
Submitted:
19 December 2025
Posted:
22 December 2025
You are already at the latest version
Abstract
Technologies for home movement rehabilitation after stroke are rapidly expanding. However, for consumers, the number and nature of available products are unclear, and the information provided by device manufacturers varies widely. To understand this landscape, we used the U.S. Food and Drug Administration (FDA) database to identify devices for stroke rehabilitation suitable for home use. We then surveyed 13 individuals with stroke to determine what information they most wanted about home-based reha-bilitation devices and contacted manufacturers to obtain those details. Thirteen FDA codes were associated with stroke rehabilitation devices, encompassing 58 devices produced by 41 companies. Nearly half were categorized under two codes: QKC (in-teractive rehabilitation exercise devices) and GZI (neuromuscular stimulators). Among devices for which information was available, 71% received FDA clearance after 2015, and 23% cost under $1,000. The top information priorities for individuals with stroke were required usage to achieve therapeutic benefit, expected benefit, ease of use, and motivational features. Despite repeated outreach, only 44% of companies responded to our queries; among those that did, details were vague and variable. These results con-firm that a large and growing number of FDA-approved devices are now available for home-based post-stroke motor rehabilitation. We further identify a need to establish industry standards for reporting ease of use, motivational effectiveness, and dose–response characteristics to help the intended consumers select appropriate technolo-gies. We include the dataset for future reference.
Keywords:
stroke
; home-based rehabilitation
; neurorehabilitation technology dataset
; FDA-cleared rehabilitation devices
; user-centered decision support
1. Introduction
Stroke is a leading cause of major disability in the U.S. [1], with more than 600,000 people surviving a stroke each year, and over 7,000,000 individuals alive today who have experienced at least one stroke, over 2% of the U.S. population [2,3,4]. Approximately 50% of chronic stroke survivors have hemiparesis, ~30% are unable to walk unassisted and ~30% have severe to moderate dependency in activities of daily living (Barthel Score < 60) [5]. Thus, persistent movement-related disability following stroke is a significant health care problem in the U.S.
Individuals typically receive hands-on therapy for several months after stroke to treat motor impairment and improve independence. Based on systematic reviews of dozens of trials, an intensity-effect relationship has been implicated between the amount of therapy individuals receive and the movement gains achieved [6,7,8,9,10,11]. However, one recent attempt to more precisely define this intensity-effect relationship for upper extremity therapy failed [12]. This failure may be due to the relatively small range of intensities tested (a range of 3200-9600 practice movements), highlighting the need to develop approaches for delivering motor training at higher dosage. As a point of reference, consider what is required in another motor learning context–learning to walk: toddlers take over 5 million steps in a year of learning to walk [13]. Recent studies that delivered higher doses of movement practice have found greater improvements in movement ability [14,15,16,17].
To become routinely incorporated into rehabilitation practice, such high dose movement training will likely need to be semi-automated with technology. The amount of therapy a patient receives involving direct contact with rehabilitation therapists is often limited by cost considerations [18]. For example, the average length of stay for stroke survivors in inpatient rehabilitation facilities in the U.S. decreased approximately 54% (31.3 days to 14.5 days) after prospective payment system reimbursement was instituted in 1983 [19]. Even with a therapist, rehabilitation exercise is often not very intense [20]. Insurance companies will pay for a small and inconsistent number of therapy sessions [21]. Patients may exercise apart from a therapist; however, independent movement practice is particularly difficult for individuals who have movement impairment, which likely contributes to the reported poor compliance with home exercise programs [22,23,24,25]. Therefore, it is essential to develop motivating technologies for delivering effective forms of therapy at a manageable cost, so that individuals can exercise for longer periods and maximize recovery.
Rehabilitation devices that can be used semi-autonomously offer the potential for increased accessibility, more intensive practice, and greater independence during recovery. Recognizing this need, there has been a surge in the number of research groups and companies that are developing robotic, sensor, stimulation and vision based devices for assisting in the movement rehabilitation of persons with disabilities, for the arms, hands, and legs (see reviews [26,27,28,29,30,31,32,33,34,35,36]). Most of this work has focused on the rehabilitation of movement after stroke because survivors of stroke are the largest target population, although there is also work on robotic movement training after spinal cord injury, cerebral palsy, and multiple sclerosis. Developers often state three main goals for this activity: automating the repetitive and/or strenuous aspects of therapy, delivering therapy in a more standardized manner, and quantifying outcomes with greater precision.
Despite the growing availability of such devices, stroke survivors and clinicians face challenges in selecting appropriate products. A few online directories exist, including the NeuroRehab Directory (a curated list of neurorehabilitation products), MedicalExpo’s rehabilitation systems section (a commercial listing of rehabilitation devices), and the Exoskeleton Report catalog (a registry of wearable exoskeletons). However, these resources are limited to specific device categories, do not systematically report clinical evidence, and/or are not updated in a way that ensures comprehensive coverage. As a result, potential users become aware of devices through internet searches, social networks, advertisements, word-of-mouth, and vendor displays at conferences. Further, the information available online about each device varies, and it is unclear whether this information matches well with the questions stroke survivors have about the devices. Even when trained rehabilitation therapists select devices, the devices they purchase often see limited uptake into regular clinical practice [37,38].
The goal of this work was to help address these gaps by developing a curated dataset of FDA-approved rehabilitation devices suitable for home use after stroke. This study presents 1) an analysis of the characteristics of the devices; 2) results from a survey of individuals post-stroke about the types of information they most want to know about the devices; and 3) insights gained from manufacturer responses to user-centered inquiries. Our findings aim to inform people post-stroke, caregivers, and therapists seeking effective home rehabilitation options. In addition, we seek to highlight areas where developers could improve information transparency and device design. Portions of this work were presented previously in conference paper format [39].
2. Materials and Methods
2.1. Device Identification and Dataset Development
We conducted a structured search to identify FDA-approved rehabilitation devices suitable for home use by individuals recovering from stroke. Our goal was to create a dataset of engineered devices that support independent or minimally supervised motor recovery in non-clinical environments. To identify candidate devices, we used the FDA’s Product Code Classification database to determine relevant product codes. We then searched the Establishment Registration & Device Listing and the 510(k) Premarket Notification databases using those product codes. Devices were included if their descriptions indicated that they supported stroke rehabilitation and the manufacturer explicitly marketed them as appropriate for use in the home.
In addition to the FDA databases, we consulted three publicly available online catalogs of rehabilitation technologies to supplement device identification and verify product information. First, the NeuroRehab Directory, which is a curated list of neurorehabilitation products that is searchable by impairment (for example, ankle/foot tightness, arm/hand weakness, balance, cognition), product category, price range, and body region. Second, the rehabilitation systems section of the MedicalExpo marketplace for medical equipment, which includes production-ready robotic rehabilitation systems, often with videos and marketing brochures. Third, the Exoskeleton Report catalog, which provides a registry of wearable exoskeletons spanning medical, industrial, military, research, and consumer applications. For all three resources, we treated entries as supplementary rather than primary inclusion sources. Devices were only added to the dataset if they could be linked to an FDA product code and met our home-use criteria. These directories frequently lacked systematic reporting of regulatory status, clinical evidence, pricing, or usability information, and are updated manually, which can lead to outdated or missing entries. As a result, we used them primarily to validate device names and manufacturers and to identify potential additional candidates for FDA code searches.
For each device, we examined manufacturer websites, online marketplaces, and available literature to extract information about device function, regulatory status, pricing, clinical validation, usability, and targeted body parts. As described in the next section, we also created fields based on information that post-stroke individuals want to know about devices. Table 1 lists the fields we chose for the dataset.
2.2. Survey of Informational Needs of Individuals Post-Stroke
We designed a survey to gain insight into the types of information that stroke survivors want to know about the devices. To do this, we first conducted structured interviews of nine individuals in the chronic phase of stroke who were participating in ongoing clinical trials of rehabilitation technologies at our institution. We generated survey items by analyzing the interviews. We then administered the survey to a cohort of thirteen individuals who had a stroke. The UC Irvine Institutional Review Board approved the study and participants provided informed consent.
For the interview stage, a single researcher conducted all interviews, which explored participants’ recovery experiences, barriers to rehabilitation, and use of devices or apps. As described more fully in [39], we performed inductive thematic and summative content analyses on the survey transcripts, with two independent researchers coding the data and reaching consensus on possible types of informational needs that the interviewees had regarding new technologies.
From this analysis we developed a survey that asked individuals to rank the types of information they most desired when searching for new rehabilitation therapy technologies. The introduction to the survey told participants that our team was developing a website to help people find devices that might be helpful to them, and that we were interested in getting their opinions on the information the website should provide, and about how it should help them search for devices. They were told that the website would provide a basic description of each device (including how it works, what it is for, a picture, and the price), but that there are other types of information it could potentially provide. We asked them to identify their priorities for the types of information they would like the website to show from the list generated from the previous interviews, choosing first their top three highest priorities, then three medium and low priorities, followed by ranking their three highest priorities. The list of priorities they scored is presented in Table 3, Part 1.
After that, the second half of the survey told them that we wanted to get their input on how the website should convey information and asked them to rate several items from 1 to 10, with 1 being “not important” and 10 being “very important”. The list of items is presented in Table 3, Part 2.
Finally, the survey asked participants to rate how concerned they would be about privacy for a device website on a scale from 1 (not concerned) to 10 (very concerned). We also included an open-ended question in which they could describe their specific privacy concerns. The complete survey is available in the Supplementary Materials.
