
Submitted:
04 December 2025
Posted:
09 December 2025
You are already at the latest version
Abstract
Ketamine’s ability to lift mood and spur new synapse growth has put glutamate biology at the center of modern neurotherapeutics. Yet the drug’s intravenous route, monitoring requirements, and dissociative effects make it a poor candidate for long-term prevention of Alzheimer’s disease (AD).Here we advance a testable hypothesis: an all-oral “synaptogenic stack” could mimic ketamine’s downstream benefits—namely, the rise in brain-derived neurotrophic factor (BDNF) and the activation of mTOR—while avoiding its toxicities.The stack combines three inexpensive agents that have decades of human use. First, dextromethorphan, kept in circulation with a small dose of a CYP2D6 inhibitor, provides gentle NMDA antagonism. Second, piracetam acts as a positive modulator of AMPA receptors, boosting fast excitatory transmission. Third, oral L-glutamine replenishes presynaptic glutamate stores and buffers against excitotoxic spill-over. Working in concert, these drugs should reduce extrasynaptic NMDA stress, enhance AMPA throughput, and preserve dendritic spine density in the ageing brain.If this mechanism proves sound, the regimen offers a low-cost, scalable way to delay the clinical onset of AD, particularly in people who already show prodromal biomarkers or genetic risk. Prospective trials are needed to evaluate safety, target engagement, and long-term cognitive outcomes.
Keywords:
Alzheimer’ s disease
; preclinical AD
; synaptic dysfunction
; glutamate
; NMDA receptor
; extrasynaptic NMDA
; AMPA receptor
; neuroplasticity
; dextromethorphan
; piracetam
; L-glutamine
; CYP2D6 inhibition
; Glutamatergic Regimen
; disease prevention
; synaptogenesis
; BDNF
; mTOR
; ketamine-like mechanism
; cognitive reserve
; APOE4
; primary prevention
Background
