Study Highlights — What is New
This is the first human study to simultaneously quantify MMP activity and glycooxidation-derived AGE structures in paired visceral and subcutaneous adipose tissue.
Molecular abnormalities of obesity are restricted to visceral adipose tissue; subcutaneous adipose tissue and plasma remain unaffected.
The coexistence of ECM proteolysis and protein glycooxidation indicates a synergistic mechanism leading to adipose tissue failure.
Circulating biomarkers do not reflect visceral adipose tissue pathology, explaining why metabolic risk cannot be reliably stratified using blood tests alone.
Visceral adipose tissue behaves as a metabolically active inflammatory–proteolytic organ, supporting the concept of obesity as a disease of adipose tissue quality rather than adipose mass.
1. Introduction
Obesity is one of the most pressing global health challenges and is strongly associated with type 2 diabetes, dyslipidemia and cardiovascular disease [
1,
2]. Current scientific understanding emphasizes that obesity is not merely a consequence of caloric excess, but a progressive systemic disease driven by chronic low-grade inflammation and qualitative disturbances in adipose tissue structure [
3,
4]. Among adipose depots, visceral adipose tissue is considered the most clinically relevant due to its distinct endocrine profile, metabolic activity and inflammatory potential.
The expansion of visceral adipose tissue triggers hypoxia, immune cell recruitment, oxidative stress and remodeling of the ECM, ultimately promoting fibrosis [
4]. A central regulator of ECM homeostasis is the family of Matrix Metalloproteinases (MMPs). Dysregulated MMP activity has been linked to adipose tissue fibrosis, endothelial dysfunction, insulin resistance and cardiometabolic risk [
5,
6,
7]. Notably, excessive MMP activity can also modify adipokine signaling and increase leptin resistance, further deepening metabolic deterioration [
8]. Beyond adipokine dysregulation, excessive MMP activity contributes to oxidative stress by disrupting antioxidant ECM structures and releasing ROS-generating fragments. This oxidative shift enhances the biochemical milieu in which non-enzymatic protein glycation and glycooxidation readily occur.
In parallel, metabolic stress induces non-enzymatic protein glycation and glycooxidation, leading to the accumulation of AGEs. AGEs irreversibly alter protein structure, amplify oxidative stress and activate pro-inflammatory pathways through receptors such as receptor for advanced glycation end-products (RAGE) [
2]. Although both MMP activation and AGE accumulation have been implicated in metabolic disease, their coexistence at the adipose tissue level has not been comprehensively investigated.
