Submitted:
16 December 2025
Posted:
17 December 2025
You are already at the latest version
Abstract
This study examines the community integration and One Health strategies employed to fight Ebola virus disease in the Democratic Republic of Congo in the years 2007–2022. We synthesized twelve outbreak reports and conducted qualitative interviews of thirty-six managers and three focus groups and adapted an analytical framework (MATCH) to evaluate three essential dimensions: integration of the One Health approach, community involvement, and bottom-up approaches. This study found evidence of progressive improvement in all domains. The first outbreaks (2007–2009) were marked by moderate community engagement and a One Health approach that was mostly limited to the human health sector, which was deemed suboptimal. The 10th outbreak represented an era of transformation, when the Incident Management System (IMS) was adopted to better manage the response to the virus. The latest outbreaks (13th to 15th) show “optimal” implementation of the “One Health” approach through effective collaboration among those in charge of ensuring human, animal, and environmental health and the community. This study demonstrates that success is largely dependent on bottom-up initiatives where local populations, their leaders (both traditional and religious leaders), community liaisons, and specific groups (women and youth) are involved in the design and implementation of such measures. The inclusion of anthropologists and psychologists in addressing the psychosocial dimensions—fear, stigma, and distress—has been critical in ensuring the success of these initiatives and the degree to which the public trust and accept them. However, there are many issues that still need to be addressed, including poor coordination between sectoral ministries and the partial implementation of IMS at the grassroots level. In summary, the authors of this study propose that these integrated and participatory models are sustainable and imperative to building the resilience of the Congolese health system to future outbreaks.
Keywords:
practices
; community
; incident management system
; Ebola outbreaks
; one health
1. Introduction
Pandemics and disease outbreaks are becoming increasingly prevalent around the world, killing large parts of the population, despite the wide range of approaches that have been put in place to prevent them. In Africa, the trajectory of these health emergencies shows that health systems should take an integrated and participatory approach, in which community members have a central voice in the management and prevention of diseases [1]. Community participation, as well as an integrated, intersectoral approach called “One Health”—which acknowledges the interrelations among human, animal, and environmental health—is increasingly regarded as an important factor in optimizing surveillance of and responses to zoonotic crises like Ebola virus disease (EVD) [2]. As a collaborative, multisectoral, and transdisciplinary approach, it must take place at local, regional, national, and global levels to achieve optimal health and well-being outcomes [3].
The Democratic Republic of Congo (DRC) has faced several public health emergencies, including the COVID-19 pandemic and EVD outbreaks. The initial EVD outbreaks in the DRC were first thought to be salmonella infections, and later viral hemorrhagic fevers, with the diagnosis of Ebola made late [4]. Unhealthy behavior among resistant communities frequently fosters scenarios which promote the spread and continuation of the disease, making the task of responding to outbreaks challenging [5]. Community buy-in to these response strategies is often slow, and affected people often resist the proposed medical interventions, for example, because of insufficient community engagement in the early phase of the crisis.
In the DRC, community trust had to be established, as follow-up outbreaks occurred. Through risk communication and community outreach, the healthcare system aimed to minimize the transmission of the disease and quickly suppress outbreaks. For this reason, the World Health Organization (WHO), World Organisation for Animal Health, Food and Agriculture Organization (FAO), and United Nations Environment Programme have accepted that the “One Health” design is best executed when local participation underpins all surveillance and response actions [6]. Moreover, the effective design and implementation of community engagement and the “One Health” approach are essential: while state-enforced and expert-imposed community or intersectoral “top-down” involvement is quicker to roll out, it is far less effective than “bottom-up” approaches [7]. These approaches place stakeholders at the forefront, including those impacted by the community and by community development or field actors, to achieve a response that ensures the implementation of interventions.
This manuscript aims to investigate the effectiveness of community engagement strategies in managing EVD outbreaks in the DRC. The primary research question guiding this study is: "How do community engagement strategies influence the response to EVD outbreaks, and what can be learned to enhance public health interventions in future viral outbreaks?".
This work contributes to the existing body of knowledge by integrating the "One Health" approach, which emphasizes the interconnectedness of human, animal, and environmental health. Our findings highlight the critical role that community involvement plays in shaping public health responses, particularly in resource-limited settings. By analyzing case studies and community feedback, we aim to provide evidence-based recommendations for improving outbreak management strategies, thereby informing policy and practice at local, national, and international levels. Through this research, we seek to bridge the gap between theoretical knowledge and practical application, illustrating how effective community engagement can lead to better health outcomes during viral outbreaks. This study not only enhances our understanding of EVD management but also offers valuable insights applicable to other emerging infectious diseases.
2. Materials and Methods
Through documentary and qualitative analysis, this study seeks to examine the modalities of implementation of community engagement and the “One Health” approach in the management of Ebola outbreaks in the DRC.
2.1. Documentary Sources
We carried out an analysis of 12 formal documents on management of the Ebola outbreak in the DRC from 2007 to 2022, that is, from the 4th to the 15th outbreaks [8,9,10,11,12,13,14]. These reports were produced by the Ministry of Public Health, the WHO, and partner organizations involved in the successive responses. All of the official reports described the coordination measures, community interventions, results achieved, and recommendations made following each crisis.
2.2. Analytical Framework
To gain an insight into the recent experiences and practices of surveilling and treating Ebola by involving the community in a “One Health” approach (Table 1), a literature review was conducted, using an adaptation of Simons’ (Appendix A) [15,16] Multi-Level Approach to Community Health (MATCH) conceptual model as an intervention model [17]. This framework was adjusted to assess three key dimensions (Figure 1):
- o The integration of the “One Health” approach: whether the human, animal, and environmental health sectors are integrated into the response or not.
- o Community involvement: degree of participation of local communities in actions to prevent, monitor, and manage outbreaks.
- o Techniques applied from the bottom up: community involvement in designing and implementing strategies.
A qualitative analysis grid was developed based on these dimensions to methodically inspect each outbreak management report. Integration levels were coded according to qualitative parameters (optimal to suboptimal; good to low involvement; and applied to non-applied).
2.3. Qualitative Data
In addition to analyzing the documents, 36 interviews were carried out with central and local managers from different sectors. To enrich our data on community perspectives, we conducted interviews with three focus groups, each with 28 participants. The criteria for being included in the research, the method of data collection, and the sociodemographic profiles of the interviewees are summarized in Table 2 and discussed in a separate article [1]. Due to the significance of psychological distress, fear, and stigma in determining the effectiveness of community engagement [18], these factors were also assessed to gauge the degree to which they should be considered when establishing practical approaches to managing health emergencies like Ebola outbreaks.
3. Results
3.1. Evaluation of Indicators from the 4th to the 15th Ebola Outbreak in the DRC
The results of the documentary analysis of reports from the 4th to the 15th Ebola outbreaks in the DRC are presented in Table 2. We also describe the models of Ebola outbreak management before and after 2017, followed by an analysis of the implementation of the One Health approach and the significance of fear and stigma as key elements in the effectiveness of community involvement according to the “bottom-up” model.
3.2. The Response to Ebola Virus Disease: An Overview
The response to EVD outbreak in the DRC is multisectoral and community-based, aimed at controlling and limiting the spread of the outbreak. The strategies employed include strengthened epidemiological surveillance capacities, rigorous contact tracing, coordination between national and international health authorities, and the promotion of social mobilization and local community engagement. It is important to involve community leaders, women’s groups, and other local influential groups to promote adherence to prevention measures and health interventions, particularly in high-risk areas, and considering the weak security in some contexts.
