
Submitted:
06 February 2025
Posted:
07 February 2025
You are already at the latest version
Abstract
Background and Purpose: Previous studies have demonstrated the effect of socioeconomic status on the mental or cognitive health in adults. Nevertheless, the effect of specific socioeconomic factors on cognitive function in older people and the mechanism remain to be further investigated. In this study, three specific socioeconomic factors (i.e., income, occupation and education) were used as independent variables, and social support and social participation were used as the parallel or serial mediating variables to investigate the effect on cognitive function in community-dwelling older adults and the specific pathway of influence.
Methods: A cross-sectional study was conducted in the Pudong New District of Shanghai, China. A total of 970 community-dwelling older adults aged over 60 years old were enrolled. Socioeconomic factors in older adults, including income, education level, and occupation before retirement, were investigated, and their cognitive function, social support and social participation levels were measured using the MoCA, MSPSS and the quantity of participation in social activities, respectively. Covariates, including lifestyle, health status, sleep quality, and nutritional status, were assessed using a self-designed questionnaire, the PSQI, and the MNA-SF scale. Omnibus mediation effect analysis was adopted to examine the mediation effect, and the mediation analysis was performed using the SPSS PROCESS program.
Results: The results showed that the higher levels of socioeconomic conditions (income, occupational experience and education) were linked with better cognitive function in community-dwelling older adults; social participation mediated the aforementioned relationship, with the relative indirect effect of income, occupation and education accounting for 18.36%-20.15%, 28.36%-35.64% and 17.14%-39.19% of their total effects, respectively, compared to their low levels; social support only mediated the relationship of income and education with cognitive function, with the indirect effect accounting for 4.21%-6.77% and 5.29%-10.32%, respectively, compared to their low levels. Serial mediation showed that income and education affected social participation through social support and subsequently cognitive function, with the relative indirect effects accounting for 2.0%-3.3% and 2.4%-4.6% of their total effects, respectively, compared to their low levels.
Conclusion: This study demonstrates that social support and social participation independently and cumulatively mediate the relationship between socioeconomic conditions and cognitive function in community-dwelling older adults. The findings provide new insights for the future improvement of cognitive function in community-dwelling older adults in the future.
Keywords:
Socioeconomic factors
; cognitive ability
; older adults
; mediating effect
; social participation
; social support
1. Introduction
With increasing in global life expectancy, the prevalence of dementia or cognitive dysfunction is rising rapidly and is becoming a significant public health problem as a major cause of disability and mortality in the elderly population [1]. According to the 7th census, China has the largest elderly population in the world, with 264 million people over the age of 60, or 18.7% of the total population [2]. Cognitive impairment has become one of the most common mental disorders among older adults in China, with an estimated prevalence of 20.4% [3]. Delaying or preventing cognitive decline is therefore a critical public health issue in an ageing society.
Cognitive function is a key determinant of independence and quality of life in older adults, and healthy cognitive function enables older people to maintain social connections and independent functioning [4,5]. However, cognitive ageing is inevitable, a process of gradual, progressive cognitive decline that occurs with age [6]. Furthermore, cognitive ageing is complex and influenced by as genetics, environment and lifestyle. Genetic factors can’t be controlled, but many environmental factors and lifestyle can be modified or managed, and early and mid-life experiences are linked to cognitive health in later life [7,8].
1.1. Socioeconomic Factors and Cognition
Social determinants of health influence the incidence and prevalence of disease and health inequalities, and are reported to account for 30-55% of health outcomes, even exceeding the contribution of medical factors [9]. Social determinants of health are generally defined as the environmental conditions in which individuals are born, live, learn, work, play and worship, which influence a wide range of health outcomes [10]. A growing body of evidence has shown that the socioeconomic status of social determinants of health is a fundamental determinant of many health outcomes and can influence health outcomes through multiple pathways, such as lifestyle and behaviors, access to health care, environmental exposures, physiological processes, and social cultural and psychological paths [11,12]. It is also important factors influencing the cognitive health of older adults, in which education, income and occupational experience play a key role [13,14]. A cohort study with nearly 30 years of follow-up (from 1985 to 2012) found that socioeconomic disadvantage, including low education and occupational position in midlife, was significantly associated with poorer cognitive function in later life [15]. Another study from a 12-year longitudinal study conducted in Mexican-origin adults also found that the trajectories of socioeconomic levels (i.e., per capita income, economic stress, educational attainment) were robustly associated with cognitive function, and that higher initial levels and greater increases in socioeconomic resources had protective associations with cognitive function [16]. It is widely accepted that part of the effects of socioeconomic conditions on cognition is related to lifestyle differences, as individuals with lower socioeconomic status tend to have poorer dietary quality and more risky health behaviors [17]. Additionally, low socioeconomic status, such as lower levels of education or occupational complexity, may also directly affect cognition through reduced cognitive reserve [18]. However, the precise mechanism is unknown, but it may play a key role through the pathway by which other social factors mediate cognitive function.
1.2. The Mediating Role of Social Participation and Social Support
Social participation is defined as engaging in activities that involve interacting with others in community life [19], and plays a crucial role in the health and well-being of older adults [20] . A growing body of research has shown that positive participation in social activities is helpful in maintaining cognitive function or mitigating cognitive decline in middle-aged and older adults [21,22,23,24], while the poor social participation was significantly associated with increased risk of dementia-related conditions [9].
Social support, which is an individual’s social network of communication with others, is another important social factor [25]. Social support can be divided into four main functions: emotional, informational, friendship and instrumental support, and is recognized as a protective factor against the negative life experiences [26]. The positive impact of social support on health is dominated by a continuous interaction and mutual influence with the social context of the individual, and perceived social support is beneficial in reducing the individual’s negative reactions to stressful experiences, leading to a reduction in the inflammatory response and in turn affecting cognitive function [27,28]. The longitudinal studies have also shown that the perceived social support from family members or friends can positively promote cognitive health in older adults [29,30].
Although socioeconomic factors, such as low income, unemployment, and low educational attainment, were negatively associated with cognitive function. Positive participation in social activities and better social support may increase mental stimulation and synaptic density and neuronal growth, promote social integration, and improve one’s social capital and healthy behaviours, which in turn may promote better cognition [31,32,33]. It is therefore possible that they mediate the effect of socioeconomic factors on cognitive function in older adults.
1.3. The Conceptual Model of Present Study
In the current study of cognitive function, socioeconomic factors, social participation and social support are seen as parallel or serial factors that independently or interactively affect cognitive function in the community-dwelling elderly population. The aim of this study was to explore how and under which behavioral conditions socioeconomic factors affect cognitive function in community-dwelling older adults, and to inspire young adults to change their behaviors to protect their cognitive function in later life, by investigating the parallel and serial mediation models (Figure 1).
In terms of parallel mediation, the following main hypotheses were examined:
1. Socioeconomic conditions (income, occupation and education) are directly associated with cognitive function (i.e., high levels of socioeconomic conditions are directly positively associated with high levels of cognitive function in community-dwelling older adults (H1)).
2. Social support mediates the relationship between socioeconomic factors and cognitive function (i.e., high levels of socioeconomic conditions are significantly associated with high levels of social support (H2), which are significantly associated with high levels of cognitive function (H5)).
3. Social participation mediates the relationship between socioeconomic factors and cognitive function (i.e., high levels of socioeconomic conditions are significantly associated with high levels of social participation (H3), which are significantly associated with high levels of cognitive function (H6).
In this mediation model, it is hypothesized that two mediating variables independently affect the association of socioeconomic factors with cognitive function. For the indirect effects of socioeconomic factors on cognitive function, higher levels of socioeconomic conditions are associated with higher levels of social support or social participation, which in turn are associated with higher levels of cognitive function.
In terms of serial mediation, it is hypothesized that two mediating variables affect sequentially, and the following hypothesis is provided:
4. Social support mediates the relationship between socioeconomic conditions and cognitive function, which in turn is mediated by social participation (i.e., high levels of socioeconomic conditions lead to high levels of social support, which in turn lead to high levels of social participation, and ultimately lead to high levels of cognitive function (path from H2, H4, to H6)).
