
Submitted:
27 November 2025
Posted:
27 November 2025
You are already at the latest version
Abstract
Background: Aging is a multidimensional process influenced by biological, psychological, and social factors. Social support contributes to cognitive reserve by reducing stress, promoting mental engagement, and reinforcing a sense of belonging. Objective: To examine the association between perceived social support and cognitive functioning among older adults, and to investigate whether social support mediates the relationship between living arrangements and cognitive performance. Methods: The sample included 265 older adults aged 65 years and above, recruited using snowball sampling between March and July 2025 in rural communities. Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA), and perceived social support was measured with the Multidimensional Scale of Perceived Social Support (MSPSS). Data were analyzed using descriptive and inferential statistics in JASP, with a significance level set at p < 0.05. Results: In this study, higher perceived social support from family, friends, and significant others was associated with better cognitive performance (MoCA: ρ = 0.363–0.497; p < 0.001). Participants with normal cognition (≥26 points) reported greater social support across all dimensions. Multiple regression showed that all three dimensions of social support significantly predicted MoCA scores (R² = 0.290), with the strongest effect from friends’ support (β = 0.371, p < 0.001). Mediation analysis revealed that perceived social support mediated the relationship between living arrangements and cognitive functioning, while the direct effect of cohabitation alone was not significant (indirect effect, p < 0.001). Conclusion: These results highlight the importance of perceived social support in preserving cognitive health in older adults.
Keywords:
social support
; cognition
; aging
; aged
; rural communities
1. Introduction
Aging is a dynamic, complex and unavoidable process that involves biological, psychological and social changes. The course and intensity of these changes are largely influenced by individual characteristics, lifestyle habits as well as environmental and genetic factors [1]. Although everyone aspires to age well by maintaining functional capacity and quality of life in advanced age, this goal largely depends on preserving optimal cognitive and brain functioning [2]. Many older adults experience cognitive decline to varying degrees, which in some may progress to severe impairment and pathological conditions, while others retain most of their cognitive abilities [3]. Continuous cognitive engagement and challenging the adaptability and flexibility of the brain can help older adults mitigate or even reverse some of the negative consequences of age-related brain degeneration through neuroplasticity [4,5].
1.1. Cognitive Aging and Concept of Cognitive Reserve
The concept of cognitive reserve, developed by Yaakov Stern and colleagues, further explains individual differences in cognitive aging by postulating the existence of compensatory mechanisms within the brain [6]. A higher level of cognitive reserve is associated with improved cognitive functioning in older age, even in the presence of brain changes observed in Alzheimer’s disease and other dementias [7]. Individuals with a higher level of cognitive reserve are able to maintain cognitive functioning despite having smaller brain volumes, indicating that the advantages of cognitive reserve operate independently of structural brain differences [8]. Strengthening cognitive re serve therefore appears to play a role in delaying the onset of clinically signifi cant cognitive decline, particularly because individuals with greater reserve enter later life with a higher baseline of cognitive functioning, enabling them to remain above impairment thresholds for a longer period even when the rate of decline does not differ between individuals [9]. Lifelong intellectual, educational, occupational, and social activities contribute to resilience against degenerative brain changes, while factors such as educational attainment, professional involvement, participation in complex mental activities, social support and community connectedness play an important role in maintaining this reserve [10]. Within the context of social support, engagement in socially enriching environments offers cognitive stimulation that may help preserve cognitive functioning even in the presence of structural brain deterioration [11].
1.2. Role of Social Support in Maintaining Cognitive Reserve
Social support contributes to the maintenance of cognitive reserve, particularly given the changing nature of social roles and interactions during aging. It encompasses the help, protection, and sense of belonging that individuals receive through reciprocal social networks and relationships characterized by trust and emotional closeness [12,13]. Moreover, social connections may buffer the effects of brain atrophy on cognition, as individuals with smaller brain volumes can maintain cognitive performance when engaged in diverse and stimulating social networks [14]. Older adults with larger and more diverse social networks tend to perform better on cognitive assessments [15].
Engagement in varied social contexts requires individuals to manage multiple roles and interactions, a cognitive challenge that may strengthen cognitive reserve. Additionally, older adults often experience changes in their social roles and interactions due to physical, emotional, social, or environmental factors. These changes may involve losses, adaptations, and new experiences that shape how older individuals perceive and maintain their social ties [13].
Conversely, individuals embedded in dense, homogenous networks experience less cognitive stimulation, as most contacts occupy similar roles and are interconnected [14]. Reciprocal social relationships and the amount of both received and provided support have a positive impact on overall health and quality of life in older adults, including disease prevention, fewer physical health problems, longer life expectancy, improved cognitive abilities, greater self-esteem, and a sense of belonging [16]. Importantly, the benefits of social support for cognitive reserve are not determined solely by the size or diversity of one’s network. Rather, the quality of relationships, characterized by emotional closeness, trust, and meaningful engagement, is crucial for maintaining cognitive function and overall well-being in older adults [17].
Given the limited effectiveness of pharmacological interventions in preventing or slowing cognitive aging [18], research has increasingly focused on non-pharmacological factors that may support cognitive health. Among these, social support has been shown to play an important role, as it can enhance cognitive reserve and help maintain cognitive function in older adults [19].
1.3. Demographic Decline, Population Ageing and Structural Vulnerability in Rural Vukovar-Srijem County
Vukovar-Srijem County is characterized by markedly adverse demographic trends, including below-average population density, a negative migration balance, and accelerated population ageing [20]. The severity of these changes is reflected in the steady annual decrease of approximately 2.5 percent in the rural population, accompanied by a substantial increase in the number of residents aged 65 years and older [21]. This demographic divergence of simultaneous depopulation and ageing intensifies structural vulnerability in rural communities. Rural areas are also additionally burdened by geographical remoteness, insufficient transport infrastructure, and limited availability of social and healthcare services, all of which reduce the mobility of older adults and hinder their social integration. Under such conditions, maintaining social networks becomes particularly challenging, as older adults face growing isolation while the younger population continues to migrate [22]. According to estimates, only about 5 percent of older adults living in rural areas of the Republic of Croatia use formal long-term healthcare services, which is substantially below the European average of 8 percent [23]. Consequently, older adults rely to a considerable extent on unpaid and private care, which may adversely affect their cognitive and psychosocial well-being in the rural communities of Vukovar-Srijem County [24]. In the context of depopulation, population ageing, and infrastructural limitations, understanding the role of social support is essential for planning interventions aimed at improving the well-being of older adults.
The objective of this study was to examine the association between perceived social support and cognitive functioning in older adults, and to determine whether social support mediates the relationship between living arrangements and cognitive performance.
2. Materials and Methods
2.1. Study Design
This quantitative, cross-sectional study was conducted between March and July 2025 in rural communities of Vukovar-Srijem County, Croatia. To reduce anxiety and increase the comfort of respondents, data were collected in participants’ private homes, an approach previously shown to enhance the reliability of cognitive testing in familiar environments [25].
2.2. Participants
The study included older adults aged 65 years and above residing in rural areas who were able to provide informed consent. Exclusion criteria were age below 65 years, residence in urban communities, and living in institutionalized care facilities.
