Submitted:
12 December 2025
Posted:
15 December 2025
You are already at the latest version
Abstract
Background: In healthcare, Electronic Medical Records (EMRs) offer centralized access to patient data and enable evidence-based clinical decision-making. and operational efficiency. However, they have introduced administrative burdens for the clinicians, potentially impacting job satisfaction and care quality. Despite the widespread EMR adoption in Saudi Arabia, the issue of time burden related to EMRs and the factors re-lated to it are underexplored. Objectives: To measure the average number of hours (per month and as percentage out of total monthly working hours) of EMR use among physicians and nurses, compare the mean monthly hours of EMR use between them, and identify the demographic predictors of extended hours of EMR use. Moreover, it aims to understand the perceived challenges and barriers of timely filling EMRs, and the impact of EMRs on quality of patient care. Methods: A sequential mixed-methods study was conducted at three Security Forces Hospitals in Riyadh, Dammam, and Makkah. Quantitively, a correlational cross-sectional design was used was employed with multistage stratified sampling using a validated 30-item questionnaire, and data were analyzed using differential and inferential statistics. The qualitative phase in-volved purposive sampling of ten clinicians and semi-structured interviews analyzed through thematic analysis. Results: A total of 503 professionals (162 physicians, 341 nurses) participated. Majority were females (67.2%), aged 30 to 40 years (44.9%), and non-Saudi (62%). Nurses reported significantly higher mean of EMR usage hours/day than physicians (5.43 versus 4.34 hours/day, p=0.001). Significant predictors of ex-tended EMR use include age 30-50 years, female gender, non-Saudi nationality, higher education, nursing profession, longer healthcare experience, 5-10 years EMR experi-ence, 10+ hours EMR training, and participants from Makkah. Qualitative analysis identified barriers such as infrastructure constraints, system performance and tech-nical issues, lack of IT support, and workflow and professional burden. Regarding EMR impact, they improved professional practice and patient safety, however, concerns were raised regarding adjustments in work routine Conclusion: EMR use carries con-siderable administrative burden, especially nurses when compared to physicians. Ad-dressing the identified barriers through targeted training, better system design, and improved workflows could boost efficiency and support high-quality patient care. The findings offer evidence-based insights to guide policy and system-level improvements.
Keywords:
Electronic Health Records
; EMR burden
; healthcare providers
; Saudi Arabia
; nurse workload
; digital health
; documentation time
; mixed‐methods research
1. Introduction
In the modern healthcare system, Electronic Medical Records (EMRs), also known as Electronic Health Records (EHRs), have increasingly replaced traditional paper systems since they offer a more accurate, accessible, and efficient method for documenting, managing, and sharing patient information across various care settings [1,2,3]. Their capability to provide real-time access to patient information enables faster, evidence-based clinical decision-making, resulting in more coordinated and higher-quality patient care [4,5].
In Saudi Arabia, national e-health programs led by the Ministry of Health have rapidly expanded the EMR adoption. These programs aim to create a unified digital infrastructure by transitioning medical records from paper to electronic formats across public and private healthcare facilities nationwide [6,7].
Nevertheless, many healthcare institutions face real-world barriers that prevent them from fully realizing the value these systems are meant to deliver. A key challenge is the significant time burden on healthcare professionals, especially nurses and doctors, who are the main users of EMRs [8,9]. Several studies have shown that physicians and nurses often devote more hours to electronic documentation than to face-to-face patient care. This imbalance disrupts the clinical workflow, leading to fatigue, emotional exhaustion, decreased overall job satisfaction, and increased stress and workload for healthcare workers [8,9,10,11].
This concern is particularly relevant within the Saudi context, where the rapid expansion of digital health systems continues to transform care delivery [6,7], and challenges related to usability, system integration, and professional adaptation have been reported [12,13]. However, the issue of time burden related to EMRs remains underexplored in Saudi Arabia, and only a limited number of studies have investigated the specific factors contributing to this challenge or its impact on healthcare professionals [12]. This lack of context-specific research creates a barrier to developing effective, evidence-based strategies aimed at improving EMR usability.
Thus, this study aims to measure the average number of hours (per month and as percentage out of total monthly working hours) of EMR use among physicians and nurses as well as compare the mean monthly hours of EMR use between them. Additionally, it aims to identify the demographic predictors of extended hours of EMR use. Furthermore, it qualitatively aims to understand the perceived challenges and barriers of timely filling EMRs that affect quality of regular healthcare services offered by physicians and nurses to patients as well as the impacts of EMR use on the quality of patient care. By employing a mixed-methods approach, the study can offer insights that inform national policies, support sustainable digital health development, and boost the well-being and efficiency of frontline healthcare staff..
2. Materials and Methods
2.1. Study Design, Setting and Duration
This study employed a sequential mixed-methods design to address the research objectives. The quantitative part employed a correlational cross-sectional design and was used to evaluate patterns of EMR use, compare the application of EMR between nurses and physicians, and identify significant demographic predictors. This was followed by a qualitative phase to explore the perceived barriers and challenges related to EMR use, and the impact of EMR. The study was conducted across three major regional hospitals under the Security Forces Hospital Program in Riyadh, Dammam, and Makkah from January to October, 2025.
2.2. Study Population and Eligibility Criteria
The study population comprised of all the nurses and physicians from the Security Forces Hospital in Riyadh, Dammam, and Makkah. Inclusion criteria required participants to have at least three months of work experience to ensure sufficient familiarity with the EMR system, and only those nurses and physicians who directly utilized the EMR system as part of their daily professional responsibilities were considered eligible. Those with less than three months of clinical experience, as well as administrative and non-clinical staff, were excluded to maintain focus on those directly engaged in patient care and documentation.
2.3. Sampling Technique
For the quantitative study, a multistage sampling technique was used to select a representative sample of physicians and nurses working in Security Forces Hospitals. The study population was stratified into six categories namely professional role, hospital, regional affiliation, nationality, clinical environment, and seniority level. This stratification ensured diverse representation across professional, institutional, cultural, and clinical dimensions. By including these distinct categories, the study design safeguarded against overrepresentation or underrepresentation of specific groups, thereby strengthening the external validity and generalizability of the findings.
For the qualitative study, a purposive sampling technique was employed to select ten participants from the three hospitals [14].
2.4. Sample Size Calculation
The sample size was calculated using an online tool called Epitools, which helps calculate the comparison of two proportions [15]. The main inputs to the calculation were obtained from the literature, which states that physicians spend approximately 21% of their working time on EMRs, while nurses spend about 35% [16]. These percentages were used to define the expected absolute difference of 14% between the two cohorts. The computation was based on a two-sided significance of 0.05, statistical power of 0.80, and a ratio of 1.3:1 between nurses and physicians, which is the approximate ratio of nurses in the clinical facility. With these parameters, the sample sizes had to be at least 156 physicians and 203 nurses, which resulted in a total of 359 participants. By adding 20% non-response rate, the sample size would be increased to 195 physicians and 254 nurses.
2.5. Data Collection Tool
2.5.1. Quantitative Tool
The quantitative data were collected using a structured questionnaire that was adapted from four previously validated studies [17,18,19,20] and refined to align with the study’s objectives. The questionnaire consisted of 30 questions divided into five sections (Supplementary File 1). The first section collected demographic information and comprised of 11 items, with some items tailored exclusively for either nurses or physicians. The second section (EMR usage) consisted of two items. The first item measured the average number of hours per shift/day spent using the EMR system, with response options ranging from “Less than 1 hour” to “More than 6 hours.” The second item explored the range of clinical tasks performed through the EMR system, allowing respondents to select multiple applicable functions. The third section (EMR training and support) comprised three items to assess participants’ EMR training experience, total training hours, perceived adequacy, and challenges encountered while using EMRs. The fourth section (perception of EMR use) consisted of eleven items addressing the barriers and challenges related to EMR systems as well as its perceived impact on patient care, and job satisfaction. The final section (suggestions and recommendations) comprised three open-ended items designed to elicit qualitative insights from participants regarding their experiences with EMRs.
The draft questionnaire was evaluated for content validity by five experts in the field of nursing, epidemiology, health systems management, and EMR specialists. Each item was rated as being essential, useful, and not essential. Using Lawshe’s method, most of the items (85%) achieved the minimum Content Validity Ratio. Extensive expert consensus and significant revisions through feedback served to confirm the content validity of the questionnaire and the final instrument was thorough, relevant and in line with the aims of the study. The questionnaire then underwent a face-validity with a focus group of five nurses and the five physicians examined to tested the clarity, readability and usability of the items. Feedback on ambiguous and problematic items was systematically analyzed, leading to improved clarity, and reduced respondent burden, and suitable to the clinical situation. The internal consistency of the EMR Time Burden Questionnaire was assessed for 11 structured items (Questions 17-27) using Cronbach’s alpha, giving an overall standardized α of 0.78 (95% CI:0.64-0.88), indicating satisfactory internal reliability.
2.5.2. Qualitative Tool
Qualitative data were collected using a semi-structured interview guide consisting of three questions including the hours spent using the EMR per shift, challenges and barriers experienced while using EMR, and the impacts of EMR usage on the respondent’s patient care quality. The researcher asked follow-up questions or additional questions based on the respondent's feedback, especially if the respondent’s feedback was insufficient.
2.6. Data Collection Procedure
For the quantitative phase, the structured questionnaire was hosted online on Google Forms. Upon receiving ethical clearance from the hospital IRB committees, the researcher coordinated with them for identifying the eligible population and stratifying participants proportionally as nurses and physicians. Within each stratum, participants were selected using spreadsheet-based randomization. Next, the IRB facilitated the secure distribution of the questionnaire link exclusively to the randomly selected staff members. The questionnaire remained open until the target sample size of 359 participants was achieved (comprising 156 physicians and 203 nurses).
For the qualitative phase, data was collected by conducting short interviews with five nurses and five physicians at the Security Forces Hospital with at least ten years of experience at Security Forces Hospital and had used the EMR system for at least five years within their respective fields. Additionally, the selected participants held senior positions within the hospital to ensure that they carried greater responsibility and accountability in using the EMR. Participants were invited via formal email which included the researcher’s identity, study title, and objectives. Interviews were conducted at the respondent's hospital and recorded using a phone voice recorder. The interview began with the researcher providing an overview of the study, and confirming the participants willingness to participate, and only proceeded after receiving the respondent's approval.
2.7. Data Analysis
2.7.1. Quantitative Data Analysis
Data were analyzed using the Statistical Package for Social Studies (SPSS 23; IBM Corp., New York, NY, USA). Continuous variables were expressed as mean ± standard deviation, and categorical variables were expressed as percentages. A t-test was used for continuous variables. Ordinal logistic regression was used to assess the predictors of extended hours of EMR use in relation to the demographic characteristics of healthcare professionals. Multiple linear regression analysis was used to assess the predictive factors of perceived challenges and barriers toward EMR use among healthcare professionals. A p-value <0.05 was considered statistically significant. Cronbach’s alpha was used to assess the reliability of the questionnaire.
