
Submitted:
17 December 2025
Posted:
18 December 2025
You are already at the latest version
Abstract
Background/Objectives: Pre-eruptive intracoronal resorption (PEIR) in impacted or un-erupted teeth often remains un-diagnosed. The aim of this study was to investigate the prevalence of PEIR with the aid of cone-beam computed tomography (CBCT) and propose a new three-dimensional (3-D) classification for the analysis of the lesions. Methods: A total of 164 CBCT of non erupted teeth scans were examined for the presence of PEIR, tooth type, angulation and position. A novel 3-D classification system was proposed and all PEIR lesions were further classified. The classification system was used to stage PEIR lesions, according to their extend from the enamel level apically, the circumferential spread and their proximity to the pulp chamber. Descriptive statistics were used to assess the prevalence and type of resorption. The association between PEIR, demographics, tooth type, position and angulation were studied. The estimation of the multivariate relationship between PEIR, patient’s demographics and tooth characteristics was conducted with the multiple binary logistic regression model. Results: The prevalence of PEIR was 33.5%, affecting mostly maxillary canines, maxillary and mandibular molars. The prevalence of PEIR in ages over 45 years was significantly high (p < 0.001). The presence of PEIR was significantly associated with buccal position (p=0.002) and buccal angulation (p=0.016) of the tooth. Conclusions: Due to the high prevalence of PEIR, CBCT is essential for baseline recording and monitoring of the lesions. The 3-D classification index enables the early detection of PEIR and may critically affect decision-making in restorative, orthodontic and surgical treatment planning.
Keywords:
cone beam computed tomography
; impacted teeth
; pre-eruptive intracoronal resorption
; resorption
; un-erupted teeth
1. Introduction
Root resorption develops as a result of physiologic or pathologic loss of hard dental tissues, including dentin and cementum [1]. Broadly, there are two categories of resorption; external and internal root resorption. External root resorption manifests in various forms depending on histological and radiographic criteria, including surface, inflammatory, replacement, cervical and transient apical root resorption [1,2,3,4]. External cervical resorption (ECR) is a destructive process, which usually starts in the cervical region of the tooth, resulting in progressive loss of cementum and dentin by odontoclasts that resorb the dental hard tissue. [3,4].
Cone beam computed tomography (CBCT) improves the detection of ECR compared to conventional radiographs [5,6,7]. CBCT has been advocated by both the AAE and the ESE for the management of ECR [8,9]. Patel et al. proposed a three-dimensional (3D) classification for ECR, based on CBCT findings, assessing lesions by height, circumferential spread, and proximity to the pulp [10]. This classification is effective in accurate diagnosis, description of the extent and severity of the lesion.
ECR in impacted or unerupted teeth is also referred to as pre-eruptive intracoronal (PEIR) or intramural resorption [11,12,13,14]. Pre-eruptive intracoronal resorption (PEIR) is a rare condition characterized by a well-defined radiolucent lesion within pulpal or root dentine of impacted or unerupted teeth, as a result of dental hard tissues breakdown [15]. It is typically detected incidentally in panoramic (OPG) or bitewing (BW) radiographs with a tooth prevalence of 0.2-3.5% in permanent mandibular and maxillary molars respectively [16]. The histological findings of PEIR correspond to those of ECR, as in most case studies, the lesions consist of similar features, including inflammatory resorptive cells without evidence of microbial invasion, caries or pulp degeneration [17].
The two-dimensional observation of teeth and potentially existing lesions, as well as the inherent geometric distortion of such images, prompts for limited capacity to detect PEIR in impacted or unerupted maxillary teeth compared to mandibular ones [13]. The diagnostic limitations to detect PEIR are further subjected to the orientation and topography of the lesion, particularly if they do not manifest in mesio-distal axis or if they are not located in labial aspect.
Despite the aforementioned limitations of two-dimensional OPG and BW, the proposed classification by Seow et al., comprised of severity scores 1-3 [Score 1: within one third dentin thickness; Score 2: two-thirds dentin thickness; Score 3: extended through the full dentin thickness of the crown] has been widely adopted [11,16,18]. Yuksel et al. proposed an advanced fifteen-grade scoring system for the detection of PEIR, but it was still based on OPG [19]. Recent studies have highlighted that the use of CBCT improves accuracy in the detection of PEIR and provide a more detailed three-dimensional description of the resorptive lesions [12,14,20].
The prevalence of ECR has been reported to be 1 to 2.3%, however this is most probably an under-estimation as these studies are based on small field of view CBCT scans only [21,22]. The application of CBCT for the detection and prevalence calculation of PEIR was implemented in the retrospective studies of Demirtas et al. and Ngamsom et al., to overcome the limitations of two-dimensional imaging [12,14]. Despite the acknowledgement of the superior potential from the use of CBCT, they continued implementing the 1-3 scoring system and minor modifications, including a fourth and fifth grade of severity. However, no attempt was made to adjust their observations into a 3-D classification system, with a view to adequately assess the 3-D nature of PEIR. Therefore, it is well documented that PEIR in unerupted or impacted teeth is not included yet in the classification systems [23]. A new classification system is required to tight the gap in international guidelines to encompass conditions involving PEIR similar to external cervical root resorption (ECR), as both share common histological and radiographic characteristics.
The aim of the study was to investigate the prevalence of PEIR on impacted and unerupted teeth with the aid of CBCT, utilize data from the 3D evaluation and propose an international classification to describe the presence of external invasive resorptive lesions in impacted or un-erupted teeth.
2. Materials and Methods
Ethical approval for the study was obtained from the Bio-Ethics Committee of the School of Dentistry, Aristotle University of Thessaloniki, Greece {Date 29/1/2025 / (anonymized for referring purposes) Meeting with protocol number 26/29-01-2025). The retrospective study involved the evaluation of CBCT data obtained from dental patients referred to a private dental radiology center, in the province of Central Macedonia, Veroia, Greece, between September 2018 and February 2024, for the diagnostic justification of dento-alveolar and/or orofacial disease. Scans were acquired using a NewTom CBCT unit under high-resolution settings (90 kVp, 4 mA, 0.1 mm voxel size, 360° rotation), in accordance with the ALARA (As Low As Reasonably Achievable) principles.
The study population included individuals aged 22 to 82 years. Patients younger than 22 were excluded to ensure that the examined teeth had completed their pre-eruptive development. A tooth was defined as impacted when it was covered by bone and/or mucosa and remained below the occlusal plane. Patient demographic data, including age and sex, along with characteristics of the impacted teeth (tooth type, position, and angulation), were recorded.