2.3. Manufacturer Outreach
To supplement the limited information available online, we contacted the manufacturers of the identified devices directly. We emailed all the companies that manufacture the devices included in the dataset. The outreach email was written from the perspective of a researcher working closely with stroke survivors who frequently request guidance on rehabilitation devices (find the full email in the Supplementary Materials). The intent was to obtain practical, user-centered information to enable informed recommendations tailored to stroke survivors’ needs. The email requested details on four main topics:
- Pricing and Return Policy: Including device prices and whether a return policy is offered if the device does not meet user expectations or needs.
- Ease of Use: Information about how easy the device is to operate, whether it requires therapist supervision or can be used independently, any associated discomfort or pain, and the proportion of customers who use the device at home.
- Usage Requirements: Recommendations on the frequency and duration of use needed to achieve benefits, along with any scientific studies supporting the device’s effectiveness.
- Motivational Features: Descriptions of any features designed to keep users engaged, such as progress tracking, social networking, gamification, goal setting, or feedback.
The email asked companies to provide separate information for each product when multiple devices were offered. Responses were analyzed for response rate and time, responder roles, and completeness of information provided.
As described in the Results, not all companies responded, so we conducted a follow-up outreach ~10 months after the initial email targeting only those that did not reply to the original email. This time, the email provided a link to a short Google Forms survey designed to capture the same key user-centered information initially requested: pricing and return policy, ease of use, recommended usage patterns, and motivational features (see Supplementary Materials). The follow-up email emphasized the benefits of participation, including increased visibility of the company’s devices among the stroke recovery community. Companies with multiple devices were asked to submit a separate survey for each product to ensure accurate and specific representation. Responses to this follow-up survey were collected and analyzed alongside the original email responses, thereby supplementing the dataset and enabling us to assess both the completeness of manufacturer-provided information and companies’ overall responsiveness to user-centered inquiries.
3. Results
3.1. Characteristics of FDA-Approved Devices for Home Use after Stroke
We identified 13 relevant FDA product codes (Table 4). The most frequently occurring codes were QKC (Interactive Rehabilitation Exercise Devices, Prescription Use; 26%), GZI (Stimulator, Neuromuscular; 22%), IPF (Stimulator, Muscle, Powered; 19%), and BXB (Exerciser, Powered; 10%), highlighting a strong focus on interactive exercise and neuromuscular stimulation technologies (Table 4). From these, using the FDA database, we identified 58 unique rehabilitation devices manufactured by 41 companies that met our inclusion criteria for suitability for home use by individuals recovering from stroke. Of these 58 devices, 48% were listed in the NeuroRehab Directory, 41% appeared in MedicalExpo, and 10% were included in the Exoskeleton Report catalog. Among the 48 devices for which approval dates were available or for which we found this information outside the FDA database, 71% were approved after 2015 (Figure 2a). Note that approval dates were challenging to find for devices that were exempt from the 510(k) premarket notification, since the FDA database does not list approval dates for these devices.
Device prices ranged from $60 to $130,000 (Figure 2b). Among the 35 devices for which we obtained cost information, 8 had a yearly price under $1,000 (23%), and 11 used a subscription-based pricing model (31%). With respect to body targets, 60% of devices were applicable to the hand, 50% to the ankle, 45% to the arm, 38% to the leg, and 25% to the torso. In terms of versatility, 47% of the devices were applicable to more than one joint or limb. Finally, 29% were wearables (actuated and sensorized), 21% were non-wearable training systems (robots and exercisers), 28% were stimulation-based (stimulators and FES bikes), and 22% were motion-sensing software systems (motion capture and VR/AR devices) (Figure 3).
3.2. Survey to Identify Information Priorities of Stroke Survivors
To determine which types of information about home rehabilitation technologies matter most to potential users, beyond a basic description and price, we surveyed 13 individuals with motor impairments following a stroke about their informational priorities and preferences for how a device-selection website should present this information. The results are shown in Figure 4. Participants prioritized information regarding how difficult it is to obtain benefits from these devices (including required frequency of use, ease of use, and motivational features) and how large a benefit they can expect (Figure 4a). With respect to the website design, they prioritized a smartphone-friendly chatbot that guided users through the selection process based on their personal profile, also allowing them to compare devices (Figure 4b). The lowest-rated feature was connecting to a salesperson.
With respect to the privacy question included in the survey, participants reported, on average, relatively low privacy concern for this type of website (mean 3.69 ± 3.38 on a 1 to 10 scale, where higher scores indicate greater concern). Participants’ open-ended explanations for their privacy ratings reflected several recurring themes. 33% of respondents explicitly emphasized control over personal information or identity (for example, not wanting their name or medical history shared or used for judgment), and 22% specifically referenced the need for security and Health Insurance Portability and Accountability Act (HIPAA) protections. At the same time, 33% of participants indicated that they were willing to share information if it helped others or improved access to rehabilitation technologies, and 22% stated that privacy was not a major concern for them or was not relevant in this context.
3.3. Manufacturer Responses
Findings from the first half of the survey about informational needs, as reported in the previous section, were used to structure the questions in our outreach to manufacturers, ensuring we requested information on the topics most relevant to stroke survivors. We sent email inquiries to the 41 companies that manufacture the 58 devices in the dataset we created. Of these, only 13 companies (32%) responded. Nine responded within two days, and four more replied within eight days. No additional replies were received thereafter until we sent a second email 10 months later, which sought to make responding easier using an online survey. 5 companies responded to the follow-up email: three of them responded within the first 2 days, and the other two in the following 25 days, bringing the percentage of responding companies to 44%.
Among the 13 original respondents, 10 companies (77%) answered our questions directly by email, and three (23%) recommended follow-up phone conversations. We were able to schedule meetings with two of these three companies, resulting in 12 companies that ultimately provided detailed information relevant to our inquiries. The 5 companies that responded to the follow-up email completed the online survey. Overall, the 17 respondent companies supplied data for 19 devices, which corresponds to detailed information for 32% of all devices in the dataset.
16 of the 17 respondent companies supplied pricing and return policy information. 15 provided responses regarding ease of use; this information generally was qualitative, such as “Very easy to use independently “ and “Quick to setup” (see Supplementary Materials). 13 described usage requirements (e.g., frequency and duration), but this was reported in widely varied form (Table 5). 14 reported on motivational features (see distribution of these features in Figure 5).
Regarding respondent roles, 33% of the replies came from C-suite executives (e.g., CEO, COO), 33% from sales representatives, 16% from clinical specialists, and the remaining 16% from managers, customer service staff, or engineers.
4. Discussion
The goal of this work was to determine the number and nature of FDA-approved devices suitable for home use after stroke, and to understand which types of information matter most to stroke survivors when evaluating these technologies. We identified relevant devices through a systematic search of FDA product codes, surveyed stroke survivors about their informational needs, and contacted manufacturers to obtain missing details about price, usability, training requirements, and motivational features. The main findings were that the number of home rehabilitation devices available in the United States has expanded considerably over the last 10 years, that stroke survivors prioritize information about ease of use, training dose, training benefit, and motivational features, and that such information is often difficult to locate online and inconsistently reported by manufacturers. Manufacturer responsiveness was limited, and recommendations for device usage lacked standardization and clear links to evidence. We archived the information we found in a dataset available in the Supplementary Materials. We discuss these results now, followed by limitations and future directions.
4.1. Increasing Number of FDA-Approved Devices for Home Movement Rehabilitation After Stroke
We found that, as recently as of 2010, there were only a handful of devices available for home stroke movement rehabilitation that had FDA-approval; today there are almost 60. These devices span a wide range of body targets and prices, and use a wide range of approaches, roughly balanced among wearables, non-wearables, stimulation, and motion-sensing software systems. This proliferation of devices is a positive development for stroke survivors and their caregivers. However, it also presents a practical challenge: how does one select a device? We discuss this question in the next section.
Academic publications on home stroke rehabilitation technologies have also grown rapidly over the same period, at approximately the same normalized rate as FDA-approved products (Figure 6). This parallel growth suggests a linkage between academic research activity and product development. However, the number of FDA-approved devices remains only about 5% of the number of academic papers, indicating that the majority of published work does not translate into cleared products. Future research could quantify what percentage of FDA-approved rehabilitation devices originated from inventions in academic settings, what proportion of academic papers represent clinical validation studies of FDA-approved devices, and what technical, regulatory, usability, or business factors most commonly prevent promising laboratory prototypes from progressing to FDA clearance.
4.2. Mismatch Between User Priorities and Available Information
In terms of how people with stroke wish to select devices, survey participants consistently expressed interest in knowing how easy devices are to be used without supervision, how much practice is required to obtain a therapeutic benefit, how large a therapeutic benefit they can expect, and what motivational features would support their use of the device. These priorities align with longstanding barriers to home-based rehabilitation, including uncertainty about setup, difficulty sustaining adherence, and the challenge of judging whether a device will be manageable for one’s impairment level [48,49].
A central finding of this study, however, is the gap between the information stroke survivors prioritize and what manufacturers make available to the public. Manufacturer websites and product materials rarely address usability constraints or day-to-day training expectations in clear terms. Motivational features are also described inconsistently, despite their importance for maintaining engagement. This mismatch suggests that individuals seeking home rehabilitation tools must either make decisions with partial information or rely on a clinician or researcher to interpret the scarce information available and give them recommendations. Our cross-check against existing online directories further underscored this gap, as each listed only a subset of the devices we identified and provided limited information, confirming that no single existing resource provides complete coverage of home-use stroke rehabilitation technologies and reinforcing the need for a more comprehensive, user-centered database.
