
Submitted:
08 December 2025
Posted:
09 December 2025
You are already at the latest version
Abstract
Background: Multimorbidity (the co-occurrence of two or more chronic conditions) is increasingly common among older adults and contributes to diminished well-being and greater healthcare use. While national data highlight regional variation, few studies have examined how multimorbidity is patterned within provinces like Saskatchewan or how it relates to access and acute care use.
Objective: To describe sociodemographic and geographic patterns of multimorbidity among older adults in Saskatchewan and examine its association with healthcare access, unmet needs, and recent emergency department (ED) visits and hospitalizations.
Methods: We conducted a secondary analysis of a population-based telephone survey of 1,093 adults aged 65+ across Saskatchewan. Respondents were categorized by chronic disease burden (none, one, or multimorbidity). Descriptive statistics and postal code–level mapping explored health status, access, and utilization.
Results: Multimorbidity (10.6%) was more prevalent among older adults aged 75+, Indigenous respondents, and those with lower education. It was associated with poorer self-rated health, greater unmet needs, and higher ED visits (20.7%) and hospitalizations (12.1%) compared to those without chronic conditions. Northern regions had proportionally higher multimorbidity, despite smaller populations.
Conclusions: Findings highlight social and spatial disparities in chronic disease burden and underscore the need for equity-focused strategies in Saskatchewan’s rural and northern communities.
Keywords:
multimorbidity
; older adults
; Saskatchewan
; hospitalization
; emergency room use
; health equity
; chronic disease
; regional variation
; rural health
; aging population
Introduction
Multimorbidity (commonly defined as the co-occurrence of two or more chronic conditions) is fast becoming a growing public health concern among older adults in Canada, with prevalence estimates exceeding 60% in seniors [1,2,3]. Unlike comorbidity, which denotes secondary conditions tied to a primary illness, multimorbidity captures the interwoven complexity of multiple chronic diseases that jointly impair functional ability, increase care needs, and erode quality of life [4,5]. Among older adults, this pattern is becoming increasingly normative.In Canada, the most prevalent multimorbidity combination among adults aged 45 and older is osteoarthritis and hypertension [6,7]. As Geda et al. (2021) notes, risk increases with age, female sex, retirement status, poor self-rated health, abnormal BMI, and sleep disturbances [6,7]. Socioeconomic disparities further influence risk: lower household income, material deprivation, and lower educational attainment are associated with higher multimorbidity prevalence and more frequent healthcare utilization [8,9,10,11].
Geographically, patterns of multimorbidity show significant regional and urban-rural variation in Canada, though findings differ by measurement approach and population studied. Some evidence suggests higher multimorbidity prevalence in urban cores compared to peripheral or rural communities, while other studies show mixed results, with rurality associated with both increased and decreased multimorbidity depending on context [12,13]. With regards to provincial variation, residents of Atlantic Canada, Ontario, and Quebec have shown increased odds of certain multimorbidity patterns (specifically osteoarthritis-hypertension), though at least one study found multimorbidity to be less likely among Quebec residents when examining overall multimorbidity prevalence [7,14]. However, area-level material deprivation consistently shows stronger associations with multimorbidity than geography alone, and multimorbidity rates in Ontario increased with material deprivation even after accounting for geographic variation [12,15,16].
Saskatchewan–a geographically diverse province with pronounced rural and Indigenous populations–has received relatively little focused attention in multimorbidity research specifically, despite its unique demographic characteristics [17,18]. Health system utilization varies by geography with rural residents showing higher emergency department use, while hospitalization rates are more strongly influenced by area-level deprivation than by rurality per se [19,20,21]. In Saskatchewan, provincial estimates suggest that 1 in 4 adults over age 65 live with three or more chronic conditions [22,23,24]. However, few studies have examined how this burden is distributed regionally or how it maps onto patterns of healthcare utilization especially in relation to hospitalizations and emergency room visits. A clearer understanding of intra-provincial disparities in multimorbidity can support more equitable health system responses, including improved chronic disease management, enhanced integration of services, and place-based resource allocation, which is why this study aims to: 1) describe the demographic and geographic distribution of multimorbidity among community-dwelling older adults in Saskatchewan; and 2) examine the association between chronic disease burden and self-reported acute care use (emergency department visits and hospitalizations). In visualizing and mapping out these patterns, we aim to inform more responsive and equitable approaches to aging, care delivery, and system planning in Saskatchewan and similar jurisdictions.
Methods
Study Design and Data Source
This study is a secondary analysis of data from a province-wide telephone survey conducted in Saskatchewan, Canada, between April 25, 2018, and April 14 2019, The survey captured sociodemographic, health status, and service use data from community-dwelling adults aged 65 years and older residing across both rural and urban regions of the province.
In this analysis, we aimed to (a) examine patterns of multimorbidity among older adults by chronic disease burden, and (b) describe geographic variation in multimorbidity and recent acute care use using postal code-based regional mapping. Sampling and data collection were supported by the Canadian Hub for Applied and Social Research (CHASR) at the University of Saskatchewan.
Ethical Approval
The study received ethics approval from the University of Saskatchewan Research Ethics Board (Beh 18-67). All participants provided verbal informed consent before participating, in accordance with the Declaration of Helsinki.