All patients had non-contributory medical histories, with no systemic conditions (e.g., hyperparathyroidism or Paget’s disease, developmental dental anomalies, unerupted teeth associated with cysts, and benign or malignant tumors) known to affect dental hard tissue resorption. Furthermore, images characterized by inadequate quality, blurring, or other severe artifacts were excluded from the analysis.
A total of 1237 CBCT scans were examined for the presence of impacted teeth. Of these, 164 scans that included at least one unerupted tooth were recorded and selected for inclusion in the study. The type, angulation, and position of each impacted tooth were evaluated. Tooth angulation and position were categorized as mesio-angular, disto-angular, vertical, horizontal, bucco-version, linguo-version, or inverted.
The CBCT scans were assessed by three independent observers [EM, SP, KI], each with over 15 years of experience, using NNT Viewer software, in cross-sectional and multiplanar views (slice thickness: 0.125 mm), under standardized office and light conditions, on the same monitor (EIZO 24’’ MX243W RadiForce, 1350:1 contrast ratio). The observers were able to enhance the images freely by adjusting the radiographic contrast, brightness and magnification.
The presence of PEIR lesions was documented and compared among all three observers to ascertain the prevalence of lesions. A calibration process involved 10% of all subjects, which were randomly and independently selected by the author CG. Intra-examiner reliability was assessed over a period of 4 weeks, and any discrepancies were resolved, through a consensus meeting among all observers involved in this study. Inter-examiner reliability was further investigated, showing an intraclass correlation (ICC) value=1, indicating 100% agreement among the measurements.
In cases where a resorptive lesion was present, a modified classification of PEIR lesions was employed. The description and assignment of the degree of resorption was based on a modified version of the three-dimensional scoring system originally proposed by Patel et al. [2018], which was originally used to assess staging of cervical root resorption [10] [Figure 1]. This CBCT-based classification system is accurate for the detailed assessment of lesion size, extent, and location in three dimensions. The modified classification was used to stage lesions extending from the enamel to an apical extend (height), according to the circumferential spread (0–360°), and proximity to the pulp chamber [Figure 2].
The height (coronal-apical extent) of the lesion is graded according to its maximum vertical extension from the crown level to the cemento-enamel junction (CEJ) and apically within the root surface [coronal, middle or apical root third]. The height of the lesion can be best assessed by using the coronal and sagittal CBCT views.
Class 1: minor lesions occurring in the enamel, enamel-dentin junction [EDJ], or below EDJ, after focal resorption of enamel.
Class 2: the lesion extends to a larger area within dentin, mid-crown level, without approaching the pulp.
Class 3: the lesion extends and/or spreads in cervical crown level, at cemento-enamel junction (CEJ).
Class 4: Extension of resorptive lesion apical from CEJ, in mid- and/or apical root third.
The circumference of the lesion is graded according to its maximum spread within the crown or root surface and its best assessed using axial CBCT views.
A: <90o
B: >90o -<180o
C: >180o-<270o
D: >270o
The proximity of the lesion to the pulp chamber or the root canal can be best assessed using axial CBCT views.
d: Lesion confined to dentine
p: (Probable) pulpal involvement
3. Statistical Analysis
Inter-rater reliability was calculated with the Cohen’s kappa coefficient of agreement and in all cases the results showed almost perfect agreement. Descriptive analysis was conducted for the assessment of the prevalence of resorption as well as the prevalence of each of the classification levels within each type of tooth. The association between resorption and demographics, age (with five categories) and gender, as well as the association between resorption and patient’s characteristics, tooth type, position and angulation, were studied with either the Fisher’s Exact test for variables with two categories or the chi-square test for variables with more than two categories. The results of the latter test were considered reliable when the expected frequency in each cell of the cross-tabulation table was greater than 1. The estimation of the multivariate relationship between resorption and patient’s demographics and tooth characteristics was conducted with the multiple binary logistic regression model and the resulted odds ratios were presented with 95% confidence intervals. All statistics were produced with the R statistical language within the RStudio integrated environment, while the statistical significance was set at p<0.05.
4. Results
The 164 studied cases originated from 91 males, aged from 25 to 82, with an average age of 47.8 years and 73 females, aged from 25 to 83, with an average age of 52 years. The prevalence of PEIR, between 25 and 45 years, was low (12.9% and 17.1% respectively), while the prevalence was significantly higher in patients who were 45+ years (p < 0.001) [Figure 3]. The prevalence of PEIR was found 40.6% between 45 and 55 years, 47.2% between 55 and 70 and 53.8% between 70 and 90 years. Accordingly, in the multiple logistic regression model, age was classified in two categories, less than 45 and at least 45.
Regarding gender, the association was significant at the 10% level but not at the 5% level of significance, though it was observed that the prevalence of resorption in females was 33% greater that in males (27.5% in males and 41.1% in females) (p = 0.066) [Table 1].
No statistically significant association was observed between resorption and type of tooth (p = 0.326), however PEIR most commonly affected canines (40.9%), maxillary third molars (34.1%) and mandibular third molars (29.2%) [Figure 4].
Statistically significant results were found for tooth position, where the prevalence of the resorption in buccal position (69.6%)was found more than two times greater than the corresponding prevalence values in central (25.9%) and lingual/palatal (30.4%) [Table 1]. Moreover, the association between resorption and tooth angulation was also significant, with buccal orientated teeth showing the greater percentage of resorption cases (68.4%; almost two times greater than the other categories except for the category linguo-version for which the prevalence was equal to 50%) (p = 0.016) [Table 1].
The prevalence of the proposed 11 classification levels of resorption within each one tooth type is presented in Table 2. Taking into account the small sample size compared to the number of classification levels, it is worth noting the high prevalence value of the 1Ad level (21.6% or 19/88 teeth) in the maxillary third molars, whereas in almost all the other tooth types most of the classification levels observed with small, nearly homogeneous values (from 1.1% to 9.1%). Furthermore, no resorption was observed in mandibular canine and mandibular premolar tooth categories.
In Table 3, the results of the multiple binary logistic regression model are presented. When all other variables are kept constant, gender is not significant at the 5% level but is significant at the 10% level of significance (p=0.065). Keeping all other variables constant, the prevalence of resorption in ages 45 and older is four times higher individuals less than 45 years (OR = 4.036, 95% CI: 1.787 - 9.115, p < 0.001), while the prevalence of resorption in types Bucco-linguo-version are expected to be three times higher than in types Mesio – Disto angular (OR = 3.194, 95% CI: 1.149-8.877, p = 0.026).