The mismatch between user priorities and manufacturer disclosures likely reflects, in part, structural factors in the device approval ecosystem rather than a simple communication failure. The FDA 510(k) process evaluates devices for substantial equivalence to predicate devices, with a focus on safety and mechanical performance. It does not emphasize systematic evaluation of home usability, long-term adherence, or dose-response effects; therefore, manufacturers are not explicitly required to generate or report the kinds of information that stroke survivors value most. As manufacturers tend to generate data that satisfies regulatory requirements, user-centered information, such as ease of independent use, specific training expectations, and motivational impact, often remains underdeveloped or unpublished. When a stroke survivor asks, “Will this motivate me?”, they ask a question that the regulatory pathway does not require the manufacturer to answer.
Furthermore, the legal landscape discourages specificity regarding “Usage Requirements.” As noted in the Introduction, the dose-response relationship for movement training after stroke is complex and patient-specific (e.g., depending on the timing and location of the stroke within the nervous system). If a manufacturer were to explicitly state, “Use this device 60 minutes daily for 3 months to restore hand function,” they would be making a specific medical claim that requires extensive clinical evidence to substantiate. Within a 510(k) framework, this may create perceived pressure to remain conservative and non-specific about expected benefits and usage requirements. Thus, current regulatory and evidentiary expectations may contribute to the transparency gap, even as users seek more concrete guidance.
Additionally, while we did not analyze the clinical evidence for each device, this evidence is almost certainly limited, relying mostly on small studies in groups of stroke survivors who meet very specific inclusion criteria (such as minimal cognitive deficits). Enhancing the dataset with a comprehensive description of available clinical evidence is an important future direction.
4.3. Manufacturer Responsiveness and Transparency Gaps
The modest responsiveness of companies to direct inquiries underscores broader transparency challenges. Only a minority of manufacturers provided detailed information despite receiving multiple requests. Even among those who responded, the depth and clarity of information varied substantially, with some offering broad marketing language rather than concrete guidance. This inconsistency leaves potential users with unequal access to essential details about device operation, supporting evidence, cost structure, and return options. Improving the accessibility and completeness of device information would likely increase confidence among both users and clinicians considering technology-supported home rehabilitation.
The finding that fewer than half of manufacturers responded to inquiries, and that some responses lacked specific data, highlights the fragility of the rehabilitation technology sector. Unlike the pharmaceutical industry, which is dominated by stable giants, the rehab tech landscape is populated by small- to medium-sized enterprises and early-stage startups. A non-response to a potential customer inquiry may reflect limited resources (a third of responses came from C-suite executives), high turnover, or commercial inactivity. For stroke survivors and clinicians, this introduces an additional dimension of “vendor risk”, in which a device may be technically available and FDA-cleared but not actively supported or responsive to user needs. Future iterations of the dataset should therefore distinguish between devices that are only regulatorily active and those that are also commercially responsive, so that users are not guided toward options that are no longer realistically accessible or supported.
4.4. Challenges in Reporting Therapeutic Dose and Ease of Use
We wish to highlight a key issue revealed by this work: the lack of standardization in reporting therapeutic dose-response and ease-of-use. For dose-response, although some manufacturers provided recommended usage schedules, these guidelines were often vague or not tied to empirical data. This is consistent with broader challenges in the rehabilitation field, where dose is rarely defined with precision and lacks a consistent international reporting standard [50,51]. Furthermore, dose–response relationships remain difficult to characterize due to complex interactions between task type, duration-since-stroke, impairment level, and training context, with recent evidence suggesting that response trajectories are highly individualized [52]. A major limitation in current practice is the reliance on “time scheduled for therapy” as a dose metric, which frequently overestimates the actual active movement practice received by the patient [20,53].
The same lack of standardization appeared in descriptions of ease of use. While quantitative scales such as the System Usability Scale (SUS) have recently become more common in rehabilitation robotics research, they are sporadically applied, with many studies continuing to rely on non-validated, ad-hoc questionnaires [54,55,56,57]. Furthermore, researchers have found that even when standardized scales are used, the standard benchmarks (originally developed for software and consumer electronics) do not accurately reflect the physical and cognitive complexity of rehabilitation robotics [54]. Some companies emphasized that a device is “simple” or “intuitive” without specifying the types of movements required, the need for caregiver assistance, or the physical demands on users with limited strength or dexterity. For individuals with stroke, especially those with moderate-to-severe impairments, such information is essential for determining whether a device is feasible in the home environment.
To address these issues, it may be useful to move toward a concise and standardized “rehabilitation device profile” that quantifies the qualitative features users prioritize. Such a profile could incorporate metrics for setup burden (e.g., time from unpacking to first repetition), level of assistance required, mechanical intensity (e.g., achievable repetitions per minute), and cognitive load associated with device operation. For dose–response, a similar standardized framework could summarize the cumulative active practice time that has been tested, the associated changes in clinically relevant outcomes, the level of evidential support, and the impairment severity for which these data are most applicable. Adopting these standards would allow stroke survivors and clinicians to compare the therapeutic potential and usability of different devices more effectively and would encourage manufacturers to align clinical validation with the information that matters most to end users.
4.5. Implications for Database Design and Clinical Decision Making
The findings directly informed the design of the stroke-focused neurotechnology dataset we include in the Supplementary Materials. We are now in the process of incorporating this dataset into a database that can be accessed using a companion website and chatbot interface.
Survey responses indicated that stroke survivors preferred to interact with a chatbot on their phone rather than contact a company salesperson for help selecting devices. They wanted to be able to ask questions in their own words, compare devices side by side, and receive personalized information in a guided, phone-accessible process instead of feeling that they were being “sold” a specific product. Further, because stroke survivors prioritized usability, dosage guidance, and motivational elements, these items are prominent fields in the database we are developing and will be highlighted in user-facing summaries. The variability and incompleteness of manufacturers’ responses emphasize the need for clearly marking when information is verified, missing, or uncertain. Presenting device characteristics in a structured, comparable format can help users more easily navigate the increasingly crowded landscape of rehabilitation technologies and make informed decisions that align with their capabilities and goals.
Consistent with the preferences identified here, the chatbot will be designed to learn from each user’s characteristics, goals, and preferences, if granted permission to use that information. This will allow it to recommend devices tailored to their needs rather than offering generic suggestions. Confidentiality must be ensured if a user wishes to have personalized responses. At the same time, the system will present a clear disclaimer stating that the suggestions provided are for informational purposes only, do not constitute medical advice, and should not replace consultation with healthcare professionals. Users will be reminded to consult their healthcare provider, physical therapist, or occupational therapist before using any rehabilitation device, and that suitability depends on individual condition, needs, and medical history. A limitation of liability statement will also explain that the app and its AI assistants are provided “as is” without warranties and that the developers are not responsible for actions taken based on the information provided. For clinicians, the database may serve as a consolidated reference that reduces the time required to review available options and supports more efficient, evidence-informed discussions with patients about home rehabilitation technologies.
4.6. Limitations, Future Directions, and Recommendations for Industry Standards
This study has several limitations. The survey sample size was modest and drawn from participants involved in ongoing research studies at a single institution, which may limit generalizability. Some devices lacked available information despite repeated outreach, leading to gaps that could not be filled without manufacturer cooperation. The analysis focused on devices cleared in the United States and does not capture products available in other regulatory environments. We may also have missed some relevant FDA codes and thus excluded relevant devices. Further, we focused on devices with FDA codes that we judged to be “higher tech”, involving electronics in some ways. There are many simpler, passive tools for stroke movement rehabilitation, such as exercise bands and grip exercisers. Some passive wearable orthoses are non-actuated and non-sensorized yet mechanically support movement in clever and therapeutically useful ways. The dataset could be expanded to include such devices in the future.
Future work will expand the dataset, refine data collection procedures, incorporate structured summaries of clinical evidence, and evaluate the usability and impact of the planned website and chatbot with stroke survivors, caregivers, and clinicians. In addition, we plan to develop automated methods for identifying new devices and updating device information, ensuring the dataset can be refreshed regularly and does not become outdated as the rehabilitation technology landscape evolves.
This study suggests that the rapidly growing home rehabilitation technology field would benefit from industry-wide reporting standards. Key information should be consistently disclosed, including price, return policies, independent usability requirements, and recommended training dose to achieve a specified benefit. Motivational design elements should be described clearly enough for users to understand how the device supports sustained engagement. Aligning these reporting practices with standardized usability and dose-response metrics, as outlined above, would help transform vague claims into comparable, evidence-based summaries. Such standardization would not only help individuals and clinicians compare devices but also promote higher-quality design and clearer expectations about device capabilities, improving transparency, trust, and translation.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figures 1-6; Tables 1-5; Dataset of devices; Survey of informational needs; and Manufacturer outreach emails.
Author Contributions
Conceptualization, L.GF., J.PI., A.F., V.C., J.M. and D.R.; methodology, L.GF., J.PI., A.F. and D.R.; validation, L.GF. and D.R.; formal analysis, L.GF. and D.R.; investigation, L.GF.; data curation, L.GF. and V.C.; writing—original draft preparation, L.GF. and D.R.; writing—review and editing, J.PI., A.F., V.C., J.M. and D.R.; visualization, L.GF.; supervision, J.PI. and D.R.; project administration, J.PI. and D.R.; funding acquisition, J.PI. and D.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded in part by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, grant number 1UM1TR004927.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the University of California Irvine (protocol code: #4862 and date of approval: October 24, 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting the results can be found in the Dataset included the Supplementary Materials.