A “good” or “optimal” response to an outbreak such as EVD in the DRC is defined by several essential criteria (as articulated in national and international strategic response plans): early detection and enhanced surveillance, multisectoral and logistical coordination, strong community engagement, targeted vaccination, adaptability and operational flexibility, and integration of survivor care.
3.3. Transformation of Intervention Models in the Management of Ebola
- (A)
- Outbreak management framework up to 2017
From the third outbreak in Kikwit in 1995 until 2017, the management of outbreaks, including EVD, was based on a tripartite structure comprising a National Coordination Committee, a Provincial Coordination Committee, and an International Scientific and Technical Coordination Committee (ICST) at the epicenter level [19]. At the national level, the National Coordination Committee, under the responsibility of the national Minister of Health, ensures communication between stakeholders and coordinates interventions to guarantee a coherent and effective response. This committee is composed of seven subcommittees: care, surveillance, laboratory and research, water, hygiene and sanitation, social communication, logistics, and psychosocial support.
At the intermediate level, the Provincial Ministry of Health, under the coordination of the Provincial Minister, chairs the Provincial Coordination Committee. This committee is responsible for the smooth implementation of all activities related to the EVD outbreak response. It coordinates interventions at the provincial level and is also subdivided into seven subcommittees.
At the epicenter of the outbreak, there is a coordinator for the CICST, which is also subdivided into seven subcommittees. This model, although organized, struggled to empower local actors in decision-making, with power limited to experts at the central level, as demonstrated by the content of the epidemiological surveillance subcommittee during the outbreaks from 2007 to 2017 (Table 3) [12].
- (B) New WHO outbreak management model adopted in DRC: Incident Management System (IMS)
The 10th outbreak (the longest—nearly 18 months) was considered a watershed, in that the DRC adopted the IMS (Figure 2) as recommended by the WHO [20]. This model states that in case of an event (e.g., outbreak), an Incident Manager (IM) should be appointed by the relevant authorities and that four sectors should be established (operations, logistics, administration and finance, and planning). This led to a more standardized and responsive approach that is now used in managing other health emergencies like MPOX outbreaks. However, effective implementation of this system at the local level remains challenging, particularly in the most remote health zones. Many questionnaire respondents highlighted the need for stronger local integration to enable operation of the Integrated Health System (IHS) in low-resource settings.
3.4. Evolution of Community Integration
The Ebola response in the DRC has moved from a biomedicine-only framework to a successful community integration approach that involves the local population. Initially, mistrust and resistance from the community hindered public acceptance of measures to improve health (vaccination, medical intervention). However, public perception has shifted recently due to systematic inclusivity, including the engagement of community leaders, women’s groups, and other influential groups. Community feedback mechanisms are in place to permit local adaptation of interventions to cultural and social customs, making community ownership of interventions more credible. In addition, policy responses to such actions have been strategically designed to include both psychosocial and humanitarian elements, which is key to sustaining community engagement moving forward by providing better living conditions and addressing community issues.
This evolution has allowed the community to play an active role instead of being a passive recipient, making the public active partners in the response process. Community health workers in Beni and other disease hotspots represent a key component in early detection, awareness-raising, and psychosocial support, improving success in the fight against outbreaks. The trends of community engagement during Ebola outbreaks (in the DRC), which have evolved over time, are as follows:
- o Early outbreaks (2007–2009): First-wave community engagement was, in general, “moderate”, and the adopted approach “suboptimal”. There were efforts to engage the community, but these efforts were not sufficient to optimize the effectiveness of the health intervention.
- o Recent outbreaks (2018–2022): In a case study of recent outbreaks, namely those between 2018 and 2022, community engagement was reported to be “optimal” in some instances, suggesting enhanced community participation and learning [14]. The impacts of the actions taken were also found to be much stronger, leading to higher community engagement and stronger community support in the response process.
3.5. Application/Implementation of the “One Health” Approach
Hunting and forestry are major sources of income in many rural areas. As a result, selling game in local markets is an essential activity; however, it contributes to the spread of EVD within the community [21]. In response to repeated outbreaks, several tactics have been used to fight the disease, such as working with local leaders to encourage adherence to prevention and treatment measures, as well as forming local volunteer organizations tasked with raising awareness of the disease and tracing contacts (report on the 12th outbreak) [22]. The perceptions of the interviewees indicated that community mobilization is as important as biomedical devices in ensuring the effectiveness of response activities [1].
The decision-makers interviewed in this study recognized the importance of the “One Health” approach in countering zoonotic diseases, stating that this approach integrates the efforts of human, animal, and environmental health professionals. The Ministry of Health officials interviewed cited some strengths of intersectoral collaboration, specifically with regard to case detection, risk communication, and field coordination. However, this approach does still have substantial governance-related weaknesses. A number of respondents complained about the relatively slow reactions of certain partner ministries, notably that of the Environment, Agriculture and Livestock, which the evidence suggests did not take timely action. In addition, a key respondent at the Ministry of Agriculture and Livestock stated that “The lethargy in the functioning of services in other ministries (Environment, Fisheries and Livestock, and Agriculture), is a formidable threat to public health. It undermines the implementation of preventive measures, disease detection, effective treatment, and epidemiological monitoring, both for individuals and animals (livestock). This has a bottleneck to the real-life execution of the One Health approach in our country.”
Intersectoral epidemiological surveillance is thus complex, and represents an issue at the national level. Some obstacles include operational coordination, sharing of information, and absence of sustainable mechanisms for consultation between sectors. As stated by another respondent from the Ministry of Environment and Sustainable Development, “The effectiveness of epidemiological surveillance depends to a great extent on the readiness of various state agencies and institutions to work together, on the joint pursuit of common goals in each specific local context, and on the concrete application of the One Health approach.”
3.6. Community Involvement and Addressing Fear and Stigmatization
The outcomes of the reports and interviews confirm slow progression of community involvement in Ebola management in the DRC. Nevertheless, this development has led to heightened engagement of public health community partners in sharing information, monitoring disease, and working together with other sectors, and even sub-sectors, to promote health, particularly in affected health zones. In fact, several practices established in this context have been mentioned in the 13th Ebola Report in the province of North Kivu/Beni. Campaigns to mobilize youth and women and increase awareness allowed information to be distributed to many populations [23]. Good practices were promoted with respect to animal health and the environment, including cessation of hunting, of the consumption of bushmeat, of the collection of game, and monitoring of parks and domestic animals. Respect for local cultural norms, for instance, through the provision of respectful and safe burial practices, also contributed to reducing social hostilities. This demonstrates that all levels of society worked together to achieve an efficient collective response [24].
Teams led by anthropologists and psychologists helped to “demystify” the disease and minimize fear and stigma surrounding ill and sick people or survivors, helping them to reintegrate into the community [25].
In addition, feedback loops have enabled interventions to be adjusted to accommodate the needs of populations. However, response success has been largely attributed to the provision of psychosocial and material support to affected families in certain settings, like in Likati. A key respondent from the Ministry of Public Health stated that “It is hard to address this rigorously and successfully without community involvement,”. Community involvement makes it possible for the whole community to be integrated into plans to curb the spread of the virus; thus, community and religious leaders, as well as traditional healers, have provided psychological and material support to families impacted by Ebola.
