
Submitted:
24 November 2025
Posted:
01 December 2025
You are already at the latest version
Abstract
Background : Antimicrobial resistance (AMR) refers to the ability of microbes to withstand the effects of antimicrobial drugs that are intended to eliminate them. Studies estimate the global disease burden caused by AMR to be approximately 4.95 million. Organisms such as Carbapenem Resistant Enterobacterales (CRE) and Carbapenem Resistant Acinetobacter baumannii (CRAB) are significant contributors to rising mortality rates due to the limited treatment options available. Methods: This scoping review o analyze the clinical challenges posed by AMR from an internal medicine viewpoint. Results: AMR significantly affects the incidence of urinary tract infections (UTIs) [95% UI: 19.79–36.30] and hospital-acquired infections (95% CI 12.39–17.15%; 16,793/164,717). It also increases multisystem infections and reduces the efficacy of drugs like colistin and penicillin. Conclusion :Antimicrobial stewardship has become a crucial responsibility for every physician. The quadripartite collaboration plays a vital role in establishing policies on judicious antibiotic use. The WHO and CDC's Global AMR Action Plans say that education, diagnostic vigilance, and responsible prescribing are all important parts of fighting AMR. These strategies are in line with those plans.
Keywords:
antimicrobial resistance (amr)
; internal medicine
; urinary tract infections (UTIs)
; methicillin-resistant staphylococcus aureus (mrsa)
; antimicrobial stewardship (AMS)
1. Introduction
- Definition and global disease burden of antimicrobial resistance
Antimicrobial resistance (AMR) is defined as the capacity of bacteria, viruses, fungi, and parasites to resist antimicrobial action, rendering standard treatments ineffective.[1] A systematic review and meta-analysis by Murray et al estimates the global disease burden of AMR to be 4.95 million [2]. Clinically, resistant infections lead to delayed recovery, longer hospital stays, and increased use of intravenous therapy. This burden extends to healthcare systems through extended bed occupancy and higher pharmacological costs. AMR has silently infiltrated modern healthcare, transforming once-manageable infections into treatment challenges. Organisms such as Carbapenem Resistant Enterobacterales (CRE), Carbapenem Resistant Acenitobacter Baumanii (CRAB) have been listed in the guidelines of The Infectious Diseases Society of America( IDSA )2024 as major clinical concerns due to limited treatment options. [3–5]
Gaps in existing literature
Underreporting in low and middle income countries