Sampling Strategy and Recruitment
We had calculated a priori a sample size of 1,000. To achieve this target sample size, 35,393 telephone numbers were randomly selected and dialed, based on landline and mobile distributions reflective of Saskatchewan households (with 25.8% mobile numbers to mirror mobile-only residences). Numbers were obtained from a third-party vendor, consistent with distribution recommendations in the Canadian Radio-television and Telecommunications Commission (CRTC)’s Communications Monitoring Report. Up to five call attempts were made per number. Interviews were conducted across three waves using WinCATI 6.0 and survey software Sensus 6.0.
Survey Instruments
Two instruments were administered during the telephone interviews:
- The Patient Action Inventory for Self-Care: this is a validated tool assessing 57 self-care behaviors across 11 domains (e.g., medication use, physical activity, emotional regulation) using dichotomous (yes/no) responses. It measures perceived importance, willingness, and ability to perform each behavior. This tool has demonstrated strong reliability and construct validity in older adult populations [25,26].
- A tailored health assessment questionnaire: adapted from a similar study conducted in the U.S. and modified for Saskatchewan’s healthcare context [27,28]. This instrument captured participant demographics (e.g., age, sex, ethnicity, education level, first three digits of postal code, immigration status), as well as health indicators including self-rated health, access to care, healthcare service utilization, transportation availability, and presence of chronic conditions.
This current analysis, however, focused exclusively on variables drawn from the health assessment questionnaire.
Key Variables and Outcome Measures
Chronic condition status was self-reported by participants and used to categorize respondents into three mutually exclusive groups: a) no chronic condition; b) one chronic condition; and c) two or more chronic conditions (i.e., multimorbidity).Chronic conditions captured included common diagnoses such as asthma, COPD, coronary artery disease, depression, diabetes, and heart failure.
Key outcome variables included: a) access to healthcare services; b) transportation availability; c) self-rated quality of life and health domains (physical, mental, emotional, spiritual); d) emergency room visits and hospitalizations within the past three months; and e) unmet healthcare needs
Postal codes were used to map participants’ geographic location by Forward Sortation Area (FSA) for spatial analysis.
Data Analysis
Descriptive statistics (frequencies, percentages, means) were calculated for all sociodemographic and health-related variables, stratified by chronic disease status. Bivariate comparisons were conducted across the three morbidity groups to examine differences in healthcare access, self-rated health domains, and service utilization.
All analyses were performed using IBM SPSS Statistics version 28.0 (IBM Corp., Armonk, NY). Statistical significance was set at p < 0.05. Pairwise deletion was applied to handle missing data.
Results
Sample Characteristics
A total of 1,093 community-dwelling older adults in Saskatchewan participated in the study (Table 1). Among them, 673 (61.6%) reported no chronic conditions, 304 (27.8%) had one chronic condition, and 116 (10.6%) had multimorbidity (defined as two or more chronic conditions). The majority of respondents were aged 65–74 years (58.7%) and female (71.3%). Most participants identified as White (89.4%), while 6.0% identified as Indigenous. About 30.1% had completed a bachelor’s degree or higher, while one in five had no formal post-secondary education. Individuals with multimorbidity were more likely to report lower educational attainment and income levels. See Table 1 for more description.
Prevalence and Patterning of Multimorbidity
As shown in Table 2, multimorbidity was more common among older participants (≥75 years), Indigenous respondents, and those with lower education. Among those with multimorbidity, the most frequently reported conditions included diabetes (54.3%), depression (76.7%), coronary artery disease (43.1%), heart failure (29.3%), asthma (32.8%), and COPD (32.8%). These often co-occurred in complex combinations, reflecting high-care needs. See Table 2 for more description.
Quality of Life and Self-Perceived Health
Table 3 illustrates a strong gradient between chronic disease burden and perceived health. Respondents with no chronic conditions reported high satisfaction with physical (92.4%), mental (83.7%), and emotional (94.9%) health. By contrast, among those with multimorbidity, satisfaction dropped to 78.4% (physical), 56.9% (mental), and 82.8% (emotional), with a higher proportion expressing dissatisfaction, particularly with mental health (41.4%). See Table 3 for more description
Access to Care and Unmet Needs
Most participants reported access to healthcare and transportation when needed, but disparities were evident by disease burden (Table 3). Only 46.6% of those with multimorbidity had access to all needed health services, compared to 54.5% in those without chronic conditions. Unmet healthcare needs were more than double in the multimorbidity group (10.3%) vs. the no-condition group (3.9%).
Acute Care Utilization
As shown in Table 4, recent ER visits and hospitalizations were substantially more common in those with multimorbidity. About 20.7% reported an ER visit in the past three months, and 12.1% reported hospitalization, compared to 7.6% and 4.0%, respectively, among those without chronic conditions.
Geographic Variation in Multimorbidity
Regional mapping of multimorbidity patterns revealed striking geographic disparities (Figure 1). Although northern Saskatchewan accounted for a smaller share of total respondents (Panel D), it had a disproportionately high percentage of older adults with multimorbidity (Panel C). Conversely, southern and central regions showed higher proportions of older adults with no chronic conditions (Panel A). These patterns highlight potential structural inequities in chronic disease prevention and access to care.