Conflicts of Interest
David J. Reinkensmeyer has a financial interest in Hocoma and Flint Rehabilitation Devices, companies that develop and sell rehabilitation devices. The terms of these arrangements have been reviewed and approved by the University of California, Irvine, in accordance with its conflict of interest policies.
Abbreviations
The following abbreviations are used in this manuscript:
| FDA | Food and Drug Administration |
| FES | Functional Electrical Stimulation |
| VR | Virtual Reality |
| AR | Augmented Reality |
| HIPAA | Health Insurance Portability and Accountability Act |
| NMES | Neuromuscular Electrical Stimulation |
| CEO | Chief Executive Officer |
| COO | Chief Operating Officer |
| SUS | System Usability Score |
| AI | Artificial Intelligence |
References
- Adamson, J.; Beswick, A.; Ebrahim, S. Is Stroke the Most Common Cause of Disability? Journal of Stroke and Cerebrovascular Diseases 2004, 13, 171–177. [Google Scholar] [CrossRef]
- Gresham, G.E.; Duncan, P.W.; Stason, W.B.; Adams, H.P.; Adelman, A.M.; Alexander, D.N.; Bishop, D.S.; Diller, L.; Donaldson, N.E.; Granger, C. V; et al. Post-Stroke Rehabilitation; U.S. Department of Health and Human Services. Public Health Service, Agency for Health Care Policy and Research: Rockville, MD, 1995. [Google Scholar]
- Aha Know the Facts, Get the Stats. In American Heart Association; 2007; Volume 4.
- Dobkin, B.H. Neurologic Rehabilitation; F.A. Davis Company: Philadelphia, 1996. [Google Scholar]
- Kelly-Hayes, M.; Beiser, A.; Kase, C.S.; Scaramucci, A.; D’Agostino, R.B.; Wolf, P.A. The Influence of Gender and Age on Disability Following Ischemic Stroke: The Framingham Study. J Stroke Cerebrovasc Dis 2003, 12, 119–126. [Google Scholar] [CrossRef]
- Feys, H.M.; De Weerdt, W.J.; Selz, B.E.; Cox Steck, G.A.; Spichiger, R.; Vereeck, L.E.; Putman, K.D.; Van Hoydonck, G.A. Effect of a Therapeutic Intervention for the Hemiplegic Upper Limb in the Acute Phase after Stroke: A Single-Blind, Randomized, Controlled Multicenter Trial. Stroke 1998, 29, 785–792. [Google Scholar] [CrossRef]
- Feys, H.; De Weerdt, W.; Verbeke, G.; Steck, G.C.; Capiau, C.; Kiekens, C.; Dejaeger, E.; Van Hoydonck, G.; Vermeersch, G.; Cras, P. Early and Repetitive Stimulation of the Arm Can Substantially Improve the Long-Term Outcome after Stroke: A 5-Year Follow-up Study of a Randomized Trial. Stroke; a journal of cerebral circulation 2004, 35, 924–929. [Google Scholar] [CrossRef]
- Kwakkel, G.; van Peppen, R.; Wagenaar, R.C.; Wood Dauphinee, S.; Richards, C.; Ashburn, A.; Miller, K.; Lincoln, N.; Partridge, C.; Wellwood, I.; et al. Effects of Augmented Exercise Therapy Time after Stroke: A Meta-Analysis. Stroke 2004, 35, 2529–2539. [Google Scholar] [CrossRef] [PubMed]
- Kwakkel, G.; Wagenaar, R.C.; Twisk, J.W.; Lankhorst, G.J.; Koetsier, J.C. Intensity of Leg and Arm Training after Primary Middle-Cerebral-Artery Stroke: A Randomised Trial. Lancet 1999, 354, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.L.; Winstein, C.J.; Miller, J.P.; Taub, E.; Uswatte, G.; Morris, D.; Giuliani, C.; Light, K.E.; Nichols-Larsen, D.; Investigators, E. Effect of Constraint-Induced Movement Therapy on Upper Extremity Function 3 to 9 Months after Stroke: The EXCITE Randomized Clinical Trial. JAMA 2006, 296, 2095–2104. [Google Scholar] [CrossRef] [PubMed]
- Byl, N.N.; Pitsch, E. a; Abrams, G.M. Functional Outcomes Can Vary by Dose: Learning-Based Sensorimotor Training for Patients Stable Poststroke. Neurorehabilitation and neural repair 2008, 22, 494–504. [Google Scholar] [CrossRef]
- Lang, C.E.; Strube, M.J.; Bland, M.D.; Waddell, K.J.; Cherry-Allen, K.M.; Nudo, R.J.; Dromerick, A.W.; Birkenmeier, R.L. Dose Response of Task-Specific Upper Limb Training in People at Least 6 Months Poststroke: A Phase II, Single-Blind, Randomized, Controlled Trial. Annals of Neurology 2016, 80, 342–354. [Google Scholar] [CrossRef]
- Adolph, K.E.; Cole, W.G.; Komati, M.; Garciaguirre, J.S.; Badaly, D.; Lingeman, J.M.; Chan, G.L.Y.; Sotsky, R.B. How Do You Learn to Walk? Thousands of Steps and Dozens of Falls per Day. Psychological Science 2012, 23, 1387–1394. [Google Scholar] [CrossRef]
- Ward, N.S.; Brander, F.; Kelly, K. Intensive Upper Limb Neurorehabilitation in Chronic Stroke: Outcomes from the Queen Square Programme. J Neurol Neurosurg Psychiatry 2019, 90, 498–506. [Google Scholar] [CrossRef]
- Cramer, S.C.; Dodakian, L.; Le, V.; See, J.; Augsburger, R.; McKenzie, A.; Zhou, R.J.; Chiu, N.L.; Heckhausen, J.; Cassidy, J.M.; et al. Efficacy of Home-Based Telerehabilitation vs In-Clinic Therapy for Adults after Stroke: A Randomized Clinical Trial. JAMA Neurology 2019. [Google Scholar] [CrossRef]
- Daly, J.J.; McCabe, J.P.; Holcomb, J.; Monkiewicz, M.; Gansen, J.; Pundik, S. Long-Dose Intensive Therapy Is Necessary for Strong, Clinically Significant, Upper Limb Functional Gains and Retained Gains in Severe/Moderate Chronic Stroke. Neurorehabil Neural Repair 2019, 33, 523–537. [Google Scholar] [CrossRef]
- Wang, C.; Winstein, C.; D’Argenio, D.Z.; Schweighofer, N. The Efficiency, Efficacy, and Retention of Task Practice in Chronic Stroke. Neurorehabil Neural Repair 2020, 34, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Ottenbacher, K.J.; Smith, P.M.; Illig, S.B.; Linn, R.T.; Ostir, G. V; Granger, C. V Trends in Length of Stay, Living Setting, Functional Outcome, and Mortality Following Medical Rehabilitation. JAMA: the journal of the American Medical Association 2004, 292, 1687–1695. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.M.; Guo, L.; Scheer, S.J. Changes in the Status of Hospitalized Stroke Patients since Inception of the Prospective Payment System in 1983. Arch Phys Med Rehabil 2002, 83, 894–898. [Google Scholar] [CrossRef]
- Lang, C.E.; MacDonald, J.R.; Gnip, C. Counting Repetitions: An Observational Study of Outpatient Therapy for People with Hemiparesis Post-Stroke. Journal of Neurologic Physical Therapy 2007, 31, 3–10. [Google Scholar] [CrossRef]
- Young, B.M.; Holman, E.A.; Cramer, S.C. STRONG Study Investigators Rehabilitation Therapy Doses Are Low After Stroke and Predicted by Clinical Factors. Stroke 2023, 54, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Bode, R.K.; Heinemann, A.W.; Semik, P.; Mallinson, T. Relative Importance of Rehabilitation Therapy Characteristics on Functional Outcomes for Persons with Stroke. Stroke; a journal of cerebral circulation 2004, 35, 2537–2542. [Google Scholar] [CrossRef]
- Turton, A.; Fraser, C. The Use of Home Therapy Programmes for Improving Recovery of the Upper Limb Following Stroke. British Journal of Occupational Therapy 1990, 53, 457–462. [Google Scholar] [CrossRef]
- Sluijs, E.M.; Kok, G.J.; van der Zee, J. Correlates of Exercise Compliance in Physical Therapy. Physical Therapy 1993, 73, 771–776. [Google Scholar] [CrossRef]
- Chen, C.Y.; Neufeld, P.S.; Feely, C.A.; Skinner, C.S. Factors Influencing Compliance with Home Exercise Programs among Patients with Upper-Extremity Impairment. The American journal of occupational therapy.: official publication of the American Occupational Therapy Association 1999, 53, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Brewer, B.R.; McDowell, S.K.; Worthen-Chaudhari, L.C. Poststroke Upper Extremity Rehabilitation: A Review of Robotic Systems and Clinical Results. Topics in stroke rehabilitation 2007, 14, 22–44. [Google Scholar] [CrossRef]
- Reinkensmeyer, D.J.; Emken, J.L.; Cramer, S.C. Robotics, Motor Learning, and Neurologic Recovery. Annual Review of Biomedical Engineering 2004, 6, 497–525. [Google Scholar] [CrossRef]
- Riener, R.; Nef, T.; Colombo, G. Robot-Aided Neurorehabilitation of the Upper Extremities. Med Biol Eng Comput 2005, 43, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Hesse, S.; Schmidt, H.; Werner, C. Machines to Support Motor Rehabilitation after Stroke: 10 Years of Experience in Berlin. Journal of rehabilitation research and development 2006, 43, 671–678. [Google Scholar] [CrossRef]
- Kwakkel, G.; Kollen, B.J.; Krebs, H.I. Effects of Robot-Assisted Therapy on Upper Limb Recovery after Stroke: A Systematic Review. Neurorehabilitation and neural repair 2008, 22, 111–121. [Google Scholar] [CrossRef]
