
Submitted:
27 November 2025
Posted:
28 November 2025
You are already at the latest version
Abstract
Access to health care is a fundamental human right established in various legal frameworks worldwide. However, increasing evidence indicates that individuals with physical disabilities in rural Ethiopia continue to face barriers and disparities in accessing health care, leading to unmet needs and worsening health. Guided by Critical Disability Theory and Intersectionality Theory, this instrumental case study explored the barriers to accessing primary health care (PHC) for adults with physical disabilities in rural Ethiopia and examined how disability intersects with poverty, gender, and rurality to shape exclusion. Following purposeful sampling, we conducted 14 interviews and one focus group discussion (n = 7) with adults with physical disabilities, supplemented by PHC facility infrastructure observation. Using reflexive thematic analysis, we identified intersecting barriers across four domains: physical and environmental barriers, socioeconomic marginalization, socio-cultural stigma and attitudinal barriers, and systemic weaknesses in health service delivery. This revealed that disability-related barriers are rooted in structural ableism and intersecting inequities, underscoring the urgent need for inclusive policies and disability-inclusive practices. Such practices include enforcing accessibility standards, expanding community-based health insurance to cover disability-specific needs, supporting transportation, and disability-specific training for health professionals. Implementing these practices is essential to advancing disability rights and ensuring equitable health access in Ethiopia.
Keywords:
primary health care
; physical disability
; rural health
; institutional ableism
; Ethiopia
1. Introduction
Disability—an umbrella term encompassing impairments, activity limitations, and participation restrictions arising from the interaction between individuals with health conditions and contextual factors—affects a significant and growing proportion of the global population. Based on global estimates as of 2021, it is estimated that approximately 1.3 billion individuals worldwide—accounting for 16% of the global population and 20% of those living in poverty—have disabilities [1]. In Ethiopia, disability prevalence is estimated at 17.6% [2], suggesting that approximately one in six Ethiopians has some form of disability [3]. People with disabilities require more frequent health care services compared to individuals without disabilities due to their increased vulnerability to health issues; hence, ensuring their access to appropriate health care services is essential for optimal health outcomes [4,5]. Delays or lack of timely health care access can lead to chronic conditions, secondary health problems, and the worsening of existing disability, ultimately resulting in poorer overall health outcomes [6,7,8].
Considering these vulnerabilities, international conventions and policies have been developed to support the health care rights of people with disabilities. For instance, Article 25 of the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) asserts that people with disabilities have the right to enjoy the highest attainable standard of health without discrimination [9]. This right is further supported by the Sustainable Development Goals (SDGs), particularly SDG 3 on universal health coverage (UHC) and SDG 10 on reducing inequalities, which highlight the importance of universal access to health care in achieving inclusive development [10]. Ethiopia has aligned with these international commitments through several policy actions, including (i) ratification of the UNCRPD in 2010 [11]; (ii) enactment of the Building Proclamation No. 624/2009, which requires all public facilities, including health centres, to be disability-friendly [12]; and (iii) establishment of community-based health insurance (CBHI) to improve financial protection and access to essential services for rural households [13].
Despite such policy commitments, people with disabilities continue to experience marked health disparities. For example, in a 2019 United Nations report, it was found that in low- and middle-income countries (LMICs) access to health care is three times lower for people with disabilities than for the general population, and 40% of people with disabilities report unmet health-care needs [14]. In Ethiopian-based studies, researchers have consistently documented physical, financial, informational, and attitudinal barriers as factors that impede health care access for people with disabilities [15,16,17,18,19,20]. Previous disability research in Ethiopia, however, has predominantly been quantitative, or disability-generic qualitative studies grounded in a biomedical model, providing descriptive accounts rather than critical analyses of structural ableism, power relations, and the intersection of social identities that reproduce these inequities.
The World Health Organization [1] emphasizes the urgency of rights-based research to guide fair health policies. Given its focus on structural ableism, intersecting oppressions, and the politics of representation [21], critical disability theory provides a transformative framework for examining why commitments to universal health coverage remain out of reach for people with disabilities in Ethiopia. Therefore, in this study, we explored the barriers to accessing primary health care (PHC) for individuals with physical disabilities in rural Ethiopia and examined how poverty, rurality, gender, and other axes of inequality intersect to shape exclusion from PHC. Addressing this critical knowledge gap is essential for developing evidence-based, structurally appropriate interventions (e.g., health policies and practices) that can help Ethiopia meet its commitments to disability-inclusive health and SDG 3, which is based on universal health coverage, access to quality health care, and health equity as vital components for sustainable development.
2. Materials and Methods
2.1. Theoretical Perspective
Our study was grounded in two complementary frameworks: Critical Disability Theory (CDT) and Intersectionality Theory. CDT is rooted in a social constructionist view of disability, emphasizing how the environment shapes who is considered disabled and who meets expectations of normalcy [21]. This theory interprets disability not solely as an individual characteristic but as a socio-political construct; it analyzes disability as a cultural, historical, social, and political phenomenon [21,22]. This perspective highlights the importance of addressing power relations, structural barriers, and the necessity of transformative action to achieve justice for individuals with disabilities.
CDT’s emphasis on an ableist social construction of disability aligns with intersectionality, which highlights the interconnected oppressive power structures that influence lived experiences and makes the argument for social change [23]. Intersectionality asserts that there is no single axis of oppression; instead, multiple factors interact in complex ways to create unique forms of disadvantage [24,25]. Therefore, intersectionality provides a framework for focusing on and critiquing disabling contexts. Recognizing its origins in Crenshaw’s analysis of discrimination against Black women at the intersections of racism, sexism, and classism, Collins and Bilge [26] also advocated for the application of intersectionality to other systems of oppression. Hence, Collins and Bilge’s Intersectionality Theory is employed as a guiding framework to analyze how overlapping social identities and power structures—such as disability status, gender, socioeconomic status, and rurality—intersect to influence individuals' health care experiences. Together, CDT and intersectionality informed the research on how physical disability intersects with other identities and structural forces in rural Ethiopia, and they guided the interpretation of findings by emphasizing intersecting power dynamics and structural inequities.
2.2. Study Design
We used an instrumental single-case study approach with embedded units of analysis [27]. The case was defined as access to PHC services for adults with physical disabilities in the Soddo district, Ethiopia, from October 2024 to February 2025. We chose an instrumental case approach because our goal was not only to describe experiences in Soddo but also to generate contextually grounded, theoretically informed insights that can influence policy and practice beyond this district. This design allows for an in-depth description of the case and its context [27].
2.3. Setting, Participants, and Recruitment
The study was conducted from October 2024 to February 2025 in the Soddo district, Central Ethiopia region. The Soddo district comprises 39 rural wards (kebeles) and has a population of 191,048. The district has one primary hospital, six health centers, and 39 health posts [28]. The administrator of the District Disability Association, ‘Lib Ke Lib People with Disabilities Association’, provided lists of potential participants.
Purposive sampling is a common and suitable approach in qualitative studies, enabling researchers to deliberately select participants who meet specific criteria relevant to the phenomenon of interest [29,30]. We included adults aged 18 years or older who self-identified as having a physical disability, could provide informed consent, communicated in Amharic (the national language), and had accessed or attempted to access PHC services at least once in the past 24 months, as of the study start date. However, individuals who were unable to recall their experiences with PHC access or were unwilling to share their experiences were excluded from the study. Using these criteria, 14 participants were enrolled in the study (see Table 1 for participant demographic characteristics).
2.4. Data Collection
The first author collected data through 14 in-depth individual interviews and one focus group discussion attended by seven participants. With participant consent, the interviews and the focus group discussion were audio-recorded. The first author took field notes during and immediately following each interview to record contextual information, non-verbal cues, and reflections that might not be evident from the audio recordings. According to Gill et al. and Kitzinger [31,32], individual interviews offer a private space for sensitive topics, and focus groups encourage participants to build on each other’s insights and develop shared perspectives. Furthermore, focus groups can generate valuable data by creating a supportive environment that encourages participants to share their stories and by fostering discussion that might not emerge during individual interviews [31]. Thus, using both approaches enabled us to capture personal narratives in depth and observe the interaction of ideas among the participants. The semi-structured interview guide used in this study is available from the corresponding author upon reasonable request.
In addition to the interviews and focus group, the first author also conducted direct observations at two health centres and two health posts to assess how well the environment accommodates people with physical disabilities. The observations aimed to identify infrastructural aspects within these facilities that could potentially impede PHC delivery for this population.
As this paper is part of the first author's doctoral thesis, he took the lead in data collection and analysis. Therefore, we acknowledge the first author’s positionality as a Black male, middle-class, and someone who does not identify as having a disability.
2.5. Data Analysis
All audio recordings were transcribed verbatim by the first author in the original language (Amharic), and the accuracy of each transcript was cross-checked against the recordings by a PhD student proficient in Amharic who was not part of the research team. This student signed confidentiality agreements and completed the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (TCPS 2) – Course on Research Ethics (CORE) through Queen’s University (Certificate). The field notes were incorporated at the end of the transcripts to serve as reminders of the reflections and contextual details noted during the interviews and focus group. The software program NVivo (version 14) was used for data management, organization, and coding. The data were analyzed using reflexive thematic analysis following the six-phase approach outlined by Braun and Clarke [33]. The process unfolded in the following order: 1) familiarity with the data occurred by repeatedly reading the Amharic transcripts while engaging in reflexive writing; 2) the transcripts were coded and the codes were organized into preliminary themes by clustering related codes that addressed common barriers or experiences; 3) the themes were reviewed and refined by returning to the data to ensure that each candidate theme was grounded in the participants’ accounts; 4) clear definitions for each theme were developed, which included assigning concise and descriptive names that accurately reflected their essence; and 5) a paper/report was created by selecting vivid, representative quotations and synthesizing an analytic narrative that connects the themes to the research questions and theoretical frameworks. Braun and Clarke [33] emphasize researcher subjectivity and reflexivity; therefore, throughout the analysis, the first author engaged in reflexive journaling to remain conscious of how his background and assumptions might influence theme development.
