
Submitted:
27 November 2025
Posted:
01 December 2025
You are already at the latest version
Abstract
Wound complications such as delayed healing and infection remain a challenge in on-coplastic breast surgery, often prolonging recovery and affecting patient comfort. This study explored the use of innovative breast-shaped polyurethane and polyester dressings impregnated with an oxygen-enriched oleic matrix designed to release reactive oxygen species that support natural tissue repair. Sixty patients undergoing unilateral qua-drantectomy with contralateral breast remodeling were included. The advanced dressing was applied to the oncologic breast, while standard premedicated patches were used on the opposite side, allowing each patient to serve as their own control. Over the first po-stoperative month, outcomes such as wound dehiscence, infection, delayed healing, and user experience were assessed. The new dressing provided excellent skin hydration, comfort, and ease of use, with complication rates comparable to traditional treatments. No infections, hematomas, or reoperations were observed. Healthcare personnel reported that the device was simple to handle and replace, while patients appreciated the comfort and absence of adhesive irritation. These preliminary findings suggest that oxygen-enriched oleic matrix breast-shaped dressings offer a safe, practical, and pa-tient-friendly alternative for postoperative care in oncoplastic breast surgery. Larger prospective studies are warranted to confirm their potential in improving healing quality and patient experience.
Keywords:
oncoplastic breast surgery
; oxygen-enriched oleic matrix
; advanced wound dressing
; reactive oxygen species
; wound healing
; patient comfort
1. Introduction
Oncoplastic breast surgery allows for excellent reconstructive and aesthetic outcomes following a lumpectomy. In a single surgical session, it enables the remodeling of the excised breast, symmetrization of the contralateral breast, correction of ptosis, and, in cases of mammary hypertrophy, a reduction in breast volume, thereby providing both functional and cosmetic benefits. This approach allows surgeons to maintain wide oncological excision margins, which translates into low rates of margin involvement [1]; moreover, contralateral breast reduction can reduce the risk of subsequent breast cancer [2].
The Wise pattern incision technique allows for proper repositioning of the nipple-areola complex [3], but postoperative wounds at the junction of vertical and horizontal sutures are particularly vulnerable due to reduced blood supply. Additionally, the nipple-areola complex, dependent on the chosen areolar pedicle, can be compromised. Various factors, including patient comorbidities, smoking, breast size, patient compliance during the postoperative period, and management during hospitalization and outpatient dressings, contribute to postoperative complications.
Postoperative wound complications in oncoplastic breast surgery, such as wound dehiscence, infection, and delayed healing, can significantly impact patient recovery. These complications often necessitate additional interventions [4], delay adjuvant therapies, reduce patient satisfaction, and increase healthcare costs. Dehiscence, with an estimated incidence of about 4%, together with other minor complications such as margin expansion (8%) [5], usually lead to unsatisfactory scar outcomes, assessable at 6–12 months, and overall lower patient satisfaction.
Endogenous reactive oxygen species (ROS) are reported to be involved in wound-healing processes, acting as secondary messengers to many immunocytes and non-lymphoid cells involved in repair, promoting lymphoid cell recruitment to the wound site and stimulating angiogenesis [6].
Furthermore, vegetable oils are reported to play an important role in supporting wound-healing processes, helping restore the lipid barrier and providing mild anti-inflammatory and antioxidative effects [7].
This study evaluates a new technology that uses polyurethane and polyester breast-shaped cups impregnated with an oxygen-enriched oleic matrix. Conducted at Ospedale di Cattinara in Trieste, this single-center post-market clinical follow-up study aims to assess the effectiveness of these devices in preventing minor complications following oncoplastic breast surgery.
2. Materials and Methods
The study design was observational, retrospective, and single-center, including 60 patients who underwent unilateral lumpectomy with contralateral breast remodeling between June 2024 and June 2025. The incision for the sentinel lymph node biopsy and axillary lymph node dissection was always performed separately from the breast incisions. The polyurethane and polyester breast-shaped cup with oxygen-enriched oleic matrix was applied to the oncologic breast immediately after surgery, covering the entire breast and sutures without the need for additional secondary dressings, while the contralateral breast received standard treatment with sterile patches [Figure 1]. All patients underwent oncoplastic breast surgery with Wise pattern incision, and the device was applied irrespective of comorbidities to assess its general applicability across a representative population. The devices evaluated are CE-marked in compliance with Regulation (EU) 2017/745; they were provided by the hospital and made available to all patients free of charge. These devices support wound healing by creating, through the consistent and gradual release of reactive oxygen species, microenvironmental conditions that are favorable to repair processes and unfavorable to pathogen proliferation. A postoperative bra was then applied to provide adequate compression. The first control and dressing change were performed at 48 hours, evaluating wound and dressing status on each breast, assessing for possible signs of infection or fluid collection, skin condition, and healing progress. If no complication occurred, the next control was performed at 7 days, and the cup was then discontinued.