2.7.2. Qualitative Data Analysis
Qualitative data were analyzed using NVivo software to conduct a thematic analysis, chosen for its ability to efficiently manage, organize, and code large volumes of qualitative data. Thematic analysis followed the six-phase process outlined by Neuendorf et al. (2018): 1. Familiarization: repeated reading of transcripts for immersive understanding. 2. Initial Coding: assigning short labels to relevant data excerpts. 3. Theme Development: grouping related codes into potential themes. 4. Theme Review: refining themes to ensure internal consistency and external distinction. 5. Theme Definition: clearly naming and defining each theme. 6. Reporting: presenting findings in relation to the research questions, supported by direct quotes [21]. Codes were assigned based on the three questions in the interview. The first question is related with how long the participant uses the EMR system. Second question is the challenges and barriers when using the EMR. Third, the impact of using EMR. Two codes were identified related to EMR barriers and challenges based on past literature review, namely delay and time consuming. Besides these two codes, inductive thematic analysis was done to identify new codes for each of the questions that aligned with the study research objectives.
2.8. Conceptual Framework
The theoretical framework in this study is based the assumption that spent by clinicians on EMRs is determined by a combination of personal characteristics, technical exposure and preparation, and environmental and contextual obstacles, and uses the Technology Acceptance Model (TAM) in articulating this relationship since it explains technology-related behavior based on two perceptions, perceived usefulness and ease of use [22]. The study does not directly measure these perceptions, but provides a framework to understand how user characteristics mediate the effectiveness of interaction with EMRs, and directs the objectives of the research and forms the basis of the interpretation of both quantitative and qualitative results (Figure 1).
2.9. Ethical Consideration
Ethical approval for this study was obtained from the King Saud University Institutional Review Board (KSU-HE-25-457) and then from the Security Forces Hospital IRB board (25-786-06). All data were only used for academic purposes. For the questionnaire phase, informed consent was sought, participation in the study was voluntary, and the purpose of the study was explained to the participants prior to consent. No identifying information was asked in the questionnaire (e.g., names or ID numbers) to maintain anonymity. For the interview phase, participants were approached individually and briefed about the aims of the interviews, the scope of the interviews and the voluntary nature of their participation. Prior to the start of the interviews, verbal consent was taken. Interview recordings were securely stored and erased after transcription and analysis. All quotations
3. Results
3.1. Quantitative Data Results
A total of 503 professionals (including 162 doctors and 341 nurses) participated in this study. Table 1 indicates that, most of the respondents were female (67.2%). Physicians were predominantly males (57.4%) while for nurses, majority were females (78.9%). The majority of the participants were aged between 30 to 40 years (44.9%). Regarding nationality, 62% of respondents were non-Saudi. Regarding the position of the physicians, the majority were residents (42.6%). In terms of the primary specialties of the physicians, majority belonged to pediatrics (27.2%). In the nurse category, the largest majority were front-line workers (61.3%), and a majority of nurses worked in inpatient hospital setting (46.6%). In terms of educational level, most respondents (65%) had a bachelor degree. Regarding years of experience in healthcare, majority of the participants (36%) had 10 to 20 years of experience in the field of healthcare. An almost similar percentage (39.8%) reported to have 1 to 5 years’ experience of using EMRs. Lastly, the regional representation of participants indicates that half (50.1%) were located in Riyadh, 26.2 percent in Makkah, and 23.7 percent in Dammam, which is a balanced geographical representation at the three hospital locations.
Table 2 shows the average number of hours of EMR use among physicians and nurses. In general, most of the participants (42.5%) spent over six hours using the EMR per shift/day. Majority of physicians (37.7%) spent between 3 to 4 hours on average and more than half of the nurses (53.7%) more than six hours. Regarding the specific tasks EMR is used for, review of test results (74%), and recording patient histories (69.2%) were most frequently reported by the participants. The highest activities identified among physicians were prescribing medications (88.9%) and upgrading progress notes (88.9%). For nurses, nursing notes (87.4 %) and nursing initial assessment (82.1 %) scored the highest. Most of the respondents (87.1 %) said they received formal training on EMR use, with a higher number of nurses (90.9 %) being trained than the physicians (79%). Regarding the duration of training, almost half (48.9%) of the participants had less than five hours of EMR training, and only 13.1% had over ten hours. Regarding challenges faced when using the EMR, time-consuming data entry (51.3%) was cited most, followed by slow system performance (47.5%). The most common barrier reported by the physicians was time-consuming data-entry (67.91%), while 51.3% of nurses cited slow system performance.
Table 3 shows the total hours per day of EMR use among physicians and nurses which used to calculate the mean of monthly hours of EMR use among physicians and nurses.
Table 4 shows mean of monthly hours of EMR used by physicians and nurses and its percentages out of total monthly working hours. Nurses have higher significant mean of EMR usage hours/day with P-value 0.001. The mean of EMR usage hours/day for nurses and physicians were 5.43 hours/day and 4.34 hours/day, respectively.
Table 5 summarizes predictors of extended EMR. Females were 3.08 times more likely (95% CI: 2.17-4.36, p<0.001) than males to report extended EMR use. Ages 30-40 years (OR=1.94, 95% CI=0.89-2.78, p=0.005) and 40-50 years (OR=1.81, 95% CI=1.09-3.04, p=0.022) were more likely to report extended EMR use/shift by 1.94 and 1.81 times, respectively compared to those <30 years. Non-Saudi healthcare providers spent 2.92 times more time on the EMRs than Saudis (95% CI=1.41-2.09, p<0.001). Nurses were 2.98 times more likely than physicians to spend more time on EMRs per shift (95% CI: 2.12-4.20). Compared to diploma holders, participants with a Master’s (OR=0.50, 95% CI: 0.25-0.99, p=0.047) or Doctorate (OR=0.28, 95% CI=0.14-0.61, p=0.001) were less likely to spend extended hours in EMR use. Professional experience was also a strong predictor, (χ2(4) 18.482, p=0.001) though had a small explanatory value (Nagelkerke pseudo R2=0.039 or 3.9%). Those with 5-10 years (OR=5.05, 95% CI: 1.88-13.55, p=0.001), 10-20 years (OR=5.23, 95% CI: 1.99-13.76, p=0.001), and >20 years of experience (OR=4.15, 95% CI: 1.55-11.14) were more likely to report extended use than those with <1 year. EMR experience of 5-10 years also increased the likelihood extended use (OR=2.13, 95% CI=1.03-4.41, p=0.041). Respondents with ≥10 hours of EMR training were more likely to report extended use (OR=2.33, 95% CI=1.22-4.47, p=0.010). Participants in Makkah were 1.54 times more likely (95% CI: 1.05-2.26, p=0.026) to report longer EMR use compared to Riyadh, while Dammam showed no significant difference (p=0.690).
Table 6 shows the mean score of perceived challenges and barriers facing physicians and nurses when using EMRs. The results revealed significant differences in several areas. Nurses reported receiving significantly more adequate EMR training than physicians (p < 0.001), and also indicated greater immediate technical support than physicians (p = .018). In contrast, physicians expressed significantly higher agreement that EMR documentation improves patient care quality than nurses (p = 0.003). Regarding perceived workload, significantly more nurses agreed that EMR tasks take more time than direct patient care than physicians (p = .001). Additionally, nurses were more likely than physicians to believe that years of experience affect their ability to use EMR (p = 0.003). A significant difference was also observed for perceptions of job position influence affecting EMR usage time, where nurses scored higher than physicians (p < 0.001). Similarly, significantly more nurses agreed that their healthcare setting impacts the time spent on EMR than physicians (p < 0.001). However, there were no significant differences between physicians and nurses in the belief that age affects EMR use (p = 0.186), that EMR affects patient interaction (p = 0.158), or that EMR enhances job satisfaction (p = 0.780 and 0.933 for related items).
Table 7 shows multiple linear regression analysis to assess the predictors factors of perceived challenges and barriers toward EMR use among healthcare professionals. The overall regression model was statistically significant (F=7.298, Sig = 0.000), explaining approximately 11.8% of the variance in perceived challenges, as indicated by the adjusted R². Examination of individual predictors revealed that position, work region, and hours of EMR training were significant predictors of perceived challenges (p < 0.05). In contrast, gender (p = 0.862), age (p = 0.431), nationality (p = 0.209), level of education (p = 0.457), years of experience in healthcare (p = .884), and years of experience using EMR (p = 0.535) were not significant predictors of perceived challenges and barriers.
3.2. Qualitative Data Results
3.2.1. Demographic Profile
The ten respondents in this study were employed at Security Forces Hospitals located in Riyadh, Dammam, and Makkah. Five of the participants were nurse, holding positions such as registered nurse and head nurse. The remaining five respondents included registrars, consultants, and senior staff midwives. The participants’ age ranged from 32 to 57 years, working experience from 10 to 35 years, and the education level ranged from diplomas to PhD.
3.2.2. Hours of EMR Use
The first question in the interview was related to hours of EMR use which aligned with the research objective to estimate the average number of hours of EMR use among physicians and nurses. Based on the interviews with the participants, EMR usage consumes a substantial portion of working hours, and indicates that the time spent on EMRs ranges from as little as 3 hours to as much as 7 hours on a standard 8 to 12-hour shift.
P1 said “I usually use the system for about three to six hours”
P2 said “Yes, I spend four to six hours every day on the new system”
P3 “So usually I spend 6 to 7 hours in using the EMR”
P4 “when it comes to electronic medical records is around four to five hours”
P7 “But on an average, we are doing, you know, in our 12-hour shift, six to seven hours is consumed with this documentation”
P8 “But if I have to compare to previously where we did not have EHR and having to write manually five hours on the HER”
P9 “I am using this EMR over 6 hours of my 12-hour shift”
P10 “So the average time of usage of this EMR in the day is around five to six hours”
Regarding the time spent on EMRs per patient, for a new patient, documentation can take between 10 to 20 minutes, which is roughly 50% of their total appointment time.
P6 “I am seeing one patient. 50% if the time of interview is short, for example, 10 to 20 minutes, it will take 50% of the time”
P6 “So I will interview with the patient for 45 minutes, for example, for the new patient. Maybe I will take to document 10 to 20 minutes”
P7 “One documentation to complete the checklist, it's most probably about 15 minutes per patient”
Thus, the data from the interviews shows that EMR use places a significant time burden on healthcare staff, consuming a substantial portion of their working hours.
3.2.3. Challenges and Barriers Related to EMRs
For EMR challenges and barriers, a total of twelve codes were identified which were grouped into four themes including infrastructure issues, system performance and technical issues, lack of support, and workflow and professional burden. Figure 2 provides an overview of the codes and themes identified for barriers and challenges related to EMR.
3.2.3.1. Infrastructure Issues
Lack of Computers
The lack of an adequate number of computers was cited by several respondents as a significant barrier to EMR implementation. Multiple participants explicitly mentioned that the number of available computers or laptops in their units was insufficient for the number of staff, which directly impacted their ability to use the EMR system efficiently.
P1 “is the number of the computers in the wards is quite less than the number of the doctors”
P9 “we have really challenged with the less computer in our unit”
P10 “lack of laptops or computers for nurses' use”
Computer not up to Date
Another challenge related to the computer is not being up to date.
P2 “hardware challenges that the computers are sometimes not very up to date”
Slow Internet
Some participants said that internet issues hinder them from effectively using EMR system.
P1 “some internet issues are also there”
P8 “the internet connection not being strong enough or it slowed down”
3.2.3.2. System Performance and Technical Issues
Slow System
Many participants mentioned the term “slow system” which relates to the time it takes to respond to commands and some participants explicitly referred to this as a challenge and barrier.