A non-probabilistic snowball sampling method was used to recruit 265 participants who met the inclusion criteria. The estimated sampling error was 6% with a 95% confidence interval, calculated using an online sample size calculator [26]. Each participant was encouraged to identify other potential respondents meeting the inclusion criteria, which allowed the recruitment of individuals who might otherwise be difficult to reach, as a part of snowball sampling [27].
2.3. Instruments
The study employed three instruments: the Montreal Cognitive Assessment (MoCA), the Multidimensional Scale of Perceived Social Support (MSPSS), and a questionnaire collecting general and sociodemographic information (age, sex, marital status, place of residence, educational attainment, number of children and grandchildren). Participants completed the questionnaire using the paper-and-pencil method.
Montreal Cognitive Assessment (MoCA) is a screening tool for mild cognitive impairment, covering multiple cognitive domains, including executive functions, language, attention and concentration, conceptual thinking, calculation, orientation, memory, and visuoconstructive abilities. The total possible score is 30, with scores of 26 or above considered normal [28]. Training for the administration and interpretation of MoCA was completed online for the purposes of this study. The Croatian version was translated by Dr. I. Martinić Popović and used with the permission of the original author, Dr. Ziad Nasreddine. The internal consistency of MoCA in this study was 0.766.
Multidimensional Scale of Perceived Social Support (MSPSS) consists of 12 items assessing perceived social support across three domains: family, friends, and significant others, with four items per domain. Responses are rated on a 7-point Likert scale from 1 (“strongly disagree”) to 7 (“strongly agree”). Subscale scores (family, friends, significant others) and the total score are calculated by averaging the relevant items. Higher scores indicate greater perceived social support [29]. This instrument was used with permission from the author, Gregory D. Zimet. The MSPSS demonstrated excellent internal consistency, with Cronbach’s α = 0.905 for the total scale, α = 0.970 for the Family subscale, α = 0.942 for the Friends subscale, and α = 0.992 for the Significant Others subscale.
2.4. Data Collection Procedure
Prior to data collection, participants received a research notice form describing the study purpose, confidentiality, voluntary participation, and the right to withdraw at any time. Researchers also explained these details verbally and confirmed participants’ understanding before they signed the informed consent form. Participants first completed the self-administered MSPSS questionnaire. Afterward, the researcher conducted the MoCA cognitive assessment. Finally, general and demographic information was collected, as personal questions could influence responses [30]. In self-administered sections, researchers provided clarifications in a neutral tone of voice without suggesting or directing responses. Completion time was not limited. The average time to complete the full assessment, including cognitive testing, self-assessment of perceived social support, and collection of general and demographic information, was 30 minutes per participant, ranging from 20 to 50 minutes.
2.5. Ethical Considerations
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Participation was voluntary and anonymous, and participants could withdraw at any time. Written approval was obtained from the Higher Institution Ethical Committee (Class: 602-01/25-12/03; IRB: 2158/97-97-10-25-12). All participants were informed, both in writing (through a research notice form) and verbally, about the study objectives, ethical aspects, and instructions for completing the questionnaire. Participation was voluntary, confirmed by signing the informed consent form. Anonymity was guaranteed by separating the questionnaire from the consent form. Respondents were informed that they could withdraw from the study at any time.
2.6. Data Analysis
The frequency distributions of the variables were described using descriptive statistical methods. The distribution of numerical variables was assessed with the Shapiro-Wilk test, which indicated a statistically significant deviation from normality for the variables under study (p < 0.05). Measures of central tendency and dispersion were expressed as medians (Me) and interquartile ranges (IQR) due to the non-normal distribution of the data. The Mann-Whitney U test was used to examine differences between two independent groups, and the Kruskal-Wallis test with Bonferroni correction was applied for comparisons among three or more groups. Multiple linear regression analysis was conducted to assess whether perceived social support predicts cognitive functioning. Mediation analysis was performed to examine whether perceived social support mediates the relationship between living arrangements and cognitive functioning. Prior to the analyses, regression assumptions were checked, confirming the absence of multicollinearity and influential outliers, and verifying the distribution of residuals. Statistical significance was set at p < 0.05. All analyses were performed using JASP software, version 0.19.3 (Department of Psychological Methods, University of Amsterdam, Amsterdam, The Netherlands).
3. Results
A total of 265 participants from rural areas of Vukovar-Srijem County took part in the study, the majority of whom were female (n = 166; 62.6%). Regarding the level of educational attainment, most participants had completed primary school (n = 179; 67.5%). More than half of the respondents were married (51.3%), while 44.2% were widowed. Most participants lived either alone (38.9%) or with their spouse in a nuclear family (35.8%). The majority had children (89.1%) and grandchildren (82.3%). The median age of the participants was 72 years (IQR = 68–75) (Table 1).
3.1. Differences in Total, Family, Friends and Significant Others Perceived Social Support
Educational Attainment
Participants with a secondary educational attainment reported significantly higher total perceived social support, family support, and friend support (p < 0.001, rrb = 0.375; p < 0.001, rrb = 0.375; p < 0.001, rrb = 0.335; medium effect sizes) compared to those with only primary education. Participants with undergraduate/graduate educational attainment also reported higher total, family, and friend support (p = 0.037, rrb = 0.423; p = 0.037, rrb = 0.423; p = 0.013, rrb = 0.482) than participants with primary education. Higher support from other significant persons was perceived in participants with secondary education compared to those with primary education (p < 0.001, rrb = 0.324; medium effect size) (Table 2).
Marital Status and Living Arrangement
Married participants reported higher total perceived social support than widowed (p < 0.001, rrb = 0.757), single (p < 0.001, rrb = 0.958), and divorced participants (p = 0.005, rrb = 0.941), all representing large effect sizes. Married participants also reported higher family support than widowed (p < 0.001, rrb = 0.318; medium effect size) and single participants (p < 0.001, rrb = 0.842; large effect size), and higher support from significant others than widowed (p < 0.001, rrb = 0.839), single (p < 0.001, rrb = 0.997), and divorced participants (p = 0.023, rrb = 0.949; large effect sizes). Widowed participants reported higher family support than single participants (p = 0.029, rrb = 0.696; large effect size), and married participants reported higher friend support than widowed participants (p = 0.005, rrb = 0.243; small effect size).
Participants living in nuclear families (with a spouse) reported higher total perceived social support than those living alone (p < 0.001, rrb = 0.783; large effect size) and those in multigenerational households (p = 0.021, rrb = 0.230; small effect size). Participants in multigenerational households reported higher total support than those living alone (p < 0.001, rrb = 0.505; medium effect size). Higher family, friend, and significant others’ support was reported by participants in nuclear families (p < 0.001, rrb = 0.371; medium; p = 0.008, rrb = 0.243; small; p < 0.001, rrb = 0.867; large) and multigenerational households (p < 0.001, rrb = 0.340; medium; p = 0.003, rrb = 0.299; small; p < 0.001, rrb = 0.462; medium) compared to those living alone. Nuclear family participants reported higher support from significant others than those in multigenerational households (p < 0.001, rrb = 0.343; medium effect size) (Table 2).