There is a lack of standardized surveillance systems in low and middle income countries. This leads to underreporting which hampers estimation of the global burden of AMR.
- Limited epidemiological data
There is a lack of epidemiological studies on emerging resistance mechanisms and novel diagnostics in AMR.
- Implementation and evaluation of stewardship
Stewardship programmes have been implemented in most countries. But, there is variability in sustainability and long term clinical impact of these strategies in diverse hospital settings.
2. Methods
Search strategy
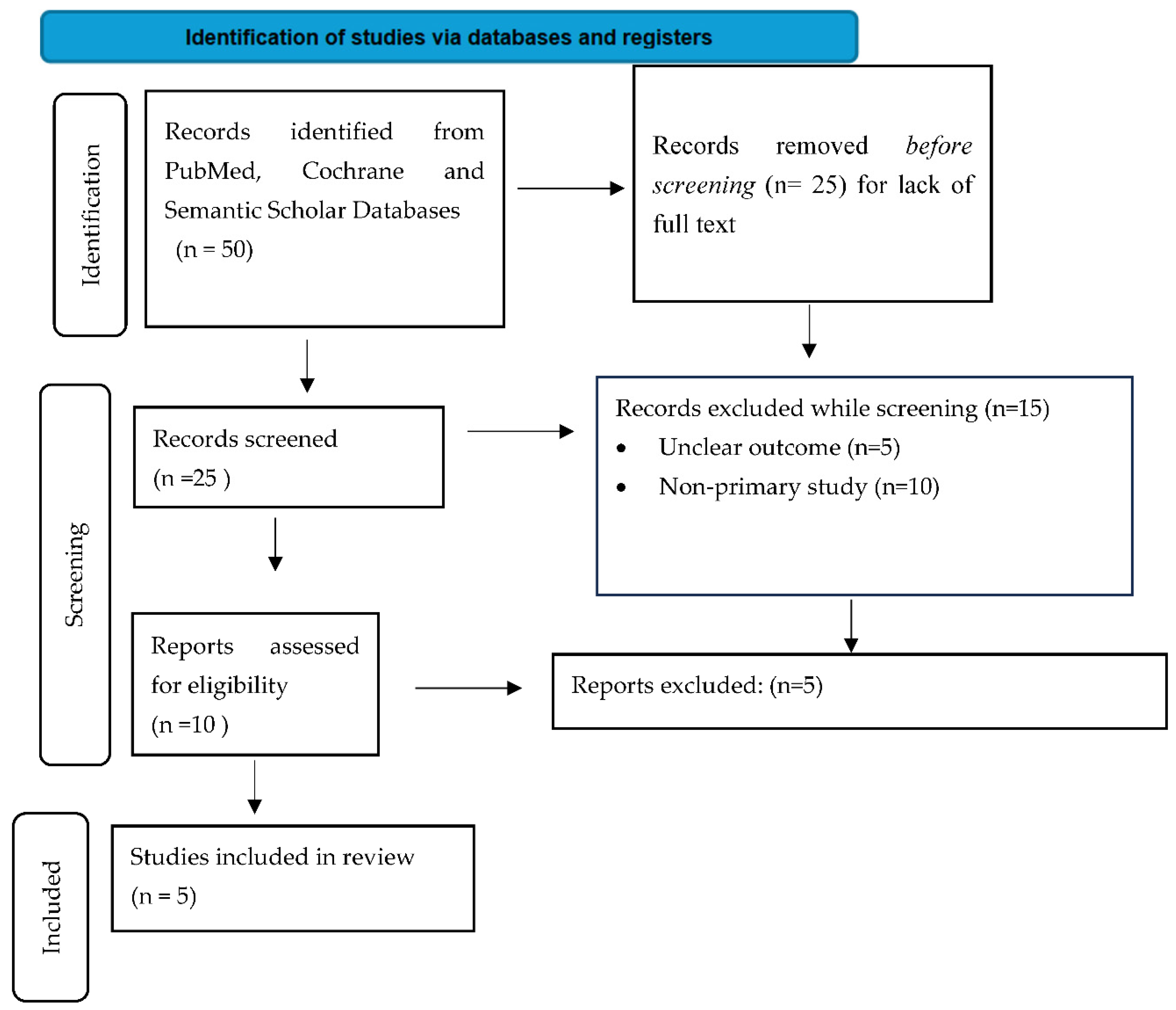
We conducted a comprehensive search of PubMed, Cochrane and Scopus databases from 26/10/2025 to 09/11/2025. Keywords were related to ‘antimicrobial resistance’, ‘clinical intervention’ and ‘stewardship’ with Boolean operators such as AND , OR, NOT used. We included randomized and non-randomized studies which assessed AMR prevalence, clinical outcomes and stewardship practices written in the English language. Non-clinical trials were excluded. A total of five articles were included in the review.

Table 1.
Search strategy. A total of 50 studies were screened, 10 were assessed for eligibility. Articles assessing the global burden of AMR in urinary tract infections (n=2), methicillin resistant staphylococcus aureus (n=2) and ventilator associated pneumonia (n=1) were included in the review.
Table 1.
Search strategy. A total of 50 studies were screened, 10 were assessed for eligibility. Articles assessing the global burden of AMR in urinary tract infections (n=2), methicillin resistant staphylococcus aureus (n=2) and ventilator associated pneumonia (n=1) were included in the review.
 |
- Data
- extraction and analysis
Data was extracted using a standardized form ( year of study, study design, methodology and outcome) created in Ms Excel 2024. Giving the scoping nature, data focused on descriptive summarization of the key findings. Data synthesis aimed to summarize key findings, highlight evidence gaps in future research and inform future research directions without conducting meta-analysis.
3. Results and Discussion
The results of included studies in our scoping review have been highlighted in Table 2
AMR occurs due to factors like overuse/misuse of antibiotics and poor hand hygiene. For example, upper respiratory tract infections are mainly caused by viruses such as influenza and rhinoviruses. Nevertheless, antibiotics are prescribed for these infections. This results in the development of resistance. Good prescription practices are key. Poor hand hygiene and neglecting proper infection control protocols results in the increase of spread of hospital acquired infections (HAI) which increases the risk of AMR.
