
Submitted:
18 December 2025
Posted:
19 December 2025
You are already at the latest version
Abstract
The aim of this study is to evaluate the impact of frontal and maxillary sinus size on the incidence and patterns of upper and middle third facial fractures, assessed using computed tomography (CT) volumetric measurements.
This retrospective observational study included CT scans from January 2019 to May 2025, analysing two cohorts: patients with frontal sinus fractures (n=47) and maxillary sinus fractures (n=244), compared against matched controls without fractures (frontal controls, n=52; maxillary controls, n=178). Sinus dimensions—height, depth, width, and volume—were measured using CT imaging. Statistical analyses employed unpaired t-tests, Cohen’s d effect size, and multivariate linear regression models to identify associations between sinus size and fracture occurrence.
Frontal sinus fracture patients exhibited significantly larger mean sinus volumes compared to controls. Similarly, maxillary sinus fracture patients had notably higher mean sinus volumes. Multivariate regression confirmed sinus height, depth, and width as highly significant predictors of sinus volume (all p< 0.001). After controlling for these dimensions, fracture status alone was not a significant independent predictor of sinus volume, indicating anatomical size primarily influences fracture susceptibility.
Individuals with larger frontal and maxillary sinuses are significantly more susceptible to facial fractures in corresponding regions, likely due to increased bone surface area and reduced structural integrity. These findings emphasize the importance of sinus size in fracture risk assessment, surgical planning, and trauma prevention strategies. Future research should prospectively validate sinus size as a predictive risk factor and explore biomechanical implications across diverse populations.
Keywords:
facial fractures
; maxillary sinus
; frontal sinus
; computed tomography
; sinus volume
; craniomaxillofacial trauma
1. Introduction
Facial fractures commonly occur in patients with multiple trauma, with midfacial fractures comprising 45.4–79.1% of these injuries and frequently involving the maxillary sinus [1,2]. Common causes include motor vehicle accidents, falls, occupational hazards, and interpersonal violence. Trauma-related disruption of maxillary sinus walls often results in sinusitis, characterized by symptoms such as nasal congestion, rhinorrhea, and facial pain [3]. Despite the regenerative capacity of maxillary sinus mucosa, extensive mucosal injuries can exceed healing potential, predisposing to acute or chronic sinusitis and associated complications [4]. Factors contributing to persistent inflammation and chronic sinusitis include hematoma formation within the sinus cavity, obstruction of drainage pathways, and displaced tissue or bone fragments [4,5]. Additionally, surgical interventions such as Le Fort I osteotomies and midfacial fracture reductions may induce sinus inflammation due to bone displacement, disrupted mucociliary clearance, or hematoma formation [6,7].
Frontal sinus fractures (FSFs), representing 5–15% of craniomaxillofacial injuries, typically result from high-energy blunt trauma and are often associated with severe intracranial injuries and concurrent facial fractures [8]. These fractures are traditionally categorized as isolated anterior table fractures, combined anterior-posterior table fractures, or isolated posterior table fractures [9,10]. The absence of universally standardized FSF treatment protocols necessitates individualized management based on fracture characteristics, comminution severity, frontonasal duct integrity, neurological assessment, and cerebrospinal fluid leakage [11].
Paranasal sinus anatomy exhibits considerable inter-individual variation, emphasizing the importance of detailed imaging assessments. Computed tomography (CT) imaging, recognized since the 1990s as superior to plain radiography, is essential for preoperative planning, anatomical navigation during endoscopic surgery (FESS), and precise anatomical and volumetric evaluation [12,13]. High-resolution CT effectively identifies even minor fractures, distinguishing surgically relevant injuries from incidental findings in complex facial trauma cases [14]. Typical sinus measurements obtained via CT include craniocaudal, anteroposterior, mediolateral dimensions, and wall thicknesses [15]. Given the variability in sinus pneumatization, this study investigated the correlation between frontal and maxillary sinus volumes and the incidence and patterns of upper and middle third facial fractures using CT data.