Most available studies focus on circulating markers, which may not reliably reflect local molecular adipose tissue pathology. Therefore, this study evaluates whether visceral adipose tissue in obesity constitutes a selective inflammatory–proteolytic niche characterized by simultaneous activation of MMPs and glycooxidation-related protein damage, in contrast to subcutaneous adipose tissue and plasma. This divergence arises from the inherently higher immunometabolic activity of visceral fat, which possesses richer vascularization, denser macrophage infiltration and greater exposure to gut-derived inflammatory mediators compared with subcutaneous fat [
2,
4,
6].
2. Materials and Methods
2.1. Metalloproteinase Activity
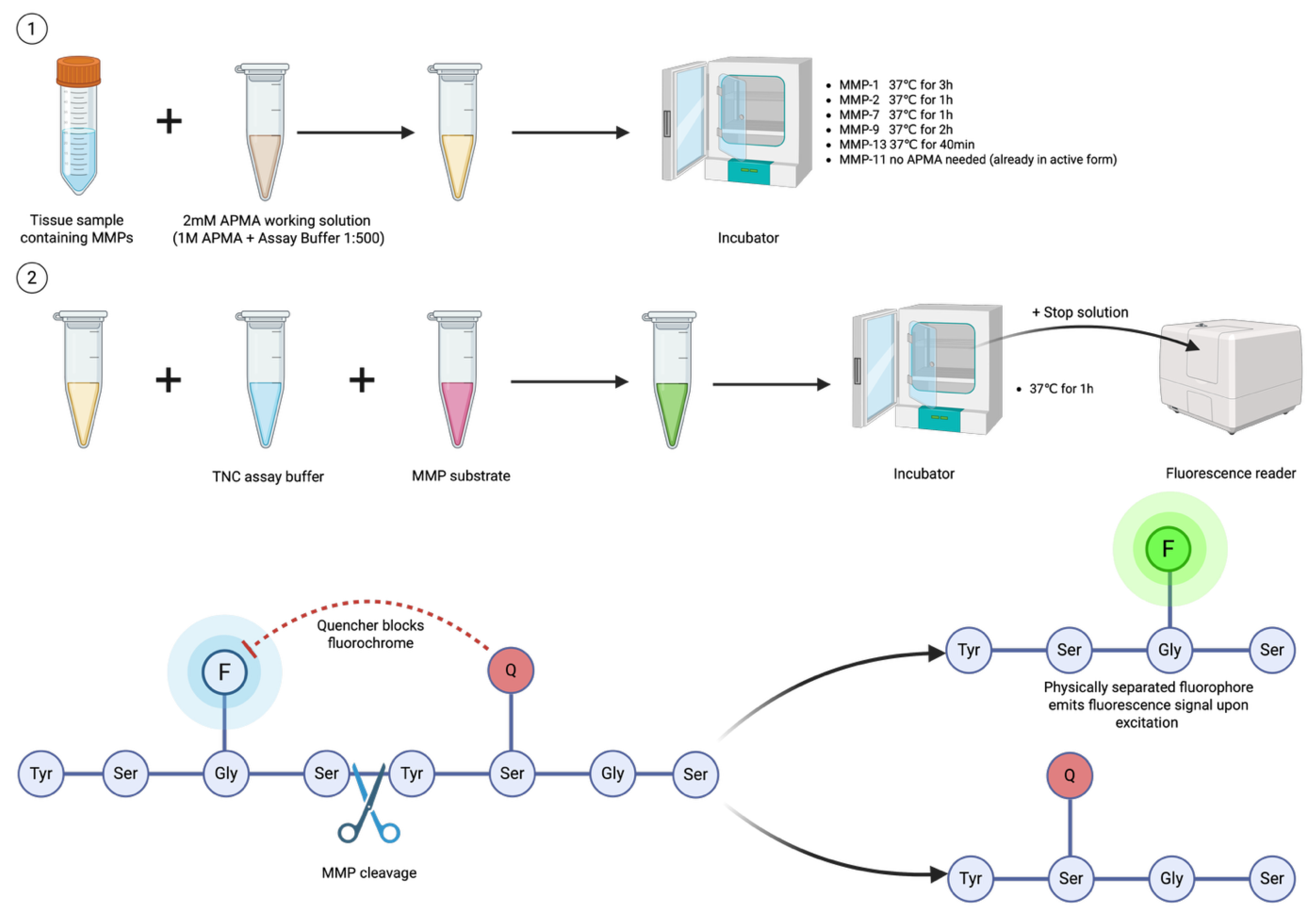
To assess the activity of various MMPs in subcutaneous and visceral fat, as well as plasma, we used a previously described FRET assay [
9]. Before the assay, the samples were pre-incubated at 37℃ with 2mM 4-aminophenylmercuric acetate (APMA). The incubation times varied depending on the MMP type (3 hours for MMP-1; 1 hour for MMP-2 and MMP-7; 2 hours for MMP-9; 40 minutes for MMP-13). Only MMP-11 did not require pre-incubation, as it is already in its active form. After pre-incubation, the MMP-containing sample was mixed with the Tris-HCl/NaCl/CaCl₂ (TNC) assay buffer, and 3 µM MMP substrate (MCA-Pro-Leu-Gly∼Leu-Dpa(Dnp)-Ala-Arg-NH
2, containing the FRET peptide was added. The substrate was obtained from Sigma-Aldrich. Typically, the FRET peptide contains a fluorophore on one side of the peptide sequence and a quencher on the other. When the protein is intact, the quencher suppresses the emission peak of the fluorophore and absorbs its energy in a distance-dependent manner. However, when active MMPs are present, the peptide is cleaved into two separate fragments, allowing the fluorescence from the fluorophore to be detected. The mixture was incubated at 37℃ for 1h, after which the stop solution was added, and fluorescence was measured. The data were presented as arbitrary fluorescence units (AFU) per 1 milligram of protein.
Figure 1 represents a simplified version of the process.
2.1. Advanced Glycation Products
Total AGE and specific AGEs such as VES, PEN and amyloid cross-β-structure were assessed using fluorimetric analysis. Additionally, we measured protein glycooxidation product - DT. Fluorescence measurements were performed using an Infinite M200 PRO multi-mode plate reader (Tecan Group Ltd., Männedorf, Switzerland). The samples were diluted in 0.02 MPBS (pH 7.4; 1:5, v/v) before analysis. The excitation/emission wavelength was set at 350/440nm for total AGE, 350/405nm for VES, 335/385nm for PEN, 365/480nm for DT and 435/485nm for amyloid cross-β-structure.
3. Results
3.1. Characteristics of the Obesity Group”
The obesity group consisted of 40 patients with severe obesity qualified for bariatric surgery according to the criteria specified in the Individual Research Project, including BMI > 35 kg/m² and the absence of active malignancy, acute inflammatory diseases, autoimmune disorders, chronic infectious diseases and alcohol or nicotine dependence.