However, tensions have also arisen, especially in places where engagement mechanisms are not deeply rooted in the local environment, as illustrated in the report on the 11th Ebola outbreak in Equateur/Mbandaka province [13]. The use of external community relays (that is, relays not from the regions affected) has at times weakened the response, and in some instances, this has led to protests, strikes, and even killings, thus increasing the risk of outbreaks returning. Based on the analysis of the 11th to 15th reports, local governments play an important role as donors, with revitalization of community outreach units and payment of local liaisons crucial in restoring trust and improving the effectiveness of interventions [13,14,22,23]. This is demonstrated by the 10th outbreak in Butembo, North Kivu, in which a series of mediations between response actors and community leaders reduced tensions allowed cooperation to recover [26].
In addition, while our analysis validates that the One Health initiative is gaining traction in the DRC, it does not provide much clarity as to the roles of the health actors involved. Despite growing representation of the human, animal, and environmental health sectors, collaboration is frequently hindered by ambiguous governance and leadership constraints. This results in on-the-ground frustration, despite the fact that well-organized multisectoral teams are widely acknowledged to be capable of monitoring and controlling outbreaks. Finally, the findings of the reports and interviews indicate that information regarding community worries (including the need to work with community members to change their perceptions) has increasingly been integrated across successive outbreaks to enhance community engagement. These advances are related not only to systematic communication channels, but also to the willingness of institutions to listen to communities and adapt strategies to their knowledge, ways of working, and local dynamics.
3.7. Bottom-Up Approach to Community Engagement Within the Framework of the “One Health” Strategy
The bottom-up approach naturally leads to better integration of communities with the “One Health” strategy, as it increases community involvement in multisectoral and systemic decision-making and actions pertaining to health. According to Dieudonné K. Mwamba et al. (2024), such local mobilization is key to managing health emergencies using a “One Health” approach (integrating human, animal, and environmental health) [1]. The WHO also adopts an enabling role in the participatory approach to improve the implementation of this global framework, as it localizes interventions and encourages the intersectoral collaborative process (WHO, 2023). Additionally, the University of Montreal’s One Health initiative fosters collaboration through co-construction, inclusion, and reciprocity, with a focus on the essential role of communities in the success of these actions.
The One Health approach is based, among other things, on a logic of multisectoral collaboration. However, its successful application also depends on a bottom-up form of execution, so initiatives must be established by community actors, such that lessons and knowledge can be drawn from communities and local practices. The bottom-up approach was not adopted in the early outbreaks, as shown by management reports. About half of those studied were interventions implemented in a top-down manner, with little to no substantial participation from the community in the design or adjustment of strategies. Only in recent outbreaks have remarkable advances been made, with increased community engagement in the development and on-the-ground implementation of activities.
This transition to a bottom-up approach has highlighted the central role of certain local actors in disease response [7,27]. The practices documented are follows:
- Participation of traditional and religious authorities: These individuals were the pivotal factor in the adoption of Ebola prevention and management interventions.
- Mobilization of youth and women’s groups: As active participants in programs established to spread awareness of Ebola, these groups have been able to engage a wide range of populations and to extend the reach of community discourse.
4. Discussion
The findings underscore the critical importance of community engagement in managing EVD outbreaks and have significant implications for public health policy and practice. The results indicate that when communities are actively involved in outbreak response efforts, not only do health outcomes improve, but also the overall resilience of health systems is enhanced. This examination of the twelve EVD outbreaks in DRC between 2007 and 2022 demonstrates slow development of coordination models and community engagement mechanisms. Until the ninth outbreak, the country had largely depended on a tripartite structure, including national coordination at a central level that was supported by the national commission structure, provincial coordination, and the international scientific committee at the center. This model was effective and enabled the early control of EVD health crises within a reasonable period of time of around three to four months. Peripheral health workers, the first to be affected by the health crisis, were left without sufficient power to manage the outbreak [12]. Consequently, response leadership rested exclusively with authorities from the center of government—the coordinator of the International Scientific and Technical Coordination Committee—and this might have weakened the internal control of response measures at the health zone level.
Since the tenth outbreak, the DRC, following the WHO’s recommendations, has adopted the IMS model of outbreak management [20]. This approach, inspired by the military’s crisis management model, consists of the appointment of an Incident Manager with support from operational leaders in four areas: operations, planning, administration, and finance and logistics. This model has already been implemented within the Emergency Operations Center of the National Institute of Public Health, an organization established for preparing and addressing health emergencies and outbreaks; it is a common approach to outbreak management, because it does not create ad hoc structures that interfere with the normal activity of already-existing structures and that are therefore ineffective for reinforcing resilience against recurring health crises, such as in the DRC.
The bottom-up approach to community involvement, combined with the “One Health” approach, is being adopted to solve the Mpox outbreak in the DRC, which was identified as the global epicenter for this disease in 2024–2025. Official reports by the DRC Ministry of Health, the WHO, and the National Public Health Institute’s in-country teams have confirmed its use for Mpox outbreak surveillance, prevention, and response. However, its involvement of the local community is insufficient. Within numerous health zones, public health officials are faced with a range of emergencies without access to integrated coordination tools, which hampers their ability to respond in a timely and coordinated manner. Moreover, recent experiences and practices highlight the significance of a well-coordinated community partnership in preventing the spread of outbreaks, especially of EVD [17].
However, obstacles remain, including fear, stigma, and mental and emotional pain, which can affect the public’s willingness to collaborate, despite the advancement of community interventions and the widespread adoption of the One Health approach [1]. The need to include a strong psychosocial dimension in the management of outbreaks is not confined to medical or logistical issues. In this context, the “One Health” approach, while increasingly embedded in national strategies, is not yet functioning practically on the ground [2]. The effectiveness of the “One Health” response requires the participation and engagement of communities based on bottom-up strategies, where action is initiated from the bottom up and takes place in all parts of the community, as well as the provision of policy support by local authorities—both provincial and national. Despite the advances achieved in community integration, the interview respondents noted that the bottom-up approach only goes halfway to solving these issues when there is a multisectoral consultative framework and other measures involved. This includes calling for the participation of all members of the community in addressing public health responses to outbreaks and other public health emergencies. Structured collaboration is essential to supplementing and strengthening skills related to human health, but also animal and environmental health, and involves stakeholders from various sectors, such as local civil society, farmer and livestock breeder organizations, and agriculture associations.
Community- and event-based surveillance to quickly identify Ebola cases within a given area requires community health workers to improve knowledge, which would contribute to minimizing unreported cases and maximizing effectiveness in tracking outbreaks. A further dimension which has been investigated is risk communication and the creation of more local community relays. According to Ryan et al. [28], trust between the health authorities and communities is crucial during outbreaks of Ebola, and communication strategies that take local fear and beliefs into account are helpful. If messages are adapted to the local culture, they create greater awareness of the dangers and promote precautionary action. In addition, Frimpong et al. argue that mobilizing local resources in the prevention of outbreaks is of paramount importance [29].