5. Discussion
ECR in both erupted and un-erupted teeth is usually asymptomatic and diagnosed as an incidental finding [2,23]. Histological differences in the enamel structure between erupted and unerupted teeth are well documented [24]. Crown impaction may predispose for progressive enamel resorption [25]. Genetic, developmental or pathological conditions can further result in hypomineralisation and enamel hypoplasia, which may contribute to or be associated with the resorptive process [26]. A correlation has been found between patient age and dental follicle inflammation as the longer the follicular tissue remains embedded in bone, the higher the probability of an inflammatory reaction developing in the connective tissue [27].
In unerupted teeth, some potential predisposing factors associated with ECR such as trauma, history of orthodontic treatment, occlusal disorders or periodontal disease are absent. However, age-related changes in the dental follicle may further combine with close proximity to surrounding inflamed areas [e.g. deep periodontal pockets, retained deciduous teeth, endodontic lesions or sinus infections]. Additionally, increased pressure on unerupted teeth may cause the reduced enamel epithelium to differentiate, potentially activating resorptive cells that initiate dentin resorption [15]. Hypoxia has also been identified as a predisposing factor for root resorption [28,29]. It remains unclear whether unerupted teeth are affected through similar mechanisms to those observed under hypoxic conditions induced by orthodontic forces.
In our study, a total of 164 impacted and unerupted teeth were evaluated. Among these, 55 teeth exhibited PEIR, which was a prevalence of 33.5% (55/164). The likelihood of resorption increased with age, indicating the progressive nature of the phenomenon, with a significantly higher prevalence observed in the age group of 45–55 years and the focal entry of resorption was detected on all surfaces of impacted or unerupted teeth. Although no statistically significant association was found between resorption and the type of tooth, relatively high prevalence values were observed for maxillary canines, and mandibular and maxillary third molars. Ngamsom et al. detected a higher resorption rate (83%) and the angulation was not found to be statistically related to increased or decreased prevalence of PEIR [14]. In this study, specific characteristics of unerupted teeth, including their angulation and spatial orientation, showed a clear correlation with the prevalence of PEIR, as bucco-linguoversion was three times more frequently associated with resorption than mesio-distal angulation.
An issue concerning the methodology of the study, as well as the definition of an unerupted tooth, relates to the age groups included. The use of the term PEIR in younger age groups clearly refers to lesions in teeth that have not yet erupted, but their eruption may still occur before adulthood. The inclusion of mixed age groups may lead to confusion regarding the definition of PEIR and, consequently, affect statistical analysis.
Earlier studies using panoramic (OPG) and bitewing (BW) radiographs in pediatric populations, showed limited diagnostic value for detecting PEIR due to geometric distortion and anatomical noise [16,20,30]. More recent investigations have used CBCT in both adult and non-adult populations [12,14,31], but none applied a 3-D classification system to characterize resorptive defects. The existing ranking systems rely solely on the appearance of a lesion in two dimensions, without further three-dimensional assessment [14,16,17,20,32].
Therefore, one of the main objectives of this study was to bridge the existing gap of the 3D observation and the descriptive analysis of the lesion in three topographic co-ordinates, including height, circumferential spread and proximity to the pulp. Hence, a novel modification of the existing ECR classification index was proposed.
Several studies, attempted to calculate the overall prevalence of resorption in population samples [16,30,33]. The prevalence of PEIR reported by CBCT studies [12,14] was lower compared to the present study. Demirtas et al. reported a prevalence of PEIR 15,1% of teeth, with higher frequency in mandibular and maxillary molars [12]. Ngamsom et al. assessed 380 patients with 590 unerupted teeth in patients aged 7–69 years, and reported resorption in 76 patients (32 males, 44 females), with a subject prevalence of 20% [14]. In total, 80 teeth exhibited resorption, resulting in a tooth prevalence of 13.6%. It is important to note that the sample population in both studies included both adult and non-adult population [12,14]. Although a study based on OPG analysis reported no significant statistical differences in the occurrence of resorption between adults and non-adult populations, our findings indicate that age influences both the onset and the progression of resorption [34]. Hence, the exclusion of non-adult patients may improve the consistency and reliability of the analysis, as resorption may not yet have developed or progressed to detectable levels. Therefore, selecting adult patients ensures that all teeth, including third molars, can reasonably be considered unerupted, thereby avoiding misclassification.
The occurrence of external invasive resorption in unerupted teeth [PEIR], has not yet been categorized as a distinct clinical entity. The following criteria may be considered in the diagnosis of PEIR, including: [a], the use of CBCT for the detection and classification of the lesion; [b] the presence of a focal surface defect; [c] the presence of intact predentin layer of the pulp; and [d] the histopathological findings [23].
In clinical practice, PEIR should be easily differentially diagnosed from caries, due to the location of unerupted teeth and the lack of crown exposure in the oral cavity. In addition, early diagnosis of PEIR is contributory to treatment planning and risk factor management, especially in orthodontics when impacted canines require intervention, surgical exposure and orthodontic alignment. More particularly, considering the high prevalence of PEIR in impacted maxillary canines, the use of CBCT enables the clinicians to inspect tooth structural integrity and suitability for further treatment.
Surgical extraction of such teeth, when indicated, is more complex, due to the risk of crown fracture and the potential ankylosis that may co-exist in such cases. Finally, the early detection and diagnosis of PEIR is essential as far as tooth re-implantation or transplation procedures are concerned. Following tooth loss after trauma and especially in young ages, apart from the close inspection of external root and crown anatomy of candidate teeth for extraction and re-implantation, it is critical essential to inspect impacted teeth, for the presence of PEIR. It remains unknown whether a transitional biological process from PEIR to ECR may exist, soon after a tooth is transplanted in a functional position, intra-orally. Hence, the existence of undetected PEIR may compromise treatment outcomes, which in principle are of complex nature.
6. Conclusions
The occurrence of PEIR in impacted and un-erupted teeth is higher than is commonly perceived. The use of CBCT as a diagnostic improves the detection and diagnosis of PEIR. When PEIR is diagnosed, it is essential to record and monitor the progression of these lesions. The proposed 3-D classification enables the early detection of PEIR in impacted and un-erupted teeth and may critically affect decision-making in restorative, orthodontic and surgical treatment planning.
