Submitted:
01 December 2025
Posted:
03 December 2025
Read the latest preprint version here
Abstract
Major depressive disorder was, until recently, framed as a single entity arising from a linear stress–monoamine–hypothalamic–pituitary–adrenal (HPA) axis cascade, modeled by forced swim and learned helplessness tests and evaluated by brief Hamilton Depression Rating Scale (HAM-D)/Montgomery–Åsberg Depression Rating Scale (MADRS) symptom trials. This “unitary cascade” view has been dismantled by imaging, immune–metabolic and sleep profiling, and plasticity markers, which reveal divergent circuit, inflammatory, and chronobiological patterns across anxious, pain-laden, and cognitively weighted depression, with non-response and relapse common. Translationally, face-valid rodent assays that equated immobility with despair have yielded limited bedside benefit, whereas cross-species bridges—electroencephalography (EEG) motifs, rapid eye movement (REM) architecture, effort-based reward tasks, and inflammatory/metabolic panels—are beginning to provide mechanistically grounded, clinically actionable readouts. In current practice, depression care is shifting toward systems psychiatry: inflammation-high and metabolic-high archetypes, anhedonia- and circadian-dominant subgroups, formal treatment-resistant depression (TRD) staging, connectivity-guided neuromodulation, esketamine, selected pharmacogenomic panels, and early digital phenotyping, as endpoints broaden to functioning and durability. A central gap is that heterogeneity is acknowledged but rarely built into trial design or implementation. This perspective advances a plasticity-centered systems psychiatry in which a testable prediction is that manipulating defined prefrontal–striatal and prefrontal–limbic circuits in sex-balanced, chronic-stress models will reproduce human network-defined biotypes and treatment response, and proposes hybrid effectiveness–implementation platforms that embed immune–metabolic and sleep panels, circuit-sensitive tasks, and digital monitoring under a shared, preregistered data standard.
Keywords:
major depressive disorder (MDD)
; neurocircuitry
; synaptic plasticity
; neuroimmune interactions
; metabolic syndrome
; treatment-resistant depression (TRD)
; neuromodulation
; biomarkers
; kynurenine
; precision medicine
1. Framing the Journey—Prompts
Major depressive disorder has long been framed through a monoamine-centric lens, a narrative that catalyzed pharmacotherapy yet left substantial non-response and relapse [1]. Historical reassessments of the monoamine hypothesis and contemporary work on clinical, neurobiological, and treatment advances now converge on a simple conclusion: incremental refinements of the same model are no longer sufficient [2,3]. In an era of high dimensional neuroimaging, immune profiling, and digital phenotyping, revisiting the trajectory from 1960s monoamine theories to emerging systems psychiatry is therefore a strategic necessity [4,5](Figure 1). (4 refs)
This perspective views major depressive disorder as a nexus condition with dense cross talk to anxiety, chronic pain, and dementia, where shared and distinct pathways blur categorical boundaries [6]. Large scale cohort and imaging studies reveal common yet dissociable alterations in prefrontal and limbic circuitry across depression, anxiety, post-traumatic stress disorder, and pain, while mechanistic work highlights bidirectional links with cardiometabolic and neurodegenerative disease [7,8,9]. Within this landscape, anxious, pain enriched, and cognitively loaded depression exemplify how comorbidity patterns reshape prognosis, treatment response, and trial outcomes [10,11]. (5 refs)
Our central thread traces the shift from neurotransmitter first thinking toward an integrated immune, metabolic, and circuit-based framework that can anchor precision care [12]. This perspective synthesizes evidence on central–peripheral immune interactions, network-level biotypes, and model-driven subtypes of brain organization, and outlines how these advances should inform next-generation therapeutics and trial design [13,14,15]. Rather than another unitary model of depression, this perspective advances frameworks that treat heterogeneity as signal, not noise, enabling stratified, personalized interventions across intertwined spectra of mood, anxiety, pain, and cognitive decline [16]. (4 refs)
Box A—Key Terms
A biomarker is an objective biological signal that indexes state, risk, or treatment response. An endophenotype reflects a heritable, mechanistic intermediate—closer to circuitry than symptoms. Anhedonia captures reduced reward sensitivity or effort, a core transdiagnostic deficit. Treatment-resistant denotes limited response after adequate therapeutic trials. Rapid-acting refers to interventions producing meaningful change within hours to days. A network target is a circuit-defined node guiding drug or device precision. A digital endpoint leverages passive or task-based sensors to quantify behavior in real time.
2. Early Paradigms & Assumptions (1960s–1990s)
Early paradigms of depression research crystallized around stress, monoamines, and the hypothalamic pituitary adrenal axis as the primary translators of adversity into “behavioral despair” [2,17] Forced swim and learned helplessness tests, later complemented by chronic stress paradigms in rodents and primates, operationalized immobility, withdrawal, and subdued exploration as proxies for hopelessness [18,19]. These models were highly sensitive to monoaminergic and hypothalamic–pituitary–adrenal axis (HPA) modulating drugs and, for a time, appeared to bridge synapse and symptom [20,21]. Parallel work on glucocorticoid feedback, neurosteroids, and early immune and gut brain signals refined this picture, yet still treated depression largely as a unitary endpoint of a relatively linear stress monoamine HPA cascade [22,23].
On the clinical side, the introduction of DSM III and DSM III R reconfigured nosology around symptom checklists, while Hamilton Depression Rating Scale (HAM-D) and later Montgomery–Åsberg Depression Rating Scale (MADRS) scores became the dominant trial endpoints [24,25]. Response and remission were quantified by cutoffs on these scales, and short, fixed duration trials with single primary mood outcomes became the gold standard for regulatory sensitive evidence [26,27]. Placebo run in phases, designed to screen out early improvers and sharpen drug signal, further shaped effect sizes and sample composition, often at the cost of ecological validity [26,28]. Translation across trials relied on scale equivalence rather than deeper phenotyping or mechanistic anchors [29,30].
Within this framework, crucial sources of heterogeneity were marginalized [31]. Sex and age dependent profiles of mood, anxiety, and somatic symptoms were rarely modeled explicitly in either preclinical or clinical research, despite emerging data on sex specific monoamine and HPA signatures [32,33,34,35]. Ancestry, social context, chronic pain, and subthreshold anxiety were treated as noise, not structure [36]. Endpoint myopia, focused on short term mood change in narrowly defined samples, left longer term trajectories, functional outcomes, and comorbidity patterns largely uncharted, planting many of the seeds for the replication, generalization, and treatment resistance challenges that later decades would confront [37,38,39].
3. Pivot Suite (10 Mini-Cards)
This Pivot Suite condenses ten mechanistic “mini-cards” that reorient depression from a monoamine-shortage model toward a multiscale systems disorder. Each card anchors a specific lever—plasticity and circuit dynamics, reward and stress alignment, immune–metabolic and genomic milieu, or multi-point intervention logic—and links it to concrete translational readouts. Together, these pivots outline how synapses, circuits, body-wide signals, and trial architectures can be jointly tuned to redesign treatment-resistant depression (TRD) as a tractable, stratified systems problem.
3.1. Plasticity & Circuit Control of Depressive States
Across these cards, depression science shifts from monoamine scarcity toward dynamic systems. Each mini-anchor foregrounds mechanisms, actionable readouts, and clinically tractable targets that scaffold next-generation translational trial designs.
3.1.1. Synaptic Plasticity & Intrinsic Excitability
- Long-term potentiation and depression, α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptor throughput, and evoked excitatory postsynaptic potentials (eEPSPs) index rapid remodeling, while neurogenesis and extracellular signal-regulated kinase (ERK)-sensitive priming by ketamine extend effects [42,43,44,45].
3.1.2. Glutamate/γ-Aminobutyric Acid (GABA) Microcircuit Control
3.1.3. Circuit-Level Nodes (Drugs & Devices)
- Circuit-level nodes highlight how drugs and devices now target networks connecting habenula, subcallosal cingulate, and ventromedial prefrontal cortex.
- Deep brain, vagus nerve, and transcranial magnetic stimulation, including accelerated theta-burst protocols, are steered by connectivity-guided targeting and TMS-EEG physiology.
- Proof of target engagement, intensified dosing schedules, and responder enrichment by baseline network topology redefine how device parameters map onto durable outcomes [57].
3.2. Reward, Motivation & Stress Systems
The pivot pair tracks how stress reshapes reward pursuit and timekeeping, linking mesolimbic opioid tone and HPA plus circadian drift to anhedonia and fatigue.
3.2.1. Reward, motivation, and stress–opioid tone
3.2.2. HPA–Circadian–Stress Axis
3.3. Immune–Metabolic–Genomic Modifiers of Risk and Treatment Response
This pivot gathers immune, metabolic, and genomic modifiers that quietly bias risk, symptom expression, and durability of response, turning background milieu into explicit treatment design variables.
3.3.1. Tryptophan (Trp)–kynurenine (KYN) steering
Tryptophan (Trp)-kynurenine (KYN) steering links immune activation to serotonin scarcity and neurotoxic load [75]. indoleamine 2,3-dioxygenase (IDO) and tryptophan 2,3-dioxygenase (TDO) divert Trp into KYN, tuning kynurenic acid (KYNA) versus quinolinic acid (QA) and aryl hydrocarbon receptor (AhR) signaling [76]. Peripheral C-reactive protein (CRP), KYN/Trp ratios, and microglia astrocyte metabolism align with cognitive, affective, and somatic symptom clusters, inviting inflammation stratified, longitudinal KYN panels in back translation [77,78,79,80,81,82,83,84,85,86,87].
3.3.2. Neuroimmune and glia
- Trials should treat sex, inflammatory state, and electroconvulsive or stimulation induced immune shifts as designable dimensions for precision psychiatry [95].
3.3.3. Metabolic–endocrine crosstalk
- Metabolic endocrine crosstalk highlights insulin resistance, adiposity, and glucagon-like peptide-1 (GLP-1) signaling as levers that couple energy allocation to mood, cognition, and treatment response.
- Metabolic syndrome phenotypes and type 2 diabetes (T2D) comorbidity flag patients in whom antidepressant efficacy, tolerability, and neuromodulation outcomes hinge on brain insulin signaling.
- Pragmatic trials should embed metabolic stratification and functional endpoints.
3.3.4. Epigenetic/transcriptional gating
3.4. Multi-Point Precision Strategies & Emerging Targets
The pivot turns from single levers to integrated playbooks, treating TRD as a heterogeneous systems problem that demands multiscale, multi-point intervention logic frameworks.
3.4.1. Multi-point strategies and next-wave targets
4. Divergence → Reconnection
As monoamine and stress-based models began to fray, a new translational strategy sought bridges that could genuinely scale across species rather than rely on face validity alone [108]. Electrophysiological motifs, such as frontal alpha asymmetry and reward related event related potentials, emerged as candidate intermediate phenotypes that can be measured in rodents and humans using homologous paradigms [109,110,111]. Sleep architecture, particularly REM density and slow wave fragmentation, offered another shared metric, mirrored by alterations in stress exposed animals and patients with melancholic or TRD [112,113,114]. In parallel, probabilistic reward tasks and cognitive control batteries were adapted across rodents, non-human primates, and humans, while longitudinal inflammatory and endocrine panels were integrated into both preclinical and clinical protocols, enabling richer cross species modeling of reward inflammation coupling [115,116].