- Mehrholz, J.; Platz, T.; Kugler, J.; Pohl, M. Electromechanical and Robot-Assisted Arm Training for Improving Arm Function and Activities of Daily Living after Stroke. Cochrane database of systematic reviews (Online) 2008, (4), CD006876. [Google Scholar]
- Adans-Dester, C.P.; Lang, C.E.; Reinkensmeyer, D.J.; Bonato, P. Wearable Sensors for Stroke Rehabilitation. In Neurorehabilitation Technology; Reinkensmeyer, D.J., Marchal-Crespo, L., Dietz, V., Eds.; Springer International Publishing: Cham, 2022; pp. 467–507. ISBN 978-3-031-08995-4. [Google Scholar]
- Maceira-Elvira, P.; Popa, T.; Schmid, A.-C.; Hummel, F.C. Wearable Technology in Stroke Rehabilitation: Towards Improved Diagnosis and Treatment of Upper-Limb Motor Impairment. J Neuroeng Rehabil 2019, 16, 142. [Google Scholar] [CrossRef]
- Boukhennoufa, I.; Zhai, X.; Utti, V.; Jackson, J.; McDonald-Maier, K.D. Wearable Sensors and Machine Learning in Post-Stroke Rehabilitation Assessment: A Systematic Review. Biomedical Signal Processing and Control 2022, 71, 103197. [Google Scholar] [CrossRef]
- Takeda, K.; Tanino, G.; Miyasaka, H. Review of Devices Used in Neuromuscular Electrical Stimulation for Stroke Rehabilitation. Medical Devices: Evidence and Research 2017, 10, 207–213. [Google Scholar] [CrossRef]
- Khan, M.A.; Fares, H.; Ghayvat, H.; Brunner, I.C.; Puthusserypady, S.; Razavi, B.; Lansberg, M.; Poon, A.; Meador, K.J. A Systematic Review on Functional Electrical Stimulation Based Rehabilitation Systems for Upper Limb Post-Stroke Recovery. Front Neurol 2023, 14, 1272992. [Google Scholar] [CrossRef]
- Celian, C.; Swanson, V.; Shah, M.; Newman, C.; Fowler-King, B.; Gallik, S.; Reilly, K.; Reinkensmeyer, D.J.; Patton, J.; Rafferty, M.R. A Day in the Life: A Qualitative Study of Clinical Decision-Making and Uptake of Neurorehabilitation Technology. J Neuroeng Rehabil 2021, 18, 121. [Google Scholar] [CrossRef] [PubMed]
- Celian, C.; Redd, H.; Smaller, K.; Ryali, P.; Patton, J.L.; Reinkensmeyer, D.J.; Rafferty, M.R. Use of Technology in the Rehabilitation Setting: Therapy Observations, Mixed Methods Analysis, and Data Visualization. Arch Rehabil Res Clin Transl 2025, 7, 100425. [Google Scholar] [CrossRef]
- Perez-Ibarra, J.C.; Garcia-Fernandez, L.; Farrens, A.J.; Bender, M.; Han, J.J.; Reinkensmeyer, D.J. User Preferences and Information Gaps for AI-Assisted Selection of Engineered Devices for Home Rehabilitation After Stroke. In Proceedings of the 2025 International Conference On Rehabilitation Robotics (ICORR), May 2025; pp. 1536–1541. [Google Scholar]
- McGibbon, C.A.; Sexton, A.; Jayaraman, A.; Deems-Dluhy, S.; Gryfe, P.; Novak, A.; Dutta, T.; Fabara, E.; Adans-Dester, C.; Bonato, P. Evaluation of the Keeogo Exoskeleton for Assisting Ambulatory Activities in People with Multiple Sclerosis: An Open-Label, Randomized, Cross-over Trial. J NeuroEngineering Rehabil 2018, 15, 117. [Google Scholar] [CrossRef]
- Sanders, Q.; Chan, V.; Augsburger, R.; Cramer, S.C.; Reinkensmeyer, D.J.; Sharp, K. Feasibility of Home Hand Rehabilitation Using Musicglove after Chronic Spinal Cord Injury. Spinal Cord Ser Cases 2022, 8, 86. [Google Scholar] [CrossRef]
- Telerehabilitation Robotics: Overview of Approaches and Clinical Outcomes. In Rehabilitation Robotics; Academic Press, 2018; pp. 333–346.
- Saric, L.; Knobel, S.E.J.; Pastore-Wapp, M.; Nef, T.; Mast, F.W.; Vanbellingen, T.; Saric, L.; Knobel, S.E.J.; Pastore-Wapp, M.; Nef, T.; et al. Usability of Two New Interactive Game Sensor-Based Hand Training Devices in Parkinson’s Disease. Sensors 2022, 22. [Google Scholar] [CrossRef]
- Curteza, A.; Cretu, V.; Macovei, L.; Poboroniuc, M. The Manufacturing of Textile Products with Incorporated Electrodes. AUTEX Research Journal 2016, 16, 13–18. [Google Scholar] [CrossRef]
- Metani, A.; Popović-Maneski, L.; Mateo, S.; Lemahieu, L.; Bergeron, V. Functional Electrical Stimulation Cycling Strategies Tested during Preparation for the First Cybathlon Competition – a Practical Report from Team ENS de Lyon. Eur J Transl Myol 2017, 27, 7110. [Google Scholar] [CrossRef] [PubMed]
- Mura, A.; Maier, M.; Ballester, B.R.; De la Torre Costa, J.; López-Luque, J.; Gelineau, A.; Mandigout, S.; Ghatan, P.H.; Fiorillo, R.; Antenucci, F.; et al. Bringing Rehabilitation Home with an E-Health Platform to Treat Stroke Patients: Study Protocol of a Randomized Clinical Trial (RGS@home). Trials 2022, 23, 518. [Google Scholar] [CrossRef] [PubMed]
- Geerse, D.J.; Hoogendoorn, E.M.; van Doorn, P.F.; van Bergem, J.S.; van Dam, A.T.; Hardeman, L.E.S.; Roerdink, M. Cueing-Assisted Gamified Augmented-Reality Gait-and-Balance Rehabilitation at Home for People with Parkinson’s Disease: Protocol of a Pragmatic Randomized Controlled Trial Implemented in the Clinical Pathway. Front. Neurol. 2025, 16. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Abel, K.T.; Janecek, J.T.; Chen, Y.; Zheng, K.; Cramer, S.C. Home-Based Technologies for Stroke Rehabilitation: A Systematic Review. International Journal of Medical Informatics 2019, 123, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, A.; Howes, S.; Murphy, P.J.; Deutsch, J.E.; Stokes, M.; Pedlow, K.; McDonough, S.M. Factors Influencing the Delivery of Telerehabilitation for Stroke: A Systematic Review. PLOS ONE 2022, 17, e0265828. [Google Scholar] [CrossRef] [PubMed]
- Hayward, K.S.; Churilov, L.; Dalton, E.J.; Brodtmann, A.; Campbell, B.C.V.; Copland, D.; Dancause, N.; Godecke, E.; Hoffmann, T.C.; Lannin, N.A.; et al. Advancing Stroke Recovery Through Improved Articulation of Nonpharmacological Intervention Dose. Stroke 2021, 52, 761–769. [Google Scholar] [CrossRef]
- Borschmann, K.; Hayward, K.S.; Raffelt, A.; Churilov, L.; Kramer, S.; Bernhardt, J. Rationale for Intervention and Dose Is Lacking in Stroke Recovery Trials: A Systematic Review. Stroke Research and Treatment 2018, 2018, 8087372. [Google Scholar] [CrossRef]
- Gauthier, L.V.; Ravi, R.; DeLuca, D.; Zhou, W. Dose Response to Upper Extremity Stroke Rehabilitation Varies by Individual: Early Indicators of Treatment Response. Stroke 2024, 55, 696–704. [Google Scholar] [CrossRef]
- Lang, C.E.; Macdonald, J.R.; Reisman, D.S.; Boyd, L.; Jacobson Kimberley, T.; Schindler-Ivens, S.M.; Hornby, T.G.; Ross, S.A.; Scheets, P.L. Observation of Amounts of Movement Practice Provided during Stroke Rehabilitation. Arch Phys Med Rehabil 2009, 90, 1692–1698. [Google Scholar] [CrossRef]
- Nicora, G.; Santangelo, G.; Marzero, G.; Dagliati, A.; Aprile, I.; Quaglini, S. Exploring Usability Standards in Robotic Rehabilitation: A Meta-Analysis of System Usability Scale Scores. IEEE Int Conf Rehabil Robot 2025, 2025, 476–482. [Google Scholar] [CrossRef]
- Moulaei, K.; Moulaei, R.; Bahaadinbeigy, K. The Most Used Questionnaires for Evaluating the Usability of Robots and Smart Wearables: A Scoping Review. DIGITAL HEALTH 2024, 10, 20552076241237384. [Google Scholar] [CrossRef]
- Zanatta, F.; Giardini, A.; Pierobon, A.; D’Addario, M.; Steca, P. A Systematic Review on the Usability of Robotic and Virtual Reality Devices in Neuromotor Rehabilitation: Patients’ and Healthcare Professionals’ Perspective. BMC Health Serv Res 2022, 22, 523. [Google Scholar] [CrossRef]
- Nguyen, C.M.; Uy, J.; Serrada, I.; Hordacre, B. Quantifying Patient Experiences with Therapeutic Neurorehabilitation Technologies: A Scoping Review. Disability and Rehabilitation 2024, 46, 1662–1672. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Representative examples of FDA-cleared rehabilitation devices suitable for home use after stroke. The collage shows one example device for each of the eight device categories used in this study. From top left to top right: actuated wearable (Keeogo – B-Temia [40]), sensorized wearable (MusicGlove – Flint Rehab [41]), robot (Motus Foot – Motus Nova [42]), and exerciser (GripAble Home – GripAble [43]). From bottom left to right: stimulator (L300 – Bioness [44]), FES bike (RT300 FES Cycle Ergometer – Restorative Therapies [45]), motion capture software (RGS – Eodyne [46]), and VR/AR headset (Reality DTx – Strolll [47]).