Author Contributions
Conceptualization, Emmanuel Mazinis and Konstantinos Ioannidis; Data curation, Emmanuel Mazinis, Konstantinos Ioannidis and Vassilis Karagiannis; Formal analysis, Konstantinos Ioannidis and Vassilis Karagiannis; Investigation, Emmanuel Mazinis, Konstantinos Ioannidis, Shanon Patel and Christos Gogos; Methodology, Emmanuel Mazinis, Konstantinos Ioannidis and Shanon Patel; Resources, Emmanuel Mazinis and Konstantinos Ioannidis; Software, Emmanuel Mazinis, Konstantinos Ioannidis and Vassilis Karagiannis; Supervision, Shanon Patel and Christos Gogos; Validation, Konstantinos Ioannidis, Shanon Patel and Christos Gogos; Visualization, Emmanuel Mazinis, Konstantinos Ioannidis and Shanon Patel; Writing – original draft, Emmanuel Mazinis and Konstantinos Ioannidis; Writing – review & editing, Emmanuel Mazinis, Konstantinos Ioannidis, Shanon Patel, Vassilis Karagiannis and Christos Gogos.
Funding
This research received no external funding
Institutional Review Board Statement
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Patel, S.; Saberi, N.; Pimental, T.; et al. Present status and future directions: Root resorption. Int. Endod. J. 2022, 55, 892–921. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Krastl, G.; Weiger, R.; et al. ESE position statement on root resorption. Int. Endod. J. 2023, 56, 792–801. [Google Scholar] [CrossRef] [PubMed]
- Mavridou, A.M.; Hauben, E.; Wevers, M.; et al. Understanding external cervical resorption in vital teeth. J. Endod. 2016, 42, 1737–1751. [Google Scholar] [CrossRef] [PubMed]
- Heithersay, G.S. Invasive cervical resorption. Endod. Topics 2004, 7, 73–92. [Google Scholar] [CrossRef]
- Patel, S.; Mavridou, A.M.; Lambrechts, P.; et al. External cervical resorption—Part 1: Histopathology, distribution and presentation. Int. Endod. J. 2018, 51, 1205–1223. [Google Scholar] [CrossRef]
- Patel, S.; Dawood, A.; Wilson, R.; Horner, K.; Mannocci, F. The detection and management of root resorption lesions using intraoral radiography and cone beam computed tomography: An in vivo investigation. Int. Endod. J. 2009, 42, 831–838. [Google Scholar] [CrossRef]
- Mazón, R.M.; Garcia-Font, M.; Doria, G.; Duran-Sindreu, F.; Abella, F. Influence of cone-beam computed tomography in clinical decision-making among specialists in external cervical resorption lesions: A before–after study. J. Endod. 2022, 48, 1121–1128. [Google Scholar] [CrossRef]
- American Association of Endodontists; American Association of Oral and Maxillofacial Radiology. Joint position statement: Use of cone beam computed tomography in endodontics—2015/2016 update.
- Patel, S.; Brown, J.; Semper, M.; Abella, F.; Manocci, F. European Society of Endodontology position statement: Use of cone beam computed tomography in endodontics. Int. Endod. J. 2019, 52, 1675–1678. [Google Scholar] [CrossRef]
- Patel, S.; Foschi, F.; Mannocci, F.; Patel, K. External cervical resorption: A three-dimensional classification. Int. Endod. J. 2018, 51, 206–214. [Google Scholar]
- Uzun, I.; Gunduz, K.; Canitezer, G.; Avsever, H.; Orhan, K. Prevalence and characteristics of pre-eruptive intracoronal resorption in permanent unerupted teeth: A multicentre study. Int. Endod. J. 2015, 48, 1069–1076. [Google Scholar] [CrossRef]
- Demirtas, O.; Tarim Ertas, E.; Dane, A.; Kalabalik, F.; Sozen, E. Evaluation of pre-eruptive intracoronal resorption on cone-beam computed tomography: A retrospective study. Scanning 2016, 38, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Gurdán, Z.; Balázs, D.; Pásti, D.; Fathi, M.; Maroti, P.; Kardos, K.; Pacheco, A.; Szalma, J. Pre-eruptive intracoronal resorption in orthodontic patients: A retrospective analysis of 3,143 patients. Heliyon 2023, 9, e18699. [Google Scholar] [CrossRef] [PubMed]
- Ngamsom, S.; Arayapisit, T.; Asavanamuang, P.; Anurakwongsri, R.; Sonthinane, K.; Kretapirom, K. Pre-eruptive intramural resorption in unerupted teeth: A cone-beam computed tomography evaluation of prevalence and related factors. Clin. Oral Investig. 2024, 28, 279. [Google Scholar] [CrossRef] [PubMed]