Infections which we see in our day to day lives : such as urinary tract infections (UTI’s), pneumonia, and wounds lead to chronic complications which hamper our daily lives. A study by Li et al in 2022 stated that Escherechia coli ( E.coli) was responsible for 40% of AMR related deaths in UTI globally. [95% UI: 19.79–36.30]. Four classes of antibiotics were implicated in AMR related deaths. These were fluoroquinolones (169.15 thousand [95% UI: 119.64–240.75], cephalosporins (113.06 thousand [95% UI: 78.60–163.97], aminopenicillin (107.72 thousand [95% UI: 84.82–139.29] and beta-lactamase inhibitors (104.54 thousand [95% UI: 76.74–144.36][6]
Staphylococcus aureus is a gram positive bacteria which is a commensal on the body’s skin. However, it has been implicated in several systemic as well as localized infections (Figure 1).
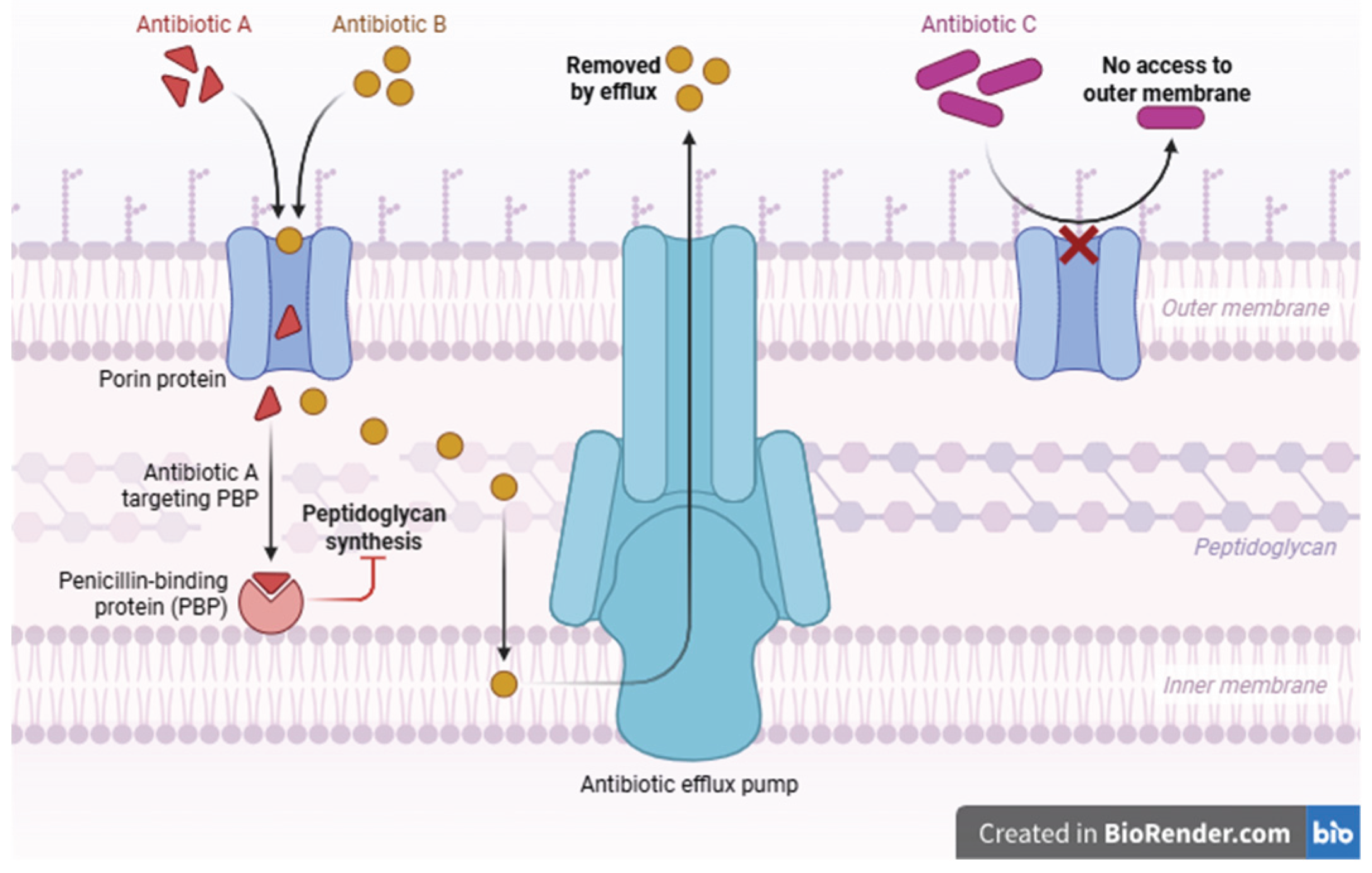
Methicillin is an extended spectrum penicillin which acts on the cell wall via penicillin binding proteins (PBP).In MRSA, the mecA gene sequence alters the structure of PBP to PBP2a which lowers the affinity of antibiotics to bind to the cell membrane which leads to methicillin resistance. A study by Hasanpour et al estimated the global disease burden caused by MRSA to be 14.69% (95% CI 12.39–17.15%; 16,793/164,717).[7] Intravenous vancomycin is the drug of choice for MRSA infections. However vancomycin resistant strains have emerged( VRSA).Therefore, there has been a shift to third generation oxazolidinone antibiotics like linezolid.[9]
A systematic review by Howroyd et al in 2024 stated that there was an increased risk of developing VAP after antimicrobial therapy was administered 90 days prior to ICU admission(OR 13.5) [8]. This is shown in figure 2. Combination of imipenem and cilastatin have proved to be an effective combination therapy for VAP. The increased burden in clinical practice leads to prolonged hospitalization and greater mortality risks.
Figure 2.
Diagram showing colistin resistance in ventilator associated pneumonia (VAP). Studies have shown that this is associated with multi-drug resistant Acenitobacter baumanii.[11].
Figure 2.
Diagram showing colistin resistance in ventilator associated pneumonia (VAP). Studies have shown that this is associated with multi-drug resistant Acenitobacter baumanii.[11].
- Treatment
A schematic representation of the AWaRe (Access, Watch and Reserve) classification of antibiotics is given in Table 3