This design allowed each patient to serve as their own control, comparing the effects of the advanced dressing on the more complication-prone oncologic breast to the standard treatment on the other. While each patient served as their own control, the study design is purely retrospective, and outcomes were compared between the oncologic and non-oncologic breasts treated with different dressings.
The study was conducted at Ospedale di Cattinara in Trieste.
The evaluation period spanned from 1st June 2024 to 30th June 2025.
The inclusion and exclusion criteria are summarized in Table 1.
Data on possible wound complications were collected at each follow-up visit, specifically incidence of dehiscence, seroma, infection, delayed wound healing, and need for additional interventions were assessed. Data integrity was ensured through standardized collection methods and trained personnel. Patient and staff experiences with the device were also recorded. The primary endpoint was the incidence of wound dehiscence and other minor complications. Secondary endpoints included the wound healing process evaluation, patient comfort and satisfaction, and healthcare personnel assessment.
While the primary endpoint of the study was the incidence of complications, we also gathered feedback from patients and healthcare staff on their experience with the advanced dressing. Specifically, patients were asked about comfort, such as the softness of the material, the absence of adhesive tape, any irritation or pruritus, and the ability of the dressing to absorb secretions and maintain dryness. Healthcare staff provided feedback on the ease of application and removal of the dressing, as well as its adaptability during postoperative care. Although these questions were not part of a standardized questionnaire, they provided valuable insights into patient satisfaction and the practical usability of the dressing.

Table 1.
Inclusion and exclusion criteria.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Unilateral lumpectomy | Known hypersensitivity to any device component |
| Controlateral breast remodeling Compliance to 1 year follow-up Ability to sign for informed consent |
Known hypersensitivity to any device component Any disorder compromising informed consent signing Previous breast radiotherapy |
3. Results
The study included 60 patients aged between 33 and 64 years, with a mean age of 47.3 years; the BMI range was 18.5–29.6, with a mean of 24.3. All oncologic-side surgeries utilized volume displacement techniques, and no volume replacement cases were included. All patients underwent contralateral breast surgery. Among these procedures, 54 were breast reductions and 6 were mastopexies. Fifty-four patients (90%) underwent axillary sentinel lymph node biopsy, while 6 patients (10%) had axillary lymph node dissection. The initial breast sizes ranged from A to F cups. Twelve patients (20%) were smokers, and 3 patients (5%) were diabetic, none of whom experienced complications. Notably, no infections or seromas occurred, and no additional surgeries were required. Furthermore, no allergies or skin pathologies were reported.
Wound dehiscence occurred in 6 patients (10%), equally distributed between the two groups. Delayed healing was also observed in 6 patients (10%), with 3 in the oncologic breasts treated with the advanced dressing and 3 in the control breasts. No patients developed hematomas. Regarding fat necrosis, no cases led to delayed healing, dehiscence, or the need for re-intervention. However, late or deep fat necrosis was not included in the analysis, as no imaging studies (e.g., ultrasound) were performed. Patients parameters are summarized in Table 2. While the advanced dressing provided adequate hydration crucial for healing, it did not significantly reduce the incidence of delayed healing compared with the control group.
The use of the advanced dressing resulted in excellent skin hydration and high patient comfort. Medical staff reported that the device was easy to apply and remove. Patients also found it comfortable, and the incidence of complications was comparable between breasts treated with the advanced dressing and those treated with standard patches. No infections were observed.
Table 1.
