
Submitted:
15 December 2025
Posted:
17 December 2025
You are already at the latest version
Abstract
Purpose: To investigate the long-term effects of phacoemulsification by the eight-chop technique on intraocular pressure (IOP) in patients with primary open-angle glaucoma (POAG). Methods: This study comprised the eyes of patients with cataracts who had undergone phacoemulsification and posterior chamber intraocular lens implantation. Patients with corneal disease or opacity, uveitis, pupillary dilation problem, and previous trauma or surgery were excluded. Cataract surgeries were performed using the eight-chop technique. The operative time, phaco time, aspiration time, cumulative dissipated energy, and volume of fluid used were measured intraoperatively. Best-corrected visual acuity and corneal endothelial cell density (CECD) were measured postoperatively at 7 and 19 weeks.Results: In total, 150 eyes of 98 patients were followed up. The POAG group had a CECD loss rate of 1.5% and 1.2% at 7 and 19 weeks postoperatively, respectively. The control group had a CECD loss rate of 0.8% and 1.4% at 7 and 19 weeks postoperatively, respectively. The IOP reduction rate at 1 year postoperatively was 12.7% and 12.5% in the POAG and control groups, respectively. In the subgroups with preoperative IOP below 15 mmHg, IOP decreased significantly (p<.01, paired t-test) at 7 weeks and remained significantly lower at 1 year postoperatively.Conclusions: The eight-chop technique remained effective in lowering IOP after 1 year in the POAG and control groups. This effect did not diminish in patients preoperative IOP below 15 mm Hg. Phacoemulsification using the eight-chop technique may be effective for patients with glaucoma.
Keywords:
cataract surgery
; phacoemulsification
; primary open-angle glaucoma
; intraocular pressure
; eight-chop technique
Introduction
Intraocular pressure (IOP) decreases after phacoemulsification in patients with primary open-angle glaucoma (POAG) [1,2,3,4,5,6]. Several studies have also reported changes in IOP after phacoemulsification in patients with cataract who do not have glaucoma [4,7,8]. However, the degree of IOP reduction remains controversial, and the extent to which phacoemulsification and lens implantation reduce IOP in glaucomatous and normal patients is unclear.
The phacoemulsification techniques employed in previous reports on the changes in IOP after phacoemulsification include the divide-and-conquer [2,9], stop and chop [8,9,10], or unknown [5,11,12,13,14]. However, no study has utilized the eight-chop technique. Furthermore, no studies have examined intraoperative parameters; therefore, the surgical details are unknown.
The eight-chop technique manually divides the nucleus under an ophthalmic viscosurgical device before phacoemulsification [15]. Compared with conventional grooving, divide-and-conquer, and phaco-chop techniques, the eight-chop technique reduces the total ultrasound energy, aspiration time, and volume of the fluid used [15].
In 2002, the prechop technique [16,17] was improved, and the eight-chop technique was developed. Here, the lens nucleus was divided into eight segments instead of four, as in the prechop technique.
When investigating the relationship between phacoemulsification and IOP, the impact of surgery on intraocular tissues must be considered. More accurate results can be obtained if changes in IOP after phacoemulsification are examined by measuring intraoperative parameters and the surgical involvement of intraocular tissues is considered.
This study aimed to evaluate the effects of IOP after phacoemulsification using the eight-chop technique in glaucomatous and normal patients for 1 year.
Methods
The study protocol adhered to the guidelines of the Declaration of Helsinki and was approved by the review board. Informed consent for participation in this study was obtained from each patient after explaining the nature and possible consequences of the study. This study comprised the eyes of patients with cataracts who had undergone phacoemulsification and posterior chamber intraocular lens (IOL) implantation between January 2015 and November 2021. Patients who had visited the clinic with cataracts were enrolled in the study. Exclusion criteria involved patients with corneal disease or opacity, uveitis, pupillary dilation problem, and previous trauma or surgery. Patients with POAG who had not commenced glaucoma treatment were promptly treated with cataract surgery without prior glaucoma treatment. Normal eyes had no glaucoma history, ocular medications, and glaucomatous optic nerve changes (defined as a cup-to-disc ratio of more than 0.7, disc asymmetry, total or partial thinning of the neural rim, and peripapillary atrophy). Glaucomatous eyes had previously diagnosed glaucoma, with apparent optic nerve changes and Humphrey 30-2 visual field defects (three contiguous points greater than -5 dB or one point greater than -10 dB).
The number of preoperative glaucoma medications of all patients was recorded. Preoperatively, all patients underwent slit-lamp and retinal examinations, and their best-corrected visual acuity (BCVA) and IOP were measured. Corneal endothelial cell density (CECD) (cells/mm2) was measured using a non-contact specular microscope (EM-3000, Topcon, Hasunumacho). The firmness of the nucleus was graded using the Emery classification [18]. The same surgeon, who is experienced in the eight-chop technique, performed phacoemulsification using the phacoemulsification unit (Centurion®, Alcon Labs Inc).