P1 “the system which is installed here is at times we encounter that it is quite slow to respond so there is a time delay”
P3 “slow system”
P4” and also the system is very slow”
P5 “But the main challenges, which is the slow system”
P6 “Previously, we had some issue delay in giving the orders”
P9 “The barrier that I use this system, sometimes when it came to the system slow”
P10 “there are some barriers and challenges being encountered with the EMR, such as slow system”
System Down
System downtime was a major challenge mentioned by six participants.
P2 “sometimes the system goes down”
P5 “But the main challenges, or system down, usually, to give us a hard time”
P6 “and system shut down”
P8 “So when I think about the barriers and challenges that we encounter using the electronic medical records, I think about downtime”
P8 “systems crashing due to updates that are not routinely done”
P9 “system also sometimes freeze”
System Stability
Another concerning issue is system reliability. According to P2, around 5% of the time the system failed to process or give feedback on the task that they do. As result, the user needs to redo the task.
P2 “five percent of the time yes there are issues”
System Access Restriction
Another challenge of using the EMR system is access restriction. P2 said that only consultants have the access for all information. Additionally, certain types of data can only be entered by consultants into the system. In both situations, residents and specialists are excluded. Furthermore, the restriction on access also extend to remote access from outside of the hospital.
P2 “certain entries are only to be entered by consultants rather than specialists or residents a lot of information most information is accessible to all but some information is restricted to consultants”
P2 “there is no remote access available for others I mean only, only a few people have remote access”
User Interface Issue
P5 cited system interface as a huge challenge when using EMR as there are multiple forms for one reorder, which is highly tedious and repetitive. Moreover, users need to move from one page to another for each new data entry.
P5 “The other issue, which is moving between steps, if you want to reorder, make an order for labs, for investigation, for medication, for admission, for referral. So, this is, for me, it's a concern because you need to move from icon to another icon”
System Database Update
One participant mentioned there are functionality issues with the EMR when there is a new type of order and also to change date for reordering.
P6 “But actually, we have some issues, yes, with some requests, especially in the new implemented vaccine order, and how to change the date”
P6 “we'll have some struggles with the new implemented idea…. But the standard system, we have no issue with it”
3.2.3.3. Lack of Support
Lack of support from the IT department
It was mentioned by some participants as contributing to difficulty in using the EMR system.
P1 “updates have been done which we cannot do so there is lack of support from the IT department”
P4 “if we are having some issue with the system, we will call IT. It's quite a late reply or response from this team to fix out whatever is the problem in the system”
P9 “if we have problem with the system, the response from the IT support system is very late.:
P10 “lack of support, and delayed IT support at times”
3.2.3.4. Workflow and Professional Burden
Time Consuming
Three respondents said that EMR is highly time consuming. Moreover, P5 mentioned that EMR is actually taking more time compared to the manual paperwork since the EMR system requires the users to follow documentation criteria and some aspects can only be filled by certain roles.
P3 “Usually the challenge is time consuming”
P5 “But in concern with the time, I can tell you that it is taking more time in comparison with the paperwork, because it's restricting our rules and requires specific documentation and specific rules to go through the system. So, we need to write a note, then we need to write an order and to go to update the visit, to update the diagnosis. So, it takes long time to go through these steps”
P6 “But of course, for us, it will be difficult because you are writing everything in computer and there are no dictations. And of course, it takes time”
Increase in Interactions
Another challenge mentioned by one participant is that EMR use has increased the amount of interaction and need to meet physicians and doctors from other departments regarding EMR management and documentation. This has resulted in an increased workload.
P4 “The challenges that I'm having is the interaction that I'm getting from some department like doctor, nurses, they're calling us from the office”
3.2.4. Impact of EMR Usage
As shown in Figure 3, seven codes were identified related to the impact of using EMR which were grouped into three themes including improved professional practice, improved patient safety, and work routine adjustment.
3.2.4.1. Improved Professional Practice
More Attached with Patient
One participant stated that the EMR made him feel more attached with the patients.
P1 “that I feel more attached to the patient that is that I get know about the patient more”
Organized and Structured
P2 mentioned that his works are now more organized, structured and up to international standard. P2 compared EMR with the traditional system, which he said is really hard to understand due to handwriting, hard to organize and most importantly, cannot be replicated and distributed easily. P3 supported this notion by saying EMR made collecting and documenting data more chronological.
P2 “Now the input is more organized, structured and the documentation is more up to international standards”
P3 “it is the chronological order of collecting of data and documenting patient”
On another note, P4 mentioned that the overall efficiency of her work improved through EMR. This is because now all information and data are located at one location, hence making it easier to manage and access
P4 “The impact that I'm having as an overall efficiency for this clinic in the clinical practice, it is a good thing because everything is in the EMR”
3.2.4.2. Improved Patient Safety
Secured
P5 stated that EMR makes sure the data and information are more secured. There are strict documentation requirement and guidelines as well as restriction on data access. This ensures all the sensitive information and data are highly secured from any internal or external threat. Furthermore, EMRs follow standard documentation guidelines, hence it protects all involved parties from a legal perspective.
P5 “But it's more of safety”
P7 “It's very complete legally”
Solve Handwriting Issue
P6 reported that the EMR system has solved one of the main weakness paperwork systems, which is the difficulty in reading handwriting.
P6 “And even the note itself, it is easier for us to read, not like before, handwritten. Yes, the electronic is better than before. From the point of reading other notes and knowing what has been done before”
P10 “the doctor's orders are written clearly and it will minimize the error in causing medication error because you can see from the system”
3.2.4.3. Work Routine Adjustment
Lost Patient Bedside Time
On contrary, there are also negative impacts of using EMR. P3 said since EMR is time consuming, she lost time that she can spend at patient bedside. Meanwhile for P9, the constant issues with EMR system and infrastructure make her waste time that can be used for other work.
P3 “Oh, it's time consuming because where I could have spent time more to the patient at the bedside”
P7 “six to seven hours is consumed with this documentation. So we have less time for our patients in the bedside”
P9 “Negative way, I waste my time”
Reduce Assessment Time Allocation
In addition, P7 expanded on the time-consuming issues and said that it changes how she attends to the patient as more time is spent with EMRs, less time is devoted on patient bedside and this shapes how the patient is assessed and reassessed. P10 also echoed the same sentiment by saying EMR change her patient care time allocation and she now needs to make sure she has enough time to do EMR before her shifts end. Thus, she reduces the time allocated at patient bedside.
P7 “You know, a brief question from the patient, we automatically and run. Not like, you know, spend time and fully check how are you really doing, talk to them and fully assess the patient as it is. Because it consumes time”
P7 “And then instead of spending time with our patient, you know, establishing rapport, what do you call this one? Understanding their feelings. What happens is that we cut that time to attend to EMR documentation”
P10 “So it affects patient care because we cannot be at the bedside most of the time because we have to complete the required documentation within our shift”
P10 “And sometimes we tend to do more in the computer than to be at the bedside”
Difficulty Reverting to Manual Method
P8 reported that the implementation of EMR changed his work and routine habits. Thus, when the hospital is in emergency situation, or also called as Code Brown, he finds it difficult to revert back to the manual method. P8 said his mind and body are used to EMR and he already forget the manual method. Therefore, when Code Brown occur, his overall workflow declined.
P8 “With the recent Code Brown, we had to write out the blood requests manually. And I had to dig deep into my files of my brain on how to do it, where to get the documentation, what to write, the stickers that need to be printed. So, it slowed. It slowed me down just a tad little bit because I've forgotten how to do the manual thing. Because now it's so much easier to do it electronically. You get what I'm saying?”
4. Discussion
4.1. Mean EMR Use Hours for Physicians and Nurses
In the present study, it was shown that physicians spent an average of 4.34 hours per shift using EMRs, while nurses spent 5.43 hours, suggesting a relatively higher EMR load on the nursing staff. When compared to international studies, the results of the current study on firm and contradict the previous findings, thus demonstrating the diversity of EMR use patterns in different healthcare systems. For instance, lower daily EMR use was reported in studies from the United States [23,24,25,26,27], Japan [28], and Jordan [29]. The difference can be attributed to the tertiary-care setting of the present study, complicated and multidisciplinary care of the patients, broader range of EMR functions, inclusion of nurses and physicians across multiple clinical departments, and higher patient volume.
On the contrary, there are studies that have indicated similar or even higher levels of EMR engagement. For instance, Goldstein et al. (2018) reported an average of 4.3 hours per day using EMRs [30]. The comparably high duration may be due to the comprehensive EMR facilitating a wide range of clinical and administrative tasks. Moreover, the research was carried out in Oregon Health and Science University, which is a huge tertiary hospital with high levels of patients and complicated care delivery units. This institutional resemblance to Security Forces Hospital indicates that EMR engagement levels may be similar due to the similar workflow requirements and patient-care complexity. The similarity between the two studies supports the validity of the present findings and shows that the high use of EMRs is not specific to the Saudi setting, but it is a global tendency in technology-based healthcare settings. Another study reported that residents spent 5.38 hours/shift, although this study considered shifts of 12-hours and units where patient acuity levels were greater [31].
4.2. Difference Between EMR Use Between Physicians and Nurses
The most salient observation of this study is the significantly higher EMR use among nurses compared to physicians (p=0.001). Several plausible reasons may explain this. Firstly, nursing practice is an ongoing, patient-related process throughout the shift [32]. Moreover, since nurses care for multiple patients and keep up-to-date records on each patient, their engagement with the EMR is not limited to specific blocks of activities [33]. By contrast, the work of physicians in EMR is usually centralized in patient interactions and decision-making activities. The difference in workflow generates an accumulated EMR time among nurses [30]. Secondly, in the current study setting, EMR has a wider scope of functional coverage among nurses (e.g., medication administration, monitoring of vital signs, pre- and post-operative examinations) that require continuous entry and real-time updates. This increases the general EMR interaction with nurses compared to physicians [27]. Thirdly, regulatory and institutional procedures can require nurses to fill detailed and redundant documentation forms to comply with safety, quality, and accreditation standards [34]. Other reasons are associated with the staffing patterns, delegation and role distribution [35].
This role-based difference in EMR use may lead to high fatigue, burnout, and job dissatisfaction among nurses [36], suggesting that medical organizations should reassess the documentation procedures to ensure a fair digital workload, and the need for role-based EMR optimization and supportive interventions to decrease the number of documents that nursing staff have to complete.
4.3. Predictors of Extended EMR Use
Gender was found to be a predictive variable of extended EMR use with female participants spending more time compared to males. Similarly, it was earlier reported that female physicians spent significantly more time on EHR-related activities in eight hours of planned clinical shifts compared to male physicians (5.81 versus 5.23 h) [37]; indicating that female clinicians might have different communication expectations or documentation patterns resulting in higher EMR involvement.
Regarding nationality, non-Saudi workers were found to dedicate more time to EMRs than their Saudi counterparts. Non-native clinicians might have lengthy documentation times due to language barriers, differences in previous EMR exposure, and institutional norms [38,39]. These are probably quite influential in Saudi Arabia, where the healthcare workforce is comparatively very multinational [12]. The findings, therefore, indicate that EMR optimisation plans must be tailored to local training modules that support the presence of the diverse linguistic and cultural backgrounds, thus maximizing efficiency within the entire workforce.
Clinicians who had master or doctorate were less likely to spend too much time using EMR as compared to those with diplomas or bachelor’s degrees. Higher educational attainment has been frequently linked with an increase in information-management and digital-literacy skills [40]. Moreover, those with advanced degrees may work as supervisors or decision makers, which could decrease direct data-entry time. User capability and the understanding of health informatics have been indicated to have a positive impact on system efficiency, leading to faster documentation and fewer cognitive demands [41].
