
Submitted:
16 December 2025
Posted:
17 December 2025
You are already at the latest version
Abstract
In this review, we examine boron-containing agents for boron neutron capture therapy (BNCT) with a focus on absorption, distribution, metabolism, excretion and toxicity (ADMET) and model-informed design. BNCT is a binary radiotherapeutic modality in which high linear energy transfer particles are generated in the vicinity of ^10B, ideally within boron-loaded tumour cells, so the therapeutic outcome depends critically on the pharmacokinetics and biodistribution of boron carriers. We survey low-molecular-weight compounds, peptide conjugates, polymeric and nanostructured platforms and cell-based vectors, and discuss how physicochemical properties, transporter engagement and nano–bio interactions govern tumour uptake, subcellular localisation and normal-tissue exposure. We also describe a shift from maximising boron content towards optimising exposure profiles using positron emission tomography (PET), physiologically based pharmacokinetic (PBPK) modelling and in silico ADMET tools to define irradiation windows. Classical agents such as boronophenylalanine (BPA) and sodium borocaptate (BSH) are contrasted with newer polymeric and metallacarborane-based carriers, with attention to brain penetration, endosomal escape, linker stability, biodegradation and elimination routes, as well as platform-specific toxicities. We argue that further progress in BNCT will depend on integrating imaging-derived kinetics with PBPK-informed dose planning and engineering subcellularly precise yet degradable carriers, and that ADMET-guided design and spatiotemporal coordination are central to achieving reproducible clinical benefit from BNCT’s spatial selectivity.
Keywords:
boron neutron capture therapy
; BNCT
; ADMET
; physiologically based pharmacokinetic modelling
; boron delivery
; nanomedicine
; metallacarborane
; dose planning
1. Introduction
Boron Neutron Capture Therapy (BNCT) is a binary radiotherapeutic modality [1,2,3]predicated on the nuclear reaction between boron-10 (^10B) and low-energy thermal neutrons. The interaction produces high linear energy transfer (LET) α-particles and lithium-7 (^7Li) nuclei with path lengths of approximately 5–9 μm—comparable to a single cell diameter—thus confining cytotoxicity to boron-loaded tumour cells and sparing adjacent healthy tissues. This spatial selectivity, not achievable with conventional external beam radiotherapy, offers advantages in recurrent or otherwise inoperable malignancies [4,5], notably glioblastoma, head-and-neck cancers, and melanoma.
Clinical success depends critically on the ADMET profile of boron-containing agents [6,7]. To achieve selective tumour ablation, approximately 20–35 μg of ^10B per gram of tumour tissue is required, with a tumour-to-normal tissue (T/N) ratio exceeding ~3 and a tumour-to-blood (T/B) ratio sufficiently high at the time of irradiation [2,8,9]Accordingly, chemical design, biodistribution, metabolism, and elimination must be co-optimised within the ADMET framework.
1.1. Historical Overview and Clinical Progress
Since the early clinical explorations at Brookhaven in the 1950s, several generations of boron delivery agents have emerged. The benchmarks—boronophenylalanine (BPA) and sodium borocaptate (BSH)—remain reference standards owing to known clinical pharmacokinetics and safety, albeit with limited tumour selectivity and suboptimal retention. BPA relies on LAT1 transport and shows heterogeneous uptake; BSH distributes largely extracellularly with minimal active transport [1,10,11,12]. The monograph by Sauerwein et al. (2012) integrated biokinetics with clinical translation and catalysed subsequent rational design [1]. Parallel advances in synthetic boron chemistry—particularly metallacarborane-modified nucleosides and DNA-intercalating constructs—have expanded the scope of agents combining high boron payloads with favourable biophysics [13,14,15].
1.2. Emergence of ADMET-Guided Design
Historically, optimisation prioritised bulk boron concentration over pharmacokinetic metrics. Contemporary programmes integrate quantitative PK, dynamic imaging (PET/MRI), and computation to predict tissue penetration and retention [3,7,14]. For example, nanocarriers—PEGylated liposomes, boronated dendrimers and mesoporous silica nanoparticles—are engineered to exploit the EPR effect, typically improving tumour exposure versus small molecules [3,15,16]. PEGylation prolongs systemic residence and can markedly lengthen apparent half-life relative to free BPA, improving synchronisation between peak tumour concentrations and neutron exposure [15,17].
1.3. Molecular Classes of Boron-Containing Agents
Boron agents for BNCT may be grouped into: (1) low-molecular-weight compounds (e.g., BPA, BSH, boronated nucleosides) [10,11,14]; (2) peptide-based conjugates (e.g., EGFR or integrin-targeted) [14,18,19]; (3) polymeric carriers (e.g., PAMAM dendrimers, PEGylated borates) [15,16,17]; (4) nanostructured materials (e.g., boron nitride nanotubes, liposomes, hybrid nanogels); and [20,21,22](5) bio-cellular delivery systems (e.g., macrophages or stem cells) [18,21,23]. Each class exhibits distinct ADMET trade-offs: low-molecular-weight agents permeate rapidly but clear renally; polymeric/nanoparticulate systems extend circulation and improve EPR-mediated accumulation yet raise questions of biodegradation and long-term safety; cellular carriers provide pathophysiological homing, including into hypoxic regions, at the expense of higher biological variability [14,23,24].
1.4. European Contributions with Emphasis on Poland
European groups have played a pivotal role in metallacarborane chemistry and BNCT pharmacology. Work led from Łódź and collaborating Polish institutions reported metallacarborane intercalators and boronated nucleosides with balanced lipophilicity (logP ≈ 2–3) and high chemical stability, translating into improved cellular retention in preclinical models [25,26]. Polish investigators have also demonstrated macrophage-mediated delivery of boron carbide nanoparticles, achieving homing into poorly perfused tumour regions and sustained intratumoural presence. Across Europe, teams in Finland and Italy advanced hybrid polymer–silica carriers that enable imaging-guided delivery and controlled release. Collectively, these efforts illustrate a shift from merely maximising bulk boron to ADMET-guided optimisation of exposure, selectivity and subcellular localisation [13,14,15,21,23,24,27]. These advances in boron chemistry are paralleled by the establishment of dedicated BNCT infrastructure at the MARIA research reactor in Poland, enabling preclinical radiobiological studies [28].
1.5. Aim and Structure of the Review
This review provides an ADMET-centred analysis of boron-containing compounds and carriers relevant to BNCT, correlating chemical structure with PK parameters (t_½, CL, V_d), biodistribution, metabolic fate and toxicity. The review is organised by the five ADMET pillars, each supported by representative data, mechanistic considerations, and literature cross-references.
2. Absorption
Efficient absorption and systemic bioavailability are prerequisites for achieving therapeutic intratumoural ^10B at irradiation. Key determinants include molecular weight, lipophilicity (logP), solubility, ionisation, and membrane permeability. The principal challenge is to maximise tumour selectivity while securing sufficient exposure to deliver high T/B ratios at the time of neutron capture [2,3,7,14,24]. Table 1 (revised), “ADMET Parameters Related to Absorption of Representative Boron-Containing Compounds”, summarises key ADMET parameters discussed in this section. Foundational ADMET principles relevant to this section include classical drug-likeness and permeability heuristics, as well as the BCS framework[29,30,31,32]. Transporter effects, which modulate apparent absorption beyond passive diffusion, are reviewed by the International Transporter Consortium and recent clinical DDI methodology work [33]. Complementary BNCT-focused overviews of boron-agent classes further contextualise absorption behaviour [34,35,36]. A concise platform-level overview of absorption-relevant properties across boron classes is provided in [23]. Additional class-level insights relevant to uptake and formulation are provided by reviews on CA IX-targeted boron scaffolds, single-boron pharmacophores, and sugar-based/PEGylated PET-tracers [19,37,38,39].
2.1. Physicochemical Determinants
Key small-molecule carriers such as BPA and BSH exemplify the trade-off between permeability and selectivity. Optimising logP in the range ~2–3 while maintaining aqueous compatibility tends to favour transmembrane passage and endocytic uptake, especially when carborane motifs are balanced by polar linkers [13,14,15,59]. Hydrogen-bond donors/acceptors, steric compactness and charge state at physiological pH collectively determine LAT1 engagement and passive diffusion [10].
BPA, an amino-acid analogue, engages LAT1, overexpressed in multiple tumours, yet its low passive permeability (logP ≈ −1.2) constrains diffusion [14]. BSH (logP ≈ −4.8) is highly hydrophilic, exhibits minimal membrane permeability and undergoes rapid renal elimination, limiting tumour accumulation [11,12]. Incorporation of carborane/metallacarborane motifs increases lipophilicity (often to logP 2–3) and can enhance passive and endocytic uptake without forfeiting aqueous compatibility when combined with polar linkers [13,14,15,60]. Reports of DNA-intercalating metallacarboranes document greater cellular uptake than BPA with sustained intracellular retention in vitro [13,14,61].
For peptide and ligand-decorated constructs, avidity effects and receptor cycling kinetics set the ceiling for maximal cellular uptake. Endosomal escape can be engineered via pH-labile linkers or membrane-active segments to avoid lysosomal sequestration and degradation [15,21]. For cell-mediated delivery, macrophage homing into hypoxic regions provides access to poorly perfused compartments that are otherwise difficult for small molecules to reach [23,24].
2.2. Absorptive Pathways
Absorptive pathways comprise active transport (e.g., LAT1 for BPA; nucleoside transporters for boronated nucleosides) and passive diffusion; peptide conjugates exploit receptor-mediated endocytosis (e.g., EGFR, α_vβ_3) [10,14,18]. Nanoparticles and polymers enter predominantly via clathrin/caveolin-mediated endocytosis with subsequent endosomal trafficking; design solutions include pH-labile linkers and membrane-disruptive elements to promote endosomal escape [15,21,22,62]. Cellular vectors such as macrophages or MSCs function as cellular carriers, traversing barriers and releasing cargo within the tumour microenvironment[23,24].
2.3. Quantitative Considerations
Small-molecule BPA typically achieves rapid plasma peaks with short biological half-life, whereas PEGylated liposomes and related platforms reach higher C_max and substantially longer t_½, consistent with reduced opsonisation and RES uptake [15,63]. PET using ^18F-BPA-fructose (FBPA-Fr) supports clinically relevant tumour-to-normal brain uptake ratios around 2–3+ in glioma patients, aligning PET readouts with boron analyses from surgical samples [8,9,64].
2.4. Strategies to Enhance Absorption
Approaches include: prodrugging to transiently increase lipophilicity; PEGylation to extend circulation and leverage EPR; nano-engineering particle sizes ~50–150 nm for endothelial permeability–stability balance; biological carriers for hypoxia-directed uptake; and co-administration with permeation enhancers to augment transmembrane transport [14,15,21,22,63]
2.5. Key Insights
3. Distribution
Physiologically based pharmacokinetic (PBPK) approaches linking time-varying boron concentrations to dose kernels are increasingly used to synchronise irradiation with peak tumour-to-blood ratios [64]. PEGylation reduces opsonisation and reticuloendothelial uptake, prolonging the terminal half-life and enabling more predictable exposure windows [15,63]. See Table 2 for a concise summary of key ADMET parameters discussed in this section. Distribution behaviour is strongly shaped by transporter expression, protein binding and tissue barriers; contemporary ITC guidance and transporter-centric clinical designs provide the broader context for interpreting BNCT carriers [33]. For distribution and selectivity across contemporary agent classes, recent BNCT reviews and clinical guidance are informative [34,35,65]. Early animal work on borylated ferrocenium derivatives provides additional context on organ distribution and handling [66] Class-level distribution and selectivity considerations are summarised in [23]. Distribution and targeting considerations are further illustrated by carborane-containing polymers, BODIPY imaging scaffolds, and organotrifluoroborate conjugates [11,57,67,68,69,70,71] .
