidelines.
2.7. Data Synthesis
Given the heterogeneity of the included studies, a qualitative narrative synthesis was used. To provide clarity and structure, the findings were grouped according to study types: preclinical animal studies, in vitro investigations, case reports, and case series.
3. Results
3.1. Study Selection
The PRISMA 2020 flow diagram illustrates the study selection process (Figure 1).
A comprehensive PubMed database search yielded 48 studies. Following the consolidation of results from two reviewers and the removal of eight duplicate records, unique articles were screened based on their titles and abstracts. Of these, 15 studies were excluded: 10 were not related to magnesium, two were non-English publications, and three focused on orthopaedic topics. Consequently, 25 studies met the inclusion criteria and were included in the full-text review.
3.2. Evidence Quality Distribution (Oxford CEBM)
The evidence was classified as Levels 1, 2, 3, 4, and 5 in 0 (0%), 0 (0%), 0 (0%), 11 (44%), and 14 (56%), studies, respectively.
3.3. Study Characteristics
The 25 studies included one systematic review, one literature review and case series, four narrative reviews, two in vitro studies, one retrospective case series, four original in vivo research, one survey, three preclinical in vivo and in vitro research articles, five clinical case reports, and four case series (Table 2). All studies were published between 2010 and 2025.
Across the included studies, magnesium membranes consistently demonstrated high mechanical strength, excellent handling properties, controlled biodegradation, and effective support of bone regeneration. Magnesium’s inherent biocompatibility and structural resilience enable the membrane to maintain its shape during early healing and gradually resorb, eliminating the need for secondary removal surgery [13,18]. Rider et al. [13] demonstrated that magnesium membranes preserve space for bone formation and exhibit exceptional tensile strength, far exceeding that of wet collagen or polymeric membranes. The membrane also proves adaptable in immediate dentoalveolar regeneration, where the magnesium shield technique yields successful bone formation and soft tissue healing without the need for re-entry surgery [19].
Magnesium membranes provide reliable stability in complex defects following extraction of impacted teeth [20] and enable predictable horizontal and vertical ridge augmentation with stable two-year outcomes [21]; additional clinical cases demonstrated stable augmented bone at one year despite minor soft-tissue recession around implants [22]. Magnesium membranes also prove effective in large cystic lesions, with long-term follow-up showing preservation of bone and soft-tissue contours [23]. In sinus lift procedures, Elad et al. [24] reported 10–20 mm vertical bone gains with complete membrane resorption and stable regenerated bone. A separate case in the posterior mandible confirmed that magnesium membranes combined with fixation screws support graft consolidation with uneventful healing and predictable bone formation [25].
Magnesium membranes can be readily shaped to fit periodontal intrabony defects, achieving radiographic bone fill and significant reductions in probing depth with uneventful healing [26]. Their use in combination with resorbable magnesium fixation screws further enhanced mechanical stability while yielding regeneration comparable to that with titanium, without requiring hardware removal [27]. Across all indications, defects arising from extractions [20,28], tooth loss [21,29], cysts [23], sinus perforations [24], or periodontal lesions [26], the combination of magnesium membranes and fixation screws consistently supports predictable space maintenance and bone formation. Beyond membranes, other magnesium-containing biomaterials also demonstrated regenerative ability, with magnesium-substituted hydroxyapatite achieving nearly 5 mm of vertical bone gain and showing complete integration into new bone [30].
Magnesium’s biological activity also contributes to regenerative outcomes. As the membrane degrades, it releases Mg²⁺ ions that promote mesenchymal and periosteal stem cell differentiation via Wnt/β-catenin and JAK1-STAT3 signaling pathways [14,31], enhancing osteogenic marker expression and matrix production. Magnesium surfaces support soft-tissue integration by improving fibroblast adhesion and forming a continuous cell layer [15]. Degradation induces localized pH changes that inhibit bacterial growth [32], reducing infection risks associated with collagen membrane exposure, as demonstrated by the successful open-healing outcomes reported by Blaskovic et al. [28]. In vitro studies further confirmed that magnesium ions enhance osteogenic differentiation of maxillary sinus membrane stem cells in a concentration-dependent manner [33], while magnesium oxide nanoparticles promoted osteoblast activity and mineralization in in vitro and in vivo models [34].
Degradation activity of magnesium membranes follows a predictable pattern: the most active corrosion occurred between Weeks 1–8, with near-complete resorption by 16 weeks, while barrier function was maintained during the critical healing phase [35]. Corrosion generated a protective mineral layer that temporarily extended structural support [13], and although hydrogen gas release formed transient cavities, they did not impair bone regeneration [35,36]. In rare cases, gas accumulation may have contributed to slight wound dehiscence [20]. Surface modifications, such as HF treatment or biomimetic coatings, can modulate corrosion and enhance cytocompatibility [36,37]. Additional preclinical work demonstrated that magnesium membranes with physical vapor deposition (PVD) coatings showed acceptable in vivo biocompatibility but induced less favorable immune modulation compared to uncoated magnesium, which more closely resembled collagen in its tissue response [38]. Micro arc oxidation (MAO) coated magnesium membranes further slowed degradation while maintaining osteogenic potential comparable to titanium barriers [39].
Overall, clinical complications of magnesium membranes were minimal, with most studies reporting uneventful healing and no graft failures [20,21,22,23,24,25,26,28,32]. The most significant soft-tissue complications were observed in the study by Tabanella et al. [40], where all four cases experienced membrane exposure; nevertheless, no infections occurred, and both vertical and horizontal bone gains were preserved, highlighting magnesium’s resilience under open-healing conditions. Minor transient sensations or partial screw visibility were reported during degradation, but they resolved spontaneously without affecting regenerative outcomes [22].
Discussion
Bone regeneration is a complex challenge, both physiologically and technically [22]. For implant placement, clinicians may opt for short implants or a staged two-step procedure. However, achieving optimal implant positioning often requires prior bone augmentation. GBR is commonly used to increase vertical and horizontal bone volume, typically employing titanium-reinforced membranes or meshes for mechanical support [7,10]. While resorbable collagen membranes are an option, they may collapse during vertical augmentation without reinforcement, thereby reducing the final bone gain, underscoring the need for strategies that provide both stability and biological support [22]. To address the limitations of conventional resorbable membranes in GBR, a novel resorbable magnesium membrane (NOVAMag® membrane, botiss biomaterials GmbH, Germany) has been developed [13].
Mechanical Strength, Handling, and Clinical Advantages
Magnesium has a long history of use in medical devices due to its favorable mechanical strength and high biocompatibility, with applications in cardiovascular, orthopedic, and general surgical procedures [18]. Its combination of structural stability and controlled degradation enables magnesium membranes to maintain their shape during early healing while gradually resorbing, thereby eliminating the need for a secondary surgery for removal [13]. These characteristics make the magnesium membrane an important innovation in oral surgery [13]. A study conducted by Rider et al. [13], demonstrated the membrane’s capacity to preserve its shape within the defect and maintain space for new bone formation, which is crucial for achieving a successful regenerative outcome. Static tensile testing confirmed the magnesium membrane’s exceptional mechanical resilience [13]. Unlike collagen or polymeric membranes, whose strength diminishes when wet, the metallic structure of magnesium preserves stability and handling during surgery. The membrane achieved a maximum tensile stress of 183 ± 10.7 megapascal (MPa), far exceeding the performance of conventional resorbable membranes [13].
