Submitted:
09 December 2025
Posted:
09 December 2025
You are already at the latest version
Abstract
Background: While Behavioral Activation (BA) is a validated and widely used treatment for depression, a subset of cases exhibits a paradoxical failure: patients demonstrate insight, express motivation, and engage in therapy but fail to initiate any behavioral change. Existing behavioral and cognitive models offer limited structural explanations for such ignition failure. Objective: This paper applies Cognitive Drive Architecture (CDA), an emerging structural field grounded in Lagunian Dynamics and governed by Lagun’s Law of Primode and Flexion Dynamics, to reinterpret a well-documented BA treatment failure. The goal is not to critique BA but to examine whether ignition failure may reflect deeper architectural misalignment rather than motivational deficit. Method: Using secondary analysis, the clinical case of “Karen” (Hopko et al., 2011) is reinterpreted through the CDA framework. Six structural variables (Primode, CAP, Flexion, Anchory, Grain, and Slip) were mapped to observed behaviors, therapeutic responses, and contextual factors. Latent Task Architecture (LTA), a domain-specific extension of Lagunian Dynamics, is used to model task readiness and resistance layering. Results: Karen’s persistent non-initiation is structurally explained by a configuration of near-zero Primode, low CAP, poor Flexion, weak Anchory, high Grain, and minimal Slip. This Drive profile mathematically predicts near-zero behavioral output despite motivation or understanding, resolving the paradox without pathologizing the patient. Conclusion: CDA reframes treatment nonresponse not as resistance or noncompliance, but as a predictable structural outcome under specific internal configurations. This suggests a future direction in which therapeutic approaches are selected based on drive architecture assessment rather than symptom profiles alone. Implications for pre-intervention calibration, clinical modeling, and the structural classification of treatment resistance are discussed.
Keywords:
behavioral activation
; cognitive drive architecture
; depression
; primode
; treatment resistance
; motivational paradox
1. Introduction
1.1. The Clinical Paradox of Karen
Behavioral Activation (BA) is widely recognized as an empirically supported treatment for depression, grounded in decades of behavioral theory and validated across numerous randomized controlled trials (Lewinsohn, 1974; Jacobson et al., 1996; Dimidjian et al., 2006). The central tenet of BA is that re-engaging in meaningful behavior can disrupt avoidance cycles and produce downstream improvements in affect (Martell et al., 2001). In most cases, this model is clinically and theoretically effective. Yet, a small subset of patients presents a striking paradox: individuals who understand the intervention, express motivation for change, and actively participate in therapy but remain unable to initiate even the smallest behavioral actions outside of session.
The case of Karen, documented by Hopko, Magidson, and Lejuez (2011), exemplifies this clinical dilemma. Over twelve sessions of BA, Karen demonstrated insight into her behavioral patterns, agreed with the rationale for activation, and verbally committed to change. Despite this alignment of cognition, affect, and therapeutic engagement, she failed to complete activity monitoring, initiate scheduled behaviors, or exhibit any measurable activation in her daily life. Hopko and colleagues offered a thoughtful case analysis, identifying factors such as medical burden, diminished reinforcement, and motivational difficulty. However, the stark contradiction of clarity plus willingness plus therapeutic adherence, followed by complete non-initiation, remains conceptually unresolved.
This is more than a clinical anomaly. Karen’s case highlights a deeper theoretical blind spot: traditional behavioral models can explain why patients stop doing things, but not why they never start, especially when they want to. This raises a structural question: what internal architecture governs the transition from intention to action, and why might that structure fail despite motivation, understanding, and treatment fidelity?
1.2. Limitations of Existing Behavioral and Cognitive Models
The aim of this paper is not to critique Behavioral Activation or the clinicians involved, whose application of the model was comprehensive within the scope of existing theory, but to explore why activation failure occurs in some patients despite seemingly optimal therapeutic conditions.
Several explanatory gaps emerge when reinterpreting Karen’s case through classical and contemporary frameworks:
-
Behavioral models explain avoidance but not ignition failure.Foundational theories of depression, such as those by Ferster (1973) and Lewinsohn (1974), highlight how avoidance behaviors are maintained by the absence of reinforcing experiences. These models explain behavioral persistence but offer little insight into why action never initiates, even when reinforcement is anticipated and values are identified.
-
Reinforcement theory accounts for maintenance, not structural inertia.Karen’s environment lacked strong sources of reinforcement, as Hopko et al. (2011) observed. Yet the theory assumes that behavior begins and then extinguishes when reinforcement is insufficient. It does not explain why behavior fails to initiate in the first place, even when the task is small and the stakes are understood.
-
Cognitive models do not explain the action gap.Karen demonstrated insight into her depressive cycle and agreed with the logic of BA. Cognitive theories, such as Beck’s model or later appraisal frameworks, can explain rumination and negative schema but lack a mechanistic model for how understanding fails to convert into action. Insight is assumed to support change, but this assumption is not always borne out in practice.
-
Comorbidity increases friction but lacks structural specificity.Karen’s breast cancer and caregiving demands clearly increased her distress and emotional load. These contextual burdens may raise the “cost” of behavior, but they do not fully account for complete behavioral paralysis across all tasks and time points, especially when Karen remained engaged and verbally committed.
-
Emerging models address effort but remain partial.Recent frameworks in motivation science, such as Motivational Intensity Theory (Brehm & Self, 1989), the Behavioral Inhibition System (BIS) theory (Gray & McNaughton, 2000), and Reward Prediction Error (RPE) models (Montague et al., 1996; Huys et al., 2015), offer insights into how effort, salience, and action tendencies are modulated. However, they typically focus on value prediction, response inhibition, or cost–benefit analysis and lack a multivariable structure for explaining why effort fails to emerge even when the behavior is internally valued and externally supported.
Taken together, these gaps suggest that existing theories can describe the context and experience of activation failure, but not its architecture. Karen’s case represents a scenario where all necessary ingredients (desire, insight, therapist support) are present, yet no behavioral output occurs. This signals a failure not of motivation, but of structure.
1.3. Structural Framework: Cognitive Drive Architecture (CDA)
To address this paradox, we apply Cognitive Drive Architecture (CDA), a field-level framework developed to model the internal structure of behavioral drive. CDA is not introduced here for the first time; it was formally proposed in earlier work (Lagun, 2025b) as a field of study distinct from behavioral or cognitive theory. CDA is grounded in Lagunian Dynamics, a theoretical system that defines how internal variables interact to support or block initiation, and is governed by Lagun’s Law, a formal equation that models the dynamics between Primode (ignition potential) and Flexion (task–self alignment).
CDA proposes that Drive is not produced directly by motivation or reinforcement but is an emergent property of six interacting variables:
- Primode: Governs whether task initiation is structurally possible
- CAP (Cognitive Activation Potential): Reflects available volitional energy
- Flexion: Measures the internal compatibility between the task and the self
- Anchory: Supports attentional tethering and sustained focus
- Grain: Captures internal resistance or friction (e.g., emotional drag, shame, cognitive dissonance)
- Slip: Models behavioral variability or execution instability
These variables are grouped into three domains:
- Ignition (Primode, CAP)
- Tension (Flexion, Anchory, Grain)
- Flux (Slip)
The organization of these six variables into the three domains of Ignition, Tension, and Flux is shown in Figure 1.
In this system, drive emerges only when all variables align within viable thresholds. Even one extreme value, such as a suppressed Primode or high Grain, can produce complete behavioral collapse, despite the presence of motivation, reinforcement, or insight.
Karen’s case fits this architecture. Her Primode was likely near-zero, meaning that task ignition was structurally blocked. High Grain may have created intense friction, while low CAP and weak Anchory prevented even minimal task adherence. Within CDA, this is not seen as avoidance but as mechanical failure.
Latent Task Architecture (LTA) (Lagun, 2025c) extends CDA by modeling how unresolved internal demands compress readiness. In contexts of chronic illness, caregiving, or psychological overload, LTA models the residual task weight that prevents activation even when the task is small. It explains how “low-cost” behaviors can still exceed internal structural capacity.
1.4. Purpose and Contribution of This Paper
This paper reinterprets Karen’s case not to challenge the efficacy of Behavioral Activation, but to show that it operates within limits defined by internal structural readiness. BA’s tools are effective when drive systems are responsive. When they are structurally impaired, additional models may be needed to diagnose and intervene.
Specifically, this paper will:
- Reconstruct Karen’s Drive configuration using CDA and LTA
- Explain behavioral non-initiation as a structural misalignment rather than a motivational deficit
- Illustrate how variables like suppressed Primode, high Grain, and weak Anchory generate mechanical paralysis
- Offer a generalizable model for similar BA nonresponse cases, especially in high-load clinical populations
By framing treatment resistance as a configuration issue, not a failure of will, CDA opens new directions for theory, assessment, and intervention. In this framing, Karen is not an exception to BA but a structural boundary case that shows where activation-based models reach their limit.
2. Method: Secondary Case Selection Approach
2.1. Case Source
This study presents a structural reinterpretation of the case of “Karen” as originally described by Hopko, Magidson, and Lejuez (2011). The case documents the course of Behavioral Activation (BA) treatment for a woman diagnosed with recurrent Major Depressive Disorder, compounded by significant medical and caregiving burden. The case was selected for its theoretical significance: it offers a clear example of treatment nonresponse within an evidence-based behavioral framework, despite apparent insight, motivation, and therapeutic engagement.
The original authors provided detailed process notes and a transparent clinical narrative, which enables reanalysis through Cognitive Drive Architecture (CDA). At the time of its publication, CDA and its parent theory, Lagunian Dynamics, were not yet available as explanatory frameworks. This analysis uses their structural lens to examine how behavioral non-initiation may emerge from internal configuration, rather than from a deficit of motivation or therapeutic alignment.
2.2. Inclusion Criteria for Case Selection
This case was selected based on four a priori criteria, chosen to ensure its suitability for CDA-based structural analysis:
- Motivational paradox: The patient demonstrated insight into BA principles, verbalized desire for behavioral change, and participated consistently in sessions, yet failed to initiate any behavioral tasks over a 12-session course. This paradox is a hallmark indicator of potential ignition failure within the CDA framework.
- High-resolution process documentation: The original case report includes session-by-session descriptions of values clarification, behavioral task planning, psychoeducation delivery, and client–therapist interaction. This granularity enables reliable mapping of CDA variables to real clinical moments.
- Explicit recognition of treatment nonresponse: Hopko et al. (2011) openly acknowledged that the patient’s inactivity was difficult to reconcile with standard behavioral models. Their transparency makes the case ideal for reanalysis via an alternative structure-oriented lens.
- Contextual complexity and load: The patient faced multifactorial adversity, including a breast cancer diagnosis, caregiving responsibilities, and reduced social-emotional reinforcement. These conditions are ideal for the application of Latent Task Architecture (LTA), a domain-specific extension of CDA that models how load and internal friction compound to suppress behavioral readiness (Lagun, 2025c).
Together, these features make the Karen case a structurally coherent subject for reinterpretation under Lagun’s Law and the six-variable Drive model (Lagun, 2025a; 2025b).
2.3. Data Extraction and Mapping Procedure
All material used in this reinterpretation was extracted directly from the published case report. No speculative inferences were made. To maintain fidelity to the original account and to align with CDA’s modeling requirements, we categorized extracted data into four domains corresponding to key indicators of Drive dynamics:
- Behavioral Observations: Patterns of withdrawal, inactivity, sleep regulation, and instances of attempted activation.
- Values Exploration: Patient statements during values exercises, including role identity narrowing and difficulty articulating self-relevant goals beyond caregiving.
