Submitted:
28 April 2023
Posted:
29 April 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Introduction: The reduced implementation of surveillance programs and limited bedside infectious diseases consultations due to the pressure of COVID-19 pandemic in healthcare systems led to increased rates of irrational use of antimicrobials and incidence of infections by multidrug-resistant microorganisms. The aim of the present study is to evaluate the incidence of antimicrobial resistance and the management of bloodstream infections before and during COVID-19 pandemic at the University General Hospital of Alexandroupolis (Greece). Material-Methods: This is a retrospective study conducted from January 2018 to December 2022. Data were collected from the University Microbiology Laboratory per semester regarding the isolated strains of Gram positive and negative bacteria in blood cultures and respiratory samples in hospitalized patients in medical and surgical wards and in the Intensive Care Unit (ICU). Additionally, bloodstream infections with requested infectious diseases consultation were reported (n=400), determining whether these were carried out via telephone contact or at the patient's bedside. Demographic data, comorbidities, focus of infection, antimicrobial regimen, duration of treatment, length of hospitalization and clinical outcome were analysed. Results: A total of 4569 strains of Gram positive and negative bacteria were isolated. An increasing trend was reported compared to the pre-pandemic period in the incidence of resistant Gram-negative bacteria, particularly in ICUs. Prior antimicrobial use and the rate of hospital-acquired infections were increased significantly during the pandemic. In the pre-pandemic period 2018-2019, a total of 246 infectious diseases consultations were carried out, while during the period 2020-2022 154, with the percentage of telephone consultations 15% and 76% respectively. Detection of the source of infection and timely administration of appropriate antimicrobial agents were more frequently recorded before the pandemic and 28-day mortality was significantly reduced in cases with bedside consultations. Conclusion: Empowering of infectious diseases surveillance programs and committees, rational use of antimicrobials agents and bedside infectious diseases consultations are vital in order to reduce the impact of infections caused by multidrug-resistant strains.
Keywords:
COVID-19 pandemic
; antimicrobial resistance
; infectious diseases consultation
; multi-drug resistant bacteria
; infection prevention and control group
; antibiotic stewardship
1. Introduction
The COVID-19 pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was spread rapidly and overwhelmed healthcare systems worldwide [1]. Simultaneously, the rise in multi-drug resistant (MDR) infections continues to threaten public heath leading to high rates of morbidity, mortality and economic loss [1]. Antimicrobial resistance (AMR) is globally rising and considered as an ongoing pandemic with an estimated 700,000 deaths globally each year [2]. AMR can be defined as an increasing resistance to antibiotics that undermines the ability to treat common and serious infectious diseases [2]. The estimated number of deaths due to infections with multiple drug resistant pathogens by the year 2050 is expected to reach 10 million/year in case of not applying a strict action plan to combat AMR [2]. The WHO declared AMR as one of the top 10 global health threats and, although often more silent than COVID-19 pandemic, it can have similar devastating consequences [3]. A European Centre for Disease Control and Prevention (ECDC) study in 2015 on the health burden of antimicrobial resistance measured in numbers of cases, attributable deaths and disability-adjusted life-years (DALYs) concluded that 33110 deaths and 874541 DALYs were caused by infections with antibiotic-resistant bacteria which were mainly health-care-associated (75%) [4].
The emergence of antimicrobial resistance is an unforeseen and unavoidable consequence of the COVID-19 pandemic. Several recent reports have described an increase in multidrug-resistant bacteria during the COVID-19 pandemic [5,6]. The cause is multifactorial, but a major reason is the high rate of antimicrobial agents utilisation in COVID-19 patients despite the relatively low rates of co- or secondary infections [5]. A retrospective study found that the incidence of carbapenem-resistant Enterobacterales colonisation in ICU patients increased from 6.7% in 2019 to 50% in March–April 2020 [6]. Because of the COVID-19 emergency in healthcare systems, planned activities were deprioritized and already implemented preventive measures were reversed [7]. The pandemic has put tremendous strain on healthcare systems, diverting resources, personnel, and attention away from AMR diagnosis and management while AMR studies were hampered and surveillance programs were de-emphasized or stopped [8].
The aim of the present study is to evaluate the impact of COVID-19 pandemic on antimicrobial resistance and the management of bloodstream infections caused by multidrug resistant bacteria in University General Hospital of Alexandroupolis (Greece) during the period 2018-2022. The antimicrobial resistance rates in Greece are high mainly due to Carbapenem-resistant Gram-negative bacilli. The pressure on healthcare systems due to the pandemic was enormous causing alterations in daily practices and limiting the prevention of infectious diseases and control programmes. Surveillance programmes and reports of AMR before and after the COVID-19 pandemic are vital in order to better understand the impact of pandemic and decide appropriate interventions.
2. Materials and Methods
This was a retrospective study conducted in the University Lab of Microbiology and Department of Infectious Diseases of the University General Hospital of Alexandroupolis (Greece). Data from lab records and routine care patient charts during the period 1st January 2018 to 31st December 2022 were retrospectively analysed. The study was carried out in accordance with the Helsinki Declaration of Human Rights.
During the 5-year period, routine susceptibility data of Gram-negative and Gram-positive bacterial isolates from blood and respiratory specimens of hospitalized patients in surgical and medical wards and Intensive Care Unit (ICU) were reported emphasizing to the most clinically important species (Acinetobacter baumannii, Klebsiella pneumoniae, Pseudomonas aeruginosa, Enterococcus faecium, and Staphylococcus aureus). From each patient, only the first isolate of a given species recovered was included, regardless of susceptibility profile or specimen type. The classification of the isolates as susceptible, intermediate or resistant was based on the Clinical & Laboratory Standards Institute (CLSI) and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines [9,10]. The antimicrobial susceptibility testing was performed by automated antimicrobial susceptibility testing system for the minimal inhibitory concentration (MIC) determination.
The number of non-susceptible isolates was divided by the number of isolates tested in order to determine the non-susceptibility rate for every assessment period defined as a semester. The isolates were analysed based on microorganism, ward type (ward, ICU), specimen type and antibiotic. The administration of antibiotics prior to pathogen’s isolation was reported. The percentage of isolates attributed to health-care associated infections was estimated for each year. The clinical outcome was evaluated by documenting the risk of death and increased hospital stay due to the isolated pathogens.
Additionally, the cases of bloodstream infections with reported consultation by an Infectious Diseases specialist during the period 2018-2022 were documented. The patients were divided into two groups based on period of time, Group A for prepandemic period (2018-2019) and Group B for COVID-19 pandemic period (2020-2022). Type of consultation (bedside or via telephone), demographic characteristics of patients (age, gender), comorbidities using the Charlson comorbidity index (CCI), duration of symptoms before consultation, type of infection (community or hospital acquired), foci of infection, clinical outcome (mortality within 28 and 90 days after first pathogen isolation) and features of antibiotic therapy (duration, combination of antibiotics) were analysed.
Statistical analysis of the data was performed using IBM Statistical Package for the Social Sciences (SPSS), version 19.0 (IBM Corp., Armonk, NY, USA). The normality of quantitative variables was tested with Kolmogorov-Smirnov test. Normally distributed quantitative variables are expressed as the mean ± standard deviation (SD), while non normally distributed quantitative variables are expressed as the median value and range. Qualitative variables were expressed as absolute and relative (%) frequencies. Student’s t-test, Mann-Whithey U-test and chi-square test were used to determine differences in demographic and clinical characteristics between the two groups of patients. All tests were two tailed and statistical significance was considered for p values <0.05.
3. Results
During the period 2018-2022, a total number of 4569 bacteria were isolated in blood and respiratory samples from patients hospitalized in wards (n=3353) and ICU (n=1216). Number of isolates by semester is shown for ICU in Table 1 and for wards in Table 2. After the initiation of COVID-19 pandemic a significant increase is reported in numbers of isolated bacteria, eventually for Gram-negative bacilli and Enterococcus isolates.
In Acinetobacter baumannii isolates from hospitalized patients in ICU the non-susceptibility to carbapenems remained high during the whole study period (Figure 1). The percentage of Acinetobacter baumannii isolates from blood and respiratory samples in ICU resistant to meropenem was 92.6% in the first semester of 2018 and 97.9% in the second semester of 2022 (p <0.001). The non-susceptibility to meropenem in wards was increased from 82.3% in the first semester of 2018 to 91.6% in the second semester of 2022 (p <0.001). A significant difference was found in the non-susceptibility trend for amikacin, ranging from 81.6% in the first semester of 2018 to 93.4% in the second semester of 2022 in ICU and from 63.2% to 74.5% respectively in wards (p <0.001). A decreasing trend was reported in the slope of the non-susceptibility for colistin in ICU samples during the pre-pandemic period (from 43.6% to 41.4%, p= 0.05) followed by an increasing trend during the pandemic period (from 42.5% to 59.6%, p<0.001).