3.1. Pharmacokinetic Determinants and Modelling
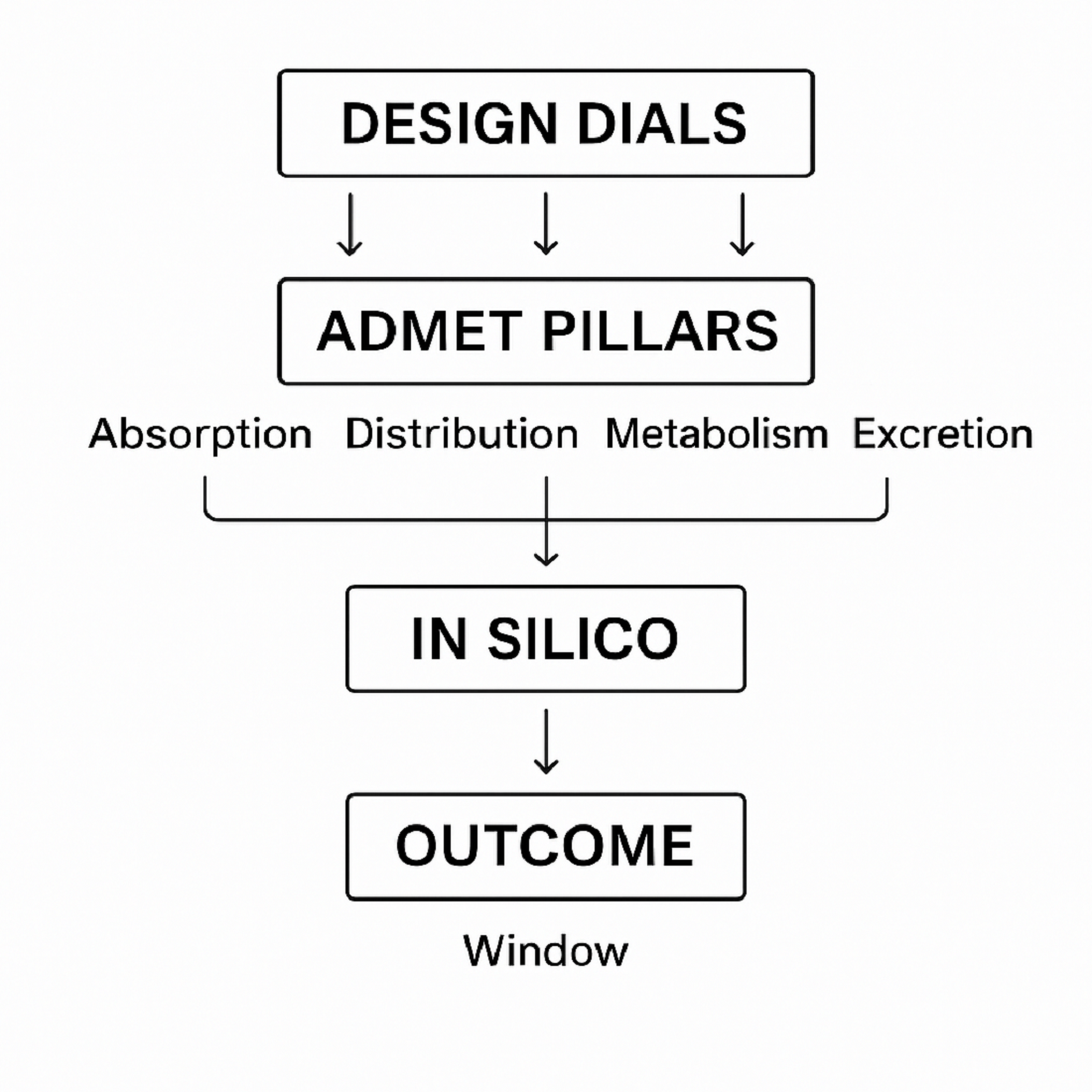
Low-molecular-weight agents such as BPA/BSH generally show limited V_d (≈0.4–0.6 L/kg), consistent with extracellular confinement and rapid clearance [1,11,12]. Nanocarriers and peptide conjugates often exhibit higher V_d (≈1.5–3.5 L/kg), reflecting deeper tissue penetration and longer residence, aided by PEGylation and lipid encapsulation [15,63]. Emerging PBPK and time-dependent boron-dose models seek to harmonise biodistribution with irradiation timing and dosimetry [64]. This concept is illustrated schematically in Figure 1.
Strategies to enhance brain penetration include tuning particle size (50–100 nm), surface charge near neutrality, and grafting ligands for receptor-mediated transcytosis. Nevertheless, clinical translation requires balancing enhanced BBB transport with off-target uptake and potential microglial activation [8,15,23].
3.2. Tissue Distribution and Tumour Selectivity
BPA preferentially accumulates in LAT1-expressing tumours but is subject to inter- and intra-tumoural heterogeneity [10]. BSH is comparatively non-selective with higher hepatic/renal uptake [11,12]. Structural targeting (e.g., nuclear-affine metallacarboranes) and ligand-directed systems (e.g., RGD, folate) can increase T/N ratios in preclinical models [13,14,15,21]. Cellular carriers (e.g., macrophages) have delivered more uniform intratumoural distributions, including in hypoxic/necrotic regions [23,24].
3.3. Blood–Brain Barrier (BBB) and Blood-Tumour Barrier (BTB)
For primary CNS tumours and metastatic brain tumours, penetration of the BBB/BTB remains a key hurdle. Importantly, primary CNS tumours exhibit different BTB anatomy and permeability compared with metastatic brain tumours arising from peripheral primary cancers such as lung and breast. According to[72] the BTB in primary CNS tumours is generally more permeable than in brain metastases. This phenomenon requires more comprehensive investigation. Studies indicate that BSH does not cross the intact BBB. It is assumed that delivery of BSH to brain tumour cells relies on passive diffusion across the BTB, owing to its pathologically increased permeability compared with the normal BBB structure [73,74,75]. However, BTB permeability is still insufficient for most molecules.
BPA/BPA-fructose partially circumvents the BBB via LAT1 transporters but shows heterogeneous uptake. PEGylated liposomes, boronated polymeric nanoparticles and boron-rich clusters can exploit receptor-mediated transcytosis or adsorptive endocytosis; functionalisation (e.g., transferrin-like ligands) and intermediate lipophilicity can improve brain exposure, although translation into consistent clinical benefit requires further validation[15,23,62,76].
Studies on intracerebral drug delivery to brain tumours by intrathecal injection into the cerebrospinal fluid or convection-enhanced delivery directly to intracranial tumours, as potential methods of BBB/BTB bypass, show enhanced ^10B cellular uptake in lesion areas and higher T/N ratios [75]. However, these methods are highly invasive, and further work on safer BBB/BTB permeability enhancement is required. BBB/BTB permeability for therapeutic drugs can be modified by osmotic mannitol-induced opening of endothelial tight junctions. Furthermore, stimulation of endothelial cell receptors via intra-arterial administration of vasoactive compounds, ultrasound-based techniques combined with microbubble administration, and electropermeabilisation have all been reported as potential methods for clinical BNCT applications[9,72,75,77,78,79,80,81,82]. Nevertheless, despite their potential benefits, these approaches are generally considered invasive and potentially damaging. Consequently, strategies that exploit physiological BBB transport mechanisms and/or the pathophysiological properties of the BTB are being extensively developed as more advantageous and safer alternatives.
3.4. Intracellular Distribution and Organelle Targeting
Given the micrometric range of BNCT particles, subcellular localisation matters. Nuclear-accumulating metallacarborane intercalators and boronated nucleosides enhance DNA-proximate ^10B deposition, potentially increasing cytotoxic yield at equal bulk boron levels. Liposomal/polymeric carriers may localise to endo-lysosomal compartments unless engineered for triggerable release[13,14,15,25,26,61,83,84].
3.5. Distribution Kinetics and Clearance
Small molecules approach distribution equilibrium rapidly (≈15–30 min), whereas nano-systems often show bi-exponential kinetics with prolonged α- and β-phases owing to stealth coatings and reduced RES uptake[15,63]. Biodistribution patterns typically favour tumour and liver for silica/BN-based nanocarriers, with PEG minimising splenic/renal deposition relative to non-PEGylated analogues [15,21].
3.6. Clinical Distribution Data
Clinical FBPA-PET studies in glioma demonstrate T/N ratios commonly around 2–3+ with supportive T/B values, guiding patient selection and scheduling [8,40,64]. Accelerator-based BNCT platforms and prospective trials are expanding the clinical dataset and will enable more robust ADMET-dosimetry integration [5,11,24,85].
4. Metabolism of Boron-Containing Agents
Successful BNCT requires that chemically stable ^10B remains associated with tumour cells long enough to match the neutron-irradiation window, while minimising residues in normal organs. Here, “metabolism” encompasses (i) enzymatic and non-enzymatic transformation of small-molecule agents and linkers, (ii) intracellular trafficking and processing that determine subcellular fate, and (iii) biodegradation of carrier matrices and ligands that release, retain, or inactivate boron payloads [1,2,3,7,14,15,76,84,85]. See Table 3 for a concise summary of key ADMET parameters discussed in this section. In silico ADMET platforms can be used to anticipate metabolic liabilities of linkers and to triage designs prior to in vivo testing [34]. Mechanistic reviews of boron pharmacophores (including carborane-based scaffolds) summarise metabolism-relevant design trade-offs [34,35]. Metabolic stability of boron pharmacophores and linker design considerations are overviewed in [64]. Metabolism-relevant design trade-offs (cluster stability vs linker liability) and polymer platforms are discussed in recent reviews and case studies [19,39,48].
4.1. Low-Molecular-Weight Agents
BPA/BPA–fructose. Boronophenylalanine (BPA) is transported predominantly by LAT1 and, after cellular entry, does not undergo extensive biotransformation; its apparent “metabolic” behaviour is governed by reversible intracellular partitioning and relatively rapid egress from cells lacking sustained LAT1-mediated transport[10]. Clinically, the fructose complex improves aqueous handling and exposure but does not introduce a distinct metabolic pathway; PET studies with ^18F-labelled BPA (18F-BPA)analogues show time-dependent tumour uptake and washout consistent with transporter-coupled distribution rather than covalent metabolism [8,40]. Consequently, strategies to increase functional retention rely on formulation or co-delivery that delays efflux (Section 4.4) [3,15,17,87].
BSH. Sodium borocaptate (BSH) is highly hydrophilic and largely extracellular; it exhibits limited membrane permeability and is cleared renally with negligible metabolic conversion, which constrains intracellular boron residence times in many tumours [1,11,12]. Attempts to alter BSH fate therefore emphasise conjugation or encapsulation rather than exploiting intrinsic biotransformation [3,7,27].
4.2. Metallacarborane and Carborane-Containing Small Molecules
Carborane clusters are exceptionally resistant to oxidative and hydrolytic degradation under physiological conditions, a property that underpins their use as metabolically robust boron carriers [7,13,14,15,25,26,41]. When appended to nucleosides, intercalators or other scaffolds, metabolic “soft spots” shift from the cluster to organic linkers and heteroatom-rich tethers. Reported designs mitigate premature cleavage through steric shielding, hydrolytically stable linkages, and balanced lipophilicity (logP ≈ 2–3) that reduces lysosomal sequestration without sacrificing uptake [7,13,14,15,25,26,41].
4.3. Bioconjugates: Peptides and Targeted Ligands
For peptide or small-protein conjugates, in vivo stability is dominated by proteolysis and linker chemistry. Protease-resistant backbones, cyclisation, and PEGylated spacers reduce proteolytic turnover, whereas cleavable linkers (e.g., acid-labile or enzyme-responsive) can trigger intracellular release from endosomes—minimising lysosomal degradation of the cargo [10,14,15,18,19,83]. Receptor cycling kinetics also shape fate: repeated endocytosis–recycling can maintain intracellular exposure if the conjugate avoids rapid lysosomal destruction [14,15].
4.4. Polymeric and Lipid Carriers
Polymeric dendrimers and PEGylated liposomes protect boron payloads from premature efflux and metabolism by slowing opsonisation and reticuloendothelial uptake; their effective half-lives are therefore controlled by colloidal stability, stealth coatings and gradual matrix erosion rather than classical xenobiotic metabolism [15,52,62,63] . PEG corona density, particle size and surface charge govern protein-corona formation and downstream clearance; insufficient stealth accelerates hepatic and splenic processing, curtailing the therapeutic window [16,17,56]. Within cells, endosomal–lysosomal trafficking can entrap carriers; endosomolytic components or pH-responsive gates are used to achieve cytosolic release before degradative processing reduces functional boron content [15,16,17].
4.5. Inorganic Nanoplatforms
Functionalised mesoporous silica nanoparticles (MSNs) do not undergo enzymatic metabolism; their fate reflects surface chemistry and biodegradation into silicic acid over extended timescales. Gatekeepers and ligand shells dictate when and where boron is released; careful control of linker stability is required to prevent premature shedding in blood or rapid endo-lysosomal degradation after uptake [20,21,53,54,55]. As with polymeric systems, protein-corona evolution influences cellular routing and organ-level processing [21,56].
4.6. Cell-Based Delivery Systems
Macrophages and related cellular carriers internalise boron payloads and traffic them into hypoxic and poorly perfused tumour regions. In this context, “metabolism” comprises intracellular processing of the payload (e.g., nanoparticle dissolution or linker cleavage) and carrier-cell viability and activation state, which together govern release kinetics at the disease site. Available data indicate that macrophage-borne boron carbide nanoparticles can maintain payload integrity during homing and enable sustained intratumoural release, thereby prolonging intratumoural residence without chemical modification of the boron core [23,24].
4.7. Analytical Read-Outs and Modelling of Metabolic Fate
Dynamic PET with ^18F-BPA analogues offers a non-invasive surrogate for time-dependent boron handling in LAT1-positive tissues, informing whether apparent loss reflects distributional washout rather than chemical turnover [8,40,87]. Integrating such data into physiologically based pharmacokinetic and dose-planning frameworks allows explicit scheduling of irradiation to coincide with peak tumour-to-blood ratios and to account for carrier-specific retention versus clearance processes. Contemporary reviews emphasise aligning subcellular localisation with BNCT radiobiology to maximise high-LET yield per retained ^10B atom [3,14,76].
4.8. Design Principles from a Metabolism Perspective
Favour chemically inert boron cores and shift control to linkers and trafficking; tune linkers for on-target release while resisting plasma degradation [7,13,14,15,25,26,41].
Reduce endo-lysosomal loss by incorporating pH-labile or membrane-active features to promote endosomal escape [14,15,16,17].
Exploit transporter biology without creating new liabilities; for LAT1-mediated entry, adjust polarity and sterics to curb rapid efflux while retaining engagement [3,10,14,15,87].