Discussion
This study offers one of the first regionally detailed, population-based snapshots of multimorbidity among older adults in Saskatchewan. While the overall prevalence of multimorbidity (10.6%) in our sample appears lower than national estimates, (which often exceed 60% in seniors depending on definitions and data sources) [29,30,31], the stratified patterns and spatial variations observed reflect deeper structural and health system realities within Saskatchewan. Rather than simply quantifying multimorbidity burden, our findings illuminate how that burden is unevenly distributed across sociodemographic and geographic lines, with implications for care access, quality of life, and acute care reliance.
Consistent with the broader Canadian literature, older age, lower education, and Indigenous identity were associated with higher multimorbidity in our sample. These trends align with existing research showing that social and structural determinants (such as colonial legacies, cumulative disadvantage, and differential exposure to environmental stressors) shape chronic disease trajectories across the life course [12,14,16,29,32,33,34]. The relatively high proportion of Indigenous respondents reporting multimorbidity, while based on small numbers, echoes national disparities and underscores the need for Indigenous-governed, culturally safe models of chronic care and prevention [23,34,35]. Of note, our ongoing work co-developing a deprivation index with relevant stakeholders and rightsholders for Saskatchewan, drawing on census-linked material and social indicators, may offer future opportunities to more precisely quantify how area-level disadvantage intersects with individual-level chronic disease burden, especially in northern and rural regions.
A steep gradient in self-perceived health across morbidity strata is evident in our data. Compared to those without chronic conditions, individuals with multimorbidity reported significantly lower satisfaction across physical, mental, emotional, and spiritual domains. These findings are consistent with Canadian studies linking multimorbidity to diminished life satisfaction, functional impairment, and lower health confidence [5,11]. However, what often remains less visible is the compounding role of emotional and spiritual health dimensions frequently undervalued in standard measures yet clearly salient among older adults navigating complex care needs. This speaks to the importance of broadening how health systems define and respond to multimorbidity, not merely as a tally of conditions, but as an embodied experience that disrupts wellbeing across multiple dimensions [23,35].
Despite overall high reported access to healthcare, respondents with multimorbidity were notably less likely to have access to all needed services and more likely to report unmet needs. While this finding is not new, it remains unresolved. Previous work shows that people with multiple chronic conditions often face fragmented care, overlapping appointments, contradictory treatment plans, and long wait times, especially when care systems remain oriented around single-disease pathways [18,36,37,38]. In Saskatchewan, where vast distances, primary care shortages, and limited specialist availability converge, these gaps are not merely administrative–they are structural [39,40]. Interestingly, even basic enablers such as transportation access (reported as near-universal across groups) may obscure qualitative differences in reliability, affordability, or cultural appropriateness. Future directions of this work would disaggregate these dimensions further, particularly in under-served regions.
Our finding that one in five older adults with multimorbidity reported an emergency department visit in the past three months is striking, and consistent with literature showing higher ED and hospitalization rates among this population [19,41,42,43,44]. These visits may be appropriate in some cases, but they often reflect system failures upstream: lack of timely primary care, inadequate medication management, or caregiver burnout [41,43]. Rather than framing these individuals as “high users,” we should consider the context in which acute care becomes the default. In rural and northern communities, where after-hours care or walk-in clinics are limited or absent, the ED may be the only consistent point of contact with the health system [8,17,44,45]. These findings suggest an opportunity for Saskatchewan to strengthen community-based, integrated care models–tailored not just to disease type, but to geography, culture, and capacity.
Our maps reveal a nuanced but important pattern: while the absolute number of older adults with multimorbidity is highest in more populated southern regions, the proportional burden is greatest in the north. This divergence between volume and vulnerability should be central to health system planning. Resource allocation based solely on headcounts risks under-serving high-need but sparsely populated regions. When paired with deprivation metrics and local knowledge, spatial analyses like ours can guide the development of more place-based, equity-sensitive strategies. The province’s new commitments to primary care reform and team-based care models must be informed by such insights if they are to be effective for older adults with complex health needs [39].
Strengths and Limitations
Our study adds important detail to the relatively underexplored landscape of multimorbidity in Saskatchewan. Its strengths include: a) a large, population-based sample capturing rural, urban, and northern voices; b) the use of stratified analysis and mapping to expose patterns often masked in aggregate data; and c) relevance for aging and health equity policy agendas across Canada’s diverse jurisdictions.
However, several limitations warrant attention. As a cross-sectional survey, the data do not capture changes over time. Secondly, all information was self-reported, raising the possibility of recall bias or underreporting. Additionally, the list of chronic conditions may not reflect the full spectrum of multimorbidity, especially neurological, musculoskeletal, or culturally-specific diagnoses. Also, the number of small cell sizes in some geographic regions limit generalizability. Finally, functional limitations, disease severity, or medication burden were not assessed.
Future Directions and Implications
Findings from this study highlight that the geography of aging is not neutral: place, power, and policy matter. Addressing multimorbidity in older adults (particularly those in northern, rural, or equity-deserving contexts) requires moving beyond reactive care toward longitudinal, integrated, and relationship-based approaches that centre the full spectrum of what it means to age well.
Our future research would consider linking self-reported data to administrative records to better understand care pathways and service utilization over time. We are working with and engaging older adults, including Indigenous communities in a qualitative study to shed light on lived experiences, resilience strategies, and culturally grounded approaches to wellness.