In Klebsiella pneumonia isolates from blood and respiratory samples in ICU a decreasing trend in non-susceptibility to meropenem and colistin prior to COVID-19 pandemic initiation (Figure 2). However, during pandemic period the rate of non-susceptibility to colistin was increased from 58.3% in the second semester of 2019 to 71.8% in the second semester of 2022 and to meropenem from 79.8% to 92.4%, respectively (p<0.001) (Figure 2). Similar findings were documented in the wards with 56.4% of Klebsiella pneumonia isolates resistant to colistin and 72.6% to meropenen during second semester of 2022 (Figure 2).
In Pseudomonas aeruginosa isolates from patients hospitalized in wards and ICU statistically significant changes were found in the rates of non-susceptibility trends before and during COVID-19 pandemic (Figure 3). The non-susceptibility of isolates in ICU to meropenem was increased from 43.5% in the first semester of 2018 to 53.6% in the second semester of 2022 (p<0.001). Similarly, the non-susceptibility to amikacin was reported 41.3% in the first semester of 2018 and was increased to 53.6% in the pandemic period (p<0.001). In wards the non-susceptibility to levofloxacin remained high during 2018-2022 ranging from 42.5% in the first semester of 2018 to 49.6% in the second semester of 2022 (p <0.001). Despite the decreasing trend of non-susceptibility to meropenem and amikacin in wards in the first semester of 2020, during the pandemic period the rate of non-susceptibility to meropenem increased to 42.5% and to amikacin to 38.6% (p<0.001).
A decreasing rate of non-susceptibility to vancomycin was reported in the second semester of 2019 for Enterococcus feacium isolates in wards. However, during pandemic period the non-susceptibility rate to vancomycin was increased from 33.5% to 44.6% in second semester of 2022 (p<0.001) (Figure 4).
In Staphylococcus aureus isolates in wards during the pre-pandemic period a decreasing trend of non-susceptibility to methicillin was found, from 33.2% in the first semester of 2018 to 30.5% in the first semester of 2019 (p=0.052). During COVID-19 pandemic the rate was increased significantly to 38.6% (p<0.001) (Figure 5).
The estimated percentage of isolates attributed to hospital acquired infections was increased from 42% in 2018 to 60% in 2021 and 64% in 2022 (p=0.05). Antibiotic consumption before the isolation of bacteria in blood and respiratory samples was reported in high rates during 2018-2022, ranging from 53% in 2018 to 78% in 2022 (p=0.005). The results of multivariable logistic regression analysis are shown in Table 3. The increased numbers of isolates in wards and ICU and high rates of non-susceptibility to antibiotics led to increased risk of death and prolonged hospital stay particularly for Gram negative bacilli.
A total of 400 adults with bloodstream infection and reported infectious diseases consultation were eligible for inclusion in the study. During pre-pandemic period (group A) 246 consultations were documented, 85% carried out bedside. During COVID-19 pandemic (group B) the number of consultations was lower (n=154) mainly conducted via telephone (76%). Demographic data (age, gender) of patients between the two groups were similar (Table 4). The first consultation was reported within 24 hours from symptoms onset in 64.2% of patients in Group A while 47.4% in Group B (Table 4). The proportion of patients with Charlson comorbidity index Score ≥3 was approximately 40% for both groups (Table 5). The proportion of patients with prosthetic material was higher in Group B compared to Group A (30.5% vs. 22.8%, p 0.02).
Overall, approximately 60% of bloodstream infections were hospital acquired and 30% were community acquired (Table 6). The frequency of hospital-acquired infections and multi-drug resistant isolated bacteria were higher in group B (63.6% vs. 61%, p < 0.001 and 37% vs. 33.7%, p<0.001, respectively). The most common foci of infection were skin and soft tissue infections, central venous catheters associated infections, respiratory infections and osteomyelitis (Table 6). The proportion of patients with an unknown focus was higher in group B (11.7% vs. 6.5%, p 0.04). Certain foci of infection such as thrombophlebitis, implanted vascular device, prosthetic joint infection, urinary tract infections and intra-abdominal infections were more frequently identified in group A compared to group B (Table 6). The frequency of a complicated infection was similar between the two groups (54.5% vs. 56.5%, p 0.001).
The percentage of patients whom bloodstream infection was complicated with septic shock was 3.3% in group A and 4.5% in group B (p=0.118) (Table 7). Need for hospitalization in intensive care unit (4.5% vs. 7.8%, p=0.245) and length of hospital stay (29 days vs. 30 days, p=0.457) were not significantly different between the two groups (Table 7). The duration of antibiotic treatment was longer in group A compared to group B (15 days vs. 11 days, p=0.04). Higher frequency of treatment with combination of antibiotics was reported in group A (10.6% vs. 7.1%, p<0.001). The mortality rate within 28 days and 90 days was significantly higher in group B with mainly via telephone infectious diseases consultation (Table 7). The proportion of cases in which new blood cultures after treatment initiation were collected and repeated consultations were carried out was higher in group A with bedside infectious diseases consultations. There was no significant difference in recurrent bacteraemia between the two groups.
4. Discussion
The COVID-19 pandemic induced a new burden on health systems worldwide and aggravated existing health challenges in many aspects of global health [11]. According to the annual Tripartite AMR Country Self-Assessment Survey 2020–21, 151 (94%) of 161 countries ascribed the pandemic as having impacted their national response to control the problem of antimicrobial resistance [12]. An acute increase in the burden of antimicrobial resistance was a feared outcome of the pandemic, but this speculation had not been comprehensively measured [11,12]. The present study showed that the rates of multi-drug resistant bacteria during COVID-19 pandemic were increased significantly. An increasing trend was reported in numbers of isolated Gram-negative bacteria, especially for Acinetobacter Baumannii non-susceptible to colistin and Pseudomonas aeruginosa non-susceptible to carbapenems and quinolones, leading to increased risk of death and longer hospital stay. The management of bloodstream infections was altered during COVID-19 pandemic based on the results of our study, while infectious diseases consultations were mainly conducted via telephone and not bedside. Telephone infectious diseases consultations were associated with higher rates of mortality and lower probability for appropriate antimicrobial scheme and repeated clinical evaluation.
A special report by the Centre for Disease Control and Prevention (CDC) with country-level estimates of the effect of COVID-19 on antimicrobial resistance in the USA highlights a devastating undoing of progress in efforts to control antimicrobial resistance [13]. Although deaths from antimicrobial resistance were reduced by 18% from 2012 to 2017, including a 30% reduction in US hospitals, during 2020 a 15% increase in drug-resistant nosocomial infection rates in 2020 was reported compared with the previous year [13]. Pathogen–drug combinations, classified as critical by WHO based on their risk to human health, showed alarming increases in rates of infection since 2019 especially in rates of carbapenem-resistant Enterobacterales infections up 35%, and carbapenem-resistant Acinetobacter increasing by 78% [13]. Similar findings were documented in the results of the Greek Electronic System for the Surveillance of Antimicrobial Resistance (WHONET-Greece) which analysed routine susceptibility data of 17,837 Gram-negative and Gram-positive bacterial isolates from blood and respiratory specimens of hospitalized patients in nine COVID-19 tertiary hospitals in two periods, January 2018–March 2020 and April 2020–March 2021 [1]. Increase was observed in the number of bloodstream and respiratory isolates from ICU patients in the last six months of the study period (October 2020–March 2021) mainly due to A. baumannii isolates in both blood and respiratory specimens and E. faecium blood isolates compared to the previous six months [1]. Significant differences were found in the slope of non-susceptibility trends of Acinetobacter baumannii blood and respiratory isolates to amikacin, tigecycline and colistin and of Pseudomonas aeruginosa respiratory isolates to imipenem, meropenem and levofloxacin [1].