Figure 1.
Representative examples of FDA-cleared rehabilitation devices suitable for home use after stroke. The collage shows one example device for each of the eight device categories used in this study. From top left to top right: actuated wearable (Keeogo – B-Temia [40]), sensorized wearable (MusicGlove – Flint Rehab [41]), robot (Motus Foot – Motus Nova [42]), and exerciser (GripAble Home – GripAble [43]). From bottom left to right: stimulator (L300 – Bioness [44]), FES bike (RT300 FES Cycle Ergometer – Restorative Therapies [45]), motion capture software (RGS – Eodyne [46]), and VR/AR headset (Reality DTx – Strolll [47]).

Figure 2.
Characteristics of FDA approved rehabilitation devices suitable for home use after stroke. (a) Distribution of FDA approval years for devices with available approval dates (n = 50), illustrating the increasing availability of devices; (b) Estimated yearly device expenses for devices with available pricing information (n = 38), where purchase prices, subscription fees, and leasing costs were converted to an approximate yearly cost.
Figure 2.
Characteristics of FDA approved rehabilitation devices suitable for home use after stroke. (a) Distribution of FDA approval years for devices with available approval dates (n = 50), illustrating the increasing availability of devices; (b) Estimated yearly device expenses for devices with available pricing information (n = 38), where purchase prices, subscription fees, and leasing costs were converted to an approximate yearly cost.
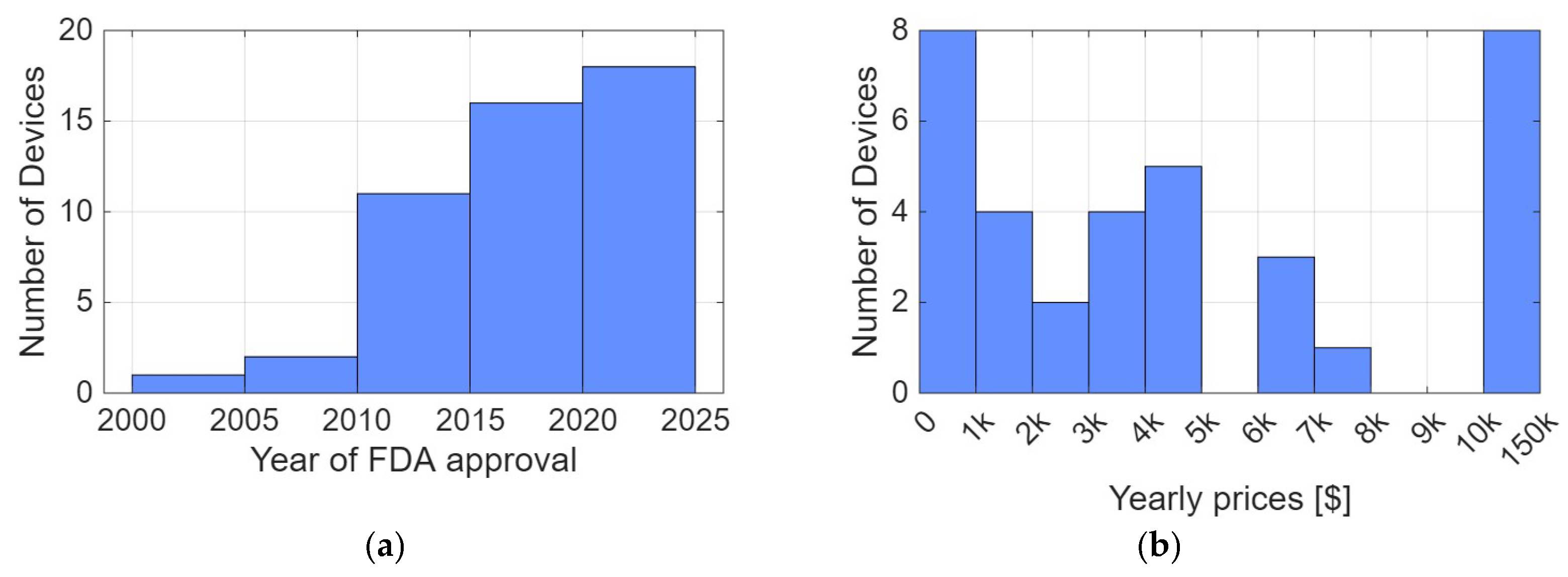
Figure 3.
Distribution of FDA approved rehabilitation devices suitable for home use after stroke across the eight technological categories defined in Table 2 and exemplified in Figure 1.
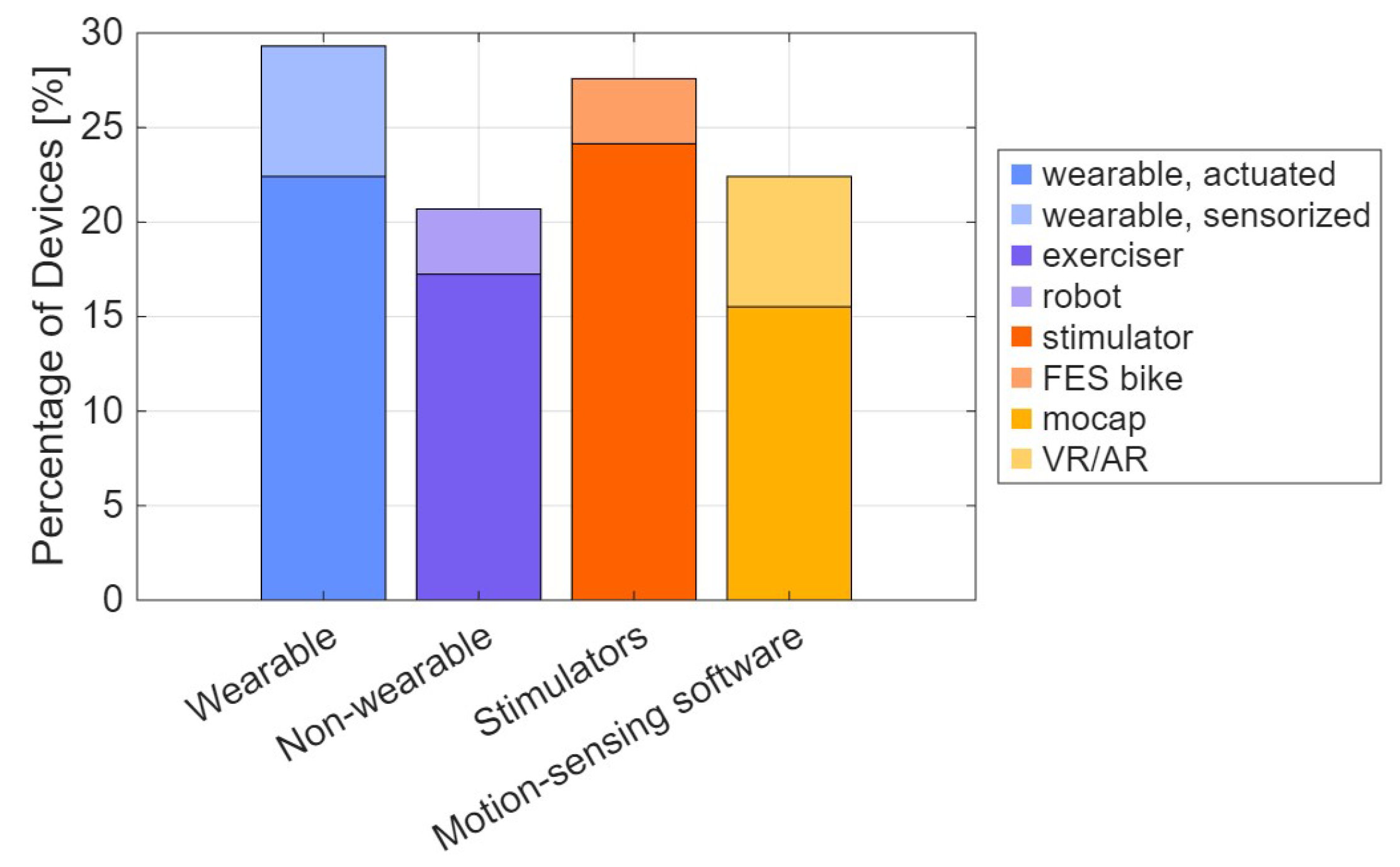
Figure 4.
Summary of survey responses about informational needs and preferred website features. (a) Participants selected their three highest priority, three medium priority, and three lowest priority types of information about rehabilitation devices from a list of nine options; for visualization, these selections were coded as high (3), medium (2), or low (1) importance, and bars show the mean importance score for each information type with error bars indicating the standard deviation; (b) Participants rated the importance of eight possible features of a device selection website on a 10-point scale, where 1 indicated “not important” and 10 indicated “very important,” and bars show the mean rating for each feature with error bars indicating the standard deviation.