2.6. Trustworthiness
2.7. Ethical Considerations
Ethics approval was obtained from Queen's University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (TRAQ file #: 6041959) and University of Gondar Research Ethics Board (Protocol #: CMHSSH-UOG IRERC/50/11/24). We also secured permission and collaboration from the Sodo District Health Office and the Disability Association to conduct the research in the community (Ref#: 20249). All the participants provided informed consent prior to engaging in the interview or focus group. Each participant received a detailed explanation of the study’s purpose, procedures, and their rights, including the right to decline to answer any questions or to withdraw from the study at any time without consequence. Participants provided consent by signing or thumbprinting (for those with limited literacy), and the first author verbally reaffirmed consent before each interview and the focus group. To ensure confidentiality and privacy, the interviews were conducted at participants’ homes, pseudonyms were assigned to all participants, and all personal identifiers were removed from the transcripts. During the focus group, ground rules were established to maintain the confidentiality of shared information (e.g., participants were asked not to disclose others’ stories outside the group). The de-identified data was stored on a secure server at Queen’s University and was accessible only to research team members. No incentives were provided beyond reimbursement of travel expenses for attending the focus group.
3. Results
From the analysis, four main themes about the barriers faced by people with physical disabilities seeking PHC in rural Ethiopia were identified: physical and environmental barriers; socioeconomic marginalization; socio-cultural stigma and attitudinal barriers [sub-themes: community prejudice and health care providers' negative attitudes; and gendered health care neglect and domestic burdens]; and systemic weaknesses in health service delivery.
3.1. Physical and Environmental Barriers: “Every Negative Aspect is Stacked Against Us”: Challenges in Travelling to and Within Health Centers
This theme—physical and environmental barriers—is about how participants describe how the natural and built environments hinder their access to primary health facilities in Ethiopia. The participants consistently emphasized that geographic isolation, inadequate transportation, and inaccessible clinic infrastructure intersected with their disabilities and poverty, limiting their ability to seek timely health care. This theme revealed a continuum of barriers, from the journey to health care facilities to the structure of those facilities, demonstrating how physical and environmental factors—rather than individual incapacitating impairments—created systemic exclusion from health care access for these participants. The participants consistently described the overwhelming challenges posed by long distances and rough terrain, exacerbated by insufficient or prohibitively expensive transport options. Many lived in mountainous areas where journeys to the nearest health centre often required several hours navigating muddy pathways and rocky roads. Sashine explained that it takes her two and a half hours to walk to the health centre with a walking stick because “the road is bumpy and hilly… uneven.” and conditions worsen during rainfall, “It's just mud—slippery, dangerous.” Similarly, Kokit shared her experience despite living relatively close to services.
The health center is not very far—but for me, but for me, it is very challenging. I can't walk, so I have to use my hands to move. It can take me hours to get there … When I got there, there were many people in front of me, so I had to wait a long time … I came back home so tired. If it rains, it turns to mud, and the motorbikes can't pass—it just makes everything harder.
These narratives reveal how environmental factors made getting to health care services a formidable challenge in and of themselves. Since the rural infrastructure is not designed to accommodate the needs of individuals (such as the study participants) with physical disabilities, routine health care visits are an extraordinary ordeal. For some participants, the journey required assistance that highlighted this social disability. Maru, who uses crutches, recalled:
I was carried on a local stretcher for more than three hours just to reach the asphalt…
Then still a long way to the health center. Travelling this distance is hard with crutches, especially during the winter, when the road is muddy and slippery.
This extreme effort underscores how inaccessible transportation infrastructure created suffering and dependence for participants, forcing families to take extraordinary measures merely to access care. The physical exhaustion of navigating such routes was amplified by safety concerns, particularly for women participants who felt vulnerable travelling alone. Mazi articulated this intersectional vulnerability:
Sometimes I'm so afraid of falling and hurting myself. So I stay home ... just dealing with the pain on my own. And you know, I can't travel that distance alone. Anything could happen—what if I fall, or someone tries to take advantage of me? It's scary. So I always need someone to go with me.
Her experience demonstrated how disability, gender, and rurality intersected to compound vulnerability for this participant, often leading to health care avoidance rather than risking exposure to environmental dangers and potential exploitation.
Financial barriers further intensified the burden of distance for study participants. Public transportation was either unavailable or inaccessible to participants with disabilities, forcing impossible choices between unaffordable fares or dangerous journeys on foot. Sis, a wheelchair user, described discriminatory pricing:
Drivers only agree if we double the price. Putting the wheelchair in the car took some time, and it also takes up space. One day, I remember no vehicles stopped; they refused completely. I ultimately paid 200 birr, while the normal cost was 100 birr. That's robbery.
This pricing discrimination reflected how transportation systems significantly disadvantage individuals by failing to accommodate them equitably. Consequently, many participants relied entirely on family or neighbours for mobility, as public transportation was not attainable. As Kokit explained: “I have to rely on someone pushing me… the cars or other transportation is not really an option for me.” The compounding nature of these barriers was powerfully articulated during the focus group discussion. Yibe, a male participant, summarized the collective experience: “We all live far from town, too far from the clinic. Who lives nearby? No one. We can't afford the trip. We share disability. Every negative aspect—poverty, stigma—is stacked against us.” This reflection illustrates what could be termed a ‘rural penalty’ for individuals with physical disabilities—the intersection of distance, terrain, inadequate transport, gender, and poverty, creating a ‘perfect storm’ of barriers that make access to much-needed health facilities insurmountable.
Reaching the clinic was only the beginning of the accessibility challenges participants faced. Even after managing the difficult journey, the participants encountered inaccessible infrastructure that prevented entry, navigation, and full utilization of available services. These disability-unfriendly facilities, designed without considering the needs of people with disabilities, are institutional barriers that reflect what disability scholars such as Lundberg and Chen [36] called ‘institutional ableism’. A common challenge faced by people with physical disabilities at health facilities was navigating the entrance stairs. As shown in the photograph (Figure 1), health centers were one-story buildings with stairs at the entrance, posing a significant access obstacle. Sis articulated her frustration with this type of basic barrier to care:
There are four or five sets of steps at the entrance, but no way to pass them. So, how do I get in? I need to ask others for help. It's a shame … how often should I beg others to be lifted up like an object? I'm a human, and humans are respected creatures, right?
Sis’s rhetorical question is both heartbreaking and a poignant condemnation of how fundamental human rights are denied when public-serving institutions (such as health centres) make architectural design choices that gatekeep who receives treatment in favour of those without disability—these choices and their implications are perceived as blatantly marginalizing those with disability, seemingly making them not worthy of consideration or equal in their humanness. The absence of ramps reflects social assumptions about and deference to ‘normal’ bodies, as well as the implication that access to institutions is the responsibility of individuals, not the institution.