Static tensile testing confirmed the magnesium membrane’s exceptional mechanical resilience. Unlike collagen or polymeric membranes, whose strength diminishes when wet, the metallic structure of magnesium preserves stability and handling during surgery. The membrane achieved a maximum tensile stress of 183 ± 10.7 MPa, far exceeding the performance of conventional resorbable membranes [13].
Performance of Magnesium Membranes and Fixation Screws in Bone Regeneration
The effectiveness of magnesium membranes and fixation screws in vertical and horizontal bone defects depends on their mechanical stability, handling, and resorbability. In a clinical case by Frosecchi [20], the extraction of impacted teeth created a complex, deep defect with horizontal and vertical components, highlighting the potential of magnesium membranes to reinforce collagen membranes in such challenging situations.
In a retrospective case series, Palkovics et al. [21] reported that magnesium membranes enabled effective horizontal and vertical ridge augmentation, with stable bone volume and no peri-implant bone loss at two years, demonstrating their ability to maintain space and support regeneration where collagen membranes may be insufficient.
In another retrospective case, a one-year follow-up after GBR with a magnesium membrane showed stable augmented bone, although some soft tissue loss around the implants was observed [22].
Chaushu et al. [23] reported that a combined approach of marsupialization, enucleation, and GBR with a magnesium membrane and bovine xenograft may be an effective strategy for treating large periapical cystic lesions. At 16 months post-augmentation, the patient remained asymptomatic, the treated teeth were stable with no mobility, and both alveolar bone and soft tissue contours were well-preserved, maintaining the architecture of the site.
Elad et al. [24] applied magnesium membranes in four cases to repair damaged Schneiderian membranes and support bone grafting using a combination of xenograft and allograft materials. Healing resulted in newly formed alveolar bone, with vertical bone gains ranging from approximately 10 mm to 15-20 mm. No residual magnesium membrane was observed at follow-up, and both vertical and horizontal bone augmentations remained stable. The regenerated bone was sufficient to support implant placement in all treated sites.
In a study by Hangyasi et al. [26], magnesium membranes were shaped into customized forms, including strips, T shapes, and M shapes, to fit the specific morphology of intrabony defects in three cases. After 4–6 months of healing, radiographic evaluation demonstrated bone regeneration and an average reduction in periodontal probing depth of 1.66 ± 0.29 mm, indicating improved bone support. Soft-tissue healing was favorable, and no major complications occurred during follow-up.
An in vivo case study demonstrated that pure magnesium membranes, combined with resorbable magnesium fixation screws, are promising materials for GBR in humans. Their favorable mechanical properties, controlled degradability, ease of handling, and positive clinical outcomes support their potential as viable alternatives to conventional barrier membranes [27].
Bone defects in the reviewed cases arose from tooth extractions [20], tooth loss [21], large cystic lesion [23], sinus membrane perforations [24], and intrabony periodontal defects [26], and the use of magnesium membranes with resorbable fixation screws demonstrated effective space maintenance, mechanical stability, and predictable bone regeneration across these diverse clinical scenarios [27].
Biological Activity and Effect of Magnesium Ion Release
Magnesium is a naturally occurring element in the human body, playing essential roles in bone metabolism and cellular function [28]. Magnesium membranes degrade to release magnesium ions, which stimulate periosteal and mesenchymal stem cells and osteoblasts to promote cortical bone growth, reinforcing the osteoinductive potential of magnesium-based materials beyond membranes alone [14,34]. This occurs via key signaling pathways, including the Wnt/β-catenin and JAK1-STAT3 pathways, enhancing osteogenic marker expression and matrix protein production [31]. In vitro evidence showed that optimal Mg²⁺ levels significantly enhance osteogenic differentiation of maxillary sinus membrane stem cells, supporting magnesium’s role in improving sinus grafting outcomes [33].
Magnesium also promotes soft tissue adhesion, as evidenced by increased attachment of human gingival fibroblast-1 (HGF-1) cells and the formation of a continuous, well-organized cell layer on magnesium membrane surfaces, suggesting improved integration with surrounding gingival tissue during the healing process [15].
Additionally, Magnesium membranes exhibit intrinsic antibacterial properties, largely due to the localized increase in pH and osmolarity that occurs during their degradation [29,32]. The antibacterial environment created during magnesium degradation suppresses bacterial colonization and biofilm formation, reducing infection risk and protecting the membrane from premature breakdown, an issue commonly observed with collagen membranes exposed to bacterial collagenase [41]. Notably, even when the magnesium membrane was left intentionally exposed, no signs of infection were observed, a finding attributed to the membrane’s intrinsic antibacterial behavior, as demonstrated by Blaskovic et al. [28].
Beyond barrier membranes, Felice et al. [30] showed that magnesium-containing biomaterials used as graft substitutes have also demonstrated notable regenerative potential. Magnesium-substituted hydroxyapatite showed nearly 5 mm of vertical bone gain and histological evidence of complete integration into newly formed bone, indicating that magnesium’s bioactivity extends beyond membrane-mediated effects to direct graft-enhanced osteogenesis.
Degradation Behavior and the Role of the Corrosion Process
The degradation of magnesium membranes used for guided bone regeneration is characterized by a gradual corrosion process in physiological environments, leading to the release of magnesium ions, the formation of a salty corrosion layer, and the formation of transient gas cavities [13]. The most significant membrane degradation occurs during the first 1–8 weeks post-implantation and continues through 16 weeks, with the membrane maintaining its barrier function during the critical early healing phase [35].
The corrosion process is crucial to the membrane’s resorbability and clinical performance. As magnesium corrodes, it forms a protective layer of magnesium salts and hydroxides, which temporarily extends the membrane’s functional lifespan and space-maintaining capability [13]. The release of hydrogen gas during corrosion can result in local gas cavities, but these are typically self-limiting and do not compromise bone regeneration or tissue health [35,36]. However, temporary gas accumulation beneath the membrane may, in some cases, exert pressure along the suture line, potentially contributing to wound dehiscence [20]. The corrosion products are gradually resorbed and replaced by new bone, with only healthy tissue remaining after complete membrane degradation [13,35].
Surface Modifications
Surface modifications, such as hydrofluoric acid treatment and biomimetic coatings, can adjust the corrosion rate, minimize gas cavity formation, and enhance cytocompatibility, enabling a controlled degradation profile that better aligns with the timing of bone healing [36,37]. Additional animal studies showed that PVD coated magnesium membranes demonstrated acceptable biocompatibility but induced a less favorable immune profile compared with uncoated magnesium, suggesting that surface chemistry significantly influences host responses [38]. MAO coated magnesium membranes further reduced early corrosion while maintaining osteogenic potential comparable to other barriers, highlighting the importance of coating technologies in achieving predictable clinical performance [39].