Years of professional experience was an important predictor of extended EMR use. Clinicians with moderate to extensive experience spent more time on EMRs than less experienced clinicians. Generally, mid-career clinicians both practice and have administrative duties, which increases their load of documentation. Residents and junior physicians have been reported to spend more time on EHRs on average with patients at first but become more efficient over time, but senior staff tend to outsource documentation [26]. At the Middle Eastern hospital, mid-career professionals were involved in both care provision and supervision, resulting in increased cumulative EMR interaction time [42]. This observation points to the need to develop EMR systems that effectively facilitate multitasking and supervisory roles.
Clinicians with 5 to 10 years of experience with EMR spent significantly more time using the system. This trend is possibly an indication that users with moderate experience are the most active in EMR daily usage, and beginners are still learning the platform, and the most seasoned users might have learned shortcuts or outsourced some of their tasks. Similar patterns have been reported through audit-log interactions of EMR use, with clinicians with intermediate experience having higher interactions with more EMR modules and more interactions with alerts, in-basket messages, and order entries than other groups [43,44].
Longer EMR training duration (10+ hours) demonstrated a longer time of EMR utilization. This might seem paradoxical as training is usually anticipated to improve efficiency and reduce time spent on the system. However, it has been shown that extended training leads to more engagement with the advanced features of the system [45].
4.4. Challenges and Barriers Related to EMR
Infrastructure issues (such as lack of enough computers, outdated hardware, and slow internet connectivity) emerged as a key barrier to timely and proper EMR use among nurses and physicians. Similar constraints have been noted in a study conducted in Addis Ababa [46], and are associated with documentation delays [47,48], as well as risks to patient safety and data integrity [49]. These issues have an impact on the workflow, decrease the productivity, and can affect the quality-of-care, as decisions may be based on outdated or incomplete data [50,51]. This finding highlights the need for investment in hardware enhancement, the number of workstations provided per clinician, and reliable internet. Additionally, the routine upkeep and upgrading of computers, including maintaining current processing capacity and adequate memory, can reduce latency and downtime. Institutional leadership and IT governance should consider infrastructure support as a part of EMR usability and data quality. Unless these underlying infrastructure problems are addressed, other interventions, including training, workflow optimisation, or user-interface improvements, are likely to be limited in their ability to reduce EMR time burden or improve documentation quality.
System performance and technical issues (such as slow system, system downtime and instability) was another obstacle found to affect workflow and hamper the quality of clinical documentation. A previous study in Saudi Arabia indicated that slow system performance was a major cause of user dissatisfaction with EMRs due to its interference with time-sensitive work and distraction of clinical decision-making [52]. In South Africa, it was shown that a significant impediment to EMR reliability was regular server outages which necessitated clinicians to defer data entry or occasionally use paper-based documentation and thus disrupted the digital record-keeping process [53]. Unexpected or frequent downtimes not only influence productivity, but can also threaten patient safety [54], since they interfere with the user workflow and cognitive flow as clinicians have to alternate between troubleshooting and patient care activities, which can reduce their efficiency and cause documentation mistakes [55]. System access restriction was another concern mentioned. While this helps to secure data, over-enforcement may hinder cooperation and decelerate clinical practices. According to Dutta and Hwang (2020), Saudi healthcare facilities that had restrictive EMR access policies impeded interdepartmental communication and delayed decision-making about patients, highlighting the need to balance security with usability [56]. The study participants also reported challenges in using the complicated interfaces of EMR. Weak user interface design has been directly linked to longer data entry time and perceived workload in clinicians [57]. Furthermore, frequent system database updates were reported to cause short-term interruptions and forced users to re-learn existing workflows which sometimes created confusion and opposition especially when announced without prior notice or necessary training. Similarly, in India unplanned system upgrades were linked to reduced short-term productivity and higher user frustration [58]. Addressing these issues involves strong technical infrastructure, forward looking system governance, user-friendly interfaces, and open communication regarding system updates.
A third theme that stood out in the interviews was the felt lack of support from the IT department in cases where technical problems like inability to log in, frozen screen or inability to retrieve data occurred. A lack of responsiveness in the IT department has been reported earlier to contribute to the inhibition of EMR use and increased frustration among Saudi Arabian clinicians [59]. Similarly, another study stressed that a lack of on-site IT support leads to burnout in users, under-use of the system, and diminished perceived value of EMR systems, particularly when the users have to guess the solution to a problem on their own [40]. In view of this finding, it is urgent to build an effective, well-staffed, and responsive IT support system so that the clinical workflow can run smoothly, documentation delays can be reduced, and users remain confident in the EMR technology.
The last theme that emerged related to EMR challenges and barriers was the workflow and professional burden of EMR documentation. Time-consuming documentation was widely reported by participants as a key contributing factor to work strain. Several clinicians opined that EMR entry procedures were lengthy, comprising of several screens and unnecessary fields, taking time away from patient care. This is consistent with a study in the U.S. that reported primary-care physicians spent almost half of their working time on EMR-related activities, resulting in exhaustion and decreased patient interaction [44]. Moreover, the interviewees reported increased interaction related to the extra coordination demanded by the EMR systems, such as periodic alerts, communication, and follow-ups. This is consistent with a study that reported a significant portion of the screen time of physicians was spent on electronic communication processes that led to fragmentation of the workflow and feeling of constant interruption [36].
Regarding the impact of EMRs, one of the main benefits cited in terms of patient safety was the elimination of handwriting errors. This aligns with earlier studies from Saudi Arabia, which reported that EMRs eliminated illegible handwriting and reduced documentation errors [59,60]. Conversely, participants stated that EMRs have a negative impact on work-routine by reducing assessment time and patient bedside time. Similarly, previous research has indicated that EHR systems impeded nurse-patient communication by restricting opportunities for empathetic interaction [33].
4.5. Study Limitations, Strengths, and Future Research
A key strength of this study is its mixed-methods design which enabled gaining a better insight into the phenomenon. The research was carried out in three large Security Forces Hospitals in Riyadh, Dammam and Makkah which enhanced the overall transferability of the findings and the possibility of comparison between various healthcare settings working in the same organizational context and EMR [61]. The study’s large and diverse target population of nurses and physicians allowed comparison between professional groups and highlighted role-based disparities in EMR utilisation. Multistage sampling method increased the representativeness of the sample [62]. The sample size was also sufficiently large to perform rigorous analytical processes, and validated instruments were used which further enhanced the strength of the quantitative findings.
The study has several limitations which should be considered. First, the study involved several sites; however, all of them were Security Forces Hospitals. This restriction limits the extrapolation to other healthcare organizations in Saudi Arabia, especially non-military or private hospitals with different EMR systems, administrative organization, or resources. Second, the quantitative data were self-reported, which may introduce recall bias or social desirability bias despite anonymity measures [63]. Third, the cross-sectional design does not allow determining causality [64]. The qualitative element relied on short interviews with a small sample of participants that limited more in-depth insights on the psychological, cultural, or organizational process that affects EMR use [65]. Inconsistencies in EMR usage measurement across departments, patient loads, and staff roles may also have affected self-reported time, as no objective system-recorded data were used [66]. Finally, lack of time and available resources restricted the extent of data collection and data analysis preventing the examination of other variables like job satisfaction, burnout, or patient outcomes.
Future research should include longitudinal evaluations of EMR use to examine the effect of system upgrades or policy interventions on time burden over time. Moreover, comparative analysis of the public and private hospitals in Saudi Arabia may yield contextual and organisational factors that influence EMR efficiency. Qualitative studies that explore the emotional and cognitive effects of EMR-related workload can enhance the understanding on burnout and job satisfaction among healthcare professionals.
5. Conclusions
The study revealed significant difference in EMR use among healthcare professionals, with nurses experiencing a higher workload than physicians. Gender, age, nationality, position, education, experience, and training of EMR were found to be significant demographic predictors of extended EMR use. These findings were supported by qualitative insights that revealed infrastructure constraints, issues related to system performance and technical instability, lack of IT support, and workflow disruption to be critical barriers to success of EMRs. Participants found EMRs beneficial in improving their professional practice and patient safety, however, concerns were raised regarding adjustments in work routine such as losing bedside time and less patient interaction. The findings emphasize the need for robust infrastructure, responsive IT support, user-centered system design, and comprehensive training programs to enhance EMR efficiency, reduce documentation burden, and support high-quality patient care in digitally evolving healthcare environments.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
AY: Conceptualization; Data curation; Formal analysis; Funding acquisition; Methodology; Sample selection, Development of Tool, Data collection, analysis, and interpretation ,Resources; Software; Validation; Statistical support and visualization of findings ,Writing – original draft; Writing – review & editing. HA: Supervision, Conceptualization; Data curation; Formal analysis; Investigation; Methodology; AI detection Software; Validation; Visualization; Writing – original draft; Writing – review & editing.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review King Saud University (KSU-HE-25-457l) and then from the Security Forces Hospital IRB board (25-786-06).
Informed Consent Statement
Informed consent was sought, participation in the study was voluntary, and the purpose of the study was explained to the participants prior to consent.
Data Availability Statement
Data is contained within the article or the supplementary materials.
Acknowledgments
The authors would like to thank all the selected participants for their participation in the study. Special thanks are extended to all who supported us during the research process, and to the hospital administration staff for facilitating the data collection. On a personal note, we are profoundly grateful to our families and friends for their patience, encouragement, and unconditional love, which sustained our motivation during the most challenging phases of this journey.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Menachemi, N.; Collum, T.H. Benefits and drawbacks of electronic health record systems. Risk Manag Healthc Policy 2011, 4, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Jabali, K.; Jarrar, M.t. Electronic Health Records Functionalities in Saudi Arabia: Obstacles and Major Challenges. Global Journal of Health Science 2018, 10, 50–50. [Google Scholar] [CrossRef]
- Akwaowo, C.D.; Sabi, H.M.; Ekpenyong, N.; Isiguzo, C.M.; Andem, N.F.; Maduka, O.; Dan, E.; Umoh, E.; Ekpin, V.; Uzoka, F.M. Adoption of electronic medical records in developing countries-A multi-state study of the Nigerian healthcare system. Front Digit Health 2022, 4, 1017231. [Google Scholar] [CrossRef] [PubMed]
- Alotaibi, Y.K.; Federico, F. The impact of health information technology on patient safety. Saudi Med J 2017, 38, 1173–1180. [Google Scholar] [CrossRef]
- De Benedictis, A.; Lettieri, E.; Gastaldi, L.; Masella, C.; Urgu, A.; Tartaglini, D. Electronic Medical Records implementation in hospital: An empirical investigation of individual and organizational determinants. PLoS One 2020, 15, e0234108. [Google Scholar] [CrossRef]
- Abdullah Alharbi, R. Adoption of electronic health records in Saudi Arabia hospitals: Knowledge and usage. Journal of King Saud University - Science 2023, 35, 102470. [Google Scholar] [CrossRef]
- National E-Health Strategy. Available online: https://www.moh.gov.sa/en/Ministry/nehs/Pages/Ehealth.aspx (accessed on November 25).