Engineer carrier shells for controlled processing; PEG density, size and surface chemistry govern protein-corona formation, RES uptake and intracellular routing [15,16,52,56].
5. Excretion of Boron-Containing Agents
The elimination of boron carriers determines the width of the therapeutic window, the off-target dose to radiosensitive organs, and the long-term safety profile. For BNCT agents, “excretion” encompasses glomerular filtration and tubular handling for low-molecular-weight compounds, hepatobiliary elimination following uptake by hepatic sinusoidal endothelium and Kupffer cells, and mononuclear phagocyte system (MPS/RES) processing of nano- and bio-carriers, often preceded by protein-corona formation. See Table 4 for a concise summary of excretion-relevant ADMET parameters across representative agents. Elimination considerations for BPA/BSH and newer classes are discussed in current BNCT guidance and reviews [34,86]. Early animal work on borylated ferrocenium derivatives provides additional context on organ distribution and handling [66]. Elimination routes and practical safety context for boron classes are discussed in [23]. Elimination and material handling can be informed by reports on 2D boron nitride nanosheets and tracer pharmacokinetics [58,89,90].
5.1. General Principles and Elimination Pathways
Small, hydrophilic molecules are typically cleared rapidly by the kidneys; increased lipophilicity and plasma protein binding reduce filtration and may favour hepatobiliary routes. For nanoparticles and supramolecular carriers, hydrodynamic size, surface chemistry (including PEG density and charge), and the acquired biomolecular corona govern MPS recognition and organ retention, thereby shaping biliary versus renal elimination and any lymphatic drainage component [49,50,51,90]. In practice, systems that avoid opsonisation and remain below renal filtration size cut-offs are more likely to undergo efficient urinary clearance; larger or poorly “stealthed” constructs preferentially accumulate in liver and spleen before slow hepatobiliary excretion [49,50,51].
5.2. Low-Molecular-Weight Agents
BPA/BPA–fructose. After LAT1-mediated uptake and redistribution, BPA is eliminated predominantly via the kidneys; clinical PET kinetics consistently show relatively rapid blood clearance with time-dependent tumour washout, reflecting transporter biology more than metabolic turnover [3,40,62]. Adjusting infusion schedules and irradiation timing aims to exploit transiently favourable tumour-to-blood ratios while limiting renal exposure [3,14]
5.3. Bioconjugates (Peptides, Targeted Ligands)
Peptide conjugates below the renal filtration size tend to be cleared renally unless protected by plasma binding or sustained receptor engagement; proteolysis generates smaller fragments that further favour urinary elimination. Where conjugates engage high-turnover endocytic pathways, intracellular routing to lysosomes can precede efflux of catabolites and subsequent renal clearance. Linker design (e.g., acid-labile, enzyme-responsive) modulates when intracellular release occurs and may indirectly alter the balance between renal and biliary routes [14,15,18,19,83]
5.4. Polymeric and Lipid Carriers
PEGylated liposomes and dendrimers generally exhibit prolonged circulation with progressive uptake by the MPS in liver and spleen; elimination typically proceeds via hepatobiliary excretion of lipidic or polymeric catabolites and, to a lesser extent, renal clearance of low-molecular fragments. Higher PEG density and near-neutral surface charge reduce opsonisation and slow RES capture, whereas insufficient stealth accelerates hepatic processing and shortens systemic exposure [15,16,17,52]. Re-engineering endosomal escape may paradoxically increase apparent elimination if it accelerates cytosolic release and subsequent renal clearance of small payloads [16,17,52].
5.5. Inorganic Nanoplatforms
Functionalised mesoporous silica nanoparticles (MSNs) do not undergo enzymatic metabolism; instead, they experience gradual biodegradation to silicic acid, with rates governed by particle size, porosity and surface functionalisation. Depending on corona composition and organ uptake, elimination can involve slow hepatobiliary routes, with urinary excretion of soluble degradation products. Gatekeepers and ligand shells, while enabling on-target release, also influence organ retention and therefore the timescale of excretion [20,21,52,54]
5.6. Cell-Based Delivery Systems
For macrophage-mediated delivery, the primary determinant of excretion is the fate of the carrier cell and the persistence of the internalised payload. After tumour homing and release, residual payload may be sequestered by local phagocytes or cleared via lymphatics and hepatic pathways; when cargo consists of inert boron carbide nanoparticles, systemic redistribution is limited and elimination depends on slow biological turnover rather than classical renal or biliary routes.
5.7. Transporters and Clinical Pharmacology
Although most BNCT carriers are not classic substrates for drug-metabolising enzymes, renal and hepatic transporters modulate apparent clearance of small molecules and catabolites. Contemporary guidance highlights clinically relevant transporters (e.g., OATs/OCTs, OATP/BCRP/P-gp) and study designs for evaluating transporter-mediated interactions; such principles are valuable when BNCT agents are co-administered with supportive medications that may affect renal secretion or biliary efflux [33,46].
5.8. Design Principles for Favourable Elimination
Match elimination route to clinical scheduling: for BPA and similar small molecules, fast renal clearance demands irradiation windows aligned to peak tumour exposure; for nano-carriers, anticipate slower hepatobiliary excretion and plan accordingly. Exploit size and stealth judiciously: maintain hydrodynamic sizes and surface chemistries that avoid excessive RES uptake while not preventing eventual elimination; higher PEG density and neutrality generally prolong circulation but may also delay clearance [16,17,49,50,51].
Design degradability without premature loss: for polymeric and silica systems, incorporate controlled-degradation features that permit eventual elimination (renal or biliary) after the therapeutic window, avoiding long-term organ retention [20,21,52,53,54,55].
Consider transporter context: when feasible, avoid strong interactions with renal/hepatic transporters liable to drug–drug interactions in multi-agent regimens; consult transporter frameworks when planning clinical protocols [33].
6. Toxicity and Safety of Boron-Containing Agents
Clinical translation of BNCT depends on delivering a cytocidal high-LET dose selectively to tumour while maintaining acceptable systemic and organ-specific safety. Toxicity arises from (i) the carrier itself (chemical/biological effects), (ii) off-target boron deposition in normal tissues exposed during irradiation, and (iii) platform-specific liabilities (e.g., nanocarrier MPS uptake, peptide immunogenicity) [1,2,3,4,5,7,14,76,85,91]. See Table 5 for a concise summary of toxicity-relevant considerations across representative agents. A recent review on boron nanodrugs for BNCT provides an integrated overview of efficacy, biodistribution and safety issues for nano-scale delivery systems [92].
6.1. Clinical Safety Experience and Normal-Tissue Effects
Modern trials and clinical series, particularly with accelerator-based BNCT for recurrent head-and-neck cancer and other indications, report toxicity profiles dominated by expected radiotherapy-like adverse events in the irradiated field (mucositis, dermatitis, xerostomia), with systemic events generally mild to moderate when BPA or BSH are employed according to contemporary protocols [4,39,76,84,85,91,93]. Dose planning that integrates time-dependent tumour-to-blood ratios reduces normal-tissue dose and correlates with acceptable acute and subacute toxicity in prospective cohorts [5,64,76,84,85,93].
6.2. Small-Molecule Agents
BPA/BPA–fructose. Clinical use is associated most commonly with transient nausea, flushing and infusion-related symptoms; significant organ toxicity is uncommon at recommended exposures when irradiation is scheduled to favourable T/B windows. Because BPA relies on LAT1-mediated transport, heterogeneity in transporter expression can lead to variable normal-tissue uptake, which is mitigated by PET-based selection and scheduling [3,8,10,14,40].
6.3. Bioconjugates and Targeted Ligands
Peptide and ligand-bearing constructs introduce platform risks: proteolysis (yielding reactive fragments), potential immunogenicity, and off-target binding where receptors are expressed on normal tissues. Rational design (protease-resistant backbones, constrained/cyclised scaffolds, stable yet triggerable linkers) reduces these liabilities; nonetheless, receptor density heterogeneity implies that patient selection and imaging confirmation remain crucial to limit unintended normal-tissue dose during irradiation [14,15,18,19,83]
6.4. Polymeric and Lipid Carriers
PEGylated liposomes and dendrimers prolong circulation and can enhance tumour exposure, but they interact with the mononuclear phagocyte system (MPS), driving hepatic/splenic deposition. Safety considerations therefore include hepatosplenic enlargement, alteration of liver enzymes, complement activation, and—less commonly—infusion reactions; these are mitigated by optimising PEG density, surface charge and size, as well as by step-wise dosing where appropriate [15,16,17,52]. Endosomal escape motifs that improve intracellular delivery must be balanced against membrane-active toxicity at high concentrations.
6.5. Inorganic Nanoplatforms
Functionalised mesoporous silica nanoparticles (MSNs) are not metabolised enzymatically but undergo gradual biodegradation to silicic acid, the rate of which depends on particle size, porosity and surface chemistry. Reported safety concerns reflect long-term organ retention if degradation is slow, and inflammatory responses modulated by protein-corona composition; design strategies that favour biodegradation after the therapeutic window and neutral corona profiles generally improve tolerability [20,21,54,55,56,92].
6.6. Cell-Based Delivery Systems
Macrophage-mediated delivery offers deep penetration into hypoxic tumour territories but raises distinct safety questions: persistence of carrier cells, ectopic accumulation, and immune activation. Preclinical work shows tumour-homing with sustained intratumoural presence and limited systemic redistribution of inert boron carbide payloads; translation requires GMP-compliant manufacturing, release criteria, and monitoring for cytokine-related events [23,24].
6.7. Radiobiology-Informed Risk Management
Because the path length of α/^7Li particles is micrometric, toxicity from BNCT is tightly coupled to where boron resides at irradiation. Contemporary radiobiology overviews emphasise aligning subcellular localisation—with a preference for DNA-proximal boron for efficacy—with sparing of normal tissues, especially in organs at risk adjacent to the target volume. PET read-outs (e.g., with ^18F-BPA analogues) combined with PBPK-aware dose planning reduce normal-tissue exposure by matching neutron fields to windows of maximal tumour selectivity [8,40,64,76,84]
6.8. Drug–Drug Interactions and Supportive Care
While BNCT agents are not classical substrates for drug-metabolising enzymes, small boronated molecules and catabolites can be substrates of renal or hepatic transporters. Guidance from the International Transporter Consortium and recent clinical methodology highlights the need to consider transporter-mediated interactions when planning antiemetics, analgesics or other supportive medications that might alter renal secretion or biliary efflux [33]. For nano-platforms and bioconjugates, interactions are more likely to be physicochemical/biological (e.g., complement activation, opsonisation) than enzymatic, and should be addressed through premedication policies and infusion-rate control where indicated.
6.9. Practical Design Principles (Safety)
Engineer selectivity first: subcellular localisation and tumour selectivity (T/N, T/B at irradiation) are dominant determinants of toxicity in BNCT; imaging-guided scheduling is central to risk reduction [3,4,5,8,22,40,64,76,85,93]
Minimise pro-inflammatory cues: favour PEGylation and near-neutral surfaces to reduce opsonisation/complement activation for nano-platforms; avoid highly cationic designs associated with haemolysis or membrane damage][15,16,17].
Implement time-controlled degradability: for inorganic/polymeric carriers, design controlled post-treatment biodegradation, to prevent long-term organ retention while preserving intratumoural residence during therapy [20,21,53,54].
Constrain peptide/ligand risk: use protease-resistant motifs and validate receptor expression in normal tissues to limit off-target uptake; consider immunogenicity screening for repeated dosing [14,15,18,19,83]
Account for transporters and co-medications: map plausible transporter liabilities for small molecules and plan supportive therapy to avoid increasing systemic exposure or altering renal clearance[33].
6.10. Genetic and Oxidative Safety
Genetic and oxidative risks associated with boron-containing agents arise from two separable sources: (i) material-intrinsic effects (e.g., surface reactivity of inorganic frameworks, redox or photoactive motifs, linker-driven off-target chemistry) and (ii) BNCT irradiation, when boron is mislocalised to normal tissues. Contemporary radiobiology underscores that the micrometric range of the α/^7Li particles confines DNA injury to boron-loaded cells; hence, genotoxicity in healthy tissues is primarily a function of biodistribution at the instant of irradiation, rather than of intrinsic mutagenicity of the carrier [76,84]. For small molecules (BPA/BPA-fructose; BSH), clinical and translational reports have not identified consistent genotoxic signals at therapeutic exposures when irradiation is scheduled to favourable tumour-to-blood ratios and patient selection uses PET read-outs [3,4,5,8,40,84,85]. For supramolecular and inorganic platforms (PEGylated liposomes/dendrimers; mesoporous silica), oxidative read-outs largely reflect protein-corona composition, endo-lysosomal residence and long-term organ retention; neutral coronas, controlled post-treatment biodegradation (for silica), and calibrated endosomal-escape features mitigate these risks. Boron nitride nanosheets prepared under sustainable, biocompatible protocols likewise exhibit favourable oxidative profiles contingent on surface passivation and synthesis route [89]. Overall, genetic safety is dictated by selective localisation at the time of neutron exposure and by surface/linker engineering that minimises ROS-linked stress during residence within the reticuloendothelial system [15,16,17,54,55,56,76,89].