Clinical Complications and Healing Outcomes
Through the included studies, magnesium membranes consistently demonstrated a favorable clinical safety profile, with most cases showing uneventful healing and no signs of infection or graft failure [20,21,23,24,26,27,28,29]. Soft-tissue healing was generally stable, and the membranes provided sufficient mechanical support to maintain regenerative space during early healing, contributing to predictable bone formation across different defect types [21,23,24].
A central topic in the literature concerns soft-tissue complications, particularly membrane exposure. Among all studies, Tabanella et al. [40] documented the most significant soft-tissue issues, reporting varying severity of wound dehiscences in all four cases. These ranged from minor exposures less than 3 mm to extensive exposures that revealed up to three-quarters of the membrane. Despite the magnitude of these complications, no infections occurred, and both vertical and horizontal bone gain were confirmed at re-entry, demonstrating that magnesium membranes can maintain their regenerative role even under open-healing conditions [40]. However, localized necrosis and discomfort caused by a loose screw were noted, indicating that although magnesium membranes tolerate exposure better than collagen, soft-tissue handling remains clinically important [32,40].
In contrast, Franke et al. [22] reported only minor, self-limiting complications during membrane degradation. The patient described a brief “prickly” sensation during the first two postoperative weeks, likely related to hydrogen gas release as the membrane and screws resorbed. This effect required no intervention and resolved spontaneously. At three weeks, partial screw visibility was observed, but complete soft-tissue healing occurred by three months with a stable zone of keratinized mucosa [22]. At the one-year follow-up, bone volume remained preserved, confirming that early transient symptoms did not compromise the regenerative outcome [22].
5. Conclusions
Magnesium membranes represent a promising advancement in guided bone regeneration, combining mechanical stability, controlled biodegradation, and biologically active ion release. Clinical and preclinical evidence demonstrates reliable space maintenance, favorable handling, soft-tissue compatibility, and predictable bone formation across various defect types, including ridge augmentation, sinus elevation, cystic lesions, and periodontal defects. Complications were generally minor and did not compromise regenerative outcomes, even in cases of membrane exposure. Magnesium’s osteogenic, antibacterial, and soft-tissue–supportive properties further enhance its regenerative potential.
However, current evidence is largely limited to case reports, small series, and early laboratory studies. Larger, well-designed clinical trials with long-term follow-up are needed to establish standardized protocols and confirm the long-term efficacy and safety of magnesium membranes for oral and maxillofacial regeneration.
Supplementary Materials
Not applicable.
Author Contributions
Conceptualization, D.G. and Y.R.; methodology, I.P. and I.S.; validation, D.G., Y.R., I.S. and L.M.; formal analysis, D.G., Y.R. and I.P.; investigation, Y.R. and I.S.; resources, Y.R. and L.M.; data curation, Y.R., I.P. and I.S.; writing—original draft preparation, D.G., Y.R. and L.M.; writing—review and editing, I.P. and I.S.; visualization, Y.R. and I.P.; supervision, D.G. and L.M. All authors have read and agreed to the published version of the manuscript
Funding
This research was funded as part of the project 'Evaluation of Innovative and Standard Protocols in Endodontic and Surgical Therapy', no. SFZG-05-2025, INOENDO, co-financed from the funds of the National Recovery and Resilience Plan (NRRP).
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| GBR | Guided Bone Regeneration |
| e-PTFE | Expanded Polytetrafluoroethylene |
| HGF-1 | Human Gingival Fibroblast 1 |
| Mpa | Megapascal |
| Mg | Magnesium |
| CT | Computed Tomography |
| PVD | Physical Vapor Deposition |
| ALP | Alkaline Phosphatase |
| MAO | Micro Arc Oxidation |
| DMEM | Dulbecco’s Modified Eagle Medium |
| Runx2 | Runt Related Transcription Factor 2 |
| OCN | Osteocalcin |
| COL1 | Collagen Type 1 |
| CBCT | Cone Beam Computed Tomography |
References
- Covani, U.; Giammarinaro, E.; Marconcini, S. Alveolar socket remodeling: The tug-of-war model. Med. Hypotheses 2020, 142, 109746. [Google Scholar] [CrossRef]
- Araújo, M.G.; Dias, D.R.; Matarazzo, F. Anatomical characteristics of the alveolar process and basal bone that have an effect on socket healing. Periodontol. 2000, 2023(93), 277–288. [Google Scholar] [CrossRef] [PubMed]
- Vrotsos, J.A.; Parashis, A.O.; Theofanatos, G.D.; Smulow, J.B. Prevalence and distribution of bone defects in moderate and advanced adult periodontitis. J. Clin. Periodontol. 1999, 26, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Hollý, D.; Klein, M.; Mazreku, M.; Zamborský, R.; Polák, Š.; Danišovič, Ľ.; Csöbönyeiová, M. Stem Cells and Their Derivatives—Implications for Alveolar Bone Regeneration: A Comprehensive Review. Int. J. Mol. Sci. 2021, 22, 11746. [Google Scholar] [CrossRef] [PubMed]
- Ramanauskaite, A.; Becker, K.; Kassira, H.C.; Becker, J.; Sader, R.; Schwarz, F. The dimensions of the facial alveolar bone at tooth sites with local pathologies: a retrospective cone-beam CT analysis. Clin. Oral Investig. 2020, 24, 1551–1560. [Google Scholar] [CrossRef]
- Milinkovic, I.; Cordaro, L. Are there specific indications for the different alveolar bone augmentation procedures for implant placement? A systematic review. Int. J. Oral Maxillofac. Surg. 2014, 43, 606–625. [Google Scholar] [CrossRef]
- Benic, G.I.; Hämmerle, C.H.F. Horizontal bone augmentation by means of guided bone regeneration. Periodontol 2000 2014, 66, 13–40. [Google Scholar] [CrossRef]
- Retzepi, M.; Donos, N. Guided Bone Regeneration: biological principle and therapeutic applications. Clin. Oral Implants Res. 2010, 21, 567–576. [Google Scholar] [CrossRef]
- Stevenson, S.; Emery, S.E.; Goldberg, V.M. Factors affecting bone graft incorporation. Clin. Orthop. Relat. Res. 1996, 324, 66–74. [Google Scholar] [CrossRef]
- Kim, K.; Su, Y.; Kucine, A.J.; Cheng, K.; Zhu, D. Guided Bone Regeneration Using Barrier Membrane in Dental Applications. ACS Biomater. Sci. Eng. 2023, 9, 5457–5478. [Google Scholar] [CrossRef]
- Ma, Y.F.; Yan, X.Z. Periodontal Guided Tissue Regeneration Membranes: Limitations and Possible Solutions for the Bottleneck Analysis. Tissue Eng. Part B Rev. 2023, 29, 532–544. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Zhao, L.; Huang, C.; Yin, X.; Zhang, X.; Li, P.; Gu, X.; Fan, Y. Recent Advances in the Development of Magnesium-Based Alloy Guided Bone Regeneration (GBR) Membrane. Metals 2022, 12, 2074. [Google Scholar] [CrossRef]
- Rider, P.; Kačarević, Ž.P.; Elad, A.; Tadić, D.; Rothamel, D.; Sauer, G.; Bornert, F.; Windisch, P.; Hangyási, D.B.; Molnar, B.; Bortel, E.; Hesse, B.; Witte, F. Biodegradable magnesium barrier membrane used for guided bone regeneration in dental surgery. Bioact. Mater. 2021, 14, 152–168. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xu, J.; Ruan, Y.C.; Yu, M.K.; O'Laughlin, M.; Wise, H.; Chen, D.; Tian, L.; Shi, D.; Wang, J.; et al. Implant-derived magnesium induces local neuronal production of CGRP to improve bone-fracture healing in rats. Nat. Med. 2016, 22, 1160–1169. [Google Scholar] [CrossRef]
- Amberg, R.; Elad, A.; Rothamel, D.; Fienitz, T.; Szakacs, G.; Heilmann, S.; Witte, F. Design of a migration assay for human gingival fibroblasts on biodegradable magnesium surfaces. Acta Biomater. 2018, 79, 158–167. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Phillips, B.; Thornton, H. The 2011 Oxford CEBM Levels of Evidence (Introductory Document). Oxford Centre for Evidence-Based Medicine. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence.