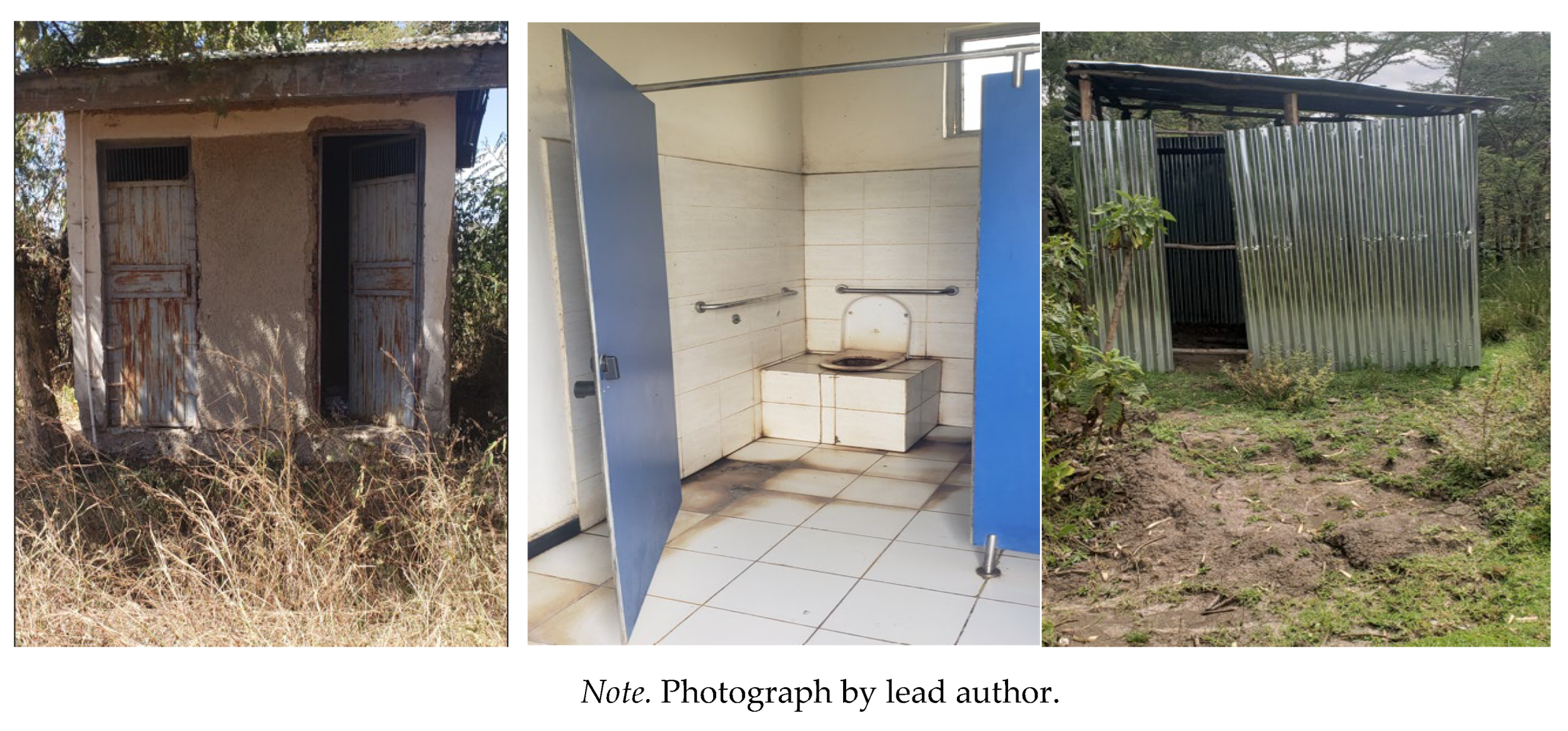
Interior barriers added yet another layer of difficulty. Basic facilities, such as restrooms, are often unusable or hazardous. Alex described the impossibility of providing routine samples: “They [the staff] say, ‘Go to the toilet and bring a stool sample.’ Who helps me to sit on the toilet? It’s so difficult for me, unthinkable.” Kal developed coping strategies, which unfortunately compromised his health: “If I know I'm going to the clinic, I don't drink or eat anything … I don’t use their toilet until I get home … who else would help me here? No one.” These accounts illustrate how exclusionary designs force individuals to jeopardize their health and sacrifice their dignity to conform to inaccessible systems that are meant to be for all.
Figure 2.
Washrooms in the Health Facilities.
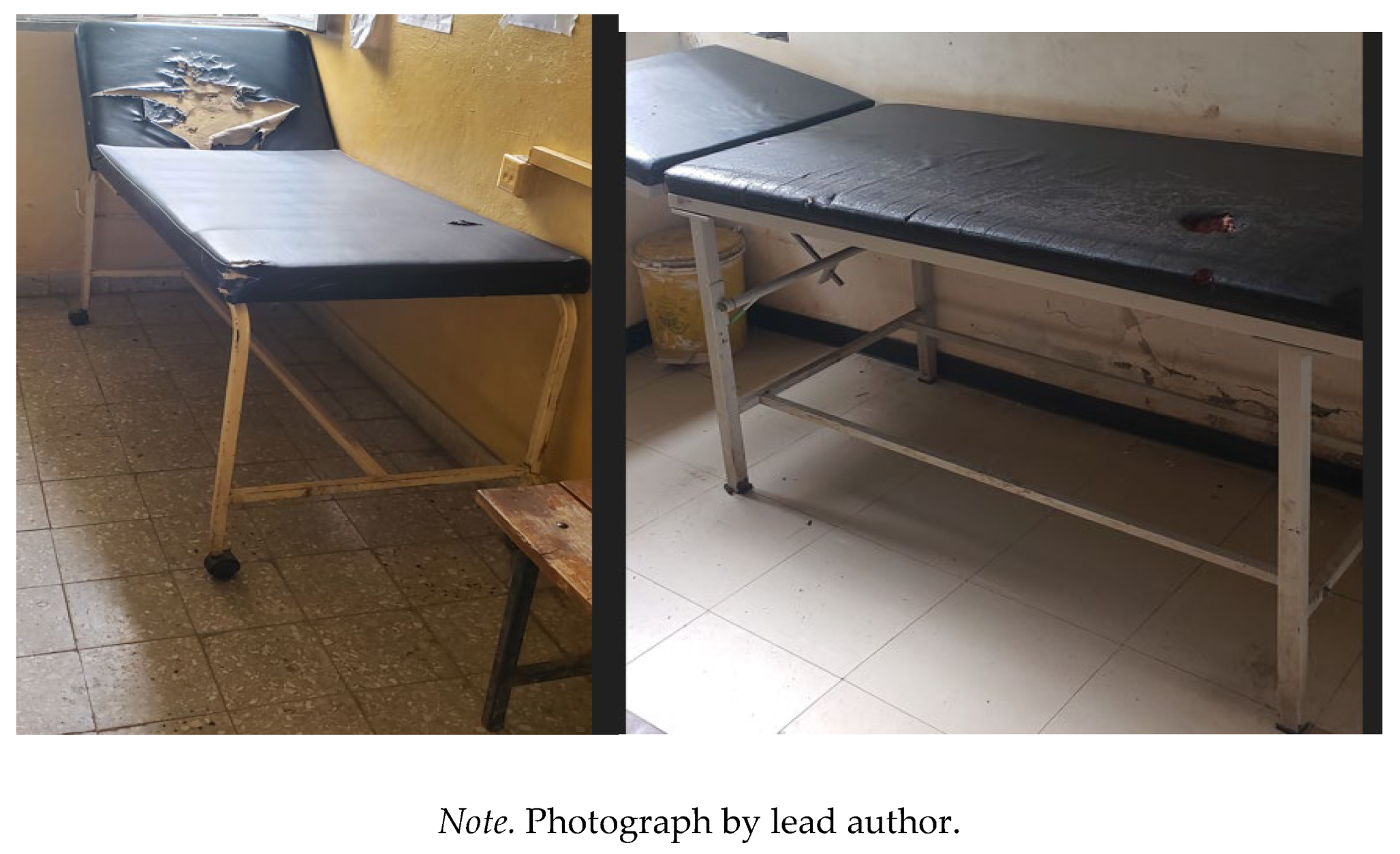
High, non-adjustable examination tables created additional barriers that particularly affected women participants. Shashie recounted her experience:
I know men are okay with this, but for us women, it feels so much worse—especially with this dress, skirt ... they asked me to climb onto that table, and I'm terrified. I'm thinking, 'Will I slip? Will I fall?' I feel so exposed up there. A man [health professional] carried and lifted me up. I hate that moment. And it's even more embarrassing, because it makes me feel completely helpless.
Her experience illustrated how routine medical examinations became dehumanizing when infrastructure failed to accommodate diverse bodies. The intersection of gender and disability intensified feelings of indignity for this participant, as being lifted onto tables violated independence and cultural modesty norms. The examination table thus functioned not merely as a physical barrier but as a violation of dignity, comfort, and privacy.
Figure 3.
Examination Tables in the Health Facilities.
Notably, participants demonstrated awareness of accessible alternatives despite being excluded from them due to financial constraints. Maru contrasted his local clinic with better-equipped facilities:
I know that clinic [local clinic] isn't meant for me. But what choice do I have? I struggle to get inside with one leg. I've heard private clinics, even Butajira Hospital [in a town], have better equipment and are easy to move around for us [have a ramp and accessible washroom]. But how would I get there? But how would I ever get there? No money for transport…It's frustrating, but what can I do?
His account revealed how the health care system linked quality, accessible care to expensive private facilities in distant urban areas, creating multiple barriers that privileged those with financial resources and transportation access. His resigned question, “What can I do?”, captured the powerlessness this participant experienced when confronting systems that never anticipate their needs, illustrating a form of structural oppression. However, his awareness of better alternatives confirmed that barriers lay not in individual impairments but in inhospitable environments—echoing the core principle of critical disability theory that disability is socially constructed through exclusionary practices and policies.
3.2. Socioeconomic Marginalization: Financial Hardship and Poverty
The study participants discussed financial challenges that impacted nearly every aspect of their health care access. Most participants experienced structural poverty, defined as resulting from systemic exclusion from economic opportunities rather than individual deficits. The intersection of disability and poverty created what can be understood as economic violence [37,38], wherein participants were forced to choose between health care and basic survival needs like food. This theme revealed how economic inequities operated through multiple mechanisms: discriminatory pricing policies that ignored differential earning capacity, employment systems that excluded persons with disabilities, and health care financing structures that perpetuated rather than addressed existing disadvantages. These interconnected barriers created compounding marginalization that trapped participants in cycles of dependency, demonstrating how ableist economic systems function to maintain inequality. Due to chronic poverty, participants often faced impossible choices between health care and other basic necessities, which led to delayed care and loss of independence. Many reported needing to choose between spending money on medical visits or on food, farming inputs, and other essentials for survival. For most participants, health care became a luxury they could hardly afford, resulting in postponed or skipped treatment. Liya, a 30-year-old woman, illustrated this dilemma:
To be honest, there are times when I have to make a hard choice—either buy medicine or buy food. … I sit there thinking, 'Should I get treated or should I eat today?' And most times, I just keep quiet and try to endure the pain. … Choosing between medicine and food—it hurts every time.