Figure 4.
Summary of survey responses about informational needs and preferred website features. (a) Participants selected their three highest priority, three medium priority, and three lowest priority types of information about rehabilitation devices from a list of nine options; for visualization, these selections were coded as high (3), medium (2), or low (1) importance, and bars show the mean importance score for each information type with error bars indicating the standard deviation; (b) Participants rated the importance of eight possible features of a device selection website on a 10-point scale, where 1 indicated “not important” and 10 indicated “very important,” and bars show the mean rating for each feature with error bars indicating the standard deviation.
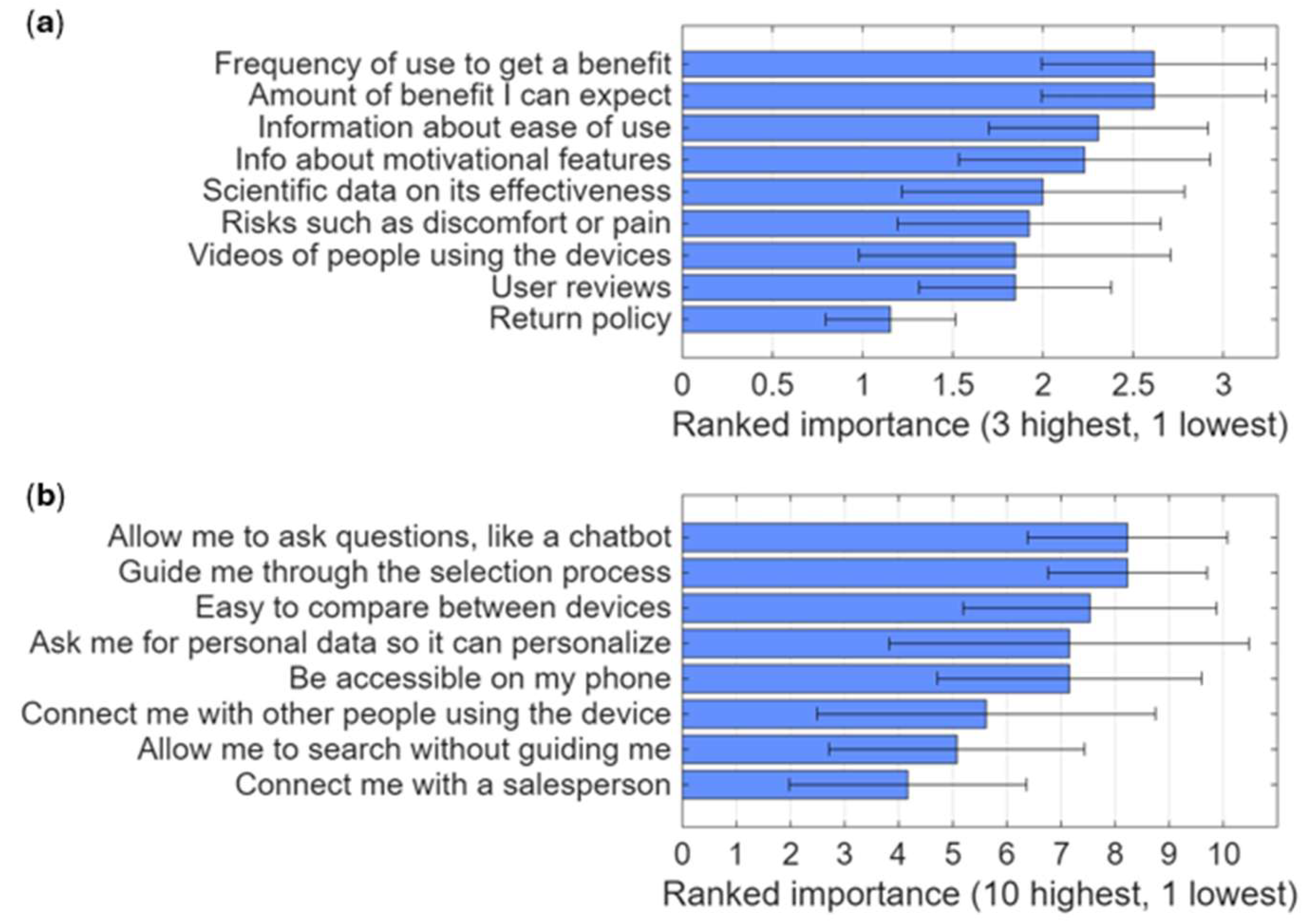
Figure 5.
Motivational features of devices. Bars indicate the percentage of devices that include feedback, progress tracking, gamification, goal setting, or social networking functions.
Figure 5.
Motivational features of devices. Bars indicate the percentage of devices that include feedback, progress tracking, gamification, goal setting, or social networking functions.
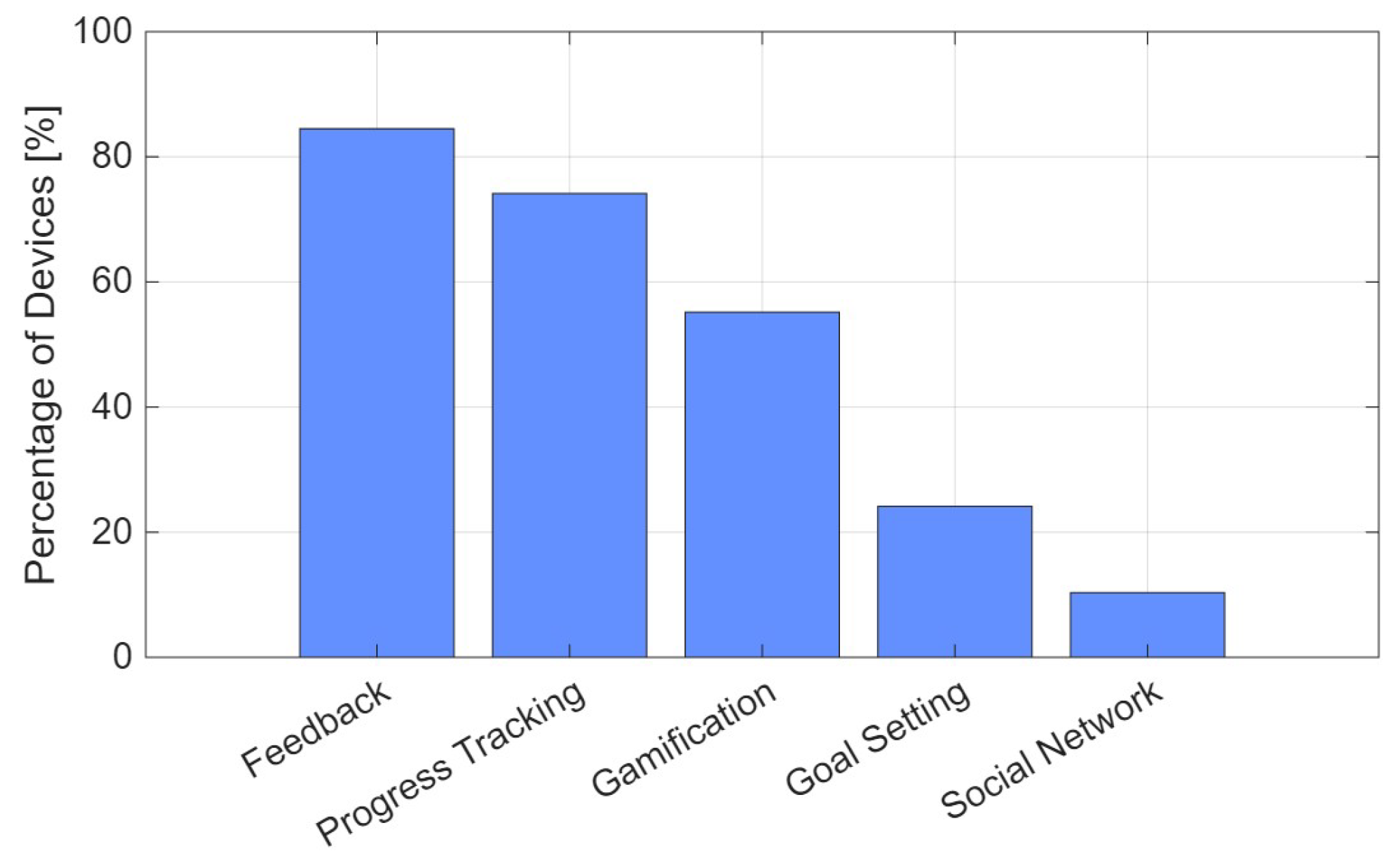
Figure 6.
Cumulative number of publications and FDA-cleared devices related to home-based movement rehabilitation after stroke. The left y-axis shows the cumulative count of PubMed-indexed papers retrieved with the query stroke[Title/Abstract] AND home[Title/Abstract] AND (robot*[Title/Abstract] OR sensor*[Title/Abstract] OR wearable*[Title/Abstract] OR stimulation[Title/Abstract] OR “motion capture”[Title/Abstract] OR “virtual reality”[Title/Abstract] OR VR[Title/Abstract] OR “augmented reality”[Title/Abstract] OR AR[Title/Abstract]) by publication year. The right y-axis shows the cumulative number of FDA-cleared home rehabilitation devices identified in this study for which we found year of approval (48 devices).
Figure 6.