- Seow, W.K.; Hackley, D. Pre-eruptive resorption of dentin in primary and permanent dentitions: Case reports and review. Pediatr. Dent. 1996, 18, 67–71. [Google Scholar]
- Seow, W.K.; Wan, A.; McAllan, L.H. Prevalence of pre-eruptive dentin radiolucencies in permanent dentition. Pediatr. Dent. 1999, 21, 26–33. [Google Scholar]
- Kane, G.; Cash, A.; Seehra, J. Pre-eruptive coronal resorption of unerupted molars in orthodontic patients. J. Orthod. 2019, 46, 155–161. [Google Scholar] [CrossRef]
- Yildiz, F.N.; Pamukcu, U.; Altunkaynak, B.; Peker, I.; Arkaslan, Z.Z. Idiopathic coronal resorption in impacted permanent teeth and its relationship with age: Radiologic study. Eur. Oral Res. 2021, 55, 16–20. [Google Scholar] [CrossRef]
- Yüksel, H.T.; Türkmenoğlu, A.; Çelikkol, B.; Evirgen, S.; Gulsahi, K.; Gulsahi, A. Pre-eruptive intracoronal resorption of permanent dentition: A new classification and multidisciplinary study. Aust. Endod. J. 2023, 49, 162–169. [Google Scholar] [CrossRef]
- Demirtas, O.; Dane, A.; Yildirim, E. Comparison of cone-beam computed tomography and panoramic radiography in the assessment of pre-eruptive intracoronal resorption. Acta Odontol. Scand. 2016, 74, 636–641. [Google Scholar] [CrossRef]
- Irinakis, E.; Aleksejuniene, J.; Shen, Y.; Haapsalo, M. External cervical resorption: A retrospective case–control study. J. Endod. 2020, 46, 1420–1427. [Google Scholar] [CrossRef]
- Huang, J.; Walsh, R.M.; Witherspoon, D.E.; Khalighinejad, N.; Tam, E.C.; Jalali, P.; He, J. Prevalence, characteristics, and risk factors of external cervical resorption: A retrospective practice-based study. Clin. Oral Investig. 2023, 27, 5595–5604. [Google Scholar] [CrossRef]
- Mazinis, E.; Thomaidis, V. Cone-beam computed tomography evaluation of external invasive resorption of unerupted teeth: Three case reports. J. Endod. 2023, 49, 1747–1753. [Google Scholar] [CrossRef] [PubMed]
- Walsh, L.J.; Liewehr, F.R. Clinical and radiologic appearances of invasive cervical resorption. J. Endod. 2011, 37, 883–894. [Google Scholar]
- Palamara, J.; Phakey, P.P.; Rachinger, W.A.; Orams, H.J. Electron microscopy of enamel surfaces of unerupted and erupted human teeth. Arch. Oral Biol. 1980, 25, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Suda, N. Role of reduced enamel epithelium in root resorption. J. Oral Biosci. 2022, 64, 43–48. [Google Scholar] [CrossRef]
- Khorasani, S.N.; Samiezadeh, N. Histopathologic evaluation of the dental follicle of asymptomatic impacted third molars. Ann. Maxillofac. Surg. 2018, 8, 291–295. [Google Scholar]
- Krishnan, V.; Davidovitch, Z. Cellular, molecular and tissue-level reactions to orthodontic force. Am. J. Orthod. Dentofacial Orthop. 2006, 129, 469.e1–469.e32. [Google Scholar] [CrossRef]
- Iglesias-Linares, A.; Yañez-Vico, R.M. Molecular and genetic aspects of orthodontic root resorption. J. Oral Pathol. Med. 2010, 39, 588–597. [Google Scholar]
- Al-Batayneh, O.B.; AlTawashi, E.K. Pre-eruptive intra-coronal resorption of dentine: A review of aetiology, diagnosis and management. Eur. Arch. Paediatr. Dent. 2020, 21, 1–11. [Google Scholar] [CrossRef]
- Shimabukuro, K.; Konishi, M.; Wongratwanich, P.; et al. CBCT-based investigation of pre-eruptive intracoronal resorption prevalence. Odontology 2024, 112, 256–263. [Google Scholar] [CrossRef]
- Manmontri, C.; Mahasantipiya, P.M.; Chompu-Inwai, P. Pre-eruptive intracoronal radiolucencies: Detection and nine-year monitoring. Case Rep. Dent. 2017, 2017, 6261407. [Google Scholar]
- Uzun, I.; Gunduz, K.; Canitezer, G.; Avsever, H.; Orhan, K. Pre-eruptive intracoronal resorption in permanent unerupted teeth: Multicentre study. Int. Endod. J. 2015, 48, 1069–1076. [Google Scholar]
- Umansky, M.; Tickotsky, N.; Friedlander-Barenboim, S.; Moskovitz, M. Age-related prevalence of pre-eruptive intracoronal radiolucent defects in permanent teeth. J. Clin. Pediatr. Dent. 2016, 40, 103–106. [Google Scholar] [CrossRef]
Figure 1.
The novel classification system of PEIR based on 3D assessment of lesion size and probable pulpal involvement.
Figure 1.
The novel classification system of PEIR based on 3D assessment of lesion size and probable pulpal involvement.
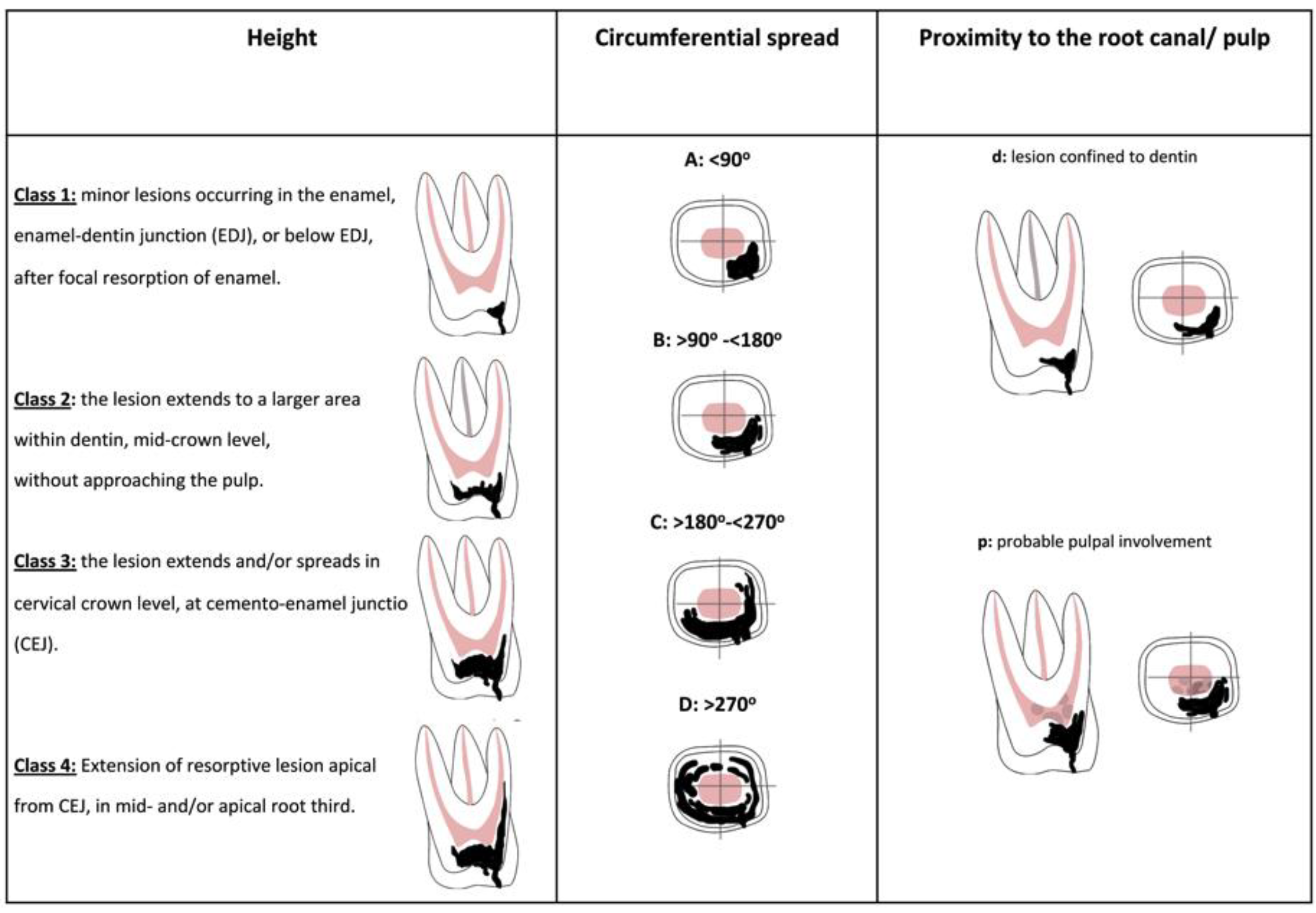
Figure 2.