There were 28 women and 12 men. The median age of the patients was 43 years (interquartile range [IQR]: 35–50 years), with a range from 20 to 73 years, and a mean age of 42.6 ± 12.1 years.
Anthropometric data confirmed advanced obesity. The median body weight was 113 kg (IQR: 97–136.5 kg, range: 82–185 kg) and the median BMI was 39.24 kg/m² (IQR: 36.19–44.41 kg/m², range: 32.37–51.79 kg/m²).
Median height was approximately 1.7 m.
Laboratory data were consistent with a chronic low-grade inflammatory state: the median CRP concentration was 13.6 mg/L (IQR: 7.6–26.0 mg/L, range: 3.7–85.9 mg/L), the median fibrinogen level was 358 mg/dL (IQR: 323–391 mg/dL, range: 258–484 mg/dL) and the median white blood cell count was 11.19 ×10³/µL (IQR: 9.9–12.47 ×10³/µL, range: 5.73–17.92 ×10³/µL).
In total, 15 patients met the criteria for metabolic syndrome. Surgical procedures included 29 sleeve gastrectomies (one combined with crural repair to prevent gastroesophageal reflux symptoms), 9 gastric bypass procedures (one combined with hiatal hernia repair) and 2 SADI procedures. Overall, the study cohort represents a typical population of patients with severe obesity referred for bariatric surgery, with a high burden of metabolic complications and chronic inflammation, but without comorbidities that would exclude participation in the study.
A detailed summary of the anthropometric and biochemical characteristics of the obesity group is presented in
Table 1.
3.2. Characteristics of the Control Group.
The control group consisted of 21 patients qualified for elective surgical procedures in accordance with the inclusion and exclusion criteria defined in the Individual Research Project, including the absence of obesity, metabolic disorders, autoimmune diseases, active malignancy, acute or chronic inflammatory diseases and alcohol or nicotine dependence. The group included 13 women and 8 men. The median age was 50 years (interquartile range [IQR]: 39–66 years), with a range of 25 to 78 years.
The median BMI in the control group remained within the reference range for the majority of individuals, although a few patients presented BMI values above 25 kg/m². This deviation was accepted due to the considerable difficulty in obtaining a sufficiently large number of eligible healthy volunteers. Additional bioethics committee approval was obtained to increase recruitment and ensure adequate statistical power of the study.
All laboratory inflammatory markers were within reference ranges, which was consistent with the inclusion criteria and confirmed the absence of systemic inflammation. Surgical indications included 17 hernia repair procedures and 4 laparoscopic cholecystectomies, with no history of metabolic or bariatric surgery in any participant.
3.3. Ethical Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki and approved by the Bioethics Committee of the Medical University of Bialystok (resolution No. APK.002.98.2023, issued on 16 February 2023). An additional approval was obtained by resolution No. R-I-002/475/2019, issued on 19 September 2024, which authorized the Humana Medica Omeda center as an additional site for biological sample collection and permitted the continuation of the medical experiment at this location. Informed consent was obtained from all participants prior to inclusion in the study. Each patient signed the Patient Information Form describing the study objectives, procedures and potential risks, as well as the Consent Form for participation in scientific research and Annex No. 1 and Annex No. 2 to the Personal Data Protection Rules for Research at the Medical University of Bialystok.
3.4. Metalloproteinase Activity
MMPs are zinc-dependent proteases responsible for cleaving and modifying ECM components, including collagen, elastin, and gelatin. They have an essential role in numerous physiological processes, such as cell-cycle regulation, signal transduction, cell differentiation and ECM turnover [
10]. These functions are important for normal growth and morphogenesis. Indeed, an increased MMPs activity was observed during embryogenesis, angiogenesis, wound repair and bone development [
11] . Conversely dysregulated MMPs activity can be associated with a variety of pathological conditions, including inflammation, fibrosis, autoimmune diseases, diabetes mellitus, and cancer progression and metastases [
11].