- Compliance and Activation: Completion of tasks, homework adherence, initiation of scheduled behaviors, and therapeutic documentation of missed or incomplete assignments.
- Treatment Engagement: The patient’s expressed understanding of BA concepts, responses to psychoeducation, and affective resonance with intervention logic.
No additional data beyond what was publicly reported were used. Table 1 summarizes the extracted elements across these domains and their relevance for CDA-based reinterpretation.
2.4. Ethical Compliance
This manuscript presents a secondary theoretical analysis of a clinical case that has already been published in a peer-reviewed academic source. No new clinical data were collected, and no direct or indirect contact with the patient occurred. All interpretations were made using publicly available information, and no identifying details beyond what was reported in the original article are included.
As such, this study does not constitute human-subjects research under current ethical guidelines and does not require institutional review board approval. The intent of this work is to offer a complementary structural lens through which to understand an already-documented case of treatment nonresponse, with full respect for the original clinicians and the complexity of the case.
3. Summary of the Original Case
3.1. Patient Background
The patient, referred to as Karen in the original case study by Hopko, Magidson, and Lejuez (2011), was a 54-year-old woman presenting with complex psychosocial and medical challenges. She lived with her chronically ill husband, for whom she served as the primary caregiver, and an adult daughter who provided minimal emotional or logistical support. Karen’s home environment was described as low in positive reinforcement, particularly given her husband’s emotional withdrawal and limited capacity to support her therapeutic efforts.
Concurrently, Karen had recently received a diagnosis of breast cancer, adding physical fatigue, pain, and uncertainty to her daily experience. This medical burden, combined with long-standing caregiving responsibilities, created a context of high functional load, conditions now modeled structurally within Latent Task Architecture (LTA) as compressive to drive ignition and behavioral readiness. These factors framed the onset and persistence of her depressive symptoms and significantly shaped her response to treatment.
3.2. Psychiatric Presentation
Karen met the criteria for Major Depressive Disorder, Recurrent, and presented with a classical but severe symptom profile: low mood, anhedonia, feelings of hopelessness, diminished motivation, and cognitive fatigue. Her behavior was marked by near-total withdrawal from daily activity. She reported long periods of sleep, minimal social contact, and decreased involvement in both personal and household tasks. This pattern had persisted across multiple depressive episodes over her adult life.
Her clinical profile reflected profound functional impairment, with both internal psychological mechanisms and external contextual demands reinforcing the depressive cycle. At intake, she expressed insight into her condition and demonstrated verbal openness to treatment.
3.3. Behavioral Activation Protocol: Components and Implementation
Karen was treated using a standard Behavioral Activation (BA) protocol, consistent with widely accepted models and manuals (e.g., Martell et al., 2001). The treatment unfolded over twelve sessions and included the following core components:
- Psychoeducation: Karen was introduced to the foundational principles of BA, namely, the role of avoidance in sustaining depression and the premise that behavioral engagement precedes mood improvement.
- Activity Monitoring: She was asked to log daily behaviors and emotional states, with the goal of identifying avoidance patterns and opportunities for behavioral reinforcement.
- Functional Analysis: Sessions explored the antecedents and consequences of specific behaviors, seeking to uncover how inaction or avoidance was being maintained in her routine.
- Values Clarification: The therapist facilitated reflection on life domains that Karen found meaningful, using these values as anchors for later behavioral planning.
- Activity Scheduling: Together, the therapist and patient designed simple, values-aligned behavioral tasks to be implemented between sessions.
- Reinforcement Shaping: The therapist attempted to involve Karen’s husband in encouraging activation by positively reinforcing her efforts and engagement.
While the BA protocol was delivered with fidelity, Karen’s functional engagement with it remained minimal. The sequence of intervention, from psychoeducation through reinforcement, was followed as designed, but breakdowns occurred repeatedly at the ignition point: activity monitoring was incomplete, scheduled tasks were not attempted, and no behavioral shift was observed, as illustrated in Figure 2.
3.4. Documented Process Challenges
Despite participating in all sessions and expressing willingness to improve, Karen encountered several persistent implementation difficulties that cumulatively blocked therapeutic progress:
- Incomplete Activity Logs: Karen frequently returned without having completed her activity or mood monitoring sheets. This limited the therapist’s ability to identify avoidance patterns or calibrate future tasks based on real data.
- Values Identification Difficulties: When prompted to articulate core values, Karen focused exclusively on caregiving. She struggled to name goals or sources of meaning outside this role, restricting the range of behaviors that could be targeted for activation.
- Lack of Behavioral Follow-Through: Although activities were collaboratively scheduled and tailored to be feasible, Karen reported not attempting them. She cited fatigue, self-doubt, and a persisting belief that mood must improve before action could occur.
- Limited External Reinforcement: Efforts to involve her husband in reinforcement strategies were unsuccessful. His emotional unavailability created an environment where even attempted behaviors received little acknowledgment, and her depressive withdrawal was sometimes unintentionally reinforced.
Across sessions, these challenges recurred with little change, producing a recognizable pattern of persistent ignition failure, a concept now structurally defined in CDA as a failure in Drive emergence despite motivational expression.
3.5. Clinical Outcome
After twelve sessions of Behavioral Activation, Karen showed no measurable improvement in behavioral engagement, mood, or functional capacity. Her activity logs remained largely unfilled, scheduled behaviors were not attempted, and depressive symptoms, including hopelessness and fatigue, remained unremitting.
The clinicians interpreted this as a treatment nonresponse and cited multiple contextual contributors: her medical burden, caregiving load, lack of environmental reinforcement, and possible motivational deficits. Their analysis reflected the depth and limitations of existing behavioral frameworks available at the time.
In the absence of a multivariable structural model, however, Karen’s case remained clinically important but theoretically anomalous. It is this contradiction between insight, expressed willingness, and functional inertia that the present paper aims to reinterpret using Cognitive Drive Architecture and Lagun’s Law.
4. CDA Reinterpretation (Core Analysis)
To reinterpret Karen’s treatment course through Cognitive Drive Architecture (CDA), it is essential to first outline the structural mechanics that govern Drive within Lagun’s Law. CDA posits that effort is not the product of motivation alone but the emergent output of six interacting system variables (Primode, CAP, Flexion, Anchory, Grain, and Slip) organized across three domains: Ignition, Tension, and Flux (Lagun, 2025a; Lagun, 2025b). These variables interact according to the formal Drive Equation:
This structure provides a quantitative way to understand why effort emerges, stalls, or collapses.
Briefly, the variables function as follows:
- Primode: ignition threshold, determining whether action can begin at all (e.g., the system’s behavioral “spark plug”).
- CAP (Cognitive Activation Potential): emotional-volitional “voltage” that amplifies Primode exponentially.
- Flexion: degree of fit between the task and the individual’s cognitive configuration (task-to-self alignment).
- Anchory: strength of attentional tethering required to sustain effort (mental grip or tethering).
- Grain: internal friction: emotional drag, fatigue, shame, or contextual burden (like running through molasses).
- Slip: baseline system variance affecting behavioral consistency.
The equation implies several structural laws documented in Lagun’s work:
-
If Primode = 0, the entire Drive collapses to near-zero regardless of CAP or Flexion.
- ○
- This is mathematically embedded:
- High Grain in the denominator reduces Drive yield, even when all other variables are favorable.
- CAP amplifies Primode nonlinearly, meaning emotional energy only matters if ignition is already possible.
- Slip adds behavioral variability but cannot compensate for a zeroed ignition system.
These dynamics create a structure in which an individual can want to act, understand how to act, and cognitively endorse the value of action yet remain completely unable to initiate behavior. This is precisely the paradox observed by Hopko, Magidson, and Lejuez (2011).
To frame the analysis mathematically, consider the specific observations from the case:
- No initiation of any BA task → Primode ≈ 0
- Expression of desire to improve → CAP > 0, but low amplitude
- Activities felt incompatible with identity and physical state → Flexion low
- Inconsistent monitoring, rapid drift → Anchory low
- Hopelessness, fatigue, caregiving burden → Grain extremely high
- Stable inactivity → Slip low
Plugging these qualitative estimates into the Drive Equation yields a predictable structural outcome:
This matches Karen’s behavioral presentation: complete non-initiation across twelve sessions.
From a BA standpoint, this is puzzling because BA assumes that once values are clarified and actions are scheduled, Primode implicitly becomes available. CDA does not make this assumption. Instead, it formalizes the dependency structure of ignition and explains how someone can be internally aligned with change yet remain behaviorally inert.
This is essential because:
- Each variable will now be mapped to concrete behaviors reported in the original case.
- The Drive Equation constrains interpretation, ensuring we do not over-attribute any single variable.
- It clarifies how multivariate interactions produce simple clinical outcomes (in this case, non-activation).
- It sets the stage for explaining contradictions that BA could not organize without critiquing the BA model itself, which was never designed to model ignition mechanics.
With this foundation in place, the following sections analyze each CDA variable as it appears in Karen’s presentation.
4.1. Primode: Structural Ignition Blockade
Primode is the ignition variable in Cognitive Drive Architecture. It determines whether the system can transition from intention to action at all (Lagun, 2025a; Lagun, 2025b). Unlike motivation, which can be high even in severely depressed states, Primode reflects a structural readiness threshold. If it remains near zero, Drive collapses, regardless of desire, understanding, or external reinforcement.
Karen’s case demonstrates the clearest possible presentation of a Primode-zero configuration. Despite full engagement in therapy sessions, repeated expressions of wanting improvement, and cognitive understanding of the BA rationale, she did not initiate a single BA assignment across twelve weeks (Hopko, Magidson & Lejuez, 2011). Within CDA, this pattern is diagnostic of ignition failure rather than motivational deficit.
4.1.1. Behavioral Evidence of Primode Suppression
Every observable data point in the case indicates that the ignition system failed to activate:
- 1.
-
No assignment was ever initiated between sessions
- a.
- No walks.
- b.
- No calls to friends.
- c.
- No completion of monitoring logs.
- d.
- No attempts at value-aligned actions.
This total absence of activation across months of treatment is incompatible with models assuming that motivation or understanding alone generates behavior. BA presumes that insight + scheduling produce at least minimal behavioral momentum. Karen produced none.
- 2.
-
Her verbal reasoning revealed an ignition gateKaren repeatedly said variants of:“I can’t start until I feel better.”This belief acts as a cognitive key that locks the ignition system. In CDA, such a belief is not a thought error; it is a structural permission rule. If the internal rule for action is “mood → action” and the treatment rule is “action → mood,” the ignition point is blocked by a contradictory gate condition.
- 3.
-
Medical burden created physiological Primode inhibitionBreast cancer and associated fatigue significantly reduced Karen’s internal availability for task initiation. In CDA, severe fatigue reduces Primode independent of motivation:If energy availability is extremely low, Primode stays below the threshold even if CAP is moderate.
- 4.
- Caregiving identity created a second permission blockadeKaren’s self-concept of “caregiver first, self never” meant that initiating self-directed action required violating an internalized role. Within CDA, identity-based permission rules are part of the Primode structure.
Action is impossible if the system does not grant itself permission to start.
4.1.2. Structural Interpretation Using the Drive Equation
The Drive Equation is:
When Primode = 0, the entire numerator collapses. Let us illustrate this with a realistic structural simulation:
Assume (based on case patterns):
- Primode = 0.05 (near zero; ignition not available)
- CAP = 2 (she wanted to improve, but emotional voltage low)
- Flexion = 0.3 (tasks felt mismatched)
- Anchory = 0.2 (weak tethering)
- Grain = 1.8 (high emotional friction)
- Slip = 0.05 (rigid, stable depressive pattern)
Plugging into the equation:
A Drive value of corresponds behaviorally to no meaningful action. This exactly matches the empirical outcome: 12 sessions, zero activation.