CBCT images of various types of PEIR according to novel classification.
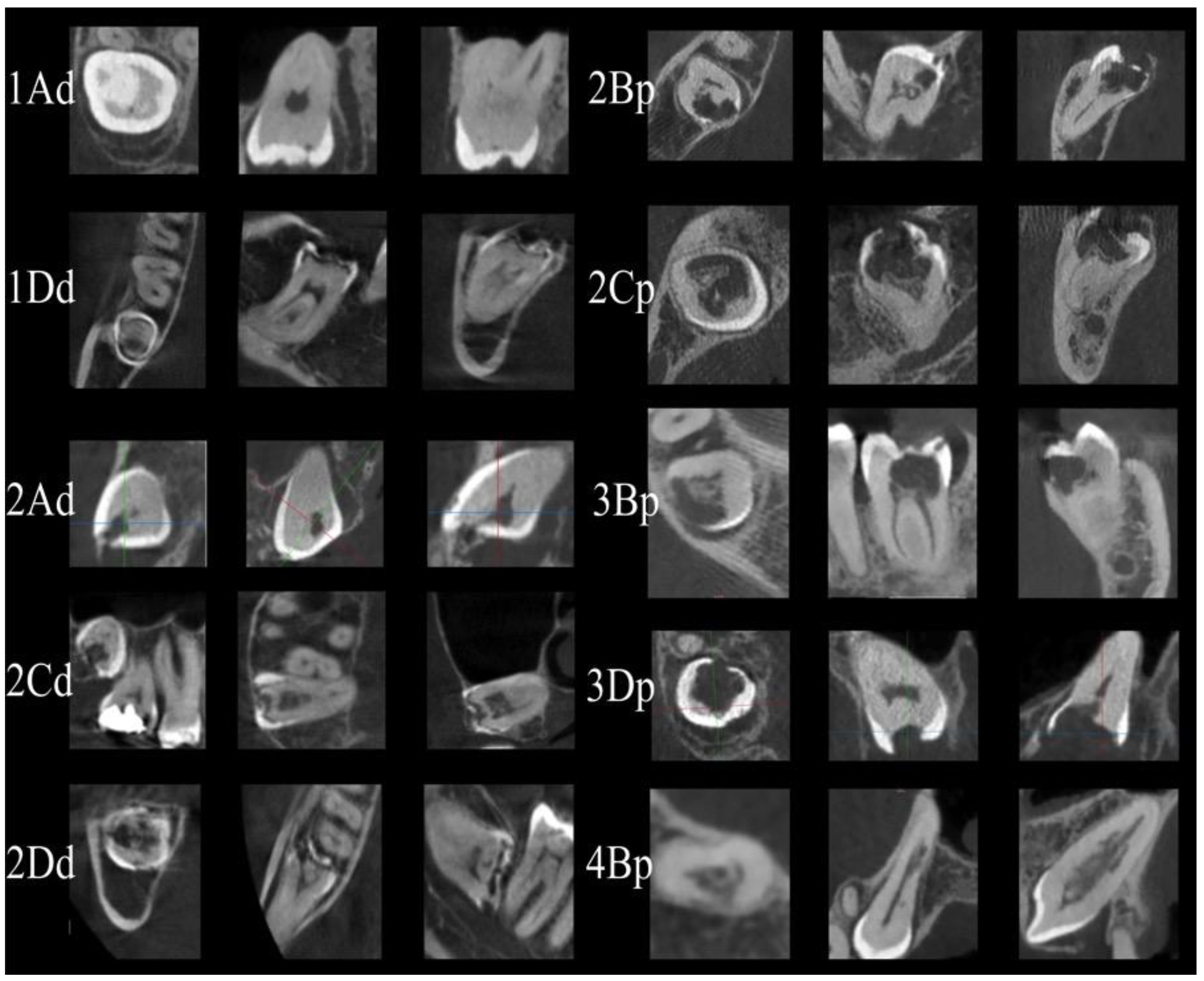
Figure 3.
Prevalence of RESORPTION within AGE categories, N = 164 cases.