- Witte, F. The history of biodegradable magnesium implants: a review. Acta Biomater. 2010, 6, 1680–1692. [Google Scholar] [CrossRef]
- Elad, A.; Rider, P.; Rogge, S.; Witte, F.; Tadić, D.; Kačarević, Ž.P.; Steigmann, L. Application of Biodegradable Magnesium Membrane Shield Technique for Immediate Dentoalveolar Bone Regeneration. Biomedicines 2023, 11, 744. [Google Scholar] [CrossRef]
- Frosecchi, M. Horizontal and Vertical Defect Management with a Novel Degradable Pure Magnesium Guided Bone Regeneration (GBR) Membrane-A Clinical Case. Medicina 2023, 59. [Google Scholar] [CrossRef]
- Palkovics, D.; Rider, P.; Rogge, S.; Kačarević, Ž.P.; Windisch, P. Possible Applications for a Biodegradable Magnesium Membrane in Alveolar Ridge Augmentation-Retrospective Case Report with Two Years of Follow-Up. Medicina 2023, 59, 1698. [Google Scholar] [CrossRef]
- Franke, T.; Korzinskas, T. Guided Bone Regeneration in the Posterior Mandible Using a Resorbable Metal Magnesium Membrane and Fixation Screws: A Case Report. Case Rep. Dent. 2024, 2024, 2659893. [Google Scholar] [CrossRef]
- Chaushu, G.; Reiser, V.; Rosenfeld, E.; Masri, D.; Chaushu, L.; Čandrlić, M.; Rider, P.; Kačarević, Ž.P. Use of a Resorbable Magnesium Membrane for Bone Regeneration After Large Radicular Cyst Removal: A Clinical Case Report. Healthcare 2025, 13, 1068. [Google Scholar] [CrossRef] [PubMed]
- Elad, A.; Pul, L.; Rider, P.; Rogge, S.; Witte, F.; Tadić, D.; Mijiritsky, E.; Kačarević, Ž.P.; Steigmann, L. Resorbable magnesium metal membrane for sinus lift procedures: a case series. BMC Oral Health 2023, 23, 1006. [Google Scholar] [CrossRef] [PubMed]
- Lv, Z.; Peng, B.; Ye, Y.; Xu, H.; Cai, X.; Liu, J.; Dai, J.; Bian, Y.; Wen, P.; Weng, X. Bolstered bone regeneration by multiscale customized magnesium scaffolds with hierarchical structures and tempered degradation. Bioact. Mater. 2025, 46, 457–475. [Google Scholar] [CrossRef] [PubMed]
- Hangyasi, D.B.; Körtvélyessy, G.; Blašković, M.; Rider, P.; Rogge, S.; Siber, S.; Kačarević, Ž.P.; Čandrlić, M. Regeneration of Intrabony Defects Using a Novel Magnesium Membrane. Medicina 2023, 59, 2018. [Google Scholar] [CrossRef]
- Rider, P.; Kačarević, Ž.P.; Elad, A.; Rothamel, D.; Sauer, G.; Bornert, F.; Windisch, P.; Hangyási, D.; Molnar, B.; Hesse, B.; et al. Biodegradation of a Magnesium Alloy Fixation Screw Used in a Guided Bone Regeneration Model in Beagle Dogs. Materials 2022, 15, 4111. [Google Scholar] [CrossRef]
- Blašković, M.; Butorac Prpić, I.; Aslan, S.; Gabrić, D.; Blašković, D.; Cvijanović Peloza, O.; Čandrlić, M.; Perić Kačarević, Ž. Magnesium Membrane Shield Technique for Alveolar Ridge Preservation: Step-by-Step Representative Case Report of Buccal Bone Wall Dehiscence with Clinical and Histological Evaluations. Biomedicines 2024, 12, 2537. [Google Scholar] [CrossRef]
- Blašković, M.; Butorac Prpić, I.; Blašković, D.; Rider, P.; Tomas, M.; Čandrlić, S.; Botond Hangyasi, D.; Čandrlić, M.; Perić Kačarević, Ž. Guided Bone Regeneration Using a Novel Magnesium Membrane: A Literature Review and a Report of Two Cases in Humans. J. Funct. Biomater. 2023, 14, 307. [Google Scholar] [CrossRef]
- Felice, P.; Lizio, G.; Marchetti, C.; Checchi, L.; Scarano, A. Magnesium-substituted hydroxyapatite grafting using the vertical inlay technique. Int. J. Periodontics Restorative Dent. 2013, 33, 355–363. [Google Scholar] [CrossRef]