Alzheimer's disease (AD) is now viewed less as a sudden loss of memory and more as a very long slide into synaptic failure that can start 20 or 30 years before a diagnosis [1,2]. In the earliest phase, two things go wrong with glutamate signalling. First, extrasynaptic NMDA receptors—especially those that carry the NR2B sub-unit—become hyperactive. At the same time AMPA receptors, which should sit in the synapse and pass the fast excitatory message, are pulled inside the neuron and degraded [3,4,5,6] Together these shifts set off calcium overload, oxidative stress, loss of long-term potentiation, spine shrinkage and, finally, cell death [7]. Drugs on the market today arrive late in that process and work on only half of the problem—for example, memantine mostly calms the rogue NMDA channels [8]. A better preventive approach would dampen toxic NMDA activity, rescue AMPA traffic and spark new synapse growth while the network is still salvageable.
The Cheung Glutamatergic Regimen
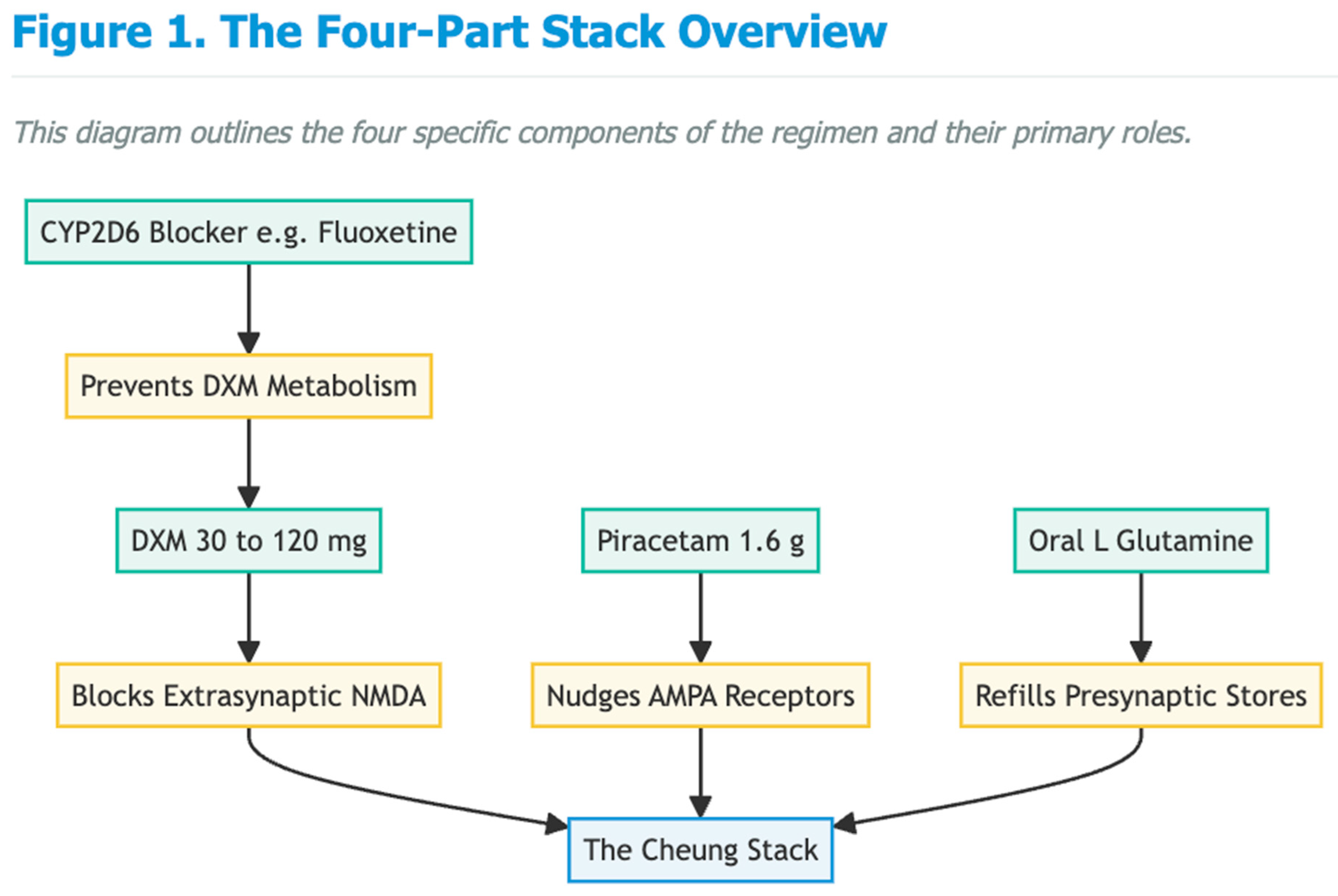
Cheung's four-part oral stack was first built for stubborn mood and anxiety illnesses, yet its design maps neatly onto those early AD defects [9,10,11]. The plan is simple and inexpensive: dextromethorphan (DXM) at 30–120 mg a day; a low dose of a strong CYP2D6 blocker such as fluoxetine, paroxetine or high-dose duloxetine to keep DXM in the blood; piracetam 1.6 g a day to nudge AMPA receptors; and supplementary oral l-glutamine to refill presynaptic stores and curb excitotoxicity. Together, these agents reproduce the "NMDA-to-AMPA flip" that underlies ketamine's burst of plasticity [12,13,14].
Mechanistic Alignment with Early AD Pathophysiology
Selective dampening of extrasynaptic NMDA noise is the first pillar. Like low-dose ketamine or memantine, high but steady DXM blocks open NMDA channels in a voltage-dependent way and shows a clear preference for NR2B-rich receptors [8]. Because soluble Aβ forces exactly these receptors to the cell surface and even drives damaging metabotropic signals without ion flow ([15,7], DXM held in circulation by a CYP2D6 inhibitor [11] could blunt calcium overload and tau mis-chief long before plaques appear.