6.11. In Vivo Toxicological Profiles and NOAEL Values
For inorganic borates/boric acid outside the BNCT context, classical toxicology synthesises organ-level hazards and NOAEL benchmarks in animals; these reviews provide a conservative backdrop for interpreting systemic exposure (notably renal) and for framing dose-setting in boron-containing platforms [94]. In nanomedicine, clearance-centred analyses relate hydrodynamic size, PEG density, surface charge and corona formation to organ sequestration and elimination, offering practical levers to reduce long-term tissue burden and to interpret hepatic or splenic findings under repeat dosing [49,50,51]. Translational BNCT series indicate that with contemporary BPA/BSH protocols, imaging-guided scheduling and PBPK-aware planning, systemic toxicity is usually limited and dominated by field-restricted radiotherapy reactions rather than multi-organ failure, aligning with clinically acceptable safety margins [4,93]. For mesoporous silica and polymeric carriers, in vivo profiles improve when matrices are degradable on clinically relevant timescales and when surfaces limit opsonisation, thereby facilitating eventual elimination and tempering chronic organ retention [20,21,52,54]. Precise NOAELs are compound-, species- and regimen-dependent; where they exist, they should be invoked in context and not extrapolated across platforms without adjustment for formulation and exposure kinetics [94].
6.12. Immunotoxicity and Inflammatory Responses [14,15,16,17,18,20,54,56,83]
Immunotoxicity with BNCT delivery systems is generally platform-determined. For liposomes and dendrimers, principal concerns include complement activation and mononuclear phagocyte system (MPS/RES) uptake, exacerbated by low PEG density, cationic surfaces or “sticky” coronas; mitigation relies on increasing PEG coverage, maintaining near-neutral charge, moderating infusion rates, and using premedication where indicated. For mesoporous silica and related inorganics, inflammatory signatures track with biodegradation kinetics and surface chemistry; designs that promote neutral coronas and triggerable (pH/enzyme-labile) gates tend to suppress innate activation and favour “silent” clearance. Peptide/ligand conjugates carry risks of immunogenicity and off-target binding where receptors are expressed in normal tissues; protease-resistant scaffolds, validated receptor maps and monitoring for infusion reactions are prudent safeguards. Cell-based carriers may elicit cytokine responses contingent on cell activation state and persistence; GMP-compliant manufacture, explicit release criteria, and protocolised clinical monitoring are required. In practice, surface neutrality, controlled degradability and calibrated intracellular escape reduce inflammatory risk, while precise irradiation timing minimises radiogenic inflammation in normal tissues adjacent to the target volume. For a compact cross-platform comparison of safety endpoints and mitigations, see Table 5.
7. Key Insights
7.1. Absorption
Transporter biology dominates small-molecule entry: LAT1 for BPA and nucleoside transporters for selected boronated bases, while formulations such as BPA–fructose primarily modulate exposure without creating new biotransformation pathways [8,10,14,23,29,30,32,40]. For nano- and polymeric systems, hydrodynamic size (≈50–150 nm), near-neutral surface charge and PEGylation govern epithelial/endothelial passage and endocytic uptake; optimising these variables improves synchrony between tumour exposure and irradiation [11,15,16,17,23,48,49,50,51]. Carborane motifs increase lipophilicity and membrane interaction; balancing logP (~2–3) with polar linkers enhances uptake while mitigating lysosomal sequestration [7,13,14,15,41,42,43,44]. In practice, transporter-aware design combined with pro-retention features (e.g. endosomal escape, linker selection) and PET tracers, where available, allows absorption trajectories to be quantified and scheduled [8,38,39,40,57,58].
7.2. Distribution
Clinical distribution is heterogeneous and indication-dependent: BPA shows LAT1-linked tumour uptake with typical glioma T/N ratios around 2–3+, whereas BSH remains largely extracellular with lower selectivity [1,3,8,10,11,12,14,23,34,86]. PEGylated carriers extend circulation but are progressively taken up by MPS organs (liver, spleen); ligand grafting can redirect a fraction towards tumours, whereas BBB entry generally requires specific targeting mechanisms [11,15,16,23,34,35,49,50,51,52,62]. Subcellular localisation is critical given the micrometric range of BNCT particles: DNA-proximal constructs, such as metallacarborane intercalators, can increase radiobiological yield at similar bulk boron levels [13,14,15,41,43,44]. Integration of PBPK-based planning with imaging read-outs allows irradiation to be scheduled at maximal T/B ratios and within platform-specific biodistribution windows [8,40,64,84].
7.3. Metabolism
Carborane clusters are metabolically robust; liabilities are shifted to linkers and attached scaffolds, where hydrolysis can be controlled via amide/urea linkages, steric shielding and appropriate lipophilicity [7,13,14,15,41,42,43,44,45]. Polymeric and lipid carriers undergo colloidal processing rather than classical enzymatic metabolism; their fate is dictated by protein corona formation, stealth properties and intracellular routing [11,15,16,17,23,48,49,50,51,56].MSNs degrade slowly to silicic acid, with surface chemistry and gate design controlling the timing of payload release and material clearance [20,21,54,55]. For BPA/BSH, most apparent “metabolic” behaviour reflects distributional washout, so linker and gate design should align intracellular release with the planned irradiation window [3,8,14,22,37,40,64].
7.4. Excretion
Small hydrophilic agents are predominantly cleared renally, whereas nano- and polymeric systems tend to follow hepatobiliary routes after MPS uptake, with clearance rates governed by degradability and corona evolution [1,3,11,12,15,23,49,50,51,56]. Controlled degradability of matrices enables eventual elimination while preserving sufficient exposure during therapy [20,21,52,54,55]. Consequently, particle size and stealth should be tuned for predictable clearance, and irradiation should be planned near the pharmacokinetic peak for small molecules or within the exposure plateau for long-circulating carriers [8,40,49,50,51,63].
7.5. Toxicity
Most observed clinical toxicities resemble conventional radiotherapy-related effects within the irradiated field; systemic events are generally mild when scheduling aligns with favourable T/B ratios [4,5,76,84,85,91,93]. Platform-specific risks include complement activation (liposomes, dendrimers), inflammatory responses with slowly degradable inorganics, and immunogenicity or off-target binding for peptide/ligand conjugates [14,15,18,20,21,52,53,54,55,83]. These risks can be mitigated by surface neutrality and adequate PEG coverage, controlled biodegradation, validated receptor expression maps and appropriate supportive-care protocols, while PET/PBPK-based planning helps minimise normal-tissue dose [8,14,15,40,52,54,55,56,63,76,84].
These key insights can be mapped back onto the design control framework outlined in Figure 2, emphasising how quantitative ADMET goals translate into concrete choices of BNCT carrier platforms.
8. Conclusions & Outlook
Dimodality of BNCT and interdisciplinary collaborative research implies that the development in the multidisciplinary scientific areas and evaluation of new technologies is in demand. To achieve high effectiveness of BNCT, an adequate therapeutic dose delivery is desired. The ADMET framework allows defining input parameters for treatment plan establishment and BNCT implementation. Quantitative theranostics approach, subcellular precision of targeting molecules providing long-circulating yet degradable platforms design, biological vectors evaluation, transporter-aware pharmacology are the main pillars indicating future directions of BNCT development.
8.1. Future directions
Quantitative theranostics. Systematically combined PET-derived kinetics (e.g., ^18F-labelled amino acids and sugars) with PBPK models and time-resolved dosimetry to personalise neutron-field timing and reduce the risk of normal-tissue exposure [8,38,39,40,57,58,64,84]. Table 6 summarises the in silico toolbox that underpins ADMET-guided optimisation of BNCT agents and treatment schedules.
Subcellular precision. Further develop nuclear-affine boron pharmacophores and triggerable gates to maximise DNA-proximate ^10B at a given total boron load, with an emphasis on linker chemistries that couple endosomal escape to controlled intracellular release [13,14,15,41,43,44].
Long-circulating yet degradable platforms. Design long-circulating carriers with well-characterised biodegradation profiles to balance exposure and clearance, and to define post-treatment degradation timeframes that avoid chronic organ retention [11,15,48,49,50,51,52,53,54,55,62,63].Biological vectors. cell-based delivery under GMP conditions with robust release criteria and clinical monitoring frameworks to exploit homing into hypoxic tumour regions while maintaining safety [23,24].Transporter-aware pharmacology. Map LAT1 and other clinically relevant transporters across indications to stratify patients and to anticipate drug–drug interactions affecting renal and hepatic transport [10,14,33,87].
8.2. Perspective
Research on BNCT is conducted at the intersection of radiobiology, medical chemistry, medical physics, medicine, dosimetry and nuclear engineering . The main challenge is spatiotemporal correlation boron dose deposition, namely high-LET dose delivery within the therapeutic window in which boron is concentrated at the specified subcellular location within the tumour but it hardly ever accumulates in normal tissues. The ADMET framework clarifies chemical and biophysical therapy pillars providing a basis for treatment plan establishment and adequate physical dose deposition in target volume to achieve an expected therapeutic effect and minimize side effects: transporter engagement and formulation (Absorption), PBPK-synchronised tissue exposure (Distribution), linker- and route-of-entry control (Metabolism), degradability-tuned clearance (Excretion), and platform-aware risk management (Toxicity). Progress over the next few years is likely to be driven by imaging-guided treatment planning evaluation, specific subcellularly targeting carriers and materials that combine prolonged circulation with predictable degradation, enabling BNCT to deliver its spatial therapeutic selectivity with reproducible clinical benefit.
Funding
The project is financed by the National Science Centre (R. No. 2018/02/X/NZ7/03011).
Acknowledgments
The authors express gratitude to all collaborating research teams contributing to the development of boron pharmacology and BNCT translational studies.
Conflicts of Interest
The authors declare no competing financial or personal interests that could influence the content of this review.