Yet the field also accumulated clear failures to learn from earlier missteps [117]. The assumption that immobility equals despair persisted long after it became evident that forced swim behavior reflects a narrow coping style, not the multidimensional construct of depression [118,119]. Short duration trials and brief stress paradigms continued to dominate despite growing evidence that synaptic, circuit, and immune remodeling unfold over weeks to months [120,121]. Single endpoint thinking, usually centered on global depression scores or single behavioral tests, repeatedly obscured domain specific gains and masked heterogeneity in trajectories [122,123].
The most promising advances have come from deliberate back translation [124,125]. Symptom clusters and rating scale factors are first decomposed into Research Domain Criteria (RdoC) like domains of negative valence, reward processing, arousal, and cognition, then re instantiated as tractable tasks and physiological readouts in animals [125,126]. Multimodal biomarker programs now use human defined phenotypes to guide the design of cross species EEG batteries, reward and cognitive paradigms, and peripheral immune signatures [127,128]. In doing so, they begin to reconnect bench and bedside around shared dimensions rather than diagnostic labels alone [129,130].

Table 1.
Cross-species bridge map for depression-relevant constructs and translatable assays. Cross-species bridge map linking human constructs to preclinical assays, quantitative readouts, and clinical analogs that can be implemented in contemporary trials. “Status” summarizes translational maturity (routine, emerging, or exploratory), while “Design tip” highlights one concrete way to embed each bridge into mechanistically anchored, heterogeneity-aware study designs.
Table 1.
Cross-species bridge map for depression-relevant constructs and translatable assays. Cross-species bridge map linking human constructs to preclinical assays, quantitative readouts, and clinical analogs that can be implemented in contemporary trials. “Status” summarizes translational maturity (routine, emerging, or exploratory), while “Design tip” highlights one concrete way to embed each bridge into mechanistically anchored, heterogeneity-aware study designs.
| Human construct | Preclinical assay | Readout | Clinical analog | Status | Design tip |
| Anhedonia/ motivational deficit | Effort-based decision tasks (progressive ratio, T-maze barrier, operant sucrose) | Breakpoint, lever presses, willingness to work under stress or inflammation | Probabilistic reward tasks, EEfRT, ventral striatal BOLD, anhedonia scales | Emerging trial biomarker | Separate hedonic “liking” from motivational “wanting”; include stress/inflammation challenge blocks. |
| Negative affect/threat bias | Fear conditioning and extinction; chronic social defeat | Freezing/avoidance, extinction curves, startle, social withdrawal | Fear-learning and extinction tasks, startle paradigms, threat-bias tasks in anxious/MDD subgroups | Robust basic science; limited clinical use | Use as domain-specific endpoint in anxious and trauma-loaded depression; pair behavior with EEG/fMRI. |
| Cognitive control/executive dysfunction | Attentional set-shifting, 5-CSRTT, reversal learning | Errors, omissions, reaction times, perseveration indexes | Set-shifting (e.g., CANTAB), n-back, Stroop, Trail Making, DLPFC activation | Secondary endpoint in several trials | Pre-stratify “cognitively loaded” depression; link change to functioning and return-to-work outcomes. |
| Sleep and circadian disruption | Rodent EEG/EMG with chronic stress or light-cycle shift; REM-deprivation models | REM latency/density, NREM slow-wave power, activity rhythms, phase shifts | Polysomnography, actigraphy, DLMO, sleep/circadian questionnaires | Strong observational; emerging endpoints | Align dosing and assessments with chronotype; treat sleep/circadian metrics as primary modifiable targets. |
| HPA axis and stress reactivity | Chronic mild stress, restraint, social defeat; Dex/CRH challenges | Corticosterone profiles, GR sensitivity, coping style, stress-induced behavioral shift | Cortisol awakening response, DST, lab stress tests, hair cortisol | Mixed but promising for subtyping | Sample across diurnal cycle; co-model stress markers with symptom domains (anergy, anxiety, cognitive fog). |
| Inflammation–KYN steering | LPS/IFN-α or stress-sensitized immune activation; Trp–KYN pathway assays | KYN/Trp ratio, QA/KYNA balance, microglial activation, cytokine panels | CRP, IL-6/TNF panels, plasma KYN/Trp, symptom clusters (anergia, anhedonia, psychomotor slowing) | High translational interest | Pre-specify “inflammation-high” strata; collect longitudinal KYN panels and align with treatment response. |
| Metabolic–endocrine load | High-fat diet, genetic obesity, insulin-resistance models | Glucose tolerance, insulin signaling, adiposity, spontaneous activity | BMI, waist-to-hip ratio, HOMA-IR, HbA1c, metabolic-syndrome indices | Growing but underused in trials | Embed metabolic panels into TRD studies; design dedicated obesity/T2D depression trials with functional endpoints. |
| Synaptic plasticity / rapid-acting response | Ketamine/psychedelic paradigms; LTP/LTD, in vivo spine imaging, AMPA-forward assays | Spine density, AMPA/NMDA ratio, LTP/LTD magnitude, early oscillatory changes | Early EEG/MEG plasticity markers, TMS-LTP readouts, 24–72 h symptom and cognition shifts | Strong mechanistic, clinical for ketamine | Build in early (24–72 h) windows and plasticity markers as key secondary endpoints in rapid-acting trials. |
| Network-level connectivity biotypes | Chemogenetic/optogenetic PFC–striatal/limbic manipulation; rodent rsfMRI/EEG | Resting-state connectivity, oscillatory coupling, causal node influence, behavior under circuit control | rsfMRI biotypes, TMS-EEG connectivity, SCC/vmPFC network markers for neuromodulation targeting | Emerging targeting tool | Require “target engagement” thresholds for drugs/devices; enrich samples by baseline network topology. |
| Digital behavior and passive monitoring | Home-cage automated monitoring of movement, sleep, and social interaction | Continuous activity, sleep–wake structure, social proximity, exploration patterns | Smartphone-based mobility, call/text patterns, speech and behavior passively captured by sensors | Early exploratory | Predefine digital endpoints (e.g., mobility, social withdrawal) and link them to functional and relapse outcomes. |
5-CSRTT, five-choice serial reaction time task; BMI, body mass index; AMPA, α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid; BOLD, blood-oxygen-level–dependent; CANTAB, Cambridge Neuropsychological Test Automated Battery; Dex/CRH, dexamethasone/corticotropin-releasing hormone; DLPFC, dorsolateral prefrontal cortex; DLMO, dim light melatonin onset; DST, dexamethasone suppression test; EefRT, Effort Expenditure for Rewards Task, EEG, electroencephalograph; EMG, electromyography; fMRI, functional magnetic resonance imaging; GR, HbA1c, glycated hemoglobin; glucocorticoid receptor; HOMA-IR, homeostatic model assessment of insulin resistance; HPA, hypothalamic–pituitary–adrenal; IFN-α interferon-alpha; IL-6, interleukin-6; KYN, kynurenine; LTD, long-term depression; LPS, lipopolysaccharide; LTP, long-term potentiation; MEG, magnetoencephalography; MMD, major depressive disorder; NMDA, N-methyl-D-aspartate; NREM, non- rapid eye movement; PFC, prefrontal cortex; QA, quinolinic acid; REM, rapid eye movement; rsfMRI, resting-state functional magnetic resonance imaging; SCC, subcallosal cingulate; T2D, type 2 diabetes; TMS, transcranial magnetic stimulation; TNF, tumor necrosis factor; TRD, treatment-resistant depression; Trp, tryptophan; vmPFC, ventromedial prefrontal cortex.
5. Clinical Applications Today
Clinical applications of systems psychiatry are moving beyond one-size-fits-all algorithms toward stratified care grounded in biology and behavior [131]. Depression is increasingly parsed into inflammation high, metabolically burdened, anhedonia dominant, and sleep or circadian disrupted profiles, overlaid on formal staging of treatment resistance [132,133]. Elevated CRP altered neutrophil to lymphocyte ratios, and immune metabolic gene signatures delineate patients whose symptoms cluster around anergia and anhedonia, while sleep fragmentation and circadian misalignment identify another modifiable axis that cuts across stages of non-response [134]. Parallel work on pharmacogenomics, circuit-based biotypes, and age specific EEG signatures is entering specialist clinics and early phase trials [13,135,136].
A clear distinction now separates tools that are clinically ready from those that are almost ready [137]. Structured TRD staging, esketamine, neuromodulation devices, and several pharmacogenomic panels have achieved regulatory approval and are supported by comparative effectiveness data [106,138,139]. By contrast, multiplex inflammatory and metabolic panels, task based cognitive emotional biomarkers, and digital phenotyping batteries remain largely in the candidate domain, often validated in carefully selected cohorts but not yet embedded in stepped care pathways [128,140].
Translating these advances into everyday practice faces substantial hurdles [141]. Access to neuromodulation, ketamine-based interventions, and genomic testing is uneven, constrained by cost, infrastructure, and workforce training [142]. Regulatory frameworks still privilege drug over device and algorithm, and reimbursement rarely rewards stratified assessment [143]. Without deliberate attention to equity, biologically enriched care risks deepening disparities, as populations with higher inflammatory burden, multimorbidity, and limited digital access may be the least likely to receive precision guided interventions [144,145,146].
Figure 2.