2. Materials and Methods
This retrospective observational case-control study was conducted at Sri Ramachandra Institute of Higher Education and Research, Chennai, India. The study aimed to examine the relationship between paranasal sinus size and the incidence of facial fractures. Institutional Ethics Committee approval (Ref: CSP-III/25/MAR/19/190) was obtained from the university ethics board. The case group included adult patients (≥18 years) diagnosed with frontal sinus or unilateral zygomaticomaxillary complex (ZMC) fractures confirmed by computed tomography (CT). The control group consisted of patients who underwent facial CT imaging for indications unrelated to fractures, demonstrating intact frontal or maxillary sinuses. Controls were frequency-matched by age and sex to the cases. Patient data were collected retrospectively from departmental electronic records, noting demographic details, fracture diagnosis, and preoperative CT scans ranging from January 2019 to May 2025. Imaging was performed using a Phillips Brilliance helical CT scanner with a slice thickness of 0.67 mm. All images were reviewed using the Picture Archiving and Communications System (PACS) via Medsynapse CT imaging software (version 5.9). The inclusion criteria were patients aged ≥18 years with confirmed frontal or unilateral ZMC fractures by high-resolution CT (slice thickness ≤0.7 mm) and adequate image quality were included. Patients with bilateral sinus or pan-facial fractures, previous craniofacial surgery involving sinuses, pathological sinus conditions (e.g., tumours, chronic sinusitis), or incomplete clinical or imaging records were excluded. Sinus dimensions, including height (craniocaudal), depth (anteroposterior), and width (mediolateral), were measured on axial, coronal, and sagittal CT views. Sinus volume was calculated using a standardized cuboid approximation formula (0.5 × height × depth × width), validated against semi-automated segmentation methods in selected cases. The primary outcome was the difference in mean sinus volume (cm³) between fracture and control groups. Secondary outcomes involved comparisons of individual sinus dimensions and demographic correlations.
Statistical analysis was performed using IBM SPSS Statistics Version 27 (IBM Corp., Armonk, NY, USA). Data normality was assessed via the Shapiro–Wilk test. Continuous variables (sinus height, depth, width, and volume) were reported as mean ± standard deviation (SD). Differences in sinus dimensions and volumes between fracture (test) and non-fracture (control) groups were evaluated using unpaired t-tests. Cohen's d effect size assessed the magnitude of differences (≥0.70 indicating moderate to large effects). Multivariate linear regression analyzed associations between sinus volume (dependent variable) and independent variables (group, age, sex, height, depth, width), with regression coefficients (β), standard errors, 95% confidence intervals, and p-values reported. Significance was defined at p < 0.05, with p < 0.01 indicating high significance.
3. Results
3.1. Demographic and Morphometric Overview
This study included two cohorts: upper-third facial fractures involving the frontal sinus (n=47 test; n=52 control) and midfacial fractures involving the maxillary sinus (n=244 test; n=178 control). Mean ages were comparable across groups, with a notable male predominance (~90%). Frontal sinus dimensions were consistently larger in the fracture group, particularly in width (5.60 ± 0.6 cm test vs. 5.11 ± 0.7 cm control). Similarly, maxillary sinus dimensions were significantly greater in height (3.46 ± 0.4 cm vs. 3.26 ± 0.7 cm) and depth (3.91 ± 0.3 cm vs. 3.32 ± 0.7 cm), while width remained similar between groups.

Table 1.
Demographics and sinus dimensions (mean ± SD) in test and control groups.
| Frontal Sinus (Test) n = 47 |
Frontal Sinus (Control) n = 52 |
Maxillary Sinus (Test) n = 244 |
Maxillary Sinus (Control) n = 178 |
|
|---|---|---|---|---|
| Age (years) | 33.1 ± 11.5 | 38.4 ± 15.2 | 35.9 ± 13.1 | 32.2 ± 12.0 |
| Sex (% male) |
95.8% |
82.7% |
89.8% |
90.4% |
|
Height (CC, cm) |
2.66 ± 0.40 |
2.58 ± 0.40 |
3.46 ± 0.40 |
3.26 ± 0.70 |
|
Depth (AP, cm) |
1.50 ± 0.20 |
1.39 ± 0.30 |
3.91 ± 0.30 |
3.32 ± 0.70 |
|
Width (ML, cm) |
5.60 ± 0.60 |
5.11 ± 0.70 |
3.09 ± 0.50 |
3.12 ± 0.70 |
|
Volume (cm3) |
11.18 ± 2.59 |
9.14 ± 2.80 |
20.93 ± 4.63 |
16.87 ± 6.93 |
CC = craniocaudal; AP = anteroposterior; ML = mediolateral.