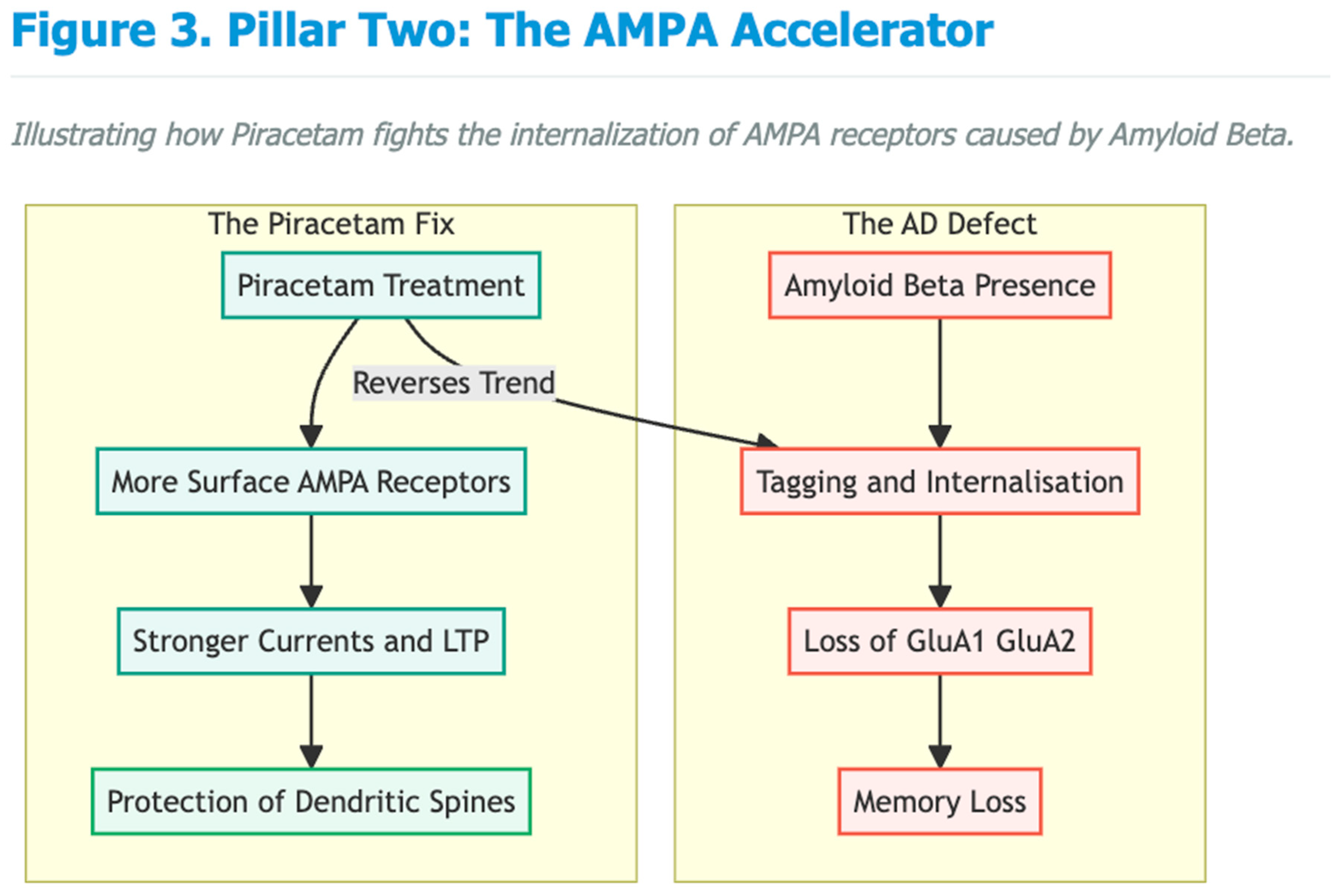
The second pillar is keeping AMPA receptors where they belong. Aβ promotes rapid tagging and internalisation of GluA1/GluA2 receptors, a change that tracks closely with memory loss [4,5,6]. Piracetam reverses that trend: work in aged and amyloid-exposed systems shows more surface AMPA receptors, stronger currents and better LTP after treatment [16,17]. By preserving fast transmission, piracetam may protect dendritic spines through the long pre-clinical window.