- Babbott, S.; Manwell, L.B.; Brown, R.; Montague, E.; Williams, E.; Schwartz, M.; Hess, E.; Linzer, M. Electronic medical records and physician stress in primary care: results from the MEMO Study. J Am Med Inform Assoc 2014, 21, e100-106. [Google Scholar] [CrossRef]
- Murad, M.H.; Vaa Stelling, B.E.; West, C.P.; Hasan, B.; Simha, S.; Saadi, S.; Firwana, M.; Viola, K.E.; Prokop, L.J.; Nayfeh, T.; et al. Measuring Documentation Burden in Healthcare. J Gen Intern Med 2024, 39, 2837–2848. [Google Scholar] [CrossRef]
- Harris, D.A.; Haskell, J.; Cooper, E.; Crouse, N.; Gardner, R. Estimating the association between burnout and electronic health record-related stress among advanced practice registered nurses. Appl Nurs Res 2018, 43, 36–41. [Google Scholar] [CrossRef]
- Ehrenfeld, J.M.; Wanderer, J.P. Technology as friend or foe? Do electronic health records increase burnout? Curr Opin Anaesthesiol 2018, 31, 357–360. [Google Scholar] [CrossRef]
- Alhur, A. Overcoming Electronic Medical Records Adoption Challenges in Saudi Arabia. Cureus 2024, 16, e53827. [Google Scholar] [CrossRef] [PubMed]
- Khalifa, M. Barriers to Health Information Systems and Electronic Medical Records Implementation. A Field Study of Saudi Arabian Hospitals. Procedia Computer Science 2013, 21, 335–342. [Google Scholar] [CrossRef]
- Ilker, E.; Sulaiman Abubakar, M.; Rukayya Sunusi, A. Comparison of Convenience Sampling and Purposive Sampling. American Journal of Theoretical and Applied Statistics 2015, 5, 1–4. [Google Scholar] [CrossRef]
- Sample size to detect a significant difference between two proportions. Available online: https://epitools.ausvet.com.au/twoproportions (accessed on 20 November).
- What specialty spends the most time on paperwork and administration? Available online: https://www.beckersphysicianleadership.com/physician-workforce/what-specialty-spends-the-most-time-on-paperwork-and-administration (accessed on November 25).
- AlOtaib, Y.; AlSaedi, M. Physicians’ Perceptions and Attitudes toward Use of Electronic Medical Record Systems in Riyadh. World Family Medicine Journal /Middle East Journal of Family Medicine 2022, 20. [Google Scholar] [CrossRef]
- Alessa, T. Clinicians' Attitudes Toward Electronic Health Records in Saudi Arabia. Cureus 2024, 16, e56281. [Google Scholar] [CrossRef]
- Asiri, S. Factors Influencing Electronic Health Record Workflow Integration Among Nurses in Saudi Arabia: Cross-Sectional Study. SAGE Open Nurs 2024, 10, 23779608241260547. [Google Scholar] [CrossRef]
- Al Otaybi, H.F.; Al-Raddadi, R.M.; Bakhamees, F.H. Performance, Barriers, and Satisfaction of Healthcare Workers Toward Electronic Medical Records in Saudi Arabia: A National Multicenter Study. Cureus 2022, 14, e21899. [Google Scholar] [CrossRef]
- Neuendorf, K.A. Content analysis and thematic analysis. In Advanced research methods for applied psychology; Routledge, 2018; pp. 211–223. [Google Scholar]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS quarterly 1989, 319–340. [Google Scholar] [CrossRef]
- Rotenstein, L.S.; Holmgren, A.J.; Downing, N.L.; Bates, D.W. Differences in Total and After-hours Electronic Health Record Time Across Ambulatory Specialties. JAMA Intern Med 2021, 181, 863–865. [Google Scholar] [CrossRef]
- Rotenstein, L.S.; Holmgren, A.J.; Healey, M.J.; Horn, D.M.; Ting, D.Y.; Lipsitz, S.; Salmasian, H.; Gitomer, R.; Bates, D.W. Association Between Electronic Health Record Time and Quality of Care Metrics in Primary Care. JAMA Netw Open 2022, 5, e2237086. [Google Scholar] [CrossRef]
- Overhage, J.M.; McCallie, D., Jr. Physician Time Spent Using the Electronic Health Record During Outpatient Encounters: A Descriptive Study. Ann Intern Med 2020, 172, 169–174. [Google Scholar] [CrossRef]
- Holmgren, A.J.; Lindeman, B.; Ford, E.W. Resident Physician Experience and Duration of Electronic Health Record Use. Appl Clin Inform 2021, 12, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Bakhoum, N.; Gerhart, C.; Schremp, E.; Jeffrey, A.D.; Anders, S.; France, D.; Ward, M.J. A Time and Motion Analysis of Nursing Workload and Electronic Health Record Use in the Emergency Department. J Emerg Nurs 2021, 47, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Seto, R.; Inoue, T.; Tsumura, H. Clinical documentation improvement for outpatients by implementing electronic medical records. Stud Health Technol Inform 2014, 201, 102–107. [Google Scholar] [PubMed]
- Alkasasbeh, A.; Jarrah, S.; Alhusamiah, B.; Tarawneh, F. Factors Influencing the Utilization and Adoption of Electronic Health Records among Nurses in Jordanian Hospitals. Jordan Journal of Nursing Research 2025, 4, 1–13. [Google Scholar] [CrossRef]
- Goldstein, I.H.; Hribar, M.R.; Reznick, L.G.; Chiang, M.F. Analysis of Total Time Requirements of Electronic Health Record Use by Ophthalmologists Using Secondary EHR Data. AMIA Annu Symp Proc 2018, 2018, 490–497. [Google Scholar]
- Wang, J.K.; Ouyang, D.; Hom, J.; Chi, J.; Chen, J.H. Characterizing electronic health record usage patterns of inpatient medicine residents using event log data. PLoS One 2019, 14, e0205379. [Google Scholar] [CrossRef]
- Tamli, N.; Sain, M. Exploring Innovative Strategies For Patient-Centered Care In The Nursing Profession. A Bi-annual South Asian Journal of Research & Innovation 2023, 10, 19–30. [Google Scholar] [CrossRef]
- Forde-Johnston, C.; Butcher, D.; Aveyard, H. An integrative review exploring the impact of Electronic Health Records (EHR) on the quality of nurse-patient interactions and communication. J Adv Nurs 2023, 79, 48–67. [Google Scholar] [CrossRef]
- Camilleri, N.; Henks, N.; Seo, K.; Kim, J.H. EMR usage and nurse documentation burden in a medical intensive care unit. In Proceedings of the International Conference on Human-Computer Interaction, 2022; pp. 165–173. [Google Scholar]
- AlQahtani, M.; AlShaibani, W.; AlAmri, E.; Edward, D.; Khandekar, R. Electronic Health Record-Related Stress Among Nurses: Determinants and Solutions. Telemed J E Health 2021, 27, 544–550. [Google Scholar] [CrossRef]
- Gaffney, A.; Woolhandler, S.; Cai, C.; Bor, D.; Himmelstein, J.; McCormick, D.; Himmelstein, D.U. Medical Documentation Burden Among US Office-Based Physicians in 2019: A National Study. JAMA Intern Med 2022, 182, 564–566. [Google Scholar] [CrossRef] [PubMed]
- Rotenstein, L.S.; Fong, A.S.; Jeffery, M.M.; Sinsky, C.A.; Goldstein, R.; Williams, B.; Melnick, E.R. Gender Differences in Time Spent on Documentation and the Electronic Health Record in a Large Ambulatory Network. JAMA Netw Open 2022, 5, e223935. [Google Scholar] [CrossRef] [PubMed]
- Asaad Nasser Izzuldeen Qasimi, S.A.S.A.M.M.M.T.M.H.A.B.M.H. Privacy Issues Hindering Implementation and Use of Electronic Health Records in the Middle East. Journal of International Crisis and Risk Communication Research 2025, 1274–1278. [Google Scholar] [CrossRef]