Similarly, Alex, a barber, shared his experience of prioritizing his children’s food over personal health care: "They [health care providers] prescribed glasses costing 1,700 birr. I didn’t buy them because I need to feed my children." He sacrificed his eyesight so his children could eat, putting his family’s food needs over his vision care. For both participants, health needs are consciously suppressed to meet immediate basic needs, a pattern that can lead to significantly worse health in the long term. The narratives highlight health care as a necessity, but the access to which requires significant personal sacrifice.
Due to financial constraints, people with physical disabilities were forced to rely on others, such as family, neighbours, or charitable organizations, for health care financing. However, a profound consequence of this financial reliance was the erosion of autonomy in health care decision-making, which subsequently undermined their sense of self. Kokit explained how her dependence compromised her sense of identity:
I have no choice but to depend on others for everything—food, clinic, even small things. It feels like I’ve lost all my strength and even a sense of who I am. … I don’t really have a say in my own treatment because someone else covers all my costs, so, obviously, I’m not in control of my own health.
Her narrative exposes the intersectional oppression faced by women with disabilities in poverty, where gender, disability, and economic disadvantage combine to create what McCall called ‘complex inequality’ [25]. The erosion of health care autonomy through financial dependence represents a form of systematic disempowerment that extends beyond medical decision-making to encompass fundamental questions of selfhood and agency. This relationship of dependency positions participants as recipients of charity rather than as holders of rights, illustrating how economic systems sustain hierarchical power relationships, even within families.
The participants described how their disability and poverty created a self-perpetuating vicious cycle, trapping them in debt and dependency. Many shared stories of falling into debt, selling assets, or losing their livelihood because of illness, which in turn further limited their ability to pay for health care—a kind of loop from which they could not break free. Shashie summarized the pattern succinctly:
We can’t find a job easily; nobody wants to hire someone who can’t walk. … Because of my disability, I can’t work anymore. I have no stable income, so I remain poor and there’s no money for medicine or transport to the clinic. … It feels like a never-ending circle of debt and pain. I can’t get out of it.
Shashie’s narrative captured how multiple oppressive systems—labour market discrimination, health care commodification, and social welfare inadequacy—functioned synergistically to ‘trap’ participants in positions of permanent economic marginalization. Despite being locked in debt and dependency, many emphasized that there are “no special discounts or support for people with physical disabilities” (Degu, Male), forcing them to pay the same price as everyone else. Kid, a salaried librarian with an upper-limb impairment, expressed:
We pay the same price as everyone else. There is no discount or help for disabled people, no priority. … We're treated the same, but it's harder for me to earn money. … The medicines cost a lot. If I can't afford them, there is no solution. Why not create a system to help those with bigger barriers?
Kid’s words expose the health care system—a system that is to help those in need and promote well-being—as committed to procedural equality and without any consideration of substantive equity. Even this salaried participant noted that her income was inadequate to cover medical expenses, revealing how seemingly neutral policies produce inequitable outcomes when applied to populations with systematically reduced earning capacity.
3.3. Socio-Cultural Stigma and Attitudinal Barriers
Apart from physical and financial challenges, the participants faced socio-cultural and attitudinal barriers at various levels—family, community, and health care institutions—creating an environment wherein people with physical disabilities feel devalued, shamed, and discouraged from seeking health services. This theme emphasizes how stigma, prejudice, and discriminatory attitudes toward individuals with physical disabilities—shaped by cultural norms, gender roles, and misconceptions—operate in community and health care settings, leading to their exclusion, decreased confidence, and reluctance to seek care.
3.3.1. Community Prejudice and Health Care Providers' Negative Attitude
The participants detailed how negative societal attitudes and misconceptions about disability manifested in an unwelcoming environment, discouraging them from going out in public or seeking care. They described prevalent community beliefs linking disability to curses, divine punishment, or evil spirits, leading to isolation and stigma. Alex said, “People say that we [people with physical disabilities] are possessed by devils … that my feet are like this because Satan lives in me. They whisper about me like I’m cursed by God and sinful.” The psychological impact of being labelled ‘cursed’ or ‘sinful’ can be as constraining as physical barriers, leading individuals to hide themselves and avoid seeking help. For instance, certain families choose to hide their children with disabilities to avoid gossip and shame. Kokit recalled that her grandmother never let her go to school for fear of community insults: “My grandmother kept me at home, she didn't want me to go to school because she thought people would make fun of me.” While motivated by protective intentions, the grandmother’s shame and fear of judgment caused the participant to remain out of school, leading to significant long-term detriment. It exemplifies how social pressure or anticipation of stigma results in self-isolation or family-imposed isolation, which in turn limits life opportunities and access to services like health care or education. The quote reflects a tendency in rural areas for families to conceal a child with a disability to maintain their social standing. Consequently, as an example, educational prospects are lost, perpetuating low literacy and disempowerment, which ultimately restrict access to health care.
The impact of stigma and isolation in regard to lack of educational opportunities is significant, with lasting implication to health and well-being. Yibe’s narrative captures his ongoing struggles in health care due to his limited education:
I didn’t learn to read because I couldn’t hold a pen and others would mock me… now I can’t read or write and can’t understand what the doctor advises me… I feel too shy and even ashamed to ask anything, so I just nod and pretend I understand, even when I don’t.
This illustrates how disability and lack of education (illiteracy) intersect to create shame and silence, causing Yibe to pretend he understands and to accept care he cannot fully comprehend, as he is too embarrassed to ask for clarification. Thus, he left the clinic without fully grasping his treatment—a scenario that can result in misuse of medication or failure to follow through on therapy. Here, it is not his impairment that limits him, but rather a system (i.e., people) that has failed to correct social wrongs and to provide him with an education, denying him the right to learn and to benefit from that knowledge throughout his life; further, having initially denied him formal education, the system offers no accommodation to present health information in a way he can understand.
Negative attitudes do not stop at the community—they extend into health care settings, manifesting in disrespectful treatment, impatience, and neglect by providers. Unfortunately, these experiences contribute to a poor patient-provider relationship and erode trust in the health care system, discouraging participants from seeking health care services. During the focus group discussion, Alex highlighted the humiliation he experienced: “When I asked for help, they [providers] would say, ‘Why don’t you ask your assistant to come and help you? Just stay there, you can manage it on your own’.” Nega added, emphasizing how these experiences silenced them: “… If I ask, he [the doctor] gets angry and walks me out … We [people with physical disabilies] don’t like speaking up. They [health care providers] just do what they want.” Kal summed up the humiliation and illustrated how stigma compounded his burden:
When I go there [clinic], they don’t even see me as a person, only my clothes and disability, saying, ‘Go buy the medicine somewhere else.’ I wish I had power or a relative. You know, I would have confronted him. But nothing ... Honestly, it feels like I carry two burdens on my shoulders—my illness and their pitying attitude.
Being summarily dismissed in this way not only left Kal’s medical issue unresolved but also inflicted an additional wound: the psychological ‘disease’ of stigma. His metaphor of ‘two burdens’—his illness plus the negative attitude of others feeling sorry for him—underscores how the words, gestures, and actions of health care workers can be experienced as painful emotions, made more difficult to contend with when one is trying to manage a health condition and all the physical and emotional elements that come with it. His desire for power, or any relative, highlights how social status and connections often determine who is acknowledged in the clinic, rendering one silent if lacking both wealth and physical capability.
Over time, the participants began to view themselves through society’s negative lens, absorbing those unfavourable views and perceiving themselves as having low status. This perception can discourage them from seeking care or advocating for themselves. Sis, a 30-year-old female, described how the feeling of inferiority affects her daily life:
They assume it is a punishment from God, and honestly, I sometimes felt same … so I don’t talk to people. I’m afraid, and also, you know, women should be reserved. ... yeah, I feel fine at home, but outside, ohh … everybody stares.
Here, fear of judgment and gender rules intersect to silence her and keep her largely confined to her home. She believes people see her disability as a ‘punishment’, implying she has done something wrong. Additionally, within the culture, women are to be quiet, kept back, further exacerbating the stigma. These overlapping power structures confine her to her home, limiting her social life and potentially causing her to delay or avoid going to the clinic. In essence, the real obstacle here is not her physical impairment but the intersecting influences of society’s cultural norms, judgment, and gender expectations, which diminish her confidence, voice, and freedom of movement.
3.3.2. Gendered Health Care Neglect and Domestic Burdens
Women with disabilities face unique challenges, as they must navigate not only ableism but also sexism and rigid gender roles. Our participants included seven women with physical disabilities, and their stories revealed a pattern of what can be termed double discrimination [39]. They are expected to fulfill traditional female roles (e.g., caregiving, homemaking, deference to male authority) while being underestimated because of their disabilities. Most of the women we interviewed were responsible for financially supporting their households, as many remained unmarried due to discrimination against women with disabilities in marriage. Their roles as the sole providers created a barrier to accessing care for themselves and their dependents. As the only providers, seeking care meant lost income, thus adversely affecting their households. “It is OK for a disabled man to marry a normal woman. But if a normal man marries me, people will talk, what is wrong with him? No one helps me” (Liya, Female, 30). Cultural norms and social attitudes regarding marriage partners result in her denial of the social and economic security of marriage. Without a partner with whom to share costs, each clinic visit means skipping the market and losing a day’s income.