New surgical instruments have been designed and developed to perform the eight-chop technique [15]. However, our research team designed eight choppers and requested a manufacturing company to produce them. Eight-chopper I (SP-8193; ASICO) has a smaller tip than the conventional prechopper, with a length and width of 3.2 mm and 1.4 mm, respectively, and a sharper leading edge and was used for the grade II group. Eight-chopper II (SP-8402; ASICO) has a smaller angular tip (2.5 mm long and 0.8 mm wide) that can be inserted vertically into the lens nucleus for the grade III group (Figure 1).
In all surgeries, a temporal, clear, corneal incision was made using a 3.0-mm steel keratome. After injecting sodium hyaluronate into the anterior chamber, a 6.2–6.5-mm continuous curvilinear capsulorrhexis was created using capsule forceps. The soft-shell technique [19] was used in the grade III group. Hydrodissection was performed using a 27-G cannula; however, hydrodelineation was never performed. The lens nucleus was cracked into eight segments using Eight-chopper I or II in grade II and III groups. The eight segments were phacoemulsified and aspirated at the depth of the iris plane. The capsular bag was aspirated with the irrigation/aspiration tip to remove cortical materials. The ophthalmic viscosurgical device was injected, and a foldable IOL (Alcon Labs Inc.) with polymethyl methacrylate haptics was inserted in the capsular bag using an injector system. The ophthalmic viscosurgical device was then aspirated. The phacoemulsification unit was used in all cases and had a flow rate of 32 mL/min, a maximum ultrasound power of 80%, and a 1.1-mm tip. The wound was sealed using stromal hydration if necessary. The anterior chamber was replaced with a balanced salt solution containing moxifloxacin (0.5 mg/mL) after the operation. The intraoperative outcome measures were operative time (min), phaco time (s), aspiration time (s), cumulative dissipated energy (CDE), volume of fluid used (mL), and the rate of intraoperative complications. The operative time was calculated from the beginning of the corneal incision to the end of the ophthalmic viscosurgical device aspiration. Patients were followed up on postoperative days 1 and 2, at 1, 3, 7, and 19 weeks, and at 1 year. The postoperative outcome measures were BCVA, IOP, and CECD (cells/mm2). The BCVA and CECD measurements were obtained at 7 and 19 weeks postoperatively, while IOP measurements were obtained at 7, 19 weeks, and 1 year postoperatively. Using the method of Poley et al. and based on the preoperative IOP, the POAG and control groups were divided into subgroups for analysis: those with IOP levels above and below 15 mmHg [11].
Statistical analyses were performed to compare results among groups using one-way analysis of variance, Kruskal–Wallis test, or Kruskal–Wallis test followed by the Steel–Dwass post hoc test using Excel Toukei® (version 7.0, Esumi Co. Ltd.). Paired t-tests were used to compare preoperative IOP to each postoperative time point. Statistical significance was set at p <.05. The Pearson correlation coefficient was utilized to assess the relationships between IOP decrease and other parameters.
Results
This study comprised 150 eyes of 98 patients with cataract who had undergone phacoemulsification and posterior chamber IOL implantation. Of the 98 patients with cataract, 48 had concurrent glaucoma. Table 1 shows the patients’ characteristics and intraoperative parameters. No significant differences were observed in the mean ages between the POAG and control groups (p=.095, unpaired t-test). No significant differences were observed in the operative time, phaco time, aspiration time, and CDE between the POAG and control groups (p=.38, p=.68, p=.31, and p=.66, respectively; unpaired t-test). Furthermore, no significant differences were observed in the volume of fluid used between the POAG and control groups (p=.80, unpaired t-test).
In this study, patients first diagnosed with glaucoma had their IOP measured preoperatively, without glaucoma medications, if they were scheduled for cataract surgery within 2 months. Patients with POAG were not treated for glaucoma before cataract surgery; therefore, they received fewer medications before the surgery. Of the 75 eyes, 25 received glaucoma medications before cataract surgery, while 50 underwent surgery without medications. Seven patients commenced glaucoma medications within 1 year after cataract surgery. None of the patients required glaucoma surgery or additional laser treatment during follow-up.
Table 2 shows the pre-and post-operative changes in BCVA. No significant differences were observed in the BCVA preoperatively, 7 and 19 weeks, and 1 year postoperatively between the POAG and control groups (p=.53, .08, .083, and .08, respectively; unpaired t-test). BCVA between preoperative and 7 weeks postoperative, preoperative and 19 weeks postoperative, and preoperative and 1 year postoperative in the POAG and control groups differed significantly (all p<.01, paired t-test).