This work has also planted seeds to co-create a provincial deprivation index, combining these indicators with multimorbidity data to strengthen its predictive utility and support resource prioritization. We intend to use this to evaluate the uptake and outcomes of emerging rural chronic care models, home-based supports, and Indigenous-led health initiatives.
Conclusion
This study provides one of the first province-wide descriptive analyses of multimorbidity among older adults in Saskatchewan, revealing how the burden of chronic conditions is socially and geographically patterned. While most older adults reported good health and access to care, those living with multimorbidity (particularly in northern and socioeconomically marginalized communities) faced notable disparities in wellbeing, service access, and reliance on acute care. Our findings affirm that multimorbidity is not evenly distributed, and that structural and spatial inequities shape both experience and outcome. By integrating self-reported data with geospatial analysis, this study underscores the need for health planning that goes beyond population counts to consider proportional burden, regional vulnerability, and lived experience. These insights can inform more responsive, integrated, and equity-oriented approaches to aging and chronic disease management across Saskatchewan and similar jurisdictions.
Author Contributions
Conceptualization, Udoka Okpalauwaekwe and Huey-Ming Tzeng; Methodology, Udoka Okpalauwaekwe; Software, Rana Masud; Validation, Udoka Okpalauwaekwe and Huey-Ming Tzeng; Formal analysis, Udoka Okpalauwaekwe and Rana Masud; Investigation, Udoka Okpalauwaekwe and Huey-Ming Tzeng; Resources, Udoka Okpalauwaekwe and Huey-Ming Tzeng; Data curation, Udoka Okpalauwaekwe; Writing – original draft, Udoka Okpalauwaekwe; Writing – review & editing, Udoka Okpalauwaekwe and Huey-Ming Tzeng; Visualization, Udoka Okpalauwaekwe; Supervision, Udoka Okpalauwaekwe and Huey-Ming Tzeng; Project administration, Udoka Okpalauwaekwe; Funding acquisition, Huey-Ming Tzeng.
Funding
Not applicable.
Institutional Review Board Statement
The study received ethics approval from the University of Saskatchewan Research Ethics Board (Beh 18-67).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest Statement: The authors have declared no conflict of interest.
References
- Canadian Institute for Health Information (CIHI). Seniors and aging dashboard. 2025. Available online: https://www.cihi.ca/en/dashboards/seniors-and-aging.
- Fortin, M. Multimorbidity and quality of life: a closer look. Health Qual Life Outcomes 2007, 5, 52. [Google Scholar] [CrossRef]
- Nicholson, K. The co-occurrence of multimorbidity and polypharmacy among middle-aged and older adults in Canada: A cross-sectional study using the Canadian Longitudinal Study on Aging (CLSA) and the Canadian Primary Care Sentinel Surveillance Network (CPCSSN). PLoS One 2025, 20, e0312873. [Google Scholar] [CrossRef]
- Geda, N.R.; Janzen, B.; Pahwa, P. Chronic disease multimorbidity among the Canadian population: prevalence and associated lifestyle factors. Arch Public Health 2021, 79, 60. [Google Scholar] [PubMed]
- Johnston, M.C. Defining and measuring multimorbidity: a systematic review of systematic reviews. Eur J Public Health 2019, 29, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Griffith, L.E. Multimorbidity Frameworks Impact Prevalence and Relationships with Patient-Important Outcomes. J Am Geriatr Soc 2019, 67, 1632–1640. [Google Scholar]
- Mortey, O. Prevalence and risk factors of the most common multimorbidity among Canadian adults. PLoS One 2025, 20, e0317688. [Google Scholar]
- Bai, Y.; Stranges, S.; Sarma, S. Investigation of rural-urban differences in hospitalization for ambulatory care-sensitive conditions: Analysis of linked survey, hospitalization, and tax data from Canada. J Rural Health 2025, 41, e70010. [Google Scholar] [CrossRef] [PubMed]
- Dugravot, A. Social inequalities in multimorbidity, frailty, disability, and transitions to mortality: a 24-year follow-up of the Whitehall II cohort study. Lancet Public Health 2020, 5, e42–e50. [Google Scholar] [CrossRef]
- Sibley, L.M.; Weiner, J.P. An evaluation of access to health care services along the rural-urban continuum in Canada. BMC Health Serv Res 2011, 11, 20. [Google Scholar] [CrossRef]
- Johnston, K.J.; Wen, H. K.E. Joynt Maddox, Lack Of Access To Specialists Associated With Mortality And Preventable Hospitalizations Of Rural Medicare Beneficiaries. Health Aff (Millwood) 2019, 38, 1993–2002. [Google Scholar]
- Ingram, E. Household and area-level social determinants of multimorbidity: a systematic review. J Epidemiol Community Health 2021, 75, 232–241. [Google Scholar] [CrossRef]
- Zheng, C. The impact of place on multimorbidity: A systematic scoping review. Soc Sci Med 2024, 361, 117379. [Google Scholar] [CrossRef]
- Xiao, X.; Beach, J.; Senthilselvan, A. Prevalence and determinants of multimorbidity in the Canadian population. PLoS One 2024, 19, e0297221. [Google Scholar] [CrossRef]
- Kone, A.P. Rising burden of multimorbidity and related socio-demographic factors: a repeated cross-sectional study of Ontarians. Can J Public Health 2021, 112, 737–747. [Google Scholar] [CrossRef]
- Ryan, B.L. Beyond the grey tsunami: a cross-sectional population-based study of multimorbidity in Ontario. Can J Public Health 2018, 109, 845–854. [Google Scholar] [CrossRef]
- Wilk, P. Geographic variation in preventable hospitalisations across Canada: a cross-sectional study. BMJ Open 2020, 10, e037195. [Google Scholar] [CrossRef]