The participation of community leaders and local Non-Governmental Organizations (NGOs) has also led to the establishment of networks which support disease surveillance and management in the region. Because conventional treatment and isolation methods are applied during outbreaks, they are subject to more appropriate localization. Regarding the One Health working environment, we need to encourage practical collaborations and between all actors, from local organizations to research centers, anthropologists, sociologists, government representatives, and international organizations, and establish platforms that facilitate such collaborations, to enable the sharing of information and practices that will support One Health [27]. Donors and financiers will undoubtedly play an important role in advancing One Health approaches when creating development priorities, policy decisions, and resource allocation. Several different factors and sectors need to come together to accommodate the complexity of EVD outbreaks in the context of people and animals and the widespread ecological degradation caused by EVD in the region. A multisectoral and multidisciplinary approach is the only way to address this challenge, taking into account the participation of institutions and the community, all with different missions, priorities, funding, levels, training, and outlooks [30].
Implications for public health policy emphasize the importance of community engagement, tailored communication strategies, and the integration of a One Health approach. Community engagement during EVD outbreaks provides valuable insights that can enhance future outbreak responses. Evidence suggests that public health policies should prioritize community involvement in outbreak response, promoting trust and relationships between health authorities and communities to enhance cooperation during health crises. Developing communication strategies that are culturally relevant and actionable is crucial; public health messages must align with local beliefs and practices, supported by training for community health workers in effective communication. Additionally, incorporating the One Health approach—recognizing the interconnectedness of human, animal, and environmental health—into public health strategies can help mitigate factors contributing to viral outbreaks, including environmental changes and zoonotic transmission. Data-driven decision-making can lead to tailored interventions, improving acceptance and effectiveness. Empowering communities builds health system resilience, ensuring sustained health practices beyond outbreaks. Additionally, establishing feedback mechanisms encourages continuous dialogue, allowing public health agencies to adapt strategies based on community experiences and challenges.
5. Conclusions
The study findings advocate for a paradigm shift in public health policy towards a more inclusive and community-centered approach. By recognizing the pivotal role of community engagement in enhancing health outcomes and building resilience, public health agencies can better prepare for and respond to future outbreaks. This study serves as a call to action for policymakers to invest in community engagement as an essential element of public health strategy, ultimately leading to healthier and more resilient populations. Effective management of EVD outbreaks and other health crises in the DRC must be grounded in community engagement and the concrete implementation of a One Health approach. The data from this study, based on the analysis of twelve outbreak reports and interviews from various levels of stakeholders, suggest the need for holistic responses, locally calibrated strategies, and a trust- and collaboration-based platform to guide action and response approaches. Nonetheless, it is necessary to continue analyzing and readjusting response strategies through future crises considering changing socio-cultural contexts and community movements. When fear, stigma, and psychological distress are addressed and when communities are meaningfully involved, prevention and control efforts become reliable and effective.
These reflections on Ebola management in the Congolese setting can inform interventions worldwide in populations affected by disease outbreaks, highlighting the applicability of the “One Health” approach. An intersectoral and participatory strategy, rooted in trust, proximity, and shared knowledge, represents a strong tool for improving the resilience of health systems to future challenges.
Author Contributions
D.K.M. produced the first draft of the article. All of the other authors contributed to enhancing the quality of the article. C.M., G.M., and C.Z. guided the writing of the article. All authors revised this article and approved its submission. G.M. and C.Z. approved the submission of the article. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study has been approved by the ethics committee of the University of Montreal (UdeM).
Data Availability Statement
The collected data is available and can be shared anonymously.
Acknowledgments
We thank everyone who directly or indirectly contributed to the completion of this work. We offer special thanks to the technical experts from the government and the technical government and financial partners of the DRC who helped to respond to the Ebola outbreak.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A. Qualitative Indicators of the MATCH Framework

Table A1.
“One Health” approach.
| Analysis Criteria | Observation: Involvement of Sectors |
|||||||
|---|---|---|---|---|---|---|---|---|
| Outbreak Code |
Year | Province/Health Zones | Strain | Multisectoral Coordination |
Data Sharing | Intersectoral Collaboration |
Actors Involved | Level of Integration: |
| E1 | 2007 | Western Kasai—Mweka, Luebo, Bulape | Ebola Zaire | Limited coordination, led by Ministry of Health (MS) alone | Fragmented data, limited dissemination | Minimal collaboration with Non-Governmental Organizations (NGOs) | MS, World Health Organization (WHO), National Institute of Biomedical Research (INRB), UNICEF, Doctors Without Borders (MSF), Red Cross: (Technical and Scientific Committee) | Suboptimal |
| E2 | 2008 | Western Kasai—Mweka, Luebo, Bulape | Ebola Zaire | Coordination similar to 2007 | Non-harmonized data | Limited collaboration | MS, WHO, INRB, UNICEF, MSF, Red Cross: (Technical and Scientific Committee) | Suboptimal |
| E3 | 2012 | Orientale Province—Isiro, Haut-Uélé, Viadana | Ebola Zaire | Enhanced coordination with WHO | Data shared via radio/NGO | Collaboration with Church/schools | Human health (National Coordinating Committee and International Scientific and Technical Coordinating Committee (ICST)) | Not optimal |
| E4 | 2014 | Equator Province (Boende) | Increased multisectoral coordination | Limited but real sharing | NGO and authority collaboration | Human health (Ministry of Health, Red Cross, local authorities) | Suboptimal | |
| E5 | 2017 | Bas-Uele—Likati | Ebola Zaire | Improved coordination, local involvement | Sharing via village committees | Increased collaboration with community liaisons (RECO) and survivors | MS, WHO, INRB, UNICEF, MSF, Food and Agriculture Organization (FAO), Red Cross (multidisciplinary team from the Ministry of Health and the National Coordination Committee) | Suboptimal |
| E6 | 2018 | Ecuador—Bikoro, Iboko, Wangata | Ebola Zaire | Enhanced WHO/MS Coordination | Structured sharing | NGO collaboration, traditional leaders | MS, WHO, INRB, UNICEF, MSF, FAO, Red Cross (multidisciplinary team from the Ministry of Health and the National Coordination Committee) | Suboptimal |
| E7 | 2018 | North Kivu, Ituri, South Kivu—Mabalako | Ebola Zaire | Complex multisectoral coordination | Data shared via platforms | Strong multisectoral collaboration | Multisectoral Committee for the Ebola Response (CMRE) and Ministry of Health | Suboptimal |
| E8 | 2020 | Ecuador—Bikoro, Iboko, Wangata | Ebola Zaire | Partial coordination | Limited sharing | Limited collaboration | CMRE and Ministry of Health | Suboptimal |
| E9 | 2021 | North Kivu—Biena, Butembo, Katwa, Musienne | Ebola Zaire | Improved coordination, leadership involvement | Structured sharing | Good collaboration between survivors and NGOs | National Coordination Committee (NCC) and Incident Management System: MS, WHO, INRB, UNICEF, MSF, Red Cross | Suboptimal |
| E10 | 2021 | North Kivu—Beni | Ebola Zaire | Fragile coordination | Limited data | Weak collaboration | CNC and SGI: MS, WHO, INRB, UNICEF, MSF, Red Cross | Suboptimal |
| E11 | 2022 | Ecuador—Mbandaka, Wangata, Bolenge | Ebola Zaire | Consolidated coordination | Regular sharing | NGO and authority collaboration | CNC and SGI: MS, WHO, INRB, UNICEF, MSF, Red Cross | Suboptimal |
| E12 | 2022 | North Kivu—Beni | Ebola Zaire | Reduced coordination, local tensions | Low sharing | Weak collaboration | CNC and SGI: MS, WHO, INRB, UNICEF, MSF, Red Cross | Suboptimal |
Outbreak codes (E1–E12) refer to Ebola outbreaks in the DRC from 2007 to 2022. Not optimal: involvement of a single sector (e.g., human health). Suboptimal: involvement of 2 sectors (e.g., human and animal health). Optimal: involvement of 3 sectors (human, animal, and environmental health).