If we hypothetically raise CAP to a high level (e.g., CAP = 5):
Even extremely high motivation produces almost no Drive when Primode ≈ 0. This is why Karen’s verbal desire for improvement did not translate into action. This dynamic is illustrated in Figure 3, which depicts how Drive remains near zero until Primode crosses the ignition threshold.
4.1.3. Why Primode Remained Near Zero in Karen’s System
- 1.
- Cancer-related fatiguePhysical depletion lowered readiness so severely that initiation was structurally impossible, not merely difficult.
- 2.
- Emotional gating rule: “Mood must improve first”This rule set the ignition threshold infinitely high. Primode cannot rise when the system believes it must wait.
- 3.
- Caregiving load and self-permission deficitKaren implicitly deprived herself of permission to allocate energy toward her own well-being.
- 4.
- Absence of reinforcing environmentAlthough this affects Grain and Anchory more directly, it indirectly reduced Primode by removing any anticipatory sense of reward.
These factors collectively made ignition impossible.
4.1.4. Why BA Could Not Explain This but CDA Can
Behavioral Activation assumes:
- Once a patient understands the rationale,
- And values are identified or clarified,
Primode > 0.
BA methods work downstream of ignition. They were never designed to assess or model the ignition threshold itself. In Karen’s case:
- She understood the rationale (cognition intact),
- She endorsed the goal (motivation intact),
- The therapist delivered the protocol correctly (method intact),
yet the ignition system never activated. This produced a paradox that BA can describe but cannot structurally explain.
What CDA provides
CDA introduces a formal ignition variable.
If Primode = 0:
- No task begins,
- No amount of motivation produces action,
- No scheduling yields behavior,
- No reinforcement becomes available (because nothing happens to reinforce).
It turns Karen’s paradox into a mechanically coherent outcome:
Which matches the 12-session outcome exactly.
4.2. CAP: Activation Potential Misalignment
CAP (Cognitive Activation Potential) represents the emotional-volitional “voltage” in Lagun’s Law, the intensity of internal energy available to amplify Primode at the moment of task initiation (Lagun, 2025a; Lagun, 2025b). Unlike motivation, which can be stable and conceptual, CAP describes dynamic, moment-specific readiness energy. Within the Drive Equation, CAP serves as an exponential multiplier on Primode:
Even small reductions in CAP dramatically reduce the effective output of Primode. In Karen’s case, CAP was not absent; she repeatedly expressed a desire to improve, but it remained insufficiently energized to overcome high Grain or compensate for a Primode at or near zero.
4.2.1. Evidence of Low CAP Despite Verbal Desire
Hopko, Magidson & Lejuez (2011) note that Karen often expressed a wish to feel better and endorsed the idea that activation might help. The therapist described her as cooperative, attentive, and engaged during sessions. These features indicate that a cognitive-level desire for improvement was present.
However, several elements suggest low emotional-volitional voltage:
- 1.
-
Emotional flatnessKaren acknowledged BA principles but did not appear emotionally mobilized by them. She “understood but did not internalize” the rationale. Emotional resonance is a key contributor to CAP; without it, initiation energy stays weak.
- 2.
-
Hopelessness as a CAP dampenerShe frequently described her situation as overwhelming and doubted that small actions would make any difference. Hopelessness suppresses CAP by reducing the internal sense that action is consequential.
- 3.
-
Cancer-related fatigueThe physical burden of cancer treatment depleted not only physical energy but also emotional voltage. Chronic fatigue has a direct lowering effect on CAP because it reduces the moment-to-moment energetic availability required for ignition.
- 4.
-
Lack of reinforcing social contextIn CDA, CAP is influenced by anticipated emotional return. Since Karen’s environment offered little reinforcement, her husband was emotionally unavailable, her daughter uninvolved, and her internal activation potential had no anticipatory signal to rise. Together, these factors indicate a persistent CAP value below the minimum needed to meaningfully amplify Primode.
4.2.2. Structural Interpretation Using the Drive Equation
To grasp the role of CAP mathematically, consider the exponential relationship between CAP and Primode:
Even modest CAP levels (e.g., CAP = 3 to 5) can significantly boost a mid-range Primode. But when Primode is near zero, even extremely high CAP produces negligible activation.
Example Simulation Based on Karen’s Presentation
From Section 4.1, we estimated:
- Primode ≈ 0.05
- CAP ≈ 2 (reflecting desire without emotional ignition)
- Flexion ≈ 0.3
- Anchory + Grain ≈ 2.0
- Slip ≈ 0.05
Now observe the effect of increasing CAP.
Case A: CAP = 2 (likely Karen’s range)
Drive contribution remains negligible.
Case B: CAP = 4 (hypothetical strong emotional voltage)
Even strong CAP produces nearly no activation because the base (Primode) is too small.
Case C: CAP = 10 (extremely high voltage for illustration)
Even massive emotional voltage cannot meaningfully magnify a near-zero Primode. As shown in Figure 4, increasing CAP produces a meaningful rise in Drive only when Primode is mid-range or higher, while near-zero Primode remains almost flat regardless of CAP level.
Interpretation
Karen’s emotional desire to improve, however sincere, could not translate into movement because:
- CAP was not strong enough to overcome extraordinarily high Grain.
- CAP was not volatile enough to produce spontaneous small actions.
- CAP could not amplify Primode because Primode itself was suppressed.
Thus, even if Karen had moments of wanting to try something new, these were structurally incapable of catalyzing real-world activation.
4.2.3. Depression’s Effect on CAP: Emotional Amplitude Flattening
CDA integrates emotional modulation structurally rather than descriptively. Depression flattens emotional amplitude, reducing the volatility needed for CAP to rise spontaneously (Lagun, 2025b). In Karen’s case:
- Hopelessness constricted upward CAP fluctuations.
- Emotional numbing reduced the “spark” that normally initiates new behavior.
- Fatigue lowered the voltage supply itself.
- Contextual invalidation (lack of familial reinforcement) prevented CAP surges.
Therefore, even when Karen said, “I want to get better,” the internal voltage required to amplify Primode remained consistently below the activation threshold.
4.2.4. Why BA Could Not Explain This but CDA Can
Limitations of BA Regarding CAP
Behavioral Activation presumes that once patients understand the rationale and articulate their values:
- motivation becomes behaviorally usable,
- emotional readiness is sufficient for small steps,
- the patient possesses enough internal energy to begin scheduled tasks.
BA does not distinguish between:
- verbal desire and
- activation voltage capable of initiating behavior.
Thus, from a BA viewpoint, Karen’s lack of action appears inconsistent with her expressed intentions.
How CDA Clarifies the Paradox
CDA draws a clear structural distinction:
- Motivation = conceptual desire.
- CAP = ignition voltage.
Karen had motivation but not voltage.
CDA shows mathematically why:
- A person can sincerely want change,
- Understand the treatment model,
- Agree to try new behaviors and still produce zero activation.
Because:
If Primode is tiny, increasing CAP barely moves Drive.
This resolves the paradox BA could not organize. Karen was not resistant or unmotivated; her internal activation potential was simply too low to amplify a suppressed Primode.
4.3. Flexion: Task–System Misfit
Flexion in Cognitive Drive Architecture refers to the system’s ability to adapt or “bend” a task into a workable shape. A system with high Flexion can scale tasks down, reshape them, or reframe them so that they feel cognitively compatible with the individual’s internal state. When Flexion is low, even simple tasks appear rigid, non-negotiable, and emotionally or physically incompatible with the person’s moment-to-moment configuration (Lagun, 2025a; Lagun, 2025b).
Karen’s presentation during Behavioral Activation (BA) is a case of a Flexion collapse: every BA task, no matter its size, duration, or structure, felt unworkable to her, not because of its difficulty but because it never matched her internal constraints.
This section examines how Flexion operated in Karen’s system, using only observable evidence from Hopko, Magidson & Lejuez (2011).
4.3.1. Behavioral Evidence of Flexion Failure
- 1.
-
Global rejection of tasks regardless of size or contentKaren declined nearly all behavioral tasks assigned during BA, including the smallest possible ones:
- a.
- a few minutes of walking,
- b.
- calling a friend,
- c.
- writing brief notes,
- d.
- completing monitoring sheets.
She did not reject tasks strategically but globally. This pattern indicates low Flexion; her system could not adjust or reshape the task demands to her internal state. - 2.
-
“Not worth it,” “not possible right now,” “too tired” responsesThese phrases appeared repeatedly in session summaries (Hopko et al., 2011). In CDA, these responses indicate that the task geometry felt incompatible with her present cognitive and physiological configuration.A high-Flexion system would say, “Maybe I’ll try a smaller version.” A low-Flexion system says only, “No.”Karen consistently produced the latter.
- 3.
-
Narrowed values space (caregiving identity only)Karen struggled to identify any value outside her caregiving role. She did not articulate values related to:
- a.
- personal health
- b.
- emotional restoration
- c.
- social connection
- d.
- autonomy or competence
This severe narrowing of valued domains leaves BA with almost no “flexible handles” to map tasks onto. When values collapse, Flexion collapses with them. - 4.
-
Physical fatigue eliminating cognitive task adaptabilityCancer-related fatigue limited not just her energy but also her adaptability. Hopko et al. (2011) describe her as “exhausted,” “worn down,” and “overwhelmed.” In CDA, physical exhaustion directly constrains Flexion by reducing:
- a.
- cognitive bandwidth,
- b.
- emotional responsiveness,
- c.
- capacity for micro-adjustments in task shape.
A fatigued system cannot reconfigure tasks well. - 5.
-
Lack of generative alternativesPatients with moderate Flexion usually propose alternative activity forms:
- a.
- shorter versions,
- b.
- different times,
- c.
- different contexts,
- d.
- different people.
Karen generated almost no alternatives. This absence is a direct behavioral signature of Flexion deficiency.
4.3.2. Structural Interpretation of Flexion in Karen’s System
Flexion determines whether tasks “bend to fit” the system. Karen’s system provided no bendability for several reasons:
- 1.
- Identity rigidity (“caregiver first, self last”)
Karen operated within a strict identity structure that limited what kinds of actions were permissible. Tasks involving self-care or personal well-being did not fit this identity architecture.
Low identity flexibility → low Flexion.
- 2.
-
Emotional hopelessness rigidified cognitive configurationHopko et al. (2011) note repeated expressions of hopelessness and futility. Hopelessness reduces:
- a.
- openness to reinterpreting tasks,
- b.
- willingness to experiment,
- c.
- tolerance for ambiguity.
This flattens the internal landscape, leaving tasks unable to fit. - 3.
-
Physical burden reduced degrees of freedomFatigue limited not only capacity but also adaptability. Karen’s system had fewer “degrees of freedom” to transform a task into something executable.
- 4.
-
Values constriction blocked task adaptationBecause her values map contained a single node (caregiving), tasks that did not directly serve that role felt meaningless. Tasks without perceived meaning cannot bend to fit.
4.3.3. Numerical Illustration: Flexion Near Zero
To emphasize the structural effect (not actual measurement), consider a qualitative simulation.
Let Flexion be approximated at 0.1 on a normalized scale where:
- 1.0 = high adaptability
- 0.5 = moderate adaptability
- 0.1 = extremely low adaptability
With Flexion ≈ 0.1:
- A “small” task remains effectively the same size.
- A “modifiable” task cannot be modified.