3.2. Intergroup Comparison of Sinus Volume
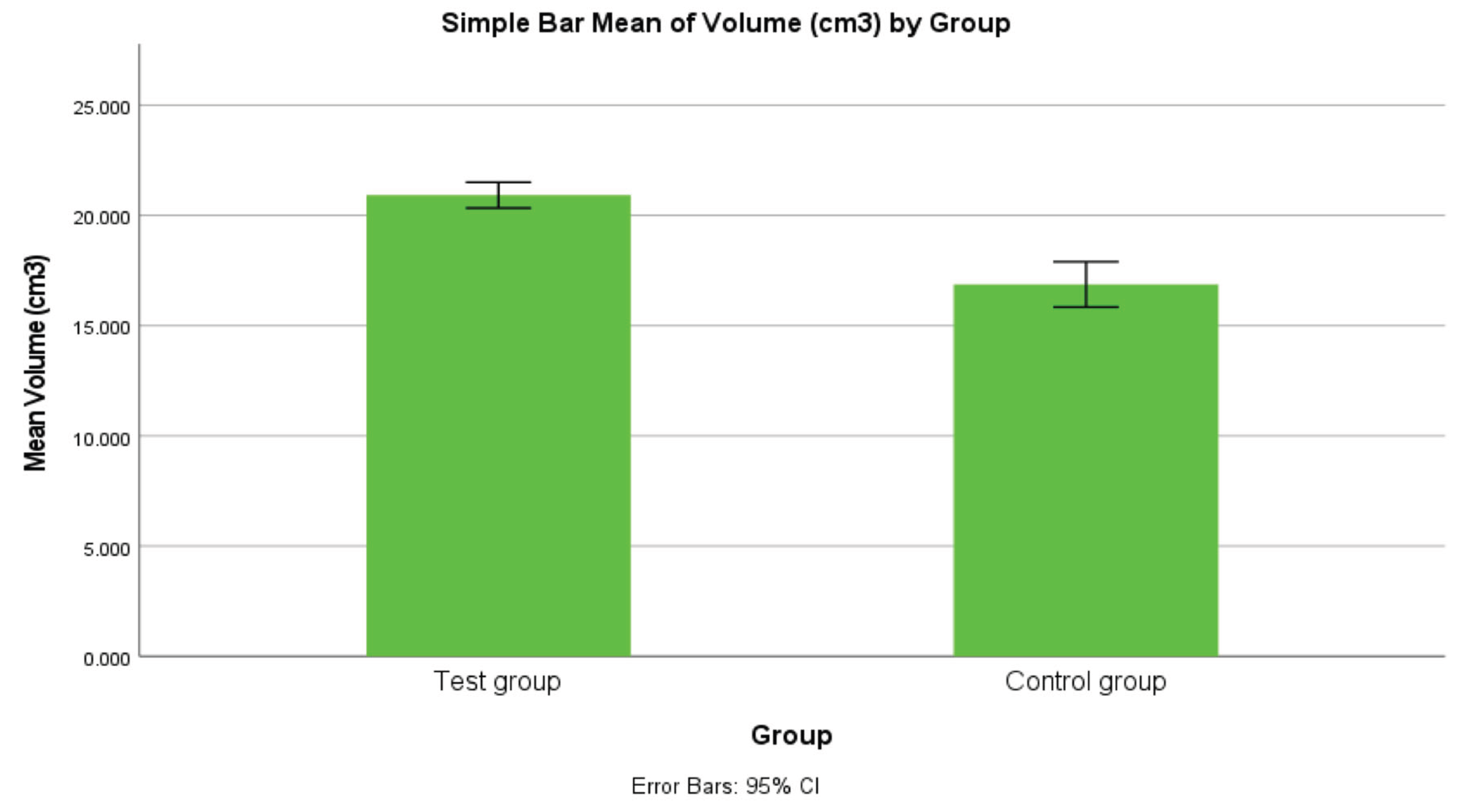
Frontal sinus volume was significantly higher in fracture patients compared to controls (11.18 ± 2.59 cm³ vs. 9.14 ± 2.80 cm³; p<0.001, Cohen’s d=0.754). Likewise, maxillary sinus volume showed a substantial difference between groups (20.93 ± 4.63 cm³ test vs. 16.87 ± 6.93 cm³ control; p<0.001, Cohen’s d=0.710). Thus, larger sinus volumes were strongly associated with facial fractures, more notably in the maxillary sinus cohort.