Table 3 shows the changes in the CECD. No significant differences were observed in the CECD preoperatively, 7, and 19 weeks postoperatively between the POAG and control groups (p=.57, .43, and .68, respectively, unpaired t-test). The CECD between preoperative and 7 weeks postoperative in the POAG group differed significantly (p=0.036, paired t-test). However, no significant differences were observed in the CECD between preoperative and 19 weeks postoperative in the POAG group (p=.20, paired t-test). No significant differences were observed in the CECD between preoperative and 7 weeks postoperative (p=.48, paired t-test) and between preoperative and 19 weeks postoperative in the control group (p=.18, paired t-test).
Table 4 shows the changes in the IOP. No significant differences were observed in the IOP preoperatively and 1 year postoperatively between the POAG and control groups (p=.57 and .13, respectively, unpaired t-test). However, the IOP between the POAG and control groups 7 and 19 weeks postoperatively differed significantly (p=.011 and .025, respectively, unpaired t-test). The preoperative and postoperative IOP at 7, 19 weeks, and 1 year in the POAG and control groups differed significantly (p<.01, paired t-test).
Table 5 shows the changes in the IOP of the subgroups with preoperative IOP above and below 15 mmHg of the POAG and control groups. In the POAG group, IOP significantly decreased at 7 weeks postoperatively and remained significantly lower at 1 year postoperatively in subgroups with preoperative IOP below and above 15 mmHg (all p<.01, paired t-test). In the control group, IOP significantly decreased at 7 weeks postoperatively and remained significantly lower at 1 year postoperatively in subgroups with preoperative IOP below and above 15 mmHg (all p<.01, paired t-test).
Table 6 shows the Pearson correlation coefficients between the IOP decrease 1 year after surgery and other parameters. The analysis revealed a significant correlation between IOP decrease and preoperative IOP in the POAG and control groups (p=.002 and .048, respectively). No other significant correlations were observed regarding age, operative time, phaco time, aspiration time, CDE, and volume of fluid used.
The POAG group had an average of 0.37 ± 0.56 (mean ± SD) glaucoma medications preoperatively, which significantly decreased after cataract surgery to an average of 0.093 ± 0.29 at 1 year postoperatively (p<.01, unpaired t-test). No intraoperative complications and capsulorrhexis tears were observed in the POAG or control groups.
Discussion
This study revealed that the eight-chop technique had an operative time of 4.71–4.87 minutes in the POAG and control groups, which is extremely shorter than other techniques that require 10–19 minutes [19,20,21]. Furthermore, this technique had lower phaco time and CDE, and the volume of fluid used is only one-third to one-fourth of that used by other techniques [21,22]. Particularly, using a low volume of fluid may influence trabecular meshwork cells and Schlemm's canal cells, including corneal endothelial cells, since the ultrasound and irrigation/aspiration tips are inserted into the eye for a shorter period.
CECD assessment is crucial for comparing various techniques because it represents the true summation of intraocular insult during surgery [23]. Previous studies have reported a 5–16% decrease in CECD after cataract surgery in the first few postoperative months [19,20,21,24]. However, in this study, the decrease was only 1.5% and 1.2% at 7 and 19 weeks postoperatively, respectively, in the POAG group, and 0.8% and 1.4% at 7 and 19 weeks postoperatively, respectively, in the control group. These results indicate that the eight-chop technique may be advantageous in minimizing the surgical involvement of the intraocular tissues, including the trabecular meshwork and Schlemm's canal.
Many investigators have reported an IOP decrease after phacoemulsification cataract extraction and IOL implantation in patients without preexisting disease [7,8]. Irak-Dersu et al. observed a 1–1.4 mmHg (4–8%) reduction in IOP after cataract surgery [9]. Shingleton et al. observed a slightly higher (9–10%) IOP reduction after clear corneal phacoemulsification in normal patients [6]. Poley et al. reviewed the charts of 223 eyes of normal patients after phacoemulsification and discovered that the IOP reduction was 1.4 mmHg (8.8%) at 1 year, which remained at a mean of 1.6 mmHg (10.0%) at 10 years [11]. Furthermore, postoperative IOP changes are proportional to preoperative IOP. For example, normal eyes with a mean preoperative IOP of 12.7 mmHg had a 0.2 mmHg (0.1%) increase in IOP at 1 year compared to preoperative levels [11]. Furthermore, in POAG eyes with a preoperative mean IOP of 11.6 mmHg, a 1.3-mmHg (0.1%) increase in IOP was reported after 1 year compared to preoperative levels [25]. In this study, IOP reduction rate was 12.7% in the POAG group and 12.5% in the control group at 1 year postoperatively, which is higher than previously reported data in both groups. Furthermore, in the POAG and control groups with IOP below 15 mmHg, IOP significantly decreased (p<0.01, paired t-test) at 7 weeks and remained significantly lower at 1 year postoperatively. However, Poly et al. reported increases in IOP in the POAG and normal groups at 1 year compared to preoperative levels [11,25]. One possible reason for the greater IOP reduction may be that the eight-chop technique is superior to the divide-and-conquer and phaco-chop techniques in minimizing the surgical involvement of the intraocular tissues. Phacoemulsification may lower postoperative IOP; the higher the preoperative IOP, the greater its IOP-lowering effect. However, surgical involvement may reduce the IOP-lowering effect of phacoemulsification. Therefore, Poly et al. could not detect IOP reduction in the group with the lowest preoperative IOP [11,25], suggesting that the surgical involvement of the technique used may have significantly counteracted the effect of IOP reduction. The eight-chop technique is less invasive and may have preserved the IOP-lowering effect of phacoemulsification.