Parental Status and Grandparent Status
Participants with children reported higher total perceived social support (p < 0.001, rrb = 0.426; medium effect size) and family support (p < 0.001, rrb = 0.584; large effect size) than participants without children. Participants with grandchildren reported higher total perceived social support (p = 0.006, rrb = 0.254; small effect size) and family support (p < 0.001, rrb = 0.397; medium effect size) than those without grandchildren (Table 2).
Chronological Age and Gender
Participants aged 65–74 years (p = 0.008, rrb = 0.614; large effect size) and 75–84 years (p = 0.004, rrb = 0.589; large effect size) reported significantly higher perceived friend support than participants aged 85 years and older. Additionally, male participants reported higher perceived social support from significant others (p=0.003, rrb=0.215; small effect size) (Table 2).
Measures of central tendency indicate an overall lower level of cognitive functioning in the sample, with a median total MoCA score of 20 (IQR = 17–24). Participants with a secondary educational attainment (p < 0.001, rrb = 0.701; large effect size) and those with undergraduate/graduate education (p < 0.001, rrb = 0.790; large effect size) demonstrated significantly higher cognitive functioning compared to participants with only primary education. Married participants exhibited significantly higher cognitive functioning than widowed participants (p < 0.001, rrb = 0.384; medium effect size). Participants living in a nuclear family (with a spouse) (p < 0.001, rrb = 0.341; medium effect size) and those living in multigenerational households (p < 0.001, rrb = 0.373; medium effect size) also showed significantly higher cognitive functioning. Participants with children had significantly higher cognitive functioning compared to those without children (p = 0.002, rrb = 0.349; medium effect size). Finally, participants aged 65–74 years demonstrated significantly higher cognitive functioning than those aged 75–84 years (p < 0.001, rrb = 0.694; large effect size) and those aged 85 years and older (p < 0.001, rrb = 0.410; medium effect size) (Table 3).
A statistically significant positive association was observed between the total MoCA score and levels of perceived social support, including its subscales. Higher levels of total perceived social support (ρ = 0.497; p < 0.001), family support (ρ = 0.405; p < 0.001), friend support (ρ = 0.466; p < 0.001), and support from other significant persons (ρ = 0.363; p < 0.001) were associated with higher MoCA scores (Table 4).
Participants with normal cognitive functioning reported significantly higher levels of perceived social support compared to those with impaired cognitive functioning, including total perceived social support (rrb = 0.569), family support (rrb = 0.536), friend support (rrb = 0.582), and support from other significant persons (rrb = 0.423), all representing large effect sizes (Table 5).
The model included three independent variables (subscales of social support: family, friends, and significant others). The model was statistically significant (F(3, 261) = 35.583, p < 0.001) and explained 29% of the total variance in MoCA scores (R² = 0.290, Adjusted R² = 0.282). All three dimensions of social support were significant predictors of MoCA scores, with the strongest contribution from friends support (β = 0.371, p < 0.001), while family support (β = 0.160, p = 0.007) and support from significant others (β = 0.162, p = 0.004) also had a significant positive effect. Higher perceived social support was associated with better cognitive functioning (Table 6).
Significant positive correlations were found between perceived social support and cognitive functioning (r = 0.497, p < 0.001), and between living arrangement, social support (r = 0.452, p < 0.001), and cognitive functioning (r = 0.292, p < 0.001) (Table A1).
The direct effect of living arrangement on cognitive functioning was positive but not statistically significant (β = 0.258, p = 0.062), suggesting a trend toward a positive association. The indirect effect, mediated by perceived social support, was β = 0.332 (p < 0.001; 95% CI [0.177, 0.487]), confirming a significant mediation. Individuals living with someone reported higher levels of perceived social support, which in turn contributed to better cognitive functioning. The total effect of living arrangement on the MoCA score was β = 0.589 (p < 0.001), indicating that living arrangement has a significant positive impact on cognitive functioning, primarily through the effect of social support (Table 7, Figure 1).
4. Discussion
The results of the conducted study indicate that older adults represent a heterogeneous population in which social and cognitive outcomes differ across factors such as age, gender, level of education, marital status, and family structure. These findings confirm the need for a comprehensive, holistic approach to the health of older adults, as emphasized by Livingston et al. [31].
Regarding participants’ characteristics, most participants were aged 65–74, whereas adults aged 85 and older were underrepresented. Such a distribution is common in healthcare and gerontological research, as the oldest-old are less likely to participate due to health, mobility, or functional limitations [32]. Additionally, it was observed that older adults with higher educational attainment perceive greater social support, which is consistent with previous studies [33]. It could be postulated that older adults with lower educational attainment may have smaller or less active social networks, as lower educational attainment has frequently been associated with social isolation [34]. Furthermore, higher educational attainment influences older adults’ opportunities to access social activities, participate, and achieve better social integration, and it also enables them to make more effective use of community resources [35]. Therefore, individuals with higher educational attainment are expected to exhibit better cognitive function, largely due to the enhancement of cognitive reserve through lifelong intellectual, educational, occupational, and social activities [10]. This is also because individuals with greater cognitive reserve enter later life with a higher baseline level of cognitive functioning [9].
In addition to marital status, family roles such as being a parent or grandparent also contribute to perceived social support. Married older adults perceive higher levels of social support and achieve better cognitive outcomes, consistent with Sommerlad et al. [36], who report that being married is associated with healthier lifestyle behaviors and lower mortality, and may reduce the risk of dementia due to life-course factors, as well as increased daily social interaction and support, which enhance cognitive reserve. In contrast, lower levels of perceived social support and cognitive functioning are more frequently observed among single and widowed older adults, likely due to the impact of social isolation and its association with adverse cognitive outcomes [37,38].
Older adults who are parents and/or grandparents perceive higher overall social support, particularly from family, which is consistent with previous findings [39]. Hou et al. [39] demonstrated that intergenerational support from adult children is positively associated with cognitive functioning in middle-aged and older adults, and may mediate the relationship between grandparenting and cognitive function. Thus, caring for grandchildren can indirectly influence cognitive functioning by fostering intergenerational support from adult children [39]. Frequent, high-quality interactions with children and grandchildren contribute to emotional stability and help maintain cognitive abilities through social engagement and stimulation, supporting previous evidence on the role of social interactions in preserving cognitive function [39,40]. A difference was also observed in the perception of social support from significant others by men, as it is assumed that the significant other category most often includes their spouse, who is expected to care for their partner’s needs. Men tend to rely on their spouse for intimacy, emotional, instrumental, and caregiving support [35]. Al-Kandari [41] also states that having a living wife is an important factor for men’s health and well-being in general, as the wife is one of the major sources of social support for elderly men.