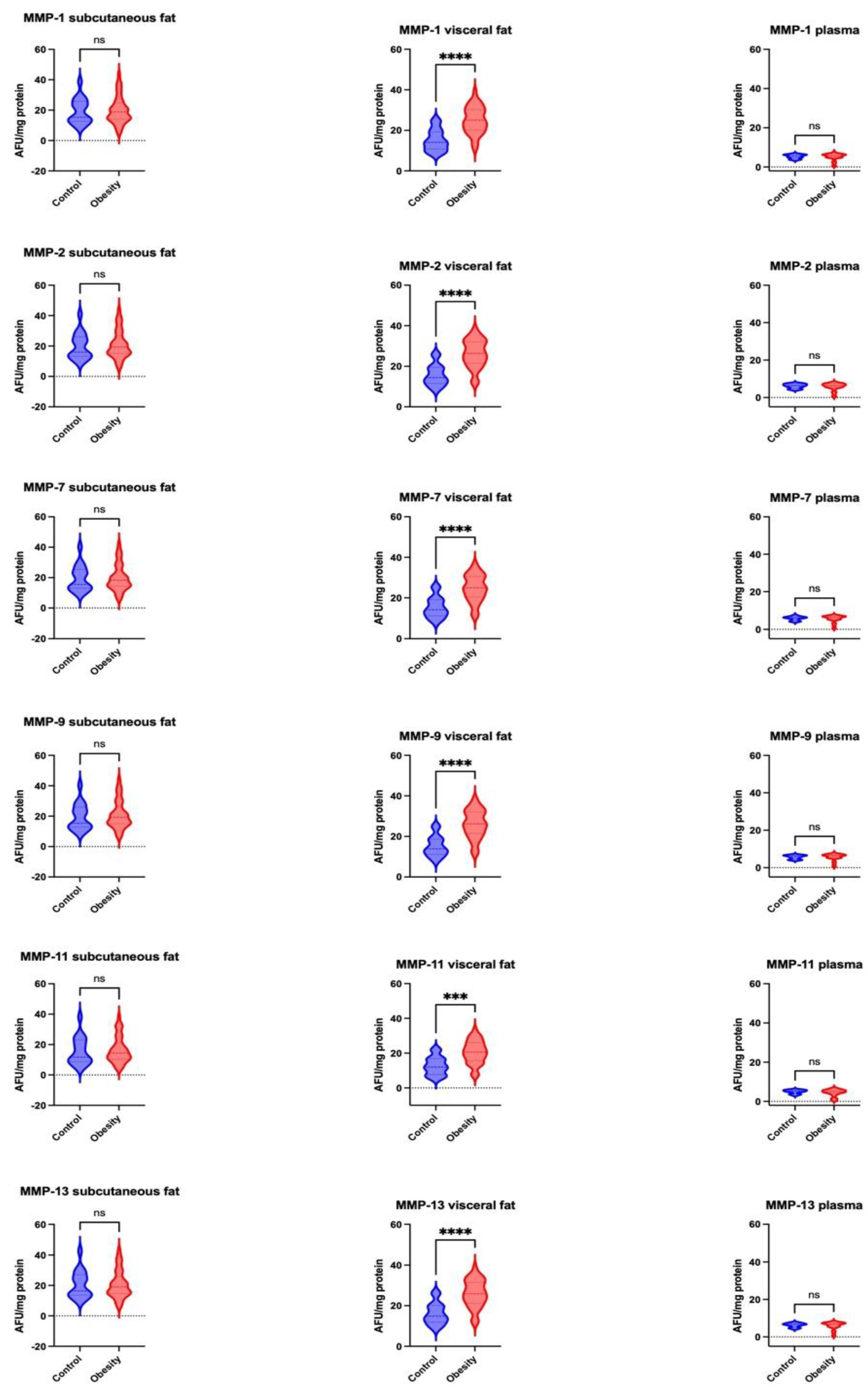
In our study we found that visceral fat MMP activity in obese patients was significantly increased compared to the control group with the following percentage changes: MMP-1 (MD +54.74%; p < 0.0001), MMP-2 (MD +54,49%; p < 0.0001), MMP-7 (MD +56,59% ; p < 0.0001), MMP-9 (MD +53.07%; p < 0.0001), MMP-11 (MD +58.21%; p = 0.0001), MMP-13 (MD +57,56%; p < 0.0001) (
Figure 2). No significant difference in MMPs activity were observed in plasma and subcutaneous fat for any of the assessed MMPs.
3.5. Advanced Glycation Products
Protein glycation is a non-enzymatic process in which a free amino group reacts with the carbonyl group, forming an unstable Schiff base. This intermediate then undergoes rearrangement into a more stable Amadori product (AP). Ultimately, APs can further promote protein degradation by generating AGEs with a prolonged half-life [
12,
13]. These changes alter protein structure and function, making it resistant to modifications and breakdown. This leads to the accumulation of damaged proteins, resulting in inflammation and various pathological conditions, including diabetes mellitus, cardiovascular diseases, and neurodegenerative diseases [
14].
VES and PEN are the final glycation products. Amyloid cross-β-structure is a peptide that is especially prone to glycation and forms deposits present in Alzheimer’s disease [
12]. DT is a byproduct of glycooxidation that arises when the reactive oxygen species (ROS) interact with glycated proteins, resulting in more complex alterations [
14].