Few studies try to approach the causes of the significant impact of COVID-19 pandemic on antimicrobial resistance. The antibiotic consumption was irrational during the pandemic while the rates of microbiologically confirmed bacterial coinfection were low [14,15,16,17,18]. In a meta-analysis including 24 studies and focusing on bacterial co-infections in patients hospitalized for COVID-19 co-infection was reported in 3.5% (95%CI: 0.4–6.7%) and secondary infection in 14.3% (95%CI: 9.6–18.9%) of patients with COVID-19 [19]. The reported bacterial infection was 6.9% ranging from 5.9% in hospitalized patients to 8.1% in critically ill patients [19]. Many microorganisms have been reported as co-pathogens, including Streptococcus pneumoniae, S. aureus, K. pneumoniae, Mycoplasma pneumoniae, Chlamydophila pneumoniae, Legionella pneumophila, E. coli, P. aeruginosa, S. maltophilia, A. baumannii, Mycobacterium tuberculosis, Candida spp., Aspergillus spp. and viruses such as influenza, rhinovirus/enterovirus, parainfluenza virus, metapneumovirus and human immunodeficiency virus (HIV) [20,21,22,23,24]. The majority of multidrug resistant microorganisms were developed in patients with severe or critical COVID-19 resulting in prolonged hospitalisation and increased mortality rates [25].
In our study a high frequency of A. baumannii blood and respiratory isolates was observed with high levels of non-susceptibility to carbapenem and colistin throughout the study period. A. baumannii is one of the ESKAPE organisms (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, A. baumannii, Pseudomonas aeruginosa, and Enterobacter spp.) and remains a therapeutic challenge with constantly increasing resistance [26]. Multi-drug-resistant A. baumannii isolates have been identified in COVID-19 patients in both blood and respiratory isolates, mainly from ICUs, and with high rates of resistance in almost all widely used antibiotics, such as carbapenems, colistin and tigecycline [27,28,29,30]. Increasing trend was also reported in non-susceptible strains of Klebsiella pneumoniae during COVID-19 pandemic period. In Greece high rates of carbapenem-resistant K. pneumoniae isolates due to carbapenemase-producing strains have been documented since 2002 [31]. A literature review of carbapenem-resistant Klebsiella pneumoniae infections in patients hospitalized due to COVID-19 the prevalence of coinfection ranged from 0.35% to 53% [32].
Studies have shown that over 70% of patients with COVID-19 receive antibiotics, with the majority constituting broad-spectrum agents such as fluoroquinolones and third-generation cephalosporins [19]. A study including 138 hospitalised patients showed that moxifloxacin, ceftriaxone and azithromycin were prescribed in 89 (64.5%), 34 (24.6%) and 25 (18.1%) patients, respectively [33]. In a large-scale study with 1099 patients 58% received intravenous antibiotics [34]. In a smaller Brazilian cohort of 72 hospitalised patients 84.7% had received intravenously antibiotic therapy [35]. Among antibiotics, β-lactams were the main antibiotic category administered during pandemic period [36,37]. Azithromycin, the macrolide most used alone or in combination with β-lactams, vancomycin, carbapenems, tigecycline, ceftriaxone and linezolid, which are all classified as critically important antimicrobials (CIA) by WHO are being widely prescribed during this pandemic [38].
Our study findings support that the use of routine bedside consultation in the prepandemic period for the management of bloodstream infections is superior to telephone consultation which was mainly applied during COVID-19 pandemic. Patients in group A with bedside consultations were more likely to have an identified focus of infection, a better clinical outcome and receive longer courses of antimicrobial therapy often with combination of antibiotics. Longer treatment course in group A was probably due to higher rates of inpatient follow-up estimation by the infectious diseases specialist resulting to improved compliance to recommendations, higher frequency for repeated blood cultures and appropriate evaluation of clinical and lab biomarkers. An observational cohort study of 571 adults with Staphulococcus aureus bacteraemia at a teaching hospital in the United Kingdom between July 2006 and December 2012 showed that bedside consultation was associated with lower mortality at 30 days compared to telephone consultation (12% vs. 22%, p 0.07) [39]. Another study in Helsinki University Central Hospital in Finland including 342 adults with at least 1 positive blood culture for S. aureus were retrospectively analysed [40]. Seventy-two percent of patients received bedside, 18% telephone, and 10% no consultation [40]. Patients with bedside consultation had lower mortality than patients with telephone consultation at 7 days (OR,0.09; 95% CI, .02–.49; P = .001; 1% vs 8%), at 28 days (OR, 0.27; 95% CI, .11–.65; P = .002; 5% vs 16%) and at 90 days (OR, 0.25; 95% CI, .13–.51; P < .0001; 9% vs 29%) [40]. The above findings suggest that bedside consultations are superior to telephone and should become the standard of care for the management of bloodstream infections.
One of the limitations of the study is its retrospective. Further studies in larger patient series with simultaneous analyse of data from other hospitals are needed in order to better determine the impact of COVID-19 pandemic on antimicrobial resistance.
5. Conclusions
Our study provides significant results for the possible impact of COVID-19 pandemic on antimicrobial resistance which could be valuable for possible effective interventions. The high prevalence of multidrug-resistant pathogens, mainly due to carbapenem-resistant Gram-negative bacilli, is a major public health problem. The pressure of COVID-19 pandemic in healthcare systems was enormous limiting the surveillance programmes of infectious diseases. Antimicrobial resistance is an emerging silent parallel pandemic. The present study showed an increased frequency of isolated multidrug resistant bacteria in blood and respiratory samples during the COVID-19 period with high non-susceptibility rates to antibiotics. The management of bloodstream infections was also affected, while infectious diseases consultations were conducted mainly via telephone and not bedside. However, telephone consultations were associated with poorer clinical estimation and outcome with higher mortality rates. Our study, similarly with published data in the literature, concludes that they cannot replace bedside clinical estimation. Empowering of infectious diseases surveillance programs and committees and bedside infectious diseases consultations are vital in order to reduce the irrational use of antibiotics and the impact of infections by multidrug-resistant microorganisms.
Author Contributions
V.P. and M.P. conceived the idea; V.P., G.L., N.L. performed the collection of medical records; V.P. and P.P. wrote the manuscript; V.P. performed the statistical analysis; V.P, P.P., I.T, P.R. and D.P. were responsible consultants of the patients. All authors have read and agreed to the published version of the manuscript.
Funding
No funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
PP has been an advisory board member of GS, MSD, JANSSEN; received honoraria as a speaker for GS, JANSSEN, MSD..6. Patents.
References
- Polemis, M.; Mandilara, G.; Pappa, O.; Argyropoulou, A.; Perivolioti, E.; Koudoumnakis, N.; Pournaras, S.; Vasilakopoulou, A.; Vourli, S.; Katsifa, H.; et al. COVID-19 and Antimicrobial Resistance: Data from the Greek Electronic System for the Surveillance of Antimicrobial Resistance-WHONET-Greece (January 2018-March 2021). Life (Basel). 2021, 11, 996. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J. Review on Antimicrobial Resistance: Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. Wellcome Trust; London, UK: 2016. 20p. Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf. (accessed on 18 August 2021).
- WHO Global Action Plan on Antimicrobial Resistance. https://www.who.int/publications/i/item/9789241509763.
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; Ouakrim, D.A.; Oliveira, T.C.; Struelens, M.J.; Suetens, C.; Monnet, D.L.; Burden of AMR Collaborative Group. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: a population-level modelling analysis. Lancet Infect Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Chen, S.Y.; Ko, W.C.; Hsueh, P.R. Increased antimicrobial resistance during the COVID-19 pandemic. Int J Antimicrob Agents. 2021, 57, 106324. [Google Scholar] [CrossRef] [PubMed]
- Tiri, B.; Sensi, E.; Marsiliani, V.; Cantarini, M.; Priante, G.; Vernelli, C.; et al. Antimicrobial stewardship program, COVID-19, and infection control: spread of carbapenem-resistant Klebsiella pneumoniae colonization in ICU COVID-19 patients. What did not work? J Clin Med. 2020, 9, E2744. [Google Scholar] [CrossRef] [PubMed]
- Knight, G.M.; Glover, R.E.; McQuaid, C.F.; Olaru, I.D.; Gallandat, K.; Leclerc, Q.J.; Fuller, N.M.; Willcocks, S.J.; Hasan, R.; van Kleef, E.; Chandler, C.I. Antimicrobial resistance and COVID-19: Intersections and implications. Elife 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Baño, J.; Rossolini, G.M.; Schultsz, C.; Tacconelli, E.; Murthy, S.; Ohmagari, N.; Holmes, A.; Bachmann, T.; Goossens, H.; Canton, R.; Roberts, A.P.; Henriques-Normark, B.; Clancy, C.J.; Huttner, B.; Fagerstedt, P.; Lahiri, S.; Kaushic, C.; Hoffman, S.J.; Warren, M.; Zoubiane, G.; Essack, S.; Laxminarayan, R.; Plant, L. Key considerations on the potential impacts of the COVID-19 pandemic on antimicrobial resistance research and surveillance. Trans R Soc Trop Med Hyg. 2021, 115, 1122–1129. [Google Scholar] [CrossRef]
- CLS Clinical and Laboratory Standards Institute. Available online: https://clsi.org/standards/products/microbiology/. (accessed on 24 April 2023).