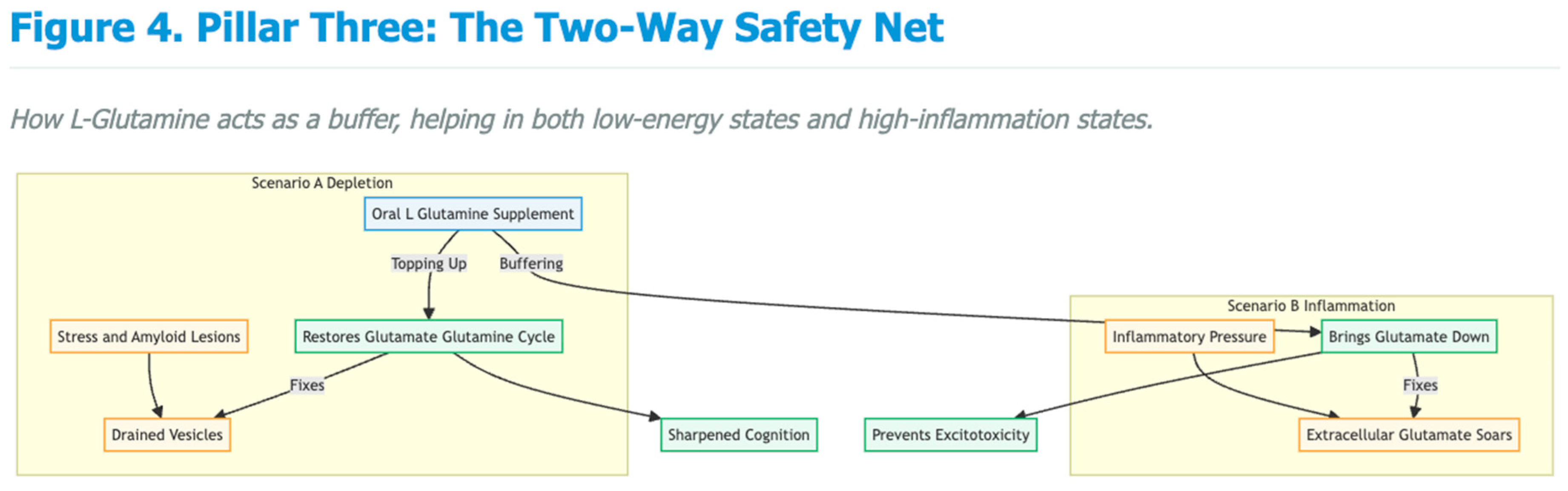
Third, presynaptic glutamate stores need topping up. Stress and early amyloid lesions drain vesicular glutamate and weaken release probability [18,19]. Oral l-glutamine quickly restores the glutamate–glutamine cycle, normalises excitatory postsynaptic currents and sharpens cognition in stressed or amyloid-bearing animals [18,19]. Curiously, when extracellular glutamate soars under inflammatory pressure, high-dose glutamine can actually bring it down [20,19], providing a two-way safety net against excitotoxicity.
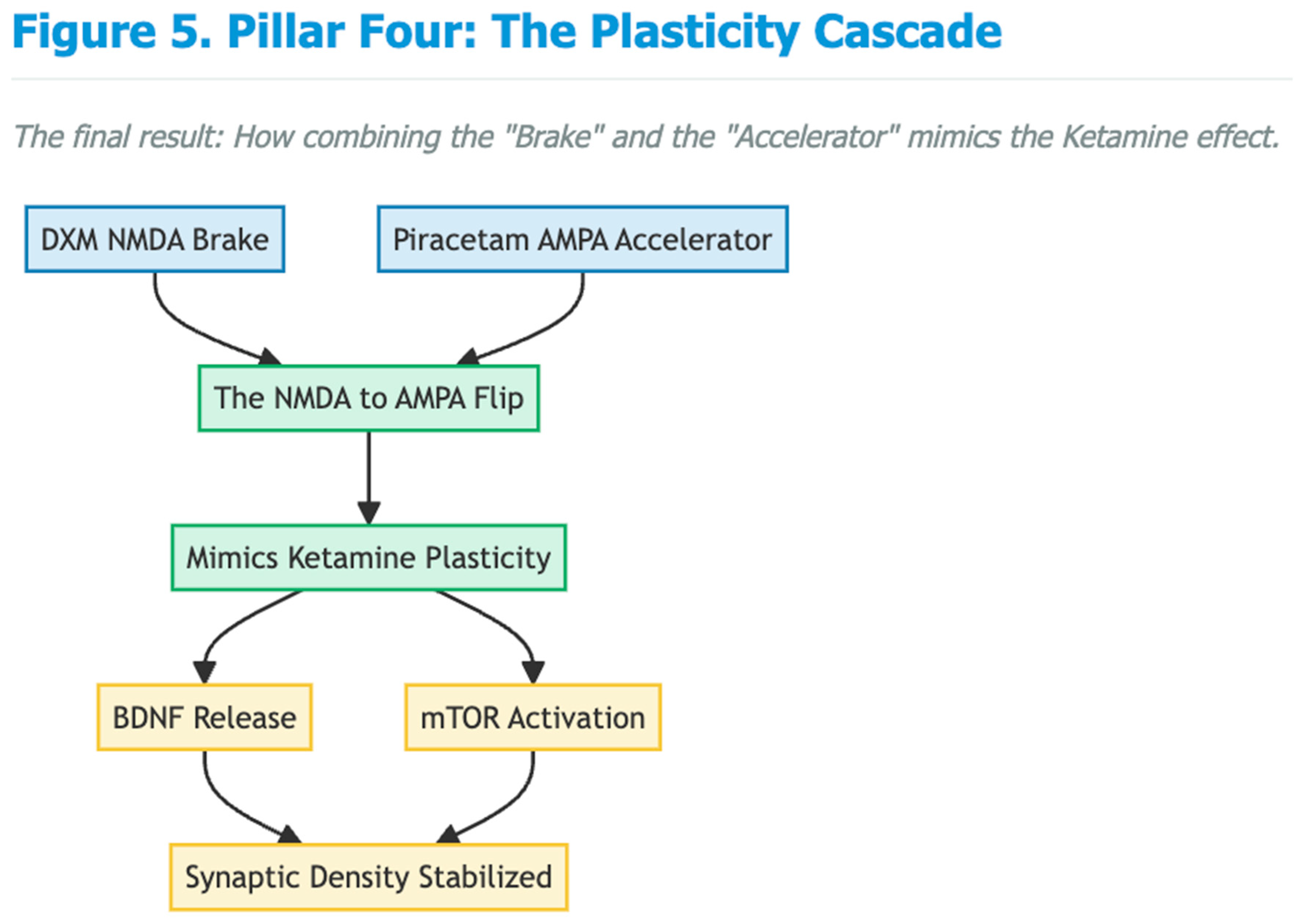
Finally, the pairing of an NMDA brake with an AMPA accelerator triggers a well-studied plasticity cascade: BDNF release and mTOR-dependent spine formation [12,21]. Because BDNF/TrkB signalling falters early in AD, repeated activation through the Cheung stack could hold synaptic density steady in people at risk [9].
Emerging Clinical Signals Relevant to Cognition and Neuroprotection
Case reports already hint at brisk cognitive gains with the full or partial regimen. Patients describe clearer thinking, faster processing and stronger working memory within weeks—improvements that mirror the subtle executive losses seen years before an AD diagnosis [22,23,24,25]. One young man with schizoaffective disorder said the stack "cleared decades of mental sludge" after everything else had failed [23]. Although anecdotal, such stories match the known importance of healthy AMPA throughput for high-order cognition.
Feasibility for Long-Term Prevention
All four ingredients are off-patent, cheap (well under two dollars a day), taken by mouth and backed by decades of safety data. Side-effects tend to be mild—occasional insomnia, jitters or stomach upset—and usually ease with dose adjustment [9,11]. Because many clinicians already prescribe the stack off-label, it is uniquely positioned for pragmatic prevention trials in APOE-ε4 carriers, people with subjective cognitive decline or biomarker-positive preclinical AD.
Conclusions
The earliest biology of Alzheimer's looks like a tilt from a balanced NMDA–AMPA partnership toward runaway extrasynaptic NMDA activity and dwindling AMPA support. The Cheung Glutamatergic Regimen addresses both faults at once: sustained DXM plus a CYP2D6 blocker reins in toxic NMDA signalling; piracetam revives AMPA strength; glutamine refuels presynaptic stores and cushions against spill-over damage. Given its low cost, oral delivery and growing clinical experience, the regimen deserves fast-tracked trials as a primary or secondary preventive for Alzheimer's disease.
Conflict of Interest and Source of Funding Statement