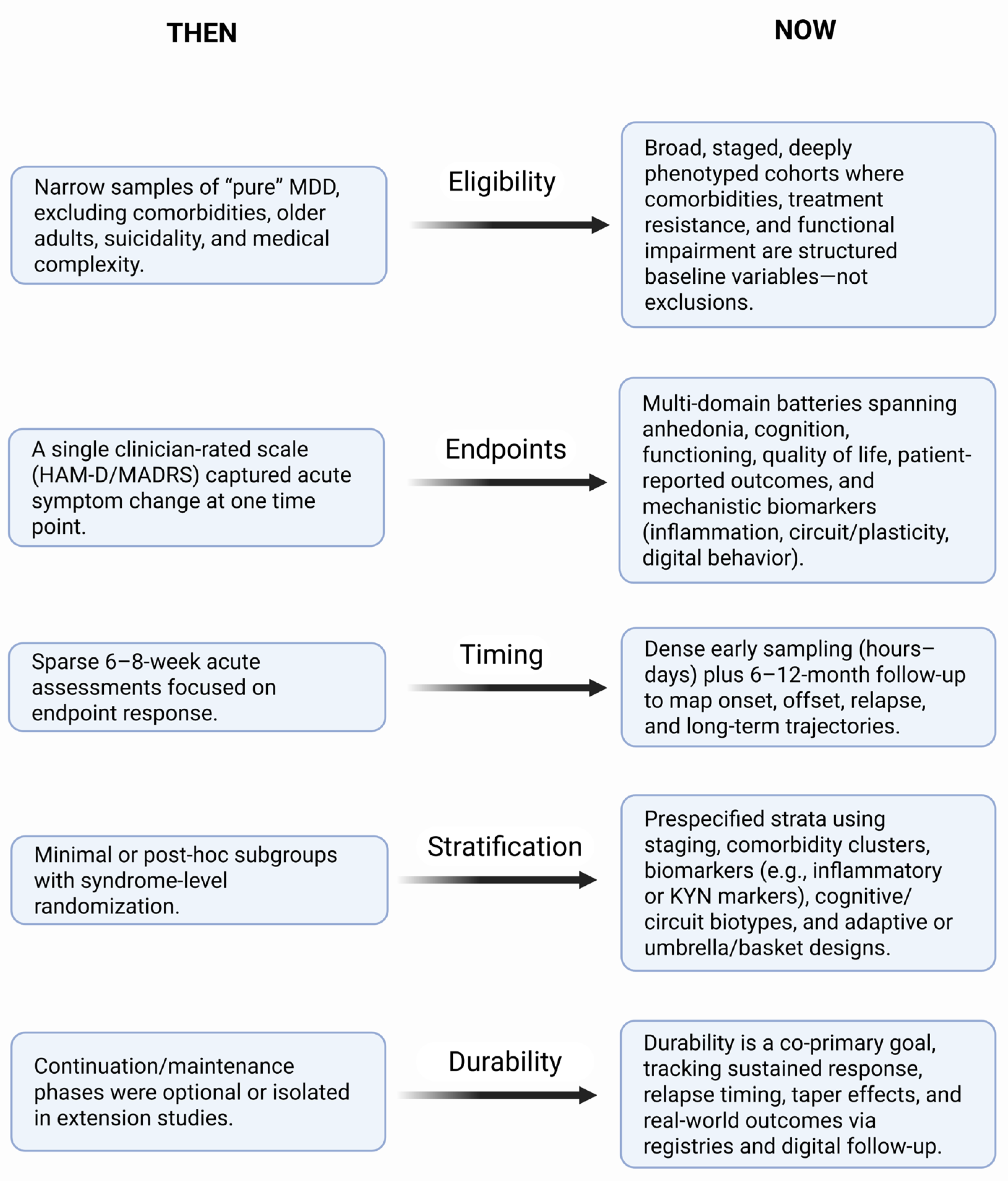
Evolution of depression trial design across eligibility, endpoints, timing, stratification and durability. The schematic contrasts conventional antidepressant trials (Then, left) with emerging systems-psychiatry-informed designs (Now, right). Eligibility. Earlier trials typically enrolled narrowly defined adults with “pure” major depressive disorder, excluding common comorbidities, older age, suicidality and medical complexity; contemporary designs move toward staged, better-characterized and more inclusive samples, with comorbidities, treatment resistance and functional impairment captured as structured baseline variables rather than automatic exclusions. Endpoints. Traditional studies relied on a single clinician-rated symptom scale (for example, HAM-D or MADRS) at one acute time point; modern trials incorporate multi-domain outcome batteries, including anhedonia and cognition, functioning and quality of life, patient-reported outcomes, and mechanistic readouts (for example, inflammatory markers, circuit or plasticity measures, digital behavior). Timing. Classic trials emphasized 6–8-week acute response with relatively sparse visits; new designs layer dense early sampling windows (hours to days for rapid-acting agents) onto longer follow-up to 6–12 months, enabling characterization of onset, offset and relapse dynamics. Stratification. Earlier studies used minimal or post-hoc subgrouping (for example, melancholic versus atypical) and randomization only at the syndrome level; contemporary designs prespecify strata and enrichment rules based on clinical staging, comorbidity clusters, biomarkers (such as inflammation or KYN metrics), cognitive or circuit biotypes, and sometimes deploy adaptive or umbrella/basket architectures. Durability. Historically, continuation and maintenance phases were optional or handled in separate extension studies; current trials increasingly embed durability as a co-primary objective, tracking time to relapse, sustained response, taper/discontinuation effects and real-world effectiveness via registries or digital follow-up, thereby aligning trial design with the long-term course of depressive illness. HAM-D, Hamilton Depression Rating Scale; KYN, kynurenine; MADRS, Montgomery–Åsberg Depression Rating Scale; MDD, major depressive disorder.
Figure 2.
Evolution of depression trial design across eligibility, endpoints, timing, stratification and durability. The schematic contrasts conventional antidepressant trials (Then, left) with emerging systems-psychiatry-informed designs (Now, right). Eligibility. Earlier trials typically enrolled narrowly defined adults with “pure” major depressive disorder, excluding common comorbidities, older age, suicidality and medical complexity; contemporary designs move toward staged, better-characterized and more inclusive samples, with comorbidities, treatment resistance and functional impairment captured as structured baseline variables rather than automatic exclusions. Endpoints. Traditional studies relied on a single clinician-rated symptom scale (for example, HAM-D or MADRS) at one acute time point; modern trials incorporate multi-domain outcome batteries, including anhedonia and cognition, functioning and quality of life, patient-reported outcomes, and mechanistic readouts (for example, inflammatory markers, circuit or plasticity measures, digital behavior). Timing. Classic trials emphasized 6–8-week acute response with relatively sparse visits; new designs layer dense early sampling windows (hours to days for rapid-acting agents) onto longer follow-up to 6–12 months, enabling characterization of onset, offset and relapse dynamics. Stratification. Earlier studies used minimal or post-hoc subgrouping (for example, melancholic versus atypical) and randomization only at the syndrome level; contemporary designs prespecify strata and enrichment rules based on clinical staging, comorbidity clusters, biomarkers (such as inflammation or KYN metrics), cognitive or circuit biotypes, and sometimes deploy adaptive or umbrella/basket architectures. Durability. Historically, continuation and maintenance phases were optional or handled in separate extension studies; current trials increasingly embed durability as a co-primary objective, tracking time to relapse, sustained response, taper/discontinuation effects and real-world effectiveness via registries or digital follow-up, thereby aligning trial design with the long-term course of depressive illness. HAM-D, Hamilton Depression Rating Scale; KYN, kynurenine; MADRS, Montgomery–Åsberg Depression Rating Scale; MDD, major depressive disorder.
6. What We Got Wrong/Right
Many of the field’s “failures” now look like solvable design problems rather than fatal errors [147,148]. Trial and error prescribing, short term symptom focused trials, and inflated remission estimates exposed what happens when heterogeneity is ignored and protocols drift [147,149,150]. The corrective principles are clearer now: implement decision support and data driven personalization, redesign trials to prioritize long term functioning and real-world effectiveness and adhere strictly to pre specified protocols with transparent reporting [151,152,153]. The concept of difficult to treat depression and consensus definitions of TRD are direct products of these lessons [104,154,155].
A second cluster of mistakes involved what and whom we chose to measure [156,157]. Overbroad diagnostic criteria without biomarkers, unclear psychotherapy “active ingredients,” late recognition of comorbidity, and neglect of patient preference and digital engagement all narrowed impact [147,158,159,160]. The responses are already reshaping practice [161]. Biomarker informed and endophenotype based frameworks, component focused psychotherapy trials, integrated care models, shared decision tools, guided digital and blended interventions, and Delphi based TRD guidelines collectively represent durable gains and a more realistic architecture for precision psychiatry [104,155,159,162].
7. Outlook
The next decade will be judged by whether it can turn systems psychiatry from an attractive narrative into falsifiable science [163,164]. Two preclinical predictions are within reach. First, that manipulating specific prefrontal–striatal and prefrontal–limbic circuits in sex balanced, chronic stress models will yield biotypes that map onto human imaging defined network patterns and differential treatment response [165,166,167]. Second, that patient derived cellular systems combined with multi-omic profiling will prospectively predict which immune and metabolic perturbations in animals reproduce anhedonia dominant, inflammation high phenotypes observed in humans [134,168].
On the clinical side, trial design must shift in two concrete ways. Large, multivariate, cross trial prediction studies should be powered not only to detect average effects but to learn stable individual level treatment rules [169,170,171]. In parallel, factorial and adaptive designs need to dissect psychotherapy and combined treatment “active ingredients” rather than testing monolithic packages [172,173,174,175].
A viable implementation pathway is hybrid effectiveness implementation research embedded in integrated care, where stratification tools, targeted pharmacotherapy, and digital monitoring are co designed with health systems [176]. Underpinning all of this should be a shared data standard that harmonizes symptom networks, EEG and imaging markers, and trial metadata, with preregistered analytic pipelines and mandatory external validation [177,178].
8. Conclusions
In this perspectives review, I propose plasticity centered systems psychiatry as the key lens through which both model building and bedside decisions can be restructured. Synaptic remodeling, circuit dynamics, immune metabolic context, and sleep dependent homeostasis become explicit levers for intervention rather than diffuse background. A concrete practice change is to implement structured, plasticity informed care pathways that link symptom profiles to simple circuit sensitive indices such as reward tasks, sleep and circadian metrics, and low burden immune or metabolic panels. A parallel research change is to develop adaptive, multimodal platforms in which the ten subsequent papers systematically interrogate promising synaptic, microcircuit, network, immune, and chronobiological targets for depression treatment.
Author Contributions
Conceptualization, M.T.; methodology, M.T.; software, M.T.; validation, M.T.; formal analysis, M.T.; investigation, M.T.; resources, M.T.; data curation, M.T.; writing—original draft preparation, M.T.; writing—review and editing, M.T.; visualization, M.T.; supervision, M.T.; project administration, M.T.; funding acquisition, M.T. Author has read and agreed to the published version of the manuscript.
Funding
This work was supported by the HUN-REN Hungarian Research Network.
Acknowledgments
The graphical abstract and figures are created using biorender.com (accessed on 1 December 2025)
Conflicts of Interest
The author declares no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| 5-CSRTT | five-choice serial reaction time task |
| AhR | aryl hydrocarbon receptor |
| AMPA | α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid |
| ATAC | assay for transposase-accessible chromatin |
| BMI | body mass index |
| BOLD | blood-oxygen-level–dependent |
| CANTAB | Cambridge Neuropsychological Test Automated Battery |
| CRP | C-reactive protein |
| CSF1R | colony-stimulating factor 1 receptor |
| Dex/CRH | dexamethasone/corticotropin-releasing hormone |
| DLMO | dim light melatonin onset |
| DLPFC | dorsolateral prefrontal cortex |
| DNMTs | DNA methyltransferases |
| DSM | Diagnostic and Statistical Manual of Mental Disorders |
| EEG | electroencephalography |
| EefRT | Effort Expenditure for Rewards Task |
| eEPSPs | evoked excitatory postsynaptic potentials |
| ERK | extracellular signal-regulated kinase |
| EMG | electromyography |
| fMRI | functional magnetic resonance imaging |
| GABA | γ-aminobutyric acid |
| GLP-1 | glucagon-like peptide-1 |
| GR | glucocorticoid receptor |
| HAM-D | Hamilton Depression Rating Scale |
| HbA1c | glycated hemoglobin |
| HDACs | histone deacetylases |
| HOMA-IR | homeostatic model assessment of insulin resistance |
| HPA | hypothalamic–pituitary–adrenal axis |
| IDO | indoleamine 2,3-dioxygenase |
| IFN-α | interferon-alpha |
| IL-6 | interleukin-6 |
| IPSPs | inhibitory postsynaptic potentials |
| κ | kappa |
| KYN | kynurenine |
| KYNA | kynurenic acid |
| LFP | local field potential |
| LPS | lipopolysaccharide |
| LSD1 | lysine-specific demethylase 1 |
| LTD | long-term depression |
| LTP | long-term potentiation |
| MADRS | Montgomery–Åsberg Depression Rating Scale |
| MDD | major depressive disorder |
| MEG | magnetoencephalography |
| NMDA | N-methyl-D-aspartate |
| PET | positron emission tomography |
| PFC | prefrontal cortex |
| QA | quinolinic acid |
| RDoC | Research Domain Criteria |
| REM | rapid eye movement |
| RNA | ribonucleic acid |
| rsfMRI | resting-state functional magnetic resonance imaging |
| SCC | subcallosal cingulate cortex |
| T2D | type 2 diabetes |
| TDO | tryptophan 2,3-dioxygenase |
| TMS | transcranial magnetic stimulation |
| TMS-EEG | transcranial magnetic stimulation–electroencephalography |
| TNF | tumor necrosis factor |
| TRD | treatment-resistant depression |
| Trp | tryptophan |
| vmPFC | ventromedial prefrontal cortex |
| VNS | vagus nerve stimulation |
References
- Hirschfeld, R.M. History and evolution of the monoamine hypothesis of depression. J Clin Psychiatry 2000, 61 Suppl 6, 4-6.