- EUCAST European Committee on Antimicrobial Susceptibility Testing. [(accessed on 24 Aoril 2023)]. Available online: https://www.eucast.org/.
- Patel, J.; Sridhar, D. The pandemic legacy of antimicrobial resistance in the USA. Lancet Microbe. 2022, 3, e726–e727. [Google Scholar] [CrossRef]
- Food and Agriculture Organization of the United Nations. World Organisation for Animal Health. WHO Global Database for the Tripartite Antimicrobial Resistance (AMR) Country Self-assessment Survey (TrACSS) https://amrcountryprogress.org/#/response-overview.
- Centers for Disease Control and Prevention. US Department of Health and Human Services, CDC; Atlanta, GA: 2022. COVID-19: US impact on antimicrobial resistance, special report 2022.
- Liew, Y.; Lee, W.H.L.; Tan, L.; Kwa, A.L.H.; Thien, S.Y.; Cherng, B.P.Z.; Chung, S.J. Antimicrobial stewardship programme: A vital resource for hospitals during the global outbreak of coronavirus disease 2019 (COVID-19) Int. J. Antimicrob. Agents. 2020, 56, 106145. [Google Scholar] [CrossRef]
- Molla, M.M.A.; Yeasmin, M.; Islam, M.K.; Sharif, M.M.; Amin, M.R.; Nafisa, T.; Ghosh, A.K.; Parveen, M.; Arif, M.M.H.; Alam, J.A.J.; et al. Antibiotic prescribing patterns at COVID-19 dedicated wards in Bangladesh: Findings from a single center study. Infect. Prev. Pract. 2021, 3, 100134. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. J. Am. Med. Assoc. 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Castaldi, S.; Luconi, E.; Marano, G.; Auxilia, F.; Maraschini, A.; Bono, P.; Ungaro, R.; Bandera, A.; Boracchi, P.; Biganzoli, E. Hospital acquired infections in COVID-19 patients in sub intensive care unit. Acta Biomed. 2020, 91, e2020017. [Google Scholar]
- Hughes, S.; Troise, O.; Donaldson, H.; Mughal, N.; Moore, L.S.P. Bacterial and fungal coinfection among hospitalized patients with COVID-19: A retrospective cohort study in a UK secondary-care setting. Clin. Microbiol. Infect. 2020, 26, 1395–1399. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: a living rapid review and meta-analysis. Clin Microbiol Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Sharifipour, E.; Shams, S.; Esmkhani, M.; Khodadadi, J.; Fotouhi-Ardakani, R.; Koohpaei, A.; et al. Evaluation of bacterial co-infections of the respiratory tract in COVID-19 patients admitted to ICU. BMC Infect Dis. 2020, 20, 646. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Wang, C.Y.; Hsueh, P.R. Co-infections among patients with COVID-19: the need for combination therapy with non-anti-SARS-CoV-2 agents? J Microbiol Immunol Infect. 2020, 53, 505–512. [Google Scholar] [CrossRef] [PubMed]
- 32. Lai C.C.; Yu W.L. COVID-19 associated with pulmonary aspergillosis: a literature review. J Microbiol Immunol Infect. 2021, 54, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Vilbrun, S.C.; Mathurin, L.; Pape, J.W.; Fitzgerald, D.; Walsh, K.F. Case report: Multidrug-resistant tuberculosis and COVID-19 coinfection in Port-au-Prince, Haiti. Am J Trop Med Hyg. 2020, 103, 1986–1988. [Google Scholar] [CrossRef]
- Yousaf, Z.; Khan, A.A.; Chaudhary, H.A.; Mushtaq, K.; Parengal, J.; Aboukamar, M.; et al. Cavitary pulmonary tuberculosis with COVID-19 coinfection. IDCases. 2020, 22, e00973. [Google Scholar] [CrossRef]
- Sharifipour, E.; Shams, S.; Esmkhani, M.; Khodadadi, J.; Fotouhi-Ardakani, R.; Koohpaei, A.; et al. Evaluation of bacterial co-infections of the respiratory tract in COVID-19 patients admitted to ICU. BMC Infect Dis. 2020, 20, 646. [Google Scholar] [CrossRef]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Kyriakidis, I.; Vasileiou, E.; Pana, Z.D.; Tragiannidis, A. Acinetobacter baumannii antibiotic resistance mechanisms. Pathogens 2021, 10, 373. [Google Scholar] [CrossRef] [PubMed]
- Lima, W.G.; Brito, J.C.M.; da Cruz Nizer, W.S. Ventilator-associated pneumonia (VAP) caused by carbapenem-resistant Acinetobacter baumannii in patients with COVID-19: Two problems, one solution? Med. Hypotheses. 2020, 144, 110139. [Google Scholar] [CrossRef] [PubMed]
- Yock-Corrales, A.; Lenzi, J.; Ulloa-Gutiérrez, R.; Gómez-Vargas, J.; Yassef, A.-M.O.; Rios Aida, J.A.; del Aguila, O.; Arteaga-Menchaca, E.; Campos, F.; Uribe, F.; et al. Antibiotic prescriptions in children with COVID-19 and multisystem inflammatory syndrome: A multinational experience in 990 cases from Latin America. Acta Paediatr. 2021, 110, 1902–1910. [Google Scholar] [CrossRef] [PubMed]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaëlo, M.; Flandre, P.L.; Dubert, M.; Cally, R.; Logre, E.; Fraissé, M.; Mentec, H.; et al. Bacterial and viral co-infections in patients with severe SARS-CoV-2 pneumonia admitted to a French ICU. Ann. Intensive Care. 2020, 10, 119. [Google Scholar] [CrossRef] [PubMed]
- Polemis, M.; Tryfinopoulou, K.; Giakkoupi, P.; Vatopoulos, A. ; WHONET-Greece Study Group Eight-year trends in the relative isolation frequency and antimicrobial susceptibility among bloodstream isolates from Greek hospitals: Data from the Greek electronic system for the surveillance of antimicrobial resistance—WHONET Greece, 2010 to 2017. Eurosurveillance 2020, 25, 1900516. [Google Scholar] [PubMed]
- Mędrzycka-Dąbrowska, W.; Lange, S.; Zorena, K.; Dąbrowski, S.; Ozga, D.; Tomaszek, L. Carbapenem-resistant klebsiella pneumoniae infections in ICU COVID-19 patients—A scoping review. J. Clin. Med. 2021, 10, 2067. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Teich, V.D.; Klajner, S.; Santiago de Almeida, F.A.; Batista Dantas, A.C.; Laselva, C.R.; Torritesi, M.G.; et al. Epidemiologic and clinical features of patients with COVID-19 in Brazil. Einstein (Sao Paulo) 2020, 18, eAO6022. [Google Scholar] [CrossRef]
- Lai, C.C.; Chen, S.Y.; Ko, W.C.; Hsueh, P.R. Increased antimicrobial resistance during the COVID-19 pandemic. Int. J. Antimicrob. Agents. 2021, 57, 106324. [Google Scholar] [CrossRef]
- Gonzalez-Zorn, B. Antibiotic use in the COVID-19 crisis in Spain. Clin. Microbiol. Infect. 2021, 27, 646–647. [Google Scholar] [CrossRef] [PubMed]
- Barrasa, H.; Rello, J.; Tejada, S.; Martin, A.; Balziskueta, G.; Vinuesa, C.; Fernandez-Miret, B.; Villagra, A.; Vallejo, A.; San Sebastian, A.; et al. SARS-CoV-2 in Spanish intensive care units: Early experience with 15-day survival in Vitoria. Anaesth. Crit. Care Pain Med. 2020, 39, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Saunderson, R.B.; Gouliouris, T.; Nickerson, E.K.; Cartwright, E.J.; Kidney, A.; Aliyu, S.H.; Brown, N.M.; Limmathurotsakul, D.; Peacock, S.J.; Török, M.E. Impact of routine bedside infectious disease consultation on clinical management and outcome of Staphylococcus aureus bacteraemia in adults. Clin Microbiol Infect. 2015, 21, 779–85. [Google Scholar] [CrossRef] [PubMed]
- Forsblom, E.; Ruotsalainen, E.; Ollgren, J.; Jarvinen, A. Telephone Consultation Cannot Replace Bedside Infectious Disease Consultation in the Management of Staphylococcus aureus Bacteremia. Clinical Infectious Diseases 2013, 56, 527–535. [Google Scholar] [CrossRef]
Figure 1.