Abbreviations
The following abbreviations are used in this manuscript:
ADMET Absorption, Distribution, Metabolism, Excretion and Toxicity
BBB Blood–Brain Barrier
BCRP Breast Cancer Resistance Protein
BN Boron Nitride
BNCT Boron Neutron Capture Therapy
BODIPY Boron-Dipyrromethene
BPA p-Boronophenylalanine
BPA–F / BPA-fructose Boronophenylalanine-fructose
18F-BPA / FBPA 18F-labelled Boronophenylalanine
FBPA-Fr / 18F-BPA-fructose 18F-labelled Boronophenylalanine-fructose
BSH Sodium Mercaptoundecahydro-closo-Dodecaborate (Sodium Borocaptate)
BTB Blood–Tumour Barrier
CA IX Carbonic Anhydrase IX
Cmax Maximum Plasma Concentration
CL Clearance
CNS Central Nervous System
DDI Drug–Drug Interaction
DNA Deoxyribonucleic Acid
EPR Enhanced Permeability and Retention (effect)
EGFR Epidermal Growth Factor Receptor
GMP Good Manufacturing Practice
LAT1 L-Type Amino Acid Transporter 1
LET Linear Energy Transfer
logP Logarithm of the Partition Coefficient (octanol/water)
MPS Mononuclear Phagocyte System
MRI Magnetic Resonance Imaging
MSCs Mesenchymal Stromal Cells
MSNs Mesoporous Silica Nanoparticles
NOAEL No-Observed-Adverse-Effect Level
OATs Organic Anion Transporters
OATPs Organic Anion Transporting Polypeptides
OCTs Organic Cation Transporters
PBPK Physiologically Based Pharmacokinetic
PEG Polyethylene Glycol
PET Positron Emission Tomography
P-gp P-Glycoprotein
RES Reticuloendothelial System
RGD Arginine–Glycine–Aspartate (integrin-binding motif)
ROS Reactive Oxygen Species
t1/2 Half-Life
T/B Tumour-to-Blood Ratio
T/N Tumour-to-Normal Tissue Ratio
Vd / Vd Volume of Distribution
References
- Sauerwein, W.A.; Wittig, A.; Moss, R.; Nakagawa, Y. Neutron Capture Therapy: Principles and Applications; Springer, 2012. [Google Scholar]
- Dymova, M.A.; Taskaev, S.Y.; Richter, V.A.; Kuligina, E.V. Boron Neutron Capture Therapy: Current Status and Future Perspectives. Cancer Communications 2020, 40, 406–421. [Google Scholar] [CrossRef] [PubMed]
- Monti Hughes, A.; Hu, N. Optimizing Boron Neutron Capture Therapy (BNCT) to Treat Cancer: An Updated Review on the Latest Developments on Boron Compounds and Strategies. Cancers 2023, 15, 4091. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Li, F.; Liang, L. Boron Neutron Capture Therapy: Clinical Application and Challenges. Current Oncology 2022, 29, 622. [Google Scholar] [CrossRef]
- Kawabata, S.; Suzuki, M.; Hirose, K.; Tanaka, H.; Kato, T.; Goto, H.; Narita, Y.; Miyatake, S.-I. Accelerator-Based BNCT for Patients with Recurrent Glioblastoma: A Multicenter Phase II Study. Neurooncol Adv 2021, 3, vdab067. [Google Scholar] [CrossRef]
- Zhou, Y.-T.; Cheng, K.; Liu, B.; Cao, Y.-C.; Fan, J.-X.; Liu, Z.-G.; Zhao, Y.-D. Recent Progress of Nano-Drugs in Neutron Capture Therapy. Theranostics 2024, 14, 3193–3212. [Google Scholar] [CrossRef]
- Coghi, P.; Li, J.; Hosmane, N.S.; Zhu, Y. Next Generation of Boron Neutron Capture Therapy (BNCT) Agents for Cancer Treatment. Medicinal Research Reviews 2023, 43, 1809–1830. [Google Scholar] [CrossRef]
- Watanabe, T.; Yoshikawa, T.; Tanaka, H.; Kinashi, Y.; Kashino, G.; Masunaga, S.; Hayashi, T.; Uehara, K.; Ono, K.; Suzuki, M. Pharmacokinetic Study of 14C-Radiolabeled p-Boronophenylalanine (BPA) in Sorbitol Solution and the Treatment Outcome of BPA-Based Boron Neutron Capture Therapy on a Tumor-Bearing Mouse Model. Eur J Drug Metab Pharmacokinet 2023, 48, 443–453. [Google Scholar] [CrossRef]
- Fukuda, H. Response of Normal Tissues to Boron Neutron Capture Therapy (BNCT) with 10B-Borocaptate Sodium (BSH) and 10B-Paraboronophenylalanine (BPA). Cells 2021, 10, 2883. [Google Scholar] [CrossRef]
- Hu, K.; Yang, Z.; Zhang, L.; Xie, L.; Wang, L.; Xu, H.; Josephson, L.; Liang, S.H.; Zhang, M.-R. Boron Agents for Neutron Capture Therapy. Coordination Chemistry Reviews 2020, 405, 213139. [Google Scholar] [CrossRef]
- Zhang, X.; Rendina, L.M.; Müllner, M. Carborane-Containing Polymers: Synthesis, Properties, and Applications. ACS Polym. Au 2024, 4, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Tang, F.; Wei, Y.; Zhang, S.; Wang, J.; Gu, W.; Tang, F.; Peng, X.; Wei, Y.; Liu, J.; Chen, W.; et al. Evaluation of Pharmacokinetics of Boronophenylalanine and Its Uptakes in Gastric Cancer. Front. Oncol. 2022, 12, 925671. [Google Scholar] [CrossRef]
- Gos, M.; Cebula, J.; Goszczyński, T.M. Metallacarboranes in Medicinal Chemistry: Current Advances and Future Perspectives. J. Med. Chem. 2024, 67, 8481–8501. [Google Scholar] [CrossRef] [PubMed]
- Seneviratne, D.S.; Saifi, O.; Mackeyev, Y.; Malouff, T.; Krishnan, S. Next-Generation Boron Drugs and Rational Translational Studies Driving the Revival of BNCT. Cells 2023, 12, 1398. [Google Scholar] [CrossRef] [PubMed]
- Oloo, S.O.; Smith, K.M.; Vincente, M.d.G.H. Multi-Functional Boron-Delivery Agents for Boron Neutron Capture Therapy of Canceres. Cancers 2023, 15, 3277. [Google Scholar] [CrossRef] [PubMed]
- Pitto-Barry, A. Polymers and Boron Neutron Capture Therapy (BNCT): A Potent Combination. Polym. Chem. 2021, 12, 2035–2044. [Google Scholar] [CrossRef]
- Maruyama, K.; Ishida, O.; Kasaoka, S.; Takizawa, T.; Utoguchi, N.; Shinohara, A.; Chiba, M.; Kobayashi, H.; Eriguchi, M.; Yanagie, H. Intracellular Targeting of Sodium Mercaptoundecahydrododecaborate (BSH) to Solid Tumors by Transferrin-PEG Liposomes, for Boron Neutron-Capture Therapy (BNCT). Journal of Controlled Release 2004, 98, 195–207. [Google Scholar] [CrossRef]
- Seneviratne, D.; Advani, P.; Trifiletti, D.M.; Chumsri, S.; Beltran, C.J.; Bush, A.F.; Vallow, L.A. Exploring the Biological and Physical Basis of Boron Neutron Capture Therapy (BNCT) as a Promising Treatment Frontier in Breast Cancer. Cancers 2022, 14, 3009. [Google Scholar] [CrossRef]
- Song, S.; Gao, P.; Sun, L.; Kang, D.; Kongsted, J.; Poongavanam, V.; Zhan, P.; Liu, X. Recent Developments in the Medicinal Chemistry of Single Boron Atom-Containing Compounds. Acta Pharmaceutica Sinica B 2021, 11, 3035–3059. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Y.; Hosmane, N.S.; Zhou, Y. Nanostructured Boron Agents for Boron Neutron Capture Therapy: A Review of Recent Patents. Medical Review 2023, 3, 425–443. [Google Scholar] [CrossRef]
- Monti Hughes, A. Importance of Radiobiological Studies for the Advancement of Boron Neutron Capture Therapy (BNCT). Expert Rev. Mol. Med. 2022, 24, e14. [Google Scholar] [CrossRef]
- Li, X.; He, P.; Wei, Y.; Qu, C.; Tang, F.; Li, Y. Application and Perspectives of Nanomaterials in Boron Neutron Capture Therapy of Tumors. Cancer Nano 2025, 16, 25. [Google Scholar] [CrossRef]
- Ali, F.; S Hosmane, N.; Zhu, Y. Boron Chemistry for Medical Applications. Molecules 2020, 25, 828. [Google Scholar] [CrossRef]
- Wróblewska, A.; Kruszakin, R.; Migdał, P.; Pędzich, Z.; Pajtasz-Piasecka, E. Macrophages as Carriers of Boron Carbide Nanoparticles Dedicated to BNCT. Journal of Nanobiotechnology 2024, 22, 183. [Google Scholar] [CrossRef] [PubMed]
- Olejniczak, A.B.; Plešek, J.; Leśnikowski, Z.J. Nucleoside–Metallacarborane Conjugates for Base-Specific Metal Labeling of DNA. Chemistry A European J 2007, 13, 311–318. [Google Scholar] [CrossRef]
- Leśnikowski, Z.J.; Paradowska, E.; Olejniczak, A.B.; Studzińska, M.; Seekamp, P.; Schüßler, U.; Gabel, D.; Schinazi, R.F.; Plešek, J. Towards New Boron Carriers for Boron Neutron Capture Therapy: Metallacarboranes and Their Nucleoside Conjugates. Bioorganic & Medicinal Chemistry 2005, 13, 4168–4175. [Google Scholar] [CrossRef]
- Wójciuk, K.; Dorosz, M.; Prokopowicz, R. AB028. Selected 10-Atom Derivatives of Mercaptoborate as Substrates for the Coupling Reaction with the Neurotransmitter Protein. Ther Radiol Oncol 2025, 9, AB028–AB028. [Google Scholar] [CrossRef]
- Michaś, E.; Dorosz, M.; Wójciuk, K.; Tymińska, K.; Wiliński, M.; Maciak, M.; Domański, S.; Wojtania, G.; Bartosik, Ł.; Małkiewicz, A.; Lechniak, J.; Gryziński, M.A. Reactor Laboratory for Biomedical Research in National Centre for Nuclear Research in Poland. Polish Journal of Medical Physics and Engineering 2021, 27, 119–122. [Google Scholar] [CrossRef]
- Lipinski, C.A.; Lombardo, F.; Dominy, B.W.; Feeney, P.J. Experimental and Computational Approaches to Estimate Solubility and Permeability in Drug Discovery and Development Settings 1PII of Original Article: S0169-409X(96)00423-1. The Article Was Originally Published in Advanced Drug Delivery Reviews 23 (1997) 3–25. 1. Advanced Drug Delivery Reviews 2001, 46, 3–26. [Google Scholar] [CrossRef] [PubMed]
- Veber, D.F.; Johnson, S.R.; Cheng, H.-Y.; Smith, B.R.; Ward, K.W.; Kopple, K.D. Molecular Properties That Influence the Oral Bioavailability of Drug Candidates. J. Med. Chem. 2002, 45, 2615–2623. [Google Scholar] [CrossRef]
- Amidon, G.L.; Lennernäs, H.; Shah, V.P.; Crison, J.R. A Theoretical Basis for a Biopharmaceutic Drug Classification: The Correlation of in Vitro Drug Product Dissolution and in Vivo Bioavailability. Pharm Res 1995, 12, 413–420. [Google Scholar] [CrossRef]
- Lipinski, C.A. Lead- and Drug-like Compounds: The Rule-of-Five Revolution. Drug Discovery Today: Technologies 2004, 1, 337–341. [Google Scholar] [CrossRef]
- Paglialunga, S.; Benrimoh, N.; Van Haarst, A. Innovative Approaches to Optimize Clinical Transporter Drug–Drug Interaction Studies. Pharmaceutics 2024, 16, 992. [Google Scholar] [CrossRef]
- Xu, H.; Liu, J.; Li, R.; Lin, J.; Gui, L.; Wang, Y.; Jin, Z.; Xia, W.; Liu, Y.; Cheng, S.; Yuan, Z. Novel Promising Boron Agents for Boron Neutron Capture Therapy: Current Status and Outlook on the Future. Coordination Chemistry Reviews 2024, 511, 215795. [Google Scholar] [CrossRef]
- Murilla, R.M.; Edilo, G.G.; Budlayan, M.L.M.; Auxtero, E.S. Boron Delivery Agents in BNCT: A Mini Review of Current Developments and Emerging Trends. Nano TransMed 2025, 4, 100081. [Google Scholar] [CrossRef]
- Kawasaki, R.; Miura, Y.; Kono, N.; Fujita, S.; Yamana, K.; Ikeda, A. Boron Agent Delivery Platforms Based on Natural Products for Boron Neutron Capture Therapy. ChemMedChem 2024, 19, e202400323. [Google Scholar] [CrossRef] [PubMed]
- Kugler, M.; Nekvinda, J.; Holub, J.; El Anwar, S.; Das, V.; Šícha, V.; Pospíšilová, K.; Fábry, M.; Král, V.; Brynda, J.; et al. Inhibitors of CA IX Enzyme Based on Polyhedral Boron Compounds. ChemBioChem 2021, 22, 2741–2761. [Google Scholar] [CrossRef]