Although gender differences in overall MoCA scores were not significant in the present study, previous research indicates that women often perform better in verbal domains, as highlighted in methodological evaluations of the MoCA [42]. Beyond gender, age related differences were also observed, with the oldest-old reporting lower levels of perceived social support. Lower perceived levels of social support among the oldest-old may reflect a decrease in social interactions and the size of social networks as age increases [43]. Since social participation has been found to decrease with age in both women and men, it is hypothesized that perceived social support also declines alongside reduced social engagement, particularly in women, although this gender difference diminishes after the age of 80 [35] In contrast, Lara et al. [37] and Fjell et al. [44] report that women, on average, have broader and more functional social networks and utilize social support more effectively as a protective mechanism, although this was not observed in the present study. It could be hypothesized that this is due to sociocultural specificities, as Plužarić et al. [45] in the context of connectedness with family and friends, did not find any significant gender differences among older adults in Croatia.
Age has consistently been identified as a key predictor of cognitive decline, as reported by Piolatta et al. [16], and the results of this study align with these findings, with older participants achieving lower MoCA scores. The positive association between perceived social support and cognitive functioning is consistent with previous evidence [19,46] linking social support and cognitive activity to a reduced risk of subsequent cognitive impairment. Subjective feelings of social support and social integration may benefit cognitive functioning, particularly in stressful situations, by reducing stress and lowering levels of stress hormones such as cortisol, which has been shown to negatively affect cognitive performance [47].
Additionally, the highest correlation and the greatest explained variance in cognitive functioning were observed within the friend support subscale, which may be explained by the fact that friendships often encourage participation in social and cognitively stimulating activities and enhance older adults’ sense of belonging [40]. Because maintaining friendships has been shown to require more active effort and engagement in shared activities, activity engagement may be an underlying pathway explaining the distinct associations between contact frequency with friends versus family and cognition [40]. Friendship ties also play a uniquely protective role in later-life cognitive functioning. Maintaining or restoring active friendship networks promotes social engagement and cognitive stimulation, with the recovery of previously lost friendships being particularly beneficial for cognitive functioning, especially among older men [48]. Therefore, individuals who perceive higher levels of support from family, friends, or significant others may experience better cognitive outcomes, as social engagement provides emotional, instrumental, and cognitive stimulation that helps preserve cognitive functioning. The results also highlight the importance of the perceived level of social support, rather than merely the absence of social isolation.
Mediation analysis indicates that living with someone is associated with higher cognitive functioning primarily through perceived social support, rather than through the mere number of cohabitants. This aligns with results reported by Amieva et al. [49], highlighting the importance of the quality and perception of social relationships in maintaining cognitive abilities in older adults. Participants who felt satisfied with their relationships had a 23% lower risk of dementia, and those who reported giving less support than they received over their lifetime had a 55% lower risk of dementia and a 53% lower risk of Alzheimer’s disease, respectively. Importantly, the only variables associated with subsequent dementia or Alzheimer’s disease were those reflecting the quality of relationships. These findings from the mediation analysis suggest that the perceived level of social support, rather than the mere number of cohabitants, is an important factor for maintaining cognitive functioning in older adults.
4.1. Limitations and Implications for Future Research
Despite the valuable findings, this study has several limitations. The cross-sectional design does not allow causal inferences, and longitudinal research is needed to clarify the direction of the association between perceived social support and cognitive abilities. Furthermore, the instruments used carry methodological constraints: the MoCA is sensitive to educational attainment [50], while the MSPSS reflects a subjective perception of support that may not correspond to its actual structure or quality [29]. The sample was relatively homogeneous in geographical and cultural terms, which limits the generalizability of the findings, particularly given the known cultural variations in social support structures [51]. In addition, the participants were predominantly younger older adults compared to the oldest-old group, which may result in a somewhat more optimistic picture relative to the broader older population.
Nevertheless, the study highlights the importance of perceived social support for cognitive functioning in older adults and points to key directions for future research. Longitudinal studies are needed, as well as a combination of quantitative and qualitative approaches, the inclusion of diverse cultural contexts, and the development of intervention models aimed at enhancing social engagement. Particular attention should be given to digital forms of social support, which are becoming increasingly relevant in preventing social isolation [52].
5. Conclusions
The present study demonstrates that older adults in rural areas of Vukovar-Srijem County represent a heterogeneous population, with cognitive functioning and perceived social support varying according to age, education level, marital status, family roles, and living arrangements. Older adults with higher educational attainment, those who were married, those with children and grandchildren, and those living in nuclear or multigenerational households exhibited higher levels of social support. Additionally, older adults with higher educational attainment, those who were married, those living in nuclear or multigenerational households, and those with children demonstrated significantly better cognitive functioning. Perceived social support was positively correlated with cognitive outcomes across all domains, with friend support showing the strongest association and also emerging as the most significant predictor of cognitive functioning. Mediation analysis revealed that the beneficial effect of living with others on cognitive functioning is largely explained by the perceived level of social support, highlighting that the perception of social support, rather than mere cohabitation, is crucial for maintaining cognitive abilities in older adults. These findings underscore the importance of interventions aimed at enhancing social support networks, promoting social engagement, and fostering meaningful interpersonal relationships in rural communities. Such measures may help mitigate the negative effects of ageing and limited access to formal care, ultimately supporting cognitive health and overall well-being in older adults.
Author Contributions
Conceptualization. M.K., Ž.M., K.M.P. and J.V. methodology. M.K., Ž.M., I.B. and N.F.; software. Ž.M. and I.B.; validation. M.K., Ž.M., N.F. and M.Č.; formal analysis. Ž.M., I.B., J.V. and R.L.; investigation. M.K., Ž.M., M.B. and M.Č.; resources. M.K. and M.B.; data curation. R.L., K.M.P., J.V. and M.Č.; writing—original draft preparation. M.K., Ž.M., N.F., K.M.P. and M.B.; writing—review and editing. M.K., Ž.M., M.Č., R.L., I.B. and J.V.; visualization. M.K., M.B. and K.M.P.; supervision. N.F. and R.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Higher Institution Ethical Committee Faculty of Dental Medicine and Health Osijek (Class: 602-01/25-12/03; IRB: 2158/97-97-10-25-12).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study. Participation was voluntary and anonymous, with participants retaining the right to withdraw at any time.
Data Availability Statement
The original data presented in the study are openly available on FigShare at https://doi.org/10.6084/m9.figshare.30705632.
Acknowledgments
We sincerely thank all the older adults who participated in this study for their time, cooperation, and valuable contribution.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Appendix A.1

Table A1.
Spearman Correlations Between Perceived Social Support, Total Cognitive Functioning and Living arrangement.
Table A1.
Spearman Correlations Between Perceived Social Support, Total Cognitive Functioning and Living arrangement.
| Variable | 1 | 2 |
|---|---|---|
| 1. Total score of MSSP | - | - |
| 2. Total score of MoCa | 0.497* | - |
| 3. Living arrangement | 0.452* | 0.292* |
*< 0.001.