Rates (%) of non-susceptible Acinetobacter baumannii isolates from blood and respiratory specimens to meropenem, amikacin and colistin, per semester, from patients hospitalized in wards and ICU, 2018–2022.
Figure 1.
Rates (%) of non-susceptible Acinetobacter baumannii isolates from blood and respiratory specimens to meropenem, amikacin and colistin, per semester, from patients hospitalized in wards and ICU, 2018–2022.
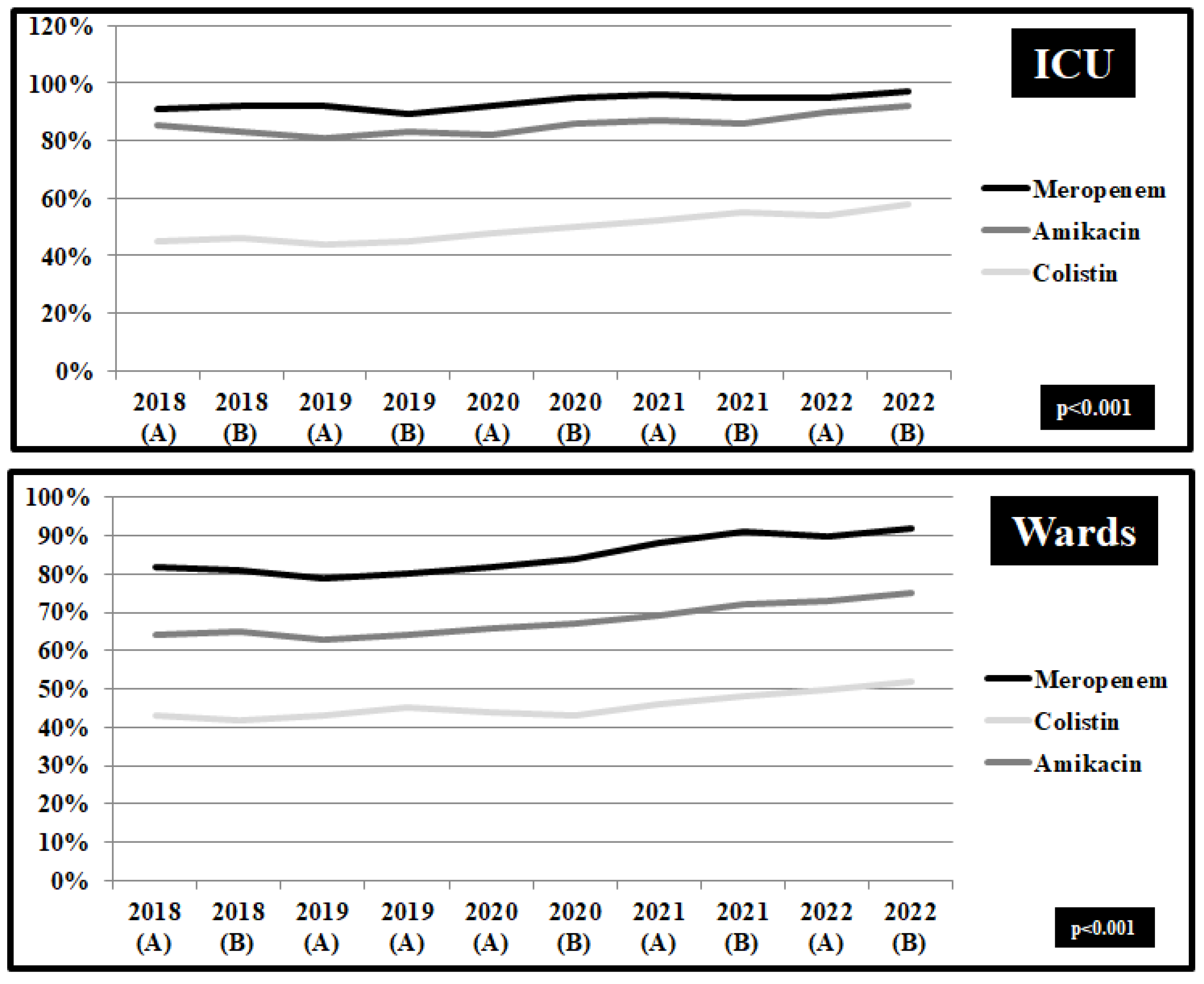
Figure 2.
Rates (%) of non-susceptible Klebsiella pneumoniae isolates from blood and respiratory specimens to meropenem and colistin, per semester, from patients hospitalized in wards and ICU, 2018–2022.
Figure 2.
Rates (%) of non-susceptible Klebsiella pneumoniae isolates from blood and respiratory specimens to meropenem and colistin, per semester, from patients hospitalized in wards and ICU, 2018–2022.
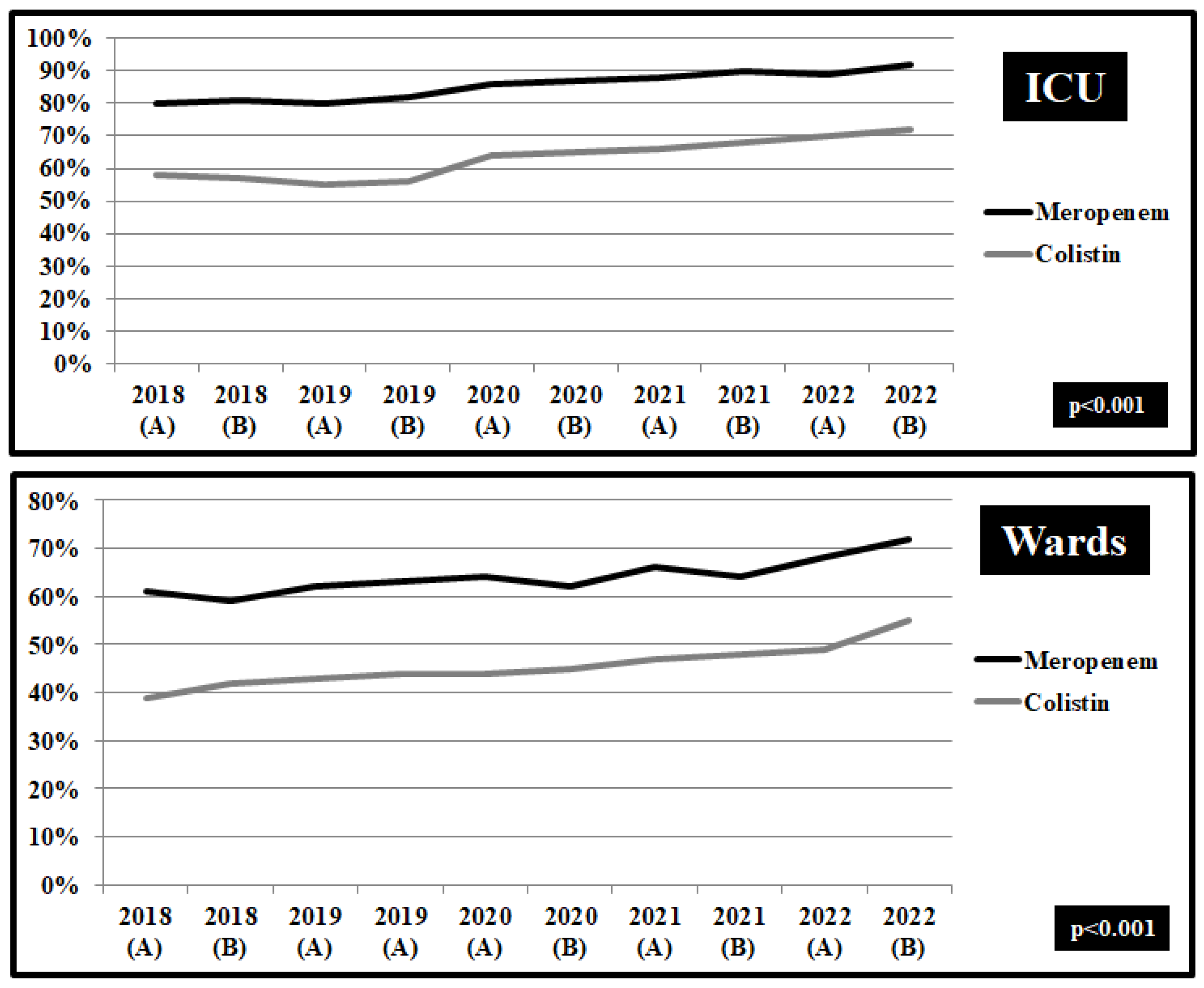
Figure 3.