Antimicrobial stewardship (AMS) is a frontline defense against AMR’s spread. According to Tang et al. (2023), laboratory-informed prescribing, de-escalation based on culture results, and regular review of antibiotic regimens are the pillars of good clinical practice.[12] It is regulated by the quadripartite which includes WHO (World Health Organization), FAO ( Food and Agriculture Organization), UNEP( United Nations Environment Programme) and WOAH (World Organisation for Animal Health).[13] A study by Patel et al stated that engaging pharmacists and microbiologists trained in infectious diseases for stewardship protocols.enhanced the quality of outcomes.[14]
Guidelines regarding antimicrobial stewardship programs recommend an infectious diseases-trained physician and an infectious diseases-trained pharmacist as core members. Inclusion of clinical microbiologists, infection-control practitioners, information systems experts and hospital epidemiologists is considered optimal. Recommended stewardship interventions include prospective audit and intervention, formulary restriction, education, guideline development, clinical pathway development, antimicrobial order forms and the de-escalation of therapy.
It is essential that antibiotics should be prescribed only for confirmed or highly suspected bacterial infections.A study by Marepalli et al stated that several women who are prescribed antibiotics for urinary tract infections(UTI) might have asymptomatic bacteriuria and not infection. Thus prescription of antibiotics for UTI could lead to adverse treatment outcomes [15] Pharmaceutical interventions in AMR such as therapeutic drug monitoring helped in preventing adverse drug-drug interactions De-escalation strategies such as ‘Time Out’ ‘( stopping of antibiotics 48 hours after its initiation) helped to reassess the need and choice of antibiotics.[16]
4. Conclusion
- Limitations
AMR faces diagnostic limitations. Culture methods are considered the gold standard to detect AMR. They are limited by their long turnaround time (TAT) and inability to detect microrganisms below the minimum inhibitory concentrations. Newer methods like next generation sequencing, disk diffusion, polymerase chain reaction (PCR) are being adapted. Yet, standardized protocols regarding these methods have not been fully integrated. Included studies differ in study designs, sample, population studied, prescription practices. This heterogeneity limits the generalizability of findings. Low and middle income countries (LMIC) have poor surveillance systems. This leads to underreporting and bias.