- Aldosari, B.; Al-Mansour, S.; Aldosari, H.; Alanazi, A. Assessment of factors influencing nurses acceptance of electronic medical record in a Saudi Arabia hospital. Informatics in Medicine Unlocked 2017, 10. [Google Scholar] [CrossRef]
- Yehualashet, D.E.; Seboka, B.T.; Tesfa, G.A.; Demeke, A.D.; Amede, E.S. Barriers to the Adoption of Electronic Medical Record System in Ethiopia: A Systematic Review. J Multidiscip Healthc 2021, 14, 2597–2603. [Google Scholar] [CrossRef]
- Samadbeik, M.; Fatehi, F.; Braunstein, M.; Barry, B.; Saremian, M.; Kalhor, F.; Edirippulige, S. Education and Training on Electronic Medical Records (EMRs) for health care professionals and students: A Scoping Review. Int J Med Inform 2020, 142, 104238. [Google Scholar] [CrossRef]
- Hamdan AB, M.R.; Mahmud, A. Challenges in the use Electronic Medical Records in Middle Eastern Countries: A Narrative Review. Malaysian Journal of Medicine and Health Sciences 2023, 19, 334–340. [Google Scholar] [CrossRef]
- Rule, A.; Chiang, M.F.; Hribar, M.R. Using electronic health record audit logs to study clinical activity: a systematic review of aims, measures, and methods. J Am Med Inform Assoc 2020, 27, 480–490. [Google Scholar] [CrossRef]
- Arndt, B.G.; Beasley, J.W.; Watkinson, M.D.; Temte, J.L.; Tuan, W.J.; Sinsky, C.A.; Gilchrist, V.J. Tethered to the EHR: Primary Care Physician Workload Assessment Using EHR Event Log Data and Time-Motion Observations. Ann Fam Med 2017, 15, 419–426. [Google Scholar] [CrossRef]
- del Mar Rodriguez, T.L.M.; O'Hara, K.; McKanna, T.M.D.; Decker, S. Implementing a New EMR. How Should We Train the Staff? Journal of PeriAnesthesia Nursing 2021, 36, e18–e19. [Google Scholar] [CrossRef]
- Bekele, T.A.; Gezie, L.D.; Willems, H.; Metzger, J.; Abere, B.; Seyoum, B.; Abraham, L.; Wendrad, N.; Meressa, S.; Desta, B.; et al. Barriers and facilitators of the electronic medical record adoption among healthcare providers in Addis Ababa, Ethiopia. Digit Health 2024, 10, 20552076241301946. [Google Scholar] [CrossRef] [PubMed]
- Sugiarto, P.; Purnami, C.; Jati, S. Supporting and Inhibiting Factors in Implementing Electronic Medical Records (EMR) Policy in Indonesia. BIO Web of Conferences 2024, 133, 00038. [Google Scholar] [CrossRef]
- Feryansyah, A.; Suprapto, S.; Wardani, R. Analysis of the Implementation of Electronic Medical Records in Community Health Centers. Indonesian Journal of Global Health Research 2025, 7, 919–930. [Google Scholar] [CrossRef]
- Gutiérrez, O.; Romero, G.; Pérez, L.; Salazar, A.; Charris, M.; Wightman, P. HealthyBlock: Blockchain-Based IT Architecture for Electronic Medical Records Resilient to Connectivity Failures. International Journal of Environmental Research and Public Health 2020, 17, 7132. [Google Scholar] [CrossRef]
- Avula, R. Addressing Barriers in Data Collection, Transmission, and Security to Optimize Data Availability in Healthcare Systems for Improved Clinical Decision-Making and Analytics. Applied Research in Artificial Intelligence and Cloud Computing 2021, 4, 78–93. [Google Scholar]
- Kessy, E.C.; Kibusi, S.M.; Ntwenya, J.E. Electronic medical record systems data use in decision-making and associated factors among health managers at public primary health facilities, Dodoma region: a cross-sectional analytical study. Front Digit Health 2023, 5, 1259268. [Google Scholar] [CrossRef]
- El Mahalli, A. Adoption and Barriers to Adoption of Electronic Health Records by Nurses in Three Governmental Hospitals in Eastern Province, Saudi Arabia. Perspect Health Inf Manag 2015, 12, 1f. [Google Scholar]
- Kiri, V.A.; Ojule, A.C. Electronic medical record systems: A pathway to sustainable public health insurance schemes in sub-Saharan Africa. Nigerian Postgraduate Medical Journal 2020, 27, 1–7. [Google Scholar] [CrossRef]
- Larsen, E.; Rao, A.; Sasangohar, F. Understanding the scope of downtime threats: A scoping review of downtime-focused literature and news media. Health Informatics Journal 2020, 26, 146045822091853. [Google Scholar] [CrossRef]
- Chen, J.; Li, Z.; Ma, W.; Tang, Y.; Liu, C.; Ma, S.; Xu, M.; Zhang, Q. Enhancing the timeliness of EMR documentation in resident doctors: the role of PDCA cycle management. BMC Medical Education 2024, 24, 1367. [Google Scholar] [CrossRef]
- Dutta, B.; Hwang, H.G. The adoption of electronic medical record by physicians: A PRISMA-compliant systematic review. Medicine (Baltimore) 2020, 99, e19290. [Google Scholar] [CrossRef] [PubMed]
- Mattingly, N.S. EVALUATION OF USER INTERFACE DESIGN IN ELECTRONIC MEDICAL RECORDS SOFTWARE FOR DIRECT PRIMARY CARE CLINICS; California State Polytechnic University: Pomona, 2022. [Google Scholar]
- Afzal, F.; Ahmad, A.; Ali, Q.; Joshi, S.; Mehra, S. Fulfilling the need of hour: Systematic review of challenges associated with electronic medical record (EMR) implementation-SBEA model. Vidyabharati International Interdisciplinary Research Journal 2021, 13, 649–662. [Google Scholar]
- Albagmi, S. The effectiveness of EMR implementation regarding reducing documentation errors and waiting time for patients in outpatient clinics: a systematic review. F1000Res 2021, 10, 514. [Google Scholar] [CrossRef] [PubMed]
- Li, E.; Clarke, J.; Ashrafian, H.; Darzi, A.; Neves, A.L. The impact of electronic health record interoperability on safety and quality of care in high-income countries: systematic review. Journal of medical Internet research 2022, 24, e38144. [Google Scholar] [CrossRef]
- Flynn, L. The benefits and challenges of multisite studies: lessons learned. AACN Adv Crit Care 2009, 20, 388–391. [Google Scholar] [CrossRef]
- Sedgwick, P. Multistage sampling. Bmj 2015, 351, h4155. [Google Scholar] [CrossRef]
- Anvari, F.; Efendić, E.; Olsen, J.; Arslan, R.C.; Elson, M.; Schneider, I.K. Bias in self-reports: An initial elevation phenomenon. Social Psychological and Personality Science 2023, 14, 727–737. [Google Scholar] [CrossRef]
- Taris, T.W.; Kessler, S.R.; Kelloway, E.K. Strategies addressing the limitations of cross-sectional designs in occupational health psychology: What they are good for (and what not). 2021, 35, 1–5. [Google Scholar] [CrossRef]
- De la Croix, A.; Barrett, A.; Stenfors, T. How todo research interviews in different ways. The clínical teacher 2018, 15, 451–456. [Google Scholar] [CrossRef]
- Redd, T.K.; Doberne, J.W.; Lattin, D.; Yackel, T.R.; Eriksson, C.O.; Mohan, V.; Gold, J.A.; Ash, J.S.; Chiang, M.F. Variability in Electronic Health Record Usage and Perceptions among Specialty vs. Primary Care Physicians. AMIA Annu Symp Proc 2015, 2015, 2053–2062. [Google Scholar]
Figure 1.
Conceptual framework.
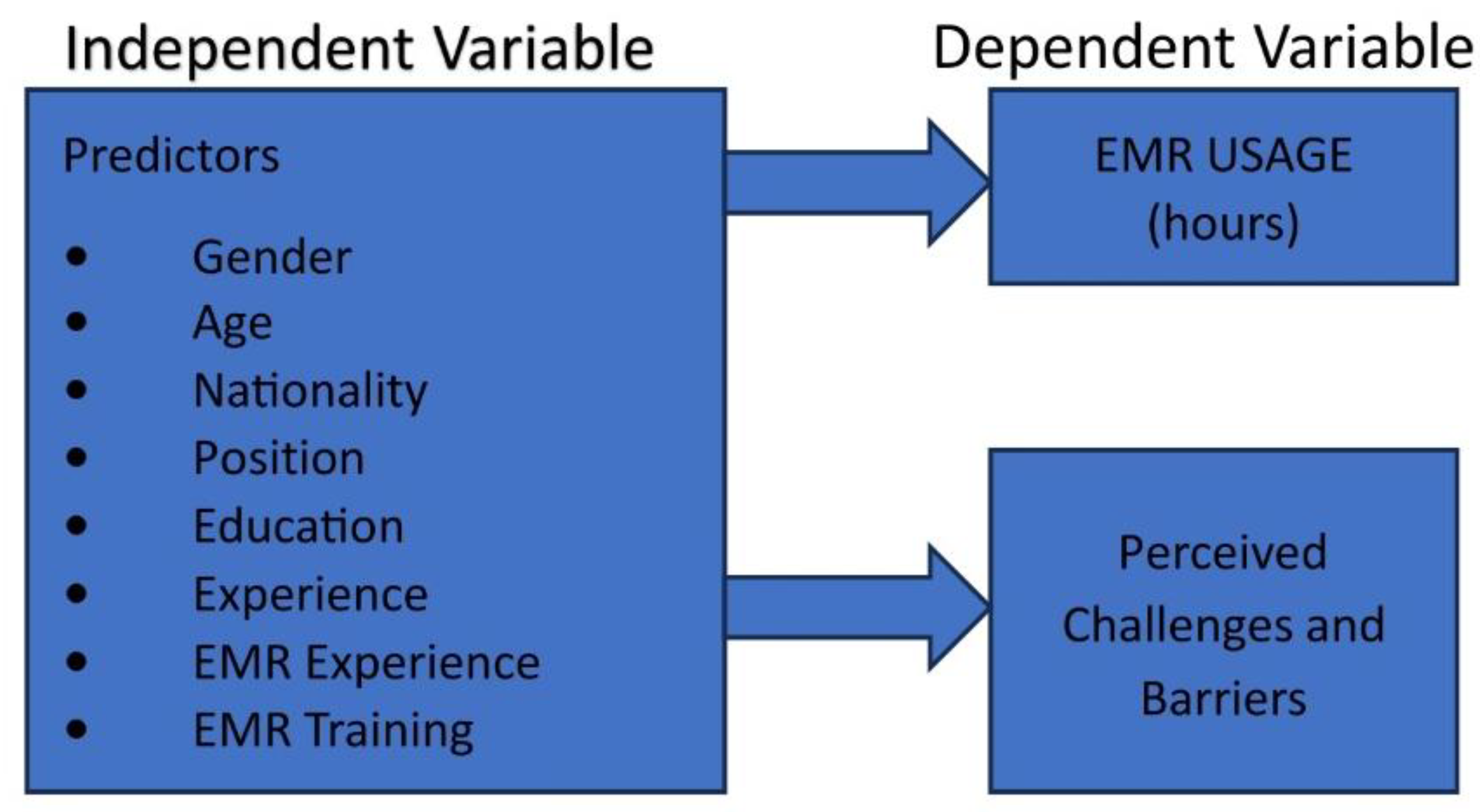
Figure 2.
Codes and themes identified for barriers and challenges related to EMR.
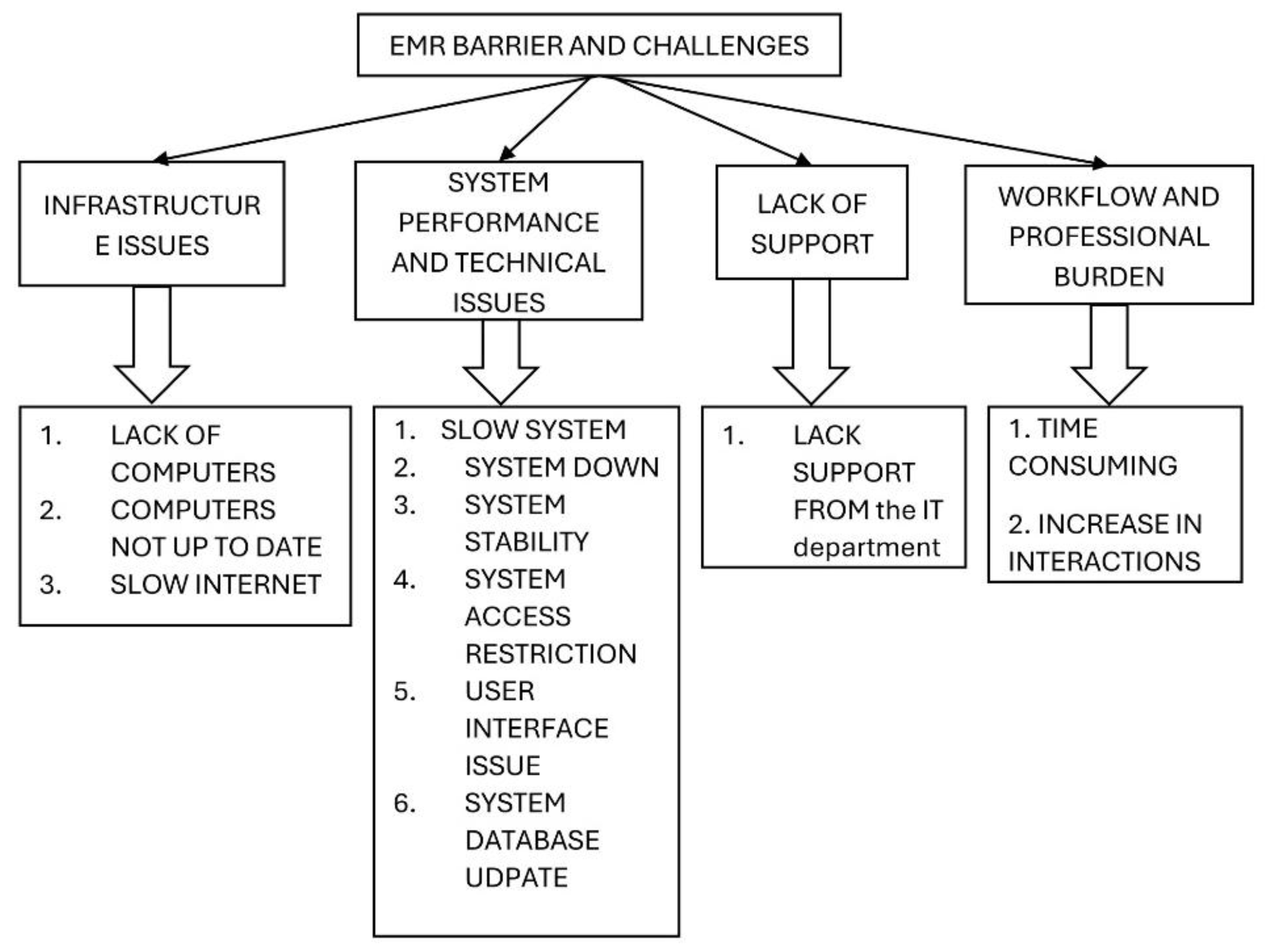
Figure 3.