References
- Argentieri, M.A.; Amin, N.; Nevado-Holgado, A.J.; Sproviero, W.; Collister, J.A.; Keestra, S.M.; et al. Integrating the environmental and genetic architectures of aging and mortality. Nat Med 2025, 31, 1016–1025. [Google Scholar] [CrossRef]
- Waddell, C.; Van Doorn, G.; Power, G.; Statham, D. From Successful Ageing to Ageing Well: A Narrative Review. Gerontologist 2024, 65, gnae109. [Google Scholar] [CrossRef]
- Cohen, R.A.; Marsiske, M.M.; Smith, G.E. Chapter 10 - Neuropsychology of aging. In: Handbook of Clinical Neurology; Dekosky ST. Asthana S. Eds.; Elsevier: Amsterdam. The Netherlands. 2019; Volume 167. pp. 149–180. [CrossRef]
- Pauwels, L.; Chalavi, S.; Swinnen, S.P. Aging and brain plasticity. Aging (Albany NY) 2018, 10, 1789–1790. [Google Scholar] [CrossRef]
- Rehan, S.; Phillips, N.A. Psychosocial Function in Mild Cognitive Impairment: Social Participation is Associated With Cognitive Performance in Multiple Domains. J Appl Gerontol 2025, 44, 1629–1640. [Google Scholar] [CrossRef]
- Stern, Y. What is cognitive reserve? Theory and research application of the reserve concept. J Int Neuropsychol Soc 2002, 8, 448–460. [Google Scholar] [CrossRef]
- Lin, L.; Ni, L.; Wang, X.; Sheng, C. Longitudinal cognitive change and duration of Alzheimer’s disease stages in relation to cognitive reserve. Neuroscience 2022, 504, 47–55. [Google Scholar] [CrossRef]
- Yang, W.; Wang, J.; Guo, J.; Dove, A.; Qi, X.; Bennett, D.A.; et al. Association of Cognitive Reserve Indicator with Cognitive Decline and Structural Brain Differences in Middle and Older Age: Findings from the UK Biobank. J Prev Alzheimers Dis 2024, 11, 739–748. [Google Scholar] [CrossRef]
- Corley, J.; Conte, F.; Harris, S.E.; Taylor, A.M.; Redmond, P.; Russ, T.C.; et al. Predictors of longitudinal cognitive ageing from age 70 to 82 including APOE e4 status, early-life and lifestyle factors: the Lothian Birth Cohort 1936. Mol Psychiatry 2023, 28, 1256–1271. [Google Scholar] [CrossRef]
- Stern, Y.; Arenaza-Urquijo, E.M.; Bartrés-Faz, D.; Belleville, S.; Cantilon, M.; Chetelat, G.; et al. Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dement 2020, 16, 1305–1311. [Google Scholar] [CrossRef]
- Evans, I.E.M.; Llewellyn, D.J.; Matthews, F.E.; Woods, R.T.; Brayne, C.; Clare, L.; et al. Social isolation, cognitive reserve, and cognition in healthy older people. PLOS ONE 2018, 13, e0201008. [Google Scholar] [CrossRef]
- Langford, C.P.; Bowsher, J.; Maloney, J.P.; Lillis, P.P. Social support: a conceptual analysis. J Adv Nurs 1997, 25, 95–100. [Google Scholar] [CrossRef]
- Sims, R.C.; Hosey, M.; Levy, S.A.; Whitfield, K.E.; Katzel, L.I.; Waldstein, S.R. Distinct functions of social support and cognitive function among older adults. Exp Aging Res 2014, 40, 40–59. [Google Scholar] [CrossRef]
- Perry, B.L.; Roth AR: Peng, S.; Risacher, S.L.; Saykin, A.J.; Apostolova, L.G. Social Networks and Cognitive Reserve: Network Structure Moderates the Association Between Amygdalar Volume and Cognitive Outcomes. J Gerontol B Psychol Sci Soc Sci 2022, 77, 1490–1500. [Google Scholar] [CrossRef]
- Rai, P.; Sundarakumar, J.S. Association between social networks and cognition among middle-aged and older adults in rural India. Neuropsychology 2024, 38, 740–748. [Google Scholar] [CrossRef]
- Piolatto, M.; Bianchi, F.; Rota, M.; Marengoni, A.; Akbaritabar, A.; Squazzoni, F. The effect of social relationships on cognitive decline in older adults: an updated systematic review and meta-analysis of longitudinal cohort studies. BMC Public Health 2022, 22, 278. [Google Scholar] [CrossRef]
- Dodds, L.; Brayne, C.; Siette, J. Associations between social networks, cognitive function, and quality of life among older adults in long-term care. BMC Geriatr 2024, 24, 221. [Google Scholar] [CrossRef]
- Pazan, F.; Petrovic, M.; Cherubini, A.; Cruz-Jentoft, A.J.; Denkinger, M.; van der Cammen, T.J.M.; et al. A Systematic Review of the Current Evidence from Randomised Controlled Trials on the Impact of Medication Optimisation or Pharmacological Interventions on Quantitative Measures of Cognitive Function in Geriatric Patients. Drugs Aging 2022, 39, 863–874. [Google Scholar] [CrossRef]
- Ma, T.; Liao, J.; Ye, Y.; Li, J. Social support and cognitive activity and their associations with incident cognitive impairment in cognitively normal older adults. BMC Geriatr 2024, 24, 38. [Google Scholar] [CrossRef]
- Vukovar-srijem county, plan of development 2021. - 2027. Available online: https://vusz.hr/plan-razvoja-vsz-2021-2027/ (accessed on 8 September 2025).
- Urban-rural Europe - demographic developments in rural regions and areas. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Urban-rural_Europe_-_demographic_developments_in_rural_regions_and_areas (accessed on 8 September 2025).
- Državni zavod za statistiku - Objavljeni konačni rezultati Popisa 2021. Available online: https://dzs.gov.hr/vijesti/objavljeni-konacni-rezultati-popisa-2021/1270 (accessed on 9 September 2025).
- World Bank - Successfully Adapting Health and Social Care to an Older Population in Croatia : Policy Note. Available from: https://documents1.worldbank.org/curated/en/333531592972673248/pdf/Successfully-Adapting-Health-and-Social-Care-to-an-Older-Population-in-Croatia-Policy-Note.pdf (accessed on 11th September 2025).
- Barišić, M.; Mudri, Ž.; Farčić, N.; Čebohin, M.; Degmečić, D.; Barać, I. Subjective Well-Being and Successful Ageing of Older Adults in Eastern Croatia—Slavonia: Exploring Individual and Contextual Predictors. Sustainability 2024, 16, 7808. [Google Scholar] [CrossRef]
- Cyr, A.A.; Romero, K.; Galin-Corini, L. Web-Based Cognitive Testing of Older Adults in Person Versus at Home: Within-Subjects Comparison Study. JMIR Aging 2021, 4, e23384. [Google Scholar] [CrossRef]
- Sample Size Calculator. Available online: https://www.calculator.net/sample-size-calculator.html (accessed on 1 September 2025).
- Remler, D.K.; Van Ryzin, G.G. Research methods in practice: strategies for description and causation. 3rd ed.; SAGE: Los Angeles. USA. 2022; p. 650.