Table 2.
Intergroup comparison of frontal sinus volume (unpaired t-test).
| Group | Mean Volume (cm3) | SD | SE Mean | Cohen’s d | t | p-value |
|---|---|---|---|---|---|---|
| Test | 11.176 | 2.591 | 0.378 | 0.754 | 3.746 | < 0.001 ** |
| Control | 9.139 | 2.797 | 0.388 | – | – | – |
p < 0.05 significant; p < 0.01 highly significant.
3.3. Multivariate Regression Analysis
Regression analyses confirmed sinus height, depth, and width as significant predictors of sinus volume (all p<0.001). For frontal sinus volume, depth (β≈6.749), height (β≈3.660), and width (β≈1.591) positively predicted volume, while group membership, age, and sex showed no independent significance. Similarly, maxillary sinus volume strongly correlated with linear dimensions (height β=5.529, depth β=5.416, width β=5.994; all p<0.001), with no independent predictive value from group membership, age, or sex. Thus, anatomical differences, rather than demographic or fracture group status, fully explained the observed volume disparities. These findings highlight anatomical hyperpneumatization as a primary determinant of increased fracture susceptibility.
Table 3.
Intergroup comparison of maxillary sinus volume (unpaired t-test).
| Group | Mean Volume (cm3) | SD | SE Mean | Cohen’s d | t | p-value |
|---|---|---|---|---|---|---|
| Test | 20.926 | 4.633 | 0.297 | 0.710 | 7.198 | < 0.001 ** |
| Control | 16.872 | 6.929 | 0.519 | – | – | – |
p < 0.05 significant; p < 0.01 highly significant.
Table 4.
Multivariate linear regression for frontal sinus volume (dependent variable).
| Predictor | β Coefficient | Std. Error | 95% CI | p-value |
|---|---|---|---|---|
| Group (Test vs Control) | -0.180 | 0.108 | -0.394 to 0.034 | 0.099 |
| Age (Years) | +0.001 | 0.003 | -0.006 ro 0.008 | 0.724 |
| Sex (Female vs Male) | -0.103 | 0.161 | -0.422 to 0.217 | 0.525 |
| Height (cm) | +3.660 | 0.123 | 3.417 to 3.904 | < 0.001 ** |
| Depth (cm) | +6.749 | 0.173 | 6.405 to 9.093 | < 0.001 ** |
| Width (cm) | +1.591 | 0.076 | 1.440 to 1.742 | < 0.001 ** |
| (Constant) | -17.674 | 0.602 | -18.869 to -16.478 |
< 0.001 ** |
p < 0.05 significant; p < 0.01 highly significant.
Table 5.
Multivariate linear regression for maxillary sinus volume (dependent variable).
| Predictor | β Coefficient | Std. Error | 95% CI | p-value |
|---|---|---|---|---|
| Group (Test vs Control) | +0.063 | 0.134 | -0.200 to 0.327 | 0.637 |
| Age (Years) | +0.000 | 0.004 | -0.009 to 0.009 | 0.941 |
| Sex (Female vs Male) | +0.069 | 0.193 | -0.310 to 0.448 | 0.720 |
| Height (cm) | +5.529 | 0.107 | 5.319 to 5.739 | < 0.001 ** |
| Depth (cm) | +5.416 | 0.107 | 5.206 to 5.627 | < 0.001 ** |
| Width (cm) | +5.994 | 0.093 | 5.810 to 6.178 | < 0.001 ** |
| (Constant) | -37.914 | 0.649 | -39.190 to -36.639 | < 0.001 ** |
p < 0.05 significant; p < 0.01 highly significant.