Codes and themes identified for impact of EMR.
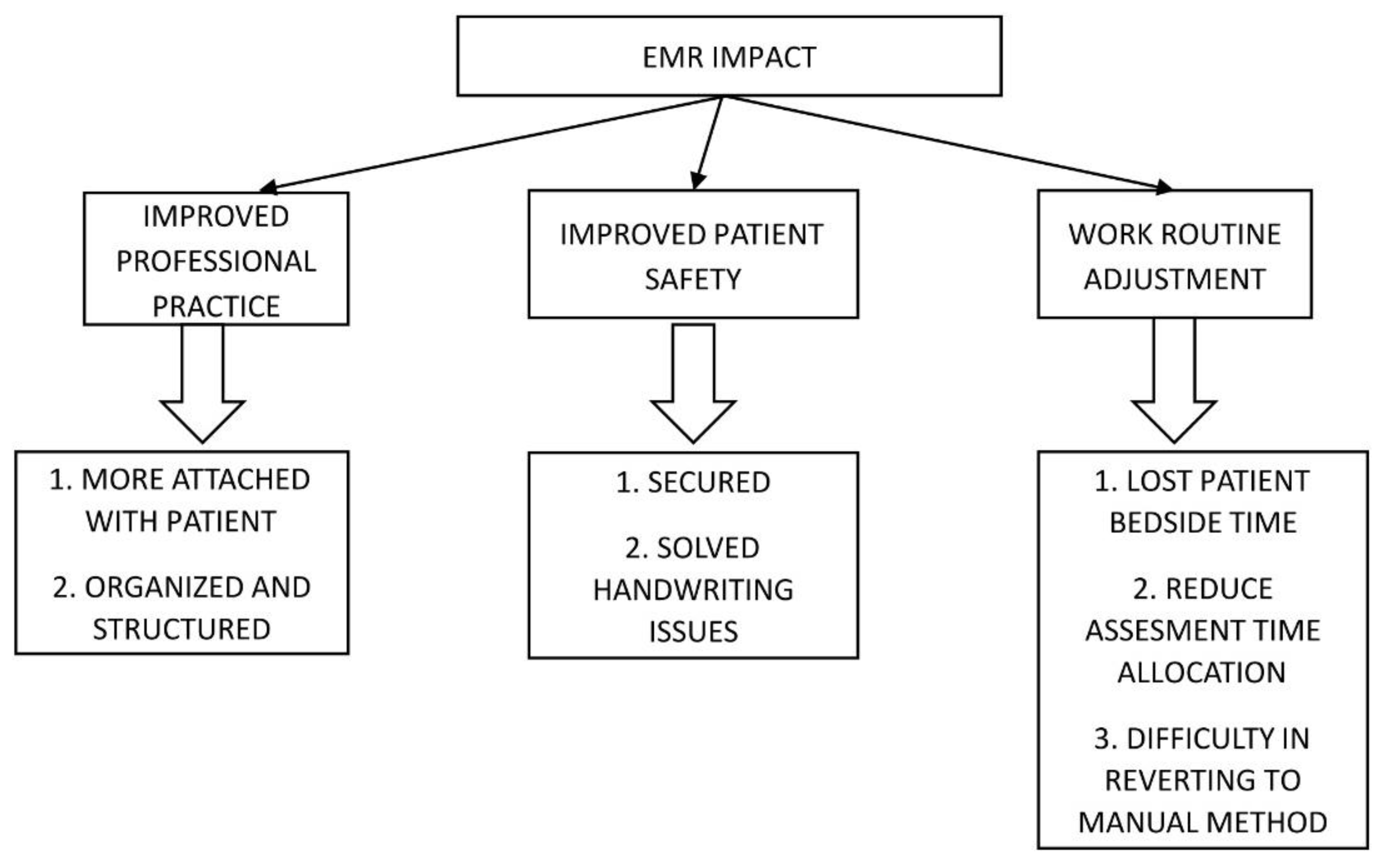

Table 1.
Deemographic characteristics of nurses and physicians (N=503).
|
Total participants (n=503) |
Physicians (n=162) |
Nurses (n=341) |
|||||
| Gender | Number | % | Number | % | Number | % | |
| Male | 165 | 32.8 | 93 | 57.4 | 72 | 21.1 | |
| Female | 338 | 67.2 | 69 | 42.6 | 269 | 78.9 | |
| Age (years) | |||||||
| Below 30 | 82 | 16.3 | 40 | 24.7 | 42 | 12.3 | |
| 30 to below 40 | 226 | 44.9 | 59 | 36.4 | 167 | 49 | |
| 40 to below 50 | 122 | 24.3 | 48 | 29.6 | 74 | 21.7 | |
| 50 and above | 73 | 14.5 | 15 | 9.3 | 58 | 17 | |
| Nationality | |||||||
| Saudi | 191 | 38 | 117 | 72.2 | 74 | 21.7 | |
| Non-Saudi | 312 | 62 | 45 | 27.8 | 267 | 78.3 | |
| Position of physicians | |||||||
| Intern | 4 | 0.8 | 4 | 2.5 | - | - | |
| Resident | 69 | 13.7 | 69 | 42.6 | - | - | |
| Fellow | 10 | 2 | 10 | 6.2 | - | - | |
| Specialist | 36 | 7.2 | 36 | 22.2 | - | - | |
| Consultant | 38 | 7.6 | 38 | 23.5 | - | - | |
| General Practitioner | 5 | 1 | 5 | 3.1 | - | - | |
| Primary specialty for physicians | |||||||
| Anaesthesia | 7 | 1.4 | 7 | 4.3 | - | - | |
| Cardiology | 4 | 0.8 | 4 | 2.5 | - | - | |
| Emergency medicine | 5 | 1 | 5 | 3.1 | - | - | |
| Family medicine | 21 | 4.2 | 21 | 13 | - | - | |
| General practitioner | 5 | 1 | 5 | 3.1 | - | - | |
| Intensivist | 4 | 0.8 | 4 | 2.5 | - | - | |
| Internal medicine | 20 | 4 | 20 | 12.3 | - | - | |
| Neurosurgery | 8 | 1.6 | 8 | 4.9 | - | - | |
| OB/Gynaecology | 13 | 2.6 | 13 | 8 | - | - | |
| Ophthalmology | 3 | 0.6 | 3 | 1.9 | - | - | |
| Orthopaedic | 11 | 2.2 | 11 | 6.8 | - | - | |
| Paediatric | 44 | 8.7 | 44 | 27.2 | - | - | |
| Surgery | 17 | 3.4 | 17 | 10.5 | - | - | |
| Position of nurses | |||||||
| Clinical nurse specialist | 82 | 16.3 | - | - | 82 | 24 | |
|
Front line (Direct patient care provider) |
209 | 41.6 | - | - | 209 | 61.3 | |
| Nurse manager/supervisor | 50 | 9.9 | - | - | 50 | 14.7 | |
| Work setting for nurses | |||||||
| Hospital (inpatient) | 159 | 31.6 | - | - | 159 | 46.6 | |
| Hospital (outpatient) | 43 | 8.5 | - | - | 43 | 12.6 | |
| Emergency room (ER) | 35 | 7 | - | - | 35 | 10.3 | |
| Intensive Care Unit (ICU) | 98 | 19.5 | - | - | 98 | 28.7 | |
| Transitional Care Unit (TCU) | 1 | 0.2 | - | - | 1 | 0.3 | |
| Surgical/Operating Room | 29 | 5.8 | - | - | 29 | 8.5 | |
| Primary Healthcare centre | 14 | 2.8 | - | - | 14 | 4.1 | |
| Nursing admin | 9 | 1.8 | - | - | 9 | 2.6 | |
| Burn unit | 1 | 0.2 | - | - | 1 | 0.3 | |
| Neonatal Intensive Care Unit (NICU) | 1 | 0.2 | - | - | 1 | 0.3 | |
| Burn Care Unit (BCU) | 1 | 0.2 | - | - | 1 | 0.3 | |
| Highest level of education certificate in profession | |||||||
| Diploma | 46 | 9.1 | 3 | 1.9 | 43 | 12.6 | |
| Bachelor’s degree | 327 | 65 | 73 | 45.1 | 254 | 74.5 | |
| Master’s degree | 83 | 16.5 | 43 | 26.5 | 40 | 11.7 | |
| Doctorate (PhD or equivalent) | 47 | 9.3 | 43 | 26.5 | 4 | 1.2 | |
| Years of experience in healthcare | |||||||
| Less than 1 year | 16 | 3.2 | 5 | 3.1 | 11 | 3.2 | |
| 1 to less than 5 years | 86 | 17.1 | 53 | 32.7 | 33 | 9.7 | |
| 5 to less than 10 years | 109 | 21.7 | 34 | 21 | 75 | 22 | |
| 10 to less than 20 years | 181 | 36 | 35 | 21.6 | 146 | 42.8 | |
| 20 years and above | 111 | 22.1 | 35 | 21.6 | 76 | 22.3 | |
| Years of experience in healthcare setting utilizing EMR | |||||||
| Less than 1 year | 30 | 6 | 11 | 6.8 | 19 | 5.6 | |
| 1 to less than 5 years | 200 | 39.8 | 80 | 49.4 | 120 | 35.2 | |
| 5 to less than 10 years | 142 | 28.2 | 34 | 21 | 108 | 31.7 | |
| 10 to less than 20 years | 107 | 21.3 | 32 | 19.8 | 75 | 22 | |
| 20 years and above | 24 | 4.8 | 5 | 3.1 | 19 | 5.6 | |
| Region of work | |||||||
| Riyadh | 252 | 50.1 | 101 | 62.3 | 151 | 44.3 | |
| Makkah | 132 | 26.2 | 31 | 19.1 | 101 | 29.6 | |
| Dammam | 119 | 23.7 | 30 | 18.5 | 89 | 26.1 | |
Table 2.