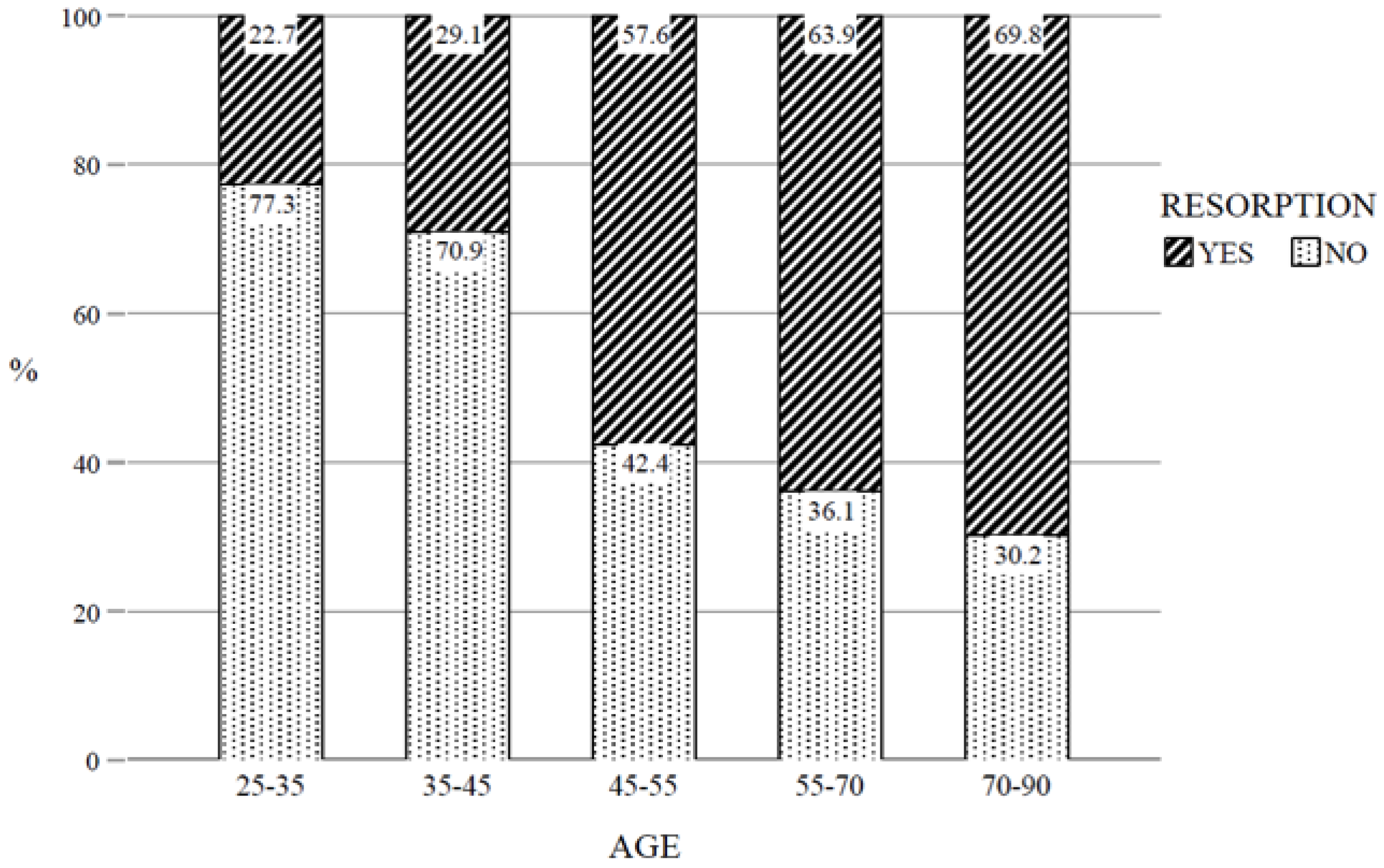
Figure 4.
Prevalence of RESORPTION for each TYPE OF TOOTH, N = 164 cases.
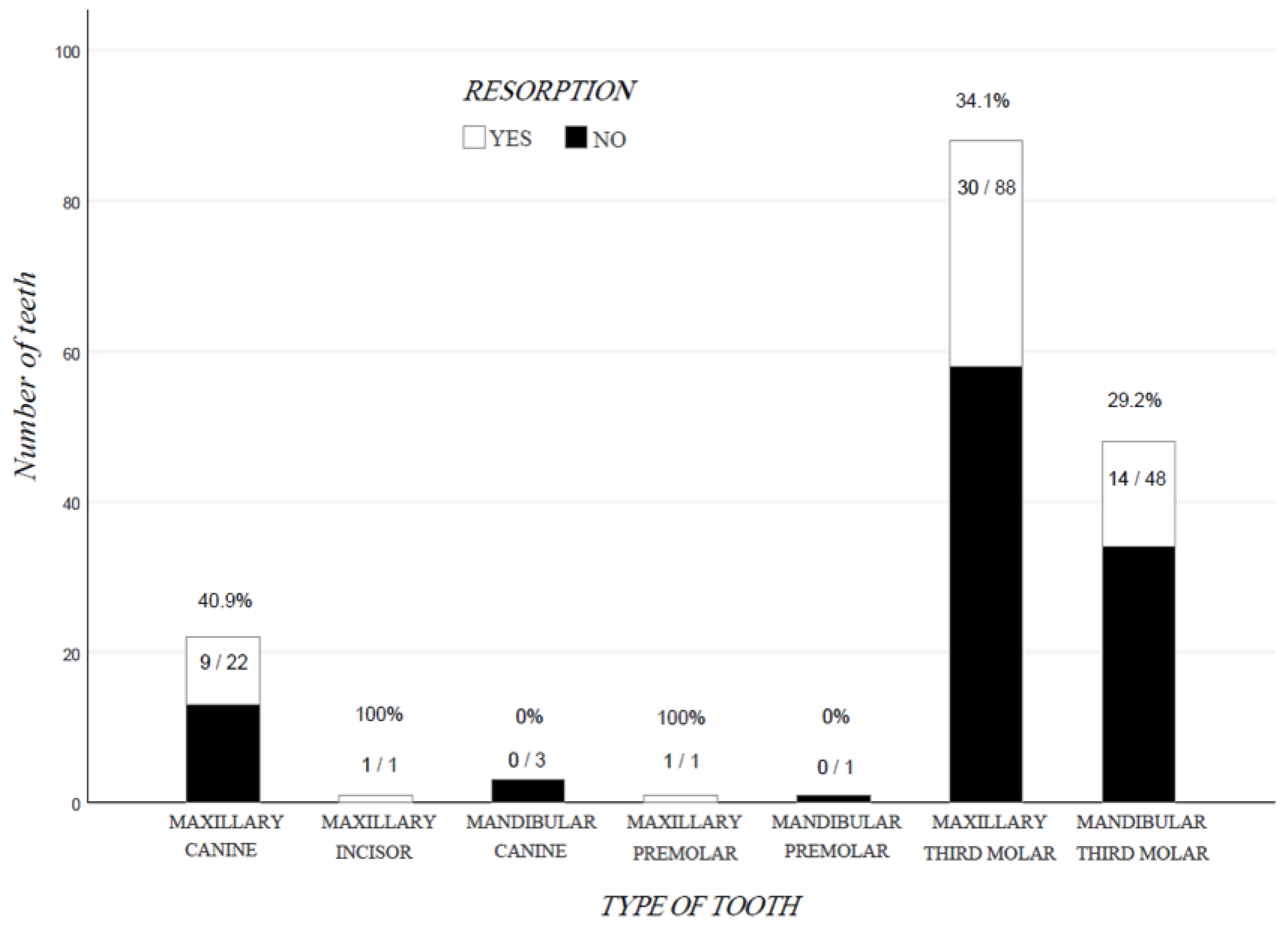

Table 1.
The frequency, distribution of RESORPTION within patients’ demographics as well as within the tooth characteristics TOOTH TYPE, POSITION and ANGULATION and the corresponding p-values from the association tests between RESORPTION and each one of the mentioned variables.
Table 1.