Another prominent issue is the expectation that women, even when they have a disability or are ill, must fulfill traditional domestic duties. Most female participants were unmarried; however, those who were married or living with family had significant household responsibilities despite their disabilities. They described having no respite from chores, which not only exacerbates their health problems but also leaves them little time or energy to seek care. This situation has a direct impact on their health and obscures their needs—a woman with domestic responsibilities is less likely to be seen at clinics or community gatherings where health information is disseminated. “The priest says a wife’s duty is to care for the home. So, even in pain, I must fetch water and cook always. Who else takes care of my kitchen?” (Mazi, female). Apart from the domestic burdens, women with disabilities also face stigma surrounding their reproductive health and family life. Community members and health providers question their ability and right to motherhood, which subsequently impacts their health care decisions. Liya described an incident during a prenatal visit that left her deeply hurt:
He [provider] said, ‘Are you sure you want to continue [the pregnancy]? Do you want a baby, or do you want yourself first? You have a disability—how could you manage a child? What do you do for a living?’ Just a series of questions… I totally stopped going to the clinic altogether and delivered at home.
The health provider’s questioning was not neutral; instead, it frames Liya’s disability as incompatible with poverty, and motherhood, casting doubt on her ability to parent. Rather than supporting her, the health worker questioned her capability to be a mother because she is poor and has a disability. This caused Liya to feel judged, ashamed, and unwelcome, pushing her away from formal care and toward a riskier home birth. Thus, her choice to avoid care and deliver at home reflects not a real choice per se, but rather exclusion, driven by the attitudes that regard low-income women with disabilities as unfit mothers.
3.3.3. Systemic Weaknesses in Health Service Delivery: Gaps in Resources, Coordination, and Implementation
The participants moved beyond personal hardship to highlight structural failures, including under-resourced facilities and a fragmented referral process. They reported that local clinics often lacked medications, assistive devices, and staff trained in disability care. Alex said, “They [providers] just write a prescription and tell me to buy it outside [private pharmacy]. But, they [private pharmacy] ask thousands of birr, and I don’t have that kind of money”. For people with physical disabilities, who may experience health complications or secondary conditions such as infections resulting from mobility impairments, this lack of capacity means their needs go unmet. Thus, even after overcoming obstacles related to distance and stigma to reach the clinic, participants face empty pharmacy shelves and are referred to the private market, which further worsens their financial barriers. As a result, pain relief becomes a privilege, something only those with money can afford, while low-income people with disabilities are pushed further into poor health and hardship. When a clinic lacks basic medications, every patient suffers; however, for a person with a disability and who has already overcome significant hurdles to reach the clinic, they suffer even more and may lack the means to seek alternatives.
Another critical issue was the referral process. The participants mentioned that the referral system is unsupportive and discouraging. Degu described his feelings regarding the referral process:
What’s the point of giving me that paper? Do they [providers] think I can travel there with this stick? Or that I have money to pay for it? They just gave me a paper to go to Butajira Hospital. It’s funny. I tore up the paper right there and went back home. Thank God nothing bad happened. I found relief through holy water.
For Degu, the referral to a distant hospital (far and costly to reach) felt like being rejected from care. No consideration was given to how he would manage the trip—the distance, cost, and his mobility impairment were all barriers that the referring clinic ignored. Here, simply by issuing a piece of paper, the health facility clears itself and offloads responsibility onto an individual. Without transportation, follow-up, or guidance, the official referral was meaningless. It was so unrealistic for Degu, he destroyed the referral paper in anger and turned to a spiritual solution.
Finally, despite hearing local district officials talk about supporting people with physical disabilities at various community gatherings, participants reported that they did not see this in practice. Kal said, “The report looks good for show, but even in new hospitals, I still need people to lift me in [to the clinic]. They just mention disability in reports. No real change.” While regulations may require that new buildings are accessible, Kal noted that recent constructions still fail to meet their needs. This suggests that disability inclusion might be mentioned in official reports or proposals (perhaps to satisfy donors or central mandates), but actual building designs remain non-compliant. The tangible outcome—a person still needing to be carried—completely contrasts with any polished documents or promises about accessibility.
4. Discussion
The findings of this study reveal that people with physical disabilities in rural Ethiopia face complex, intersecting barriers—physical, socioeconomic, attitudinal, and systemic—that hinder their access to PHC. This finding is consistent with other research, wherein disability-related health care access challenges are widespread and multifaceted [40,41,42,43,44]. Additionally, Tesfaye et al. [16] found, in their cross-sectional survey involving 406 adults with disabilities in Hawassa City, Ethiopia, that 68% of facilities lacked ramps, transportation costs exceeded one day’s wages for 54% of the participants, 41% encountered disrespectful providers, and unclear referral pathways doubled the likelihood of forgoing care.
Physical inaccessibility of the environment and health care infrastructure emerged as a major barrier in our study. The participants described impassable terrain, long distances to get to the clinics without transportation, and difficult-to-enter clinic buildings. These findings align with studies done in other African contexts: for example, researchers conducting studies in Ghana [45] and Uganda [46] have reported that people with disabilities often encounter hardships travelling to health facilities due to mobility challenges, lack of transport, and unfriendly physical infrastructure. Participants in the Ugandan study recounted having to travel 18 kilometres or more to reach the nearest clinic, leading many to delay or avoid care altogether [46]. Our participants shared similar experiences, including being carried on someone’s back or a local stretcher to access distant clinics. These extreme efforts reflect what is called in CDT a ‘disabling social condition’—it is the inaccessible route and built environment, rather than the impairment itself, that fundamentally disables the person [21,47]. In our research context, the absence of wheelchair-accessible infrastructure and the presence of stairs without ramps make access the responsibility of individuals with disabilities, rather than the health systems, which are intended to serve all people. This situation exemplifies institutional ableism, where health care facilities are designed under the presumption of able-bodied users, thereby marginalizing those with different mobility needs [48,49]. As Titchkosky [50] argues, the absence of ramps or other accommodations represents more than mere poor design—it signifies a form of social exclusion through neglect. Furthermore, Rotoli et al [48] note that such structural barriers violate the rights of persons with disabilities and deepen their marginalization by making basic services, such as health care, difficult to access.
The second theme of our study centers on socioeconomic marginalization. Our findings indicate that poverty and disability intersect, leaving participants in precarious circumstances wherein prioritizing health care is sacrificed. This compounded marginalization exemplifies the well-documented vicious cycle between disability and poverty: disability may lead to reduced employment opportunities and increased expenses, while poverty, in turn, constrains access to essential services, often exacerbating health conditions and intensifying disability [51,52,53]. In Ethiopia, an estimated 60% of working-age persons with disabilities (3.6 million people) are unemployed [54], reflecting the extensive economic exclusion experienced by this population. Consequently, poverty compels many to delay or omit necessary care and to depend on others, thereby undermining their autonomy.
These experiences align with substantial evidence suggesting that financial hardship presents a significant barrier to health care access for individuals with disabilities [55,56,57,58,59]. The World Report on Disability also highlights that the affordability of health care services and transportation is a key reason why individuals with disabilities are unable to access necessary care in low-income countries [60]. Globally, approximately 51–53% of people with disabilities cannot afford health care, compared to about 32–33% of those without disabilities [61]. They are also approximately 50% more likely to incur catastrophic health expenditures than individuals without disabilities [60]. This financial disparity is attributed to the extra costs associated with disability, such as assistive devices, medications, and travel [46,55,56], coupled with limited earning opportunities due to discrimination and inaccessible workplaces [46,55,58].
Despite the clear need, the existing Ethiopian health care system does not provide disability-targeted subsidies [15,62]. Instead, it implements a uniform flat fee policy for all individuals—a practice that unjustly assumes all patients have an equal ability to pay. The policy penalizes those with disability when they must pay the same charges as others, despite incurring higher costs for transportation, assistive devices, frequent visits, and earning less income on average. It promotes the image of all patients as fully independent and equal, while ignoring the structural disadvantages that many people with physical disabilities face. The Ethiopian community-based health insurance scheme was established to ensure equitable health care access; however, it leaves individuals with disabilities vulnerable, excluding them from essential disability-related items such as assistive devices and rehabilitation services and forcing them to pay out of pocket [62]. As a result, as our participants described, flat fees that appear fair on paper ultimately create unequal outcomes: medications and services become unaffordable, health declines, and people with physical disabilities are pushed further to the margins, with many skipping essential care and choosing traditional or spiritual treatments because they cannot afford modern medical care.
In addition to physical and financial barriers, our findings highlight deeply rooted social stigma and negative attitudes as major obstacles. The participants reported community beliefs about disability as a curse or divine punishment. These beliefs promote harmful stereotypes, social exclusion, and internalized shame among individuals with disabilities. In health care settings, disrespectful providers and gender-based discrimination further discourage many from seeking care or returning for follow-up visits. As such, participants described feeling embarrassed or unworthy of care because of their community's and health care professionals' attitudes, which erode their confidence in accessing services. This finding is consistent with extensive literature across Africa showing that attitudinal barriers, including stigma, discrimination, and misunderstanding, often prevent people with physical disabilities from obtaining health care [16,42,43,44,46,63]. Prejudicial attitudes appear in the community and health care settings, with the participants describing health care providers as dismissive, disrespectful, or abusive toward them. Researchers have documented similar phenomena, with people with physical disabilities reporting health care providers as insensitive [42,46], rude or disrespectful [16,44], unaware of their needs [42,43], and being surprised that women with disabilities were sexually active [45,46].