Figure 1.
Bar graph comparing mean frontal sinus volumes (cm³) between groups. The test group (fracture patients) shows a higher average frontal sinus volume than controls (p < 0.001). The error bars (±1 SD) indicate some overlap in variability, but the notably taller bar for the test group illustrates the larger frontal aeration associated with upper-third facial fractures.
Figure 1.
Bar graph comparing mean frontal sinus volumes (cm³) between groups. The test group (fracture patients) shows a higher average frontal sinus volume than controls (p < 0.001). The error bars (±1 SD) indicate some overlap in variability, but the notably taller bar for the test group illustrates the larger frontal aeration associated with upper-third facial fractures.
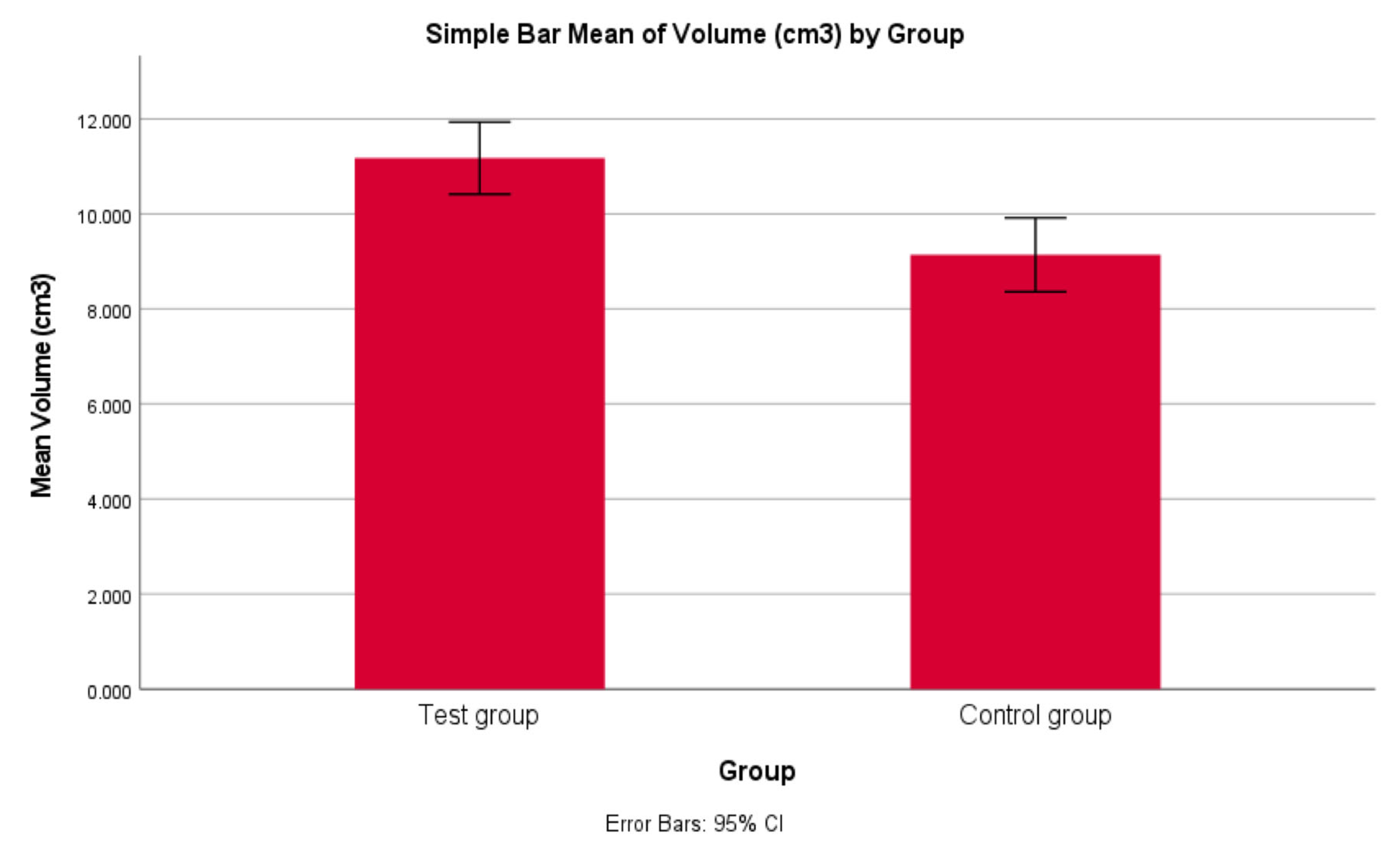
Figure 2.