- Martin, D. Canada’s universal health-care system: achieving its potential. Lancet 2018, 391, 1718–1735. [Google Scholar] [CrossRef]
- Fisher, K.A. Effect of socio-demographic and health factors on the association between multimorbidity and acute care service use: population-based survey linked to health administrative data. BMC Health Serv Res 2021, 21, 62. [Google Scholar] [CrossRef]
- Janzen, B. Exploring diversity in socioeconomic inequalities in health among rural dwelling Canadians. J Rural Health 2015, 31, 186–198. [Google Scholar]
- Stewart, M.; Ryan, B. Ecology of health care in Canada. Can Fam Physician 2015, 61, 449–453. [Google Scholar]
- Alonzo, R. Association between physical activity and life satisfaction among adults with multimorbidity in Canada. Can J Public Health 2022, 113, 598–606. [Google Scholar] [CrossRef]
- Josewski, V.; de Leeuw, S.; Greenwood, M. Grounding Wellness: Coloniality, Placeism, Land, and a Critique of “Social” Determinants of Indigenous Mental Health in the Canadian Context. Int J Environ Res Public Health 2023, 20. [Google Scholar] [CrossRef]
- Yang, G.; Arcy, C. D. Physical activity and social support mediate the relationship between chronic diseases and positive mental health in a national sample of community-dwelling Canadians 65+: A structural equation analysis. J Affect Disord 2022, 298, 142–150. [Google Scholar] [CrossRef]
- Tzeng, H.M.; Pierson, J. Marcus. Measuring patient engagement: which healthcare engagement behaviours are important to patients? J Adv Nurs 2017, 73, 1604–1609. [Google Scholar] [CrossRef]
- Tzeng, H.M.; Pierson, J.M. What are the highly important and desirable patient engagement actions for self-care as perceived by individuals living in the southern United States? Patient Prefer Adherence 2017, 11, 181–191. [Google Scholar] [CrossRef]
- Tzeng, H.M.; Okpalauwaekwe, U.; Yin, C.Y. Older adults’ suggestions to engage other older adults in health and healthcare: a qualitative study conducted in western Canada. Patient Prefer Adherence 2019, 13, 331–337. [Google Scholar]
- Tzeng, H.M. Do patients’ demographic characteristics affect their perceptions of self-care actions to find safe and decent care? Appl Nurs Res 2018, 43, 24–29. [Google Scholar] [CrossRef]
- Im, J.H.B. Examining the prevalence and correlates of multimorbidity among community-dwelling older adults: cross-sectional evidence from the Canadian Longitudinal Study on Aging (CLSA) first-follow-up data. Age Ageing 2022, 51. [Google Scholar] [CrossRef]
- Nicholson, K. Examining early and late onset of multimorbidity in the Canadian Longitudinal Study on Aging. J Am Geriatr Soc 2021, 69, 1579–1591. [Google Scholar] [CrossRef]
- Salive, M.E. Multimorbidity in older adults. Epidemiol Rev 2013, 35, 75–83. [Google Scholar] [CrossRef]
- Ferris, J.K. Trends and inequalities in multimorbidity from 2001/2002 to 2019/2020: A population-based study in British Columbia. Health Rep 2025, 36, 3–16. [Google Scholar]
- Ketter, N.I. Describing the Profile of Individuals at Heightened Risk for Cardiometabolic Multimorbidity: A Secondary Analysis of the Canadian Longitudinal Study on Aging Data. Am J Health Promot 2025, 8901171251374738. [Google Scholar] [CrossRef]
- Shahunja, K.M. Multimorbidity among the Indigenous population: A systematic review and meta-analysis. Ann Epidemiol 2024, 98, 8–17. [Google Scholar] [CrossRef]
- Okpalauwaekwe, U. Enhancing health and wellness by, for and with Indigenous youth in Canada: a scoping review. BMC Public Health 2022, 22, 1630. [Google Scholar] [CrossRef]
- Ali, S.; Stranges, S.; Le, B. Social and health determinants of wait times for primary care in Canada. Can Fam Physician 2025, 71, 646–655. [Google Scholar]
- Bierman, A.S. Preventing and managing multimorbidity by integrating behavioral health and primary care. Health Psychol 2019, 38, 851–854. [Google Scholar] [CrossRef]
- Ho, J.W.; Kuluski, K.; Im, J. “It’s a fight to get anything you need” - Accessing care in the community from the perspectives of people with multimorbidity. Health Expect 2017, 20, 1311–1319. [Google Scholar] [CrossRef]
- Okpalauwaekwe, U. Facilitators, barriers, and priorities for enhancing primary care recruitment and retention in Saskatchewan, Canada. BMC Prim Care 2025, 26, 373. [Google Scholar] [CrossRef]
- Shah, T.I.; Milosavljevic, S.; Bath, B. Determining geographic accessibility of family physician and nurse practitioner services in relation to the distribution of seniors within two Canadian Prairie Provinces. Soc Sci Med 2017, 194, 96–104. [Google Scholar] [CrossRef]
- Ahn, S. Emergency department and inpatient utilization among U.S. older adults with multiple chronic conditions: a post-reform update. BMC Health Serv Res 2020, 20, 77. [Google Scholar] [CrossRef]
- Naseer, M. Individual and contextual predictors of emergency department visits among community-living older adults: a register-based prospective cohort study. BMJ Open 2022, 12, e055484. [Google Scholar] [CrossRef]
- Rodrigues, L.P. Association between multimorbidity and hospitalization in older adults: systematic review and meta-analysis. Age Ageing 2022, 51. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, L.P. Multimorbidity patterns and hospitalisation occurrence in adults and older adults aged 50 years or over. Sci Rep 2022, 12, 11643. [Google Scholar] [CrossRef] [PubMed]
- Pong, R.W. Patterns of health services utilization in rural Canada. Chronic Dis Inj Can 2011, 31, 1–36. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Regional distribution of self-reported health outcomes among older adults across Forward Sortation Areas (FSAs) in Saskatchewan.