2. Methods
2.1. Participants and Procedures
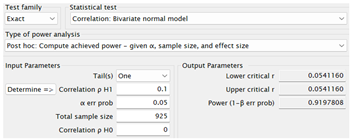
1000 community-dwelling older adults were recruited from the community in Shanghai, China, by the convenience sampling method. They were eligible to participate in the study if they were: aged 60 years or older; had lived in their current location for more than 5 years; and gave informed consent. After obtaining informed consent from community-dwelling older adults, a face-to-face survey was conducted to collect the variable information. Data collection was completed between 1 December 2022 and 1 May 2023. A total of 979 eligible older adults were identified by excluding 21 participants who refused to cooperate with the completion of the investigation. The procedures in this study adhered to the Declaration of Helsinki and were approved by the Ethics Committee of author’s institution (No. 2022-ZGH-013). A post-hoc power analysis was conducted using G*power 3.1 to assess the current effective sample size for correlation analysis. With a total sample size of 925 participants, a significant level of α=0.05, and an effect size of r=0.1, the statistical power reached 0.92 [34].
2.2. Measures
2.2.1. Cognitive Function
Cognitive function of the participants was assessed using the Montreal Cognitive Assessment (MoCA) scale (Beijing version). The MoCA scale consists of eight sub-dimensions of cognitive function, each of which assesses respectively the visuospatial/executive function, naming, memory, attention, verbal fluency, abstraction, delayed recall and orientation. The maximum score on the MoCA scale is 30 points, with the higher scores indicating better cognitive functioning [35].
2.2.2. Socioeconomic Factors
The socioeconomic factors in this study were mainly involved three socioeconomic variables (i.e., education, income and occupational experience before retirement). To reflect the lifetime exposure of community-dwelling older individuals to socioeconomic conditions, the income, education and occupational exposure of each participant in this study were identified as the retirement pension, education and training experience, and occupational complexity before retirement. Due to the well-established pension insurance system in Shanghai, China, most of the community-dwelling retirement older adults in Shanghai had a fixed pension, and the retirement pension is generally calculated on the basis of the individual’s social pension contributions paid during his or her working life, and the individual’s pension contributions are positively proportional to his or her wage income. For this reason, the retirement pension can be used as an indicator for the assessment of the income level of the elderly before their retirement. Taking into account the situation of Shanghai retirement pension, the income level of participants was divided into 3 categories: 2000 RMB and below per month as low level, 2000-6000 RMB per month as medium level, AND more than 6000 RMB per month as high level. The educational level in this study was assessed by a combined score of years of formal education and vocational or training courses, in which each year of primary, secondary and high school was assigned 1 point if successfully completed, and the vocational or training course was assigned 0.5 points for each 6-month course. The educational level of participants was categorized as low, medium or high according to the total education scores using the tertile principle. Occupational exposures included the type and years of work in adulthood occupations before retirement, and work activities were categorized into six levels according to the type of work: low-skilled manual work, skilled manual work, skilled non-manual or technical work, professional work, and highly intellectual work. The scores for occupational complexity were calculated as the product of the level and the years of work activity in adulthood. Occupational levels were divided into three classes according to the total occupational scores, namely, low, medium and high, based on the tertile principle [36].
2.2.3. Social participation and social support
Social participation was defined as recent participation in any social activity. It includes five types of activities and is scored on a 4-point scale, with “not participating” scored as 1, “not regularly (about once a month)” scored as 2, “sometimes (about every week)” scored as 3, “often (almost daily)” scored as 4; higher scores indicate higher levels of participation [37].
Social support was assessed using the Multidimensional Scale of Perceived Social Support (MSPSS), which consists of 12 items assessing perceptions of social support from family, friends and significant other sources, and each item is scored from 1 to 7 according to the degree of agreement (very strongly disagree = 1, strongly disagree = 2, mildly disagree = 3, neutral = 4, mildly agree = 5, strongly agree = 6, very strongly agree = 7), with higher total scores indicating greater social support [38].
2.2.4. Covariates
Participants’ demographic characteristics (e.g., age, sex, height, weight, marital status, place of residence), lifestyle (e.g., smoking, drinking), and health status (e.g., chronic diseases) were assessed using a self-designed questionnaire. The body mass index (BMI) was calculated as body weight (kg) divided by the square of height (m). Sleep quality was assessed using the Chinese version of the Pittsburgh Sleep Quality Index (PSQI) [39]. Nutrition status was assessed using the Chinese version of Mini Nutritional Assessment Short Form (MNA-SF) [40]. The definition and assignment of the variables are shown in Table 1.
2.3. Statistical Analysis
IBM SPSS Statistics software (version 25) was used for all the statistical analyses, and the difference was considered statistically significant with a 95% confidence interval (95% CI) or P<0.05 on both sides. The missing data were imputed using Markov Chain Monte Carlo (MCMC) multiple imputation. Descriptive statistics were expressed as the means and standard deviations (SDs) for the continuous variables and frequencies and percentages for categorical variables. Independent samples t-test or F-test was used to identify covariates that may be related to cognitive function by comparing the difference in cognitive function between different characteristics/levels of covariates. Pearson correlation coefficients were used to assess the relationship between cognitive function and social participation and social support. The SPSS macro PROCESS 4.1 plugin was employed to conduct a mediated analysis [41]. The Model 4 and Model 6 were respectively used to examine the parallel or serial mediation effect of social participation and social support between socioeconomic factors and cognitive function. Considering that the three independent variables were multi-categorical variables, the omnibus mediation effect analysis based on the research results of Preacher and Hayes was performed before the mediation effect analysis [42]. The k dummy variables were set for each multi-categorical independent variable, and k-1 relative direct and relative indirect effects compared to reference level were estimated (Figure 2). If the omnibus effect was not significant, it means that the potential mediating effect did not exist and the medicating effect analysis was not performed. k dummy variables were set for each multi-categorical independent variable, and the k-1 direct and indirect effects were estimated as the k-1 relative mediation effect. The bootstrap method with a sample size of 5000 was used to examine the mediating effect. All tests were within the 95% confidence interval (95% CI). If the interval of 95% CI did not include zero, it indicated that the mediating or moderating effect was significant at the 0.05 level.
3. Results
3.1. Analysis for Common Method Bias
The Harman single-factor test with the untwisted principal component factor mothed was used to analyze the potential common method bias for all variables in the current data. The results showed that the first factor explained 14.2% of the variance, indicating that there was no obvious common method bias in the current research data.
3.2. Descriptive Statistics and Correlation Analysis for the Study Variables
The samples consisted of 979 community-dwelling older adults aged over 60 years old recruited from the residential area of Pudong district in Shanghai, China. Table 2 shows the comparison of cognitive function in different characteristics of demographic, independent and covariate variables among participants. There were significant differences in MoCA scores between different levels of participants’ income, occupation and education (all P<0.01). Age, marital status, smoking, drinking, nutritional status and sleep quality significantly affected the participants’ cognitive function (all P<0.05). Correlation analysis showed that social participation and social support was positively correlated with cognitive function (Table 3).
3.3. Mediation Effect Analysis
3.3.1. Omnibus Mediation Effect Analysis
The analysis of the omnibus effect after controlling for the older adult’s age, marital status, smoking, drinking, nutrition status and sleep quality is shown in Table 4. When cognitive function was taken as the dependent variable and socioeconomic factors (income, occupation and education) as the independent variables, regardless of whether the social participation or social support was taken as the mediating variable, all of the omnibus total effect tests and the omnibus direct effect tests were significant (all P<0.05), indicating that at least one of the relative total effects and relative direct effects there was not equal to 0. The bootstrap 95% CI of all of the omnibus mediation effect tests was not included 0, indicating that further relative mediation effect analysis was need.
3.3.2. Relative Mediation Effect of Social Participation or Social Support
Based on the result of the omnibus effect analysis, the relative total effect test and the relative mediation effect test were carried out (Figure 3 and Supplementary table 1). As shown in Table 5, in terms of mediation effects through social participation, there is a significant relative mediation effect of income, occupation and education level on cognitive function through social participation. Compared with the low-income group (retirement pension <2000 yuan/month), older adults with medium or high income were more likely to improve their cognitive function through social participation. The relative mediation effect accounted for 18.36% (aib=0.358, 95%CI:0.110~0.614) and 20.45% (aib=0.777, 95%CI:0.349~1.222) of the relative total effect, respectively, indicating that 18.36% and 20.45% of the improvement in cognitive function among middle- and high-income older adults was mediated by social participation. Compared to those with low occupational experience (occupational scores <53), older adults with more complex occupational experience could improve their cognitive function through more social participation. Among the older adults with medium or high level of occupational experience, 28.36% (aib=0.358, 95%CI:0.123~0.614) and 35.64% (aib=0.561, 95%CI:0.299~0.851) of the improvement in cognitive function was mediated by social participation, and the relative mediation effect increased with the level of occupational experience promoted. Older adults with higher levels of education had better cognitive function than those with low levels of education, partly mediated by their social participation. The proportion of relative mediation effect was 17.14% (aib=0.311, 95%CI:0.058~0.572) for medium education and 39.19% (aib=0.562, 95%CI:0.294~0.851) for high education.