None declared.
Funding Declaration
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics Declaration
Not applicable.
References
- Mota, S.I.; Ferreira, I.L.; Rego, A.C. Dysfunctional synapse in Alzheimer's disease - A focus on NMDA receptors. Neuropharmacology 2014, 76 Pt A, 16–26. [Google Scholar] [CrossRef]
- Wang, R.; Reddy, P.H. Role of Glutamate and NMDA Receptors in Alzheimer's Disease. J Alzheimers Dis. 2017, 57, 1041–1048. [Google Scholar] [CrossRef]
- Chang, E.H.; Savage, M.J.; Flood, D.G.; et al. AMPA receptor downscaling at the onset of Alzheimer's disease pathology in double knockin mice. Proc Natl Acad Sci USA 2006, 103(9), 3410–3415. [Google Scholar] [CrossRef]
- Hsieh, H.; Boehm, J.; Sato, C.; et al. AMPAR removal underlies Abeta-induced synaptic depression and dendritic spine loss. Neuron 2006, 52(5), 831–843. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Guo, O.; Huo, Y.; et al. Amyloid-β Induces AMPA Receptor Ubiquitination and Degradation in Primary Neurons and Human Brains of Alzheimer's Disease. J Alzheimers Dis. 2018, 62(4), 1789–1801. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.; Li, C.; Liu, J.; et al. Impairments in endogenous AMPA receptor dynamics correlates with learning deficits in Alzheimer's disease model mice. Proc Natl Acad Sci USA 2023, 120(40), e2303878120. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Sanz, C.; Balantzategi, U.; Quintela-López, T.; et al. Amyloid β / PKC-dependent alterations in NMDA receptor composition are detected in early stages of Alzheimer´s disease. Cell Death Dis. 2022, 13(3), 253. [Google Scholar] [CrossRef]
- Danysz, W.; Parsons, C.G. Alzheimer's disease, β-amyloid, glutamate, NMDA receptors and memantine--searching for the connections. Br J Pharmacol. 2012, 167, 324–352. [Google Scholar] [CrossRef]
- Cheung, N. Clinical experience and optimisation of the Cheung glutamatergic regimen for refractory psychiatric diseases. Preprints 2025. [Google Scholar] [CrossRef]
- Cheung, N. DXM, CYP2D6-inhibiting antidepressants, piracetam, and glutamine: Proposing a ketamine-class antidepressant regimen with existing drugs. Preprints 2025. [Google Scholar] [CrossRef]
- Cheung, N. Ultra-low-dose paroxetine as CYP2D6 inhibitor enables safe OTC glutamatergic augmentation in a depressive patient on lisdexamfetamine. Preprints 2025. [Google Scholar] [CrossRef]
- Li, N.; Lee, B.; Liu, R.J.; et al. mTOR-dependent synapse formation underlies the rapid antidepressant effects of NMDA antagonists. Science 2010, 329(5994), 959–964. [Google Scholar] [CrossRef]