3.5.1. Dityrosine
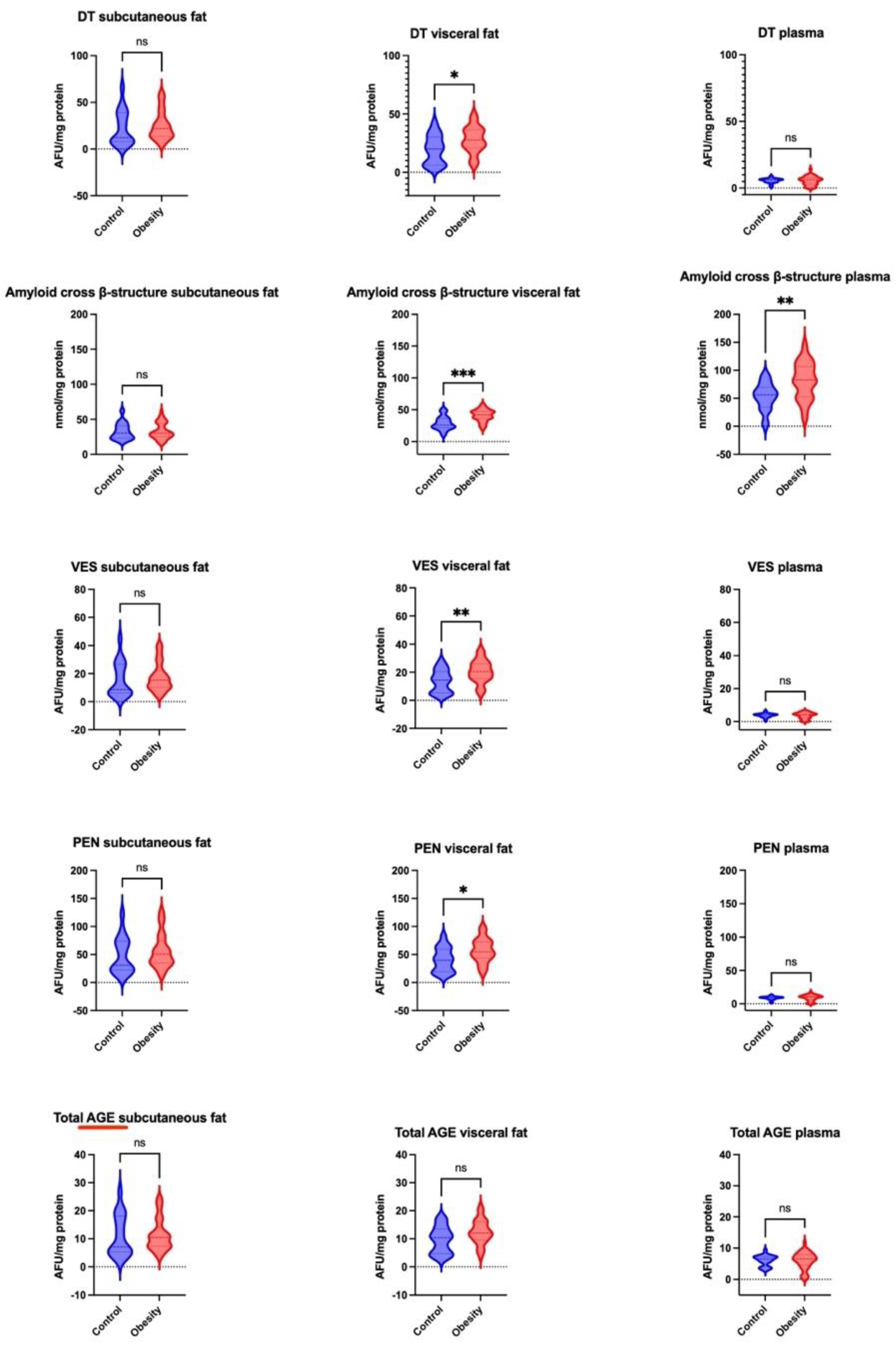
We observed a significant increase in visceral fat levels in DT (MD +72.47%; p < 0.05) among obese patients vs controls. There were no significant differences in subcutaneous fat and plasma levels between the two groups (
Figure 3).
3.5.2. Amyloid Cross-β-Structure
Levels of amyloid cross-β-structure were significantly greater in visceral fat of obese patients compared to controls (MD +61.85%; p < 0.001). Additionally, the obese group had a higher plasma concentration than the control group (MD +67.99%; p < 0.01). There was no significant change in subcutaneous fat concentration between the groups (
Figure 3).