- Islam, N.; Hashem, R.; Gad, M.; Brown, A.; Levis, B.; Renoux, C.; et al. Accuracy of the Montreal Cognitive Assessment tool for detecting mild cognitive impairment: A systematic review and meta-analysis. Alzheimers Dement 2023, 19, 3235–3243. [Google Scholar] [CrossRef]
- Ng, S.S.M.; Liu, T.W.; Ho, L.Y.W.; Chan, N.H.; Wong, T.W.L.; Tsoh, J. Assessing the level of perceived social support among community-dwelling stroke survivors using the Multidimensional Scale of Perceived Social Support. Sci Rep 2022, 12, 19318. [Google Scholar] [CrossRef]
- Lamza-Posavec, V. Metodologija društvenih istraživanja - temeljni uvidi. 1st ed.; Institut društvenih znanosti Ivo Pilar: Zagreb, Croatia, p. 334.
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Paine, N.; Lowe, M.; Young, C.; Turrell, G. Engaging under-represented oldest old in research: An approach for inclusive recruitment. Australas J Ageing 2024, 43, 844–851. [Google Scholar] [CrossRef]
- Pais, R.; Ruano, L.; Moreira, C.; Fraga, S.; P Carvalho O; Barros H. Social Support and Cognitive Impairment: Results from a Portuguese 4-Year Prospective Study. Int J Environ Res Public Health 2021, 8, 8841. [CrossRef]
- Smith, S.G.; Jackson, S.E.; Kobayashi, L.C.; Steptoe, A. Social isolation, health literacy, and mortality risk: Findings from the English Longitudinal Study of Ageing. Health Psychol 2018, 37, 160–169. [Google Scholar] [CrossRef]
- Ong, C.H.; Pham, B.L.; Levasseur, M.; Tan, G.R.; Seah, B. Sex and gender differences in social participation among community-dwelling older adults: a systematic review. Front Public Health 2024, 12, 1335692. [Google Scholar] [CrossRef]
- Sommerlad, A.; Ruegger, J.; Singh-Manoux, A.; Lewis, G.; Livingston, G. Marriage and risk of dementia: systematic review and meta-analysis of observational studies. J Neurol Neurosurg Psychiatry 2018, 89, 231–238. [Google Scholar] [CrossRef]
- Lara, E.; Caballero, F.F.; Rico-Uribe, L.A.; Olaya, B.; Haro, J.M.; Ayuso-Mateos, J.L.; et al. Are loneliness and social isolation associated with cognitive decline? Int J Geriatr Psychiatry 2019, 34, 1613–1622. [Google Scholar] [CrossRef]
- Guarnera, J.; Yuen, E.; Macpherson, H. The Impact of Loneliness and Social Isolation on Cognitive Aging: A Narrative Review. J Alzheimers Dis Rep 2023, 7, 699–714. [Google Scholar] [CrossRef]
- Hou, X.; Luo, Y.; Yang, F.; Zhu, X.; Gao, X.; Wang, W.; et al. The mediating role of children’s intergenerational support in association between grandparenting and cognitive function among middle-aged and older Chinese: findings from the CHARLS cohort study. BMC Public Health 2024, 24, 597. [Google Scholar] [CrossRef]
- Sharifian, N.; Kraal, A.Z.; Zaheed, A.B.; Sol, K.; Zahodne, L.B. Longitudinal Associations Between Contact Frequency with Friends and with Family, Activity Engagement, and Cognitive Functioning. J Int Neuropsychol Soc 2020, 26, 815–824. [Google Scholar] [CrossRef]
- Al-Kandari, Y.Y. Older Men With Living Spouses Versus Men Without Spouses: An Example From the Arab World—Kuwait. Am J Mens Health 2020, 14, 1557988320937213. [Google Scholar] [CrossRef]
- Islam, N.; Hashem, R.; Gad, M.; Brown, A.; Levis, B.; Renoux, C.; et al. Accuracy of the Montreal Cognitive Assessment tool for detecting mild cognitive impairment: A systematic review and meta-analysis. Alzheimers Dement 2023, 19, 3235–3243. [Google Scholar] [CrossRef]
- Yin, S.; Yang, Q.; Xiong, J.; Li, T.; Zhu, X. Social Support and the Incidence of Cognitive Impairment Among Older Adults in China: Findings From the Chinese Longitudinal Healthy Longevity Survey Study. Front Psychiatry 2020, 11, 254. [Google Scholar] [CrossRef]
- Fjell, A.; Cronfalk Seiger, B.; Hermann, M.; Rongve, A.; Aßmus, J.; Kvinge, L.; et al. Factors associated with self-rated health in a Norwegian population of older people participating in a preventive home visit program: a cross-sectional study. BMC Geriatrics 2020, 20, 323. [Google Scholar] [CrossRef]
- Plužarić, J.; Barać, I.; Ilakovac, V.; Lovrić, R.; Farčić, N.; Mudri, Ž.; et al. Connectedness and Successful Aging of Older Adults in Croatia. Sustainability 2023, 15, 10843. [Google Scholar] [CrossRef]
- Gui, S.; Wang, J.; Li, Q.; Chen, H.; Jiang, Z.; Hu, J.; et al. Sources of perceived social support and cognitive function among older adults: a longitudinal study in rural China. Front Aging Neurosci 2024, 16, 1443689. [Google Scholar] [CrossRef]
- Kuiper, J.S.; Zuidersma, M.; Zuidema, S.U.; Burgerhof, J.G.; Stolk, R.P.; Oude Voshaar, R.C.; Smidt, N. Social relationships and cognitive decline: a systematic review and meta-analysis of longitudinal cohort studies. Int J Epidemiol 2016, 45, 1169–1206. [Google Scholar] [CrossRef]
- Li, J. Longitudinal Associations Between Friendship and Cognitive Function Among Older Chinese Adults: Will Gender Make a Difference? J Appl Gerontol 2025, 07334648251338568. [Google Scholar] [CrossRef]
- Amieva, H.; Stoykova, R.; Matharan, F.; Helmer, C.; Antonucci, T.C.; Dartigues, J.F. What aspects of social network are protective for dementia? Not the quantity but the quality of social interactions is protective up to 15 years later. Psychosom Med 2010, 72, 905–911. [Google Scholar] [CrossRef]
- Aiello, E.N.; Gramegna, C.; Esposito, A.; Gazzaniga, V.; Zago, S.; Difonzo, T.; et al. The Montreal Cognitive Assessment (MoCA): updated norms and psychometric insights into adaptive testing from healthy individuals in Northern Italy. Aging Clin Exp Res 2022, 34, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Sohn, S.Y.; Joo, W.T.; Kim, W.J.; Kim, S.J.; Youm, Y.; Kim, H.C.; et al. Social network types among older Korean adults: Associations with subjective health. Soc Sci Med 2017, 173, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Czaja, S.J.; Boot, W.R.; Charness, N.; Rogers, W.A.; Sharit, J. Improving Social Support for Older Adults Through Technology: Findings From the PRISM Randomized Controlled Trial. Gerontologist 2018, 58, 467–477. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements. opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas. methods. instructions or products referred to in the content. |
Figure 1.
Mediation model of Perceived Social Support on Cognitive Functioning.