- Implications
- Theoretical implications
This review integrates microbial diversity, antimicrobial use and healthcare practices as key components of AMR. Future studies should analyse the socioeconomic factors that influence AMR using variables like income and human behavior
- Managerial or policy implications
Healthcare institutions should integrate AMS into the ‘One Health’ Policy. Multisectoral collaboration between health, agricultural and government sectors is the need of the hour. Greater investment in diagnostic techniques and trained personnel could lead to robust implementation of these policy
- Ideas for future research
Longitudinal studies assessing AMR patterns over long periods will establish temporal and causal association. Research on socioeconomic factors influencing AMR and adherence to stewardship protocols will help in drafting behavior change communication (BCC) models. This will increase awareness on AMR in the general public. Development of rapid and comprehensive diagnostic tools will reduce inappropriate antibiotic exposure.
From the internal medicine perspective, AMR is no longer an abstract global crisis :it’s a bedside reality. Every antibiotic order impacts not only one patient’s recovery but the sustainability of future treatment options. The clinician’s task is twofold: to cure responsibly and to preserve efficacy. Ultimately, each prescription is a responsibility, bridging personal ethics with public health stewardship in the fight against this invisible pandemic. Implementing these measures aligns with the WHO and CDC’s Global AMR Action Plans, which advocate education, diagnostic vigilance, and responsible prescribing as cornerstones of containment.
Author Contributions
Niya Mahale : Conceptualization, Methodology, Software, data curation ,editing and writing
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
The study was based on previously published anonymized data. It did not involve human and animal trials. Hence ethical clearance was not required.
Informed Consent Statement
Not applicable
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article [and/or] its supplementary materials.
Acknowledgments
Nil.
Conflicts of Interest
No conflict of interest declared
References
- Antimicrobial resistance [Internet]. [cited 2025 Nov 20]. https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance. Accessed 20 Nov 2025.
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399:629–55. [CrossRef]
- IDSA 2024 Guidance on the Treatment of Antimicrobial Resistant Gram-Negative Infections [Internet]. [cited 2025 Nov 20]. https://www.idsociety.org/practice-guideline/amr-guidance/. Accessed 20 Nov 2025.
- Smith HZ, Hollingshead CM, Kendall B. Carbapenem-Resistant Enterobacterales. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [cited 2025 Nov 20]. http://www.ncbi.nlm.nih.gov/books/NBK551704/. Accessed 20 Nov 2025.
- Iovleva A, Fowler VG, Doi Y. Treatment Approaches for Carbapenem-Resistant Acinetobacter baumannii Infections. Drugs. 2025;85:21–40. [CrossRef]
- Li X, Fan H, Zi H, Hu H, Li B, Huang J, et al. Global and Regional Burden of Bacterial Antimicrobial Resistance in Urinary Tract Infections in 2019. J Clin Med. 2022;11:2817. [CrossRef]
- Hasanpour AH, Sepidarkish M, Mollalo A, Ardekani A, Almukhtar M, Mechaal A, et al. The global prevalence of methicillin-resistant Staphylococcus aureus colonization in residents of elderly care centers: a systematic review and meta-analysis. Antimicrob Resist Infect Control. 2023;12:4. [CrossRef]
- Howroyd F, Chacko C, MacDuff A, Gautam N, Pouchet B, Tunnicliffe B, et al. Ventilator-associated pneumonia: pathobiological heterogeneity and diagnostic challenges. Nat Commun. 2024;15:6447. [CrossRef]
- Asghar MU, Tariq M, Zaidi AH, Haneef K, Asghar A, Ain NU. Unveiling the spectrum of vancomycin resistance in Staphylococcus aureus from Hospital-acquired urinary tract infections (HA-UTI) in cardiac patients. Mol Biol Rep. 2025;52:1001. [CrossRef]
- Mateescu D-M, Ilie A-C, Cotet I, Guse C, Muresan C-O, Pah A-M, et al. Global Burden of Bloodstream Infections in COVID-19: Prevalence, Antimicrobial Resistance, and Mortality Risk. Viruses. 2025;17:1353. [CrossRef]
- Tong SYC, Fowler VG, Skalla L, Holland TL. Management of Staphylococcus aureus Bacteremia: A Review. JAMA. 2025;334:798–808. [CrossRef]
- Islam MM, Jung DE, Shin WS, Oh MH. Colistin Resistance Mechanism and Management Strategies of Colistin-Resistant Acinetobacter baumannii Infections. Pathogens. 2024;13:1049. [CrossRef]
- Tang KWK, Millar BC, Moore JE. Antimicrobial Resistance (AMR). Br J Biomed Sci. 2023;80:11387. [CrossRef]
- Climate Change and AMR: Interconnected Threats and One Health Solutions - PubMed [Internet]. [cited 2025 Nov 20]. https://pubmed.ncbi.nlm.nih.gov/41009922/. Accessed 20 Nov 2025.