- A “low-cost” task feels high-cost.
If Primode and CAP were both mid-range, a Flexion of 0.1 would still severely reduce behavioral yield. When Primode is already near zero, Flexion = 0.1 compounds the paralysis. This structural pattern matches Karen’s presentation almost exactly, as shown in Figure 5.
4.3.4. How Flexion Explains Key Clinical Confusions
-
Why cognitive understanding did not translate into behaviorBA assumes that once rationale and values are understood, patients can adapt tasks to their lives. Karen understood but could not adapt.
-
Why values clarification failed to generate meaningful actionsValues clarification failed not because Karen lacked values but because her value structure was too narrow to support flexible actions. Flexion requires multiple value anchors. She had one.
-
Why “simple tasks” were rejected alongside “bigger tasks”Across all assignments, rejection was uniform. Flexion explains this uniformity: if a system cannot adapt to tasks, its size does not matter.
-
Why no “micro-steps” emerged despite therapist supportMicro-stepping requires Flexion. Karen consistently showed none.
4.3.5. Why BA Could Not Explain This but CDA Can
Limitations of BA’s conceptual tools
BA assumes:
- patients can flexibly choose and modify tasks once values are clarified;
- even fatigued or depressed patients can scale tasks down;
- values produce a menu of possible actions.
BA has no structural variable for task adaptability. Thus, Karen’s complete inability to reshape any task appeared paradoxical or resistant.
What CDA clarifies
CDA formalizes Flexion as an internal variable that can be:
- high (tasks feel shapeable),
- moderate (tasks can be adapted with effort),
- low (tasks feel rigid or impossible),
- near zero (task geometry collapses entirely).
Karen’s system shows Flexion ≈ 0: a configuration where no task, however small, can become cognitively workable.
This eliminates the paradox. Karen did not reject BA tasks because of refusal, misunderstanding, or lack of desire. She rejected them because no task geometry existed that her system could bend into action.
4.4. Anchory: Tethering Breakdown
Anchory represents the system’s ability to hold attention on a task once it is selected. It describes the stability and strength of the attentional tether required to sustain engagement long enough for a behavior to occur. Anchory is neither motivation nor attentional capacity; it is the structural glue that binds intention to execution across time (Lagun, 2025a; 2025b).
In Karen’s case, all observable indicators point to a system with extremely weak Anchory. Even if she had occasional moments of interest or intent, these moments did not persist long enough for actionable behavior to form. A system with low Anchory “slides off” tasks before they can be enacted, similar to trying to grip an object with no friction.
4.4.1. Behavioral Evidence of Tether Fragility
- 1.
-
Highly inconsistent attention to BA tasksKaren demonstrated immediate attentional collapse across nearly every assignment:
- a.
- Activity logs were rarely completed.
- b.
- Monitoring sheets returned blank even after multiple reminders.
- c.
- Tasks discussed in session were forgotten by the next session.
This is not inattentiveness in the cognitive sense. It is tethering collapse. - 2.
-
Rapid drift back into habitual avoidanceHopko et al. (2011) note that Karen often reverted to sleeping in, withdrawing, or remaining inactive. This drift occurred not after attempting tasks, but instead of any attempt at all. Low Anchory means intentions cannot be “held in working engagement” long enough to manifest behavior.
- 3.
-
In-session engagement did not carry overKaren was described as attentive and cooperative during sessions. Yet this attentional engagement was extremely context-bound: it dissolved as soon as the session ended. This session-bound engagement profile is a hallmark of weak Anchory: attention can be established but not retained.
- 4.
-
Fatigue-induced micro-lapsesSevere fatigue from cancer treatment would have weakened her ability to sustain even brief cognitive anchoring. Fatigue does not just reduce energy. It erodes attentional tether strength.
- 5.
-
No evidence of spontaneous re-engagementIndividuals with moderate Anchory may drift but later return to tasks. Karen did not spontaneously resume any BA task once attention lapsed, further indicating a system that cannot re-anchor without external scaffolding.
4.4.2. Structural Interpretation of Anchory in Karen’s System
Anchory stabilizes behavior once Primode and CAP begin to activate. Even if Karen had small sparks of readiness, low Anchory ensured these sparks dissipated instantly.
Based on the behavioral data, Karen’s Anchory level would be qualitatively estimated as very low, close to the bottom decile of functional tethering strength. To illustrate structurally:
Illustrative anchoring breakdown
Let Anchory ≈ 0.2 on a normalized 0–1 scale.
What this means in CDA terms:
- Intentions evaporate quickly.
- Engagement cannot survive even minor emotional or cognitive interruptions.
- Tasks require external scaffolding to remain in awareness.
- Internal cues fail to trigger task recall.
- Activation falters even before Grain exerts influence.
In this configuration, even a moment of willingness or emotional lift (CAP spike) cannot sustain an attempt long enough to produce behavior.
Interaction with Depression
Depressive symptoms further reduce Anchory by:
- lowering cognitive persistence,
- reducing attentional stability,
- increasing mental fatigue,
- increasing susceptibility to emotional drift.
Hopko et al.’s (2011) documentation of Karen’s exhaustion and hopelessness aligns tightly with a structurally weakened Anchory.
4.4.3. Clinical Patterns Explained by Low Anchory
- 1.
-
Incomplete activity logs despite repeated promptsBA relies heavily on monitoring as the first behavioral foothold. Karen’s inability to complete logs, even when she verbally agreed, indicates not oppositionality but failure of attentional tethering.
- 2.
-
“I forgot” as genuine structural outputKaren often returned saying she “forgot” or “never got around” to an activity. These are behavioral signatures of weak Anchory, not poor motivation.
- 3.
-
The disconnect between in-session clarity and out-of-session absenceKaren could discuss tasks coherently in session; Anchory is temporarily stabilized by therapist structure, but structural tethering collapsed outside that scaffold.
- 4.
-
Drift back to habitual patterns without attempting alternativesAnchory enables shift maintenance, not shift initiation. Karen could shift cognitively (in-session) but could not maintain the shift long enough to enact behavior (out-of-session).
- 5.
- Fatigue amplifying tether fragility
Cancer-related exhaustion directly suppressed Anchory, compounding the collapse of sustained engagement.
4.4.4 Numerical Illustration: Anchory Too Weak to Support Behavior
To illustrate structural effects, not empirical measurement, consider:
- Primode ≈ 0.05
- CAP ≈ 2
- Flexion ≈ 0.1
- Grain ≈ 1.8
- Slip ≈ 0.05
Let’s vary Anchory:
Case A: Anchory = 0.2 (likely Karen)
Intent cannot hold: behavior never forms.
Case B: Anchory = 0.5 (moderate tethering)
Even if Primode is low, moderate Anchory would allow:
- partial micro-tasks,
- occasional log attempts,
- intermittent inconsistent activation.
Karen showed none of these.
Case C: Anchory = 0.8 (strong tethering)
Strong Anchory would allow
- values to persist as guides,
- assignments to stay cognitively alive,
- tasks to be retried.
Karen’s behavior corresponds to Case A, a structural tether too weak to sustain any action. This decay pattern is illustrated in Figure 6, which contrasts the rapid tether loss of weak Anchory with the sustained tethering seen in stronger configurations.
4.4.5. Why BA Could Not Explain This but CDA Can
Limitations of BA
Behavioral Activation assumes:
- once tasks are scheduled,
- once values are clear,
- and once rationale is accepted,
attention will remain sufficiently stable to allow execution.
BA has no mechanism to detect or model attentional tether collapse. Thus, the clinicians interpreted Karen’s non-follow-through as:
- motivational deficits,
- task aversiveness, or
- emotional avoidance.
BA describes attentional drift but does not treat it as a structural variable.
What CDA Clarifies
CDA defines Anchory explicitly and shows:
- Activation cannot survive without attentional tethering.
- Even moderate motivation (CAP) cannot overcome low Anchory.
- Session-based insight cannot transfer if Anchory collapses between sessions.
- Systems with Anchory < threshold produce precisely the behavioral pattern Karen displayed.
CDA resolves the clinical puzzle: Karen was attentive in session and inert outside session not because she was unwilling, but because she lacked structural tethering to hold tasks in place long enough for action to occur.
4.5. Grain: Internal Resistance and Emotional Friction
Grain in Cognitive Drive Architecture refers to the internal resistance that pushes against activation. It includes emotional drag (hopelessness, shame, anticipated failure), physiological load (fatigue, illness), and contextual pressure (caregiving demands, limited reinforcement). Grain is not a reduction in motivation; it is an opposing force that absorbs activation before it can translate into action (Lagun, 2025a; 2025b).
Karen’s clinical presentation reflects a consistently high-Grain configuration. Emotional despair, chronic fatigue from breast cancer treatment, and the weight of full-time caregiving combined into a resistance state that overshadowed any small activation signals emerging during therapy (Hopko, Magidson, & Lejuez, 2011).
4.5.1. Behavioral and Contextual Evidence of High Grain
Several components of Karen’s life contributed directly to elevated resistance:
- 1.
-
HopelessnessKaren frequently described her situation as unchangeable and doubted that behavioral attempts would produce relief. This emotional stance creates significant resistance, as each action is filtered through futility.
- 2.
-
Medical fatigueCancer-related exhaustion made even minor tasks feel physically overwhelming. Physiological depletion increases internal friction, reducing the capacity to convert intention into movement.
- 3.
-
Caregiving burdenHer identity as the primary caregiver created internal conflict around self-directed actions. Tasks aimed at improving her well-being competed against a firmly held role expectation, generating guilt-based resistance.
- 4.
-
Lack of environmental reinforcementHer husband was emotionally unavailable, and her daughter did not participate in supporting change. The absence of anticipated reinforcement amplifies Grain, as the system predicts no external payoff for effort.
- 5.
-
Fear of failure and shameKaren expressed concern that attempting tasks might confirm personal inadequacy. This anticipation of emotional pain adds another layer of resistance.These elements interacted to create a sustained, high-resistance state.
4.5.2. Structural Interpretation of Grain’s Effect
To illustrate how Grain constrains behavioral output, consider a simplified structural example using representative values:
- Primode = 0.4
- CAP = 2
- Flexion = 0.3
- Anchory = 0.2
- Slip = 0.05
The ignition component contributes:
This value represents the activation available before resistance is applied.
Case A: Lower resistance (Grain = 0.5)
Adding Slip (0.05):
With moderate Grain, some activation survives. The behavioral expectation would be at least partial task attempts or intermittent follow-through.
Case B: Higher resistance (Grain = 1.8)
Adding Slip:
Under high Grain, the same ignition produces far less behavioral output. The clinical pattern would appear as minimal or no engagement.
Karen’s presentation aligns with the latter configuration. High emotional, physical, and contextual friction absorbed nearly all activation before it could manifest as behavior.
4.5.3. Clinical Meaning of High Grain in This Case
The persistence of Grain explains several features of Karen’s nonresponse:
- Tasks felt pointless, not simply difficult, because hopelessness blocked perceived value.
- Fatigue amplified resistance, making even micro-activities feel burdensome.
- Caregiver identity conflicted with self-directed action, creating internal prohibitions.
- A non-reinforcing environment removed the anticipated reward, reducing the likelihood of sustained engagement.
- Shame and fear of failure added emotional cost to every possible action.
Together, these produced a resistance profile strong enough to overpower any momentary desire or understanding of the treatment rationale.
4.5.4. Why BA Could Not Explain This but CDA Can
Behavioral Activation acknowledges that life stress, fatigue, and lack of reinforcement impede progress, but it does not conceptualize these elements as a unified internal resistance force. As a result, BA can describe the barriers Karen faced, but it cannot explain why no behavioral activation occurred despite comprehension, participation, and stated desire for improvement.