- Boku, S.; Nakagawa, S.; Toda, H.; Hishimoto, A. Neural basis of major depressive disorder: Beyond monoamine hypothesis. Psychiatry Clin Neurosci 2018, 72, 3-12. [CrossRef]
- Liu, B.; Liu, J.; Wang, M.; Zhang, Y.; Li, L. From Serotonin to Neuroplasticity: Evolvement of Theories for Major Depressive Disorder. Front Cell Neurosci 2017, 11, 305. [CrossRef]
- Spellman, T.; Liston, C. Toward Circuit Mechanisms of Pathophysiology in Depression. Am J Psychiatry 2020, 177, 381-390. [CrossRef]
- Fries, G.R.; Saldana, V.A.; Finnstein, J.; Rein, T. Molecular pathways of major depressive disorder converge on the synapse. Mol Psychiatry 2023, 28, 284-297. [CrossRef]
- Brandl, F.; Weise, B.; Mulej Bratec, S.; Jassim, N.; Hoffmann Ayala, D.; Bertram, T.; Ploner, M.; Sorg, C. Common and specific large-scale brain changes in major depressive disorder, anxiety disorders, and chronic pain: a transdiagnostic multimodal meta-analysis of structural and functional MRI studies. Neuropsychopharmacology 2022, 47, 1071-1080. [CrossRef]
- Sindermann, L.; Redlich, R.; Opel, N.; Böhnlein, J.; Dannlowski, U.; Leehr, E.J. Systematic transdiagnostic review of magnetic-resonance imaging results: Depression, anxiety disorders and their co-occurrence. J Psychiatr Res 2021, 142, 226-239. [CrossRef]
- Arnaud, A.M.; Brister, T.S.; Duckworth, K.; Foxworth, P.; Fulwider, T.; Suthoff, E.D.; Werneburg, B.; Aleksanderek, I.; Reinhart, M.L. Impact of Major Depressive Disorder on Comorbidities: A Systematic Literature Review. J Clin Psychiatry 2022, 83. [CrossRef]
- Tanaka, M.; Battaglia, S.; Liloia, D. Navigating Neurodegeneration: Integrating Biomarkers, Neuroinflammation, and Imaging in Parkinson's, Alzheimer's, and Motor Neuron Disorders. Biomedicines 2025, 13. [CrossRef]
- Berk, M.; Köhler-Forsberg, O.; Turner, M.; Penninx, B.; Wrobel, A.; Firth, J.; Loughman, A.; Reavley, N.J.; McGrath, J.J.; Momen, N.C.; et al. Comorbidity between major depressive disorder and physical diseases: a comprehensive review of epidemiology, mechanisms and management. World Psychiatry 2023, 22, 366-387. [CrossRef]
- Tanaka, M.; Battaglia, S. From Biomarkers to Behavior: Mapping the Neuroimmune Web of Pain, Mood, and Memory. Biomedicines 2025, 13. [CrossRef]
- Bottaccioli, A.G.; Bologna, M.; Bottaccioli, F. Rethinking Depression-Beyond Neurotransmitters: An Integrated Psychoneuroendocrineimmunology Framework for Depression's Pathophysiology and Tailored Treatment. Int J Mol Sci 2025, 26. [CrossRef]
- Tozzi, L.; Zhang, X.; Pines, A.; Olmsted, A.M.; Zhai, E.S.; Anene, E.T.; Chesnut, M.; Holt-Gosselin, B.; Chang, S.; Stetz, P.C.; et al. Personalized brain circuit scores identify clinically distinct biotypes in depression and anxiety. Nat Med 2024, 30, 2076-2087. [CrossRef]
- Jiao, W.; Lin, J.; Deng, Y.; Ji, Y.; Liang, C.; Wei, S.; Jing, X.; Yan, F. The immunological perspective of major depressive disorder: unveiling the interactions between central and peripheral immune mechanisms. J Neuroinflammation 2025, 22, 10. [CrossRef]
- Tanaka, M.; Battaglia, S. Dualistic Dynamics in Neuropsychiatry: From Monoaminergic Modulators to Multiscale Biomarker Maps. Biomedicines 2025, 13. [CrossRef]
- Drevets, W.C.; Wittenberg, G.M.; Bullmore, E.T.; Manji, H.K. Immune targets for therapeutic development in depression: towards precision medicine. Nat Rev Drug Discov 2022, 21, 224-244. [CrossRef]
- Tafet, G.E.; Nemeroff, C.B. The Links Between Stress and Depression: Psychoneuroendocrinological, Genetic, and Environmental Interactions. J Neuropsychiatry Clin Neurosci 2016, 28, 77-88. [CrossRef]
- Yankelevitch-Yahav, R.; Franko, M.; Huly, A.; Doron, R. The forced swim test as a model of depressive-like behavior. J Vis Exp 2015. [CrossRef]
- Yan, H.C.; Cao, X.; Das, M.; Zhu, X.H.; Gao, T.M. Behavioral animal models of depression. Neurosci Bull 2010, 26, 327-337. [CrossRef]
- Dale, E.; Bang-Andersen, B.; Sánchez, C. Emerging mechanisms and treatments for depression beyond SSRIs and SNRIs. Biochem Pharmacol 2015, 95, 81-97. [CrossRef]
- Abelaira, H.M.; Réus, G.Z.; Quevedo, J. Animal models as tools to study the pathophysiology of depression. Braz J Psychiatry 2013, 35 Suppl 2, S112-120. [CrossRef]
- Sharma, S.; Chawla, S.; Kumar, P.; Ahmad, R.; Kumar Verma, P. The chronic unpredictable mild stress (CUMS) Paradigm: Bridging the gap in depression research from bench to bedside. Brain Res 2024, 1843, 149123. [CrossRef]
- Ji, N.; Lei, M.; Chen, Y.; Tian, S.; Li, C.; Zhang, B. How Oxidative Stress Induces Depression? ASN Neuro 2023, 15, 17590914231181037. [CrossRef]
- Bech, P. Modern psychometrics in clinimetrics: impact on clinical trials of antidepressants. Psychother Psychosom 2004, 73, 134-138. [CrossRef]
- Regier, D.A.; Narrow, W.E.; Kuhl, E.A.; Kupfer, D.J. The conceptual development of DSM-V. Am J Psychiatry 2009, 166, 645-650. [CrossRef]
- Hengartner, M.P.; Jakobsen, J.C.; Sørensen, A.; Plöderl, M. Efficacy of new-generation antidepressants assessed with the Montgomery-Asberg Depression Rating Scale, the gold standard clinician rating scale: A meta-analysis of randomised placebo-controlled trials. PLoS One 2020, 15, e0229381. [CrossRef]
- Khan, A.; Khan, S.R.; Shankles, E.B.; Polissar, N.L. Relative sensitivity of the Montgomery-Asberg Depression Rating Scale, the Hamilton Depression rating scale and the Clinical Global Impressions rating scale in antidepressant clinical trials. Int Clin Psychopharmacol 2002, 17, 281-285. [CrossRef]
- Guizzaro, L.; Morgan, D.D.V.; Falco, A.; Gallo, C. Hamilton scale and MADRS are interchangeable in meta-analyses but can disagree at trial level. J Clin Epidemiol 2020, 124, 106-117. [CrossRef]
- Leucht, S.; Fennema, H.; Engel, R.R.; Kaspers-Janssen, M.; Szegedi, A. Translating the HAM-D into the MADRS and vice versa with equipercentile linking. J Affect Disord 2018, 226, 326-331. [CrossRef]
- Santi, N.S.; Biswal, S.B.; Naik, B.N.; Sahoo, J.P.; Rath, B. Comparison of Hamilton Depression Rating Scale and Montgomery-Åsberg Depression Rating Scale: Baked Straight From a Randomized Study. Cureus 2023, 15, e45098. [CrossRef]
- Ratheesh, A.; Berk, M.; Schmaal, L. Can we overcome the heterogeneity of mood disorders in clinical trials? Aust N Z J Psychiatry 2023, 57, 309-311. [CrossRef]
- Su, Z.; Yang, X.; Hou, J.; Liu, S.; Wang, Y.; Chen, Z. Gender differences in the co-occurrence of anxiety and depressive symptoms among early adolescents: A network approach. J Psychiatr Res 2024, 179, 300-305. [CrossRef]
- Vasiliadis, H.M.; Desjardins, F.; Roberge, P.; Grenier, S. Sex Differences in Anxiety Disorders in Older Adults. Curr Psychiatry Rep 2020, 22, 75. [CrossRef]
- Thompson, K.N.; Hübel, C.; Cheesman, R.; Adey, B.N.; Armour, C.; Davies, M.R.; Hotopf, M.; Jones, I.R.; Kalsi, G.; McIntosh, A.M.; et al. Age and sex-related variability in the presentation of generalized anxiety and depression symptoms. Depress Anxiety 2021, 38, 1054-1065. [CrossRef]
- Pavlidi, P.; Kokras, N.; Dalla, C. Sex Differences in Depression and Anxiety. Curr Top Behav Neurosci 2023, 62, 103-132. [CrossRef]
- Kuper, P.; Miguel, C.; Cuijpers, P.; Apfelbacher, C.; Buntrock, C.; Karyotaki, E.; Sprenger, A.A.; Harrer, M. Sample size and geographical region predict effect heterogeneity in psychotherapy research for depression: a meta-epidemiological study. J Clin Epidemiol 2025, 183, 111779. [CrossRef]
- Cai, N.; Choi, K.W.; Fried, E.I. Reviewing the genetics of heterogeneity in depression: operationalizations, manifestations and etiologies. Hum Mol Genet 2020, 29, R10-r18. [CrossRef]
- Hickie, I.B.; Berk, M.; Scott, J.; Crouse, J.; Scott, E.; Wray, N.; Iorfino, F. What are the best strategies for stratification of clinical cohorts with depression and other mood disorders? Research Directions: Depression 2024, 1, e18.
- Dunlop, K.; Grosenick, L.; Downar, J.; Vila-Rodriguez, F.; Gunning, F.M.; Daskalakis, Z.J.; Blumberger, D.M.; Liston, C. Dimensional and categorical solutions to parsing depression heterogeneity in a large single-site sample. Biological Psychiatry 2024, 96, 422-434.