Bar graph comparing mean maxillary sinus volumes (cm³) between groups. The test group exhibits a substantially greater maxillary sinus volume than the control group (p < 0.001). The difference in bar heights is evident, with the fracture group averaging ~20.9 cm³ versus ~16.9 cm³ in controls, reflecting the significant association between increased maxillary sinus pneumatization and midfacial fracture incidence.
Figure 2.
Bar graph comparing mean maxillary sinus volumes (cm³) between groups. The test group exhibits a substantially greater maxillary sinus volume than the control group (p < 0.001). The difference in bar heights is evident, with the fracture group averaging ~20.9 cm³ versus ~16.9 cm³ in controls, reflecting the significant association between increased maxillary sinus pneumatization and midfacial fracture incidence.
4. Discussion
This retrospective study demonstrated a clear relationship between increased frontal and maxillary sinus volumes and susceptibility to facial fractures of the upper and middle thirds. Our findings are consistent with previous studies, which suggest that extensive pneumatization compromises bone integrity, rendering the facial skeleton more vulnerable to traumatic fractures. Anatomically, larger sinus cavities correlate with thinner surrounding bone walls and increased surface area exposure, creating structural weaknesses during impact events [18].
Specifically, our frontal sinus findings concur with those reported by Buller et al. (2019), who highlighted a significantly elevated risk of anterior table fractures in patients with hyperpneumatized frontal sinuses. Their results indicated an increased likelihood of fracture occurrence in larger sinuses due to thinner anterior sinus walls [17]. The biomechanical underpinning for this association has been effectively demonstrated in finite element modeling by Pajic et al. (2017), who revealed that large sinuses act as structural "crumple zones". Under impact, the thinner anterior sinus wall fractures preferentially, absorbing traumatic energy and potentially reducing intracranial damage [19]. Further supporting this concept, Snyderman et al. found that larger frontal sinus volumes correlated with fewer brain contusions, suggesting a protective function through energy dissipation via sinus wall fractures [16]. However, this protective benefit has limitations, as excessively large sinuses can paradoxically increase trauma severity. Celiker et al. (2020) demonstrated increased mortality rates among patients with extremely pneumatized frontal sinuses, indicating an optimal sinus size range for effective trauma energy absorption and raising important considerations for trauma management and preventive measures [16,20].
For maxillary sinus fractures, our results align closely with those of Buller et al. (2023), who reported that sinus volumes exceeding roughly 20 cm³ significantly increased the risk of zygomaticomaxillary complex fractures [18]. The structural implications of an enlarged maxillary sinus—especially in its vertical dimension—result in thinner zygomatic buttresses, which inherently reduces resistance to trauma and predisposes the facial skeleton to fractures. Our multivariate regression analysis further confirmed the primacy of anatomical sinus dimensions, rather than demographic or trauma-specific factors, in predicting fracture susceptibility, reinforcing previous literature observations [21,22].
The clinical implications of recognizing the association between sinus size and facial fracture risk are significant. Clinicians can incorporate sinus volume assessments into risk stratification models, guiding preventive interventions such as tailored protective gear for high-risk individuals. In acute trauma scenarios, heightened suspicion and prompt evaluation for potential fractures may be warranted when imaging reveals large sinus cavities. Moreover, surgical treatment strategies can be optimized by accounting for sinus anatomy, potentially necessitating more aggressive interventions such as sinus obliteration or surgical exploration to mitigate chronic complications [18]. Additionally, sinus dimensions can serve as valuable forensic markers, aiding the interpretation of traumatic events and their mechanisms.