CDA treats internal friction as a structural variable. When Grain is high, activation dissipates before it becomes observable behavior, regardless of motivation. Karen’s complete non-engagement is therefore not paradoxical within CDA: her emotional, physical, and contextual conditions created a resistance load that exceeded her available activation.
This structural interpretation gives form to what BA could only describe, showing how her system’s resistance configuration made behavioral change mechanically unattainable.
4.6. Slip: Variability and Performance Entropy
Slip in Cognitive Drive Architecture represents endogenous variability in the system: the small, stochastic fluctuations in effort, attention, affect, and behavior that cause people to sometimes act “out of character,” trying a task on a good day, attempting something once, or briefly breaking from avoidance (Lagun, 2025a; 2025b). High Slip produces irregular patterns (bursts of activity amidst avoidance), whereas low Slip produces rigid patterns (the same outcome, over and over, regardless of shifts in intention or context).
Karen’s behavior across the Behavioral Activation protocol suggests a low-Slip configuration. She showed no intermittent attempts, no partial task completions, and no spontaneous deviations from her avoidance routine across twelve sessions (Hopko, Magidson, & Lejuez, 2011). Her pattern was not chaotic; it was stable non-activation.
4.6.1. Behavioral Evidence of Suppressed Variability
Evidence for low Slip in Karen’s case includes:
- 1.
-
Uniform absence of task attemptsNone of the scheduled activities were attempted, not once. There were no partial walks, no half-completed logs, and no “I tried but couldn’t finish.” This level of uniformity is characteristic of low variability.
- 2.
-
Stable daily routineHer behavior remained dominated by extended sleep, withdrawal, and sustained inactivity. Hopko et al. (2011) do not describe alternating “better days” of relative engagement; patterns were steady and fixed.
- 3.
-
No spontaneous micro-experimentsDepressed patients with moderate Slip often make unintended attempts (e.g., answering one call, stepping outside briefly, writing down a few activities). Karen did not show this kind of accidental behavioral noise.
- 4.
-
Emotional and energetic flatnessHer hopelessness and fatigue were persistent, with little documented fluctuation. Slip is often mirrored by emotional variability; a flat emotional profile suggests reduced entropy.
These features jointly indicate an architecture in which endogenous fluctuation is minimal.
4.6.2. Structural Role of Slip in the System
Slip contributes to Drive as a small, variability-based term that can occasionally push the system above the threshold required for action. When other variables are weak (low Primode, low CAP, low Flexion, weak Anchory, high Grain), Slip is often the only source of rare, accidental activation.
In a system like Karen’s, with:
- near-zero Primode,
- low CAP,
- low Flexion,
- weak Anchory,
- high Grain,
Slip becomes the only realistic pathway for a “one-off” behavior, a single completed log, a brief phone call, or a solitary walk. The fact that none of these appeared suggests Slip was very small.
4.6.3. Numerical Illustration: Slip as Variability Around a Fixed Baseline
To quantify Slip as variability, consider a simplified representation where:
- the deterministic part of Drive (from Primode, CAP, Flexion, Anchory, Grain) is near zero, say, 0.02,
- Slip represents a random fluctuation around this baseline.
Assume Slip behaves as a zero-mean noise term with magnitude sss, and that the system needs Drive ≥ 0.10 to produce any visible behavioral activation (e.g., one small task attempted).
Let:
- Baseline Drive (without Slip) = 0.02
- Activation threshold = 0.10
Define Slip as a random value drawn from a normal distribution with standard deviation sss:
The probability of a spontaneous activation event is:
Case A: Very low Slip (e.g.,)
For a standard normal, P(Z≥2.67) ≈ 0.0038, or 0.38%.
Across 12 weeks, the expected number of spontaneous activation events is 12 × 0.0038 ≈ 0.046,
effectively, zero. This pattern matches Karen’s observed behavior: no accidental task attempts.
Case B: Moderate Slip (e.g., s=0.10s = 0.10s=0.10)
P(Z≥0.8) ≈ 0.2119, or 21.2%.
Across 12 weeks, expected spontaneous activations ≈ 12 × 0.21 ≈ 2.5.
In such a system, one would expect a few isolated attempts, a log filled once, a walk tried, and
some inconsistent effort. This is the pattern often seen in depressed patients who partially respond
or show “good days.”
Karen’s pattern aligns with Case A, not Case B. Her observed behavior is consistent with a Slip
magnitude so low that the probability of crossing the activation threshold is effectively negligible.
This distribution is illustrated in Figure 7, which shows how low Slip keeps nearly all Drive values
below the activation threshold.
4.6.4. Clinical Meaning of Low Slip in Karen’s Case
Low Slip has several direct implications:
-
Inertia becomes absoluteWith minimal variability, the system remains locked in its dominant pattern, in this case, avoidance and withdrawal.
-
No footholds for reinforcement emergeBA needs at least one or two behaviors to reinforce. Without occasional deviations, there is nothing to shape.
-
Insight cannot “leak” into behaviorIn-session understanding may fluctuate slightly, but low Slip prevents these fluctuations from producing observable actions between sessions.
-
Rigidity becomes the default stateEven if the rest of the architecture changes slightly, low Slip keeps behavior nearly constant.
This helps explain why, across twelve sessions, there was not a single instance of Karen “surprising herself” by managing even a small assigned task.
4.6.5. Why BA Could Not Explain This but CDA Can
Behavioral Activation implicitly assumes some level of variability: that patients will attempt at least a small portion of tasks, sometimes inconsistently, creating opportunities to reinforce and shape behavior. When a patient exhibits unwavering non-initiation across time and conditions, BA has no dedicated construct to describe the absence of variability beyond “severe nonresponse.”
CDA treats Slip as a formal variable capturing exactly this dimension. When Slip is very low:
- spontaneous deviations from avoidance almost never occur,
- accidental successes are rare to nonexistent,
- the system generates a flat behavioral output even in the presence of insight and desire.
Karen’s pattern (no tasks attempted, no partial compliance, no behavioral spikes) fits a low-Slip profile precisely. What appeared, within BA, as puzzling rigidity becomes, within CDA, a predictable property of her Drive architecture: a configuration dominated by low Primode, low CAP, high Grain, and minimal variability.
5. Structural Integration
5.1. Reconstructing Karen’s Drive Architecture
Synthesizing the six CDA variables produces a coherent structural profile of Karen’s behavioral system during treatment. Her observed patterns across twelve Behavioral Activation (BA) sessions correspond to the following configuration:
- Primode: effectively zero, no ignition; no assignments initiated
- CAP: low, desire present but insufficient emotional–volitional energy
- Flexion: very poor, tasks did not fit her internal cognitive or emotional state
- Anchory: fragile, intentions dissipated rapidly outside the structured session context
- Grain: extremely high, persistent resistance from hopelessness, fatigue, role guilt, and lack of reinforcement
- Slip: low, minimal variability; no spontaneous attempts or deviations from avoidance
This configuration reflects a structural profile in which activation is highly unlikely to emerge. The calculated Drive output (~0.05) aligns with the complete absence of between-session behavioral change described in the case report (Hopko, Magidson, & Lejuez, 2011).
5.2. How These Variables Interact to Produce Total Inactivity
CDA clarifies how these six variables combine interactively to produce the observed clinical paralysis:
-
Primode remained below ignition thresholdWithout ignition readiness, no action can begin, regardless of motivation or insight.
-
Grain dominated the systemEmotional despair, physical exhaustion, caregiving strain, and a non-reinforcing home environment created a high-resistance field that absorbed nearly all available activation.
-
Low CAP provided insufficient voltageKaren wanted improvement but lacked the emotional energy to overcome resistance.
-
Flexion collapse prevented task adaptationBA assignments could not be reshaped into forms compatible with her depleted internal resources or rigid caregiver identity.
-
Weak Anchory prevented intentions from surviving between sessionsEngagement inside the therapy room did not translate into sustained action afterward.
-
Low Slip removed spontaneous chances for successWithout variability, no accidental or partial behaviors could emerge to generate momentum.
Together, these factors form a coherent architecture of near-zero Drive. BA does not include mechanisms for modeling ignition, resistance, or variability, so the complete lack of activation appeared paradoxical within its framework. CDA reveals the structural consistency underlying the treatment nonresponse.
5.3. Why BA Failed Coherently Within This Architecture
Behavioral Activation assumes:
- at least some ignition capacity (Primode > 0),
- sufficient emotional energy to support action,
- meaningful flexibility in how tasks are performed,
- the ability to hold task intentions between sessions, and
- enough variability for occasional success
None of these structural conditions were present.
Under BA, Karen’s nonresponse could only be described as “treatment failure.”
Under CDA, it is a predictable outcome of a system characterized by:
- Low Primode
- Low CAP
- Low Flexion
- Weak Anchory
- High Grain
- Low Slip
Her architecture was incompatible with BA’s assumptions, not because the patient was unwilling or the treatment was delivered incorrectly, but because the system could not generate activation under any BA-compliant pathway.
5.4. If the Case Were Evaluated Today
Lagun’s IJSRA paper (2025b) outlines how each CDA variable can now be quantified using available measurement tools via the Minimal Viable Application (MVA) layer. If Karen were evaluated under current conditions, clinicians could generate numeric estimates for each Drive variable before selecting an intervention. The corresponding MVA-compatible instruments for each CDA variable are summarized in Table 2.
These instruments would have made Karen’s configuration empirically visible:
- High Grain
- Near-zero Primode
- Weak Anchory
- Low Flexion
- Minimal Slip
Such a profile would clearly predict that BA would not ignite unless resistance were first reduced and ignition structurally supported.
6. Implications for Understanding & Treatment
6.1. Rethinking Treatment-Resistant Depression Through Structure
Karen’s case illustrates that what appeared as “treatment resistance” under Behavioral Activation (BA) can instead be understood as a structural mismatch between the patient’s Drive configuration and the assumptions embedded within BA.
Her configuration, suppressed Primode, low CAP, poor Flexion, fragile Anchory, high Grain, and low Slip, formed a system that could not produce ignition. Under Cognitive Drive Architecture (CDA), this is not framed as a failure of motivation or compliance. It is the predictable result of a non-igniting architecture, offering a structural explanation where BA could only describe surface behavior.
6.2. Grain Reduction as a Prerequisite to Activation
BA assumes that behavior can begin as soon as tasks are identified and scheduled. However, CDA shows that when Grain is extremely high, activation cannot occur, regardless of intention or insight.
High-Grain states often emerge when depression intersects with:
- Medical comorbidity
- Chronic fatigue
- Identity-based self-pressure
- Emotional hopelessness
- Low-reinforcement environments
Conceptually, this means that friction reduction must precede activation attempts. A system overloaded with Grain cannot translate desire or instruction into action.
6.3. Flexion as a Determinant of Task Feasibility
Flexion governs whether an individual can internally reshape a task into a workable form. Karen’s Flexion was extremely low: her caregiver identity, depleted energy, and narrowed cognitive posture prevented any BA task from being framed as doable.
This implies a key conceptual shift:
Before assigning values-driven tasks, a clinician may need to assess whether the person has the cognitive flexibility (Flexion) to adapt those tasks meaningfully.
BA presupposes Flexion.
CDA measures it.
6.4. Anchory Support as a Structural Foundation
Anchory determines how long an intention remains alive in the system. Karen’s Anchory was fragile; her in-session engagement never persisted into daily life.