3.5.3. Vesperlysine
We observed a significantly higher VES content in visceral fat in obese individuals compared to controls (MD +69,76%; p < 0.01). There was no significant difference in VES content in subcutaneous fat or plasma (
Figure 3).
3.5.4. Pentosidine
PEN levels were significantly higher in the obese group compared to controls (MD +72.77%; p < 0.05). There was no difference between the groups in subcutaneous fat or plasma (
Figure 3).
3.5.5. Total AGE
The total AGE content did not significantly differ across all the groups and tissues (
Figure 3)
4. Discussion
This study provides new insight into the pathophysiology of obesity by showing that proteolytic and glycooxidative changes occur selectively within visceral adipose tissue. The consistent upregulation of activity across all analyzed MMP isoforms in visceral adipose tissue — particularly MMP-1, MMP-2, MMP-7 and MMP-9 — coupled with the unchanged activity in subcutaneous adipose tissue and plasma, indicates that ECM breakdown is not a systemic feature of obesity but rather a highly localized hallmark of visceral adipose tissue dysfunction. Similarly, pronounced elevations in DT, amyloid cross-β-structure, VES and PEN were restricted to visceral adipose tissue, while total AGE concentrations remained unchanged, underscoring a targeted and structured molecular alteration rather than a global rise in glycooxidation
Synergy Between ECM Proteolysis and Glycooxidation as a Mechanistic Link
The observed parallel between elevated MMP activity and increased AGE accumulation suggests a synergistic mechanism rather than two independent processes. ECM degradation exposes proteins susceptible to oxidative modifications, while AGE-mediated crosslinking subsequently stiffens the ECM, perpetuating inflammation and fibrosis [
2]. This cycle ultimately impairs lipid buffering capacity and promotes a maladaptive shift toward increased lipolysis, elevated free fatty acid flux and hepatic gluconeogenesis — key drivers of insulin resistance and atherogenic dyslipidemia [
15]. These results therefore support a paradigm in which visceral adipose tissue dysfunction precedes and drives systemic metabolic disease, rather than appearing as its consequence.
Translational Implications
These insights have direct therapeutic relevance. Bariatric surgery and incretin-based pharmacotherapy have been shown to reduce systemic inflammation, oxidative stres and normalize circulating MMP levels [
16,
17,
18,
19]. Interventions that improve ECM homeostasis and reduce fibrotic signaling are associated with improved insulin sensitivity, metabolic disorders and cardiometabolic outcomes [
18,
20,
21]. However, it remains unknown to what extent tissue-level glycooxidation and fibrosis are reversible, and whether a durable “metabolic scar” persists despite weight loss. Future clinical studies will need to integrate metabolic outcomes with tissue-specific molecular profiling to determine whether normalization of visceral adipose tissue biology is a prerequisite for full metabolic recovery.
Strengths, Limitations and Perspectives
A major strength of this study is the direct molecular assessment of human adipose tissue depots from the same individuals, in contrast to exclusive reliance on circulating biomarkers. This design allowed us to clearly separate systemic from local pathology. Limitations include the cross-sectional design, which restricts inference about temporal causality, and the absence of additional ECM-associated markers (e.g., tissue inhibitors of metalloproteinases (TIMPs), collagen subtypes, integrin signaling).
5. Conclusions
The present study demonstrates that visceral adipose tissue in obesity constitutes a selective inflammatory–proteolytic microenvironment characterized by concurrent activation of matrix metalloproteinases and glycooxidation-related protein damage. This pattern was not observed in subcutaneous adipose tissue nor in plasma, indicating that circulating biomarkers may substantially underestimate local molecular injury within visceral fat. These findings highlight the role of visceral adipose tissue as a key driver of metabolic deterioration rather than a passive energy reservoir. By identifying the tight link between ECM proteolysis and protein glycooxidation, the study provides mechanistic insight into adipose tissue dysfunction and offers a potential molecular framework for future therapeutic targeting. Further longitudinal and interventional studies are likely necessary to determine whether modulation of MMP activity or attenuation of AGE accumulation within visceral fat can translate into improved metabolic outcomes.
Author Contributions
Conceptualization, K.W. , B.C. , M.M. , P.M.; methodology, K.W. and M.M. M.Ż-P.; formal analysis, K.W. , M.M. , B.C.; investigation, K.W. B.C. M.M. , A.T. , A.K..; writing—original draft preparation, K.W. , R.C.; writing—review and editing, B.C., M.M., J.D., A.Z. and P.M.; supervision, P.M. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Bioethics Committee of the Medical University of Bialystok (resolution No. APK.002.98.2023 of 16 February 2023) and by resolution No. R-I-002/475/2019 of 19 September 2024, which authorized the Humana Medica Omeda center as an additional site for biological sample collection and permitted the continuation of the medical experiment.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Each participant signed the Patient Information Form describing the study procedures and risks, as well as the Consent Form for participation in scientific research and Annex No. 1 and Annex No. 2 to the Personal Data Protection Rules for Research at the Medical University of Bialystok.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Data are not publicly available due to personal data protection regulations.