The frequency, distribution of RESORPTION within patients’ demographics as well as within the tooth characteristics TOOTH TYPE, POSITION and ANGULATION and the corresponding p-values from the association tests between RESORPTION and each one of the mentioned variables.
| RESORPTION | ||||||
|---|---|---|---|---|---|---|
| YES | NO | |||||
| N | % | N | % | P-value | ||
| AGE | 25-35 | 4 | 12.9 | 27 | 87.1 | |
| 35-45 | 6 | 17.1 | 29 | 82.9 | ||
| 45-55 | 13 | 40.6 | 19 | 59.4 | ||
| 55-70 | 25 | 47.2 | 28 | 52.8 | ||
| 70-90 | 7 | 53.8 | 6 | 46.2 | 0.001a | |
| GENDER | MALE | 25 | 27.5 | 66 | 72.5 | |
| FEMALE | 30 | 41.1 | 43 | 58.9 | 0.066b (NS) | |
| TYPE OF TOOTH | MAXILLARY CANINE | 9 | 40.9 | 13 | 59.1 | |
| MAXILLARY INCISOR | 1 | 100.0 | 0 | 0 | ||
| MANDIBULAR CANINE | 0 | 0 | 3 | 100.0 | ||
| MAXILLARY PREMOLAR | 1 | 100.0 | 0 | 0 | ||
| MANDIBULAR PREMOLAR | 0 | 0 | 1 | 100.0 | ||
| MAXILLARY THIRD MOLAR | 30 | 34.1 | 58 | 65.9 | ||
| MANDIBULAR THIRD MOLAR | 14 | 29,2 | 34 | 70,8 | 0.326a,c (NS) | |
| POSITION | CENTRAL | 29 | 25.9 | 83 | 74.1 | |
| BUCCAL | 16 | 69.6 | 7 | 30.4 | ||
| LINGUAL / PALATAL | 7 | 30.4 | 16 | 69.6 | ||
| MESIAL | 1 | 50.0 | 1 | 50.0 | ||
| DISTAL | 2 | 50.0 | 2 | 50.0 | 0.002a,c | |
| ANGULATION | MESIOANGULAR | 14 | 25.9 | 40 | 74.1 | |
| DISTOANGULAR | 6 | 31.6 | 13 | 68.4 | ||
| HORIZONTAL | 5 | 38.5 | 8 | 61.5 | ||
| VERTICAL | 10 | 23.3 | 33 | 76.7 | ||
| BUCCOVERSION | 13 | 68.4 | 6 | 31.6 | ||
| LINGUOVERSION | 6 | 50.0 | 6 | 50.0 | ||
| INVERSION | 1 | 25.0 | 3 | 75.0 | 0.016a | |
a: Chi-Square Test, b: Fisher’s Exact Test, c: Minimum Expected Count < 1 was found, NS: Not Significant.
Table 2.
Prevalence of CLASSIFICATION levels within each type of teeth (cases which were classified ‘NO RESORPTION’ are not displayed).
Table 2.
Prevalence of CLASSIFICATION levels within each type of teeth (cases which were classified ‘NO RESORPTION’ are not displayed).
| TYPE OF TOOTH | CLASSIFICATION | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IAd | IDd | IIAd | IIBd | IIBp | IIDp | IIIBp | IIICp | IIIDp | IIIDd | IVBp | Total | ||
| MAXILLARY CANINE | N | 1 | 0 | 2 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 2 | 22 |
| % | 4.5% | 0.0% | 9.1% | 4.5% | 0.0% | 0.0% | 0.0% | 4.5% | 4.5% | 4.5% | 9.1% | 100% | |
| MAXILLARY INCISOR | N | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| % | 0% | 0% | 0% | 100% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 100% | |
| MANDIBULAR CANINE | N | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3 |
| % | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 100% | |
| MAXILLARY PREMOLAR | N | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| % | 100% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 100% | |
| MANDIBULAR PREMOLAR | N | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| % | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 100% | |
| MAXILLARY THIRD MOLAR | N | 19 | 0 | 1 | 2 | 1 | 0 | 1 | 2 | 4 | 0 | 0 | 88 |
| % | 21.6% | 0.0% | 1.1% | 2.3% | 1.1% | 0% | 1.1% | 2.3% | 4.5% | 0% | 0% | 100% | |
| MANDIBULAR THIRD MOLAR | N | 4 | 1 | 1 | 0 | 1 | 2 | 0 | 1 | 4 | 0 | 0 | 48 |
| % | 8.3% | 2.1% | 2.1% | 0% | 2.1% | 4.2% | 0% | 2.1% | 8.3% | 0% | 0% | 100% | |
| Total | N | 25 | 1 | 4 | 4 | 2 | 2 | 1 | 4 | 9 | 1 | 2 | 164 |
| % | 15.2% | 0.6% | 2.4% | 2.4% | 1.2% | 1.2% | 0.6% | 2.4% | 5.5% | 0.6% | 1.2% | 100% | |
Table 3.
Odds Ratios with 95% CI, that resulted from the multiple binary logistic regression model with RESORPTION as the response and patients’ demographics and tooth characteristics as the predictors.
Table 3.
Odds Ratios with 95% CI, that resulted from the multiple binary logistic regression model with RESORPTION as the response and patients’ demographics and tooth characteristics as the predictors.
| B | S.E. | Wald | df | Odds Ratio (OR) | 95% C.I. for OR | |||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | p-value | ||||||
| GENDER | ||||||||
| Female | 1 | Reference | ||||||
| Male | -.699 | .379 | 3.410 | 1 | .497 | .237 | 1.044 | .065 |
| AGE | ||||||||
| Less than 45 | 1 | Reference | ||||||
| 45 and older | 1.395 | .416 | 11.264 | 1 | 4.036 | 1.787 | 9.115 | <.001 |
| TOOTH TYPE | ||||||||
| Posterior | 1 | Reference | ||||||
| Anterior | .452 | .558 | .657 | 1 | 1.571 | .527 | 4.688 | .418 |
| ANGULATION | ||||||||
| Mesio – Disto angular | 1 | Reference | ||||||
| Horizontal-vertical | .099 | .429 | .053 | 1 | 1.104 | .476 | 2.562 | .817 |
| Bucco-linguoversion | 1.161 | .522 | 4.956 | 1 | 3.194 | 1.149 | 8.877 | .026 |
| Inversion | -.890 | 1.604 | .308 | 1 | .411 | .018 | 9.519 | .579 |
| POSITION | ||||||||
| Buccal-lingual | 1 | Reference | ||||||
| Central | -.734 | .495 | 2.197 | 1 | .480 | .182 | 1.267 | .138 |
| Mesial-distal | .568 | 1.289 | .194 | 1 | 1.765 | .141 | 22.069 | .659 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