As Pothier and Devlin argue [21], disability is fundamentally about power—who is regarded as worthy, who receives attention, and who has agency. In our study, the power imbalance between individuals with disabilities and the community or medical personnel was evident. These power dynamics manifested in participants’ feelings of being a ‘burden’ and their diminished confidence in seeking care following negative encounters. Moreover, the participants internalized society’s low expectations, a form of self-stigmatization, which further discourages them from asserting their needs or returning for follow-up care. Thus, the prejudicial attitudes encountered by people with physical disabilities in health care are not merely individual instances of rudeness; they arise partly from inadequate disability training and partly from societal power relations that, often unconsciously, involve perceptions of those with disability as somehow less than, which then filters into medical practice [48]. In other words, personal attitudes and institutional culture are interconnected—if disability is frequently perceived through a lens of pity or inferiority, health care interactions will inevitably mirror these biases unless actively countered. Thus, our findings emphasize that addressing stigma and prejudice is as essential as implementing physical accommodations, such as ramps, or providing financial assistance—without a respectful and inclusive health care environment, other improvements may be undermined by an unwelcoming, disrespectful atmosphere.
Consistent with Intersectionality Theory [26], our study demonstrates that physical, financial, and attitudinal barriers do not occur in isolation; instead, they are intensified by other social factors, such as gender, education, and rurality. The findings of our study align with literature indicating that the interaction between poverty, low educational attainment, and rurality limits opportunities for individuals with disabilities, especially women, to fully engage in economic and social aspects of society [42,43,44]. Lower educational achievement among rural people with physical disabilities often results in less health literacy and fewer economic opportunities, which further worsen both socioeconomic barriers and stigma and negative attitudes toward disability that discourage or hinder access to care [46,58]. Meanwhile, the health care system itself tends to concentrate higher-quality services in urban centers and private clinics, effectively privileging those who can afford to travel and treatment. Gender is a key intersecting axis. Women with disabilities face more disadvantages in employment and social support than men and worse health care barriers. In the World Health Survey, conducted across 51 countries, the authors found employment rates of 52.8% for men with disabilities, compared to 19.6% for women [60]. Research also shows that women with disabilities often report worse treatment in health care settings, including higher rates of neglect or abuse by providers, compared to their male counterparts [16,46]. Our findings support this: female participants were discouraged from having a child and from travelling alone to distant clinics, as based on community norms. A similar situation was reported in rural Ghana, where women with disabilities were often ‘shut in’ due to social norms that discourage women from travelling alone [45].
4.1. Recommendations
Notably, Ethiopia has made formal commitments to disability inclusion by ratifying the UNCRPD and developing a National Plan of Action (2012–2021) [64] to mainstream disability measures across all sectors. Furthermore, the Ethiopian Building Proclamation mandates accessibility for public buildings [12]. However, our study indicates that these accessibility-related laws and policies are not being enforced at the local level. This gap between policy and practice means that those who are most disadvantaged, rural people with disabilities who are also poor, see minimal benefit from the legal protections intended to support them. Thus, first and foremost, we recommend actualizing and implementing the Building Proclamation by incorporating ramps, wide doorways, accessible toilets, and other necessary accommodations across all health facilities. Ethiopian health authorities should collaborate with architects and building regulators to either redesign existing facilities or construct new, disability-friendly infrastructures. Second, to address the root causes of financial hardship, we recommend the government work with non-governmental organizations to establish vocational training and employment placement programs for persons with disabilities in rural areas. Additionally, we recommend targeted financial support to prevent persons with disabilities from being denied care due to cost. This might involve subsidizing or providing free enrollment in the CBHI scheme for people with physical disabilities in Ethiopia and expanding coverage to include disability-related needs, such as assistive devices and rehabilitation therapies. By adjusting fees and coverage based on ability to pay and level of need, the health system can prevent catastrophic expenses and ensure that poverty is not worsened by disability (and vice versa). International examples and the World Health Organization recommendations support such measures [65,66,67], and Ethiopia’s policies should be updated accordingly. To mitigate distance barriers, local administrations should develop transport support schemes, for example, bysubsidizing or providing free access to ambulance services and wheelchair-accessible vehicles in each district to transport persons with disabilities on scheduled clinic days. Finally, addressing stigma requires transforming institutional cultures and societal narratives about disability. We recommend educating health care professionals on disability rights and involving people with physical disabilities in health care decision-making to challenge stereotypes. Engaging persons with disabilities in health care training, as trainers or acting as patients, supports the slogan “Nothing about us without us” and helps improve attitudes [68,69]. Furthermore, health care facilities should appoint dedicated personnel or disability liaisons to support patients with disabilities, ensuring their needs are met promptly. Beyond the health facilities, public education campaigns in rural areas are needed to dispel myths about disability and foster more inclusive social norms [68]. Eradicating stigma requires a comprehensive societal shift, but small changes, such as incorporating disability rights education into community health education programs, inviting disability advocates to local events, or showcasing positive portrayals of people with physical disabilities in media, can begin the dismantling of long-standing prejudices.
4.2. Strengths and Limitations of the Study
Beyond our findings, the theoretical foundations in CDT and intersectionality (which guided both the research questions and interpretation) and the focus on power and structural inequities are key strengths of our study. Another strength is our data collection method, as we used multiple sources (i.e., interviews, focus groups, and observations), which enhanced insights, reflected diverse perspectives, and improved the credibility and transferability of the findings. Our inferences about infrastructure accessibility are based on participant accounts and direct observations.
However, there is a challenge related to the potential loss of meaning when translating from Amharic to English. Although transcripts were originally analyzed in Amharic, the subsequent translated excerpts might have reduced accuracy and nuanced expression. Additionally, the outsider positionality of the first author (without a disability) could have influenced data collection and interpretation, despite reflexive mitigation. Much effort was made to amplify participants’ voices and avoid imposing personal perspectives on their experiences.
4.3. Future Research
Building on our theoretical frameworks, participatory or community-engaged studies that involve people with disabilities as co-researchers can deepen the analysis of power dynamics and the processes of structural change. Longitudinal and mixed-methods research could track how intersecting disadvantages develop over time and evaluate the long-term effects of policy and service reforms. Also, implementation-focused research is vital for designing and assessing practical solutions, such as transportation support schemes, disability competence training for providers, and disability-responsive community health insurance improvements.
5. Conclusions
In conclusion, the barriers to PHC access for individuals with physical disabilities in rural Ethiopia are rooted in a complex interplay of physical, economic, social, and systemic factors that collectively undermine their right to health care. These barriers are manifestations of structural inequalities, resulting from policy choices and social attitudes. As CDT reminds us, meaningful improvement requires changing the systems that create these barriers. This involves improving health care policies, shifting social attitudes, addressing physical and financial obstacles, and empowering people with disabilities. By addressing these factors together, we can build a health care system that actually ensures inclusivity for all.
Author Contributions
Conceptualization, A.A.; methodology and analysis, A.A.; Writing—original draft preparation, A.A.; writing—review and editing, A.A., L.D., R.W., and P.C.P.; funding acquisition, A.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Mastercard Foundation Scholars Program.
Institutional Review Board Statement
The Research Ethics Board of Queen's University Health Sciences and Affiliated Teaching Hospitals (TRAQ file #: 6041959) and University of Gondar (Protocol #: CMHSSH-UOG IRERC/50/11/24) have approved the research.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author at 20ata4@queensu.ca.
Acknowledgments
The authors would like to acknowledge the volunteers and research assistants who participated in the study. They would also like to acknowledge the Mastercard Foundation Scholars Program for its financial support of this research.
Conflicts of Interest
The authors declare no conflicts of interest. The funder had no role in designing the study, collecting, analyzing, or interpreting data, writing the manuscript, or deciding to publish the results.
Disability Language/Terminology Positionality Statement
Person-first language is used throughout this article.
References
- World Health Organization. Global report on health equity for persons with disabilities. Geneva, Swizerland: World Health Organization; 2022. Contract No.: Licence: CC BY-NC-SA 3.0 IGO.
- United Nations Ethiopia. International Day of Persons with Disabilities marked with a call to accelerate efforts to ensure disability inclusion: UN Ethiopia; 2024 [Available from: https://ethiopia.un.org/en/286846-international-day-persons-disabilities-marked-call-accelerate-efforts-ensure-disability.
- United Nations Population Fund (UNFPA). Ethiopia: Population data portal: United Nations Population Fund; 2025 [Available from: https://www.unfpa.org/data/world-population/ET.
- Krahn GL, Walker DK, Correa-De-Araujo R. Persons With Disabilities as an Unrecognized Health Disparity Population. American Journal of Public Health. 2015;105(S2):S198-S206.
- Vergunst R, Swartz L, Mji G, MacLachlan M, Mannan H. ‘You must carry your wheelchair’ – barriers to accessing healthcare in a South African rural area. Global Health Action. 2015;8(1):29003.
- Mahmoudi E, Meade MA. Disparities in access to health care among adults with physical disabilities: analysis of a representative national sample for a ten-year period. Disabil Health J. 2015;8(2):182-90.
- Krahn GL, Walker DK, Correa-De-Araujo R. Persons with disabilities as an unrecognized health disparity population. Am J Public Health. 2015;105 Suppl 2(Suppl 2):S198-206.
- Gréaux M, Moro MF, Kamenov K, Russell AM, Barrett D, Cieza A. Health equity for persons with disabilities: a global scoping review on barriers and interventions in healthcare services. Int J Equity Health. 2023;22(1):236.