Rates (%) of non-susceptible Pseudomonas aeruginosa isolates from blood and respiratory specimens to meropenem, amikacin and levofloxacin, per semester, from patients hospitalized in wards and ICU, 2018–2022.
Figure 3.
Rates (%) of non-susceptible Pseudomonas aeruginosa isolates from blood and respiratory specimens to meropenem, amikacin and levofloxacin, per semester, from patients hospitalized in wards and ICU, 2018–2022.
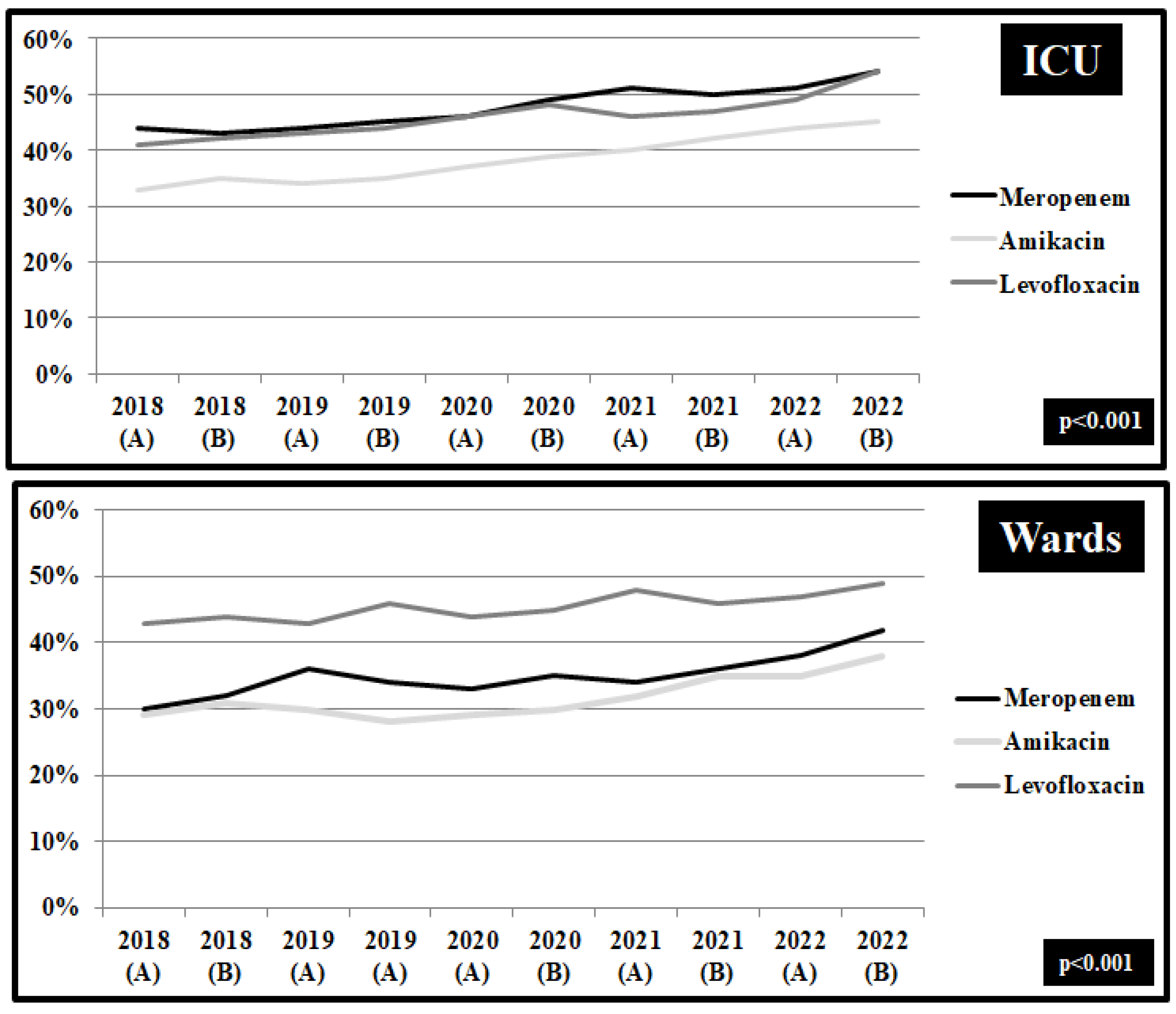
Figure 4.
Rates (%) of non-susceptible Enterococcus feacium isolates from blood and respiratory specimens to vancomycin, per semester, from patients hospitalized in wards, 2018–2022.
Figure 4.
Rates (%) of non-susceptible Enterococcus feacium isolates from blood and respiratory specimens to vancomycin, per semester, from patients hospitalized in wards, 2018–2022.
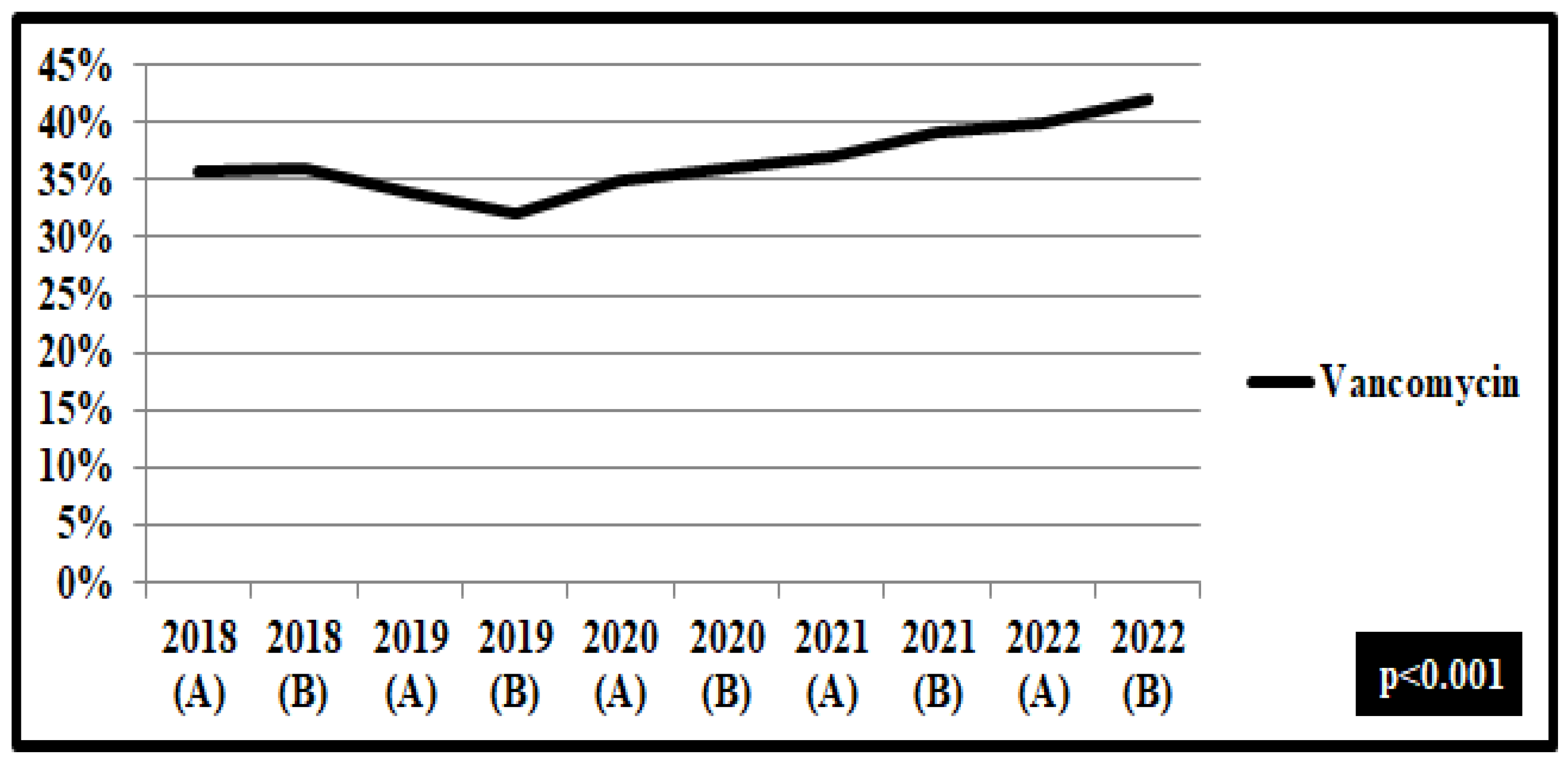
Figure 5.