Patients parameters.
| Parameter | Value |
|---|---|
| Number of patients | 60 |
| Age (years) BMI Breast Sizes (Cup) Smokers Diabetes Allergies/Skin Pathologies Axillary sentinel lymphnode biopsy Axillary lymphnode dissections Infections Seromas Hematomas Need for additional surgeries Wound dehiscence Delayed healing |
33-64 (mean: 47.3) 18.5-29.6 (mean: 24.3) A to F 12 (20%) 3 (5%) 0 (0%) 54 (90%) 6 (10%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 6 (10%) 6 (10%) |
4. Discussion
Oncoplastic breast surgery combines oncological and plastic surgery techniques to achieve both therapeutic and cosmetic outcomes, ensuring breast aesthetics while maintaining oncological clearance. The remodeling of the excised breast, coupled with the symmetrization of the contralateral breast, offers significant benefits, including improved body image and psychological well-being. Additionally, procedures such as reduction mammoplasty on the contralateral breast can reduce the risk of subsequent breast cancer and alleviate symptoms associated with mammary hypertrophy.
Traditional dressings, such as simple sterile band-aids, are commonly used to cover wounds post-surgery. While effective in maintaining cleanliness, they lack transparency for frequent monitoring and do not offer advanced healing properties. In contrast, advanced dressings like hydrofiber-hydrocolloids [8] or negative-pressure wound therapies [9] can provide enhanced moisture control and antimicrobial benefits, albeit at higher costs.
In this study, we evaluated the use of a polyurethane and polyester breast-shaped cup with oxygen-enriched oleic matrix on the oncologic breast following lumpectomy. This device is designed to gradually release reactive oxygen species (ROS), promoting microenvironmental conditions that support wound healing, lymphoid cell recruitment, and angiogenesis. The oleic matrix furthermore provides a protective and moisturizing effect, maintaining a moist wound environment. Any potential side effects or contraindications were monitored. The decision to apply this advanced dressing specifically to the oncologic breast, which is typically more prone to complications [10] such as wound dehiscence and delayed healing, was a key aspect of our design. The finding that there were no statistically significant differences in the incidence of these complications between the treated and control breasts suggests that the breast-shaped cup with oxygen-enriched oleic matrix dressing may perform comparably—or even better—than the standard of care. Nevertheless, a larger cohort and longer follow-up period are necessary to confirm these findings and assess the potential advantages in reducing minor complications.
Effective postoperative care for oncoplastic breast surgery requires optimal exudate management, infection prevention, and careful monitoring. The breast-shaped cup with oxygen-enriched oleic matrix provides favorable conditions for practical postoperative management and positive patient feedback regarding comfort.
The ability to apply the cups immediately following surgery, covering the entire surgical area without adhesive tape, was highly valued by surgeons for its efficiency and time-saving benefits. This feature also allowed for immediate monitoring of skin flap and nipple-areola complex vitality, contributing to effective postoperative management. Healthcare personnel reported that the dressing was easy to apply, replace, and adapt during follow-up care, minimizing procedural discomfort for patients and facilitating routine wound monitoring.
Patients found the cups comfortable to wear under a bra, both during hospitalization and at home. The absence of adhesive tape reduced the risk of irritation or pruritus, while the dressing’s ability to absorb secretions and maintain dryness further enhanced comfort. Although no validated tools were used to assess patient-reported outcomes, qualitative feedback highlighted these practical advantages, which are particularly relevant in optimizing patient compliance.
Together, the positive feedback from patients and staff highlights the potential of this dressing to improve postoperative care in oncoplastic breast surgery. Future studies with validated tools for patient-reported outcomes and a detailed cost-benefit analysis will provide deeper insights into its broader applicability.
Overall, the experience with these devices has been positive. They can be applied directly in the operating room, allowing immediate use of the compression bra. They provide excellent tissue hydration [Figure 2], moderate absorption of secretions, and ease of replacement. High patient comfort and the absence of adhesives that may cause allergic reactions or discomfort upon removal were noted. Healthcare personnel also reported high compliance, with the ability to easily check tissue condition and vitality. The lack of statistically significant differences in minor complications may be due to the limited sample size and short follow-up period in this study.
The results therefore indicate that the breast-shaped cup with oxygen-enriched oleic matrix is a comfortable and user-friendly option for postoperative care in oncoplastic breast surgery.
A notable limitation of this study is the small sample size, which may have constrained the statistical power to detect differences in minor complications between treatment groups. However, a strength of our study design is that each patient served as their own control, allowing for a direct comparison of outcomes within the same individual. This within-subject comparison helps mitigate variability and enhances the reliability of our findings, making the results more robust despite the limited number of participants.