- Hung, C.C.; Chaya, A.; Liu, K.; Verdelis, K.; Sfeir, C. The role of magnesium ions in bone regeneration involves the canonical Wnt signaling pathway. Acta Biomater. 2019, 98, 246–255. [Google Scholar] [CrossRef]
- Li, P.; Chen, J.; Schmidt, F.; Dai, J.; Li, J.; Xu, S.; Li, A.; Yu, Z.; Witte, F. Magnesium-based barrier membrane for guided bone regeneration: From bedside to bench and back again. Biomaterials 2025, 328, 123783. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Gong, N.; Wang, Y.; Xu, L.; Zhao, S.; Liu, Y.; Tan, F. Impact of Strontium, Magnesium, and Zinc Ions on the In Vitro Osteogenesis of Maxillary Sinus Membrane Stem Cells. Biol. Trace Elem. Res. 2025, 203, 1922–1933. [Google Scholar] [CrossRef] [PubMed]
- Malaiappan, S.; Harris, J. Osteogenic Potential of Magnesium Oxide Nanoparticles in Bone Regeneration: A Systematic Review. Cureus 2024, 16, e55502. [Google Scholar] [CrossRef] [PubMed]
- Rider, P.; Perić Kačarević, Ž.; Elad, A.; Rothamel, D.; Sauer, G.; Bornert, F.; Windisch, P.; Hangyási, D.; Molnar, B.; Hesse, B.; et al. Analysis of a Pure Magnesium Membrane Degradation Process and Its Functionality When Used in a Guided Bone Regeneration Model in Beagle Dogs. Materials 2022, 15, 3106. [Google Scholar] [CrossRef]
- Barbeck, M.; Kühnel, L.; Witte, F.; Pissarek, J.; Precht, C.; Xiong, X.; Krastev, R.; Wegner, N.; Walther, F.; Jung, O. Degradation, Bone Regeneration and Tissue Response of an Innovative Volume Stable Magnesium-Supported GBR/GTR Barrier Membrane. Int. J. Mol. Sci. 2020, 21, 3098. [Google Scholar] [CrossRef]
- Khalili, V.; Virtanen, S.; Boccaccini, A.R. Surface Treatment With Cell Culture Medium: A Biomimetic Approach to Enhance the Resistance to Biocorrosion in Mg and Mg-Based Alloys—A Review. J. Biomed. Mater. Res. Part B Appl. Biomater. 2025, 113, e35617. [Google Scholar] [CrossRef]
- Steigmann, L.; Jung, O.; Kieferle, W.; Stojanovic, S.; Proehl, A.; Görke, O.; Emmert, S.; Najman, S.; Barbeck, M.; Rothamel, D. Biocompatibility and Immune Response of a Newly Developed Volume-Stable Magnesium-Based Barrier Membrane in Combination with a PVD Coating for Guided Bone Regeneration (GBR). Biomedicines 2020, 8, 636. [Google Scholar] [CrossRef]
- Shan, X.; Xu, Y.; Kolawole, S.K.; Wen, L.; Qi, Z.; Xu, W.; Chen, J. Degradable Pure Magnesium Used as a Barrier Film for Oral Bone Regeneration. J. Funct. Biomater. 2022, 13, 298. [Google Scholar] [CrossRef]
- Tabanella, G.; Rider, P.; Rogge, S.; Čandrlić, M.; Perić Kačarević, Ž. Open Wound Healing in Guided Bone Regeneration Using a Magnesium Membrane: A Paradigm Shift. J. Biomed. Mater. Res. Part B Appl. Biomater. 2025, 113, e35642. [Google Scholar] [CrossRef]
- Duarte, A.S.; Correia, A.; Esteves, A.C. Bacterial collagenases—A review. Crit. Rev. Microbiol. 2016, 42, 106–126. [Google Scholar] [CrossRef]
Figure 1.
Preferred Reporting Items for Systematic reviews and Meta-Analyses-based flowchart illustrating the identification, screening, and selection process of the records during the search.
Figure 1.
Preferred Reporting Items for Systematic reviews and Meta-Analyses-based flowchart illustrating the identification, screening, and selection process of the records during the search.
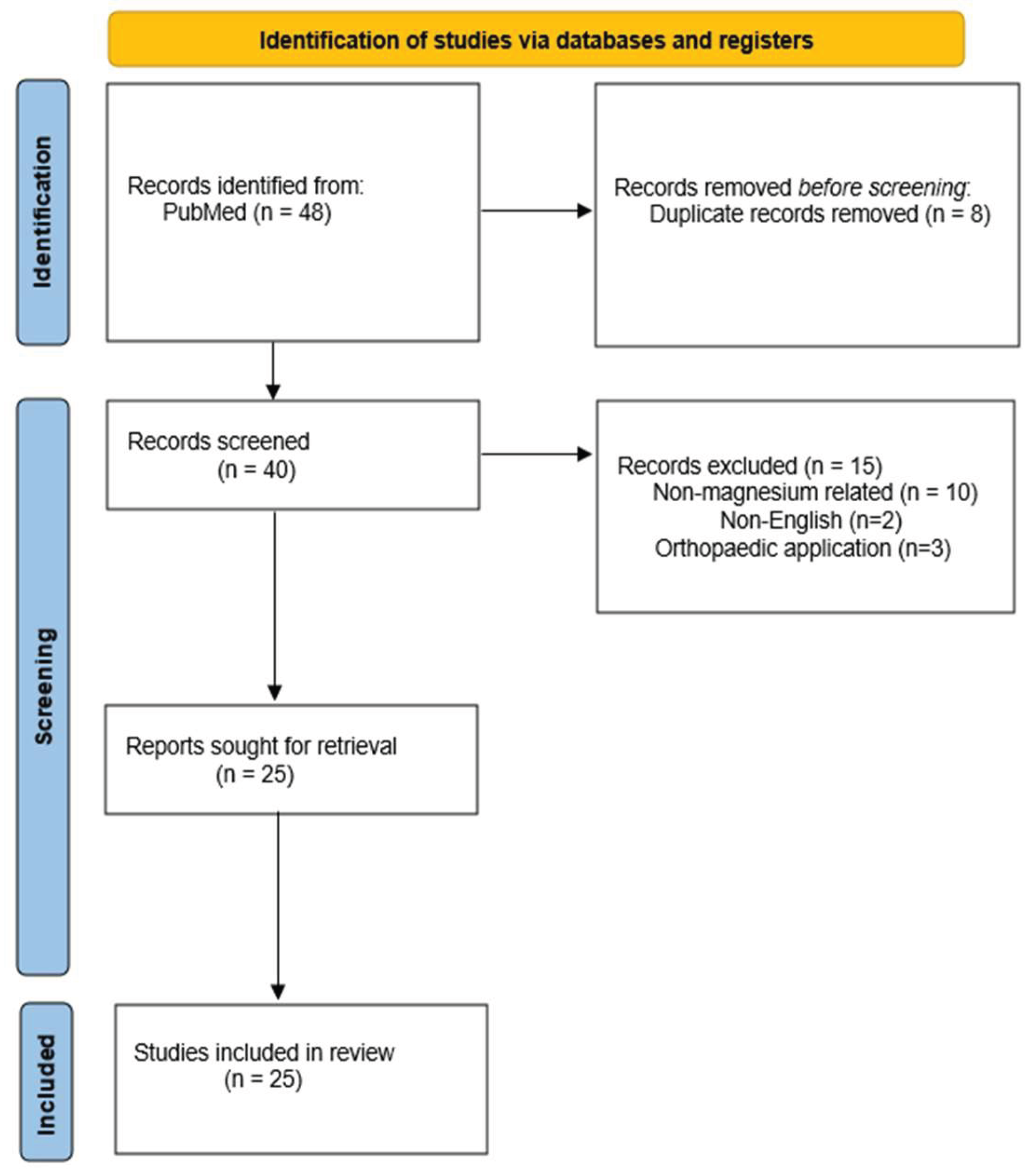

Table 1.