CDA shows that even if Primode and CAP momentarily spark, weak Anchory prevents them from surviving context transitions.
This suggests treatment approaches may require:
- Environmental scaffolding
- Simplified intention structures
- Micro-tethering strategies
These forms of support help stabilize intention over time, allowing activation to endure beyond the therapy session.
6.5. Structural Assessment Before Intervention Selection
One of CDA’s key insights is that ignition, resistance, task fit, attention tethering, and variability are prerequisites, not byproducts, of behavioral change.
Lagun’s Minimal Viable Application (MVA) framework (2025b) describes how these Drive variables can be estimated using existing clinical tools:
- Primode → Initiation latency tasks
- CAP → Emotional–volitional intensity scales
- Flexion → Task-fit/load questionnaires
- Anchory → Sustained attention metrics
- Grain → Friction, burden, or fatigue indices
- Slip → Variability and micro-fluctuation analysis
Had these variables been assessed beforehand, Karen’s low Primode and high Grain architecture would have signaled that BA alone was unlikely to succeed, not because the therapy was wrong, but because the system was structurally unready. These relationships are summarized in Table 3, which links each CDA variable to its corresponding structural treatment implication.
8.6. Toward a CDA-Aligned Intervention Framework
The analysis of Karen’s case highlights the need for treatment approaches structurally aligned with Drive dynamics. While this section focuses on conceptual implications rather than specific techniques, it is important to note that CDA is formalized enough to be operationalized.
A complete CDA-aligned therapeutic toolkit, organized around the same six variables discussed here, is provided in the Supplementary Materials. This includes:
- Standardized tools for Drive-state assessment
- Procedures for Grain (resistance) reduction
- Ignition and Anchory support techniques
- Micro-interventions targeting Flexion and stabilizing Slip
These methods are not replacements for traditional treatments but structural complements, designed to align techniques with a patient’s underlying Drive profile, as modeled by Lagun’s Law.
The purpose of referencing these materials here is not to prescribe specific interventions but to highlight that CDA provides a coherent, structurally grounded framework for both assessment and action. It allows clinicians and researchers to explore how modifying the underlying Drive architecture may precede or enhance downstream behavioral outcomes.
7. Conclusion
Karen’s case presents a paradox that has long challenged behavioral and cognitive models of depression: a patient who understands the rationale for Behavioral Activation, expresses a desire to improve, participates consistently in treatment sessions, and yet shows no behavioral activation across twelve weeks. While traditional frameworks explain nonresponse through motivational deficits, reinforcement scarcity, or maladaptive cognition, none fully account for how insight and intention can coexist with complete behavioral inertia.
Cognitive Drive Architecture (CDA) resolves this paradox by shifting the level of explanation from surface behavior to the underlying structure of the drive system. Through this lens, Karen’s nonresponse emerges not as a clinical failure but as the predictable output of a structurally misaligned system, one in which Primode was suppressed, CAP insufficient, Flexion minimal, Anchory unstable, Grain excessive, and Slip constrained. In such a configuration, ignition cannot occur, emotional voltage cannot gain traction, resistance absorbs momentum, and variability is too limited to permit accidental activation. Viewed structurally, BA did not fail despite correct delivery. It failed because the required architectural conditions were not present.
This interpretation suggests a reorientation in how clinical readiness is understood. Interventions like BA implicitly assume the existence of ignition capacity, flexible task fit, and sufficient attentional tethering. CDA reframes these not as assumptions, but as measurable variables. Structural mismatches between therapy design and system architecture may lead to perceived treatment resistance that is, in fact, predictable and preventable.
A clearer clinical implication follows: until Primode and Grain are formally assessed, activation-based therapies should be deferred in systems showing signs of ignition failure or excessive resistance. CDA’s structural assessment model, operationalized through the Minimal Viable Application (MVA) framework, provides a way to estimate readiness through instruments that already exist in clinical psychology. With such assessments in place, interventions can be selected or modified based not on diagnosis alone, but on the system’s functional capacity to initiate change.
Future directions include empirical validation of CDA-derived variables, standardization of structural assessment procedures, and longitudinal studies tracking how drive profiles shift over time. Particularly promising is the question of whether modifying structural variables, such as reducing Grain or supporting Primode, can transform nonresponse cases into treatment-engaged trajectories.
Karen’s nonresponse, seen through CDA, is not a mystery to be managed but a mechanism to be understood. Recognizing the difference between therapeutic failure and structural incapacity marks a shift in clinical reasoning. Where BA saw paradox, CDA reveals pattern, and it is that structural clarity that offers a more precise foundation for future treatment matching.
Funding
The authors received no financial support for the preparation of this manuscript.
Conflict of interest
The authors declare no conflicts of interest for this work.
Ethical approval
Ethical approval was not required because the study reinterprets an already published case and uses no identifiable patient data.
Data availability
No new data were generated, and all information used is derived from previously published sources.
References
- Brehm, J. W., & Self, E. A. (1989). The intensity of motivation. Annual review of psychology, 40, 109–131. [CrossRef]
- Dimidjian, S., Hollon, S. D., Dobson, K. S., Schmaling, K. B., Kohlenberg, R. J., Addis, M. E., Gallop, R., McGlinchey, J. B., Markley, D. K., Gollan, J. K., Atkins, D. C., Dunner, D. L., & Jacobson, N. S. (2006). Randomized trial of behavioral activation, cognitive therapy, and antidepressant medication in the acute treatment of adults with major depression. Journal of consulting and clinical psychology, 74(4), 658–670. [CrossRef]
- Ferster, C. B. (1973). A functional analysis of depression. American Psychologist, 28(10), 857–870. [CrossRef]
- Gray, J.A. and McNaughton, N. (2000). The neuropsychology of anxiety: An enquiry into the functions of the septo-hippocampal system. Oxford University Press, Oxford.
- Hopko, D. R., Magidson, J. F., & Lejuez, C. W. (2011). Treatment failure in behavior therapy: focus on behavioral activation for depression. Journal of clinical psychology, 67(11), 1106–1116. [CrossRef]
- Huys, Q. J., Daw, N. D., & Dayan, P. (2015). Depression: a decision-theoretic analysis. Annual review of neuroscience, 38, 1–23. [CrossRef]
- Jacobson, N. S., Dobson, K. S., Truax, P. A., Addis, M. E., Koerner, K., Gollan, J. K., Gortner, E., & Prince, S. E. (1996). A component analysis of cognitive-behavioral treatment for depression. Journal of consulting and clinical psychology, 64(2), 295–304. [CrossRef]
- Lagun, N. (2025a). Cognitive Drive Architecture: Derivation and Validation of Lagun’s Law for Modeling Volitional Effort. Preprints. [CrossRef]
- Lagun, N. (2025b). Lagun’s law and the foundations of cognitive drive architecture: A first principles theory of effort and performance. International Journal of Science and Research Archive. [CrossRef]
- Lagun, N. (2025c). Latent Task Architecture: Modeling Cognitive Readiness Under Unresolved Intentions. [CrossRef]
- Lewinsohn, P. M. (1974). A behavioral approach to depression. In R. J. Friedman & M. M. Katz (Eds.), The psychology of depression: Contemporary theory and research. John Wiley & Sons.
- Martell, C. R., Addis, M. E., & Jacobson, N. S. (2001). Depression in context: Strategies for guided action. W W Norton & Co.
- Montague, P. R., Dayan, P., & Sejnowski, T. J. (1996). A framework for mesencephalic dopamine systems based on predictive Hebbian learning. The Journal of neuroscience : the official journal of the Society for Neuroscience, 16(5), 1936–1947. [CrossRef]
Figure 1.
Diagram of Lagun’s Law drive architecture (six variables mapped into Ignition, Tension, and Flux).
Figure 1.
Diagram of Lagun’s Law drive architecture (six variables mapped into Ignition, Tension, and Flux).
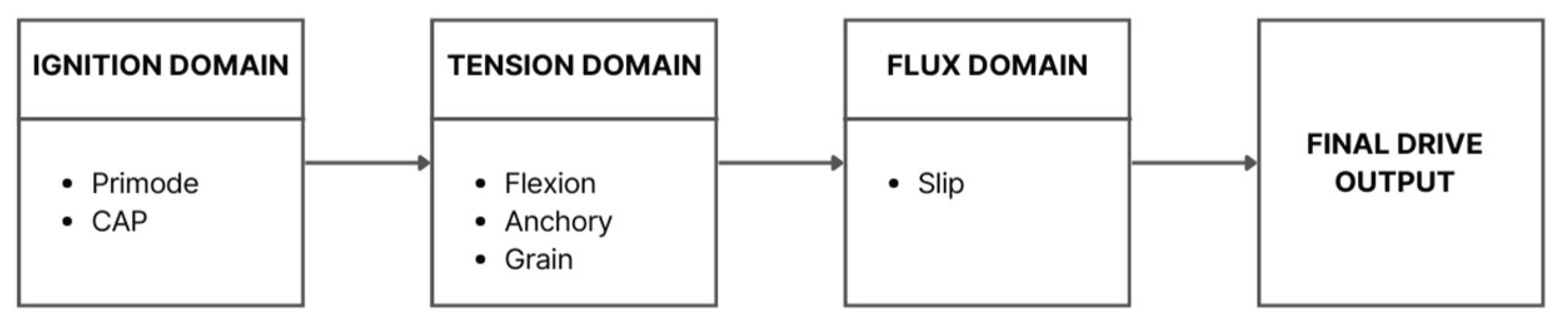
Figure 2.
A schematic flowchart illustrating the standard Behavioral Activation protocol.
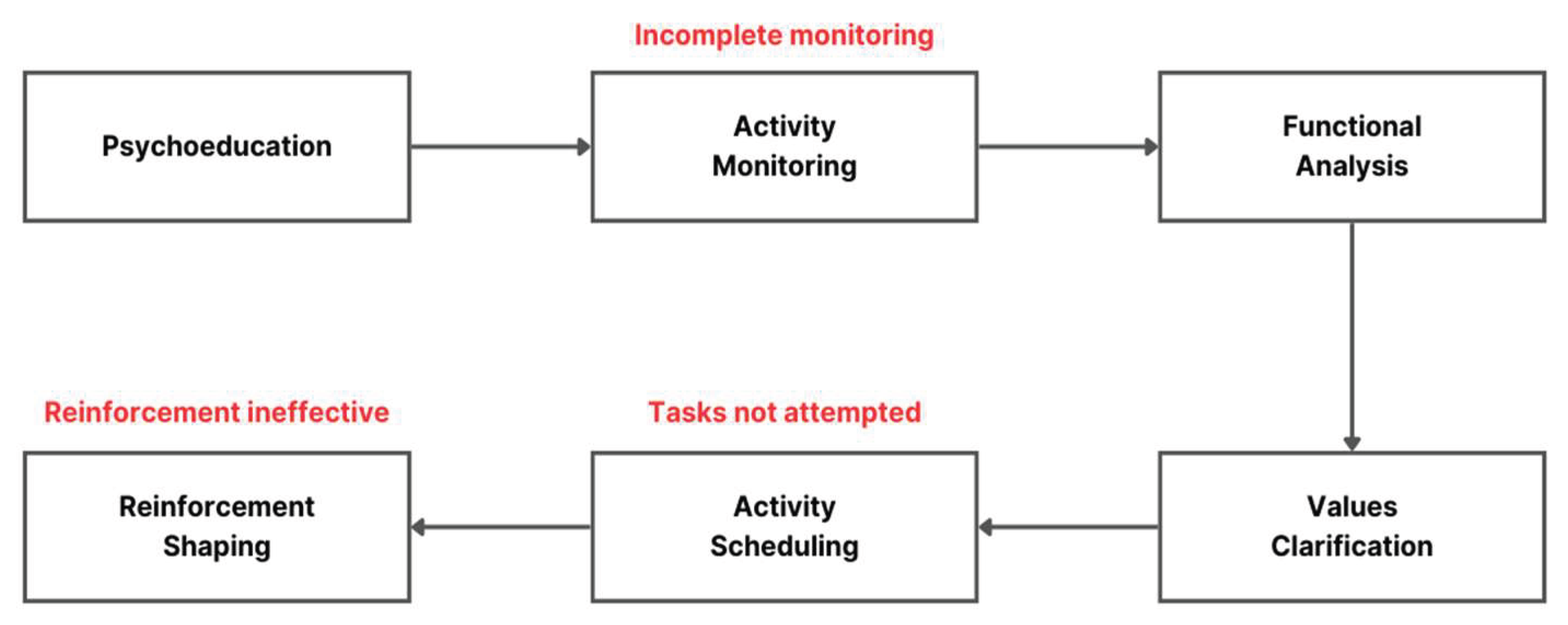
Figure 3.