From a statistical perspective, our findings should be interpreted with caution given the exploratory nature of the study. A hypothetical power analysis suggests that a much larger cohort would be required to detect clinically meaningful differences in complication rates. For example, to demonstrate a reduction in minor complications from 10% to 5% with 80% power and a two-sided α of 0.05, approximately 868 patients would be necessary in a parallel trial. In a paired within-patient design, about 280–410 patients would be required depending on discordant rate assumptions. These estimates highlight the limitations of the present sample while reinforcing the need for larger, adequately powered prospective studies to confirm the encouraging observations of our single-center experience.
Overall, while the breast-shaped cup with oxygen-enriched oleic matrix dressing showed promise in providing a comfortable and effective postoperative care option, further research with larger cohorts and longer follow-up periods is needed to fully evaluate its potential benefits and any associated risks.
5. Conclusions
The polyurethane and polyester breast-shaped cup with oxygen-enriched oleic matrix proved to be a comfortable and easy-to-use option for postoperative care in oncoplastic breast surgery, providing adequate hydration without increasing complications. These preliminary findings suggest that the device may represent a practical and patient-friendly alternative to conventional dressings, particularly in settings where comfort, ease of monitoring, and tissue hydration are priorities. Future studies with larger, adequately powered cohorts, validated patient-reported outcome measures, and longer follow-up are warranted to confirm its potential benefits and fully assess any associated risks.
Author Contributions
Conceptualization, A.R., S.B and G.P.; methodology, A.R. and S.B.; investigation, A.R., S.B., G.B.S, and E.B.; resources, G.P.; data curation, A.R.; writing—original draft preparation, A.R.; writing—review and editing, A.R.; supervision, G.P, A.L, G.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University of Trieste.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting reported results are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank the nursing staff of the Plastic Surgery Unit, Ospedale di Cattinara, for their collaboration in postoperative management and data collection.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Macmillan RD, James R, Gale KL, McCulley SJ. Therapeutic mammaplasty. J Surg Oncol. 2014 Jul;110(1):90-5. doi: 10.1002/jso.23659. Epub 2014 May 29. PMID: 24889526. [CrossRef] [PubMed]
- Palmieri B, Benuzzi G, Costa A, Grappolini S. Breast reduction and subsequent cancer: a prophylactic perspective. Breast. 2006 Aug;15(4):476-81. doi: 10.1016/j.breast.2005.09.011. Epub 2005 Dec 20. PMID: 16364646. [CrossRef] [PubMed]
- Klinger M, Giannasi S, Klinger F, Caviggioli F, Bandi V, Banzatti B, Forcellini D, Maione L, Catania B, Vinci V, Lisa A, Cornegliani G, Siliprandi M, Tinterri C. Periareolar Approach in Oncoplastic Breast Conservative Surgery. Breast J. 2016 Jul;22(4):431-6. doi: 10.1111/tbj.12590. Epub 2016 Apr 18. PMID: 27088898. [CrossRef] [PubMed]
- Ghilli M, Lisa AVE, Salgarello M, Papa G, Rietjens M, Folli S, Curcio A, Ferrari G, Caruso F, Altomare V, Friedman D, De Santis MC, De Rose F, Meduri B, De Felice F, Marino L, Cucciarelli F, Montemezzi S, Panizza P, Belli P, Caumo F, Vinci V, De Santis G, Klinger M, Roncella M; Senonetwork working group. Oncoplastic and reconstructive surgery in SENONETWORK Italian breast centers: lights and shadows. Breast. 2024 Feb;73:103601. doi: 10.1016/j.breast.2023.103601. Epub 2023 Nov 18. PMID: 38043223; PMCID: PMC10731356. [CrossRef] [PubMed]
- Benedict KC, Brown MI, Berry HA, et al. Oncoplastic Breast Reduction: A Systematic Review of Postoperative Complications. Plast Reconstr Surg Glob Open. 2023.
- Dunnill C, Patton T, Brennan J, et al. Reactive oxygen species (ROS) and wound healing: the functional role of ROS and emerging ROS-modulating technologies for augmentation of the healing process. Int Wound J. 2017.
- Poljšak N, Kreft S, Kočevar Glavač N. Vegetable butters and oils in skin wound healing: Scientific evidence for new opportunities in dermatology. Phytother Res. 2020.
- Nicotera A, Ferrando PM, Ala A, et al. An Advanced Surgical Dressing for High-risk Patients Undergoing Breast Cancer Surgery: a Case-control Study. Plast Reconstr Surg Glob Open. 2021.
- Iqbal FM, Reid JP, Vidya R. Oncoplastic breast surgery: the role of negative pressure wound therapy. J Wound Care. 2020.