- United Nations. Convention on the Rights of Persons with Disabilities and Optional Protocol. In: (Ed.) UN, editor. New York: : United Nations; 2006. p. 18.
- United Nations. Transforming our world: the 2030 Agenda for Sustainable Development New York2015 [.
- Ratification of the Convention on the Rights of Persons with Disabilities Proclamation No. 676/2010, (2010).
- Federal Democratic Republic of Ethiopia. Ethiopian Building Proclamation No. 624/2009. . 2009.
- Ethiopian Health Insurance Agency. Community-Based Health Insurance Evaluation Report. Addis Ababa, Ethiopia: Ethiopian Health Insurance Agency; 2022.
- United Nations Department of Economic and Social Affairs. UN Disability and Development Report - Realizing the SDG by, for and with persons with disabilities. New York: UN; 2019.
- Damtew B, Yigezu M. Perspectives of care providers on obstacles to healthcare access for people with disabilities in Ethiopia: a qualitative investigation. BMC Health Serv Res. 2024;24(1):1290.
- Tesfaye T, Woldesemayat EM, Chea N, Wachamo D. Accessing Healthcare Services for People with Physical Disabilities in Hawassa City Administration, Ethiopia: A Cross-Sectional Study. Risk Manag Healthc Policy. 2021;14:3993-4002.
- Fekadu H, Mekonnen W, Adugna A, Kloos H, Hailemariam D. Barriers to equitable healthcare services for under-five children in Ethiopia: a qualitative exploratory study. BMC Health Services Research. 2024;24(1):613.
- Gebrekirstos LG, Lencha TT, Asgedom YS, Wube TB. Prevalence and factors associated with violence; perceived social support and health access among people with disabilities in rural districts of southern Ethiopia: mixed study. Journal of Multidisciplinary Healthcare. 2023:2921-36.
- Dagnachew N, Meshesha SG, Mekonen ZT. A qualitative exploration of barriers in accessing community pharmacy services for persons with disability in Addis Ababa, Ethiopia: a cross sectional phenomenological study. BMC health services research. 2021;21(1):467.
- Kemal S. Assessment of Barriers of Accessing Primary Health Care Services For Persons with Hearing, Visual and Physical Impairments in Gulele Sub City of Addis Ababa, AAU. Accessed on. 2017;12.
- Pothier D, Devlin R. Critical Disability Theory: Essays in Philosophy, Politics, Policy, and Law. Vancouver: UBC Press; 2006.
- Hosking DL. Critical disability theory. 4th Biennial Disability Studies Conference; 2008; Lancaster University, UK: (Leave blank unless formally published); 2008.
- Crenshaw K. Demarginalizing the intersection of race and sex: A Black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. University of Chicago Legal Forum. 1989;1989(1):139–67.
- Hill Collins P. Intersectionality as critical social theory. Durham: Duke University Press; 2019.
- McCall L. Complex Inequality: Gender, Class and Race in the New Economy: Taylor & Francis; 2002.
- Collins PH, Bilge S. Intersectionality: John Wiley & Sons; 2020.
- Stake RE. Qualitative case studies. 2005.
- Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey. Addis Ababa, Ethiopia, and Rockville, Maryland, USA; 2017.
- Colorafi KJ, Evans B. Qualitative Descriptive Methods in Health Science Research. Herd. 2016;9(4):16-25.
- Neergaard MA, Olesen F, Andersen RS, Sondergaard J. Qualitative description – the poor cousin of health research? BMC Medical Research Methodology. 2009;9(1):52.
- Gill P, Stewart K, Treasure E, Chadwick B. Methods of data collection in qualitative research: interviews and focus groups. British Dental Journal. 2008;204(6):291-5.
- Kitzinger J. Qualitative Research: Introducing focus groups. BMJ. 1995;311(7000):299.
- Braun V, Clarke V, Hayfield N, Davey L, Jenkinson E. Doing reflexive thematic analysis. Supporting research in counselling and psychotherapy: Qualitative, quantitative, and mixed methods research: Springer; 2023. p. 19-38.
- Tracy SJ. Qualitative quality: Eight “big-tent” criteria for excellent qualitative research. Qualitative inquiry. 2010;16(10):837-51.
- Jacobson D, Mustafa N. Social identity map: A reflexivity tool for practicing explicit positionality in critical qualitative research. International journal of qualitative methods. 2019;18:1609406919870075.
- Lundberg DJ, Chen JA. Structural ableism in public health and healthcare: a definition and conceptual framework. The Lancet Regional Health - Americas. 2024;30:100650.
- Eide AH, Muderedzi JT, Braathen SH, Stray-Pedersen B. Exploring structural violence in the context of disability and poverty in Zimbabwe. African Journal of Disability. 2017;6(1):1-9.
- Pinilla-Roncancio M, Cedeño-Ocampo G. Multidimensional poverty among persons with disabilities in Colombia: Inequalities in the distribution of deprivations at the municipality level. PLoS One. 2023;18(6):e0286983.
- Groce N, Kett M. Youth with disabilities. Youth with Disabilities (2014) Working Paper. 2014;23.
- Alshami A, Nashwan A. Healthcare Access for People with Disabilities in LMICs. Healthcare Access for People with Disabilities in LMICs. Singapore: Springer Nature Singapore; 2025. p. 13-21.
- Hashemi G, Wickenden M, Bright T, Kuper H. Barriers to accessing primary healthcare services for people with disabilities in low and middle-income countries, a Meta-synthesis of qualitative studies. Disabil Rehabil. 2022;44(8):1207-20.
- Dassah E, Aldersey HM, McColl MA, Davison C. Health care providers’ and persons with disabilities’ recommendations for improving access to primary health care services in rural northern Ghana: A qualitative study. PLOS ONE. 2022;17(9):e0274163.
- Halvorsen T, Munthali A, Braathen SH, Rød JK, Eide AH. Using locational data in a novel mixed-methods sequence design: Identifying critical health care barriers for people with disabilities in Malawi. Social Science & Medicine. 2021;283:114127.
- Pucchio AMR, Stranges S, Ali S. Disability and unmet need for health care in Canada: Findings from the Canadian Community Health Survey. Disability and Health Journal. 2025:101846.
- Ganle JK, Otupiri E, Obeng B, Edusie AK, Ankomah A, Adanu R. Challenges Women with Disability Face in Accessing and Using Maternal Healthcare Services in Ghana: A Qualitative Study. PLOS ONE. 2016;11(6):e0158361.
- Ssemata AS, Smythe T, Sande S, Menya A, Hameed S, Waiswa P, et al. Exploring the barriers to healthcare access among persons with disabilities: a qualitative study in rural Luuka district, Uganda. BMJ Open. 2024;14(11):e086194.
- Oliver M. The Politics of Disablement: Red Globe Press London; 1990.
- Rotoli J, Poffenberger C, Backster A, Sapp R, Modi P, Stehman CR, et al. From inequity to access: Evidence-based institutional practices to enhance care for individuals with disabilities. AEM Educ Train. 2023;7(Suppl 1):S5-s14.
- Hall MC. Critical Disability Theory. The Stanford Encyclopedia of Philosophy [Internet]. 2019.
- Titchkosky T. The Question of Access: Disability, Space, Meaning: University of Toronto Press; 2011.
- Mitra S, Posarac A, Vick B. Disability and Poverty in Developing Countries: A Multidimensional Study. World Development. 2013;41:1-18.
- Trani J-F, Loeb M. Poverty and disability: A vicious circle? Evidence from Afghanistan and Zambia. Journal of International Development. 2012;24(S1):S19-S52.
- Banks LM, Kuper H, Polack S. Poverty and disability in low- and middle-income countries: A systematic review. PLOS ONE. 2017;12(12):e0189996.
- International Labour Organization. Ethiopia Country Profile: Employment of People with Disabilities – The Impact of Legislation2004. Geneva: International Labour Organization; 2004.
- Soltani S, Takian A, Akbari Sari A, Majdzadeh R, Kamali M. Financial Barriers to Access to Health Services for Adult People with Disability in Iran: The Challenges for Universal Health Coverage. Iran J Public Health. 2019;48(3):508-15.
- Rahman M, Rana MS, Rahman MM, Khan MN. Healthcare services access challenges and determinants among persons with disabilities in Bangladesh. Scientific Reports. 2024;14(1):19187.
- Park S, Stimpson JP. Health Care Expenses and Financial Hardship Among Medicare Beneficiaries With Functional Disability. JAMA Netw Open. 2024;7(6):e2417300.
- Nguyen L, Lee JT, Hulse ESG, Hoang MV, Kim GB, Le DB. Health Service Utilization and Out-of-Pocket Expenditure Associated with the Continuum of Disability in Vietnam. International Journal of Environmental Research and Public Health. 2021;18(11):5657.
- Ssemata AS, Smythe T, Sande S, Menya A, Hameed S, Waiswa P, et al. Engaging community groups to enhance healthcare access for persons with disabilities in rural Uganda: A qualitative exploration. PLOS Glob Public Health. 2025;5(3):e0003140.
- World Health Organization & World Bank. World Report on Disability. 2011.
- Jin S, Sun Y, Tao J, Tian L, Lin J, Qian D. Medical expenditure and its inequity for people with disabilities: Evidence from the CHARLS 2018 data. Front Public Health. 2022;10:977150.