The retrospective nature of this study introduces potential selection bias and limits causal inference. Measurements derived post-trauma may be affected by fracture-related anatomical distortions. Detailed fracture severity classification and precise impact force data were unavailable, restricting a comprehensive evaluation of fracture mechanics. Furthermore, anatomical variations like sinus septae, cortical bone thickness, and bone mineral density were not assessed. Future studies should prospectively validate these findings, addressing these limitations with controlled biomechanical analysis and expanded demographic representation.
5. Conclusions
This study demonstrates a significant correlation between increased frontal and maxillary sinus volumes and the susceptibility to upper-third and midfacial fractures. Larger sinuses appear to structurally weaken facial bones, predisposing them to fractures under traumatic impacts. Recognizing the anatomical variability of sinus size can inform clinical risk assessment, guide preventive measures, and influence surgical management strategies in craniofacial trauma care.
Author Contributions
Conceptualization, Srinath Balakrishnan. and Naveen Kumar J.; methodology, Srinath Balakrishnan, Naveen Kumar J, Pandya Kalpa Mukul.; software, Srinath Balakrishnan, Rajeev P.; validation, Srinath Balakrishnan, Naveen Kumar J, Pandya Kalpa Mukul; formal analysis, Srinath Balakrishnan.; investigation, Srinath Balakrishnan.; resources, Srinath Balakrishnan, Rajeev P.; data curation, Srinath Balakrishnan, Pandya Kalpa Mukul.; writing—original draft preparation, Srinath Balakrishnan.; writing—review and editing, Srinath Balakrishna; visualization, Naveen Kumar J, Pandya Kalpa Mukul; supervision, Naveen Kumar J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Top, H.; Aygit, C.; Sarikaya, A.; Karaman, D.; Firat, M. F. Evaluation of maxillary sinus after treatment of midfacial fractures. Journal of Oral and Maxillofacial Surgery 2004, 62(10), 1229–1236. [Google Scholar] [CrossRef]
- Jiang, L.; Wu, M.; Li, H.; Liang, J.; Chen, J.; Liu, L. Risk Factors for Maxillary Sinus Pathology after Surgery for Midfacial Fracture: A Multivariate Analysis. J. Clin. Med. 2022, 11, 6299. [Google Scholar] [CrossRef]
- Shrestha, D.; Yadav, L.K.; Thapa, P. Chronic maxillary sinusitis: Clinical and microbiological evaluation. J. Coll. Med. Sci. 2011, 7, 17–22. [Google Scholar] [CrossRef]
- Ballon, A.; Landes, C.A.; Zeilhofer, H.F.; Herzog, M.; Klein, C.; Sader, R. The importance of the primary reconstruction of the traumatized anterior maxillary sinus wall. J. Craniofac. Surg. 2008, 19, 505–509. [Google Scholar] [CrossRef]
- Cengiz, M.; Celikbilek, G.; Andic, C.; Dosemeci, L.; Yilmaz, M.; Karaali, K.; Ramazanoglu, A. Maxillary sinusitis in patients ventilated for a severe head injury and with nostrils free of any foreign body. Injury 2011, 42, 33–37. [Google Scholar] [CrossRef]
- Pereira-Filho, V.A.; Gabrielli, M.F.; Gabrielli, M.A.; Pinto, F.A.; Rodrigues-Junior, A.L.; Klüppel, L.E.; Passeri, L.A. Incidence of maxillary sinusitis following Le Fort I osteotomy: Clinical, radiographic, and endoscopic study. J. Oral Maxillofac. Surg. 2011, 69, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, M.; Watanabe, M.; Yamamoto, M.; Narita, M.; Kamio, T.; Takaki, T.; Shibahara, T.; Katakura, A. Prognostic factors for maxillary sinus mucosal thickening following Le Fort I osteotomy: A retrospective analysis. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 12. [Google Scholar] [CrossRef] [PubMed]