- Marano, Andrew A. M.D.; Grover, Karan M.D., Pharm.D.; Peysakhovich, Anya P.A.-C.; Lin, Alexandra J. M.D.; Castillo, Wendy Ph.D.; Rohde, Christine H. M.D., M.P.H. Comparing Outcomes after Oncoplastic Breast Reduction and Breast Reduction for Benign Macromastia. Plastic and Reconstructive Surgery 149(3):p 541-548, March 2022. [CrossRef]
Figure 1.
Immediate post-operative medication.
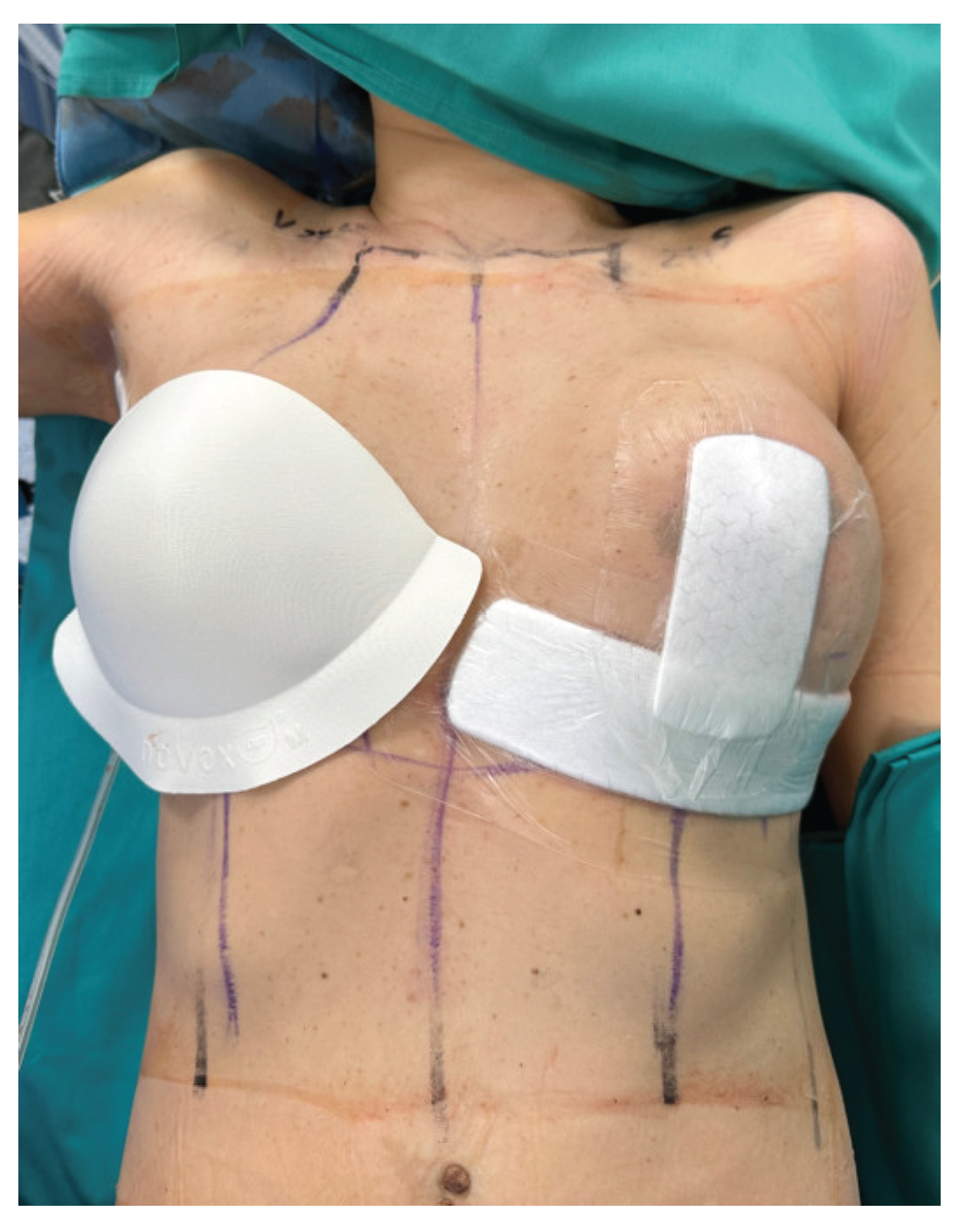
Figure 2.
Post-op assessment.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