For the social support mediation model, there was a significant relative mediation effect of income and education level on cognitive function through social support. Specifically, compared with the low income group, the older adults with medium or high income had better cognitive function, in which the proportion of relative mediation effect of social support was 6.77% (aib=0.132, 95%CI:0.019~0.282) and 4.21% (aib=0.160, 95%CI:0.017~0.372), respectively; compared with the low educational level, the older adults with medium or high educational level were more likely to improve their cognitive function by social support, and the proportion of relative mediation effect was 5.29% (aib=0.096, 95%CI:0.013~0.214) and 10.32% (aib=0.156, 95%CI:0.035~0.318), respectively.
3.3.3. Relative Seral Mediating Effect of Social Support And Social Participation
The examined serial mediating effect of social support and social participation on socioeconomic factors on cognitive function is expressed in Figure 4 and Supplementary table 2. Table 6 show the relative direct effect of each independent and mediating variables in the serial mediation model after controlling for the older adult’s age, marital status, nutrition status and sleep quality. In the model of the relation between income or education and cognitive function, all of the direct effects were all significant except for the social support for cognitive function. In the model of relationship between occupation and cognitive function, medium or high occupation level was not found to have significant direct effect on social support compared with low occupation level; social support was not found to have significant direct effect on cognitive function.
Table 7 shows the indirect effect of socioeconomic conditions (e.g., income, occupation, education), social support, social participation, and cognitive function after controlling for the older adult’s age, marital status, smoking, drinking, nutrition status and sleep quality. As shown in Table 7, in the model from income to cognitive function, compared with low income level, the medium and high income level affected cognitive function through social participation by β=0.287 (95CI:0.042~0.539), and 0.685 (95CI:0.261~1.136), accounting for 14.7% and 18.0% of the total effect, respectively; and through social support and then social participation (i.e., seral mediation effect) (β=0.065, 95% CI 0.025~0.115; β=0.078, 95% CI 0.023~0.152), explaining 3.3% and 2.0% of the total effect, respectively. But the mediating effect through social support was not significant. These results suggest that the indirect effect of the medium or high income on cognitive function through social support is completely mediated by social participation.
In the model from occupation to cognitive function, compared to low level of occupation complexity, social participation mediated the association between medium and high level of occupational complexity and cognitive function with β=0.344 (95% CI 0.117~0.591) and β=0.531 (95% CI 0.277~0.824), accounting for 27.3% and 33.7% of the total effect, respectively. There was no significant mediation effect through social support and no serial mediation effect (first through social support, then through social participation) on the association between medium and high level of occupational complexity and cognitive function.
In the model from education to cognitive function, compared with low educational level, medium and high educational level affected cognitive function through social participation with β=0.262 (95CI: 0.020~0.515), and 0.480 (95CI: 0.224~0.761), explaining 14.4% and 31.8% of the total effect; and through serial mediation (first through social support, then through social participation) with β=0.065 (95% CI 0.025~0.115) and β=0.078 (95% CI 0.023~0.152), explaining 2.4% and 4.6% of the total effect, respectively; no significant mediating effect was found through social support.
4. Discussion
This study aimed to examine the interplay between socioeconomic conditions, social participation and social support on cognitive function by investigating the parallel and serial mediating role of social support and social participation in the relationship between socioeconomic factors and cognitive function. Current study revealed three important findings. First, an individual’s socioeconomic level, including income, education and occupational exposure in their adulthood were positively associated with the cognitive function. Second, the social participation significantly mediated the association between socioeconomic conditions and cognitive function, and high levels of social participation may enhance the effect of socioeconomic factors on cognitive function in community-dwelling older adults; social support significantly mediated the income and education on cognitive function, and social support positively strengthens the effect of income and education on cognitive function in community-dwelling older adults. Third, social participation completely mediated the effect of the socioeconomic factors (income and education) on cognitive function through social support (i.e., the indirect effect of income and education on cognitive function through social support is completely mediated by social participation.).
This study confirmed that an individual’s socioeconomic conditions are positively associated with cognitive function; in other words, the higher the level of income, education or occupational experience, the higher cognitive function in community-dwelling older people, which is in line with current accepted opinion[43,44]. A growing body of research, using sophisticated behavioral and neuroimaging measures, has demonstrated the causal linkages between these socioeconomic factors and specific cognitive functions [45,46]. Higher socioeconomic conditions across life stages were independently and cumulatively associated with better neural or cognitive outcomes, as reflected by increased cortical thickness, grey matter volume, fractional anisotropy and network segregation in adult individuals [47,48]. The economic viewpoint suggests that individuals with greater economic resources were better able to purchase important products related to cognitive or brain development, such as nutritious foods, enriching learning opportunities, etc [49]. The evidence shows that educational attainment has a positive effect on cognitive function, and that the number of years of formal education completed by individuals is positively correlated with their cognitive function in adulthood and is predictive of a lower risk of dementia in later life, and that educational attainment influences cognitive function in later life primarily by contributing to individual differences in cognitive ability that emerge in early adulthood but persist into old age [50]. Adult work experience, as a general mentally stimulating activity, was found to be able to affect cognitive function in later life, and more complex adult work activities were associated with better cognitive function in later life [51,52]. The complex work activities stimulate higher mental or intellectual demands in connection with specific cognitive processes[53,54].
Second, this study roughly validated the hypothesis that social participation and social support independently mediate the effect of socioeconomic condition on cognitive function in community-dwelling older people. Specifically, when social participation was the mediating variable, it mediated about 18-20%, 28-35%, and 17-39% of the differences in cognitive function due to income inequality and education and occupation gaps. Moreover, the greater the difference between levels of socioeconomic condition, the stronger the mediating effect of social participation. Social participation, such as good and cordial relations with family, relatives and friends, are the main sources and the most important factors of life satisfaction and happiness of individuals, which are indirectly beneficial for cognitive function [55]. Although poor socioeconomic conditions can affect an individual’s physical, mental and cognitive health by limiting access to needs and opportunities [56], positive social participation could at least partially offset these negative effects of socioeconomic inequalities [57]. Existing studies have showed that the socioeconomic gap can indeed have a significant effect on the physical and mental health of older people, but that this effect may be partly explained by the mediating effect of social participation [58,59].
When social support was the mediating variable, we found that the weak mediating effect of social support on the association between income and education of socioeconomic conditions and cognitive function in community-dwelling older adults. More specifically, social support mediated about 4.2-6.8% and 5.3-10.3% of the disparity in cognitive function due to the income or education gap, with the larger the income or education gap, the higher the proportion of mediation; no significant mediating effect of social support on the association between the occupational complexity and cognitive function was found. Social support, as part of a social network of mutual help and obligation, is one of the active ingredients in the health benefits of connectedness [60], and the proposed neural mechanism is related to enhancing ventral striatum and septal area activity and inhibiting parental care (e.g., amygdala), which is linked to downstream stress-related responses [61]. One study has reported that social support, including informational, instrumental and financial support, is an effective buffer against the negative effects of poverty on mental health [62]. Another study also found significant differences in the cognitive benefits of receiving support from family or friends among older adults with different educational levels [63]. These findings were similar to the results of this study.
Finally, this study confirmed that social participation can mediate the role of income, education and social support in promoting cognitive function in community-dwelling older adults. We found that high levels of income and education were associated with high levels of social support, which led to high levels of social participation and improved cognitive function. However, when mediated by social participation, there was no significant effect of social support on cognitive function. These results suggest that the partial effects of high levels of income and education on cognitive function are due to high levels of social support and social participation, and that the effect of social support on cognitive function is entirely due to the mediation of social participation. Socioeconomic status, such as income and education levels, is an important cause of the unequal distribution of social support, and individuals with lower socioeconomic status have smaller social networks and less organizational involvement [64,65]. Therefore, socioeconomic level affected to some extent an individual’s access to social support, which in turn affected an individual’s social participation. Given that positive social support and social participation have a positive relationship with cognitive function, increasing these types of social connections may promote cognitive function in older adults, also offsetting the negative effect of low socioeconomic conditions on cognitive function[31]. Moreover, social participation may be more beneficial than social support in buffering this decline; social participation may optimize an individual’s social network, which facilitates only high-quality social interactions, and may be an important facet influencing well-being [66].
In terms of application, the findings of this study may be reflected in an individual’s ability to manage the cognitive ageing process. Social support and social participation may be considered as behavioral tools to help older adults cope with cognitive changes resulting from socioeconomic inequality in adulthood, and social participation could be more effective in helping facilitate cognitive function. For the community-dwelling older adults, improving their social support network may increase their opportunities to participate in community activities, and may be helpful in promoting their cognitive health and offsetting the negative effects of socioeconomic inequality in their adulthood.