The average number of medications used before surgery would be 1.04 ± 0.56 preoperatively, and the average number of glaucoma medications was 0.093 ± 0.291 1 year postoperatively because the 50 eyes that were not treated for glaucoma before surgery also required at least one glaucoma medication, assuming that patients received one glaucoma medication. The average number of glaucoma medications statistically reduced from baseline at 1 year (p<0.01, paired t-test).
Trabecular meshwork cell loss has been reported in POAG [26,27,28], which could result in reduced outflow facility [26,27,28]. The decrease in CECD after cataract surgery using the eight-chop technique is much less than with the divide-and-conquer and phaco-chop techniques. Therefore, the decrease in trabecular meshwork cells may also decrease, and a more normal trabecular meshwork function might be maintained, lowering IOP and maintaining this function for a longer period.
The phacoemulsification techniques employed in previous reports on changes in IOP after phacoemulsification were the divide-and-conquer [2,9], stop and chop [8,9,10], or an unknown [5,11,12,13,14] technique. No reports used the prechop or phaco-chop techniques. The phaco time, aspiration time, CDE, and volume of fluid used, including operative time, must be measured when examining changes in IOP after phacoemulsification cataract surgery. However, to our knowledge, no previous papers reporting the effects of phacoemulsification cataract surgery on IOP have reported intraoperative parameters. Hayashi et al. [5] discovered that the phacoemulsification technique may affect the degree of postoperative IOP reduction. Hence, a well-developed phacoemulsification technique that minimizes surgical involvement of the intraocular tissues when examining changes in IOP after phacoemulsification cataract surgery must be employed. Majstruk et al. reported that cataract surgery via phacoemulsification resulted in a clinically insignificant decrease in IOP and no change in the number of glaucoma medications after 1 year of follow-up for patients with medically controlled mild or moderate POAG. Moreover, they concluded that an additional procedure should be considered for patients with POAG, as standalone cataract surgery may not be beneficial [2]. However, they utilized the divide-and-conquer phacoemulsification technique, and intraoperative parameters, including operative time, were not reported. In addition, the high rate of posterior capsule rupture at 5.71% indicates that the surgical technique might have been ineffective in lowering postoperative IOP.
Our study supports previous reports highlighting the benefits of phacoemulsification surgery in managing patients with cataract who require IOP reduction. In the case of a glaucomatous eye, the expected reduction of IOP by 1.9 mmHg or 12.7% after cataract surgery may be insufficient; however, even a small IOP-lowering effect may inhibit glaucoma progression. This decrease in IOP may be approximately comparable to the response achieved with a single pharmacological antihypertensive agent, and the effect of phacoemulsification on IOP might last at least 1 year.
This study did not compare the results of the eight-chop technique with the divide-and-conquer or phaco-chop techniques, and this should be fully considered when evaluating the present results. However, many other studies have been conducted using the divide-and-conquer and phaco-chop techniques.
In further studies, changes in IOP after cataract surgery using the eight-chop technique should be investigated in patients with glaucoma, such as primary angle-closure glaucoma and pseudoexfoliative glaucoma. Although glaucoma surgery may decrease CECD[29] and lead to bullous keratopathy [30], the lowering of IOP by phacoemulsification is considered safe because anatomically, the increase in outflow facility is presumed throughout the entire trabecular meshwork, and the long-term decrease in corneal endothelial cells density is highly unlikely. Further study of the physiology and molecular biology of the trabecular meshwork after phacoemulsification could lead to the development of a more effective cataract surgery with respect to IOP reduction.
Conclusion
Many ophthalmologists consider cataract surgery a technique for reducing IOP in patients with mild to moderate glaucoma while avoiding traditional glaucoma surgery. However, cataract surgery using the eight-chop technique can significantly lower IOP in the long term and increase anterior chamber depth postoperatively. The deeper anterior chamber depth also allows for safer surgery in the future when glaucoma surgery is necessary. Therefore, we should consider cataract surgery as a glaucoma treatment method and employ a phacoemulsification technique that minimizes damage to intraocular tissues.
Author Contributions
Tsuyoshi Sato wrote the main manuscript text and prepared all figures, tables and video. Tsuyoshi Sato reviewed the manuscript.
Funding
There was no funding for this study.