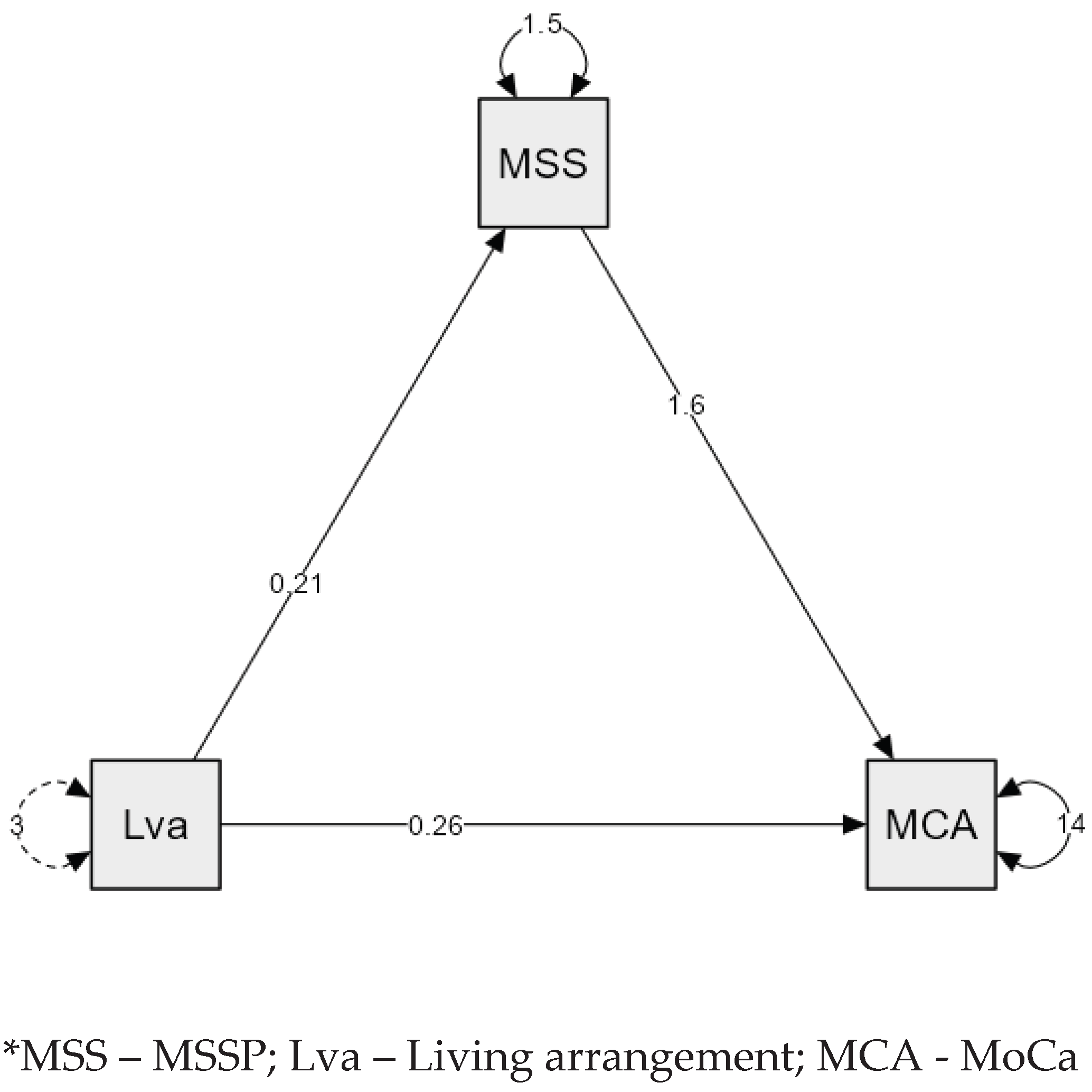
Table 1.
Sociodemographic characteristics of respondents.
| Characteristics of Respondents | Category | n (%) |
|---|---|---|
| Gender | Male | 99 (37,4) |
| Female | 166 (62,6) | |
| Other | 0 (0) | |
| Educational attainment | Primary school | 179 (67,5) |
| Secondary school | 74 (27,9) | |
| Undergraduate/graduate degree | 12 (4,5) | |
| Marital status | Married | 136 (51,3) |
| Widowed | 117 (44,2) | |
| Divorced | 5 (1,9) | |
| Never married | 7 (2,6) | |
| Living arrangement | Living alone | 103 (38,9) |
| Nuclear family (spouse) | 95 (35,8) | |
| Spouse and children | 20 (7,5) | |
| Spouse, children and grandchildren | 19 (7,2) | |
| With child/children | 20 (7,5) | |
| With child/children and grandchildren | 8 (3) | |
| Parental status | Yes | 236 (89,1) |
| No | 29 (10,9) | |
| Grandparent status | Yes | 218 (82,3) |
| No | 47 (17,7) | |
| Chronological age | 65–74 years | 186 (70,2) |
| 75–84 years | 69 (26) | |
| ≥85 years | 10 (3,8) | |
| Me (IQR) = 72 (68 - 75) |
Table 2.
Differences in Perceived Social Support (Total, Family, Friends, Significant Others) Among Older Adults by General Characteristics – MSPSS.
Table 2.
Differences in Perceived Social Support (Total, Family, Friends, Significant Others) Among Older Adults by General Characteristics – MSPSS.