There are several limitations to this study. First, the cross-sectional design of this study limits the ability to draw conclusions about causality. Therefore, future research should strengthen these findings by using a longitudinal design. Second, this study investigated the social support and social participation of older adults in their later years. Therefore, the results may not account for the long-term effects of social support and social participation on cognitive function. Third, the information on socioeconomic factors is self-reported, so the possibility of misclassification bias may not be excluded. Finally, the information on the controlled confounders only reflects the conditions at the time of the investigation and not at the time of exposed, which could influence the results. Despite the limitations mentioned above, our findings may have relevant public health implications. First, our findings suggest the importance of assessing socioeconomic conditions when investigating risk factors for cognitive impairment, even from a life course perspective. Second, as social support and social participation may effectively mediate the impacts of socioeconomic factors on cognitive function, improving social support networks or actively participating in social activities may be an effective intervention to prevent cognitive decline in older adults.
5. Conclusion
The results showed that socioeconomic factors can directly and indirectly affect the cognitive function in community-dwelling older adults, and that social support and social participation, alone or in combination, mediate the effect of socioeconomic conditions on cognitive function. These findings provide some insights into the potential pathways between socioeconomic conditions and cognitive function, as well as the protective role of social support and social participation in community-dwelling older adults.
Author Contributions
Z.G.H have designed an overall research and investigation plan. Z.Y, Y.M.Z, W.T.T and G.H.N conduct surveys to obtain data. Z.Y.L completed the data analysis and wrote the manuscript.
Funding
No sources of funding.
Ethics approval and consent to participate
The study was approved by the health research ethics committee of the Shanghai University of Medicine and Health Sciences. Each participant gave a written informed consent
Consent for publication
Not applicable.
Availability of data and materials
Data are available from the corresponding author upon reasonable request.
Acknowledgments
The authors are grateful to the Zhouxing community for providing the survey sites.
Competing interests
The authors declare no competing interests.
References
- Mobaderi T, Kazemnejad A, Salehi M. Exploring the impacts of risk factors on mortality patterns of global Alzheimer's disease and related dementias from 1990 to 2021. Sci Rep. 2024;14(1):15583. [CrossRef]
- Tu WJ, Zeng X, Liu Q. Aging tsunami coming: the main finding from China's seventh national population census. Aging clinical and experimental research. 2022;34(5):1159-63. [CrossRef]
- Yuan L, Zhang X, Guo N, Li Z, Lv D, Wang H, et al. Prevalence of cognitive impairment in Chinese older inpatients and its relationship with 1-year adverse health outcomes: a multi-center cohort study. BMC Geriatr. 2021;21(1):595. [CrossRef]
- Cigolle CT, Langa KM, Kabeto MU, Tian Z, Blaum CS. Geriatric conditions and disability: the Health and Retirement Study. Ann Intern Med. 2007;147(3):156-64. [CrossRef]
- Rivas-Sucari HC, Rodríguez-Eguizabal JL. Cognitive health in older adults, a public health challenge. Gaceta medica de Mexico. 2024;160(2):223-4. [CrossRef]
- Cox SR, Deary IJ. Brain and cognitive ageing: The present, and some predictions (…about the future). Aging brain. 2022;2:100032. [CrossRef]
- Oosterhuis EJ, Slade K, May PJC, Nuttall HE. Toward an Understanding of Healthy Cognitive Aging: The Importance of Lifestyle in Cognitive Reserve and the Scaffolding Theory of Aging and Cognition. J Gerontol B Psychol Sci Soc Sci. 2023;78(5):777-88. [CrossRef]
- Reuter-Lorenz PA, Park DC. Cognitive aging and the life course: A new look at the Scaffolding theory. Current opinion in psychology. 2024;56:101781. [CrossRef]
- Joshi P, Hendrie K, Jester DJ, Dasarathy D, Lavretsky H, Ku BS, et al. Social connections as determinants of cognitive health and as targets for social interventions in persons with or at risk of Alzheimer's disease and related disorders: a scoping review. International psychogeriatrics. 2024;36(2):92-118. [CrossRef]
- Honeycutt AA, Khavjou OA, Tayebali Z, Dempsey M, Glasgow L, Hacker K. Cost-Effectiveness of Social Determinants of Health Interventions: Evaluating Multisector Community Partnerships' Efforts. Am J Prev Med. 2024. [CrossRef]
- Chen E, Miller GE. Socioeconomic status and health: mediating and moderating factors. Annual review of clinical psychology. 2013;9:723-49. [CrossRef]
- Braveman P, Gottlieb L. The social determinants of health: it's time to consider the causes of the causes. Public health reports (Washington, DC : 1974). 2014;129 Suppl 2(Suppl 2):19-31. [CrossRef]
- Jester DJ, Kohn JN, Tibiriçá L, Thomas ML, Brown LL, Murphy JD, et al. Differences in Social Determinants of Health Underlie Racial/Ethnic Disparities in Psychological Health and Well-Being: Study of 11,143 Older Adults. The American journal of psychiatry. 2023;180(7):483-94. [CrossRef]
- Crear-Perry J, Correa-de-Araujo R, Lewis Johnson T, McLemore MR, Neilson E, Wallace M. Social and Structural Determinants of Health Inequities in Maternal Health. Journal of women's health (2002). 2021;30(2):230-5. [CrossRef]
- Rusmaully J, Dugravot A, Moatti JP, Marmot MG, Elbaz A, Kivimaki M, et al. Contribution of cognitive performance and cognitive decline to associations between socioeconomic factors and dementia: A cohort study. PLoS medicine. 2017;14(6):e1002334. [CrossRef]
- Lawson KM, Sutin AR, Atherton OE, Robins RW. Are trajectories of personality and socioeconomic factors prospectively associated with midlife cognitive function? Findings from a 12-year longitudinal study of Mexican-origin adults. Psychology and aging. 2023;38(8):749-62. [CrossRef]
- Clarke AJ, Brodtmann A, Irish M, Mowszowski L, Radford K, Naismith SL, et al. Risk factors for the neurodegenerative dementias in the Western Pacific region. The Lancet regional health Western Pacific. 2024;50:101051. [CrossRef]
- Chapko D, McCormack R, Black C, Staff R, Murray A. Life-course determinants of cognitive reserve (CR) in cognitive aging and dementia - a systematic literature review. Aging Ment Health. 2018;22(8):915-26. [CrossRef]
- Levasseur M, Lussier-Therrien M, Biron ML, Raymond É, Castonguay J, Naud D, et al. Scoping study of definitions of social participation: update and co-construction of an interdisciplinary consensual definition. Age Ageing. 2022;51(2). [CrossRef]
- Zhang H, Hao X, Qin Y, Yang Y, Zhao X, Wu S, et al. Social participation classification and activities in association with health outcomes among older adults: Results from a scoping review. J Adv Nurs. 2024. [CrossRef]
- Tomioka K, Kurumatani N, Hosoi H. Social Participation and Cognitive Decline Among Community-dwelling Older Adults: A Community-based Longitudinal Study. J Gerontol B Psychol Sci Soc Sci. 2018;73(5):799-806. [CrossRef]
- Cunha C, Rodrigues P, Voss G, Martinez-Pecino R, Delerue-Matos A. Association between formal social participation and cognitive function in middle-aged and older adults: a longitudinal study using SHARE data. Neuropsychology, development, and cognition Section B, Aging, neuropsychology and cognition. 2024;31(5):932-55. [CrossRef]
- Hou J, Chen T, Yu NX. The Longitudinal Dyadic Associations Between Social Participation and Cognitive Function in Older Chinese Couples. J Gerontol B Psychol Sci Soc Sci. 2024;79(6). [CrossRef]
- Li H, Li C, Wang A, Qi Y, Feng W, Hou C, et al. Associations between social and intellectual activities with cognitive trajectories in Chinese middle-aged and older adults: a nationally representative cohort study. Alzheimers Res Ther. 2020;12(1):115. [CrossRef]
- Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychological bulletin. 1985;98(2):310-57.