Table A2.
Community engagement.
| Analysis Criteria | Observation Community Involvement: |
|||||||
|---|---|---|---|---|---|---|---|---|
| Outbreak Code |
Year | Province/Health Zones | Strain | Awareness | Accountability | Community Stakeholders Involved | Specific Groups | Level of Involvement |
| E1 | 2007 | Western Kasai—Mweka, Luebo, Bulape | Ebola Zaire | Local campaigns through community relays (RECO), rural radio (local authorities and community leaders) | Low accountability, limited mobilization of local authorities | RECO, Red Cross, CAC | Religious leaders, local authorities, local radio stations, orchestras (general population) | Weak |
| E2 | 2008 | Western Kasai—Mweka, Luebo, Bulape | Ebola Zaire | Increased use of community radio, local posters | Greater accountability with the involvement of local health authorities | RECO, Red Cross, Community Coordination Unit (CAC) | General population, affected families | Moderate |
| E3 | 2012 | Orientale Province—Isiro, Haut-Uélé, Viadana | Ebola Zaire | Awareness sessions in villages, involvement of local NGOs | Beginning of participatory approaches (community consultations) | RECO, Red Cross, local Non-Governmental Organizations (NGOs), youth associations | Religious leaders, hunters, game sellers, Indigenous People, charcoal burners, women’s and youth associations | Moderate |
| E4 | 2014 | Ecuador (Bikoro) | Ebola Zaire | Large-scale radio and church campaigns; survivor involvement | Partial empowerment (associated traditional leaders) | RECO, religious denominations, survivors | General population (women, youth, survivors) | Good |
| E5 | 2017 | Bas-Uele—Likati | Ebola Zaire | Local communication, community theater | Strong empowerment (community leaders active in the response) | CAC, Red Cross | Community leaders, hunters, traditional healers, driver associations (general population, affected families) | Good |
| E6 | 2018 | Ecuador—Bikoro, Iboko, Wangata | Ebola Zaire | Extensive radio campaign, involvement of schools | Progressive empowerment with role sharing | RECO, teachers, health authorities | Community leaders, hunters, traditional healers, driving associations | Good |
| E7 | 2018 | North Kivu, Ituri, South Kivu—Mabalako | Ebola Zaire | Intensive campaigns, local radio, TV spots, WhatsApp (development of a map of RECOs, local supervisors and Health Area supervisors) | Strong empowerment but polarized by a climate of mistrust (training of RECOs; village/neighborhood/group leaders; and opinions of leaders on the procedure for prevention, identification of cases, collection and transmission of Ebola-related community information to health centers) | CAC | Community leaders, youth, women, schoolchildren, traditional healers | Moderate to Good |
| E8 | 2020 | Ecuador | Targeted communication in the affected areas | Partial responsibility, dependent on health authorities | RECO, churches, traditional leaders | General population | Moderate | |
| E9 | 2021 | North Kivu—Biena, Butembo, Katwa, Musienne | Ebola Zaire | Rapid mobilization via radio and local leaders | Strong accountability through vigilance committees (capacity building for community leaders: mayors, neighborhood and street chiefs) regarding Ebola virus disease | CAC, RECO, local authorities, youth associations | Community leaders (youth, affected families) | Good |
| E10 | 2021 | North Kivu—Beni | Ebola Zaire | Good | Good capacity building for community leaders (mayors, neighborhood and street chiefs) in fight against EVD | CAC | Community leaders | Good |
| E11 | 2022 | Ecuador—Mbandaka, Wangata, Bolenge | Ebola Zaire | Awareness-raising via community radio, local campaigns | Capacity building for community leaders (mayors, neighborhood and street chiefs) in fight against Ebola | CAC, RECO, local NGOs, religious denominations | Community leaders, families | Moderate |
| E12 | 2022 | North Kivu—Beni | Ebola Zaire | Targeted awareness-raising with crisis communication | Accountability consolidated by authorities and survivors (capacity building of community leaders: mayors, neighborhood and street chiefs) in fight against Ebola | CAC, RECO, survivors, NGOs, churches | Community leaders (affected communities, bereaved families) | Moderate to Good |
E1–E12 = numbering of the Ebola virus disease outbreaks in the DRC (from 2007 to 2022). The following denote the level of involvement: Absent: no trace of community involvement; Low: occasional, unstructured involvement; Moderate: partial participation, but not systematic; Good: regular and structured community engagement; Optimal: central and active involvement, with clear local ownership.
Table A3.
Bottom-up approach.
| Analysis Criteria | Observation | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Outbreak Code | Year | Province/Health Zones | Strain | Local Information Collection |
Community Involvement |
Strategic Adaptation |
Local System Strengthening |
Key Players | Application of the Approach |
| E1 | 2007 | Western Kasai—Mweka, Luebo, Bulape | Ebola Zaire | Ad hoc reports via community relays (RECO) | Low demand, fear/rumors | Limited adjustments to local customs (involvement of non-medical stakeholders) | No permanent system (involvement of the community facilitator of the Mweka Health Zone (HZ) in the management of emergency activities to address the outbreak) | Community facilitator ZS/Mweka, RECO, traditional leaders | Weak |
| E2 | 2008 | Western Kasai—Mweka, Luebo, Bulape | Ebola Zaire | Same setup as in 2007 | Limited participation, little consideration given to feedback | Little adaptation to expressed needs | No emergency structural improvement in response to the outbreak | RECO, local leaders | Weak |
| E3 | 2012 | Orientale Province—Isiro, Haut-Uélé, Viadana | Ebola Zaire | Local radio stations, parish meetings | Participation of religious leaders/teachers | Partial adjustments based on feedback | Local dialog strengthened on occasion | RECO, priests, teachers | Moderate |
| E4 | 2014 | Boende | Ebola Zaire | Community meetings, radio stations | Increased mobilization around funeral practices | Partial adjustments to funeral rituals | Limited structural reinforcement | RECO, Red Cross, local authorities | Moderate |