Drive remains near zero when Primode is below the ignition threshold, regardless of CAP level.
Figure 3.
Drive remains near zero when Primode is below the ignition threshold, regardless of CAP level.
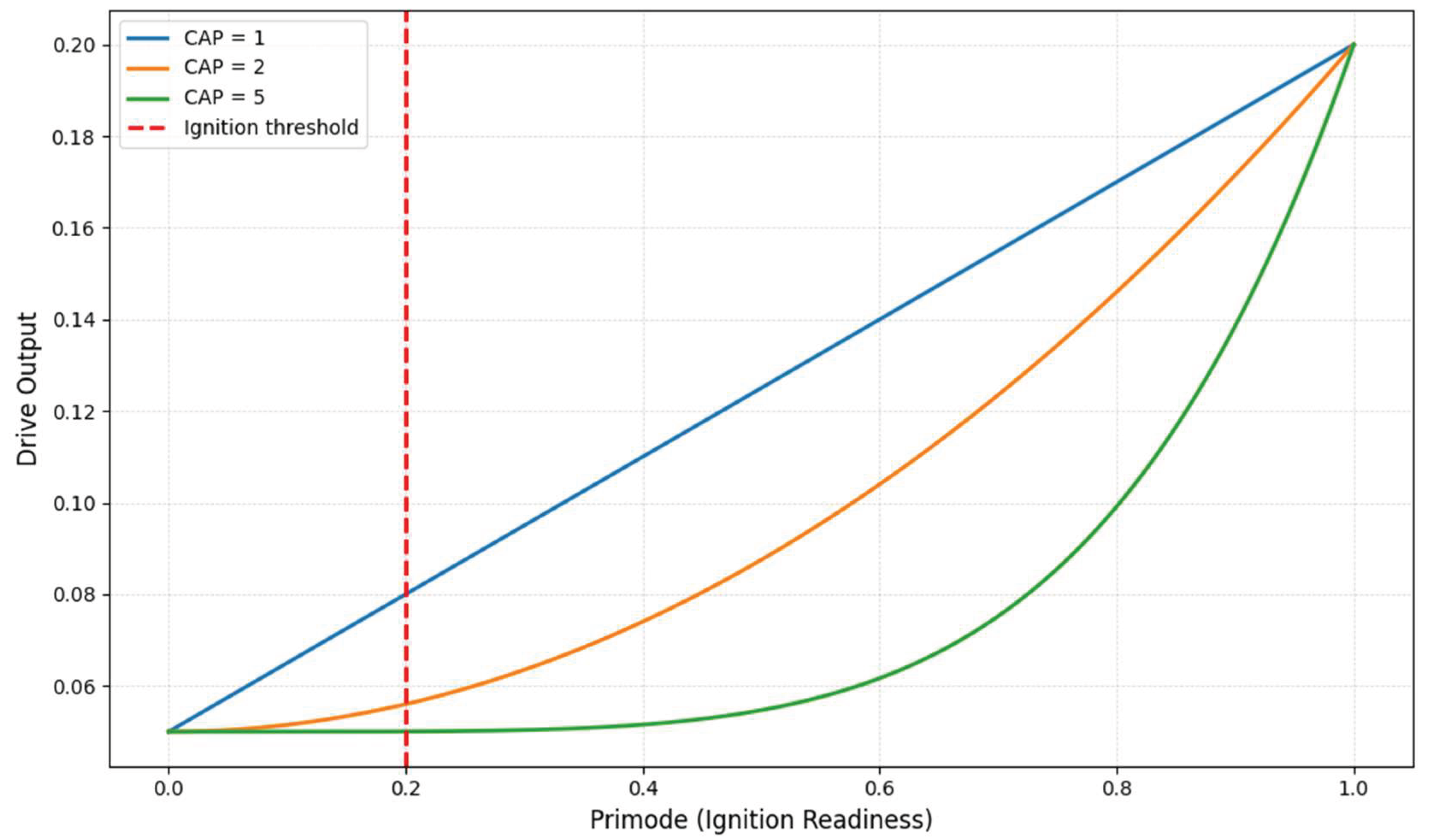
Figure 4.
Drive increases with CAP only when Primode is mid-range or higher, while near-zero Primode yields no activation regardless of CAP.
Figure 4.
Drive increases with CAP only when Primode is mid-range or higher, while near-zero Primode yields no activation regardless of CAP.
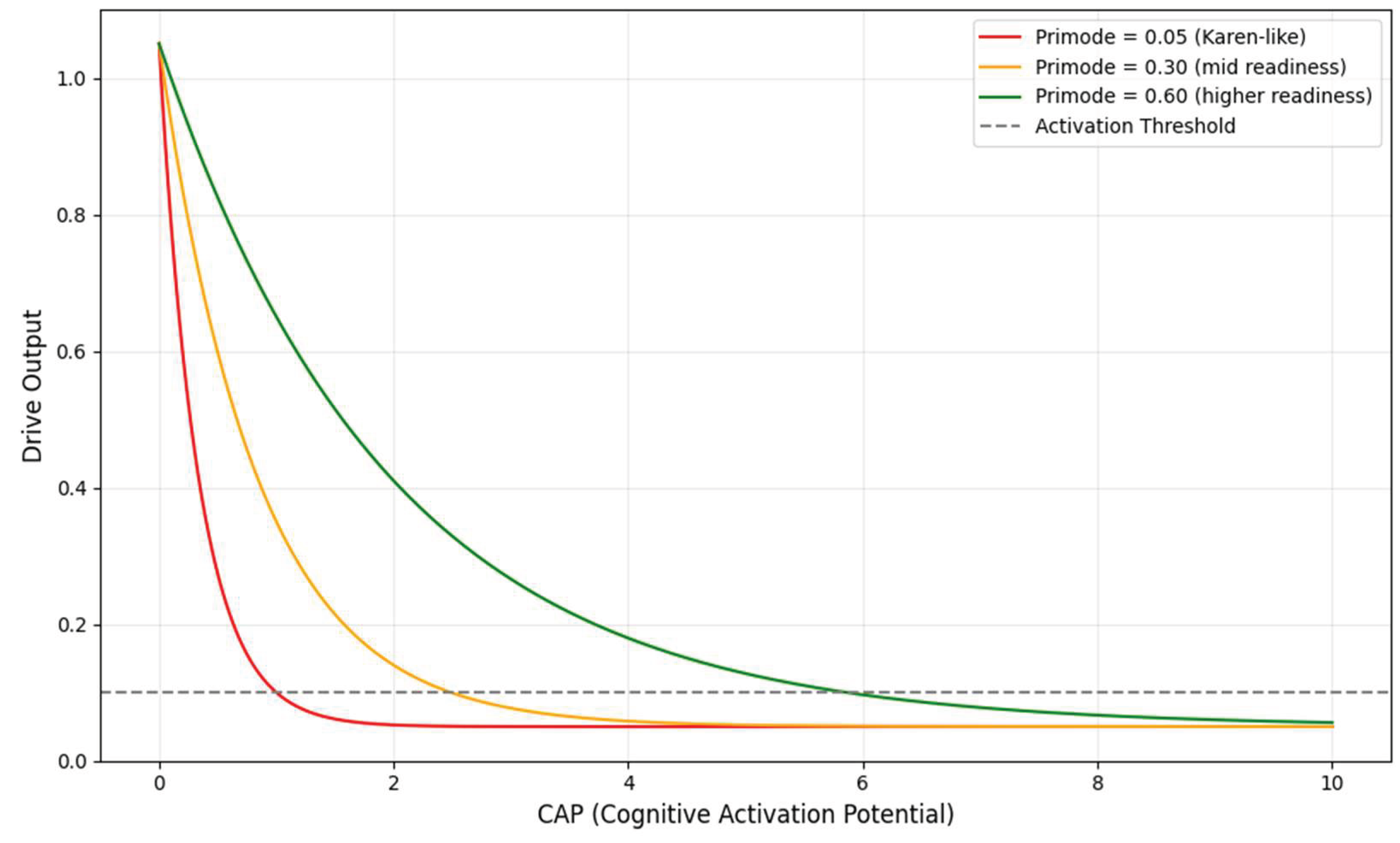
Figure 5.
Flexion heat map indicating Karen’s position in the lowest task-fit zone.
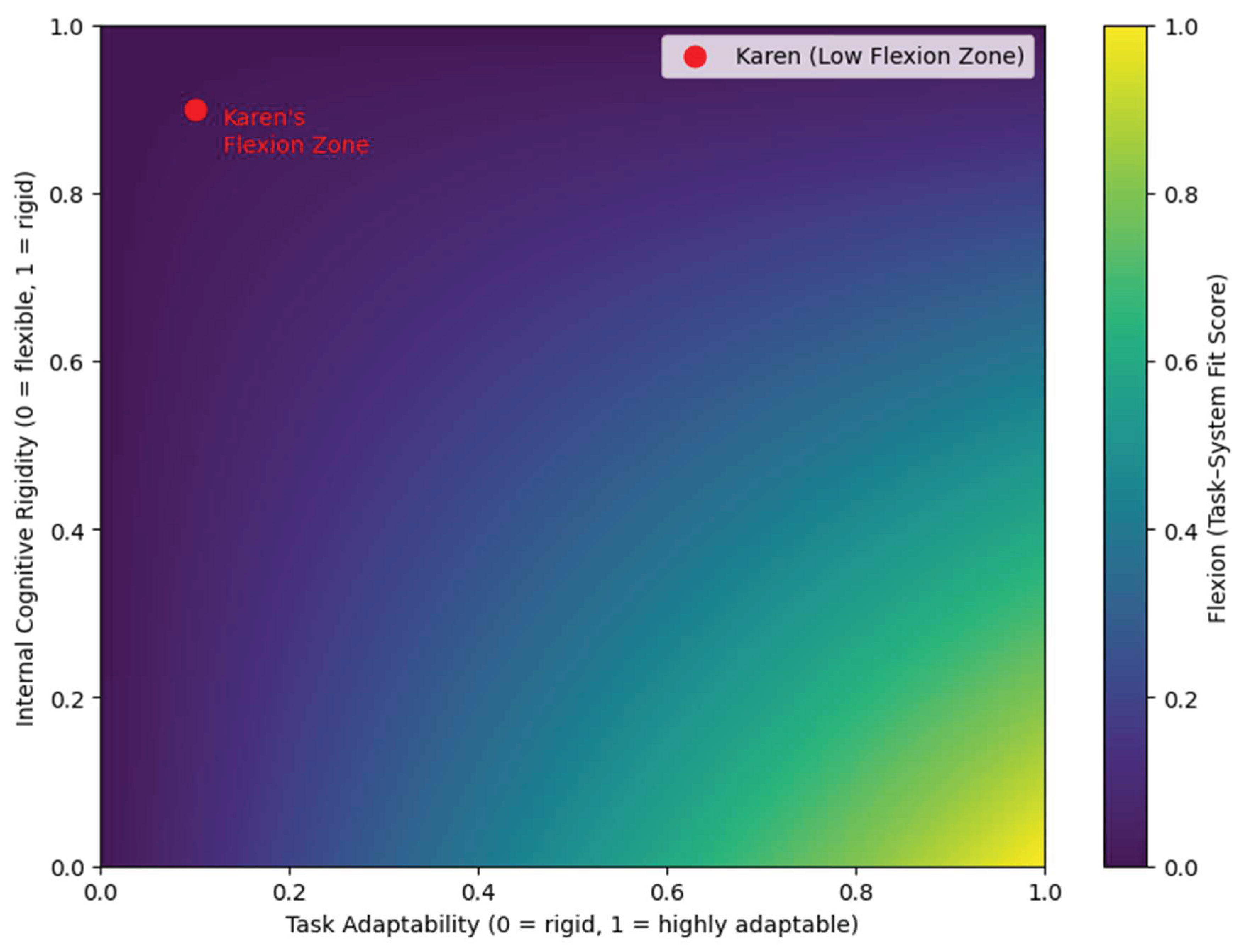
Figure 6.