- Marsden, W.N. Synaptic plasticity in depression: molecular, cellular and functional correlates. Prog Neuropsychopharmacol Biol Psychiatry 2013, 43, 168-184. [CrossRef]
- Shenoy, S.; Ibrahim, S. Perinatal Depression and the Role of Synaptic Plasticity in Its Pathogenesis and Treatment. Behav Sci (Basel) 2023, 13. [CrossRef]
- Brown, J.C.; Higgins, E.S.; George, M.S. Synaptic Plasticity 101: The Story of the AMPA Receptor for the Brain Stimulation Practitioner. Neuromodulation 2022, 25, 1289-1298. [CrossRef]
- He, J.G.; Zhou, H.Y.; Wang, F.; Chen, J.G. Dysfunction of Glutamatergic Synaptic Transmission in Depression: Focus on AMPA Receptor Trafficking. Biol Psychiatry Glob Open Sci 2023, 3, 187-196. [CrossRef]
- Brager, D.H.; Johnston, D. Plasticity of intrinsic excitability during long-term depression is mediated through mGluR-dependent changes in I(h) in hippocampal CA1 pyramidal neurons. J Neurosci 2007, 27, 13926-13937. [CrossRef]
- Cavalleri, L.; Merlo Pich, E.; Millan, M.J.; Chiamulera, C.; Kunath, T.; Spano, P.F.; Collo, G. Ketamine enhances structural plasticity in mouse mesencephalic and human iPSC-derived dopaminergic neurons via AMPAR-driven BDNF and mTOR signaling. Mol Psychiatry 2018, 23, 812-823. [CrossRef]
- Appelbaum, L.G.; Shenasa, M.A.; Stolz, L.; Daskalakis, Z. Synaptic plasticity and mental health: methods, challenges and opportunities. Neuropsychopharmacology 2023, 48, 113-120. [CrossRef]
- Cantone, M.; Bramanti, A.; Lanza, G.; Pennisi, M.; Bramanti, P.; Pennisi, G.; Bella, R. Cortical Plasticity in Depression. ASN Neuro 2017, 9, 1759091417711512. [CrossRef]
- Hu, Y.T.; Tan, Z.L.; Hirjak, D.; Northoff, G. Brain-wide changes in excitation-inhibition balance of major depressive disorder: a systematic review of topographic patterns of GABA- and glutamatergic alterations. Mol Psychiatry 2023, 28, 3257-3266. [CrossRef]
- Fee, C.; Banasr, M.; Sibille, E. Somatostatin-Positive Gamma-Aminobutyric Acid Interneuron Deficits in Depression: Cortical Microcircuit and Therapeutic Perspectives. Biol Psychiatry 2017, 82, 549-559. [CrossRef]
- Kuki, T.; Fujihara, K.; Miwa, H.; Tamamaki, N.; Yanagawa, Y.; Mushiake, H. Contribution of parvalbumin and somatostatin-expressing GABAergic neurons to slow oscillations and the balance in beta-gamma oscillations across cortical layers. Front Neural Circuits 2015, 9, 6. [CrossRef]
- Chen, G.; Zhang, Y.; Li, X.; Zhao, X.; Ye, Q.; Lin, Y.; Tao, H.W.; Rasch, M.J.; Zhang, X. Distinct Inhibitory Circuits Orchestrate Cortical beta and gamma Band Oscillations. Neuron 2017, 96, 1403-1418.e1406. [CrossRef]
- Tsuboi, D.; Nagai, T.; Yoshimoto, J.; Kaibuchi, K. Neuromodulator regulation and emotions: insights from the crosstalk of cell signaling. Front Mol Neurosci 2024, 17, 1376762. [CrossRef]
- Wagatsuma, N.; Nobukawa, S.; Fukai, T. A microcircuit model involving parvalbumin, somatostatin, and vasoactive intestinal polypeptide inhibitory interneurons for the modulation of neuronal oscillation during visual processing. Cereb Cortex 2023, 33, 4459-4477. [CrossRef]
- Tahvili, F.; Vinck, M.; di Volo, M. PV and SOM cells play distinct causal roles in controlling network oscillations and stability. Cell Rep 2025, 44, 116131. [CrossRef]
- Mazza, F.; Guet-McCreight, A.; Valiante, T.A.; Griffiths, J.D.; Hay, E. In-silico EEG biomarkers of reduced inhibition in human cortical microcircuits in depression. PLoS Comput Biol 2023, 19, e1010986. [CrossRef]
- Rademacher, J.; Grent-'t-Jong, T.; Rivolta, D.; Sauer, A.; Scheller, B.; Gonzalez-Burgos, G.; Metzner, C.; Uhlhaas, P.J. Computational modeling of ketamine-induced changes in gamma-band oscillations: The contribution of parvalbumin and somatostatin interneurons. PLoS Comput Biol 2025, 21, e1013118. [CrossRef]
- Tanaka, M.; He, Z.; Han, S.; Battaglia, S. Editorial: Noninvasive brain stimulation: a promising approach to study and improve emotion regulation. Front Behav Neurosci 2025, 19, 1633936. [CrossRef]
- Bruijnzeel, A.W. kappa-Opioid receptor signaling and brain reward function. Brain Res Rev 2009, 62, 127-146. [CrossRef]
- Wallace, C.W.; Holleran, K.M.; Slinkard, C.Y.; Centanni, S.W.; Lapish, C.C.; Jones, S.R. Kappa opioid receptors diminish spontaneous dopamine signals in awake mice through multiple mechanisms. Neuropharmacology 2025, 273, 110458. [CrossRef]
- Bekhbat, M.; Li, Z.; Dunlop, B.W.; Treadway, M.T.; Mehta, N.D.; Revill, K.P.; Lucido, M.J.; Hong, C.; Ashchi, A.; Wommack, E.C.; et al. Sustained effects of repeated levodopa (L-DOPA) administration on reward circuitry, effort-based motivation, and anhedonia in depressed patients with higher inflammation. Brain Behav Immun 2025, 125, 240-248. [CrossRef]
- Treadway, M.; Etuk, S.; Cooper, J.; Hossein, S.; Hahn, E.; Betters, S.; Liu, S.; Arulpragasam, A.; DeVries, B.; Irfan, N.; et al. A randomized proof-of-mechanism trial of TNF antagonism for motivational anhedonia and related corticostriatal circuitry in depressed patients with high inflammation. Res Sq 2024. [CrossRef]
- Felger, J.C.; Treadway, M.T. Inflammation Effects on Motivation and Motor Activity: Role of Dopamine. Neuropsychopharmacology 2017, 42, 216-241. [CrossRef]
- Lucido, M.J.; Bekhbat, M.; Goldsmith, D.R.; Treadway, M.T.; Haroon, E.; Felger, J.C.; Miller, A.H. Aiding and Abetting Anhedonia: Impact of Inflammation on the Brain and Pharmacological Implications. Pharmacol Rev 2021, 73, 1084-1117. [CrossRef]
- Hasbi, A.; Madras, B.K.; George, S.R. Daily Δ(9)-Tetrahydrocannabinol and Withdrawal Increase Dopamine D(1)-D(2) Receptor Heteromer to Mediate Anhedonia- and Anxiogenic-like Behavior Through a Dynorphin and Kappa Opioid Receptor Mechanism. Biol Psychiatry Glob Open Sci 2023, 3, 550-566. [CrossRef]
- Thomas, C.S.; Mohammadkhani, A.; Rana, M.; Qiao, M.; Baimel, C.; Borgland, S.L. Optogenetic stimulation of lateral hypothalamic orexin/dynorphin inputs in the ventral tegmental area potentiates mesolimbic dopamine neurotransmission and promotes reward-seeking behaviours. Neuropsychopharmacology 2022, 47, 728-740. [CrossRef]
- Albrecht, U. Molecular Mechanisms in Mood Regulation Involving the Circadian Clock. Front Neurol 2017, 8, 30. [CrossRef]
- Focke, C.M.B.; Iremonger, K.J. Rhythmicity matters: Circadian and ultradian patterns of HPA axis activity. Mol Cell Endocrinol 2020, 501, 110652. [CrossRef]
- Nader, N.; Chrousos, G.P.; Kino, T. Interactions of the circadian CLOCK system and the HPA axis. Trends Endocrinol Metab 2010, 21, 277-286. [CrossRef]
- Lightman, S.L.; Birnie, M.T.; Conway-Campbell, B.L. Dynamics of ACTH and Cortisol Secretion and Implications for Disease. Endocr Rev 2020, 41. [CrossRef]
- Carpenter, J.S.; Crouse, J.J.; Shin, M.; Tonini, E.; Hindmarsh, G.; de Haan, Z.; Iorfino, F.; Robillard, R.; Naismith, S.; Scott, E.M.; et al. Evidence for Internal Misalignment of Circadian Rhythms in Youth With Emerging Mood Disorders. J Biol Rhythms 2025, 40, 424-440. [CrossRef]
- Skubic, C.; Zevnik, U.; Nahtigal, K.; Dolenc Grošelj, L.; Rozman, D. Circadian Biomarkers in Humans: Methodological Insights into the Detection of Melatonin and Cortisol. Biomolecules 2025, 15. [CrossRef]
- Schrire, Z.M.; Naismith, S.L.; Pye, J.; Duffy, S.L.; Gordon, C.J.; Lewis, S.J.; Hoyos, C.M. Circadian rhythms and misalignment in older adults and those ‘at risk’for dementia: A study examining correlates of dim-light melatonin onset: Biomarkers (non-neuroimaging)/Prognostic utility. Alzheimer's & Dementia 2020, 16, e045525.
- Scott, M.R.; McClung, C.A. Circadian Rhythms in Mood Disorders. Adv Exp Med Biol 2021, 1344, 153-168. [CrossRef]
- Johnson, C.; Brzezynski, J.; Bair, A.; Smieszek, S.; Bai, H.; Polymeropoulos, C.; Birznieks, G.; Polymeropoulos, M. 0879 Dim Light Melatonin Onset in a Delayed Sleep-Wake Phase Disorder Cohort: Ongoing Clinical Trial Update. Sleep 2025, 48, A382-A382.