- Stanwix, M. G.; Nam, A. J.; Manson, P. N.; Mirvis, S.; Rodriguez, E. D. Critical Computed Tomographic Diagnostic Criteria for Frontal Sinus Fractures. Journal of Oral and Maxillofacial Surgery 2010, 68(11), 2714–2722. [Google Scholar] [CrossRef]
- Gerbino, G; Roccia, F; Benech, A. Analysis of 158 frontal sinus fractures: Current surgical management and complica tions. J Craniomaxillofac Surg 2000, 28, 133. [Google Scholar] [CrossRef]
- Buller, J; Maus, V; Grandoch, A; Kreppel, M; Zirk, M; Zöller, JE. Frontal Sinus Morphology: A Reliable Factor for Classification of Frontal Bone Fractures? Journal of Oral and Maxillofacial Surgery 2018. [Google Scholar] [CrossRef]
- Larrabee, WF, Jr.; Travis, LW; Tabb, HG. Frontal sinus fractures— Their suppurative complications and surgical management. Laryngoscope 1980, 90, 1810. [Google Scholar] [CrossRef] [PubMed]
- White, PS; Robinson, JM; Stewart, IA; Doyle, T. Computerized tomography mini-series: an alternative to standard paranasal sinus radiographs. Aust N Z J Surg 1990, 60(1), 25–29. [Google Scholar] [CrossRef]
- Kawarai, Y; Fukushima, K; Ogawa, T; Nishizaki, K; Gunduz, M; Fujimoto, M; Masuda, Y. Volume quantification of healthy paranasal cavity by three dimensional CT imaging. Acta Otolaryngol Suppl 1999, 540, 45–49. [Google Scholar] [PubMed]
- Hopper, R. A.; Salemy, S.; Sze, R. W. Diagnosis of midface fractures with CT: what the surgeon needs to know; a review publication of the Radiological Society of North America, Inc: Radiographics, 2006; Volume 26, 3, pp. 783–793. [Google Scholar] [CrossRef]
- Sahlstrand-Johnson. : Computed tomography measurements of different dimensions of maxillary and frontal sinuses. BMC Medical Imaging 2011, 11, 8. [Google Scholar] [CrossRef] [PubMed]
- Yu, JL; Branstetter, BF, 4th; Snyderman, CH. Frontal sinus volume predicts incidence of brain contusion in patients with head trauma. J Trauma Acute Care Surg 2014, 76(2), 488–92. [Google Scholar] [CrossRef]
- Buller, J; Kreppel, M; Maus, V; Zirk, M; Zöller, JE. Risk of frontal sinus anterior table fractures after craniofacial trauma and the role of anatomic variations in frontal sinus size: A retrospective case- control study. J Craniomaxillofac Surg. 2019, 47(4), 611–615. [Google Scholar] [CrossRef]
- Buller, J; Bömelburg, C; Kruse, T; Zirk, M. Does maxillary sinus size affect the risk for zygomatic complex fractures? Clin Anat. 2023, 36(4), 564–569. [Google Scholar] [CrossRef]
- Pajic, SS; Antic, S; Vukicevic, AM; et al. Trauma of the frontal region is influenced by the volume of frontal sinuses: A finite element study. Front Physiol. 2017, 8, 493. [Google Scholar] [CrossRef]
- Celiker, M; Kanat, A; Ozdemir, A; et al. Controversy about the protective role of volume in the frontal sinus after severe head trauma: larger sinus equates with higher risk of death. Br J Oral Maxillofac Surg. 2020, 58(3), 314–318. [Google Scholar] [CrossRef]
- Montovani, Jair; Campos, Lígia; Gomes, Marina; Moraes, Vinícius; Ferreira, Fabricio; Nogueira, Emanuel. Etiology and incidence facial fractures in children and adults. Brazilian journal of otorhinolaryngology 2006, 72, 235–41. [Google Scholar] [CrossRef]
- Imtiaz, H.; Khattak, M. S.; Hayat, N. Q.; Jadoon, O.; Hussain, A.; Shaheen, S. Sex-Based Differences in Frontal Sinus Anatomy: A Cross-Sectional Study: Sex-Based Differences in Frontal Sinus Anatomy. Pakistan Journal of Health Sciences 2024, 5(08), 170–175. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