Rates (%) of non-susceptible Staphylococcus aureus isolates from blood and respiratory specimens to methicilin, per semester, from patients hospitalized in wards, 2018–2022.
Figure 5.
Rates (%) of non-susceptible Staphylococcus aureus isolates from blood and respiratory specimens to methicilin, per semester, from patients hospitalized in wards, 2018–2022.
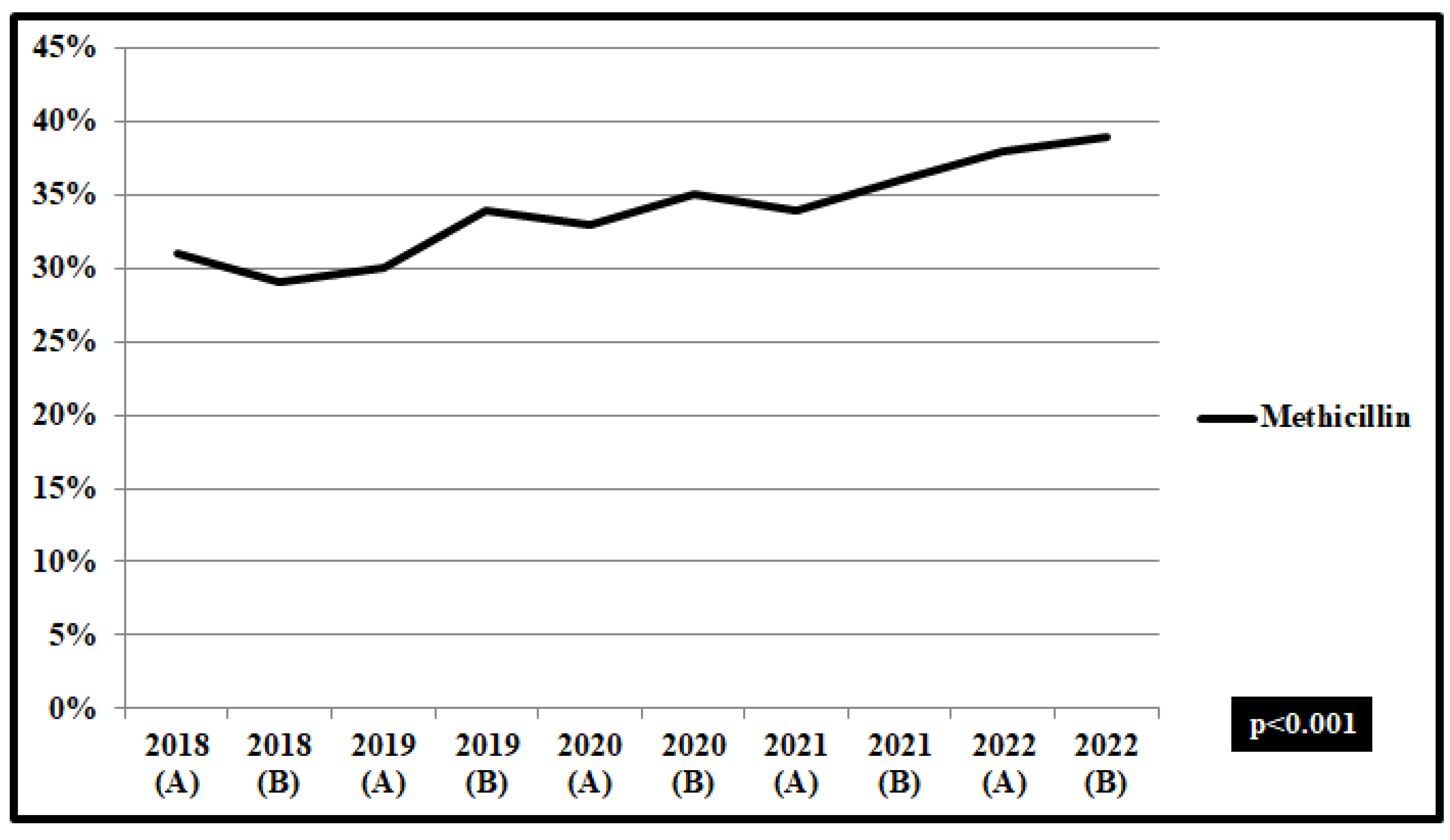

Table 1.
Gram-negative and positive bacteria isolated in blood and respiratory specimens in ICU, n=1216 (2018-2019).
Table 1.
Gram-negative and positive bacteria isolated in blood and respiratory specimens in ICU, n=1216 (2018-2019).
| Time of isolation | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Year | 2018 | 2019 | 2020 | 2021 | 2022 | |||||
| Semester | 1st | 2nd | 1st | 2nd | 1st | 2nd | 1st | 2nd | 1st | 2nd |
| Isolated Bacteria in ICU (n=1216) in blood & respiratory specimens | ||||||||||
| Acinetobacter baumannii | 40 | 33 | 39 | 40 | 47 | 41 | 49 | 48 | 53 | 50 |
| Klebsiella pneumoniae | 24 | 28 | 26 | 25 | 29 | 36 | 32 | 36 | 40 | 37 |
| Pseudomonas aeruginosa | 17 | 19 | 19 | 17 | 23 | 25 | 27 | 28 | 35 | 39 |
| Enterococcus faecium | 7 | 7 | 8 | 9 | 6 | 9 | 11 | 8 | 13 | 14 |
| Staphylococcus aureus | 8 | 9 | 10 | 10 | 14 | 12 | 16 | 10 | 16 | 19 |
| Total | 96 | 94 | 102 | 101 | 119 | 123 | 135 | 130 | 157 | 159 |
Table 2.
Gram-negative and positive bacteria isolated in blood and respiratory specimens in wards, n=3353 (2018-2019).
Table 2.
Gram-negative and positive bacteria isolated in blood and respiratory specimens in wards, n=3353 (2018-2019).
| Time of isolation | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | 2018 | 2019 | 2020 | 2021 | 2022 | ||||||
| Semester | 1st | 2nd | 1st | 2nd | 1st | 2nd | 1st | 2nd | 1st | 2nd | |
| Isolated Bacteria in wards (n=1216) in blood & respiratory specimens | |||||||||||
| Acinetobacter baumannii | 94 | 95 | 85 | 89 | 80 | 78 | 88 | 94 | 102 | 98 | |
| Klebsiella pneumoniae | 75 | 69 | 75 | 72 | 72 | 74 | 71 | 75 | 78 | 78 | |
| Pseudomonas aeruginosa | 63 | 65 | 76 | 75 | 63 | 73 | 89 | 85 | 81 | 88 | |
| Enterococcus faecium | 16 | 19 | 21 | 20 | 24 | 23 | 25 | 22 | 24 | 32 | |
| Staphylococcus aureus | 72 | 71 | 66 | 65 | 70 | 72 | 77 | 85 | 72 | 73 | |
| Total | 320 | 321 | 323 | 321 | 309 | 322 | 350 | 361 | 357 | 369 | |
Table 3.
Multivariable logistic regression analysis. Risk of death and prolonged hospital stay in hospitalized patients in wards and ICU with isolated Gram-negative/positive bacteria, per year, 2018-2022.
Table 3.