- Tanaka, M.; Tóth, F.; Polyák, H.; Szabó, Á.; Mándi, Y.; Vécsei, L. Immune Influencers in Action: Metabolites and Enzymes of the Tryptophan-Kynurenine Metabolic Pathway. Biomedicines 2021, 9. [CrossRef]
- Badawy, A.A. Kynurenine Pathway of Tryptophan Metabolism: Regulatory and Functional Aspects. Int J Tryptophan Res 2017, 10, 1178646917691938. [CrossRef]
- Salminen, A. Role of indoleamine 2,3-dioxygenase 1 (IDO1) and kynurenine pathway in the regulation of the aging process. Ageing Res Rev 2022, 75, 101573. [CrossRef]
- Stone, T.W.; Williams, R.O. Tryptophan metabolism as a 'reflex' feature of neuroimmune communication: Sensor and effector functions for the indoleamine-2, 3-dioxygenase kynurenine pathway. J Neurochem 2024, 168, 3333-3357. [CrossRef]
- MacDowell, K.S.; Munarriz-Cuezva, E.; Meana, J.J.; Leza, J.C.; Ortega, J.E. Paliperidone Reversion of Maternal Immune Activation-Induced Changes on Brain Serotonin and Kynurenine Pathways. Front Pharmacol 2021, 12, 682602. [CrossRef]
- Pathak, S.; Nadar, R.; Kim, S.; Liu, K.; Govindarajulu, M.; Cook, P.; Watts Alexander, C.S.; Dhanasekaran, M.; Moore, T. The Influence of Kynurenine Metabolites on Neurodegenerative Pathologies. Int J Mol Sci 2024, 25. [CrossRef]
- Schröcksnadel, K.; Wirleitner, B.; Winkler, C.; Fuchs, D. Monitoring tryptophan metabolism in chronic immune activation. Clin Chim Acta 2006, 364, 82-90. [CrossRef]
- Alfaro-Rodríguez, A.; Reyes-Long, S.; Roldan-Valadez, E.; González-Torres, M.; Bonilla-Jaime, H.; Bandala, C.; Avila-Luna, A.; Bueno-Nava, A.; Cabrera-Ruiz, E.; Sanchez-Aparicio, P.; et al. Association of the Serotonin and Kynurenine Pathways as Possible Therapeutic Targets to Modulate Pain in Patients with Fibromyalgia. Pharmaceuticals (Basel) 2024, 17. [CrossRef]
- Szabó, Á.; Galla, Z.; Spekker, E.; Martos, D.; Szűcs, M.; Fejes-Szabó, A.; Fehér, Á.; Takeda, K.; Ozaki, K.; Inoue, H.; et al. Behavioral Balance in Tryptophan Turmoil: Regional Metabolic Rewiring in Kynurenine Aminotransferase II Knockout Mice. Cells 2025, 14. [CrossRef]
- Tanaka, M.; Vécsei, L. From Microbial Switches to Metabolic Sensors: Rewiring the Gut-Brain Kynurenine Circuit. Biomedicines 2025, 13. [CrossRef]
- Martos, D.; Lőrinczi, B.; Szatmári, I.; Vécsei, L.; Tanaka, M. Decoupling Behavioral Domains via Kynurenic Acid Analog Optimization: Implications for Schizophrenia and Parkinson's Disease Therapeutics. Cells 2025, 14. [CrossRef]
- Juhász, L.; Spisák, K.; Szolnoki, B.Z.; Nászai, A.; Szabó, Á.; Rutai, A.; Tallósy, S.P.; Szabó, A.; Toldi, J.; Tanaka, M.; et al. The Power Struggle: Kynurenine Pathway Enzyme Knockouts and Brain Mitochondrial Respiration. J Neurochem 2025, 169, e70075. [CrossRef]
- Tanaka, M.; Szatmári, I.; Vécsei, L. Quinoline Quest: Kynurenic Acid Strategies for Next-Generation Therapeutics via Rational Drug Design. Pharmaceuticals (Basel) 2025, 18. [CrossRef]
- Naffaa, M.M. Mechanisms of astrocytic and microglial purinergic signaling in homeostatic regulation and implications for neurological disease. Exploration of Neuroscience 2025, 4, 100676.
- Bedetta, M.; Pizzo, P.; Lia, A. The Multifaceted Role of P2X7R in Microglia and Astrocytes. Neurochem Res 2025, 50, 239. [CrossRef]
- Batista, A.F.; Khan, K.A.; Papavergi, M.T.; Lemere, C.A. The Importance of Complement-Mediated Immune Signaling in Alzheimer's Disease Pathogenesis. Int J Mol Sci 2024, 25. [CrossRef]
- Liu, Y.D.; Chang, Y.H.; Xie, X.T.; Wang, X.Y.; Ma, H.Y.; Liu, M.C.; Zhang, H.M. PET Imaging Unveils Neuroinflammatory Mechanisms in Psychiatric Disorders: From Microglial Activation to Therapeutic Innovation. Mol Neurobiol 2025, 62, 15318-15335. [CrossRef]
- Werry, E.L.; Bright, F.M.; Piguet, O.; Ittner, L.M.; Halliday, G.M.; Hodges, J.R.; Kiernan, M.C.; Loy, C.T.; Kril, J.J.; Kassiou, M. Recent Developments in TSPO PET Imaging as A Biomarker of Neuroinflammation in Neurodegenerative Disorders. Int J Mol Sci 2019, 20. [CrossRef]
- Enache, D.; Pariante, C.M.; Mondelli, V. Markers of central inflammation in major depressive disorder: A systematic review and meta-analysis of studies examining cerebrospinal fluid, positron emission tomography and post-mortem brain tissue. Brain Behav Immun 2019, 81, 24-40. [CrossRef]
- Dupont, A.C.; Largeau, B.; Santiago Ribeiro, M.J.; Guilloteau, D.; Tronel, C.; Arlicot, N. Translocator Protein-18 kDa (TSPO) Positron Emission Tomography (PET) Imaging and Its Clinical Impact in Neurodegenerative Diseases. Int J Mol Sci 2017, 18. [CrossRef]
- Meyer, J.H.; Cervenka, S.; Kim, M.J.; Kreisl, W.C.; Henter, I.D.; Innis, R.B. Neuroinflammation in psychiatric disorders: PET imaging and promising new targets. Lancet Psychiatry 2020, 7, 1064-1074. [CrossRef]
- Baek, S.Y.; Lee, J.; Kim, T.; Lee, H.; Choi, H.S.; Park, H.; Koh, M.; Kim, E.; Jung, M.E.; Iliopoulos, D.; et al. Development of a novel histone deacetylase inhibitor unveils the role of HDAC11 in alleviating depression by inhibition of microglial activation. Biomed Pharmacother 2023, 166, 115312. [CrossRef]
- Du, J.; Liu, R.; Ma, L.; Liu, Y.; Wei, W.; Liu, N.; Cao, Q.; Yu, J. Novel histone deacetylase-5 inhibitor T2943 exerts an anti-depressive effect in mice by enhancing GRID1 expression. Sci Rep 2025, 15, 4522. [CrossRef]
- Sun, Z.; Zhang, B.; Zhou, J.; Luo, Y.; Zhu, X.; Wang, Y.; He, Y.; Zheng, P.; Zhang, L.; Yang, J.; et al. Integrated Single-Cell RNA-seq and ATAC-seq Reveals Heterogeneous Differentiation of CD4(+) Naive T Cell Subsets is Associated with Response to Antidepressant Treatment in Major Depressive Disorder. Adv Sci (Weinh) 2024, 11, e2308393. [CrossRef]
- Taavitsainen, S.; Engedal, N.; Cao, S.; Handle, F.; Erickson, A.; Prekovic, S.; Wetterskog, D.; Tolonen, T.; Vuorinen, E.M.; Kiviaho, A.; et al. Single-cell ATAC and RNA sequencing reveal pre-existing and persistent cells associated with prostate cancer relapse. Nat Commun 2021, 12, 5307. [CrossRef]
- Grandi, F.C.; Modi, H.; Kampman, L.; Corces, M.R. Chromatin accessibility profiling by ATAC-seq. Nat Protoc 2022, 17, 1518-1552. [CrossRef]
- Kajumba, M.M.; Kakooza-Mwesige, A.; Nakasujja, N.; Koltai, D.; Canli, T. Treatment-resistant depression: molecular mechanisms and management. Mol Biomed 2024, 5, 43. [CrossRef]
- Daeli, J.I.D.; Soemara, A. How Do Combined Pharmacological And Psychotherapeutic Interventions Impact Treatment Outcomes For Patients With Treatment-Resistant Major Depressive Disorder?: A Systematic Review. The International Journal of Medical Science and Health Research 2025, 12, 49-99.
- Ruberto, V.L.; Jha, M.K.; Murrough, J.W. Pharmacological Treatments for Patients with Treatment-Resistant Depression. Pharmaceuticals (Basel) 2020, 13. [CrossRef]
- McIntyre, R.S.; Alsuwaidan, M.; Baune, B.T.; Berk, M.; Demyttenaere, K.; Goldberg, J.F.; Gorwood, P.; Ho, R.; Kasper, S.; Kennedy, S.H.; et al. Treatment-resistant depression: definition, prevalence, detection, management, and investigational interventions. World Psychiatry 2023, 22, 394-412. [CrossRef]
- Amasi-Hartoonian, N.; Pariante, C.M.; Cattaneo, A.; Sforzini, L. Understanding treatment-resistant depression using "omics" techniques: A systematic review. J Affect Disord 2022, 318, 423-455. [CrossRef]
- Garcia, G.; Cotner, C.; Spano, R. Precision medicine in psychiatry: Case series on pharmacogenomic solutions for treatment-resistant depression. J Am Assoc Nurse Pract 2025, 37, 471-476. [CrossRef]
- Baum, M.L.; Widge, A.S.; Carpenter, L.L.; McDonald, W.M.; Cohen, B.M.; Nemeroff, C.B. Pharmacogenomic Clinical Support Tools for the Treatment of Depression. Am J Psychiatry 2024, 181, 591-607. [CrossRef]
- Young, J.W. Development of cross-species translational paradigms for psychiatric research in the Research Domain Criteria era. Neurosci Biobehav Rev 2023, 148, 105119. [CrossRef]
- Iturra-Mena, A.M.; Kangas, B.D.; Luc, O.T.; Potter, D.; Pizzagalli, D.A. Electrophysiological signatures of reward learning in the rodent touchscreen-based Probabilistic Reward Task. Neuropsychopharmacology 2023, 48, 700-709. [CrossRef]
- Cavanagh, J.F.; Olguin, S.L.; Talledo, J.A.; Kotz, J.E.; Roberts, B.Z.; Nungaray, J.A.; Sprock, J.; Gregg, D.; Bhakta, S.G.; Light, G.A.; et al. Amphetamine alters an EEG marker of reward processing in humans and mice. Psychopharmacology (Berl) 2022, 239, 923-933. [CrossRef]
- Pizzagalli, D.A.; Sherwood, R.J.; Henriques, J.B.; Davidson, R.J. Frontal brain asymmetry and reward responsiveness: a source-localization study. Psychol Sci 2005, 16, 805-813. [CrossRef]
- Kheirkhah, M.; Duncan, W.C., Jr.; Yuan, Q.; Wang, P.R.; Jamalabadi, H.; Leistritz, L.; Walter, M.; Goldman, D.; Zarate, C.A., Jr.; Hejazi, N.S. REM density predicts rapid antidepressant response to ketamine in individuals with treatment-resistant depression. Neuropsychopharmacology 2025, 50, 941-946. [CrossRef]
- Pesonen, A.K.; Gradisar, M.; Kuula, L.; Short, M.; Merikanto, I.; Tark, R.; Räikkönen, K.; Lahti, J. REM sleep fragmentation associated with depressive symptoms and genetic risk for depression in a community-based sample of adolescents. J Affect Disord 2019, 245, 757-763. [CrossRef]
- Lechinger, J.; Koch, J.; Weinhold, S.L.; Seeck-Hirschner, M.; Stingele, K.; Kropp-Näf, C.; Braun, M.; Drews, H.J.; Aldenhoff, J.; Huchzermeier, C.; et al. REM density is associated with treatment response in major depression: Antidepressant pharmacotherapy vs. psychotherapy. J Psychiatr Res 2021, 133, 67-72. [CrossRef]
- Luc, O.T.; Kangas, B.D. Validation of a touchscreen probabilistic reward task for mice: A reverse-translated assay with cross-species continuity. Cogn Affect Behav Neurosci 2024, 24, 281-288. [CrossRef]