Weak Anchory decays rapidly, while strong Anchory maintains task tethering over time.
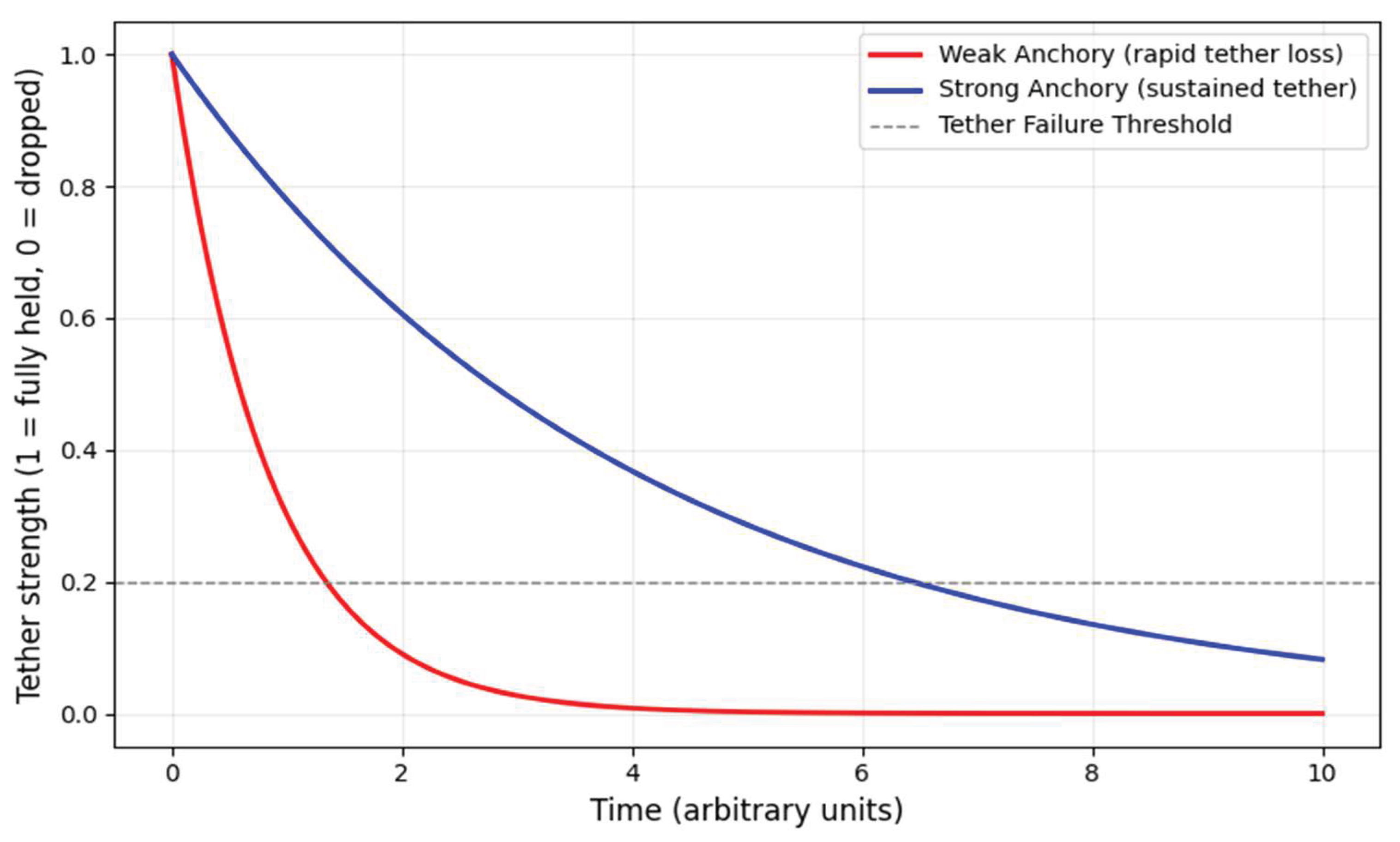
Figure 7.
Low Slip prevents Drive from reaching the activation threshold.
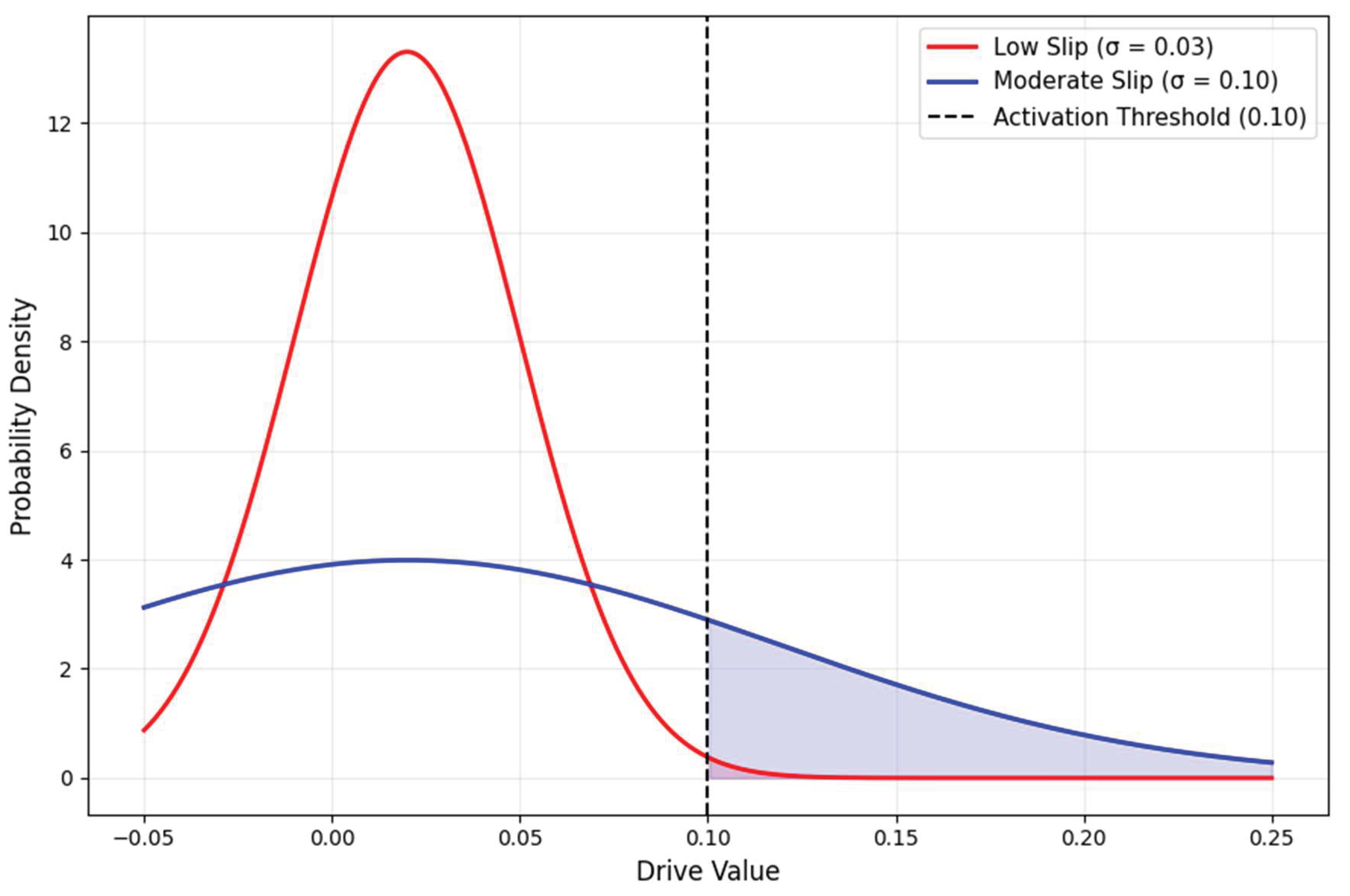

Table 1.
Summary of extracted case elements for CDA mapping.
| Domain | Extracted Elements (Hopko et al., 2011) |
| Behavioral Patterns | Long sleep duration, behavioral withdrawal, consistent inactivity |
| Values & Meaning | Identity collapsed into caregiving role; difficulty expressing non-caregiver goals |
| Compliance Indicators | Non-completion of activity logs; failure to initiate scheduled behaviors across sessions |
| Psychoeducation Engagement | Intellectual understanding of BA principles; lack of emotional integration; continued belief that mood must precede behavior |
| Psychosocial Context | Breast cancer diagnosis; caregiver strain; low environmental reinforcement; emotionally distant spousal relationship |
| Treatment Process | Twelve-session BA protocol completed; no observed activation or mood change throughout |
Table 2.
Existing tools suitable for estimating Lagun’s variables.
| CDA Variable | Reflects | Existing Measurement Approaches (MVA-Compatible) |
| Primode | Ignition readiness | Action-initiation latency tasks; voluntary response delays |
| CAP | Emotional activation potential | Affective-intensity scales; arousal indices; motivational state ratings |
| Flexion | Task–system fit | Task-fit questionnaires; cognitive load/effort scales; flow disruption measures |
| Anchory | Attention tether strength | Continuous Performance Test; fixation decay via eye-tracking; sustained attention metrics |
| Grain | Emotional/physical/contextual friction | Workload/friction indices; strain ratings; fatigue and burden metrics |
| Slip | Behavioral variability | Day-to-day performance variance; intraindividual RT spread; micro-fluctuation measures |
Table 3.
Structural Implications Linked to Lagun’s Variables.
| CDA Variable | Conceptual Treatment Implication |
| Primode | No activation occurs when ignition readiness is below the threshold. |
| CAP | Desire must generate sufficient voltage to overcome resistance. |
| Flexion | Tasks must be adaptable to a person’s cognitive architecture. |
| Anchory | Intentions need tether stability to persist across contexts. |
| Grain | High resistance must be reduced before scheduling tasks. |
| Slip | Variability allows accidental footholds; low Slip produces rigid nonresponse |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