Multivariable logistic regression analysis. Risk of death and prolonged hospital stay in hospitalized patients in wards and ICU with isolated Gram-negative/positive bacteria, per year, 2018-2022.
| Risk of Death, OR (95% CI) |
Risk of Prolonged Hospital Stay, OR(95% CI) |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2018 | 2019 | 2020 | 2021 | 2022 | 2018 | 2019 | 2022 | 2021 | 2022 | ||
| Acinetobacter baumannii | 3.6 (2.1-4.5) |
3.5 (2.4-5.1) |
3.9 (3.1-6.1) |
4.1 (3.4-6.1) |
4.2 (3.5-5.2) |
7.6 (5.3-9.5) |
7.8 (6.2-9.2) |
7.9 (7.2-9.4) |
7.8 (6.9-9.2) |
8.2 (7.6-10.1) |
|
| Klebsiella pneumoniae | 3.1 (2.4-5.1) |
3.3 (2.2-5.1) |
3.6 (2.8-5.7) |
3.5 (2.9-4.3) |
3.8 (2.6-4.1) |
6.5 (5.4-7.9) |
6.7 (5.6-8.4) |
6.7 (6.2-8.6) |
6.9 (5.9-7.8) |
7.1 (6.5-8.9) |
|
| Pseudomonas aeruginosa | 3.1 (2.4-4.7) |
3.4 (2.4-4.9) |
3.8 (2.4-5.9) |
3.7 (2.9- 2.8) |
3.9 (3.1-4.3) |
5.6 (4.6-7.3) |
5.8 (4.5-7.9) |
5.9 (4.5-7.2) |
6.4 (5.9-7.3) |
6.5 (4.9-8.2) |
|
| Enterococcus faecium | 1.4 (0.9-1.8) |
1.6 (1.1-3.6) |
1.6 (1.2-3.4) |
1.9 (1.1- 2.2) |
2.1 (1.7-2.9) |
3.9 (3.1-5.3) |
3.8 (3.1-5.7) |
4.2 (3.6-6.3) |
4.6 (4.5-7.6) |
4.8 (4.1-7.3) |
|
| Staphylococcus aureus | 3.0 (2.1-4.9) |
3.0 (2.2-4.7) |
3.1 (2.3- 4.5) |
3.2 (2.4-4.1) |
3.4 (2.8-4.9) |
2.3 (2.1-4.6) |
2.3 (2.1-4.3) |
2.4 (2.1-4.1) |
2.4 (1.8-4.3) |
2.6 (2.2-5.1) |
|
| P<0.001 | P<0.001 | ||||||||||
Table 4.
Baseline characteristics of patients with bloodstream infections.
| Prepandemic period 2018-2019 (n=246) Group A |
COVID-19 Pandemic 2020-2022 (n=154) Group B |
|
|---|---|---|
| Gender, male | 166 (67.2%) | 98 (63.6%) |
| Age, years, mean ± SD | 65.6 (50.4–76.4) | 65.8 (50.5–77.4) |
| Duration of bacteraemia symptoms before treatment initiation | ||
| 0–24 hours | 158 (64.2%) | 73 (47.4%) |
| 25–72 hours | 25 (10.2%) | 34 (22.1%) |
| >72 hours | 55 (22.4%) | 36 (23.4%) |
| Unknown | 8 (3.2%) | 11 (7.1%) |
| Telephone consultation | 37 (15%) | 117 (76%) |
| Bedside consultation | 209 (85%) | 37 (24%) |
Table 5.
Comorbidities of patients with bloodstream infection and reported infectious diseases consultation.
Table 5.
Comorbidities of patients with bloodstream infection and reported infectious diseases consultation.
| Group A, 2018-2019 (n=246) |
Group B, 2020-2022 (n=154) |
P value | |
|---|---|---|---|
| Operation within 30 days | 34 (13.8%) | 29 (18.8%) | 0,04 |
| Diabetes Mellitus type 2 | 89 (36.2%) | 68 (44.2%) | 0,12 |
| Heart Failure | 26 (10.6%) | 19 (12.3%) | 0,02 |
| Coronary disease | 49 (19.9%) | 18 (11.7%) | 0,45 |
| Peripheral Vascular Disease | 11 (4.5%) | 12 (7.8%) | 0,12 |
| Cerebrovascular Disease | 18 (7.3%) | 17 (11%) | 0,05 |
| Chronic respiratory disease | 9 (3.7%) | 8 (5.2%) | 0,04 |
| Malignancies | 25 (10.2%) | 35 (22.7%) | 0,24 |
| Transplantation | 14 (5.7%) | 11 (7.14%) | 1,02 |
| Immunosuppresion | 38 (15.4%) | 24 (15.6%) | 0,87 |
| Chronic renal disease | 22 (8.9%) | 19 (12.3%) | 0,04 |
| Prosthetic Device | 56 (22.8%) | 47 (30.5%) | 0,02 |
|
Charlson comorbidity index Score ≥3 |
102 (41%) | 67 (43.5%) | 0,02 |
Table 6.
Clinical features of infections in adults with bloodstream infections.
| Group A 2018-2019 (n=246) |
Group B 2020-2022 (n=154) |
P value | |
|---|---|---|---|
| Community acquired infection | 96 (39%) | 56 (36.3%) | 0.001 |
| Hospital acquired infection | 150 (61%) | 98 (63.6%) | 0.001 |
| Multidrug resistant bacteria | 83 (33.7%) | 57 (37%) | 0.001 |
| Focus of infection | |||
| Unknown | 16 (6,5%) | 18 (11,7%) | 0,004 |
| Central venous catheter | 46 (18.7%) | 31 (20.1%) | 0,156 |
| Peripheral venous catheter | 34 (13.8%) | 21 (13.6%) | 0,458 |
| Thrombophebitis | 12 (4.9%) | 27 (17.5%) | 0,024 |
| Implanted vascular device | 21 (8.5%) | 16 (10.4%) | 0,048 |
| Infective Endocarditis | 11 (4.5%) | 16 (10.4%) | 0,678 |
| Native valve | 6 (2.4%) | 7 (4.5%) | 0,465 |
| Prosthetic valve | 5 (2%) | 9 (5.8%) | 0,247 |
| Joint infection | 10 (4.1%) | 9 (5.8%) | 0,765 |
| Prosthetic Joint Infection | 15 (6.1%) | 19 (12.3%) | 0,223 |
| Vertebral osteomyelitis | 13 (5.3%) | 17 (11%) | 0,058 |
| Intra-abdominal infections | 26 (10%) | 18 (11.7%) | 0,047 |
| Osteomyelitis/ Diabetic foot ulcers | 29 (11.8%) | 20 (13%) | 0,023 |
| Skin and soft tissue infections | 24 (9.8%) | 19 (12.3%) | 0,027 |
| Respiratory infections | 32 (13%) | 21 (13.6%) | 0,057 |
| Urinary tract infections | 19 (7.7%) | 16 (10.4%) | 0,077 |
| Central nervous system infections | 9 (3.7%) | 7 (4.5%) | 0,065 |
| Complicated infection | 134 (54.5%) | 87 (56.5%) | 0.001 |
Table 7.
Clinical indicators and outcomes in the management of bloodstream infections.
| Group A 2018-2019 (n=246) |
Group B 2020-2022 (n=154) |
P value | |
|---|---|---|---|
| Septic shock | 8 (3,3%) | 7 (4,5%) | 0,118 |
| Hospitalization in ICU | 11 (4,5%) | 12 (7,8%) | 0,245 |
| Hospital stay, days, mean ± SD | 29 (17–52) | 30 (16–51) | 0,457 |
| Mortality | |||
| Within 28 days | 12 (4,9%) | 16 (10,4%) | 0,001 |
| Within 90 days | 19 (7,7%) | 23 (14,9%) | 0,001 |
| Repeated blood culture | 137 (55,7%) | 56 (36,4%) | 0,001 |
| Negative blood culture within 7 days | 98 (40%) | 48 (31,2%) | 0,001 |
| Recurrent disease | 9 (3,6%) | 6 (3,9%) | 0,458 |
| Duration of antibiotic treatment, days, mean ± SD | 15 (8-19) | 11 (6-12) | 0,04 |
| Repeated clinical estimation | 112 (45,5%) | 36 (23,4%) | 0,001 |
| Combination of antibiotics | 26 (10,6%) | 11 (7,1%) | 0,001 |
| Recorded bloodstream infection (isolated pathogen) in discharge summary | 124 (50,4%) | 44 (28,6%) | 0,001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