Electronic databases and search terms.
| Electronic database | Search term |
|---|---|
| PubMed | “Magnesium membrane for bone augmentation”, “NOVAMag membrane”, “Magnesium”. |
Table 2.
Characteristics of included studies.
| Author | Title | Type of study | CEBM level | Sample size | Key findings | Conclusion |
|---|---|---|---|---|---|---|
| Barbeck et al. (2020) [36] | Tissue Response of an Innovative Volume Stable Magnesium-Supported GBR/GTR Barrier Membrane | Original research in vivo |
5 | The study found that the magnesium-supported barrier membrane gradually degraded as intended, while simultaneously promoting bone regeneration beneath the membrane. Tissue response was favorable, with soft tissue healing occurring without excessive inflammation or adverse reactions. The membrane-maintained volume stability during the critical early healing phase, providing structural support while allowing controlled resorption, demonstrating a balance between mechanical integrity and bioresorbability. | The authors concluded that this innovative magnesium-based GBR/GTR* membrane shows significant promise for bone and tissue regeneration applications. Its combination of volume stability, controlled degradation, promotion of bone formation, and biocompatible tissue response suggests potential for future clinical translation. They emphasize that further studies, including larger animal models and eventual human trials, are needed to confirm its safety and effectiveness in clinical settings. | |
| Rider et al. (2021) [13] | Biodegradable magnesium barrier membrane used for guided bone regeneration in dental surgery |
Original research in vivo | 4 | 20 | A pure magnesium membrane effectively maintained barrier function and space during the early healing phase of guided bone regeneration, separating bone from soft tissue and retaining graft material. As it corroded, a protective corrosion layer and gas cavities extended its functional lifespan, and the membrane was gradually resorbed and replaced by new bone. Healing and tissue regeneration were comparable to resorbable collagen membranes, with no adverse tissue reactions observed. | biodegradable pure magnesium membranes possess all the necessary mechanical and biological properties for optimal GBR outcomes, demonstrating comparable efficacy and safety to conventional collagen membranes |
| Rider et al. (2022) [35] | Analysis of a Pure Magnesium Membrane Degradation Process and Its Functionality When Used in a Guided Bone Regeneration Model in Beagle Dogs |
Original research in vivo |
5 | 18 | Micro-CT** analysis showed that new bone formation under the magnesium membrane was comparable to that under collagen membranes at all time points. The magnesium membrane degraded most rapidly between weeks 1 and 8 and was nearly fully corroded by week 16. Early voids, likely from hydrogen gas release, and transient soft tissue reactions resolved over time without affecting bone regeneration, and no chronic inflammation or systemic adverse events were observed. | The authors conclude that the pure magnesium membrane is a viable, functional, and safe barrier membrane for GBR. It offers mechanical stability, degrades in a controlled manner over time, and yields bone regeneration outcomes comparable to those achieved with conventional collagen membranes, thus representing a promising alternative for GBR treatments. |
| Rider et al. (2022) [27] | Biodegradation of a Magnesium Alloy Fixation Screw Used in a Guided Bone Regeneration Model in Beagle Dogs |
Original research in vivo |
5 | 20 | Bone regeneration was similar between the magnesium and titanium groups, with no significant differences in new bone volume or soft tissue formation. The magnesium screws degraded gradually over time, with nearly complete resorption by 52 weeks. Early swelling and transient inflammation were observed in the magnesium group, and small voids from gas release occurred, but neither interfered with bone healing. By the end of the study, the regenerated bone quality and volume were comparable between groups. | Magnesium-alloy fixation screws provide sufficient stability for guided bone regeneration while gradually resorbing, eliminating the need for screw removal surgery. They represent a promising, resorbable alternative to titanium screws without compromising bone healing outcomes. |
| Amberg et al. (2018) [15] | Design of a migration assay for human gingival fibroblasts on biodegradable magnesium surfaces | In vitro study | 5 | The authors successfully established a reproducible migration assay adapted for magnesium biomaterials. They demonstrated that human gingival fibroblasts can attach to and migrate on biodegradable magnesium substrates, and that the assay allows quantitative evaluation of these behaviors. | The study concludes that the developed assay is a feasible and useful tool for systematically assessing cell–biomaterial interactions on magnesium surfaces, supporting future research and optimization of magnesium-based materials for dental and implant applications. | |
| Zhang et al. (2025) [33] | Impact of Strontium, Magnesium, and Zinc Ions on the In Vitro Osteogenesis of Maxillary Sinus Membrane Stem Cells |
in vitro study |
5 | Under osteogenic induction, moderate Mg+ concentrations enhanced sinus membrane stem cell differentiation, evidenced by increased ALP++ activity and staining, upregulated bone-related gene expression, greater osteocalcin production, and enhanced calcium nodule formation. However, higher Mg²⁺ levels reduced cell viability and osteogenic differentiation, indicating a concentration-dependent effect where excess magnesium can be detrimental. | Magnesium ions at an optimal concentration (1 mM in this study) significantly promote proliferation and osteogenic differentiation of human maxillary sinus membrane stem cells, boosting markers of bone formation (ALP, osteocalcin, mineral nodules). This suggests that Mg²⁺ has strong potential as a bioactive ion to enhance bone regeneration in sinus floor augmentation procedures | |
| Steigmann et al. (2020) [38] | Biocompatibility and Immune Response of a Newly Developed Volume-Stable Magnesium-Based Barrier Membrane in Combination with a PVD Coating for Guided Bone Regeneration (GBR) |
Preclinical in vivo and in vitro research | 5 | In vitro, both uncoated and PVD# -coated magnesium membranes showed poor cytocompatibility, with low cell viability and corrosion-related gas formation. In vivo, however, both membranes demonstrated acceptable biocompatibility, with tissue integration and healing comparable to collagen controls. The PVD coating did not reduce gas formation and was associated with fewer anti-inflammatory (M2) macrophages, suggesting a less favorable immune response, whereas the uncoated Mg membrane elicited an immune response similar to collagen, indicating satisfactory in vivo compatibility despite degradation. | The authors conclude that pure magnesium membranes (uncoated) represent a promising resorbable, volume-stable alternative to non-resorbable barrier materials for GBR/GTR therapy, as they meet biocompatibility and immune-response criteria comparable to established collagen membranes. The PVD-coated version, however, did not improve, and may even impair, tissue compatibility due to increased inflammatory response and persistent gas cavity formation, so the coating strategy in this case does not appear beneficial. | |
| Shan et al. (2022) [39] | Degradable Pure Magnesium Used as a Barrier Film for Oral Bone Regeneration |
preclinical in vivo and in vitro research |
5 | The MAO## coating slowed magnesium degradation, supported osteoblast viability and differentiation, and maintained structural stability. In rabbits, defects covered with MAO-Mg showed significantly more new bone formation than controls, comparable to titanium membranes by 8 weeks. | MAO-coated magnesium membranes are biocompatible, degrade at a controlled rate, and effectively support bone regeneration, offering a promising alternative to conventional barrier membranes without requiring removal. | |