Cumulative number of publications and FDA-cleared devices related to home-based movement rehabilitation after stroke. The left y-axis shows the cumulative count of PubMed-indexed papers retrieved with the query stroke[Title/Abstract] AND home[Title/Abstract] AND (robot*[Title/Abstract] OR sensor*[Title/Abstract] OR wearable*[Title/Abstract] OR stimulation[Title/Abstract] OR “motion capture”[Title/Abstract] OR “virtual reality”[Title/Abstract] OR VR[Title/Abstract] OR “augmented reality”[Title/Abstract] OR AR[Title/Abstract]) by publication year. The right y-axis shows the cumulative number of FDA-cleared home rehabilitation devices identified in this study for which we found year of approval (48 devices).
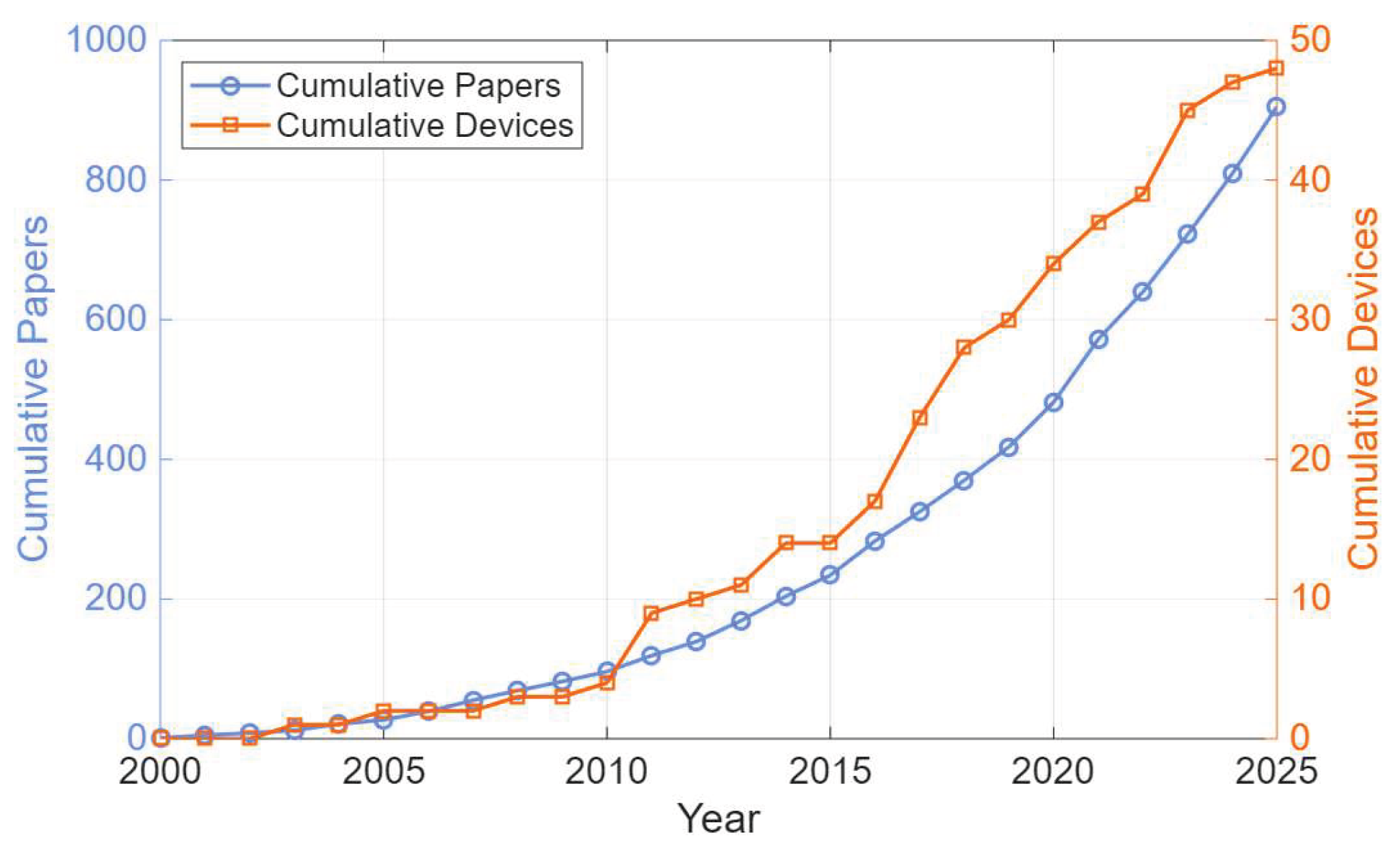

Table 1.
Dataset fields and descriptions.
| Field | Description |
|---|---|
| Name | Commercial name of the device |
| Manufacturer | Name of the company |
| Website | Official site or product page |
| FDA Code(s) | Product classification code(s) |
| Year of Approval | Year of FDA clearance or approval |
| Country | Manufacturer location |
| Price | Retail cost [$] |
| Price per Year | Annualized cost for subscriptions/rentals [$/year] |
| Trained Body Parts | Targeted body parts (e.g., hand, ankle) |
| Product Category | Type of product by technological nature |
| Return Policy | Whether a return policy is offered [Y/N] |
| Insurance Coverage | Whether coverage is available [Y/N] |
| Clinical Evidence | Existence of published validation [Y/N] |
| Ease of Use | Summary of independent use, accessibility, etc. |
| Usage Requirements | Recommended frequency and duration |
| Motivational Features | Features like feedback, goals, games, etc. |
Table 2.
Classification of FDA-cleared home rehabilitation devices by technological nature.
| Category | Description |
|---|---|
| Actuated wearable | Actuated wearable device that provides active movement assistance or resistance through built-in actuators |
| Sensorized wearable | Non-actuated wearable device that uses embedded sensors to measure movement or physiological signals |
| Robot | Non-wearable, actuated device that guides or assists limb or body movements through a robotic mechanism |
| Exerciser | Non-wearable, non-actuated device that supports task-specific movement practice using embedded sensors to track performance |
| Stimulator | Functional electrical stimulation (FES) system that delivers neuromuscular or functional stimulation without being integrated into a cycling device |
| FES bike | Stationary cycling system that combines functional electrical stimulation with a cycle ergometer for therapeutic exercise |
| Motion capture software | Software system that uses cameras or sensors to track, quantify, and visualize body or limb movements |
| VR/AR headset | Virtual or augmented reality (VR or AR) system that delivers rehabilitation tasks through a head-mounted display |
Table 3.
Survey of informational needs’ questions.
| Part 1. Information the website should provide about the devices (select three as most important, three as medium, and three lower) |
| Information about how easy each device is to use |
| Risks such as discomfort or pain |
| How often and for how long do I need to use it to get a benefit |
| What amount of benefit can I expect |
| Information about what motivational features the device offers (these could be things like progress tracking, social networks, gamification, goal setting with feedback, or motivational messages) |
| Videos of people using the devices |
| User reviews |
| Information about scientific studies that support its effectiveness |
| Return policy |
| Part 2. How the website should help you find devices (rate 1 to 10) |
| Ask me for personal information about my impairments and my goals so it can make personalized recommendations for what device would be best for me. |
| Suggest devices in a way that’s easy for me to compare them. |
| Allow me to ask questions like a chatbot. |
| Be accessible on my phone. |
| Guide me through the selection process. |
| Allow me to search without guiding me or asking me questions. |
| Connect me with other people who are using a device I am interested in to help me make my decision. |
| Connect me with a salesperson from the company that makes the device so I can get more information. |
Table 4.
FDA product codes used to identify relevant devices and percentage found.
| Code | Description | Percentage |
|---|---|---|
| QKC | Interactive Rehabilitation Exercise Devices, Prescription Use | 26% |
| GZI | Stimulator, Neuromuscular, External Functional | 22% |
| IPF | Stimulator, Muscle, Powered | 19% |
| BXB | Exerciser, Powered | 10% |
| ION | Exerciser, Non-Measuring | 7% |
| ISD | Exerciser, Measuring | 5% |
| PHL | Powered Exoskeleton | 5% |
| LXJ | Interactive Rehabilitation Exercise Devices | 3% |
| JFA | Exerciser, Finger, Powered | 3% |
| HCC | Device, Biofeedback | 2% |
| PKS | Exerciser, Non-Measuring For Stroke Rehabilitation | 2% |
| QOL | EEG-Driven Upper Extremity Powered Exerciser | 2% |
| IQZ | Hand, External Limb Component, Powered | 2% |
Table 5.
Manufacturer’s response to usage requirements inquiry: “How often and for how long would users need to use the device each week to experience benefits?”. See dataset for further usage information obtained from the websites.
Table 5.
Manufacturer’s response to usage requirements inquiry: “How often and for how long would users need to use the device each week to experience benefits?”. See dataset for further usage information obtained from the websites.
| Frequency of use |
|---|
| Designed to be used daily. Primarily effective while being worn, however with regular use over a longer period of time, customers report general increases to their endurance and speed |
| Variable, 2-3x/week, 60 minutes |
| 30 minutes, 7 days a week |
| Many chronic patients will wear the device daily for the orthotic gait benefits |
| Recommended to exercise at least 40 minutes daily |
| We recommend one hour per day to maximize outcomes |
| 3 to 5 times a week 1-hour sessions |
| 3-5 times per week, up to 1 hour each session |
| 30 minutes, 5 days a week |
| Recommend a minimum of 15 minutes 3 times a week |
| Daily for as long as it is useful. Patient can wear the device all waking hours |
| Daily use is recommended. We recommend patients begin with one 20-minute session /day and then ramp up therapy time gradually. Neuromuscular electrical stimulation (NMES) typically yields results after several months of consistent use |
| 3 times a week for an hour |
| No response (4 companies out of the respondent companies, 28 companies out of the total) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