Acknowledgments
The authors thank the staff of the 1st Department of General and Endocrine Surgery, Medical University of Bialystok, Department of Hygiene, Epidemiology and Ergonomics, Medical University of Bialystok and Humana Medica OMEDA, Białystok for their support and collaboration during manuscript preparation.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
AGE — advanced glycation end-product
ALT – Alanine aminotransferase
AP — Amadori product
AST – Aspartate aminotransferase
APMA — 4-aminophenylmercuric acetate
BMI — body mass index
CRP – C-reactive protein
DT — dityrosine
ECM — extracellular matrix
FRET — fluorescence resonance energy transfer
INR – International normalized ratio
MCH – Mean corpuscular hemoglobin
MCHC – Mean corpuscular hemoglobin concentration
MCV – Mean corpuscular volume
MMP — matrix metalloproteinase
PEN — pentosidine
RAGE — receptor for advanced glycation end-products
RBC – Red blood cells
ROS — reactive oxygen species
TIMP — tissue inhibitor of metalloproteinases
WBC – White blood cells
VES — vesperlysine
References
- Elmaleh-Sachs, A.; Schwartz, J.; Bramante, C.; Nicklas, J.; Gudzune, K.; Jay, M. Obesity Management in Adults: A Review. JAMA 2023, 330, 2000–2015. [Google Scholar] [CrossRef]
- Henning, R. Obesity and Obesity-Induced Inflammatory Disease Contribute to Atherosclerosis: A Review of the Pathophysiology and Treatment of Obesity. Am J Cardiovasc Dis 2021, 11, 504–529. [Google Scholar]
- Rubino, F.; Batterham, R.L.; Koch, M.; Mingrone, G.; le Roux, C.W.; Farooqi, I.S.; Farpour-Lambert, N.; Gregg, E.W.; Cummings, D.E. Lancet Diabetes & Endocrinology Commission on the Definition and Diagnosis of Clinical Obesity. Lancet Diabetes Endocrinol 2023, 11, 226–228. [Google Scholar] [CrossRef]
- Ruiz-Ojeda, F.J.; Méndez-Gutiérrez, A.; Aguilera, C.M.; Plaza-Díaz, J. Extracellular Matrix Remodeling of Adipose Tissue in Obesity and Metabolic Diseases. Int J Mol Sci 2019, 20. [Google Scholar] [CrossRef]
- Li, X.; Zhao, Y.; Chen, C.; Yang, L.; Lee, H.; Wang, Z.; Zhang, N.; Kolonin, M.G.; An, Z.; Ge, X.; et al. Critical Role of Matrix Metalloproteinase 14 in Adipose Tissue Remodeling during Obesity. Mol Cell Biol 2020, 40, e00564-19. [Google Scholar] [CrossRef]
- Mirica, R.M.; Ionescu, M.; Mırıca, A.; Gınghına, O.; Iosıfescu, R.; Vacarasu, A.-B.; Cıotarla, D.-C.; Rosca, A.; Zagrean, L.; Iordache, N. Pathophysiology of Metalloproteinase Matrix in Relation to Morbid Obesity and Associated Pathologies. The European Research Journal 2022, 8, 411–419. [Google Scholar] [CrossRef]
- Aksoyer Sezgin, S.; Bayoğlu, B.; Ersoz, F.; Sarici, M.; Niyazoğlu, M.; Dirican, A.; Cengiz, M. Downregulation of MMP-2 and MMP-9 Genes in Obesity Patients and Their Relation with Obesity-Related Phenotypes. Turkish Journal of Biochemistry 2022, 47. [Google Scholar] [CrossRef]
- Mazor, R.; Friedmann-Morvinski, D.; Alsaigh, T.; Kleifeld, O.; Kistler, E.B.; Rousso-Noori, L.; Huang, C.; Li, J.B.; Verma, I.M.; Schmid-Schönbein, G.W. Cleavage of the Leptin Receptor by Matrix Metalloproteinase–2 Promotes Leptin Resistance and Obesity in Mice. Sci Transl Med 2018, 10, eaah6324. [Google Scholar] [CrossRef] [PubMed]
- Troeberg, L.; Nagase, H. Monitoring Metalloproteinase Activity Using Synthetic Fluorogenic Substrates. Curr Protoc Protein Sci 2003, 33, 21.16.1–21.16.9. [Google Scholar] [CrossRef] [PubMed]