- Simone, M.I. Diastereoselective Synthesis of the Borylated D-Galactose Monosaccharide 3-Boronic-3-Deoxy-d-Galactose and Biological Evaluation in Glycosidase Inhibition and in Cancer for Boron Neutron Capture Therapy (BNCT). Molecules 2023, 28, 4321. [Google Scholar] [CrossRef]
- Li, Z.; Chen, J.; Kong, Z.; Shi, Y.; Xu, M.; Mu, B.-S.; Li, N.; Ma, W.; Yang, Z.; Wang, Y.; Liu, Z. A Bis-Boron Boramino Acid PET Tracer for Brain Tumor Diagnosis. Eur J Nucl Med Mol Imaging 2024, 51, 1703–1712. [Google Scholar] [CrossRef]
- Fukuda, H.; Honda, C.; Wadabayashi, N.; Kobayashi, T.; Yoshino, K.; Hiratsuka, J.; Takahashi, J.; Akaizawa, T.; Abe, Y.; Ichihashi, M.; Mishima, Y. Pharmacokinetics of 10B-p-Boronophenylalanine in Tumours, Skin and Blood of Melanoma Patients: A Study of Boron Neutron Capture Therapy for Malignant Melanoma. Melanoma Research 1999, 9, 75–84. [Google Scholar] [CrossRef]
- Marfavi, A.; Kavianpour, P.; Rendina, L.M. Carboranes in Drug Discovery, Chemical Biology and Molecular Imaging. Nat Rev Chem 2022, 6, 486–504. [Google Scholar] [CrossRef]
- Das, B.C.; Nandwana, N.K.; Das, S.; Nandwana, V.; Shareef, M.A.; Das, Y.; Saito, M.; Weiss, L.M.; Almaguel, F.; Hosmane, N.S.; Evans, T. Boron Chemicals in Drug Discovery and Development: Synthesis and Medicinal Perspective. Molecules 2022, 27, 2615. [Google Scholar] [CrossRef]
- Issa, F.; Kassiou, M.; Rendina, L.M. Boron in Drug Discovery: Carboranes as Unique Pharmacophores in Biologically Active Compounds. Chem. Rev. 2011, 111, 5701–5722. [Google Scholar] [CrossRef]
- Scholz, M.; Hey-Hawkins, E. Carbaboranes as Pharmacophores: Properties, Synthesis, and Application Strategies. Chem. Rev. 2011, 111, 7035–7062. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, Z.; Huang, Z.; Li, M.; Yang, F.; Wu, Z.; Guo, Q.; Mei, X.; Lu, B.; Wang, C.; et al. Isotoosendanin Exerts Inhibition on Triple-Negative Breast Cancer through Abrogating TGF-β-Induced Epithelial–Mesenchymal Transition via Directly Targeting TGFβR1. Acta Pharmaceutica Sinica B 2023, 13, 2990–3007. [Google Scholar] [CrossRef] [PubMed]
- Zamek-Gliszczynski, M.J.; Taub, M.E.; Chothe, P.P.; Chu, X.; Giacomini, K.M.; Kim, R.B.; Ray, A.S.; Stocker, S.L.; Unadkat, J.D.; Wittwer, M.B.; et al. Transporters in Drug Development: 2018 ITC Recommendations for Transporters of Emerging Clinical Importance. Clin Pharma and Therapeutics 2018, 104, 890–899. [Google Scholar] [CrossRef]
- Chu, X.; Liao, M.; Shen, H.; Yoshida, K.; Zur, A.A.; Arya, V.; Galetin, A.; Giacomini, K.M.; Hanna, I.; Kusuhara, H.; et al. Clinical Probes and Endogenous Biomarkers as Substrates for Transporter Drug-Drug Interaction Evaluation: Perspectives From the International Transporter Consortium. Clin Pharma and Therapeutics 2018, 104, 836–864. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Fu, Q.; Li, J.; Liu, H.; Zhang, Z.; Liu, T.; Liu, Z. Covalent Organic Polymer as a Carborane Carrier for Imaging-Facilitated Boron Neutron Capture Therapy. ACS Appl. Mater. Interfaces 2020, 12, 55564–55573. [Google Scholar] [CrossRef] [PubMed]
- Longmire, M.; Choyke, P.L.; Kobayashi, H. Clearance Properties of Nano-Sized Particles and Molecules as Imaging Agents: Considerations and Caveats. Nanomedicine 2008, 3, 703–717. [Google Scholar] [CrossRef]
- Alexis, F.; Pridgen, E.; Molnar, L.K.; Farokhzad, O.C. Factors Affecting the Clearance and Biodistribution of Polymeric Nanoparticles. Mol. Pharmaceutics 2008, 5, 505–515. [Google Scholar] [CrossRef]
- Yu, M.; Zheng, J. Clearance Pathways and Tumor Targeting of Imaging Nanoparticles. ACS Nano 2015, 9, 6655–6674. [Google Scholar] [CrossRef]
- Chis, A.A.; Dobrea, C.; Morgovan, C.; Arseniu, A.M.; Rus, L.L.; Butuca, A.; Juncan, A.M.; Totan, M.; Vonica-Tincu, A.L.; Cormos, G.; et al. Applications and Limitations of Dendrimers in Biomedicine. Molecules 2020, 25, 3982. [Google Scholar] [CrossRef]
- Li, L.; Liu, T.; Fu, C.; Tan, L.; Meng, X.; Liu, H. Biodistribution, Excretion, and Toxicity of Mesoporous Silica Nanoparticles after Oral Administration Depend on Their Shape. Nanomedicine: Nanotechnology, Biology and Medicine 2015, 11, 1915–1924. [Google Scholar] [CrossRef]
- Narayan, R.; Nayak, U.Y.; Raichur, A.M.; Garg, S. Mesoporous Silica Nanoparticles: A Comprehensive Review on Synthesis and Recent Advances. Pharmaceutics 2018, 10, 118. [Google Scholar] [CrossRef]
- Zhang, Y.; Lin, X.; Chen, X.; Fang, W.; Yu, K.; Gu, W.; Wei, Y.; Zheng, H.; Piao, J.; Li, F. Strategies to Regulate the Degradation and Clearance of Mesoporous Silica Nanoparticles: A Review. IJN 2024, 19, 5859–5878. [Google Scholar] [CrossRef]
- Monopoli, M.P.; Åberg, C.; Salvati, A.; Dawson, K.A. Biomolecular Coronas Provide the Biological Identity of Nanosized Materials. Nature Nanotech 2012, 7, 779–786. [Google Scholar] [CrossRef]
- Confalonieri, L.; Imperio, D.; Erhard, A.; Fallarini, S.; Compostella, F.; Del Grosso, E.; Balcerzyk, M.; Panza, L. Organotrifluoroborate Sugar Conjugates for a Guided Boron Neutron Capture Therapy: From Synthesis to Positron Emission Tomography. ACS Omega 2022, 7, 48340–48348. [Google Scholar] [CrossRef]
- Chen, X.-P.; Hsu, F.-C.; Huang, K.-Y.; Hsieh, T.-S.; Farn, S.-S.; Sheu, R.-J.; Yu, C.-S. Fluorine-18 Labeling PEGylated 6-Boronotryptophan for PET Scanning of Mice for Assessing the Pharmacokinetics for Boron Neutron Capture Therapy of Brain Tumors. Bioorganic & Medicinal Chemistry Letters 2024, 105, 129744. [Google Scholar] [CrossRef] [PubMed]
- Dąbrowska, A.; Matuszewski, M.; Zwoliński, K.; Ignaczak, A.; Olejniczak, A.B. Insight into Lipophilicity of Deoxyribonucleoside-boron Cluster Conjugates. European Journal of Pharmaceutical Sciences 2018, 111, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Kaniowski, D.; Ebenryter-Olbińska, K.; Sobczak, M.; Wojtczak, B.; Janczak, S.; Leśnikowski, Z.; Nawrot, B. High Boron-Loaded DNA-Oligomers as Potential Boron Neutron Capture Therapy and Antisense Oligonucleotide Dual-Action Anticancer Agents. Molecules 2017, 22, 1393. [Google Scholar] [CrossRef] [PubMed]
- Goszczyński, T.M.; Fink, K. Metallacarboranes: Abiotic Scaffolds for Advanced Drug Discovery. Future Medicinal Chemistry 2025, 17, 2193–2196. [Google Scholar] [CrossRef]
- Mallesch, J.L.; Moore, D.E.; Allen, B.J.; McCarthy, W.H.; Jones, R.; Stening, W.A. The Pharmacokinetics of P-Boronophenylalanine.Fructose in Human Patients with Glioma and Metastatic Melanoma. International Journal of Radiation Oncology*Biology*Physics 1994, 28, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- Kiger; Iii, W.S.; Palmer, M.R.; Riley, K.J.; Zamenhof, R.G.; Busse, P.M. A Pharmacokinetic Model for the Concentration of10 B in Blood after Boronophenylalanine-Fructose Administration in Humans. Radiation Research 2001, 155, 611–618. [Google Scholar] [CrossRef]
- Ailuno, G.; Balboni, A.; Caviglioli, G.; Lai, F.; Barbieri, F.; Dellacasagrande, I.; Florio, T.; Baldassari, S. Boron Vehiculating Nanosystems for Neutron Capture Therapy in Cancer Treatment. Cells 2022, 11, 4029. [Google Scholar] [CrossRef] [PubMed]
- Barth, R.F.; Kabalka, G.W.; Yang, W.; Huo, T.; Nakkula, R.J.; Shaikh, A.L.; Haider, S.A.; Chandra, S. Evaluation of Unnatural Cyclic Amino Acids as Boron Delivery Agents for Treatment of Melanomas and Gliomas. Applied Radiation and Isotopes 2014, 88, 38–42. [Google Scholar] [CrossRef]
- Weissfloch, L.; Wagner, M.; Probst, T.; Senekowitsch-Schmidtke, R.; Tempel, K.; Molls, M. A New Class of Drugs for BNCT? Borylated Derivatives of Ferrocenium Compounds in Animal Experiments. Biometals 2001, 14, 43–49. [Google Scholar] [CrossRef]
- Kalot, G.; Godard, A.; Busser, B.; Pliquett, J.; Broekgaarden, M.; Motto-Ros, V.; Wegner, K.D.; Resch-Genger, U.; Köster, U.; Denat, F.; et al. Aza-BODIPY: A New Vector for Enhanced Theranostic Boron Neutron Capture Therapy Applications. Cells 2020, 9, 1953. [Google Scholar] [CrossRef]
- Huang, W.; Pan, Y.; Zhong, T.; He, S.; Qi, Y.; Huang, Y. Near-Infrared 10B-BODIPY for Precise Guidance of Tracer Imaging and Treatment in Boron Neutron Capture Therapy. Chem. Commun. 2025, 61, 9079–9082. [Google Scholar] [CrossRef] [PubMed]
- Shao, C.; Lian, G.; Jin, G. Nido-Carborane Encapsulated by BODIPY Zwitterionic Polymers: Synthesis, Photophysical Properties and Cell Imaging. Journal of Saudi Chemical Society 2021, 25, 101345. [Google Scholar] [CrossRef]
- Ordóñez-Hernández, J.; Planas, J.G.; Núñez, R. Carborane-Based BODIPY Dyes: Synthesis, Structural Analysis, Photophysics and Applications. Front. Chem. 2024, 12, 1485301. [Google Scholar] [CrossRef]
- Kumar, P.P.P.; Saxena, S.; Joshi, R. BODIPY Dyes: A New Frontier in Cellular Imaging and Theragnostic Applications. Colorants 2025, 4, 13. [Google Scholar] [CrossRef]
- Blethen, K.E.; Arsiwala, T.A.; Fladeland, R.A.; Sprowls, S.A.; Panchal, D.M.; Adkins, C.E.; Kielkowski, B.N.; Earp, L.E.; Glass, M.J.; Pritt, T.A.; Cabuyao, Y.M.; Aulakh, S.; Lockman, P. Modulation of the Blood-Tumor Barrier to Enhance Drug Delivery and Efficacy for Brain Metastases. Neuro-Oncology Advances 2021, 3, v133–v143. [Google Scholar] [CrossRef]
- Yoshida, F.; Matsumura, A.; Yamamoto, T.; Kumada, H.; Nakai, K. Enhancement of Sodium Borocaptate (BSH) Uptake by Tumor Cells Induced by Glutathione Depletion and Its Radiobiological Effect. Cancer Letters 2004, 215, 61–67. [Google Scholar] [CrossRef]
- Wittig, A.; Stecher-Rasmussen, F.; Hilger, R.A.; Rassow, J.; Mauri, P.; Sauerwein, W. Sodium Mercaptoundecahydro-Closo-Dodecaborate (BSH), a Boron Carrier That Merits More Attention. Applied Radiation and Isotopes 2011, 69, 1760–1764. [Google Scholar] [CrossRef]
- Lan, G.; Song, Q.; Luan, Y.; Cheng, Y. Targeted Strategies to Deliver Boron Agents across the Blood–Brain Barrier for Neutron Capture Therapy of Brain Tumors. International Journal of Pharmaceutics 2024, 650, 123747. [Google Scholar] [CrossRef] [PubMed]
- Sumitani, S.; Oishi, M.; Yaguchi, T.; Murotani, H.; Horiguchi, Y.; Suzuki, M.; Ono, K.; Yanagie, H.; Nagasaki, Y. Pharmacokinetics of Core-Polymerized, Boron-Conjugated Micelles Designed for Boron Neutron Capture Therapy for Cancer. Biomaterials 2012, 33, 3568–3577. [Google Scholar] [CrossRef]
- Chen, W.; Mehta, S.C.; Lu, D.R. Selective Boron Drug Delivery to Brain Tumors for Boron Neutron Capture Therapy. Advanced Drug Delivery Reviews 1997, 26, 231–247. [Google Scholar] [CrossRef]