Statement of Ethics
All of the research and measurements followed the tenets of the Declaration of Helsinki and were reviewed and approved by the Sato Eye Clinic Approval Committee (approval number 150106). Written informed consent for participation was obtained from each patient after explaining the nature and possible consequences of the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Conflicts of Interest Disclosures
The author has no commercial or proprietary interest in any of the companies, products, or methods described in this article.:
Abbreviation
IOP = intraocular pressure; PAOG = primary open-angle glaucoma; CECD = corneal endothelial cell density; CDE = cumulative dissipated energy; BCVA = best-corrected visual acuity; SD = standard deviation
References
- Elgin, U; et al. Early postoperative effects of cataract surgery on anterior segment parameters in primary open-angle glaucoma and pseudoexfoliation glaucoma. Turk J Ophthalmol 2016, 46, 95–98. [Google Scholar] [CrossRef]
- Majstruk, L; et al. Long term effect of phacoemulsification on intraocular pressure in patients with medically controlled primary open-angle glaucoma. BMC Ophthalmol 2019, 19, 149. [Google Scholar] [CrossRef]
- Damji, KF; et al. Intraocular pressure following phacoemulsification in patients with and without exfoliation syndrome: a 2 year prospective study. Br J Ophthalmol 2006, 90, 1014–1018. [Google Scholar] [CrossRef] [PubMed]
- Melancia, D; et al. Cataract surgery and intraocular pressure. Ophthalmic Res 2015, 53, 141–148. [Google Scholar] [CrossRef]
- Hayashi, K; et al. Effect of cataract surgery on intraocular pressure control in glaucoma patients. J Cataract Refract Surg 2001, 27, 1779–1786. [Google Scholar] [CrossRef] [PubMed]
- Shingleton, BJ; et al. Three and five year changes in intraocular pressures after clear corneal phacoemulsification in open angle glaucoma patients, glaucoma suspects, and normal patients. J Glaucoma 2006, 15, 494–498. [Google Scholar] [CrossRef] [PubMed]
- Wirbelauer, C; et al. Intraocular pressure in nonglaucomatous eyes with pseudoexfoliation syndrome after cataract surgery. Ophthalmic Surg Lasers 1998, 29, 466–471. [Google Scholar] [CrossRef]
- Shingleton, BJ; et al. Long-term changes in intraocular pressure after clear corneal phacoemulsification: normal patients versus glaucoma suspect and glaucoma patients. J Cataract Refract Surg 1999, 25, 885–890. [Google Scholar] [CrossRef]
- Irak-Dersu, I; et al. Intraocular pressure change after temporal clear corneal phacoemulsification in normal eyes. Acta Ophthalmol 2010, 88, 131–134. [Google Scholar] [CrossRef]
- Jimenez-Roman, J; et al. Effect of phacoemulsification on intraocular pressure in patients with primary open angle glaucoma and pseudoexfoliation glaucoma. Int J Ophthalmol 2017, 10, 1374–1378. [Google Scholar]
- Poley, BJ; et al. Long-term effects of phacoemulsification with intraocular lens implantation in normotensive and ocular hypertensive eyes. J Cataract Refract Surg 2008, 34, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Salimi, A; et al. Matched cohort study of cataract surgery with and without trabecular microbypass stent implantation in primary angle-closure glaucoma. Am J Ophthalmol 2021, 224, 310–320. [Google Scholar] [CrossRef]