- Federal Ministry of Health. Health Care Financing Strategy 2022-2031. 2022.
- Alshami A, Nashwan A. Healthcare Access for People with Disabilities in LMICs. 2025. p. 13-21.
- Ministry of Labour and Social Affairs. National Plan of Action of Persons with Disabilities (2012-2021). . Addis Ababa: Government of Ethiopia; 2012.
- Koch R, Nkurunziza T, Rudolfson N, Nkurunziza J, Bakorimana L, Irasubiza H, et al. Does community-based health insurance protect women from financial catastrophe after cesarean section? A prospective study from a rural hospital in Rwanda. BMC Health Services Research. 2022;22(1):717.
- Atakorah YB, Arthur E, Osei-Fosu AK, Novignon J. The impact of Ghana’s national health insurance exemption policies on healthcare-seeking behaviour. SSM - Health Systems. 2024;3:100035.
- Tangcharoensathien V, Tisayaticom K, Suphanchaimat R, Vongmongkol V, Viriyathorn S, Limwattananon S. Financial risk protection of Thailand’s universal health coverage: results from series of national household surveys between 1996 and 2015. International Journal for Equity in Health. 2020;19(1):163.
- Iezzoni LI, Long-Bellil LM. Training physicians about caring for persons with disabilities: "Nothing about us without us!". Disabil Health J. 2012;5(3):136-9.
- Sapp RW, Sebok-Syer SS, Gisondi MA, Rotoli JM, Backster A, McClure Poffenberger C. The Prevalence of Disability Health Training and Residents With Disabilities in Emergency Medicine Residency Programs. AEM Educ Train. 2021;5(2):e10511.
Figure 1.
Stairs at the Entrance of the Health Facilities.
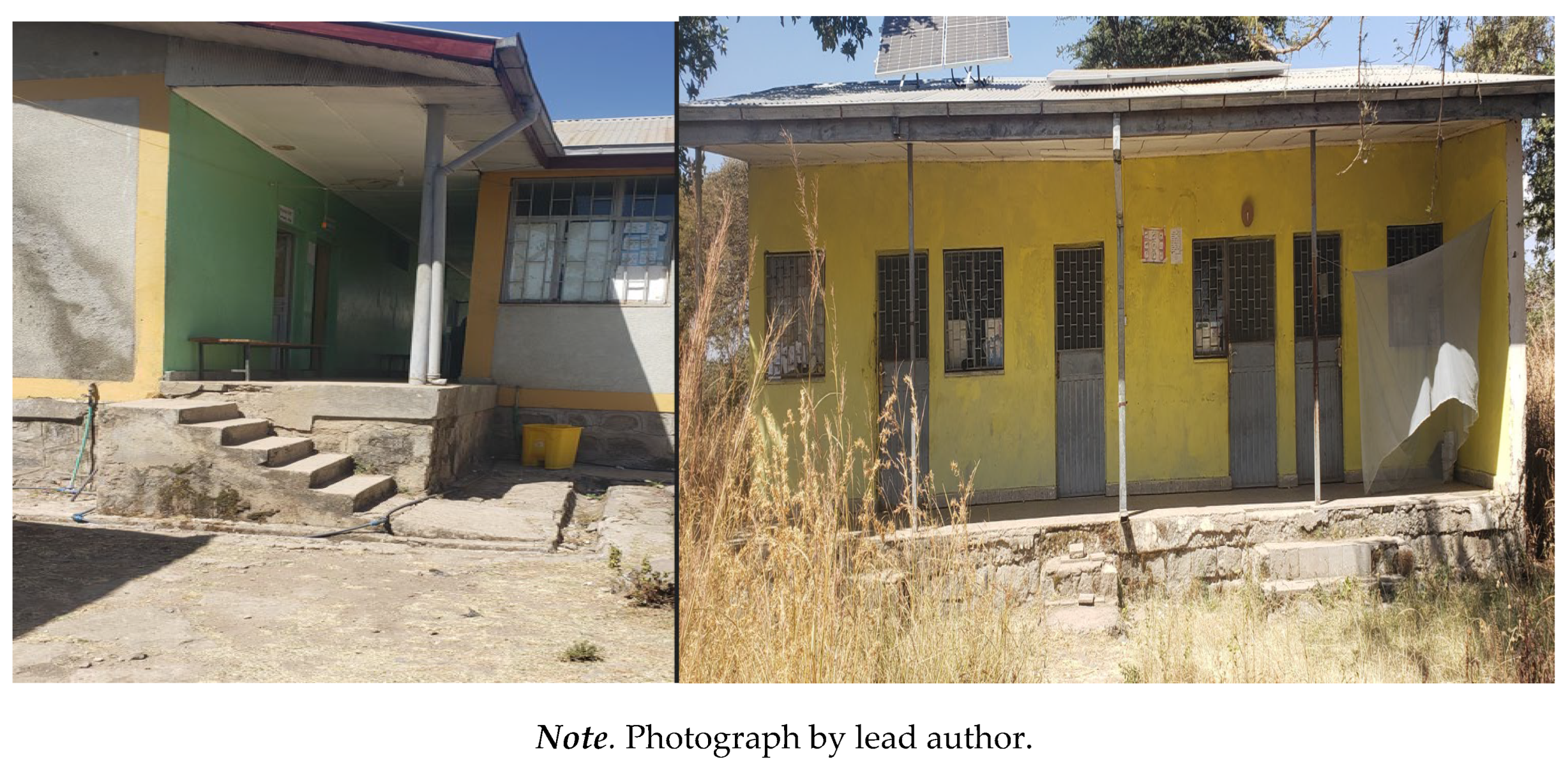

Table 1.
Participant Demographic Characteristics.
| Participants* | Gender | Age | Marital Status | Educational Status | Job (Means of Income) | Disability Type and Cause | Assistive Devices | |
|---|---|---|---|---|---|---|---|---|
| Shashie | F | 29 | Single | HSC | Hand Sewing | Congenital; Weak leg, Vision and hearing impairment | Walking Stick | |
| Kokit | F | 20 | Single | Grade 3 | Student | Congenital; Paralyzed legs | Wheelchair | |
| Kid | F | 31 | Single | College | Library assistant | Congenital; Weak and shortened hands | None | |
| Liya | F | 30 | Single | College | Selling local alcohol | Congenital; Weak and shortened hands | None | |
| Alex | M | 52 | Married | HSC | Barber | Acquired; Leg paralysis; childhood disease | Walking Stick | |
| Kal | M | 28 | Single | NFE | Shoeshine boy | Acquired; Unequal legs due to a fall in childhood age | Crutch | |
| Yibe | M | 66 | Married | NFE | Farmer | Congenital; Hand deformity | None | |
| Degu | M | 48 | Married | ESC | Farmer | Acquired; Disease (tuberculosis) Leg disability |
Walking Stick | |
| Maru | M | 37 | Widowed | NFE | Farmer | Acquired; Disease (leg amputation) | Crutch | |
| Mazi | F | 35 | Married | NFE | Selling goods | Congenital; leg deformity | Walking Stick | |
| Tasew | M | 42 | Married | ESC | Farmer | Acquired; Disease (unknown), leg deformity and weakness | Walking Stick | |
| Sis | F | 30 | Single | ESC | Hand Sewing | Congenital; Paralyzed legs | Wheelchair | |
| Baye | M | 29 | Married | HSC | Barber | Acquired; Leg shortening; unknown childhood disease | Crutch | |
| Nega | M | 45 | Married | ESC | Merchant | Acquired; Injury (amputation) | Crutch |
*Pseudonyms are used: M=Male; F=Female; HSC=High School Completed; ESC=Elementary School Completed; NFE=No Formal Education.
Table 2.
Trustworthiness.
| Criteria | Strategies |
|---|---|
| Worthy Topic | Given the increasing prevalence of disabilities in Ethiopia and the limited research on their experiences with health care access, this study is timely and relevant. |
| Rich Rigour | Sufficient data were collected (14 individual interviews and a focus group with 7 participants); Synergy between design (case study) and methods (interview and focus group), CDT and intersectionality, and an iterative, six-phase reflexive thematic analysis was performed. |
| Sincerity | The first author engaged in self-reflective practices through journaling and by creating a ‘social identity map,’ a visual tool developed by Jacobson and Mustafa [35] to better understand his social position and the influence of power and privilege in relation to the participants and the study context. |
| Credibility | Participant stories were detailed verbatim, and a combination of individual interviews and one focus group were used to garner data to identify common findings. Two compatible theoretical lenses, intersectionality and CDT were applied. Moreover, during the focus group, the participants reviewed preliminary themes developed from the individual interviews and confirmed that interpretations resonated with their lived experiences. |
| Resonance | The study's findings can be applied to similar settings, such as sub-Saharan Africa. To enhance transferability, a detailed ‘thick description’ of the research context, participants, procedures and findings has been included, allowing readers to assess the potential applicability of insights to comparable environments. |
| Significant Contribution | In practice, the findings inform actionable policy recommendations, such as integrating disability indicators into Ethiopia’s community-based health insurance scheme. Also, the findings highlight an under-researched area within the Ethiopian context (practical significance) and provide a way to promote political and critical awareness (moral significance). |
| Ethics | Procedural ethics were followed (ethics approval obtained), and data were protected on a secure university server accessible only to the authors. |
| Meaningful Coherence | There is coherence between the research question, design, data collection, data analysis, and findings. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