- Maeng, S.; Zarate, C.A., Jr.; Du, J.; et al. Cellular mechanisms underlying the antidepressant effects of ketamine: role of alpha-amino-3-hydroxy-5-methylisoxazole-4-propionic acid receptors. Biol Psychiatry 2008, 63(4), 349–352. [Google Scholar] [CrossRef]
- Zanos, P.; Moaddel, R.; Morris, P.J.; et al. NMDAR inhibition-independent antidepressant actions of ketamine metabolites. Nature 2016, 533(7604), 481–486. [Google Scholar] [CrossRef]
- Kessels, H.W.; Nabavi, S.; Malinow, R. Metabotropic NMDA receptor function is required for β-amyloid-induced synaptic depression. Proc Natl Acad Sci USA 2013, 110, 4033–4038. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.A.; Müller, W.E. Effects of piracetam on N-methyl-D-aspartate receptor properties in the aged mouse brain. Pharmacology 1993, 47, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Winblad, B. Piracetam: a review of pharmacological properties and clinical uses. CNS Drug Rev. 2005, 11, 169–182. [Google Scholar] [CrossRef]
- Son, H.; Baek, J.H.; Go, B.S.; et al. Glutamine has antidepressive effects through increments of glutamate and glutamine levels and glutamatergic activity in the medial prefrontal cortex. Neuropharmacology 2018, 143, 143–152. [Google Scholar] [CrossRef]
- Baek, J.H.; Park, H.; Kang, H.; et al. The Role of Glutamine Homeostasis in Emotional and Cognitive Functions. Int J Mol Sci. 2024, 25(2), 1302. [Google Scholar] [CrossRef]
- Guerrero-Molina, M.P.; Morales-Conejo, M.; Delmiro, A.; et al. High-dose oral glutamine supplementation reduces elevated glutamate levels in cerebrospinal fluid in patients with mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes syndrome. Eur J Neurol. 2023, 30(2), 538–547. [Google Scholar] [CrossRef] [PubMed]
- Duman, R.S.; Aghajanian, G.K. Synaptic dysfunction in depression: potential therapeutic targets. Science 2012, 338, 68–72. [Google Scholar] [CrossRef]
- Cheung, N. Clearing the fog with the Cheung's regimen: A case of OTC glutamatergic augmentation in a student with depression, somatic symptoms and cognitive dysfunction. Preprints 2025. [Google Scholar] [CrossRef]
- Cheung, N. An oral "ketamine-like" NMDA/AMPA modulation stack restores cognitive capacity in a young man with schizoaffective disorder—Case report. Preprints 2025. [Google Scholar] [CrossRef]
- Cheung, N. Case series: Marked improvement in treatment-resistant obsessive–compulsive symptoms with over-the-counter glutamatergic augmentation in routine clinical practice. Preprints 2025. [Google Scholar] [CrossRef]
- Cheung, N. Oral glutamatergic augmentation for trauma-related disorders with fluoxetine-/bupropion-potentiated dextromethorphan ± piracetam: A four-patient case series. Preprints 2025. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