- Iancu, R; Corbu, C. Intraocular pressure after phacoemulsification in patients with uncontrolled primary open angle glaucoma. J Med Life 2014, 7, 11–16. [Google Scholar]
- Falck, A; et al. A four-year prospective study on intraocular pressure in relation to phacoemulsification cataract surgery. Acta Ophthalmol 2011, 89, 614–616. [Google Scholar] [CrossRef]
- Sato, T. Efficacy and safety of the eight-chop technique in phacoemulsification for cataract patients. J Cataract Refract Surg 2023, 49, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Akahoshi, T. Phaco Prechop." Phaco Chop and Advanced Phaco Techniques; Chang, DF, Ed.; SLACK Incorporated: Thorofare, 2013; Vol. 1, pp. 55–76. [Google Scholar]
- Akahoshi, T. Phaco Prechop: re-evaluation of single-handed phacoemulsification using a new nucleofracture technique. Atarashii Ganka 1999, 16, 1219–1233. [Google Scholar]
- Emery, JM. Kelman phacoemulsification; patient selection. In Extracapsular Cataract Surgery; Emery, JM, Mclyntyre, DJ, Eds.; CV Mosby: St Louis, 1983; Vol. 1, pp. 95–100. [Google Scholar]
- Miyata, K; et al. Efficacy and safety of the soft-shell technique in cases with a hard lens nucleus. J Cataract Refract Surg 2002, 28, 1546–1550. [Google Scholar] [CrossRef]
- Sato, M; et al. Soft-shell technique using Viscoat and Healon 5: a prospective, randomized comparison between a dispersive-viscoadaptive and a dispersive-cohesive soft-shell technique. Acta Ophthalmol 2008, 86, 65–70. [Google Scholar] [CrossRef]
- Igarashi, T; et al. Effects of hydrogen in prevention corneal endothelial damage during phacoemulsification: a prospective randomized clinical trial. Am J Ophthalmol 2019, 207, 10–17. [Google Scholar] [CrossRef]
- Helvacioglu, F; et al. Outcomes of torsional microcoaxial phacoemulsification performed by 12-degree and 22-degree bent tips. J Cataract Refract Surg 2013, 39, 1219–1225. [Google Scholar] [CrossRef]
- Upadhyay, S; et al. Comparative evaluation of modified crater (endonucleation) chop and conventional crater chop techniques during phacoemulsification of hard nuclear cataracts: A randomized study. Indian J Ophthalmol 2022, 70, 794–798. [Google Scholar] [CrossRef]
- Park, J; et al. Comparison of phaco-chop, divide-and-conquer, and stop-and-chop phaco techniques in microincision coaxial cataract surgery. J Cataract Refract Surg 2013, 39, 1463–1469. [Google Scholar] [CrossRef]
- Poley, BJ; et al. Intraocular pressure reduction after phacoemulsification with intraocular lens implantation in glaucomatous and nonglaucomatous eyes: evaluation of a causal relationship between the natural lens and open-angle glaucoma. J Cataract Refract Surg 2009, 35, 1946–1955. [Google Scholar] [CrossRef]
- Alvarado, J; et al. Trabecular meshwork cellularity in primary open-angle glaucoma and nonglaucomatous normals. Ophthalmology 1984, 91, 564–579. [Google Scholar] [CrossRef]
- Grierson, I; Howes, RC. Age-related depletion of the cell population in the human trabecular meshwork. Eye (Lond) 1987, 1, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Tektas, OY; Lütjen-Drecoll, E. Structural changes of the trabecular meshwork in different kinds of glaucoma. Exp Eye Res 2009, 88, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Fang, CEH; et al. Corneal endothelial cell density loss following glaucoma surgery alone or in combination with cataract surgery: a systematic review protocol. BMJ Open 2021, 11, e050992. [Google Scholar] [CrossRef] [PubMed]