| E5 | 2017 | Bas-Uele—Likati | Ebola Zaire | Word of mouth, village committees | Involvement of survivors and families | Communication to encourage behavior change | Start of functional committees | RECO, survivors, Red Cross | Good |
| E6 | 2018 | Ecuador—Bikoro, Iboko, Wangata | Ebola Zaire | Community radio stations, structured meetings | Active customary leadership | The village-by-village and household-by-household strategy is one of the strategies that has been used to control the disease | Structuring of local mechanisms | RECO, Non-Governmental Organization (NGO), traditional leaders | Good |
| E7 | 2018 | North Kivu, Ituri, South Kivu—Mabalako | Ebola Zaire | Monitoring committees, platforms, feedback points | Present | Invitations to all village chiefs, neighborhood chiefs, group chiefs, leaders, and registered nurses (RNs) of the targeted Health Areas (HAs) to participate in operational meetings | Health personnel, managers from other sectors, administrative staff, and social organizations within the health zone are the main actors in the response | Village chiefs, community leaders, registered nurses | Optimal |
| E8 | 2020 | Ecuador | Ebola Zaire | Local radio stations, community relays | Partial involvement | Limited adjustments | Low durability | RECO, local NGOs | Moderate |
| E9 | 2021 | North Kivu—Biena, Butembo, Katwa, Musienne | Ebola Zaire | Regular community dialog | Strong involvement of survivors/young people | Invitations to all village chiefs, neighborhood chiefs, group leaders, and IT staff of the targeted AS to participate in operational meetings | Health personnel, managers from other sectors, administrative staff, and social organizations within the health zone are the main actors in the response | Community leaders and local influencers | Good |
| E10 | 2021 | North Kivu—Beni | Ebola Zaire | Ad hoc meetings | Limited involvement, persistent mistrust | Minor adjustments | Weak local reinforcement | RECO, local NGOs | Moderate |
| E11 | 2022 | Ecuador—Mbandaka, Wangata, Bolenge | Ebola Zaire | Radio and meetings reinforced | Good community participation | Adjustments to local practices | Strengthened community relays | RECO, NGO, Red Cross | Good |
| E12 | 2022 | North Kivu—Beni | Ebola Zaire | Informal, unsystematic collection | Reduced involvement | Weak adjustments | No reinforcement observed | Community leaders and local influential groups | Weak |
References
- Mwamba, D.K.; Zarowsky, C.; Manianga, C.D.; Kapanga, S.; Moullec, G. Engagement communautaire et prise en compte de la détresse psychologique, de la peur et de la stigmatisation dans la surveillance et la gestion des épidémies de la maladie à virus Ebola dans l’approche «Une seule santé» en RD. Congo. Glob. Health Promot. 2024, 32, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Olive, M.M.; Angot, J.L.; Binot, A.; Desclaux, A.; Dombreval, L.; Lefrancois, T.; Lury, A.; Paul, M.; Peyre, M.; Simard, F.; et al. Plan d’action conjoint «Une seule santé» (2022–2026). In Travailler Ensemble Pour des Êtres Humains, des Animaux, des Végétaux et un Environnement en Bonne Santé; World Health Organization: Geneva, Switzerland, 2022; Volume 30, pp. 72–81. [Google Scholar]
- Olive, M.M.; Angot, J.L.; Binot, A.; Desclaux, A.; Dombreval, L.; Lefrancois, T.; Lury, A.; Paul, M.; Peyre, M.; Simard, F.; et al. Les approches One Health pour faire face aux emergences: Un necessaire dialogue A tat-sciences-societes. Nat. Sci. Soc. 2022, 30, 72–81. [Google Scholar] [CrossRef]
- Rosello, A.; Mossoko, M.; Flasche, S.; Van Hoek, A.J.; Mbala, P.; Camacho, A.; Funk, S.; Kucharski, A.; Ilunga, B.K.; Edmunds, W.J.; et al. Ebola virus disease in the Democratic Republic of the Congo,1976–2014. Elife 2015, 4, e09015. [Google Scholar] [CrossRef] [PubMed]
- Vinck, P.; Pham, P.N.; Bindu, K.K.; Bedford, J.; Nilles, E.J. Institutional trust and misinformation in the response to the 2018–19 Ebola outbreak in North Kivu. Lancet Infect. Dis. 2019, 19, 529–536. [Google Scholar] [CrossRef] [PubMed]
- OHHLEP One Health High Level Expert Panel Annual Report 2021. World Health Organization. 2021, pp. 1–35. Available online: https://cdn.who.int/media/docs/default-source/one-health/ohhlep/ohhlep-annual-report-2021.pdf?sfvrsn=f2d61e40_10&download=true.
- Anoko, J.; Epelboin, A.; Formenty, P. Humanisation de la Réponse à la Fièvre Hémorragique Ebola en Guinée: Approche Anthropologique. 2014. Available online: https://hal.archives-ouvertes.fr/hal-01090299/file/2014_07_30Anoko.
- Democratique, R.; Congo, D.U.; La, M.D.E.; Publique, S.; Coordination, C.N.D.E.; Des, C.; Urgences, O.D.; Publique, D.E.S.; Kalenga, O.I.; et al.; Ministère de la Santé Publique Rapport de la Gestion de l’Epidémie de Fièvre Hémorragique Virale Ebola dans la Zone de Santé de Mweka, Province du Kasai Occidental; Direction de la Lutte contre la Maladie, 2007; pp. 1–73. [Google Scholar]
- Ministère de la Santé Publique (Direction de la Lutte contre la Maladie). Rapport de la Gestion de l’Epidémie de Fièvre Hémorragique Virale Ebola dans la Zone de Santé de Mweka, Province du Kasai Occidental. 2009. [Google Scholar]
- Ministère de la Santé Publique. Direction de la Lutte contre la Maladie) Gestion de l’Epidémie de la Fièvre Hémorragique a Virus Ebola a Isiro. 2012. [Google Scholar]
- de la R., P.; Ministère de la santé publique. Rapport de gestion de l’ épidemie de la maladie à virus ébola; 2014; pp. 1–62. [Google Scholar]
- de la R., P.; Ministère de la Santé Publique. Brève Situation de la Riposte à L’épidémie de la Maladie à Virus Ebola (MVE) dans la Province de l’Equateur, République Démocratique du Congo au 30e jour. 2018. [Google Scholar]
- Ministère de la Santé Publique H et P de la R. Rapport de Gestion de la 11 Ième Épidemie de la Maladie à Virus Ébola_Boende Direction de la Surveillance Epidémiologique, Direction Generale de Lutte Contre la Maladie Rapport de la 11ème Épidemie de la Maladie à Virus Ébola (MVE) Dans la Province de L’équateur. 2020. [Google Scholar]
- de la R., P.; Ministère de la Santé Publique. Rapport de la 14 Ème Épidemie de la Maladie à Virus Ébola (MVE) Dans la Province de L’équateur Juillet 2022.