- Sprowls, S.A.; Arsiwala, T.A.; Bumgarner, J.R.; Shah, N.; Lateef, S.S.; Kielkowski, B.N.; Lockman, P.R. Improving CNS Delivery to Brain Metastases by Blood–Tumor Barrier Disruption. Trends in Cancer 2019, 5, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Barth, R.F.; Yang, W.; Rotaru, J.H.; Moeschberger, M.L.; Boesel, C.P.; Soloway, A.H.; Joel, D.D.; Nawrocky, M.M.; Ono, K.; Goodman, J.H. Boron Neutron Capture Therapy of Brain Tumors: Enhanced Survival and Cure Following Blood–Brain Barrier Disruption and Intracarotid Injection of Sodium Borocaptate and Boronophenylalanine. International Journal of Radiation Oncology*Biology*Physics 2000, 47, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Barth, R.F.; Yang, W.; Bartus, R.T.; Moeschberger, M.L.; Goodman, J.H. Enhanced Delivery of Boronophenylalanine for Neutron Capture Therapy of Brain Tumors Using the Bradykinin Analog Cereport (Receptor-Mediated Permeabilizer-7). Neurosurgery 1999, 44, 351–359. [Google Scholar] [CrossRef]
- Yang, W.; Barth, R.F.; Rotaru, J.H.; Moeschberger, M.L.; Joel, D.D.; Nawrocky, M.M.; Goodman, J.H.; Soloway, A.H. Boron Neutron Capture Therapy of Brain Tumors: Enhanced Survival Following Intracarotid Injection of Sodium Borocaptate with or without Blood-Brain Barrier Disruption. International Journal of Radiation Oncology*Biology*Physics 1997, 37, 663–672. [Google Scholar] [CrossRef]
- Garg, T.; Bhandari, S.; Rath, G.; Goyal, A.K. Current Strategies for Targeted Delivery of Bio-Active Drug Molecules in the Treatment of Brain Tumor. Journal of Drug Targeting 2015, 23, 865–887. [Google Scholar] [CrossRef]
- Marforio, T.D.; Carboni, A.; Calvaresi, M. In Vivo Application of Carboranes for Boron Neutron Capture Therapy (BNCT): Structure, Formulation and Analytical Methods for Detection. Cancers 2023, 15, 4944. [Google Scholar] [CrossRef]
- Kulvik, M.E.; Vähätalo, J.K.; Benczik, J.; Snellman, M.; Laakso, J.; Hermans, R.; Järviluoma, E.; Rasilainen, M.; Färkkilä, M.; Kallio, M.E. Boron Biodistribution in Beagles after Intravenous Infusion of 4-Dihydroxyborylphenylalanine–Fructose Complex. Applied Radiation and Isotopes 2004, 61, 975–979. [Google Scholar] [CrossRef]
- Zhou, T. The Current Status and Novel Advances of Boron Neutron Capture Therapy Clinical Trials. Am J Cancer Res 2024, 14, 429–447. [Google Scholar] [CrossRef]
- Barth, R.F.; Gupta, N.; Kawabata, S. Evaluation of Sodium Borocaptate (BSH) and Boronophenylalanine (BPA) as Boron Delivery Agents for Neutron Capture Therapy (NCT) of Cancer: An Update and a Guide for the Future Clinical Evaluation of New Boron Delivery Agents for NCT. Cancer Communications 2024, 44, 893–909. [Google Scholar] [CrossRef]
- Puris, E.; Gynther, M.; Auriola, S.; Huttunen, K.M. L-Type Amino Acid Transporter 1 as a Target for Drug Delivery. Pharm Res 2020, 37, 88. [Google Scholar] [CrossRef]
- Silva, M.P.; Saraiva, L.; Pinto, M.; Sousa, M.E. Boronic Acids and Their Derivatives in Medicinal Chemistry: Synthesis and Biological Applications. Molecules 2020, 25, 4323. [Google Scholar] [CrossRef]
- Llenas, M.; Cuenca, L.; Santos, C.; Bdikin, I.; Gonçalves, G.; Tobías-Rossell, G. Sustainable Synthesis of Highly Biocompatible 2D Boron Nitride Nanosheets. Biomedicines 2022, 10, 3238. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, F. Boron Nanocomposites for Boron Neutron Capture Therapy and in Biomedicine: Evolvement and Challenges. Biomater Res 2025, 29, 0145. [Google Scholar] [CrossRef] [PubMed]
- Rudawska, A.; Szermer-Olearnik, B.; Szczygieł, A.; Mierzejewska, J.; Węgierek-Ciura, K.; Żeliszewska, P.; Kozień, D.; Chaszczewska-Markowska, M.; Adamczyk, Z.; Rusiniak, P.; Wątor, K.; Rapak, A.; Pędzich, Z.; Pajtasz-Piasecka, E. Functionalized Boron Carbide Nanoparticles as Active Boron Delivery Agents Dedicated to Boron Neutron Capture Therapy. IJN 2025, 20, 6637–6657. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.; Lv, L.; Chang, Y.; Li, J.; Xing, G.; Chen, K. Boron Nanodrugs for Boron Neutron Capture Therapy. Applied Radiation and Isotopes 2025, 225, 112044. [Google Scholar] [CrossRef]
- Wang, L.-W.; Liu, Y.-W.H.; Chu, P.-Y.; Liu, H.-M.; Peir, J.-J.; Lin, K.-H.; Huang, W.-S.; Lo, W.-L.; Lee, J.-C.; Lin, T.-Y.; Liu, Y.-M.; Yen, S.-H. Boron Neutron Capture Therapy Followed by Image-Guided Intensity-Modulated Radiotherapy for Locally Recurrent Head and Neck Cancer: A Prospective Phase I/II Trial. Cancers 2023, 15, 2762. [Google Scholar] [CrossRef]
- Baker, S.J.; Ding, C.Z.; Akama, T.; Zhang, Y.-K.; Hernandez, V.; Xia, Y. Therapeutic Potential of Boron-Containing Compounds. Future Med. Chem. 2009, 1, 1275–1288. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Liu, L.; Hu, Z.; Lu, Y.; Liu, Q.; Jin, S.; Zhang, Q.; Zhao, S.; Chou, S. Understanding High-Rate K + -Solvent Co-Intercalation in Natural Graphite for Potassium-Ion Batteries. Angew. Chem. Int. Ed. 2020, 59, 12917–12924. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Shi, S.; Yi, J.; Wang, N.; He, Y.; Wu, Z.; Peng, J.; Deng, Y.; Wang, W.; Wu, C.; Lyu, A.; Zeng, X.; Zhao, W.; Hou, T.; Cao, D. ADMETlab 3.0: An Updated Comprehensive Online ADMET Prediction Platform Enhanced with Broader Coverage, Improved Performance, API Functionality and Decision Support. Nucleic Acids Research 2024, 52, W422–W431. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PBPK-informed irradiation windows for BNCT (schematic; not to scale). Illustrative tumour and blood/normal-tissue relative 10^{10} of 10B concentration–time profiles showing how the usable irradiation window depends on time-varying selectivity (e.g., T/B ≥ 3) and an exposure constraint in blood/normal tissue. Panel A: favourable window with sustained tumour retention and faster decline in blood/normal tissue. Panel B: rapid washout and insufficient selectivity. Panel C: delayed window due to prolonged systemic exposure despite high tumour uptake. Thresholds are illustrative and protocol- and agent-specific.
Figure 1.
PBPK-informed irradiation windows for BNCT (schematic; not to scale). Illustrative tumour and blood/normal-tissue relative 10^{10} of 10B concentration–time profiles showing how the usable irradiation window depends on time-varying selectivity (e.g., T/B ≥ 3) and an exposure constraint in blood/normal tissue. Panel A: favourable window with sustained tumour retention and faster decline in blood/normal tissue. Panel B: rapid washout and insufficient selectivity. Panel C: delayed window due to prolonged systemic exposure despite high tumour uptake. Thresholds are illustrative and protocol- and agent-specific.
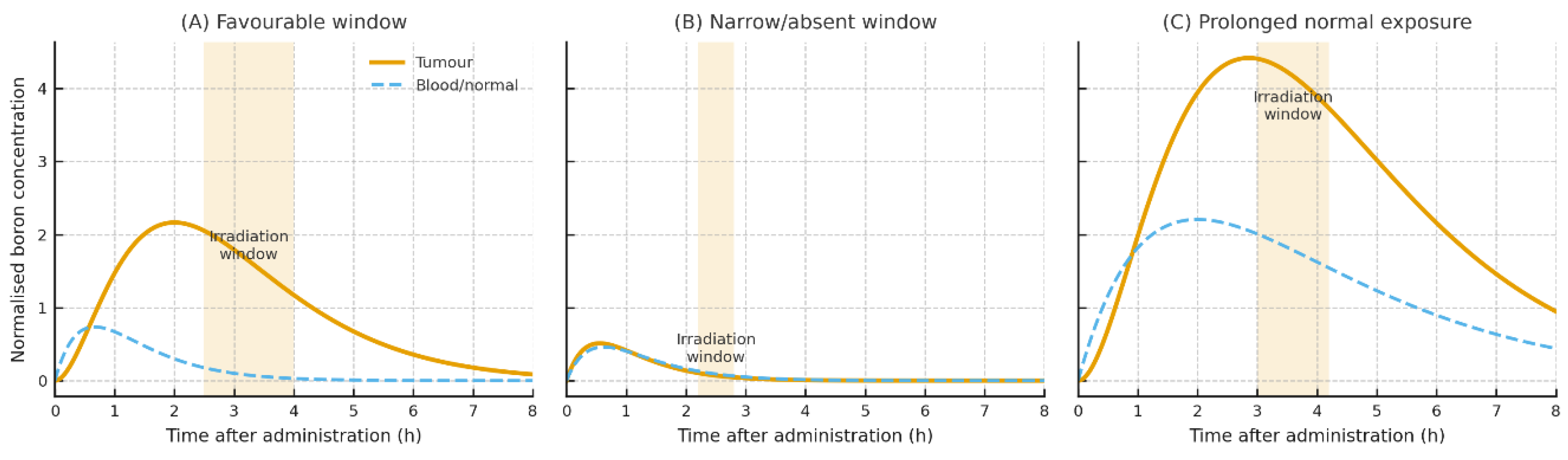
Figure 2.
ADMET-guided design control map for BNCT carriers. For each ADMET pillar (Absorption, Distribution, Metabolism, Excretion and Toxicity), target exposure and safety profiles are linked to concrete design levers (physicochemical properties, carrier architecture and targeting biology) and to representative BNCT carrier archetypes (small molecules, peptide/ligand conjugates, polymeric and inorganic nanocarriers and cell-based delivery systems).
Figure 2.
ADMET-guided design control map for BNCT carriers. For each ADMET pillar (Absorption, Distribution, Metabolism, Excretion and Toxicity), target exposure and safety profiles are linked to concrete design levers (physicochemical properties, carrier architecture and targeting biology) and to representative BNCT carrier archetypes (small molecules, peptide/ligand conjugates, polymeric and inorganic nanocarriers and cell-based delivery systems).
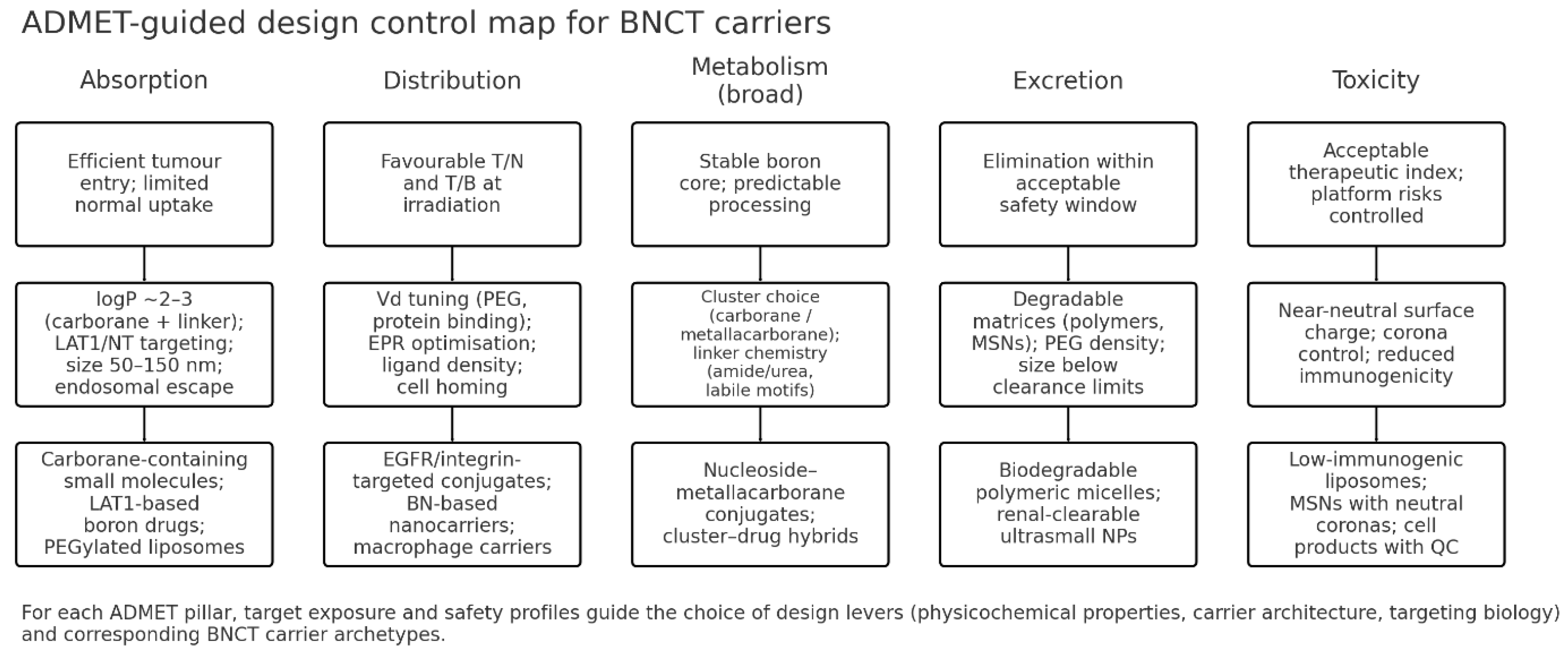

Table 1.
(revised). ADMET Parameters Related to Absorption of Representative Boron-Containing Compounds.
Table 1.
(revised). ADMET Parameters Related to Absorption of Representative Boron-Containing Compounds.
| Representative (example) | Class / format | Absorption determinants | Principal uptake pathway | Absorption-enhancing strategies | Key caveats (absorption) | Representative refs (updated) |
| Boronophenylalanine (BPA) / BPA–fructose | Low-MW amino-acid analogue | Hydrophilicity; LAT1 engagement; formulation (fructose) | Carrier (LAT1) ± limited diffusion | Transporter targeting; clinical formulation (BPA-F) | Heterogeneous uptake across tumours | [8,10,14,23,29,31,32,40] |
| Sodium borocaptate (BSH) | Low-MW polyhydroborate | Extreme hydrophilicity; minimal permeability | Primarily extracellular | High-dose/infusion; carrier-assisted approaches | Rapid renal clearance; modest selectivity | [1,3,11,12,23] |
| Metallacarborane-modified nucleosides / DNA-affine constructs | Small molecules with carborane clusters | Moderate logP (~2–3); compactness; linker stability | Passive uptake; endocytic contributions | Balance polarity; endosomal-escape motifs | Lysosomal trapping if over-hydrophobic | [7,13,14,15,23,41,42,43,44] |
| Peptide / ligand-targeted conjugates (e.g., RGD, EGFR) | Targeted bioconjugates | Affinity/avidity; receptor density; linker stability | Receptor-mediated endocytosis | Valency optimisation; protease-resistant backbones | Variable receptor expression; endosomal sequestration | [14,18,19,23,33,37,45,46,47] |
| PEGylated boronated liposomes / dendrimers | Polymeric / lipid nanocarriers (≈50–150 nm) | Size; PEG stealth; near-neutral charge | Endocytosis; EPR-mediated tissue entry | PEGylation; size tuning; long-circulating designs | RES uptake if insufficient stealth | [2,11,16,17,23,29,30,31,32,48,49,50,51,52] |
| Functionalised mesoporous silica nanoparticles | Inorganic nanocarriers | Pore/ligand functionalisation; size/shape | Clathrin/caveolin-mediated endocytosis | Ligand grafting; pH-labile gates | Biodegradation timescale context-dependent | [20,21,23,53,54,55,56] |
| Cell-based delivery (e.g., macrophages) | Cellular carriers | Cell homing; payload loading | Active trafficking into tumour microenvironments | Optimise loading/release; exploit chemotaxis | Biological variability | [23,24] |
| Selected PET-oriented tracers (boronated amino acids, sugars) | Low-MW tracers (diagnostic) | Transporter targeting; radiolabelling | Carrier-mediated uptake (LAT1, sugar transporters) | PEGylation/sugar conjugation for uptake/PK | Translation to therapy requires exposure matching | [38,39,57,58] |
Table 2.