- Saini, C; et al. Glaucoma in patients with endothelial keratoplasty. Cornea 2022, 41, 1584–1599. [Google Scholar] [CrossRef]
- Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
Figure 1.
Eight-choppers. (a) The Eight-chopper I (SP-8193; ASICO, Westmont, Illinois, USA). (b) The Eight-chopper II (SP-8402; ASICO, Westmont, Illinois, USA). (c) The Lance-chopper (SP-9989; ASICO, Westmont, Illinois, USA).
Figure 1.
Eight-choppers. (a) The Eight-chopper I (SP-8193; ASICO, Westmont, Illinois, USA). (b) The Eight-chopper II (SP-8402; ASICO, Westmont, Illinois, USA). (c) The Lance-chopper (SP-9989; ASICO, Westmont, Illinois, USA).
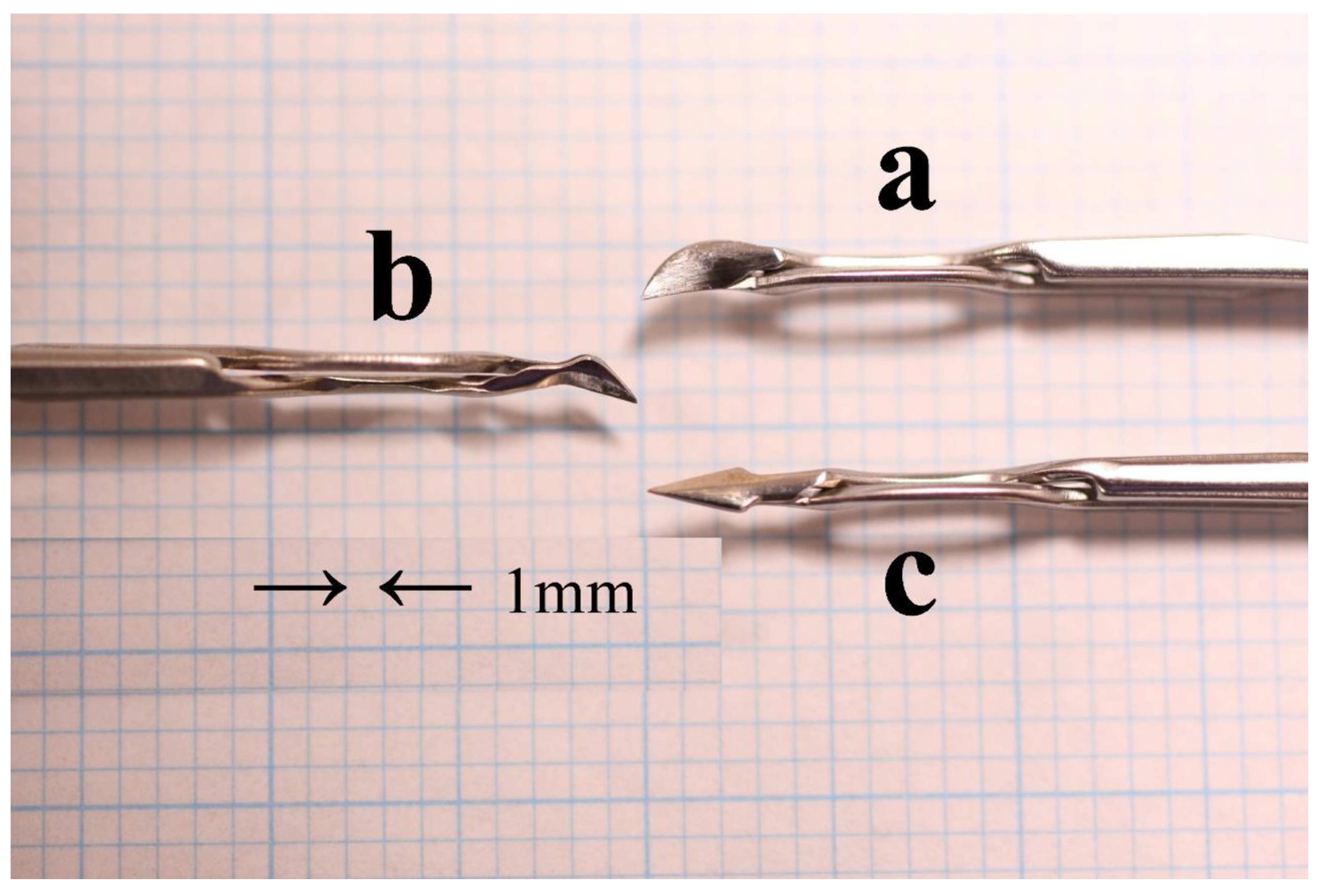

Table 1.
Preoperative characteristics and intraoperative parameters.
| Parameters | POAG group | Control group | P value |
|---|---|---|---|
| n | 75 | 75 | |
| Age (y), mean ± SD | 74.9 ± 6.8 | 73.2 ± 5.6 | 0.095a |
| Sex, n (%) M | 22 (29%) | 23 (31%) | 0.86b |
| F | 53 (71%) | 52 (69%) | |
| Operative time (min), mean ± SD | 4.71 ± 5.2 | 4.87 ± 1.15 | 0.38a |
| Phaco time (s), mean ± SD | 15.1 ± 5.2 | 14.8 ± 5.7 | 0.68a |
| Aspiration time (s), mean ± SD | 73.4 ± 17.7 | 76.4 ± 18.2 | 0.31a |
| CDE, mean ± SD | 6.65 ± 2.27 | 6.47 ± 2.56 | 0.66a |
| Volume of fluid used (mL), mean ± SD | 28.4 ± 7.8 | 28.7 ± 7.2 | 0.80a |
CDE = cumulative dissipated energy. aNo significant difference between the groups (unpaired t-test). bNo significant difference between the groups (Chi-square test).
Table 2.
Pre- and post-operative BCVA (logMAR) measurements of the study eyes.
| Parameters | POAG group | Control group | P Value | ||
|---|---|---|---|---|---|
| Preop | 0.15 ± 0.24 | 0.18 ± 0.33 | 0.53a | ||
| 7-wk postop | -0.031 ± 0.15 | -0.063 ± 0.037 | 0.080a | <0.01b | <0.01c |
| 19-wk postop | -0.032 ± 0.16 | -0.065 ± 0.036 | 0.083a | <0.01b | <0.01c |
| 1-y postop | -0.027 ± 0.18 | -0.063 ± 0.034 | 0.080a | <0.01b | <0.01c |
BCVA = best-corrected visual acuity; POAG = primary open-angle glaucoma. aNo significant difference between the groups (unpaired t-test). bSignificant difference between the preoperative and respective time values in the POAG group (paired t-test). cSignificant difference between the preoperative and respective time values in the control group (paired t-test).
Table 3.
Pre- and post-operative corneal endothelial cell density measurements (cells/mm2) of the study eyes.
Table 3.
Pre- and post-operative corneal endothelial cell density measurements (cells/mm2) of the study eyes.
| Parameters | POAG group n=29 | Control group n=26 | P Value | ||
|---|---|---|---|---|---|
| Preop | 2565 ± 202 | 2601 ± 253 | 0.57a | ||
| 7-wk postop | 2525 ± 210 | 2574 ± 249 | 0.43a | 0.036b | 0.48d |
| cell loss (%) | 1.5 ± 4.0 | 0.8 ± 6.8 | |||
| 19-wk postop | 2534 ± 225 | 2561 ± 257 | 0.68a | 0.20c | 0.18d |
| cell loss (%) | 1.2 ± 4.9 | 1.4 ± 5.6 | |||
POAG = primary open-angle glaucoma. aNo significant difference between the groups (unpaired t-test). bSignificant difference between the preoperative and respective time values in the POAG group (paired t-test). cNo significant difference between the preoperative and respective time values in the POAG group (paired t-test). dNo significant difference between the preoperative and respective time values in the control group (paired t-test).