- Lu S, Wu Y, Mao Z, Liang X. Association of Formal and Informal Social Support With Health-Related Quality of Life Among Chinese Rural Elders. Int J Environ Res Public Health. 2020;17(4). [CrossRef]
- Gellert P, Häusler A, Suhr R, Gholami M, Rapp M, Kuhlmey A, et al. Testing the stress-buffering hypothesis of social support in couples coping with early-stage dementia. PLoS One. 2018;13(1):e0189849. [CrossRef]
- McHugh Power J, Carney S, Hannigan C, Brennan S, Wolfe H, Lynch M, et al. Systemic inflammatory markers and sources of social support among older adults in the Memory Research Unit cohort. Journal of health psychology. 2019;24(3):397-406. [CrossRef]
- Gui S, Wang J, Li Q, Chen H, Jiang Z, Hu J, et al. Sources of perceived social support and cognitive function among older adults: a longitudinal study in rural China. Frontiers in aging neuroscience. 2024;16:1443689. [CrossRef]
- Du C, Dong X, Katz B, Li M. Source of perceived social support and cognitive change: an 8-year prospective cohort study. Aging Ment Health. 2023;27(8):1496-505. [CrossRef]
- Smith L, Shin JI, López Sánchez GF, Oh H, Kostev K, Jacob L, et al. Social participation and mild cognitive impairment in low- and middle-income countries. Preventive medicine. 2022;164:107230. [CrossRef]
- Chanda S, Mishra R. Impact of transition in work status and social participation on cognitive performance among elderly in India. BMC Geriatr. 2019;19(1):251. [CrossRef]
- Chiao, C. Beyond health care: Volunteer work, social participation, and late-life general cognitive status in Taiwan. Social science & medicine (1982). 2019;229:154-60. [CrossRef]
- Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behavior research methods. 2009;41(4):1149-60. [CrossRef]
- Hong Y, Zeng X, Zhu CW, Neugroschl J, Aloysi A, Sano M, et al. Evaluating the Beijing Version of Montreal Cognitive Assessment for Identification of Cognitive Impairment in Monolingual Chinese American Older Adults. J Geriatr Psychiatry Neurol. 2022;35(4):586-93. [CrossRef]
- Cao T, Zhang S, Yu M, Zhao X, Wan Q. The Chinese Translation Study of the Cognitive Reserve Index Questionnaire. Front Psychol. 2022;13:948740. [CrossRef]
- Wang Y, Chen Z, Zhou C. Social engagement and physical frailty in later life: does marital status matter? BMC Geriatr. 2021;21(1):248. [CrossRef]
- Zhou K, Li H, Wei X, Yin J, Liang P, Zhang H, et al. Reliability and validity of the multidimensional scale of perceived social support in Chinese mainland patients with methadone maintenance treatment. Comprehensive psychiatry. 2015;60:182-8. [CrossRef]
- Zhang C, Zhang H, Zhao M, Li Z, Cook CE, Buysse DJ, et al. Reliability, Validity, and Factor Structure of Pittsburgh Sleep Quality Index in Community-Based Centenarians. Front Psychiatry. 2020;11:573530. [CrossRef]
- Kaiser MJ, Bauer JM, Ramsch C, Uter W, Guigoz Y, Cederholm T, et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): a practical tool for identification of nutritional status. The journal of nutrition, health & aging. 2009;13(9):782-8. [CrossRef]
- The PROCESS macro for SPSS, SAS, and R. PROCESS macro for SPSS and SAS.
- Hayes AF, Preacher KJ. Statistical mediation analysis with a multicategorical independent variable. The British journal of mathematical and statistical psychology. 2014;67(3):451-70. [CrossRef]
- Duncan GJ, Magnuson K. Socioeconomic status and cognitive functioning: moving from correlation to causation. Wiley interdisciplinary reviews Cognitive science. 2012;3(3):377-86. [CrossRef]
- Marengoni A, Fratiglioni L, Bandinelli S, Ferrucci L. Socioeconomic status during lifetime and cognitive impairment no-dementia in late life: the population-based aging in the Chianti Area (InCHIANTI) Study. J Alzheimers Dis. 2011;24(3):559-68. [CrossRef]
- Rakesh D, Whittle S. Socioeconomic status and the developing brain - A systematic review of neuroimaging findings in youth. Neurosci Biobehav Rev. 2021;130:379-407. [CrossRef]
- Isbell E, Rodas De León NE, Richardson DM. Childhood family socioeconomic status is linked to adult brain electrophysiology. PLoS One. 2024;19(8):e0307406. [CrossRef]
- Thanaraju A, Marzuki AA, Chan JK, Wong KY, Phon-Amnuaisuk P, Vafa S, et al. Structural and functional brain correlates of socioeconomic status across the life span: A systematic review. Neurosci Biobehav Rev. 2024;162:105716. [CrossRef]
- Thomas MSC, Coecke S. Associations between Socioeconomic Status, Cognition, and Brain Structure: Evaluating Potential Causal Pathways Through Mechanistic Models of Development. Cognitive science. 2023;47(1):e13217. [CrossRef]
- Osler M, Avlund K, Mortensen EL. Socio-economic position early in life, cognitive development and cognitive change from young adulthood to middle age. European journal of public health. 2013;23(6):974-80. [CrossRef]
- Lövdén M, Fratiglioni L, Glymour MM, Lindenberger U, Tucker-Drob EM. Education and Cognitive Functioning Across the Life Span. Psychological science in the public interest : a journal of the American Psychological Society. 2020;21(1):6-41. [CrossRef]
- Fujishiro K, MacDonald LA, Crowe M, McClure LA, Howard VJ, Wadley VG. The Role of Occupation in Explaining Cognitive Functioning in Later Life: Education and Occupational Complexity in a U.S. National Sample of Black and White Men and Women. J Gerontol B Psychol Sci Soc Sci. 2019;74(7):1189-99. [CrossRef]
- Kivimäki M, Walker KA, Pentti J, Nyberg ST, Mars N, Vahtera J, et al. Cognitive stimulation in the workplace, plasma proteins, and risk of dementia: three analyses of population cohort studies. BMJ (Clinical research ed). 2021;374:n1804. [CrossRef]
- Boots EA, Schultz SA, Almeida RP, Oh JM, Koscik RL, Dowling MN, et al. Occupational Complexity and Cognitive Reserve in a Middle-Aged Cohort at Risk for Alzheimer's Disease. Arch Clin Neuropsychol. 2015;30(7):634-42. [CrossRef]
- Rydström A, Darin-Mattsson A, Kåreholt I, Ngandu T, Lehtisalo J, Solomon A, et al. Occupational complexity and cognition in the FINGER multidomain intervention trial. Alzheimers Dement. 2022;18(12):2438-47. [CrossRef]
- Azizi M, Mohamadian F, Ghajarieah M, Direkvand-Moghadam A. The Effect of Individual Factors, Socioeconomic and Social Participation on Individual Happiness: A Cross-Sectional Study. Journal of clinical and diagnostic research : JCDR. 2017;11(6):Vc01-vc4. [CrossRef]
- Barakat C, Konstantinidis T. A Review of the Relationship between Socioeconomic Status Change and Health. Int J Environ Res Public Health. 2023;20(13). [CrossRef]
- Ashida T, Kondo N, Kondo K. Social participation and the onset of functional disability by socioeconomic status and activity type: The JAGES cohort study. Preventive medicine. 2016;89:121-8. [CrossRef]
- Zhang Y, Su D, Chen Y, Tan M, Chen X. Effect of socioeconomic status on the physical and mental health of the elderly: the mediating effect of social participation. BMC Public Health. 2022;22(1):605. [CrossRef]
- Achdut N, Sarid O. Socio-economic status, self-rated health and mental health: the mediation effect of social participation on early-late midlife and older adults. Israel journal of health policy research. 2020;9(1):4. [CrossRef]
- Uchino, BN. Social support and health: a review of physiological processes potentially underlying links to disease outcomes. Journal of behavioral medicine. 2006;29(4):377-87. [CrossRef]
- Inagaki, TK. Neural mechanisms of the link between giving social support and health. Annals of the New York Academy of Sciences. 2018;1428(1):33-50. [CrossRef]
- Chang Q, Peng C, Guo Y, Cai Z, Yip PSF. Mechanisms connecting objective and subjective poverty to mental health: Serial mediation roles of negative life events and social support. Social science & medicine (1982). 2020;265:113308. [CrossRef]
- Moorman SM, Pai M. Social Support From Family and Friends, Educational Attainment, and Cognitive Function. J Appl Gerontol. 2024;43(4):396-401. [CrossRef]
- Adkins-Jackson PB, George KM, Besser LM, Hyun J, Lamar M, Hill-Jarrett TG, et al. The structural and social determinants of Alzheimer's disease related dementias. Alzheimers Dement. 2023;19(7):3171-85. [CrossRef]
- Wilding A, Munford L, Sutton M. Estimating the heterogeneous health and well-being returns to social participation. Health economics. 2023;32(9):1921-40. [CrossRef]
- Sharifian N, Grühn D. The Differential Impact of Social Participation and Social Support on Psychological Well-Being: Evidence From the Wisconsin Longitudinal Study. International journal of aging & human development. 2019;88(2):107-26. [CrossRef]
Figure 1.