Figure 1.
Regional distribution of self-reported health outcomes among older adults across Forward Sortation Areas (FSAs) in Saskatchewan.
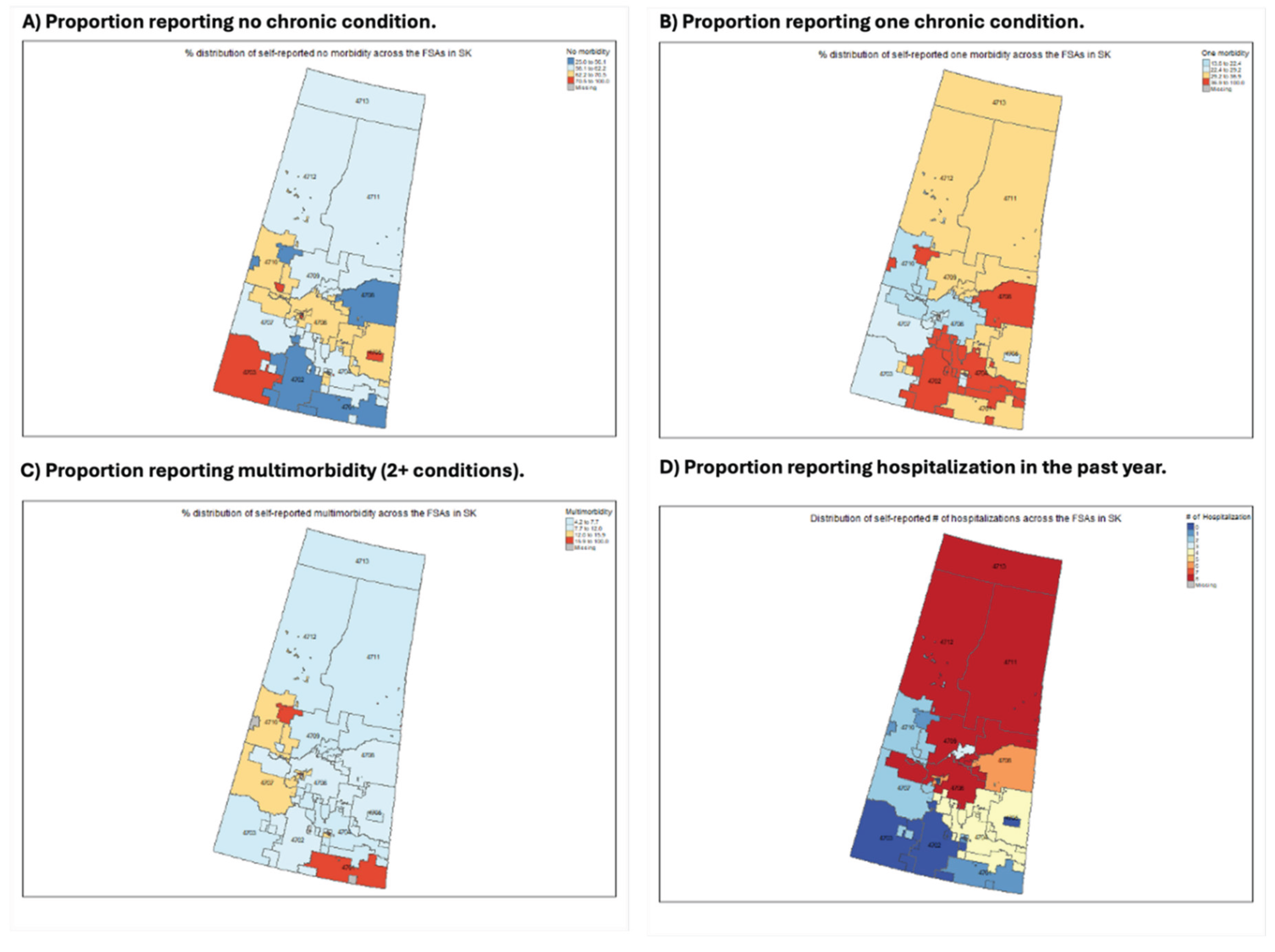

Table 1.