Table 4.
Mean IOP (mmHg) and mean decrease in IOP (mmHg) over time.
| Mean IOP ± SD (Decrease) | |||||||
|---|---|---|---|---|---|---|---|
| Parameters | POAG group | Control group | PValue | ||||
| Preop | 15.0 ± 1.9 | - | 14.4 ± 2.3 | - | 0.057a | ||
| 7-wk postop | 12.7 ± 1.9 | (2.3 ± 1.5) | 11.8 ± 2.5 | (2.6 ± 1.7) | 0.011b | <0.01c | <0.01d |
| 19-wk postop | 12.8 ± 2.1 | (2.2 ± 1.5) | 12.0 ± 2.2 | (2.4 ± 1.5) | 0.025b | <0.01 c | <0.01d |
| 1-y postop | 13.1 ± 1.9 | (1.9 ± 1.4) | 12.6 ± 2.4 | (1.8 ± 1.2) | 0.13a | <0.01 c | <0.01d |
IOP = intraocular pressure; POAG = primary open-angle glaucoma; SD = standard deviation. aNo significant difference between the groups (unpaired t-test). bSignificant difference between the groups (unpaired t-test). cSignificant difference between the preoperative and respective time values in the POAG group (paired t-test). dSignificant difference between the preoperative and respective time values in the control group (paired t-test).
Table 5.
Mean IOP (mmHg) and mean decrease in IOP (mmHg) of preoperative IOP above and below 15 mmHg Groups in POAG and control groups.
Table 5.
Mean IOP (mmHg) and mean decrease in IOP (mmHg) of preoperative IOP above and below 15 mmHg Groups in POAG and control groups.
| POAG group | ||||||
| Examination | IOP above 15 mmHg Group n=38 | PValue | IOP below 15 mmHg Group n=37 | PValue | ||
| Preoperative | 16.6 ± 1.1 | - | 13.6 ± 1.1 | - | ||
| 7 weeks | 13.9 ± 1.7 | (2.7 ± 1.6) | <0.01a | 11.6 ± 1.6 | (1.9 ± 1.4) | <0.01a |
| 19 weeks | 14.2 ± 1.6 | (2.4 ± 1.6) | <0.01a | 11.5 ± 1.7 | (2.0 ± 1.4) | <0.01a |
| 1 year | 14.4 ± 1.4 | (2.1 ± 1.5) | <0.01a | 11.8 ± 1.3 | (1.8 ± 1.3) | <0.01a |
| Control group | ||||||
| IOP above 15 mmHg Group n=37 | PValue | IOP below 15 mmHg Group n=38 | PValue | |||
| Preoperative | 16.6 ± 1.3 | 12.6 ± 1.1 | ||||
| 7 weeks | 13.7 ± 1.9 | (2.9 ± 2.0) | <0.01a | 10.3 ± 1.7 | (2.3 ± 1.5) | <0.01a |
| 19 weeks | 13.8 ± 1.6 | (2.9 ± 1.7) | <0.01a | 10.6 ± 1.6 | (2.0 ± 1.3) | <0.01a |
| 1 year | 14.6 ± 1.3 | (2.0 ± 1.3) | <0.01a | 10.9 ± 1.7 | (1.7 ± 1.2) | <0.01a |
IOP = intraocular pressure; POAG = primary open-angle glaucoma; SD = standard deviation. Mean ± SD. aSignificant difference between preoperative and respective time values (paired t-test).
Table 6.
Pearson’s correlation coefficients between IOP decrease after 1 year of surgery and other parameters.
Table 6.
Pearson’s correlation coefficients between IOP decrease after 1 year of surgery and other parameters.
| POAG group (n=75) | Control group (n=75) | |||
|---|---|---|---|---|
| Parameters | r value | P value | r value | P value |
| Age | 0.177 | 0.129 | -0.0537 | 0.647 |
| Preop IOP | 0.354 | 0.002a | 0.229 | 0.048a |
| Operative time | 0.134 | 0.252 | -0.134 | 0.251 |
| Phaco time | 0.137 | 0.243 | -0.019 | 0.873 |
| Aspiration time | 0.0195 | 0.868 | -0.0785 | 0.503 |
| CDE | 0.139 | 0.234 | -0.0559 | 0.633 |
| Volume of fluid used | 0.0530 | 0.652 | -0.0608 | 0.604 |
IOP = intraocular pressure; POAG = primary open-angle glaucoma; CDE = cumulative dissipated energy. aStatistically significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