- Palmer, D.; Dumont, J.R.; Dexter, T.D.; Prado, M.A.M.; Finger, E.; Bussey, T.J.; Saksida, L.M. Touchscreen cognitive testing: Cross-species translation and co-clinical trials in neurodegenerative and neuropsychiatric disease. Neurobiol Learn Mem 2021, 182, 107443. [CrossRef]
- Molendijk, M.L.; de Kloet, E.R. Coping with the forced swim stressor: Current state-of-the-art. Behav Brain Res 2019, 364, 1-10. [CrossRef]
- Commons, K.G.; Cholanians, A.B.; Babb, J.A.; Ehlinger, D.G. The Rodent Forced Swim Test Measures Stress-Coping Strategy, Not Depression-like Behavior. ACS Chem Neurosci 2017, 8, 955-960. [CrossRef]
- Molendijk, M.L.; de Kloet, E.R. Immobility in the forced swim test is adaptive and does not reflect depression. Psychoneuroendocrinology 2015, 62, 389-391. [CrossRef]
- Parekh, P.K.; Johnson, S.B.; Liston, C. Synaptic Mechanisms Regulating Mood State Transitions in Depression. Annu Rev Neurosci 2022, 45, 581-601. [CrossRef]
- Aleksandrova, L.R.; Wang, Y.T.; Phillips, A.G. Evaluation of the Wistar-Kyoto rat model of depression and the role of synaptic plasticity in depression and antidepressant response. Neurosci Biobehav Rev 2019, 105, 1-23. [CrossRef]
- Petković, A.; Chaudhury, D. Encore: Behavioural animal models of stress, depression and mood disorders. Front Behav Neurosci 2022, 16, 931964. [CrossRef]
- Della Valle, A.; De Carlo, S.; Sonsini, G.; Pilati, S.; Perali, A.; Ubaldi, M.; Ciccocioppo, R. Machine learning-based model for behavioural analysis in rodents applied to the forced swim test. Sci Rep 2025, 15, 22314. [CrossRef]
- Cuthbert, B.N. Research Domain Criteria (RDoC): Progress and Potential. Curr Dir Psychol Sci 2022, 31, 107-114. [CrossRef]
- Anderzhanova, E.; Kirmeier, T.; Wotjak, C.T. Animal models in psychiatric research: The RDoC system as a new framework for endophenotype-oriented translational neuroscience. Neurobiol Stress 2017, 7, 47-56. [CrossRef]
- Nusslock, R.; Alloy, L.B. Reward processing and mood-related symptoms: An RDoC and translational neuroscience perspective. J Affect Disord 2017, 216, 3-16. [CrossRef]
- Cavanagh, J.F.; Gregg, D.; Light, G.A.; Olguin, S.L.; Sharp, R.F.; Bismark, A.W.; Bhakta, S.G.; Swerdlow, N.R.; Brigman, J.L.; Young, J.W. Electrophysiological biomarkers of behavioral dimensions from cross-species paradigms. Transl Psychiatry 2021, 11, 482. [CrossRef]
- Fernandes, B.S.; Karmakar, C.; Tamouza, R.; Tran, T.; Yearwood, J.; Hamdani, N.; Laouamri, H.; Richard, J.R.; Yolken, R.; Berk, M.; et al. Precision psychiatry with immunological and cognitive biomarkers: a multi-domain prediction for the diagnosis of bipolar disorder or schizophrenia using machine learning. Transl Psychiatry 2020, 10, 162. [CrossRef]
- Sanislow, C.A.; Ferrante, M.; Pacheco, J.; Rudorfer, M.V.; Morris, S.E. Advancing Translational Research Using NIMH Research Domain Criteria and Computational Methods. Neuron 2019, 101, 779-782. [CrossRef]
- Morris, S.E.; Sanislow, C.A.; Pacheco, J.; Vaidyanathan, U.; Gordon, J.A.; Cuthbert, B.N. Revisiting the seven pillars of RDoC. BMC Med 2022, 20, 220. [CrossRef]
- Arns, M.; van Dijk, H.; Luykx, J.J.; van Wingen, G.; Olbrich, S. Stratified psychiatry: Tomorrow's precision psychiatry? Eur Neuropsychopharmacol 2022, 55, 14-19. [CrossRef]
- Milaneschi, Y.; Kappelmann, N.; Ye, Z.; Lamers, F.; Moser, S.; Jones, P.B.; Burgess, S.; Penninx, B.; Khandaker, G.M. Association of inflammation with depression and anxiety: evidence for symptom-specificity and potential causality from UK Biobank and NESDA cohorts. Mol Psychiatry 2021, 26, 7393-7402. [CrossRef]
- Tanaka, M. Special Issue "Translating Molecular Psychiatry: From Biomarkers to Personalized Therapies". Int J Mol Sci 2025, 26. [CrossRef]
- Bekhbat, M.; Treadway, M.T.; Goldsmith, D.R.; Woolwine, B.J.; Haroon, E.; Miller, A.H.; Felger, J.C. Gene signatures in peripheral blood immune cells related to insulin resistance and low tyrosine metabolism define a sub-type of depression with high CRP and anhedonia. Brain Behav Immun 2020, 88, 161-165. [CrossRef]
- Baune, B.T.; Fromme, S.E.; Aberg, M.; Adli, M.; Afantitis, A.; Akkouh, I.; Andreassen, O.A.; Angulo, C.; Barlati, S.; Brasso, C.; et al. A stratified treatment algorithm in psychiatry: a program on stratified pharmacogenomics in severe mental illness (Psych-STRATA): concept, objectives and methodologies of a multidisciplinary project funded by Horizon Europe. Eur Arch Psychiatry Clin Neurosci 2025, 275, 1453-1464. [CrossRef]
- Abi-Dargham, A.; Horga, G. The search for imaging biomarkers in psychiatric disorders. Nat Med 2016, 22, 1248-1255. [CrossRef]
- Guo, Q.; Guo, L.; Wang, Y.; Shang, S. Efficacy and safety of eight enhanced therapies for treatment-resistant depression: A systematic review and network meta-analysis of RCTs. Psychiatry Res 2024, 339, 116018. [CrossRef]
- Łysik, A.; Logoń, K.; Szczygieł, A.; Wołoszczak, J.; Wrześniewska, M.; Leszek, J. Innovative approaches in the treatment-resistant depression: exploring different therapeutic pathways. Geroscience 2025, 47, 5543-5558. [CrossRef]
- Salahudeen, M.S.; Wright, C.M.; Peterson, G.M. Esketamine: new hope for the treatment of treatment-resistant depression? A narrative review. Ther Adv Drug Saf 2020, 11, 2042098620937899. [CrossRef]
- Brietzke, E.; Hawken, E.R.; Idzikowski, M.; Pong, J.; Kennedy, S.H.; Soares, C.N. Integrating digital phenotyping in clinical characterization of individuals with mood disorders. Neurosci Biobehav Rev 2019, 104, 223-230. [CrossRef]
- Baldwin, H.; Loebel-Davidsohn, L.; Oliver, D.; Salazar de Pablo, G.; Stahl, D.; Riper, H.; Fusar-Poli, P. Real-World Implementation of Precision Psychiatry: A Systematic Review of Barriers and Facilitators. Brain Sci 2022, 12. [CrossRef]
- Dhieb, D.; Bastaki, K. Pharmaco-Multiomics: A New Frontier in Precision Psychiatry. Int J Mol Sci 2025, 26. [CrossRef]
- Zanardi, R.; Prestifilippo, D.; Fabbri, C.; Colombo, C.; Maron, E.; Serretti, A. Precision psychiatry in clinical practice. Int J Psychiatry Clin Pract 2021, 25, 19-27. [CrossRef]
- Fusar-Poli, P.; Manchia, M.; Koutsouleris, N.; Leslie, D.; Woopen, C.; Calkins, M.E.; Dunn, M.; Tourneau, C.L.; Mannikko, M.; Mollema, T.; et al. Ethical considerations for precision psychiatry: A roadmap for research and clinical practice. Eur Neuropsychopharmacol 2022, 63, 17-34. [CrossRef]
- Brown, J.E.H.; Young, J.L.; Martinez-Martin, N. Psychiatric genomics, mental health equity, and intersectionality: A framework for research and practice. Front Psychiatry 2022, 13, 1061705. [CrossRef]
- Giusti-Rodríguez, P.; Okewole, N.; Jain, S.; Montalvo-Ortiz, J.L.; Peterson, R.E. Diversifying Psychiatric Genomics: Globally Inclusive Strategies Toward Health Equity. Psychiatr Clin North Am 2025, 48, 241-256. [CrossRef]
- Blackburn, T.P. Depressive disorders: Treatment failures and poor prognosis over the last 50 years. Pharmacol Res Perspect 2019, 7, e00472. [CrossRef]
- Oasi, O.; Critchfield, K.L.; Werbart, A. Editorial: Rethinking unsuccessful psychotherapies: when and how do treatments fail? Front Psychol 2024, 15, 1514654. [CrossRef]
- Petter, J.; Schumacher, L.; Echterhoff, J.; Klein, J.P.; Schramm, E.; Härter, M.; Hautzinger, M.; Kriston, L. Heterogeneity of Treatment Outcomes Across Therapists and Sites in a Randomized Multicentre Psychotherapy Trial. Clin Psychol Psychother 2025, 32, e70087. [CrossRef]
- Huneke, N.T.M.; Fusetto Veronesi, G.; Garner, M.; Baldwin, D.S.; Cortese, S. Expectancy Effects, Failure of Blinding Integrity, and Placebo Response in Trials of Treatments for Psychiatric Disorders: A Narrative Review. JAMA Psychiatry 2025, 82, 531-538. [CrossRef]
- Bjurner, P.; Isacsson, N.H.; Abdesslem, F.B.; Boman, M.; Forsell, E.; Kaldo, V. Study protocol for a triple-blind randomised controlled trial evaluating a machine learning-based predictive clinical decision support tool for internet-delivered cognitive behaviour therapy (ICBT) for depression and anxiety. Internet Interv 2025, 40, 100816. [CrossRef]
- Lutz, W.; Deisenhofer, A.K.; Rubel, J.; Bennemann, B.; Giesemann, J.; Poster, K.; Schwartz, B. Prospective evaluation of a clinical decision support system in psychological therapy. J Consult Clin Psychol 2022, 90, 90-106. [CrossRef]
- Kwan, J.L.; Lo, L.; Ferguson, J.; Goldberg, H.; Diaz-Martinez, J.P.; Tomlinson, G.; Grimshaw, J.M.; Shojania, K.G. Computerised clinical decision support systems and absolute improvements in care: meta-analysis of controlled clinical trials. Bmj 2020, 370, m3216. [CrossRef]
- Rybak, Y.E.; Lai, K.S.P.; Ramasubbu, R.; Vila-Rodriguez, F.; Blumberger, D.M.; Chan, P.; Delva, N.; Giacobbe, P.; Gosselin, C.; Kennedy, S.H.; et al. Treatment-resistant major depressive disorder: Canadian expert consensus on definition and assessment. Depress Anxiety 2021, 38, 456-467. [CrossRef]
- Mora, F.; Ramos-Quiroga, J.A.; Baca-García, E.; Crespo, J.M.; Gutiérrez-Rojas, L.; Madrazo, A.; Pérez Costillas, L.; Saiz, P.A.; Tordera, V.; Vieta, E. Treatment-resistant depression and intranasal esketamine: Spanish consensus on theoretical aspects. Front Psychiatry 2025, 16, 1623659. [CrossRef]
- Ivarsson, M.; Danielsson, H.; Imms, C. Measurement issues in longitudinal studies of mental health problems in children with neurodevelopmental disorders. BMC Psychol 2025, 13, 267. [CrossRef]
- Lee, W.; Bindman, J.; Ford, T.; Glozier, N.; Moran, P.; Stewart, R.; Hotopf, M. Bias in psychiatric case-control studies: literature survey. Br J Psychiatry 2007, 190, 204-209. [CrossRef]
- Abbaz Yazdian, F.; Khodabakhshi-Koolaee, A. Exploring the Counselors and Psychotherapists Perceptions of Therapeutic Errors in the Treatment Room. SAGE Open 2024, 14, 21582440241257320.