- Bunker, B.S.-M. Parcel Influencing Personal and Environnemental Conditions for Community Health_A Multilevel Intervention Model; Aspen Publishers, Inc.: New York, NY, USA, 1988; pp. 25–35. [Google Scholar]
- Simons-Morton, B.; McLeroy, K.; Wendel, M. Behavior Theory in Health Promotion Practice and Research; Jones & Bartlett Learning: Burlington, MA, USA, 2011. [Google Scholar]
- Lawrence, R.S.; Bibbins-Domingo, K.; Brennan, L.K.; Daniels, N.; Gaskin, D.J.; Green, L.W.; Haveman, R.; Jenson, J.; Nieto, F.J.; Polsky, D.; et al. An Integrated Framework for Assessing the Value of Community-Based; National Academies Press: Washington, DC, USA, 2012. [Google Scholar]
- Desclaux, A.; Sow, K. Humaniser» les soins dans l’épidémie d’Ebola? Les tensions dans la gestion du care et de la biosécurité dans le suivi des sujets contacts au Sénégal. Anthropol. Santé 2015, 11, 2–17. [Google Scholar] [CrossRef]
- Frieden, T.R.; Damon, I.; Bell, B.P.; Kenyon, T.; Nichol, S. Ebola 2014—New Challenges, New Global Response and Responsibility. N. Engl. J. Med. 2014, 371, 1177–1180. [Google Scholar] [CrossRef] [PubMed]
- Wadoum, R.E.G.; Sevalie, S.; Minutolo, A.; Clarke, A.; Russo, G.; Colizzi, V.; Mattei, M.; Montesano, C. The 2018–2020 Ebola Outbreak in the Democratic Republic of Congo: A Better Response Had Been Achieved Through Inter-State Coordination in Africa. Risk Manag. Healthc. Policy 2021, 14, 4923–4930. [Google Scholar] [CrossRef] [PubMed]
- Fa, J.E.; Nasi, R.; Van Vliet, N. Bushmeat, human impacts and human health in tropical rainforests: The Ebola virus case. Sante Publique 2019, 31, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Ministère de la Santé Publique H et P de la R. Rapport de Gestion de la 12ième Épidemie de la Maladie à Virus Ébola Ministère de la Santé, Hygiène et Prévention, Direction Surveillance Epidé Miologique Direction Génèrale de Lutte Contre la Maladie Rapport se la 12 Ème Épidemie de la Maladie à Virus Ébpola (MVE) Dans la Province du Nord Kivu. 2021. [Google Scholar]
- Ébola, M. de la Santé Publique H. et P. de la R.R. de Gestion de la 13 Ième Épidemie de la Maladie à Virus Direction Surveillance Epidémiologique Rapport de la 13 Ème Epidemie de la Maladie a Virus Ebola (MVE) Dans la. 2021. [Google Scholar]
- Fotso, A.S.; Wright, C.G.; Low, A. How does HIV-related stigma correlate with HIV prevalence in African countries? Distinct perspectives from individuals living with and living without HIV. BMC Public Health 2023, 23, 1720. [Google Scholar] [CrossRef] [PubMed]
- Rabelo, I.; Lee, V.; Fallah, M.P.; Massaquoi, M.; Evlampidou, I.; Crestani, R.; Decroo, T.; Van den Bergh, R.; Severy, N. Psychological Distress among Ebola Survivors Discharged from an Ebola Treatment Unit in Monrovia, Liberia—A Qualitative Study. Front. Public Health 2016, 4, 142. [Google Scholar] [CrossRef] [PubMed]
- Crawford, N.; Holloway, K.; Baker, J.; Dewulf, A.; Kaboy, P.; Musema, E.K. The Democratic Republic of Congo’s 10th Ebola Title response Subtitle; Humanitarian Policy Group location: London, UK, 2021. [Google Scholar]
- Metta, E.; Mohamed, H.; Kusena, P.; Nyamhanga, T.; Bahuguna, S.; Kakoko, D.; Siril, N.; Araya, A.; Mwiru, A.; Magesa, S.; et al. Community perspectives of Ebola Viral Disease in high-risk transmission border regions of Tanzania: A qualitative inquiry. BMC Public Health 2024, 24, 2766. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.J.; Giles-vernick, T.; Graham, J.E. Technologies of trust in outbreak response: Openness, reflexivity and accountability during the 2014–2016 Ebola outbreak in West Africa. 2019, 4, e001272. [Google Scholar] [CrossRef] [PubMed]
- Frimpong, S.O.; Paintsil, E. Community engagement in Ebola outbreaks in sub-Saharan Africa and implications for COVID-19 control: A scoping review. Int. J. Infect. Dis. 2023, 126, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Meseko, C.A.; Egbetade, A.O.; Fagbo, S. Ebola virus disease control in West Africa: An ecological, one health approach. Pan Afr. Med. J. 2015, 21, 1–5. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Adapted conceptual MATCH model.
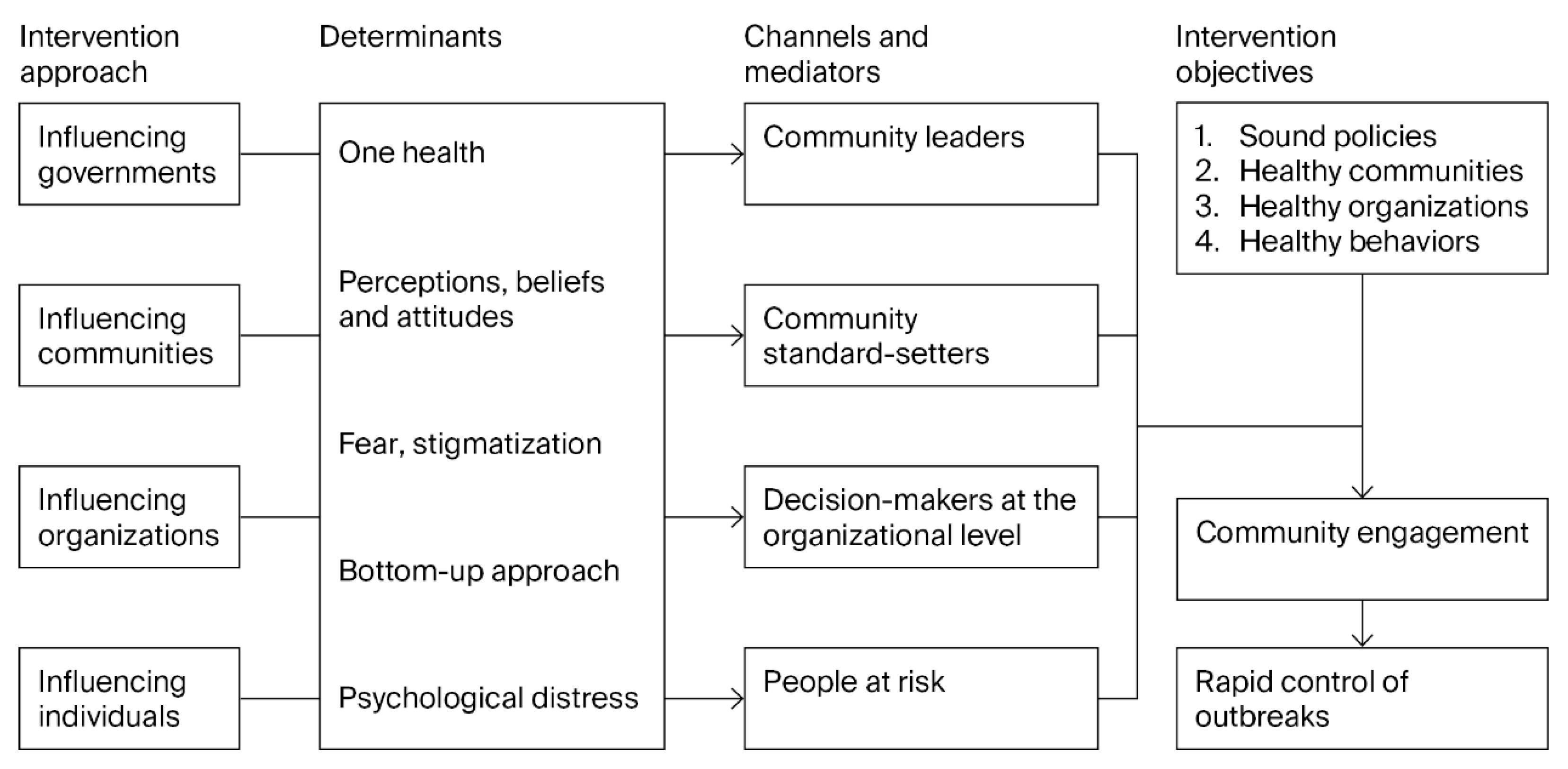
Figure 2.
Model of an Incident Management System. Source: WHO.