The theoretical framework of the study.
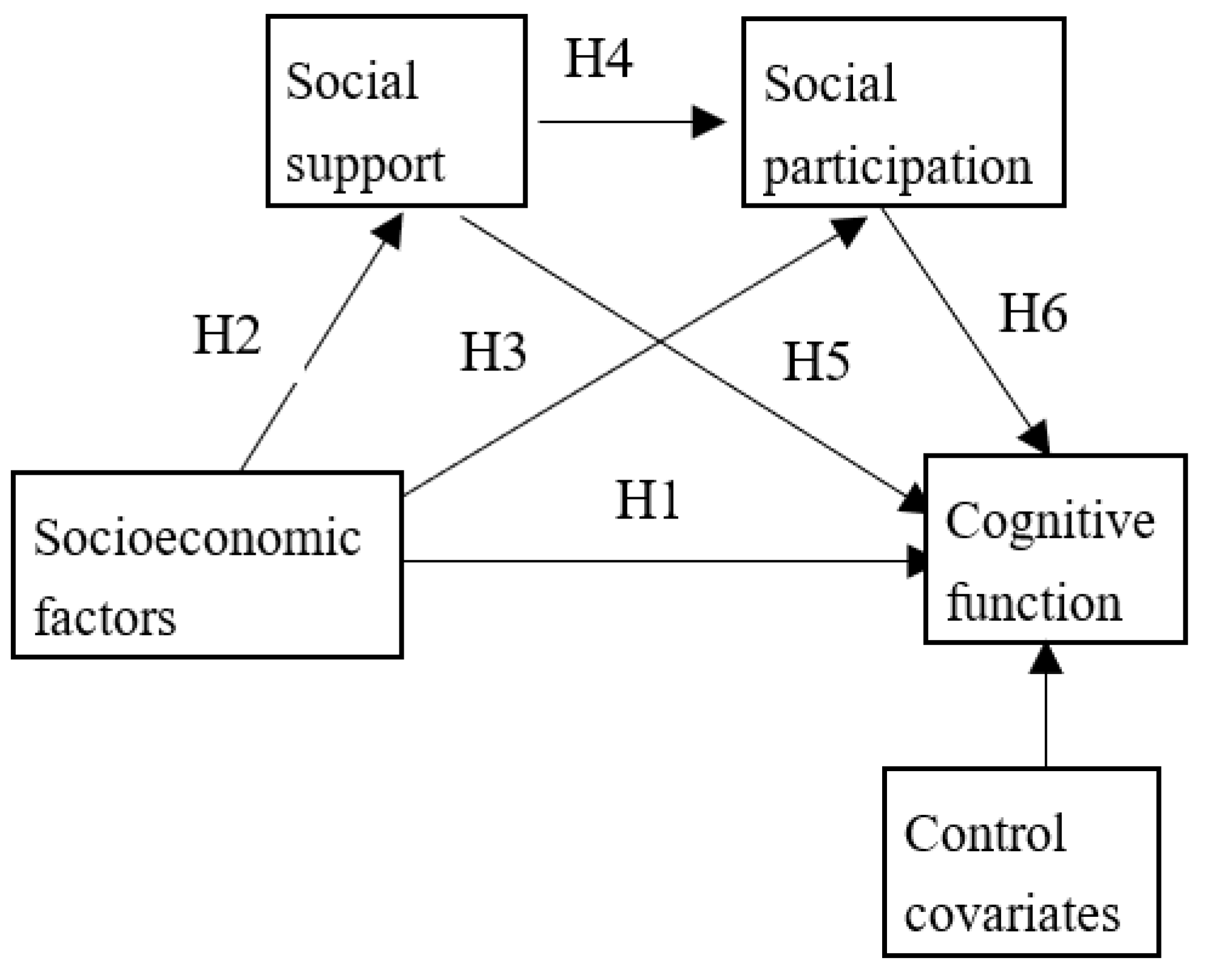
Figure 2.
The mediation model with multi-categorical independent variable (X: independent variable; Y: dependent variable; M: mediation variable; ai: the relative effects of the other k-1 levels, respectively, relative to the k level, on mediation variable; b: the association between mediation variable and dependent variable; ci: relative total effect of the k-1 levels, respectively, relative to the k level, on dependent variable; C'i: relative direct effects of the k-1 levels, respectively, relative to the k level, on dependent variable after controlling for mediation variable.).
Figure 2.
The mediation model with multi-categorical independent variable (X: independent variable; Y: dependent variable; M: mediation variable; ai: the relative effects of the other k-1 levels, respectively, relative to the k level, on mediation variable; b: the association between mediation variable and dependent variable; ci: relative total effect of the k-1 levels, respectively, relative to the k level, on dependent variable; C'i: relative direct effects of the k-1 levels, respectively, relative to the k level, on dependent variable after controlling for mediation variable.).
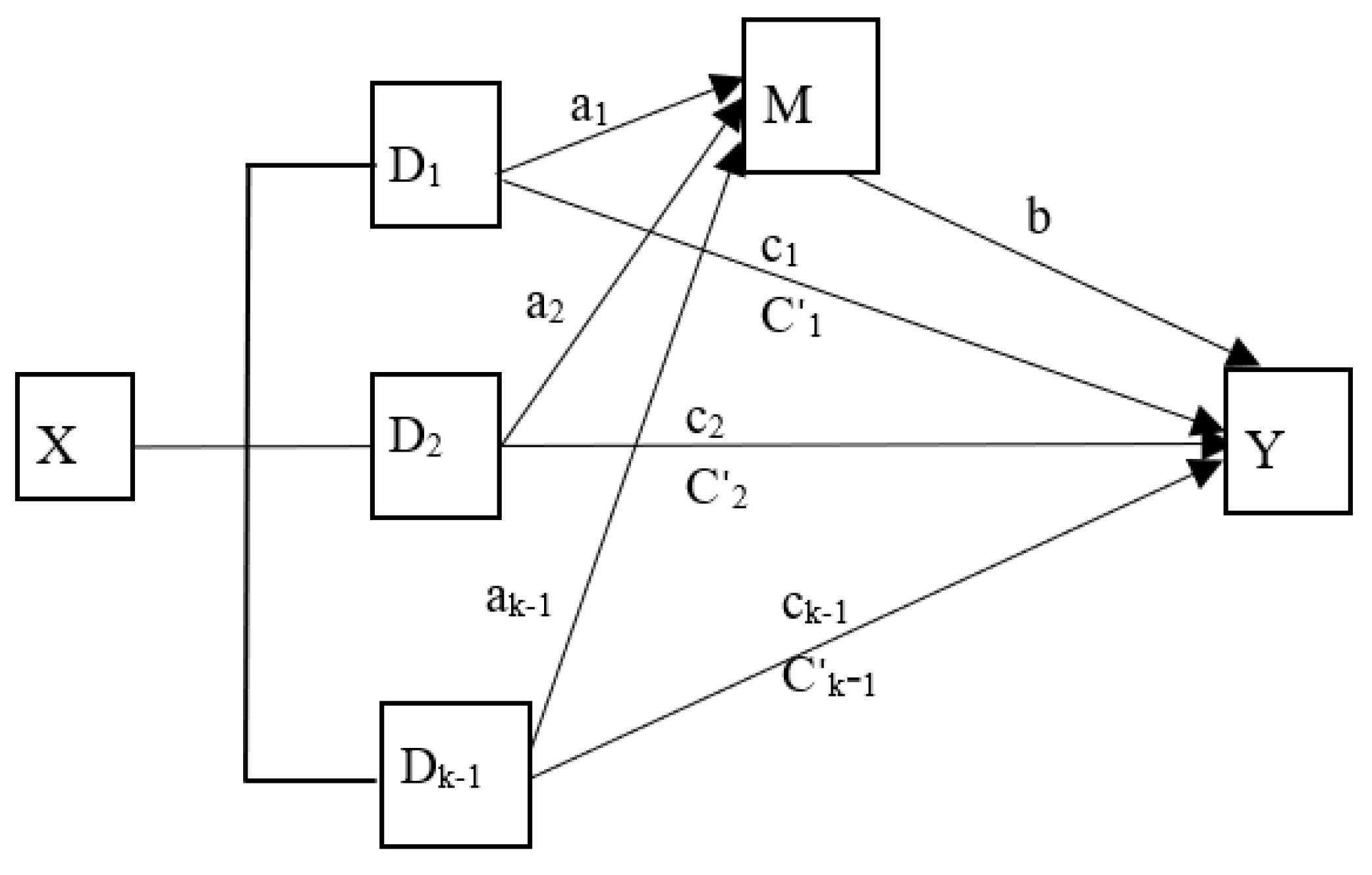
Figure 3.