| Lv et al. (2025) [25] | Bolstered bone regeneration by multiscale customized magnesium scaffolds with hierarchical structures and tempered degradation |
Preclinical in vivo and in vitro research | 5 | The scaffold maintained mechanical strength comparable to cancellous bone while supporting cell adhesion, proliferation, and osteogenic differentiation. In vivo, it promoted significantly more bone formation and bone mineral density than uncoated scaffolds, with controlled degradation preserving structural support during healing. | The multiscale, coated magnesium scaffold enables customizable, mechanically robust, and biologically active bone regeneration, making it a promising material for next-generation bone defect repair. | |
| Witte et al. (2010) [18] | The history of biodegradable magnesium implants: a review | Narrative review | 5 | The review outlines the historical development of magnesium-based implants, highlighting their biological and mechanical properties, as well as challenges such as corrosion, biocompatibility, and mechanical strength. It summarizes advances like alloying and surface treatments that address these issues. Evidence from in vitro and in vivo studies demonstrates benefits including biodegradability, biocompatibility, and avoidance of long-term foreign-body presence, while noting limitations that require further research. | The authors conclude that biodegradable magnesium implants hold promise as an alternative to permanent metallic implants, particularly in applications where gradual degradation and eventual replacement by natural tissue is desirable. However, they emphasize that further research, especially long-term in vivo and clinical studies, is needed to fully validate the safety, performance, and optimal design of magnesium-based implants before widespread clinical adoption. | |
| Chen et al (2022) [12] | Recent Advances in the Development of Magnesium-Based Alloy Guided Bone Regeneration (GBR) Membrane | Narrative review | 5 | The review outlines the advantages of magnesium-based membranes, including high mechanical strength, biodegradability, osteogenic stimulation, and antibacterial effects. It also identifies major limitations: rapid corrosion, hydrogen gas release, and stress-corrosion susceptibility, and describes strategies such as alloying and surface modification aimed at controlling degradation and improving performance. | The authors conclude that magnesium-based alloy membranes are promising next-generation GBR materials because they combine stability with bioactivity. However, achieving controlled and predictable degradation remains the primary challenge, requiring further materials-engineering research before widespread clinical adoption is feasible. | |
| Khalil et al. (2025) [37] | Surface Treatment With Cell Culture Medium: A Biomimetic Approach to Enhance the Resistance to Biocorrosion in Mg and Mg-Based Alloys-A Review | Narrative review | 5 | The review highlights that immersion in DMEM^ forms calcium phosphate–rich protective layers on Mg-based implants, enhancing corrosion resistance and supporting bone-like environments. Unlike synthetic buffers, which accelerate corrosion, and protein-rich media, which risk contamination, DMEM promotes hydroxyapatite crystallization and calcium phosphate deposition through electrostatic interactions and functionalized layers. Controlled fluid dynamics are important for layer stability, but long-term mechanical performance and in vivo effects such as immune responses and enzymatic activity remain unclear. | The authors conclude that DMEM-based biomimetic surface treatments represent a promising strategy to modulate the degradation behavior of Mg and Mg alloys for orthopedic applications. While these methods improve corrosion resistance and better replicate physiological conditions, further research is needed to evaluate long-term performance, mechanical stability, and behavior under realistic in vivo conditions before clinical translation. | |
| Li et al. (2025) [32] | Magnesium-based barrier membrane for guided bone regeneration: From bedside to bench and back again | Narrative review | 5 | Mg-based membranes demonstrate material properties that align with the clinical principles of GBR (PASS: primary wound closure, angiogenesis, space maintenance, stability). They provide an optimal balance between promoting bone regeneration and preventing bacterial infiltration, enhance clinical safety for less experienced surgeons, and may improve outcomes even in complications such as wound dehiscence. Their application has expanded beyond traditional GBR to broader clinical cases. | The review concludes that Mg-based barrier membranes hold substantial promise for regenerative dentistry and medicine. Continuous innovation and interdisciplinary research are essential to advance their clinical adoption, and successful translation from concept to practice highlights the potential of Mg-based materials to improve clinical outcomes and simplify dental procedures. | |
| Malaiappan et al. (2025) [34] | Osteogenic Potential of Magnesium Oxide Nanoparticles in Bone Regeneration: A Systematic Review |
Systematic review | 5 | The review of seven studies found that magnesium oxide nanoparticles enhance osteoblast proliferation, differentiation, and mineralization in vitro, increasing ALP activity and upregulating osteogenic genes such as Runx2^^, OCN×, and COL1××. In vivo, Magnesium oxide-containing scaffolds or coatings promoted new bone formation, increased bone density, and improved implant integration, demonstrating their bioactive role in stimulating bone regeneration. | The authors conclude that magnesium oxide nanoparticles have significant osteogenic potential and can enhance bone regeneration when incorporated into scaffolds, coatings, or graft materials. They highlight that while preclinical evidence is promising, further well-designed in vivo and clinical studies are needed to determine optimal dosages, long-term safety, and translational applicability. | |
| Blaskovic et al. (2023) [29] | Guided Bone Regeneration Using a Novel Magnesium Membrane: A Literature Review and a Report of Two Cases in Humans |
Literature review and clinical cases | 4 | 2 | literature shows that magnesium membranes offer favorable properties for guided bone regeneration, including mechanical strength, biocompatibility, degradability, and effective barrier function. In two human cases, the membranes were successfully shaped and fixed, graft material remained stable, and healing occurred without complications or adverse reactions. Radiographic follow-up confirmed satisfactory bone regeneration, with complete resorption of the membranes and screws. | The authors conclude that pure magnesium membranes with resorbable magnesium screws are promising biomaterials for GBR in humans. Their mechanical properties, degradability, handling ease, and successful clinical outcomes in the two cases support their use as viable alternatives to conventional membranes |
| Felice et al. (2013) [30] | Magnesium-substituted hydroxyapatite grafting using the vertical inlay technique |
Clinical case | 4 | 1 | After three months, vertical bone gain of 4.9 mm was achieved at implant placement. Histology showed that the grafted Mg-HA material was fully infiltrated by new bone, demonstrating integration into living tissue. Implants were restored with provisional and definitive prostheses at four and eight months, respectively, without complications. | The authors conclude that Mg-substituted hydroxyapatite, when used in a vertical inlay grafting procedure, can effectively support bone regeneration in severely atrophic posterior mandibles. The graft provided sufficient vertical augmentation and was integrated into newly formed bone, making it a viable grafting material in such challenging cases |
| Frossechi et al. (2023) [20] | Horizontal and Vertical Defect Management with a Novel Degradable Pure Magnesium Guided Bone Regeneration (GBR) Membrane-A Clinical Case |