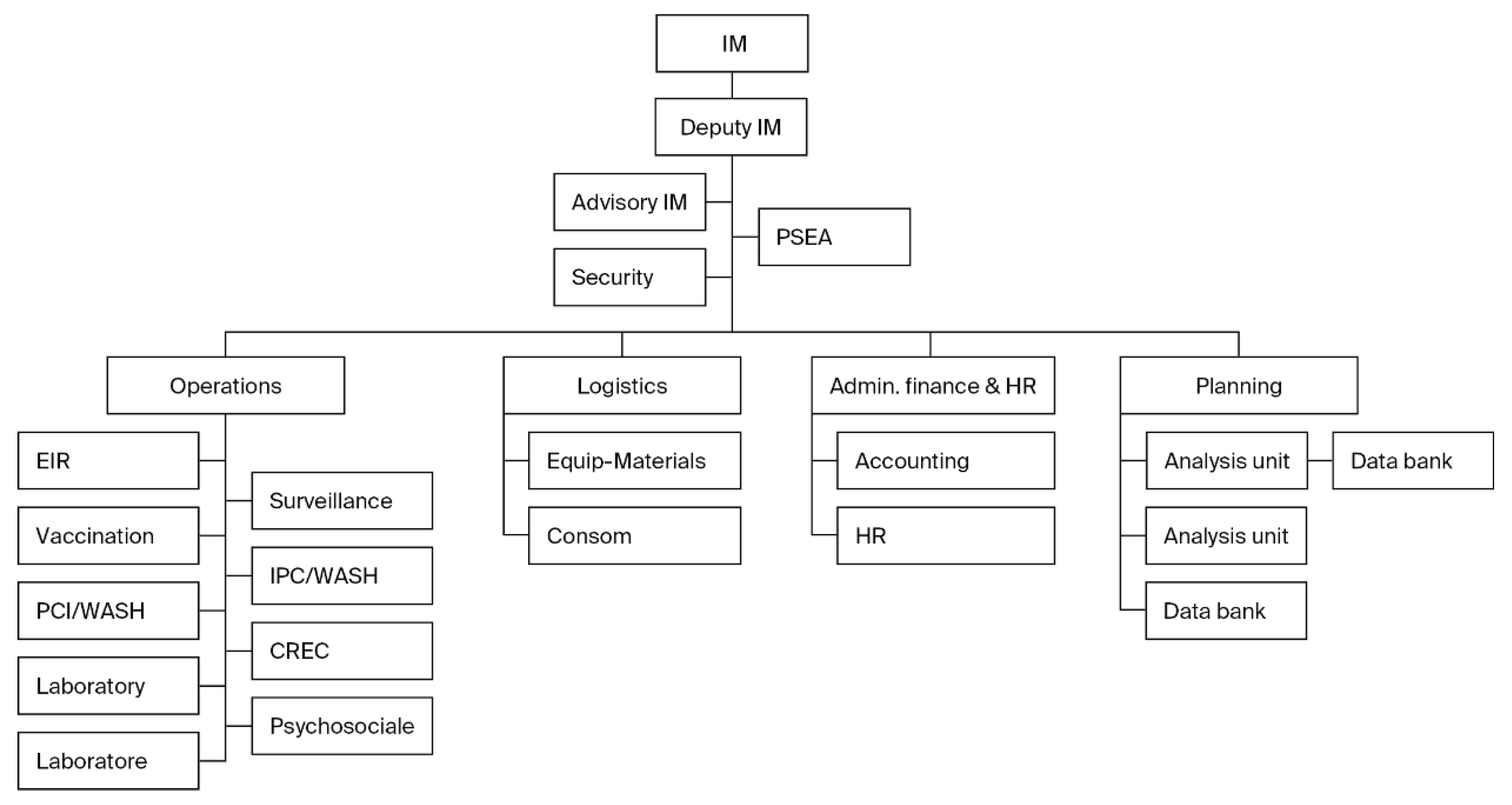
Table 1.
Analytical framework.
| No. | Qualitative Indicators Drawn from the MATCH Framework | Observation of the Evaluation of Indicators |
|---|---|---|
| 1. | One Health approach |
|
| 2. | Community involvement/ engagement |
|
| 3. | Bottom-up approach |
|
Table 2.
Evaluation of indicators from the 4th to the 15th Ebola outbreaks in the DRC.
| Period and Location | Strain | Impact | One Health | Level of Community Involvement/Engagement |
Bottom-Up Approach |
|---|---|---|---|---|---|
| 2007—Luebo (Western Kasai) 4th outbreak of Ebola, also known as the Kaluamba outbreak. |
EBOV | 264 suspected cases, including 187 deaths (case fatality rate of 71%). | Suboptimal | Moderate involvement | Not applied |
| 2008–2009—Mweka (Western Kasai): 5th Outbreak, occurring in the same region as the 2007 outbreak. |
EBOV | 32 cases, including 15 deaths (case fatality rate of 47%). | Suboptimal | Moderate involvement | Not applied |
| 2012—Isiro (Oriental Province/Haut-Uélé) Sixth Ebola virus disease (EVD) outbreak, mainly occurring in the city of Isiro. |
EBOV | 77 cases, including 36 deaths (case fatality rate of 47%). | Suboptimal | Moderate involvement | Applied |
| Report on the 8th EVD outbreak, Likati Health Zone (Bas-Uele Province), DRC 2017. |
EBOV | 8 cases and 4 deaths (case fatality rate of 50%). | Suboptimal | Good involvement | Applied |
| Report on the response to the 9th Ebola virus disease outbreak in Equateur/Bikoro province 2018. |
EBOV | From 8 May to 28 June 2018, 53 cases were recorded, including 29 deaths, of which 38 were confirmed and 15 were probable. The case fatality rate was 61%. | Suboptimal | Good involvement | Not applied |
| Report on the 10th EVD outbreak in the provinces of North Kivu, South Kivu, and Ituri. | EBOV | 2852 confirmed cases, including 1155 recoveries and 1111 deaths. Women were more affected, representing 55.9% of cases, with a case fatality rate of 66%. | Suboptimal | Good involvement | Applied |
| Report on the 11th EVD outbreak in Equateur/Mbandaka. | EBOV | 130 confirmed cases, including 55 deaths (case fatality rate of 42%). | Suboptimal | Good involvement | Applied |
| Report on the 12th EVD outbreak in the North Kivu/Beni and Butembo provinces. | EBOV | 12 confirmed cases, including 6 deaths (case fatality rate of 50%). | Suboptimal | Good involvement | Applied |
| Report on the 13th EVD outbreak in North Kivu/Beni province. | EBOV | 11 confirmed cases, including 9 deaths (case fatality rate of 82%). | Optimal | Good involvement | Applied |
| Report on the 14th EVD outbreak in Equateur/Mbandaka province. | EBOV | 5 confirmed cases, including 5 deaths (100% case fatality rate). | Optimal | Good involvement | Applied |
| Report on the 15th EVD outbreak in North Kivu/Beni province. | EBOV | 1 confirmed case, including 1 death (100% case fatality rate). | Optimal | Good involvement | Applied |
Table 3.
Epidemiological surveillance subcommittee.
| Subcommittee | Members | Objectives | Activities Carried Out |
|---|---|---|---|
| Epidemiological surveillance | The subcommittee was made up of several members, including
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