- Patel D, Lawson W, Guglielmo BJ. Antimicrobial stewardship programs: interventions and associated outcomes. Expert Rev Anti Infect Ther. 2008;6:209–22. [CrossRef]
- Marepalli NR, Nadipelli AR, Manohar Kumar Jain RJ, Parnam LS, Vashyani A. Patterns of Antibiotic Resistance in Urinary Tract Infections: A Retrospective Observational Study. Cureus. 16:e62771. [CrossRef]
- Clinical Impact of an Antibiotic Time Out Initiative at an Academic Medical Center - PubMed [Internet]. [cited 2025 Nov 20]. https://pubmed.ncbi.nlm.nih.gov/34381272/. Accessed 20 Nov 2025.
Figure 1.
This is a diagram showing the various complications caused due to MRSA ranging from skin and soft tissue infections like diabetic foot ulcer to cardiac manifestations like endocarditis.[10].
Figure 1.
This is a diagram showing the various complications caused due to MRSA ranging from skin and soft tissue infections like diabetic foot ulcer to cardiac manifestations like endocarditis.[10].
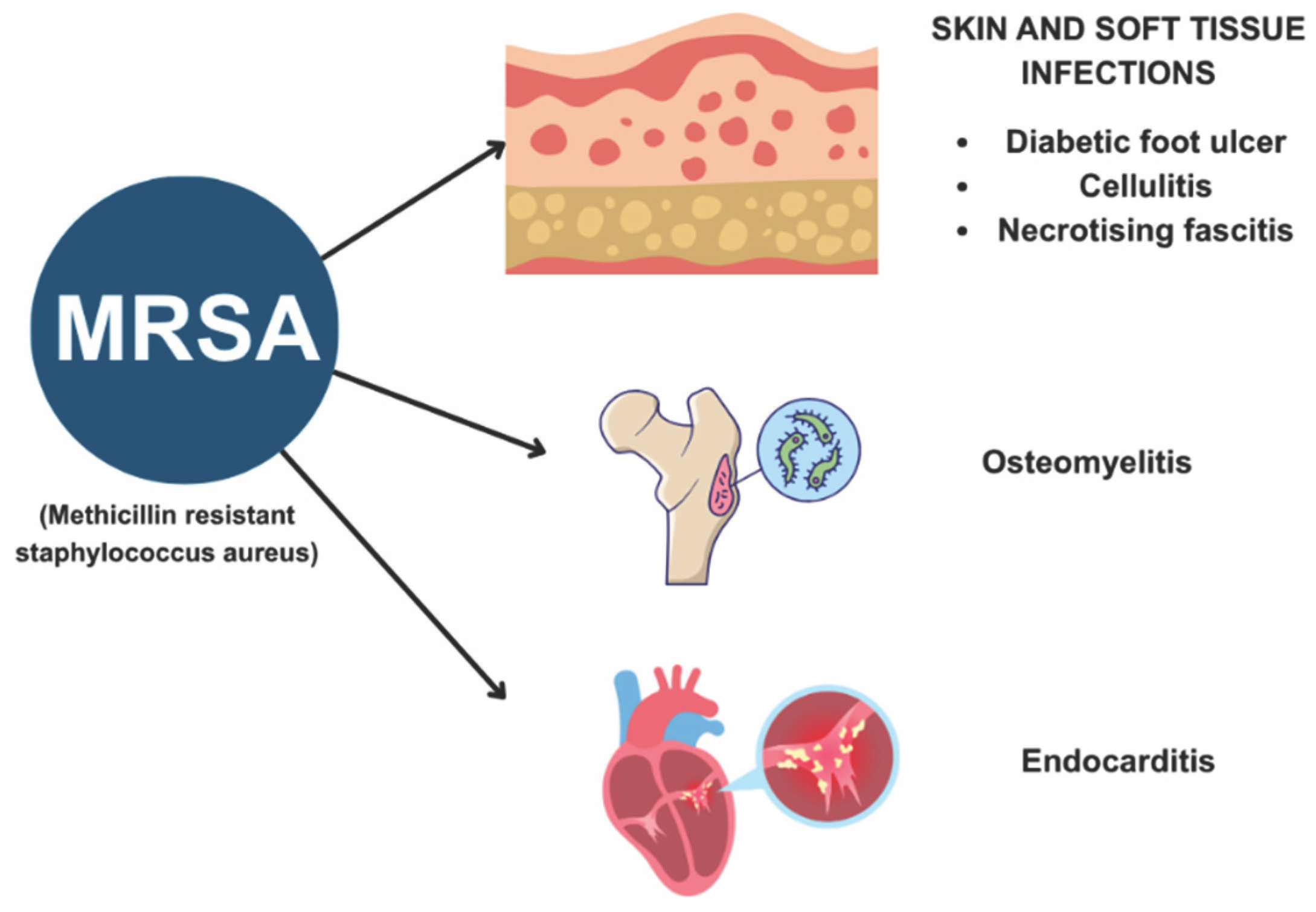
Table 2.
Results of included literature.
| Reference | Study design | Methodology | Outcome |
| [6] | Epidemiological study design | Data on disability adjusted life years (DALY’s), years of life lost (YLL) and years lived with disability (YLD) was obtained from the Global Burden of Diseases, Factors Study (GBD) | Escherechia coli ( E.coli)is the most common pathogen leading to mortality in AMR related UTI. [95% UI: 19.79–36.30] Latin America (1.91 per 100,000 [95% UI: 1.38–2.53] had the highest death rates. |
| [7] | Systematic review and meta-analysis | Systematic search of MEDLINE/PubMed, EMBASE, Scopus and Web of Science databases. Assessment of pooled prevalence (95%confidence interval) | AMR is a prevalent causes of MRSA (PR = 1.97; 95% CI 1.83–2.12), |
| [8] | Review | Narrative description | VAP, impacts 20% of critically ill patients in ICU and increases AMR risk |