Average number of hours of EMR use among physicians and nurses (N=503).
| Question | Total Participant | Physicians | Nurses | |||
| On average, how many hours per Shift/day do you spend using the EMR system? | Number | % | Number | % | Number | % |
| Less than 1 hour | 17 | 3.4 | 4 | 2.5 | 13 | 3.8 |
| 1 - 2 hours | 49 | 9.7 | 23 | 14.2 | 26 | 7.6 |
| 3 - 4 hours | 125 | 24.9 | 61 | 37.7 | 64 | 18.8 |
| 5 – 6 hours | 98 | 19.5 | 43 | 26.5 | 55 | 16.1 |
| More than 6 hours | 214 | 42.5 | 31 | 19.1 | 183 | 53.7 |
| What specific tasks do you use the EMR system for? | ||||||
| Reviewing test results | 372 | 74 | 142 | 87.7 | 230 | 67.4 |
| Documenting patient histories | 348 | 69.2 | 140 | 86.4 | 208 | 61 |
| Patient admission | 319 | 63.4 | 105 | 64.8 | 214 | 62.8 |
| Updating progress notes | 305 | 60.6 | 144 | 88.9 | 161 | 47.2 |
| Nursing notes | 305 | 60.6 | 7 | 4.3 | 298 | 87.4 |
| Nursing initial assessment | 288 | 57.3 | 8 | 4.9 | 280 | 82.1 |
| Discharge process | 285 | 56.7 | 100 | 61.7 | 185 | 54.3 |
| Writing reports | 272 | 54.1 | 114 | 70.4 | 158 | 46.3 |
| Updating treatment plans | 244 | 48.5 | 130 | 80.2 | 114 | 33.4 |
| Communication with other healthcare providers “Request/consultation” | 231 | 45.9 | 118 | 72.8 | 113 | 33.1 |
| Nursing care plan | 228 | 45.3 | 4 | 2.5 | 224 | 65.7 |
| Entering diagnostic data | 203 | 40.4 | 120 | 74.1 | 83 | 24.3 |
| Prescribing medications | 197 | 39.2 | 144 | 88.9 | 53 | 15.5 |
| Other | 19 | 3.8 | 3 | 1.9 | 16 | 4.7 |
| Have you received formal training in using the EMR system? | ||||||
| No | 65 | 12.9 | 34 | 21 | 31 | 9.1 |
| Yes | 438 | 87.1 | 128 | 79 | 310 | 90.9 |
| How many hours of EMR training have you received? | ||||||
| Zero | 65 | 12.9 | 30 | 18.5 | 35 | 10.3 |
| Less than 5 hours | 246 | 48.9 | 88 | 54.3 | 158 | 46.3 |
| 5 - 10 hours | 126 | 25 | 33 | 20.4 | 93 | 27.3 |
| More than 10 hours | 66 | 13.1 | 11 | 6.8 | 55 | 16.1 |
| What are the primary challenges you face when using the EMR system? | ||||||
| Lack of adequate training | 141 | 28 | 73 | 45.1 | 68 | 19.9 |
| Slow system performance | 239 | 47.5 | 64 | 39.5 | 175 | 51.3 |
| System crashes or errors | 169 | 33.6 | 66 | 40.7 | 103 | 30.2 |
| Difficulty navigating the system | 122 | 24.3 | 61 | 37.7 | 61 | 17.9 |
| Time-consuming data entry | 258 | 51.3 | 110 | 67.9 | 148 | 43.4 |
| Lack of user-friendly interface | 123 | 24.5 | 51 | 31.5 | 72 | 21.1 |
| Disrupts workflow | 143 | 28.4 | 54 | 33.3 | 89 | 26.1 |
| Difficulty in communication with other healthcare providers via the EMR | 110 | 21.9 | 44 | 27.2 | 66 | 19.4 |
| Lack of adequate technical support | 157 | 31.2 | 54 | 33.3 | 103 | 30.2 |
| Other | 16 | 3.2 | 5 | 3.1 | 11 | 3.2 |
Table 3.
Total hours per day of EMR use among physicians and nurses.
| ALL | Nurse | Physician | |||||
| Time Category (hour) | Approx. Midpoint (hours /day) | Number | Total hours/day | Number | Total hours/day | Number | Total hours/day |
| <1 | 0.5 | 17 | 8.5 | 13 | 6.5 | 4 | 2 |
| 1–2 | 1.5 | 49 | 73.5 | 26 | 39 | 23 | 34.5 |
| 3–4 | 3.5 | 125 | 437.5 | 64 | 224 | 61 | 213.5 |
| 5–6 | 5.5 | 98 | 539 | 55 | 302 | 43 | 236.5 |
| >6 | 7 | 214 | 1498 | 183 | 1281 | 31 | 217 |
Table 4.
Mean of monthly hours of EMR used for physicians and nurses and its percentages out of total monthly working hours.
Table 4.
Mean of monthly hours of EMR used for physicians and nurses and its percentages out of total monthly working hours.
| Position | Work Hours per Day | Work days per Week | Total Work Hours per month | Mean of EMR usage hours per day | Total of EMR usage hours per month | % of EMR usage per month out of the total monthly working hours | P-value |
| Nurses | 12 | 4 | 208 | 5.43 ± 2.03 | 86.80 | 41.73 | 0.001 * |
| Physicians | 12 | 4 | 208 | 4.34 ± 1.87 | 69.44 | 33.38 |
* Significant p value. P value was calculated for mean of EMR usage per day between nurses and physician.
Table 5.
Predictors of extended hours of use in relation to demographic characteristics by using ordinal logistic regression.
Table 5.
Predictors of extended hours of use in relation to demographic characteristics by using ordinal logistic regression.
| Odds Ratio | 95 % CI | P-value | |||
| Lower | Upper | ||||
| Gender | Male | Reference Group | |||
| Female | 3.08 | 2.17 | 4.36 | 0.001* | |
| Age | Below 30 | Reference Group | |||
| 30-40 | 1.94 | 0.89 | 2.78 | 0.005* | |
| 40-50 | 1.81 | 1.09 | 3.04 | 0.022* | |
| 50 above | 1.57 | 1.23 | 3.07 | 0.118 | |
| Nationality | Saudi | Reference Group | |||
| Non-Saudi | 2.92 | 2.09 | 1.41 | 0.001* | |
| Position | Physician | Reference Group | |||
| Nurse | 2.98 | 2.12 | 4.20 | 0.001* | |
| Education | Diploma | Reference Group | |||
| Bachelor | 0.69 | 0.39 | 1.27 | 0.241 | |
| Master | 0.50 | 0.25 | 0.99 | 0.047* | |
| Doctorate | 0.28 | 0.14 | 0.61 | 0.001* | |
| Experience | < 1 year | Reference Group | |||
| 1-5 year | 2.66 | 0.99 | 7.19 | 0.053 | |
| 5-10 year | 5.05 | 1.88 | 13.55 | 0.001* | |
| 10-20 year | 5.23 | 1.99 | 13.76 | 0.001* | |
| 20+ year | 4.15 | 1.55 | 11.15 | 0.005* | |
| EMR Experience | < 1 year | Reference Group | |||
| 1-5 year | 1.32 | 0.66 | 2.69 | 0.429 | |
| 5-10 year | 2.13 | 1.03 | 4.41 | 0.041* | |
| 10-20 year | 2.08 | 0.99 | 4.41 | 0.055 | |
| 20+ year | 2.30 | 0.85 | 6.26 | 0.101 | |
| EMR Training | 0 | Reference Group | |||
| < 5 hours | 1.00 | 0.62 | 1.65 | 0.978 | |
| 5-10 hours | 1.55 | 0.92 | 2.76 | 0.095 | |
| 10+ hours | 2.33 | 1.22 | 4.47 | 0.010* | |
| Region | Riyadh | Reference Group | |||
| Makkah | 1.54 | 1.05 | 2.26 | 0.026* | |
| Dammam | 1.08 | 0.72 | 1.64 | 0.690 | |
* Significant p value.
Table 6.
Mean score of perceived challenges and barriers facing physicians & nurses when using the EMR system.
Table 6.
Mean score of perceived challenges and barriers facing physicians & nurses when using the EMR system.
|
Number (%) |
Number (%) |
Number (%) |
Number (%) |
Number (%) |
Mean ± SD | Mean ± SD | Mean ± SD | ||
| 1. I received adequate training in using EMR | 53 (10.5) | 54 (10.7) | 146 (29) | 174 (34.6) | 76 (15.1) | 3.33 ± 1.17 | 3.04 ± 1.21 | 3.47 ± 1.13 | < 0.001* |
| 2. I always receive immediate support when facing technical issues with the EMR system | 49 (9.7) | 72 (14.3) | 175(34.8) | 152 (30.2) | 55 (10.9) | 3.18 ± 1.11 | 3.01 ± 1.15 | 3.26 ± 1.09 | 0.018* |
| 3. In my opinion, EMR documentation has significantly increased the quality of patient care | 35 (7) | 19 (3.8) | 137(27.2) | 185 (36.8) | 127(25.2) | 3.70 ± 1.1 | 3.91 ± 1.01 | 3.6 ± 1.13 | 0.003* |
| 4. EMR documentation affects my ability to interact with patients directly | 42 (8.3) | 108(21.5) | 157(31.2) | 137 (27.2) | 59 (11.7) | 2.87 ± 1.13 | 2.77 ± 1.23 | 2.92 ± 1.08 | 0.158 |
| 5. Performing tasks on the EMR takes more time compared to direct patient care | 42 (8.3) | 85 (16.9) | 159(31.6) | 131 (26) | 86 (17.1) | 2.73 ± 1.17 | 2.48 ± 1.22 | 2.85 ± 1.13 | 0.001* |
| 6. Utilizing the EMR system for performing tasks has enhanced my job satisfaction | 32 (6.4) | 44 (8.7) | 177(35.2) | 181 (36) | 69 (13.7) | 3.42 ± 1.04 | 3.44 ± 1.05 | 3.41 ± 1.04 | 0.780 |
| 7. I believe that my age affects my ability in using the EMR system | 156 (31) | 152(30.2) | 112(22.3) | 62 (12.3) | 21 (4.2) | 3.72 ± 1.15 | 3.62 ± 1.26 | 3.76 ± 1.1 | 0.186 |
| 8. I believe that my years of experience affect my ability in using the EMR system | 100(19.9) | 156 (31) | 103(20.5) | 98 (19.5) | 46 (9.1) | 3.33 ± 1.25 | 3.09 ± 1.29 | 3.44 ± 1.22 | 0.003* |
| 9. My working position (title) influences the time spent on EMR system (e.g., junior, senior, intern) | 80 (15.9) | 137(27.2) | 125(24.9) | 112 (22.3) | 49 (9.7) | 3.17 ± 1.22 | 2.69 ± 1.3 | 3.4 ± 1.11 | 0.001* |
| 10. My health care setting affects the time spent on EMR system | 52 (10.3) | 100(19.9) | 169(33.6) | 133 (26.4) | 49 (9.7) | 2.95 ± 1.13 | 2.61 ± 1.05 | 3.11 ± 1.13 | 0.001* |
| 11. The time spent using EMR system has a positive impact on my job satisfaction | 36 (7.2) | 70 (13.9) | 166 (33) | 168 (33.4) | 63 (12.5) | 3.30 ± 1.08 | 3.3 ± 1.13 | 3.3 ± 1.06 | 0.933 |
| * Significant p value | |||||||||
| Likert scale with 5 points ; where is 1 strongly disagree, 2 disagree ,3 neutral ,4 agree and 5 strongly agree | |||||||||
Table 7.
Multiple linear regression analysis to assess the predictors factors of perceived challenges and barriers toward EMR use among healthcare professionals.
Table 7.
Multiple linear regression analysis to assess the predictors factors of perceived challenges and barriers toward EMR use among healthcare professionals.
| Predictor | β | t | P value |
| Gender | 0.008 | 0.174 | 0.862 |
| Age | 0.054 | 0.788 | 0.431 |
| Nationality | 0.075 | 1.259 | 0.209 |
| Position | 0.163 | 2.877 | 0.004* |
| Education level | 0.038 | 0.744 | 0.457 |
| Years in healthcare | 0.012 | 0.146 | 0.884 |
| EMR experience | –0.033 | –0.621 | 0.535 |
| Work region | –0.110 | –2.401 | 0.017* |
| Hours of EMR training | 0.173 | 3.826 | <0.001* |
|
R² = 0.118, F=7.298, p < 0.001 * Significant p value |
|||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