Social participation or social support plays a mediating role between socioeconomic conditions (e.g., income, occupation and education) and cognitive function. The results showed that social participation and social support can positively mediate the relationship between socioeconomic factors and cognitive function. * p<0.05; ** p<0.01; ***p<0.001.
Figure 3.
Social participation or social support plays a mediating role between socioeconomic conditions (e.g., income, occupation and education) and cognitive function. The results showed that social participation and social support can positively mediate the relationship between socioeconomic factors and cognitive function. * p<0.05; ** p<0.01; ***p<0.001.
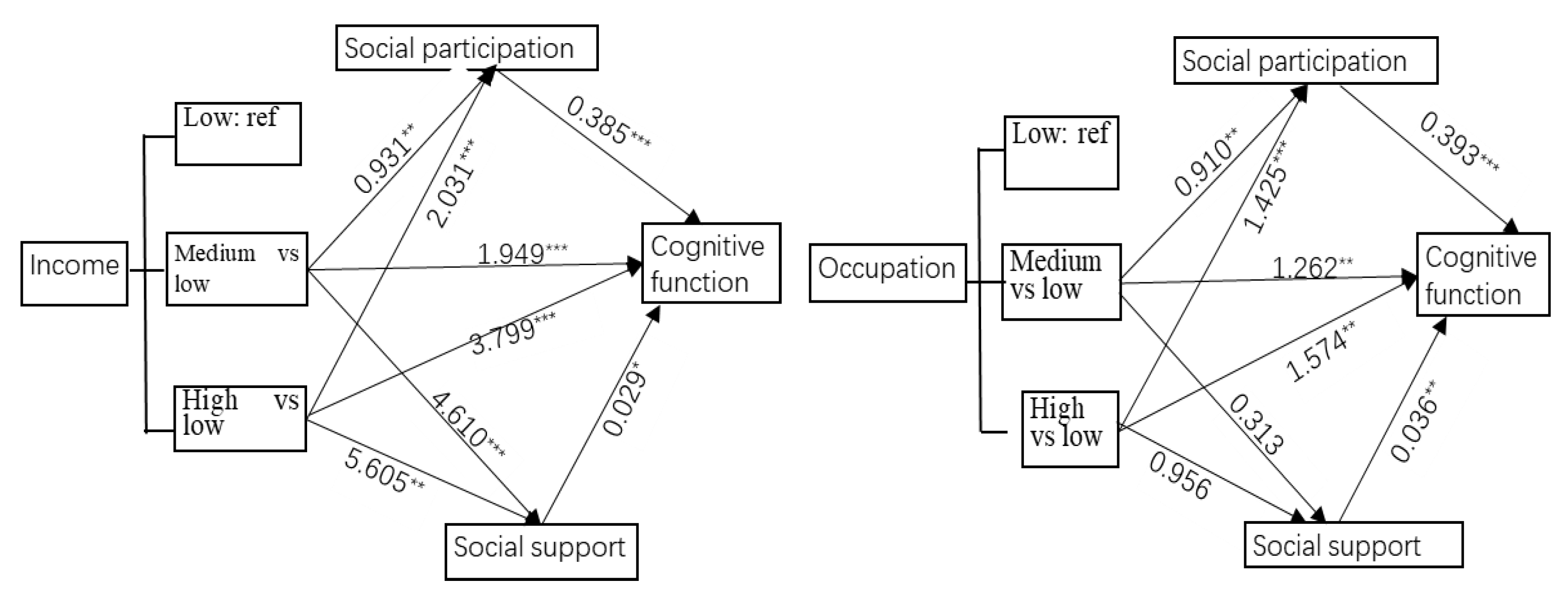
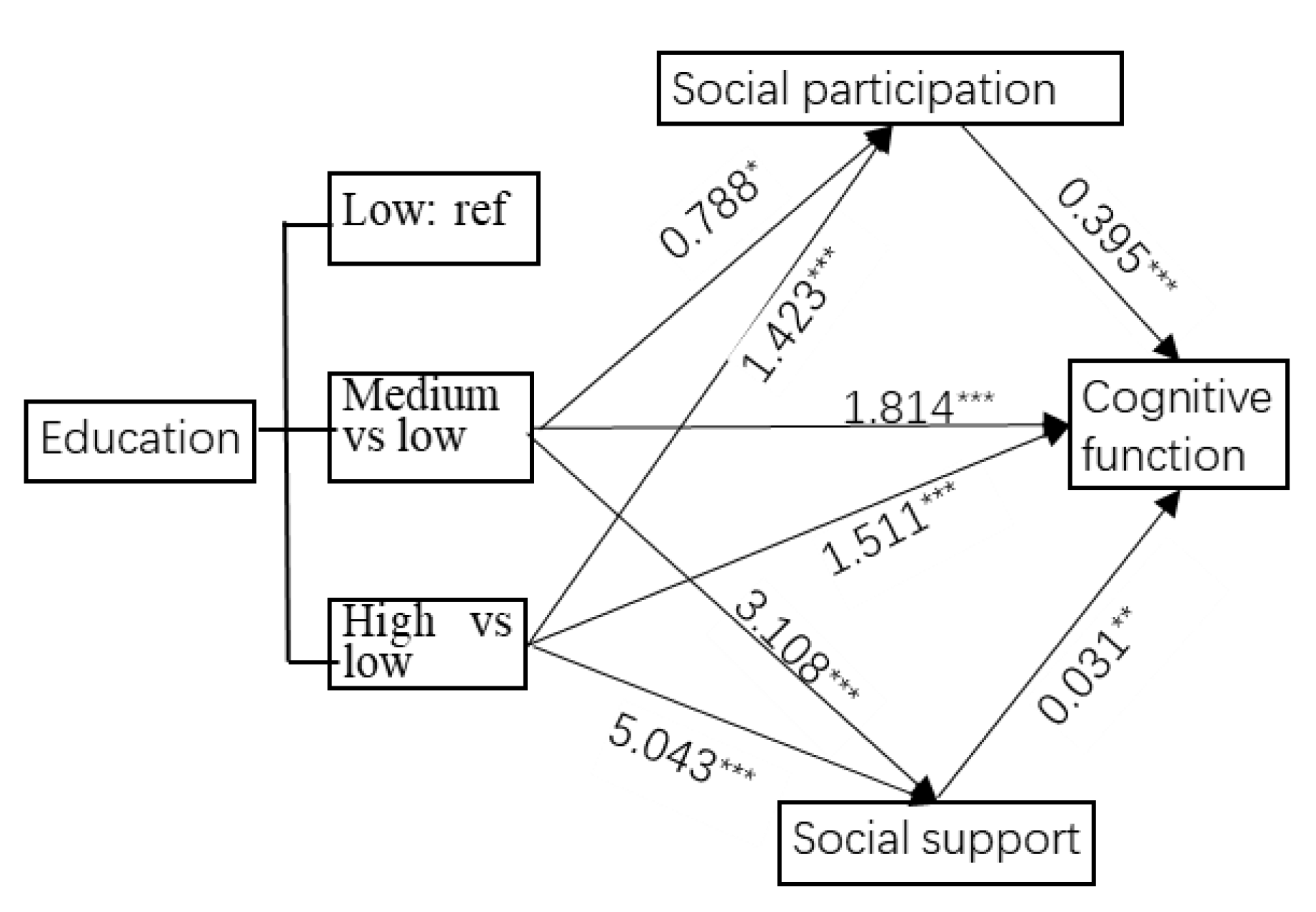
Figure 4.
Examined serial mediation model of social support and social participation on socioeconomic factors (income, occupation and education) and cognitive function in community-dwelling older adults. * p<0.05; ** p<0.01; *** p<0.001.
Figure 4.
Examined serial mediation model of social support and social participation on socioeconomic factors (income, occupation and education) and cognitive function in community-dwelling older adults. * p<0.05; ** p<0.01; *** p<0.001.