- Hayes, S.C.; Hofmann, S.G. "Third-wave" cognitive and behavioral therapies and the emergence of a process-based approach to intervention in psychiatry. World Psychiatry 2021, 20, 363-375. [CrossRef]
- Tanaka, M. Parkinson's Disease: Bridging Gaps, Building Biomarkers, and Reimagining Clinical Translation. Cells 2025, 14. [CrossRef]
- Meehan, A.J.; Lewis, S.J.; Fazel, S.; Fusar-Poli, P.; Steyerberg, E.W.; Stahl, D.; Danese, A. Clinical prediction models in psychiatry: a systematic review of two decades of progress and challenges. Mol Psychiatry 2022, 27, 2700-2708. [CrossRef]
- Figueiredo Godoy, A.C.; Frota, F.F.; Araújo, L.P.; Valenti, V.E.; Pereira, E.; Detregiachi, C.R.P.; Galhardi, C.M.; Caracio, F.C.; Haber, R.S.A.; Fornari Laurindo, L.; et al. Neuroinflammation and Natural Antidepressants: Balancing Fire with Flora. Biomedicines 2025, 13. [CrossRef]
- Haslbeck, J.; Ryan, O.; Robinaugh, D.J.; Waldorp, L.J.; Borsboom, D. Modeling psychopathology: From data models to formal theories. Psychological Methods 2022, 27, 930.
- Halassa, M.M.; Frank, M.J.; Garety, P.; Ongur, D.; Airan, R.D.; Sanacora, G.; Dzirasa, K.; Suresh, S.; Fitzpatrick, S.M.; Rothman, D.L. Developing algorithmic psychiatry via multi-level spanning computational models. Cell Rep Med 2025, 6, 102094. [CrossRef]
- Tan, T.; Wang, W.; Liu, T.; Zhong, P.; Conrow-Graham, M.; Tian, X.; Yan, Z. Neural circuits and activity dynamics underlying sex-specific effects of chronic social isolation stress. Cell Rep 2021, 34, 108874. [CrossRef]
- Bowman, R.; Frankfurt, M.; Luine, V. Sex differences in anxiety and depression: insights from adult rodent models of chronic stress and neural plasticity. Front Behav Neurosci 2025, 19, 1591973. [CrossRef]
- Mingardi, J.; Giovenzana, M.; Nicosia, N.; Misztak, P.; Ieraci, A.; Musazzi, L. Sex and Circadian Rhythm Dependent Behavioral Effects of Chronic Stress in Mice and Modulation of Clock Genes in the Prefrontal Cortex. Int J Mol Sci 2025, 26. [CrossRef]
- Bekhbat, M.; Ulukaya, G.B.; Bhasin, M.K.; Felger, J.C.; Miller, A.H. Cellular and immunometabolic mechanisms of inflammation in depression: Preliminary findings from single cell RNA sequencing and a tribute to Bruce McEwen. Neurobiol Stress 2022, 19, 100462. [CrossRef]
- Koppe, G.; Meyer-Lindenberg, A.; Durstewitz, D. Deep learning for small and big data in psychiatry. Neuropsychopharmacology 2021, 46, 176-190. [CrossRef]
- Driessen, E.; Efthimiou, O.; Wienicke, F.J.; Breunese, J.; Cuijpers, P.; Debray, T.P.A.; Fisher, D.J.; Fokkema, M.; Furukawa, T.A.; Hollon, S.D.; et al. Developing a multivariable prediction model to support personalized selection among five major empirically-supported treatments for adult depression. Study protocol of a systematic review and individual participant data network meta-analysis. PLoS One 2025, 20, e0322124. [CrossRef]
- Luedtke, A.; Sadikova, E.; Kessler, R.C. Sample size requirements for multivariate models to predict between-patient differences in best treatments of major depressive disorder. Clinical Psychological Science 2019, 7, 445-461.
- Watkins, E.R.; Newbold, A. Factorial Designs Help to Understand How Psychological Therapy Works. Front Psychiatry 2020, 11, 429. [CrossRef]
- Ciolino, J.D.; Scholtens, D.M.; Bonner, L.B. Factorial Clinical Trial Designs. Jama 2025, 333, 532-533. [CrossRef]
- Watkins, E.; Newbold, A.; Tester-Jones, M.; Javaid, M.; Cadman, J.; Collins, L.M.; Graham, J.; Mostazir, M. Implementing multifactorial psychotherapy research in online virtual environments (IMPROVE-2): study protocol for a phase III trial of the MOST randomized component selection method for internet cognitive-behavioural therapy for depression. BMC Psychiatry 2016, 16, 345. [CrossRef]
- Kotecha, G.; Ventz, S.; Fortini, S.; Trippa, L. Uncertainty directed factorial clinical trials. Biostatistics 2024, 25, 833-851. [CrossRef]
- Victor, T.A.; Khalsa, S.S.; Simmons, W.K.; Feinstein, J.S.; Savitz, J.; Aupperle, R.L.; Yeh, H.W.; Bodurka, J.; Paulus, M.P. Tulsa 1000: a naturalistic study protocol for multilevel assessment and outcome prediction in a large psychiatric sample. BMJ Open 2018, 8, e016620. [CrossRef]
- Nelson, B.; McGorry, P.D.; Wichers, M.; Wigman, J.T.W.; Hartmann, J.A. Moving From Static to Dynamic Models of the Onset of Mental Disorder: A Review. JAMA Psychiatry 2017, 74, 528-534. [CrossRef]
- Harkness, A.R.; Reynolds, S.M.; Lilienfeld, S.O. A review of systems for psychology and psychiatry: adaptive systems, personality psychopathology five (PSY-5), and the DSM-5. J Pers Assess 2014, 96, 121-139. [CrossRef]
Figure 1.
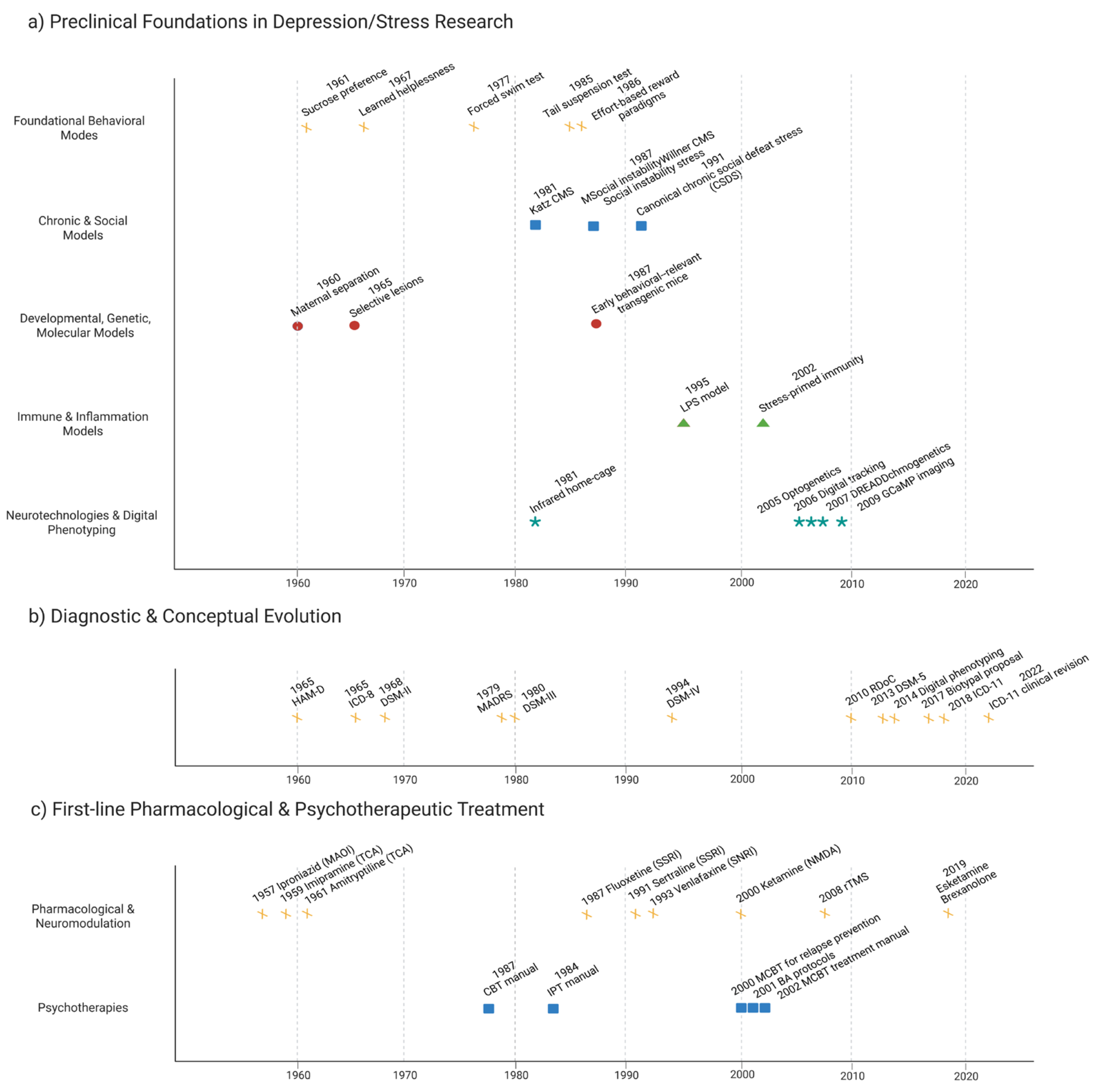
Translational timeline strip linking preclinical models, diagnostic milestones, and first-line depression treatments. Stylized timeline strip spanning the mid-20th century to the present, organized in three horizontal bands: (top) preclinical depression-relevant models, (middle) diagnostic milestones, and (bottom) first-line pharmacological and psychotherapeutic treatments. Each band highlights when core tools entered the field (e.g., forced-swim and learned helplessness assays, Diagnostic and Statistical Manual of Mental Disorders (DSM)-III formalization of major depressive disorder, the SSRI era, evidence-based psychotherapies, and rapid-acting agents such as ketamine/esketamine), emphasizing where innovation in models, nosology, and frontline care has been synchronized—or strikingly decoupled. Arrows and shaded zones indicate potential “bridgeable gaps” where contemporary preclinical assays could be explicitly linked to diagnostic refinements and treatment decisions in next-generation clinical trial designs.
Figure 1.
Translational timeline strip linking preclinical models, diagnostic milestones, and first-line depression treatments. Stylized timeline strip spanning the mid-20th century to the present, organized in three horizontal bands: (top) preclinical depression-relevant models, (middle) diagnostic milestones, and (bottom) first-line pharmacological and psychotherapeutic treatments. Each band highlights when core tools entered the field (e.g., forced-swim and learned helplessness assays, Diagnostic and Statistical Manual of Mental Disorders (DSM)-III formalization of major depressive disorder, the SSRI era, evidence-based psychotherapies, and rapid-acting agents such as ketamine/esketamine), emphasizing where innovation in models, nosology, and frontline care has been synchronized—or strikingly decoupled. Arrows and shaded zones indicate potential “bridgeable gaps” where contemporary preclinical assays could be explicitly linked to diagnostic refinements and treatment decisions in next-generation clinical trial designs.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