Clinical case | 4 | 1 | Following extraction of an impacted canine and adjacent tooth, a complex horizontal and vertical defect was augmented with bovine bone graft, covered by a bent magnesium membrane forming a supportive “arch,” and a collagen membrane for soft tissue closure. Over eight months, the grafted volume was well maintained, healing occurred without soft tissue complications, and the magnesium membrane was fully resorbed. Two dental implants were successfully placed into the regenerated bone. | The authors conclude that the biodegradable magnesium membrane, when combined with a collagen pericardium membrane, may offer a viable, fully resorbable alternative to traditional non-resorbable titanium meshes or titanium-reinforced membranes in treating complex alveolar defects with both horizontal and vertical components. |
| Franke et al. (2024) [22] | Guided Bone Regeneration in the Posterior Mandible Using a Resorbable Metal Magnesium Membrane and Fixation Screws: A Case Report |
Clinical case | 5 | 1 | The membrane supported bone graft consolidation, and at 3 months, sufficient bone volume and quality were observed for implant placement. The membrane fully resorbed, and the augmented site healed without complications, despite minor transient soft-tissue effects. | Resorbable magnesium membranes with fixation screws can effectively support bone regeneration in large posterior mandibular defects, providing stability and eliminating the need for a second surgery, though further clinical studies are needed. |
| Blaskovic et al. (2024) [28] | Magnesium Membrane Shield Technique for Alveolar Ridge Preservation: Step-by-Step Representative Case Report of Buccal Bone Wall Dehiscence with Clinical and Histological Evaluations | Clinical case | 4 | 1 | After six months, sufficient bone volume allowed implant placement. Histology showed ~47% new bone, ~19% residual graft, and no inflammation, with active remodeling at the bone-biomaterial interface. Soft tissue healed well, and the final restoration achieved good esthetic and functional outcomes. | The magnesium membrane shield technique effectively supports alveolar ridge preservation in severe buccal defects, promoting bone regeneration and maturation without requiring membrane removal. |
| Chaushu et al. (2025) [23] | Use of a Resorbable Magnesium Membrane for Bone Regeneration After Large Radicular Cyst Removal: A Clinical Case Report |
Clinical case | 4 | 1 | At 16 months post-treatment, CBCT† imaging showed significant bone regeneration: the palatal bone wall contour was restored and well-corticated, indicating new cortical bone formation. Clinically, the treated teeth remained asymptomatic, with normal mobility and healthy soft-tissue healing. The magnesium membrane provided structural support bridging the bony discontinuity, supported graft stability, and being resorbable, eliminated the need for membrane removal surgery | The authors conclude that using a resorbable magnesium membrane in GBR after large cyst removal can be a promising strategy for restoring bone in large periapical defects, combining mechanical strength with complete resorption, though larger studies are needed to verify long-term outcomes and generalizability. |
| Palkovics et al. (2023) [21] | Possible Applications for a Biodegradable Magnesium Membrane in Alveolar Ridge Augmentation–Retrospective Case Report with Two Years of Follow-Up |
Retrospective case report | 4 | 2 | In Case #1, alveolar ridge augmentation with the magnesium membrane achieved a volumetric bone gain of 0.12 cm³, while Case #2 showed a gain of 0.36 cm³, with both horizontal and vertical improvements. At two-year follow-up, hard tissue volume remained stable with no peri-implant bone loss. The membrane’s rigidity supported space maintenance and bone regeneration in defects that would be challenging for conventional resorbable collagen membranes. | The authors conclude that the use of a rigid, resorbable magnesium membrane for alveolar ridge augmentation appears promising: in these two cases, successful bone gain and stable long-term hard tissue outcomes were achieved without the need for membrane removal |
| Elad et al. (2023) [19] | Application of Biodegradable Magnesium Membrane Shield Technique for Immediate Dentoalveolar Bone Regeneration |
Case series | 4 | 4 | All cases demonstrated successful bone regeneration and soft-tissue healing, with follow-up imaging showing thick cortical bone formation in some sites. The membrane was adaptable to defect shape and could be applied as a single or double layer for mechanical support. Its biodegradable nature eliminated the need for secondary removal surgery. | The magnesium membrane shield technique proved to be a viable method for immediate dentoalveolar bone regeneration |
| Elad et al. (2023) [24] | Resorbable magnesium metal membrane for sinus lift procedures: a case series |
Case series | 4 | 4 | In all four cases, the magnesium membrane was used to repair or replace the sinus membrane and support bone grafts in the sinus cavity. Healing resulted in newly formed alveolar bone with height gains of 10-20 mm, and the magnesium membrane was fully resorbed. Vertical and horizontal bone augmentation remained stable, providing sufficient regenerated bone to support dental implants. | The authors conclude that, within the limits of this small case series, a resorbable magnesium membrane can be a viable material for sinus-lift procedures and repair of Schneiderian membrane perforations. The results show successful healing, effective new bone formation, and reliable separation between the oral cavity and maxillary sinus, suggesting that magnesium membranes may offer a promising alternative to conventional resorbable membranes or non-resorbable materials for sinus augmentation |
| Hangyasi et al. (2023) [26] | Regeneration of Intrabony Defects Using a Novel Magnesium Membrane |
Case series | 4 | 3 | In all three cases, the magnesium membrane could be easily shaped into customized forms (strip, T-shape, M-shape) to adapt to the specific morphology of each intrabony defect. After 4-6 months of healing, radiological analysis demonstrated bone regeneration and periodontal probing depth (PPD) reduction by an average of 1.66 ± 0.29 mm, indicating a gain in bone support. Soft-tissue healing was favorable, and no major complications were reported during the healing period. | The authors conclude that the use of a resorbable magnesium membrane represents a viable and promising approach for the treatment of intrabony periodontal defects, offering the benefits of mechanical stability, ease of shaping, effective bone regeneration, and satisfactory functional and esthetic outcomes |
| Tabanella et al. (2025) [40] |
Open Wound Healing in Guided Bone Regeneration Using a Magnesium Membrane: A Paradigm Shift |
Case series | 4 | 4 | Despite membrane exposure in all cases, from small to large, none of the patients experienced pain, infection, or other clinical complications. Implant placement was carried out as planned, and importantly, there was no significant bone loss observed despite exposure. The resorbable magnesium membrane maintained its barrier function and preserved the augmented bone volume, even under open-wound healing conditions. | The authors propose that using a magnesium membrane for GBR may allow for a “paradigm shift” in how wound exposures and dehiscences are managed, membrane exposure does not necessarily lead to failure or bone loss. They suggest the magnesium membrane’s resilience and resorbable nature can make open-wound healing a viable outcome rather than a complication, though they note that larger studies are needed to confirm these findings. |
*GBR/GTR- Guided Bone Regeneration/ Guided Tissue Regeneration **CT- Computed Tomography; +Mg- Magnesium; ++ALP- Alkaline Phosphatase; #PVD- Physical Vapor Deposition ##MAO- Micro Arc Oxidation; ^DMEM- Dulbecco’s Modified Eagle Medium ^^Runx2- Runt Related Transcription Factor 2; ×OCN- Osteocalcin ××COL1- Collagen Type 1; †CBCT- Cone Beam Computed Tomography.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