Sociodemographic Characteristics of Older Adults Stratified by Chronic Disease Status.
| Characteristic | Total (N = 1,093) | No Chronic Condition (N = 673) | 1 Chronic Condition (N = 304) | 2+ Chronic Conditions (N = 116) |
| Age (years) | ||||
| 65–74 | 642 (58.7%) | 409 (60.8%) | 163 (53.6%) | 70 (60.3%) |
| 75–84 | 345 (31.6%) | 201 (29.9%) | 107 (35.2%) | 37 (31.9%) |
| 85+ | 99 (9.1%) | 58 (8.6%) | 32 (10.5%) | 9 (7.8%) |
| Missing | 7 (0.6%) | 5 (0.7%) | 2 (0.7%) | 0 (0.0%) |
| Gender | ||||
| Female | 779 (71.3%) | 488 (72.5%) | 209 (68.8%) | 82 (70.7%) |
| Male | 314 (28.7%) | 185 (27.5%) | 95 (31.2%) | 34 (29.3%) |
| Ethnicity | ||||
| White | 977 (89.4%) | 611 (90.8%) | 267 (87.8%) | 99 (85.3%) |
| Indigenous | 66 (6.0%) | 31 (4.6%) | 22 (7.2%) | 13 (11.2%) |
| Asian | 6 (0.5%) | 3 (0.4%) | 2 (0.7%) | 1 (0.9%) |
| Black | 1 (0.1%) | 1 (0.1%) | 0 (0.0%) | 0 (0.0%) |
| Other | 43 (3.9%) | 27 (4.0%) | 13 (4.3%) | 3 (2.6%) |
| Highest Education Completed | ||||
| Bachelor’s degree or higher | 329 (30.1%) | 229 (34.0%) | 75 (24.7%) | 25 (21.6%) |
| Associate/diploma | 251 (23.0%) | 150 (22.3%) | 69 (22.7%) | 32 (27.6%) |
| High school | 308 (28.2%) | 172 (25.6%) | 95 (31.2%) | 41 (35.3%) |
| Some education | 124 (11.3%) | 74 (11.0%) | 37 (12.2%) | 13 (11.2%) |
| Other | 69 (6.3%) | 38 (5.6%) | 26 (8.6%) | 5 (4.3%) |
| Missing | 12 (1.1%) | 10 (1.5%) | 2 (0.7%) | 0 (0.0%) |
| Language | ||||
| English as first language | 950 (86.9%) | 586 (87.1%) | 261 (85.9%) | 103 (88.8%) |
| Not English | 139 (12.7%) | 83 (12.3%) | 43 (14.1%) | 13 (11.2%) |
| Missing | 4 (0.4%) | 4 (0.6%) | 0 (0.0%) | 0 (0.0%) |
Key: Descriptive characteristics of older adults aged 65+ in Saskatchewan, stratified by the number of self-reported chronic conditions. Multimorbidity was defined as 2 or more chronic conditions. Note: Values are presented as count (percentage). Percentages may not total 100% due to rounding. “Missing” reflects unreported responses or ‘prefer not to say’.
Table 2.
Prevalence of Selected Chronic Conditions Among Older Adults by Morbidity Group.
| Chronic Condition | Total (N = 1,093) | No Chronic Condition (N = 673) | 1 Chronic Condition (N = 304) | 2+ Chronic Conditions (N = 116) |
| Asthma | 90 (8.2%) | 0 (0.0%) | 52 (17.1%) | 38 (32.8%) |
| Chronic Obstructive Pulmonary Disease (COPD) | 51 (4.7%) | 0 (0.0%) | 13 (4.3%) | 38 (32.8%) |
| Coronary Artery Disease (CAD) | 77 (7.0%) | 0 (0.0%) | 27 (8.9%) | 50 (43.1%) |
| Depression | 145 (13.3%) | 0 (0.0%) | 56 (18.4%) | 89 (76.7%) |
| Diabetes | 102 (9.3%) | 0 (0.0%) | 39 (12.8%) | 63 (54.3%) |
| Heart Failure | 38 (3.5%) | 0 (0.0%) | 4 (1.3%) | 34 (29.3%) |
Key: Self-reported prevalence of six common chronic conditions across older adult respondents in Saskatchewan, stratified by number of chronic diseases. Note: Participants in the “No chronic condition” group reported none of the listed conditions. Percentages are based on column totals. Some participants with 1+ chronic conditions may have reported conditions outside these six. Percentages may not total 100% within rows due to rounding.
Table 3.
Healthcare Access and Quality of Life Indicators Among Older Adults, Stratified by Chronic Disease Status.
Table 3.