- Zitka, O.; Kukacka, J.; Krizkova, S.; Huska, D.; Adam, V.; Masarik, M.; Prusa, R.; Kizek, R. Matrix Metalloproteinases. Curr Med Chem 2010, 17, 3751–3768. [Google Scholar] [CrossRef] [PubMed]
- Cabral-Pacheco, G.A.; Garza-Veloz, I.; Castruita-De la Rosa, C.; Ramirez-Acuña, J.M.; Perez-Romero, B.A.; Guerrero-Rodriguez, J.F.; Martinez-Avila, N.; Martinez-Fierro, M.L. The Roles of Matrix Metalloproteinases and Their Inhibitors in Human Diseases. Int J Mol Sci 2020, 21, 9739. [Google Scholar] [CrossRef]
- Dańkowska, K.; Nesterowicz, M.; Lauko, K.K.; Trocka, D.; Żendzian-Piotrowska, M.; Ładny, J.R.; Zalewska, A.; Żebrowska-Gamdzyk, M.; Maciejczyk, M. In Vitro and in Silico Studies and a Systematic Literature Review of Antiglycation Properties of Amlodipine. Sci Rep 2025, 15, 33277. [Google Scholar] [CrossRef]
- Peyroux, J.; Sternberg, M. Advanced Glycation Endproducts (AGEs): Pharmacological Inhibition in Diabetes. Pathologie Biologie 2006, 54, 405–419. [Google Scholar] [CrossRef]
- Drygała, S.; Żendzian-Piotrowska, M.; Radzikowski, M.; Zalewska, A.; Maciejczyk, M. Inhibition of Protein Glycation by Vasodilatory β-Blockers – In Vitro Studies and in Silico Analyses. Biomedicine & Pharmacotherapy 2025, 185, 117976. [Google Scholar] [CrossRef]
- Wang, T.; He, C. Pro-Inflammatory Cytokines: The Link between Obesity and Osteoarthritis. Cytokine Growth Factor Rev 2018, 44, 38–50. [Google Scholar] [CrossRef]
- H, W.J.P.; L, B.R.; Salvatore, C.; Melanie, D.; F, V.G.L.; Ildiko, L.; M, M.B.; Julio, R.; D, T.M.T.; A, W.T.; et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. New England Journal of Medicine 2021, 384, 989–1002. [CrossRef]
- Liberale, L.; Bonaventura, A.; Carbone, F.; Bertolotto, M.; Contini, P.; Scopinaro, N.; Camerini, G.B.; Papadia, F.S.; Cordera, R.; Camici, G.G.; et al. Early Reduction of Matrix Metalloproteinase-8 Serum Levels Is Associated with Leptin Drop and Predicts Diabetes Remission after Bariatric Surgery. Int J Cardiol 2017, 245, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Choromańska, B.; Myśliwiec, P.; Łuba, M.; Wojskowicz, P.; Myśliwiec, H.; Choromańska, K.; Żendzian-Piotrowska, M.; Dadan, J.; Zalewska, A.; Maciejczyk, M. Impact of Weight Loss on the Total Antioxidant/Oxidant Potential in Patients with Morbid Obesity-A Longitudinal Study. Antioxidants (Basel) 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Choromańska, B.; Myśliwiec, P.; Łuba, M.; Wojskowicz, P.; Dadan, J.; Myśliwiec, H.; Choromańska, K.; Zalewska, A.; Maciejczyk, M. A Longitudinal Study of the Antioxidant Barrier and Oxidative Stress in Morbidly Obese Patients after Bariatric Surgery. Does the Metabolic Syndrome Affect the Redox Homeostasis of Obese People? J Clin Med 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- García-Prieto, C.F.; Gil-Ortega, M.; Vega-Martín, E.; Ramiro-Cortijo, D.; Martín-Ramos, M.; Bordiú, E.; Sanchez-Pernaute, A.; Torres, A.; Aránguez, I.; Fernández-Alfonso, M.; et al. Beneficial Effect of Bariatric Surgery on Abnormal MMP-9 and AMPK Activities: Potential Markers of Obesity-Related CV Risk. Front Physiol 2019, 10–2019. [Google Scholar] [CrossRef]
- Choromańska, B.; Myśliwiec, P.; Łuba, M.; Wojskowicz, P.; Myśliwiec, H.; Choromańska, K.; Dadan, J.; Żendzian-Piotrowska, M.; Zalewska, A.; Maciejczyk, M. Bariatric Surgery Normalizes Protein Glycoxidation and Nitrosative Stress in Morbidly Obese Patients. Antioxidants (Basel) 2020, 9. [Google Scholar] [CrossRef] [PubMed]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).