| [9] | Cross-sectional study | AMST was assessed in 189 patients in a cardiac ward via methods such as disk diffusion, minimum inhibitory concentration (MIC), and multiple antibiotic resistance indexing. | 55% of isolated VRSA showed resistance to linezolid and chloramphenicol |
| [10] | Systematic review and meta-analysis | Systematic search of PubMed Google Scholar , MDPI databases for articles from 2020 to 2025 | Rates of AMR in MRSA were 36% and ESBL (31%). Risk factors included mechanical ventilation (OR 2.6) and corticosteroid use (OR 2.4) |
*MRSA: Methicillin resistant staphylococcus aureus, VAP: Ventilator associated pneumonia,UTI: Urinary tract infections, PR: Prevalence rate, CI: Confidence interval, AMST: antimicrobial susceptibility testing, VRSA: Vancomycin resistant staphylococcus aureus, OR : Odds ratio, ESBL: Extended spectrum beta lactamases.
Table 3.
Antibiotics are classified into four classes by the AwaRe classification based on AMR impact. This hierarchy underlines the ethical duty to preserve high-importance antibiotics for severe infections.
Table 3.
Antibiotics are classified into four classes by the AwaRe classification based on AMR impact. This hierarchy underlines the ethical duty to preserve high-importance antibiotics for severe infections.
| Category | Description | Examples | Clinical Relevance |
| I | Essential for life-threatening infections, limited options | Carbapenems, Glycopeptides, Polymyxins, Fluoroquinolones | Use restricted to multidrug-resistant organisms |
| II | Important but with viable alternatives | Aminoglycosides, Cephalosporins (1st–2nd gen), Macrolides | Common in hospital and community infections |
| III | Multiple alternatives exist | Tetracyclines, Fosfomycin, TMP-SMX | Used for mild/moderate infections |
| IV | Minimal use in humans | Veterinary antimicrobials like Ionophores | Indirect relevance to human AMR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