Healthcare Access and Quality of Life Indicators Among Older Adults, Stratified by Chronic Disease Status.
| Variable | Total (N = 1,093) | No Chronic Condition (N = 673) | 1 Chronic Condition (N = 304) | 2+ Chronic Conditions (N = 116) |
| Access to healthcare when needed | ||||
| Yes (all services) | 572 (52.3%) | 367 (54.5%) | 151 (49.7%) | 54 (46.6%) |
| Yes (some services) | 410 (37.5%) | 242 (36.0%) | 123 (40.5%) | 45 (38.8%) |
| No | 64 (5.9%) | 39 (5.8%) | 16 (5.3%) | 9 (7.8%) |
| Missing | 47 (4.3%) | 25 (3.7%) | 14 (4.6%) | 8 (6.9%) |
| Transportation available when needed | ||||
| Yes | 1,050 (96.1%) | 645 (95.8%) | 294 (96.7%) | 111 (95.7%) |
| No | 32 (2.9%) | 19 (2.8%) | 9 (3.0%) | 4 (3.4%) |
| Missing | 11 (1.0%) | 9 (1.3%) | 1 (0.3%) | 1 (0.9%) |
| Able to meet healthcare needs (past 3 months) | ||||
| Yes | 1,030 (94.2%) | 641 (95.2%) | 285 (93.8%) | 104 (89.7%) |
| No | 56 (5.1%) | 26 (3.9%) | 18 (5.9%) | 12 (10.3%) |
| Missing | 7 (0.6%) | 6 (0.9%) | 1 (0.3%) | 0 (0.0%) |
| Quality of life (self-rated) | ||||
| Satisfied | 1,050 (96.1%) | 645 (95.8%) | 294 (96.7%) | 111 (95.7%) |
| Not satisfied | 32 (2.9%) | 19 (2.8%) | 9 (3.0%) | 4 (3.4%) |
| Missing | 11 (1.0%) | 9 (1.3%) | 1 (0.3%) | 1 (0.9%) |
| Satisfaction with physical health | ||||
| Satisfied | 972 (88.9%) | 622 (92.4%) | 259 (85.2%) | 91 (78.4%) |
| Not satisfied | 105 (9.6%) | 43 (6.4%) | 37 (12.2%) | 25 (21.6%) |
| Missing | 16 (1.5%) | 8 (1.2%) | 8 (2.6%) | 0 (0.0%) |
| Satisfaction with mental health | ||||
| Satisfied | 838 (76.7%) | 563 (83.7%) | 209 (68.8%) | 66 (56.9%) |
| Not satisfied | 238 (21.8%) | 100 (14.9%) | 90 (29.6%) | 48 (41.4%) |
| Missing | 17 (1.6%) | 10 (1.5%) | 5 (1.6%) | 2 (1.7%) |
| Satisfaction with emotional health | ||||
| Satisfied | 1,010 (92.4%) | 639 (94.9%) | 275 (90.5%) | 96 (82.8%) |
| Not satisfied | 68 (6.2%) | 24 (3.6%) | 25 (8.2%) | 19 (16.4%) |
| Missing | 15 (1.4%) | 10 (1.5%) | 4 (1.3%) | 1 (0.9%) |
| Satisfaction with spiritual health | ||||
| Satisfied | 989 (90.5%) | 625 (92.9%) | 266 (87.5%) | 98 (84.5%) |
| Not satisfied | 83 (7.6%) | 33 (4.9%) | 34 (11.2%) | 16 (13.8%) |
| Missing | 21 (1.9%) | 15 (2.2%) | 4 (1.3%) | 2 (1.7%) |
Key: Healthcare access, service availability, and self-rated quality of life and well-being among older adults, stratified by number of self-reported chronic conditions. Note: Values are presented as count (percentage). “Satisfied” includes all positive self-ratings; “Not satisfied” includes negative or neutral ratings. Percentages may not total 100% due to rounding. “Missing” indicates unreported values.
Table 4.
Health Service Utilization Among Older Adults, Stratified by Chronic Disease Status.
| Variable | Total (N = 1,093) | No Chronic Condition (N = 673) | 1 Chronic Condition (N = 304) | 2+ Chronic Conditions (N = 116) |
| Emergency Room Visit (past 3 months) | ||||
| Yes | 116 (10.6%) | 51 (7.6%) | 41 (13.5%) | 24 (20.7%) |
| No | 974 (89.1%) | 619 (92.0%) | 263 (86.5%) | 92 (79.3%) |
| Missing | 3 (0.3%) | 3 (0.4%) | 0 (0.0%) | 0 (0.0%) |
| Hospitalization (past 3 months) | ||||
| Yes | 67 (6.1%) | 27 (4.0%) | 26 (8.6%) | 14 (12.1%) |
| No | 1,023 (93.6%) | 643 (95.5%) | 278 (91.4%) | 102 (87.9%) |
| Missing | 3 (0.3%) | 3 (0.4%) | 0 (0.0%) | 0 (0.0%) |
| Unmet Healthcare Needs (past 3 months) | ||||
| Yes | 56 (5.1%) | 26 (3.9%) | 18 (5.9%) | 12 (10.3%) |
| No | 1,030 (94.2%) | 641 (95.2%) | 285 (93.8%) | 104 (89.7%) |
| Missing | 7 (0.6%) | 6 (0.9%) | 1 (0.3%) | 0 (0.0%) |
Key: Self-reported emergency department visits, hospitalizations, and unmet healthcare needs among older adults in Saskatchewan, stratified by number of chronic conditions. Note: Values presented as count (percentage). “Missing” indicates respondents who did not provide a response to the relevant question. Percentages may not total 100% due to rounding.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