| Characteristics of Respondents | MSPSS (total) | p value | Family | p value | Friends | p value | Significant Others | p value | |
|---|---|---|---|---|---|---|---|---|---|
| Me (IQR) | Me (IQR) | Me (IQR) | Me (IQR) | ||||||
| Gender | Male | 5.58 (4.33 - 6.25) | 0.070 | 6.00 (5.13 - 7.00) | 0.463 | 5.00 (4.00 - 5.63) | 0.619* | 6.00 (3.00 - 7.00) | 0.003* |
| Female | 4.66 (4.00 - 6.00) | 6.50 (5.81 - 7.00) | 5.00 (4.25 - 5.75) | 4.88 (1.00 - 6.19) | |||||
| Educational attainment | Primary school | 4.67 (3.92 - 5.83) | < 0.001† | 6.00 (5.00 - 7.00) | 0.003† | 5.00 (3.75 - 5.25) | < 0.001† | 5.00 (1.00 - 6.00) | < 0.001† |
| Secondary school | 5.88 (4.48 - 6.50) | 6.88 (6.00 - 7.00) | 5.00 (4.56 - 6.00) | 6.00 (2.44 - 7.00) | |||||
| Undergraduate/graduate degree | 6.08 (4.58 - 6.56) | 6.88 (6.69 - 7.00) | 5.75 (5.00 - 6.25) | 6.13 (3.00 - 6.63) | |||||
| Marital status | Married | 6.00 (5.33 - 6.50) | < 0.001† | 7.00 (6.00 - 7.00) | < 0.001† | 5.00 (4.50 - 6.00) | 0.004† | 6.00 (6.00 - 7.00) | < 0.001† |
| Widowed | 4.25 (3.58 - 4.67) | 6.00 (5.00 - 7.00) | 5.00 (3.75 - 5.00) | 1.00 (1.00 - 3.00) | |||||
| Divorced | 4.08 (4.00 - 4.17) | 5.50 (5.00 - 6.50) | 4.50 (2.75 - 5.00) | 3.00 (2.00 - 3.00) | |||||
| Never married | 2.67 (2.33 - 4.00) | 3.00 (2.50 - 5.00) | 5.00 (4.00 - 5.50) | 1.00 (1.00 - 1.00) | |||||
| Living arrangement | Living alone | 4.08 (3.38 - 4.67) | < 0.001† | 6.00 (5.00 - 6.75) | < 0.001† | 4.75 (3.00 - 5.00) | < 0.001† | 1.00 (1.00 - 3.00) | < 0.001† |
| Nuclear family (spouse) | 5.92 (5.33 - 6.38) | 7.00 (6.00 - 7.00) | 5.00 (4.50 - 6.00) | 6.00 (6.00 - 7.00) | |||||
| Multigenerational family | 5.25 (4.33 - 6.42) | 7.00 (6.00 - 7.00) | 5.00 (4.50 - 6.00) | 5.50 (1.00 - 7.00) | |||||
| Parental status | Yes | 5.17 (4.31 - 6.25) | < 0.001* | 6.75 (6.00 - 7.00) | < 0.001* | 5.00 (4.25 - 5.75) | 0.085* | 5.25 (1.00 - 6.50) | 0.222* |
| No | 3.83 (2.92 - 5.33) | 5.00 (2.50 - 6.00) | 5.00 (3.00 - 5.00) | 2.50 (1.00 - 6.50) | |||||
| Grandparent status | Yes | 5.17 (4.27 - 6.23) | 0.006* | 6.75 (6.00 - 7.00) | < 0.001* | 5.00 (4.25 - 5.75) | 0.272* | 5.13 (1.00 - 6.44) | 0.817* |
| No | 4.33 (3.46 - 5.79) | 6.00 (4.75 - 6.13) | 5.00 (3.38 - 5.00) | 3.00 (1.00 - 7.00) | |||||
| Chronological age | 65–74 years | 5.17 (4.25 - 6.31) | 0.126 | 6.50 (5.81 - 7.00) | 0.127† | 5.00 (4.25 - 6.00) | 0.005† | 5.63 (1.00 - 7.00) | 0.061† |
| 75–84 years | 4.58 (3.83 - 5.83) | 6.00 (5.00 - 7.00) | 5.00 (4.25 - 5.50) | 4.25 (1.00 - 6.00) | |||||
| 85 years and older | 5.00 (4.75 - 5.56) | 6.00 (5.13 - 6.69) | 3.63 (3.00 - 4.13) | 5.63 (5.13 - 6.00) | |||||
Mann Whitney U test; † Kruskal Wallis test.
Table 3.
Differences in Total MoCa Score According to General Characteristic.
| Variable | Category | MoCA | p-value |
|---|---|---|---|
| Median (interquartile range) | |||
| Gender | Male | 21 (18 - 21) | 0,140* |
| Female | 20 (17 - 20) | ||
| Level of education | Primary school | 19 (16 - 21) | < 0,001† |
| Secondary school | 25 (22 - 27) | ||
| Undergraduate/graduate degree | 25,5 (22,75 - 28) | ||
| Marital status | Married | 22 (19 - 25) | <0,001† |
| Widowed | 18 (16 - 22) | ||
| Divorced | 21 (20 - 21) | ||
| Never married | 19 (14 - 21,50) | ||
| Living arrangement | Living alone | 18 (15 - 22) | <0,001† |
| Nuclear family (spouse) | 21 (18,50 - 25) | ||
| Multigenerational households | 22 (19 - 25) | ||
| Parental status | Yes | 21 (18 - 24) | 0,002* |
| No | 17 (15 - 21) | ||
| Grandparent status | Yes | 20,5 (17,25 - 24) | 0,064* |
| No | 20 (15,5 - 23) | ||
| Chronological age | 65–74 years | 21 (18 - 25) | <0,001† |
| 75–84 years | 18 (16 - 21) | ||
| ≥85 years | 15 (14,25 - 16,75) |
* Mann Whitney U test; † Kruskal Wallis test.
Table 4.
Spearman Correlations Between Perceived Social Support and Total Cognitive Functioning.
| Variable | Total score of MoCA | |
|---|---|---|
| Total score of MSPSS | ρ (p-value) |
0,497 (< 0,001) |
| Family | 0,405 (< 0,001) | |
| Friends | 0,466 (< 0,001) | |
| Significant others | 0,363 (< 0,001) |
ρ - Spearman’s rank-order correlation coefficient.
Table 5.
Differences in Perceived Social Support According to the Cut-off for a Normal MoCA Score.
| Variable | Cognitive Functioning Category | Me (IQR) | p-value* |
|---|---|---|---|
| Total score of MSPSS | Normal | 6,33 (6,00 - 6,67) | < 0,001 |
| Impaired | 4,71 (4,00 - 5,83) | ||
| Family | Normal | 7,00 (7,00 - 7,00) | < 0,001 |
| Impaired | 6,00 (5,25 - 7,00) | ||
| Friends | Normal | 6,00 (5,00 - 6,00) | < 0,001 |
| Impaired | 5,00 (3,81 - 5,25) | ||
| Significant others | Normal | 7,00 (6,00 - 7,00) | < 0,001 |
| Impaired | 5,00 (1,00 - 6,00) |
* Mann Whitney U test.
Table 6.
Multiple Linear Regression of MoCA Total Score on MSPSS Subscale.
| Predictor | Unstandardized B | Standardized ß coefficient | t | p | 95 % Cl |
|---|---|---|---|---|---|
| Intercept | 10.557 | - | 9.449 | < 0.001 | [8.357, 12.756] |
| Family | 0.521 | 0.160 | 2.719 | 0.007 | [0.144, 0.898] |
| Friends | 1.193 | 0.371 | 6.332 | < 0.001 | [0.822, 1.564] |
| Significant others | 0.285 | 0.162 | 2.907 | 0.004 | [0.092, 0.478] |
*β = standardized regression coefficient; R² for the model = 0.290.
Table 7.
Mediation Analysis of Living Arrangement on Cognitive Functioning Through Perceived Social Support.
Table 7.
Mediation Analysis of Living Arrangement on Cognitive Functioning Through Perceived Social Support.
| Effect | Path | ß | SE | 95 % CL | z | p-value |
|---|---|---|---|---|---|---|
| Total | Living arrangement→ MoCa | 0.589 | 0.149 | [0.297,0.881] | 3.954 | < .001 |
| Indirect | Living arrangement→MSSP→MoCa | 0.332 | 0.079 | [0.177,0.487] | 4.196 | < .001 |
| Direct | Living arrangement→ MoCa | 0.258 | 0.138 | [-0.013, 0.528] | 1.867 | 0.062 |
* Living arrangement as a dummy variable (Living alone vs living with others in household); Delta method standard errors, ML estimator.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