(revised). ADMET Parameters Related to Distribution of Representative Boron-Containing Compounds.
Table 2.
(revised). ADMET Parameters Related to Distribution of Representative Boron-Containing Compounds.
| Representative (example) | Distribution determinants | Typical biodistribution pattern | Selectivity (T/N; T/B) | BBB / organ targeting | Distribution-enhancing strategies | Representative refs (updated) |
| BPA / BPA-fructose | LAT1 density; hydrophilicity; short t½ | Tumour uptake in LAT1-high tissues; low Vd | Glioma PET ~2–3+ (context-dependent) | Partial BBB via LAT1 | Timing vs irradiation; formulation | [8,10,14,23,34,40,86] |
| BSH | Hydrophilicity; extracellular confinement | Blood/kidney/liver; modest tumour deposition | Lower than BPA | Poor BBB penetration | Carrier-assisted delivery | [1,11,12,23,34,86] |
| Metallacarborane/DNA-affine constructs | Lipophilicity; nuclear affinity; linker routing | Enhanced cellular/nuclear localisation | Improved local (organelle) targeting | BBB depends on scaffold | Endosomal-escape/linker tuning | [13,14,15,23,41,43,44] |
| Targeted peptides/ligands | Receptor density; valency; stability | Receptor-positive tumour deposition; off-target varies | Higher apparent selectivity with high receptor expression | Transcytosis possible with ligands | Ligand grafting; protease resistance | [14,18,19,23,33,34,35,37,47,86] |
| PEGylated liposomes/dendrimers | PEG stealth; size/charge; corona | Tumour + liver/spleen; prolonged circulation | EPR-driven (model-dependent) | BBB limited; ligand-enhanced entry | Stealth; size tuning; long-circulating designs | [11,15,16,17,23,34,35,48,49,50,51,52] |
| Functionalised MSNs | Surface chemistry; porosity; corona | Tumour (EPR) and liver/spleen | Improved with targeting ligands | BBB limited; ligand-mediated routes | Ligand grafting; neutral corona design | [20,21,23,34,53,54,55,87] |
| Cell-based carriers | Homing to hypoxia/inflammation; cell kinetics | Uniform intratumoural distribution incl. hypoxic zones | Favourable functional selectivity | Cells traverse barriers | Preconditioning; loading optimisation | [23,24,34] |
| Borylated ferrocenium (animal data) | Organotropism of cationic complexes | Liver/spleen/kidney predominant sinks | — | — | — | [66] |
Table 3.
(revised). ADMET Parameters Related to Metabolism of Representative Boron-Containing Compounds.
Table 3.
(revised). ADMET Parameters Related to Metabolism of Representative Boron-Containing Compounds.
| Representative (example) | Metabolic liability / processing | Intracellular fate & trafficking | Linker chemistry / trigger | Stability-/release-enhancing strategies | Key caveats (metabolism) | Representative refs (updated) |
| BPA / BPA-fructose | Minimal biotransformation; transporter-driven behaviour | Cytosolic pool; relatively rapid egress without sustained LAT1 | — | Formulation and scheduling to delay efflux | Heterogeneous LAT1; rapid washout | [8,10,14,23,40] |
| BSH | Negligible conversion; renal elimination | Largely extracellular | — | Encapsulation/conjugation | Limited cell entry | [1,3,11,12,23] |
| Metallacarborane/DNA-affine | Carborane inert; linker is liability | Risk of endo-lysosomal trapping; possible nuclear localisation | Stable amide/urea; steric shielding | Balance logP; add endosomal-escape motifs | Over-hydrophobicity → sequestration | [13,14,15,23,41,42,43,44,88] |
| Peptide/ligand conjugates | Proteolysis; endo-lysosomal degradation | Endocytosis; recycling vs degradation | Protease-resistant backbones; cleavable linkers | Cyclisation; PEG spacers; valency tuning | Premature plasma cleavage | [14,15,18,19,23,33,47,83] |
| PEGylated liposomes/dendrimers | Colloidal stability and corona drive fate; limited enzyme metabolism | Endosomal-lysosomal routing unless engineered | pH-responsive gates; cleavable spacers | Increase stealth; tune size/charge; endosomolytic features | RES processing if insufficient stealth | [11,15,16,17,23,48,49,50,51,52,56] |
| Functionalised MSNs | Biodegradation to silicic acid; corona-driven processing | Lysosomal residence if ungated | pH/enzyme-labile gatekeepers; ligand shells | Surface chemistry control; triggerable gates | Long-term retention if slow degradation | [20,21,23,53,54,55,56] |
| Cell-based carriers | Cellular processing of payload; no chemical metabolism of boron core | Deep tumour homing; sustained presence | Payload-specific | Optimise loading/release; preserve viability | Biological variability | [23,24] |
Table 4.
(revised). ADMET Parameters Related to Excretion of Representative Boron-Containing Compounds.
Table 4.
(revised). ADMET Parameters Related to Excretion of Representative Boron-Containing Compounds.
| Representative (example) | Primary elimination route(s) | Determinants of clearance | Organ retention / sinks | Excretion-optimising strategies | Key caveats | Representative refs (updated) |
| BPA / BPA-fructose | Renal (filtration) | Hydrophilicity; transporter-mediated tissue egress | Kidney exposure during infusion; transient tumour retention | Schedule vs tumour peak; delay efflux where feasible | Rapid washout in LAT1-heterogeneous tumours | [3,8,23,30,31,32,40] |
| BSH | Renal (rapid) | Extreme hydrophilicity; poor cell entry | Kidney; minimal tumour residence | Encapsulation/conjugation | High dosing without carriers | [1,3,11,12,23] |
| Peptide/ligand conjugates | Renal for small conjugates/catabolites; hepatobiliary if plasma-bound | Proteolysis; linker stability; receptor cycling | Lysosomes; liver (if opsonised) | Protease-resistant designs; tuned cleavable linkers | Premature cleavage in plasma | [11,14,15,18,23,33,47,83] |
| PEGylated liposomes / dendrimers | Predominantly hepatobiliary; renal for fragments | PEG density; size/charge; protein corona | Liver, spleen (MPS/RES) | Increase stealth; degradable matrices | Long-term retention if non-degradable | [2,11,16,17,23,48,49,50,51] |
| Functionalised MSNs | Hepatobiliary (slow); urinary for soluble products | Size/porosity; surface chemistry; corona; biodegradation | Liver/spleen; gradual degradation to silicic acid | Gatekeepers/ligands; design for biodegradation | Clearance timescale context-dependent | [20,21,23,53,54,55,56] |
| Cell-based carriers | Biological turnover; lymphatic/hepatic routes | Carrier viability; payload stability | Tumour phagocytes; lymph nodes; liver | Optimise loading/release; ensure viability | Biological variability; regulatory complexity | [23,24] |
| Historical organ distribution example (ferrocenium derivatives) | Mixed; organ sequestration → slow clearance | Cationic complex behaviour | Liver/spleen/kidney predominant sinks | — | Preclinical context | [66] |
Table 5.
Toxicity/Safety Considerations for Representative Boron-Containing Agents.
| Representative (example) | Principal toxicity endpoints | Mechanistic drivers | Organs at risk | Mitigation strategies | Clinical/Preclinical notes | Representative refs |
| Boronophenylalanine (BPA) / BPA–fructose | Infusion-related symptoms (nausea, flushing); field-limited RT-like AEs during BNCT (mucositis, dermatitis) | Transporter-driven normal-tissue uptake (LAT1); exposure at irradiation if T/B suboptimal | Oral mucosa/skin in field; kidney (exposure during infusion) | PET selection; schedule to peak T/B; supportive care protocols | Systemic toxicity generally mild–moderate at clinical dosing with proper scheduling | [3,4,5,8,10,14,23,40,76,85,91,93] |
| Sodium borocaptate (BSH) | RT-like AEs in field; limited systemic toxicity | Extracellular distribution; blood concentrations at irradiation | Kidney (rapid renal handling); liver (minor) | Dose planning to minimise normal-tissue dose; consider carriers to improve selectivity | Conservative safety margins when scheduling is respected | [1,11,12,23,84,86] |
| Targeted peptides/ligand conjugates | Potential immunogenicity; off-target binding; infusion reactions (rare) | Proteolysis; receptor expression in normal tissues; endosomal trapping | Receptor-positive normal tissues; liver (if opsonised) | Protease-resistant designs; validate receptor maps; premedication/infusion-rate control | Risk profile depends on target expression and linker chemistry | [14,15,18,19,23,33,37,83,95] |
| PEGylated liposomes / polymeric dendrimers | Complement activation; hepatic/splenic deposition; infusion reactions | Protein corona → MPS (RES) uptake; insufficient stealth; cationic surfaces | Liver, spleen; blood (infusion) | Increase PEG density; near-neutral charge; graded dosing; endosomolytic features within safe range | Monitoring liver enzymes; mitigate CARPA-like events if relevant | [11,15,16,17,23,48,49,50,51,52,56] |
| Functionalised mesoporous silica nanoparticles (MSNs) | Inflammation with prolonged retention; long-term organ sequestration if slow degradation | Slow biodegradation to silicic acid; corona-modulated responses | Liver, spleen; reticuloendothelial system | Design for controlled post-treatment degradation; neutral corona; dose staggering | Favourable profiles when degradability and surface chemistry are optimised | [20,21,23,53,54,55,56] |
| Cell-based carriers (e.g., macrophages) | Immune activation/cytokine-related events; ectopic accumulation | Cell persistence/activation state; payload stability | Liver/spleen (clearance); lymph nodes; tumour microenvironment | GMP manufacturing; viability/release criteria; clinical monitoring | Preclinical studies show tumour homing with limited systemic redistribution of inert payloads | [23,24] |
| Imaging-oriented boron tracers (e.g., ^18F-labelled amino acids, sugars) | Low systemic toxicity at tracer doses | Transporter-mediated uptake; rapid clearance | Kidney; field-specific effects not applicable (diagnostic use) | Standard radiotracer safety; QC of radiochemistry | Useful for selection/scheduling; not therapeutic on their own | [8,38,39,40,48,57] |
| Historical ferrocene-based boron agents (preclinical) | Organ sequestration-related concerns | Cationic complex organotropism | Liver, spleen, kidney | Preclinical toxicity mapping; not for routine clinical use | Context for organ-level safety considerations | [66] |
Table 6.
In silico toolbox for ADMET-guided BNCT (overview).
| Tool / framework | Primary purpose | Typical inputs | Key outputs for BNCT | Use case in this review | Representative refs |
| Drug-likeness/BCS rules (RO5; Veber; BCS) | Rapid prescreen of solubility/permeability risk and formulation needs | Calculated physicochemical properties; class-based thresholds | Risk flags for absorption limits; oral bioavailability heuristics | Prioritise linker/scaffold variants for small boron agents | [29,30,31] |
| ADMETlab-style prediction (ADMETlab 3.0) | Batch prediction of ADME/T surrogates to rank candidates | SMILES/structure; descriptor set | Absorption/distribution/toxicity descriptors; comparative scores | Side-by-side evaluation of linker placements and polarity tuning | [96] |
| Transporter-aware modelling (LAT1 focus) | Assess transporter contribution vs passive permeation | Docking/LB models; ionisation; permeability estimates | Uptake likelihood via LAT1; interaction risk with transporters | Classify agents as transporter-dominant vs permeation-feasible | [10,14,33,47,87] |
| PET-informed PBPK | Time-aligned exposure modelling and irradiation scheduling | ^18F-BPA/sugar PET kinetics; plasma/biopsy boron; physiological priors | Tumour-to-blood trajectories; schedule windows; sensitivity analyses | Place neutron exposure at peak/plateau selectivity | [8,40,64,84] |
| Nano-clearance modelling (MPS/biodegradation) | Anticipate organ retention and elimination for carriers | Size/charge/PEG density; corona data; degradability parameters | Hepatobiliary vs renal balance; residence times; risk flags | Balance exposure with clearance; design degradability “timers” | [11,15,16,17,48,49,50,52,53,54,55,56] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