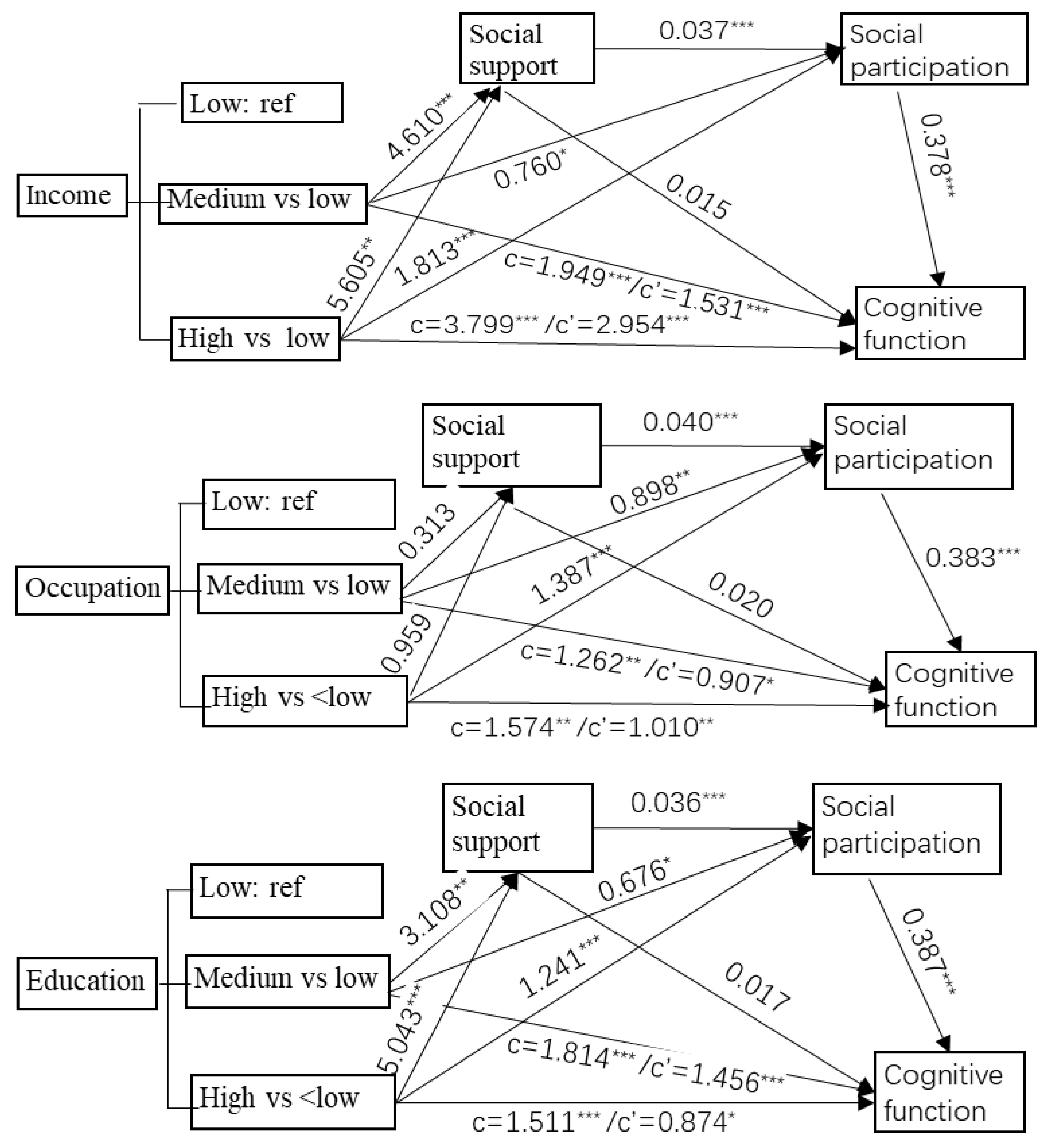

Table 1.
Variable definition and assignment.
| Variables | Variable definition and assignment |
| Dependent variable | |
| Cognitive function | MoCA scores. Value range: 0-30 scores |
| Independent variables | |
| Income | Retire pension monthly. 1=less than 2000 yuan/month; 2=2000-6000 yuan/month; 3=more than 6000 yuan/month |
| Education | Educational scores. 1=less than 6 scores; 2=6-10 scores; 3=more than 10 scores. |
| Occupation | Occupational complexity scores. 1=less than 53 scores; 2=53-90 scores; 3=more than 90 scores. |
| Mediating variables | |
| Social participation | Scores. Value range:5-20 scores |
| Social support | Scores: value range: 12-84 scores |
| Covariates | |
| Age | 1=60-65 years old; 2=66-75 years old; 3=71-75 years old; 4=more than 75 years old. |
| Sex | 1=male; 2=female |
| Marital status | 1=married and living with a spouse; 2=separated (widowed or divorced) |
| Sleep quality | PSQI scores: 1=less than 5 scores; 2=5-10 scores; 3=more than 10 scores |
| Smoking status | 1=current smoking; 2=never or quit smoking |
| Drinking status | 1=current drink; 2=never or occasional drinking |
| BMI (kg/m2) | 1=less than 24; 2=more than or equal to 24. |
| Nutrition status | MNA scores: 1=less than 12 scores; 2=more than and equal to 12 |
| Co-morbidities | 1=none; 2=one chronic disease; 3=more than two diseases |
Table 2.
Comparison of cognitive function among the sample characteristics.
| Categorical measures | N (%) |
MoCA (scores) Mean (SD) |
P value | |
| Income (yuan/month) | <2000 | 205 (20.9%) | 18.06±5.60 | |
| 2000~6000 | 695 (71.0%) | 20.31±5.30 | ||
| >6000 | 79 (8.1%) | 22.40±5.08 | <0.001 | |
| Occupation (scores) | <53 | 325 (33.2%) | 19.12±5.86 | |
| 53~90 | 336 (34.2%) | 20.33±5.29 | ||
| >90 | 318 (32.5%) | 20.57±5.10 | 0.01 | |
| Education (scores) | <6 | 315 (32.2%) | 18.50±6.03 | |
| 6~10 | 330 (33.7%) | 20.85±4.61 | ||
| >10 | 331 (33.8%) | 20.56±5.40 | <0.001 | |
| Sex | Male | 413 (42.4%) | 20.14±5.40 | |
| Female | 564 (57.6%) | 19.91±5.50 | 0.501 | |
| Age (years) | 60~65 | 288 (29.4%) | 21.33±4.57 | |
| 66~70 | 336 (34.3%) | 20.48±4.89 | ||
| 71~75 | 169 (17.3%) | 19.99±5.61 | ||
| >75 | 185 (18.9%) | 17.07±6.44 | <0.001 | |
| BMI (kg/m2) | <24 | 586 (59.9%) | 19.96±5.40 | |
| >=24 | 374 (38.2%) | 20.05±5.58 | 0.794 | |
| missing | 19 (1.9%) | |||
| Marital status | married | 848 (86.6%) | 20.33±5.27 | |
| separated | 131 (13.4%) | 17.89±6.13 | <0.001 | |
| Smoking | Yes | 177 (18.1%) | 20.67±4.85 | |
| No or quit | 802 (81.9%) | 19.86±5.58 | 0.050 | |
| Drinking | Yes | 154 (15.7%) | 20.90±4.71 | |
| No or quit | 825 (84.3%) | 19.84±5.57 | 0.014 | |
| Co-morbidities | None | 163 (16.6%) | 19.90±5.80 | |
| 1 | 375 (38.3%) | 20.09±5.43 | ||
| ≥2 | 242 (24.7%) | 19.39±5.64 | 0.311 | |
| missing | 199 (20.3%) | |||
| Nutrition status | <=12 | 30 (6.1%) | 19.32±5.67 | |
| (MNA, scores) | >12 | 465 (93.9%) | 20.29±5.35 | 0.011 |
| Sleep Quality | <5 | 573 (58.5%) | 20.63±5.26 | |
| (PSQI, scores) | 5~10 | 327 (33.4%) | 19.38±5.57 | |
| >10 | 79 (8.1%) | 18.12±5.72 | <0.001 | |
Table 3.
descriptive statistical results and correction analysis between dependent and moderating variables (Pearson correlation coefficient).
Table 3.
descriptive statistical results and correction analysis between dependent and moderating variables (Pearson correlation coefficient).
| Variables | Mean (SD) | Cognitive function (MoCA, scores) |
Social participation (scores) | Social support (scores) |
| Cognitive function (MoCA,scores) | 20.1 (5.46) | 1 | ||
| Social participation (scores) | 11.3 (4.1) | 0.350*** | 1 | |
| Social support (scores) | 59.1 (14.8) | 0.139*** | 0.169*** | 1 |
***. P<0.001.
Table 4.
Omnibus effect analysis (F values).
| Mediation variable | Independent variables | Dependent variable (cognitive function) | ||
| Omnibus total effect | Omnibus direct effect | Bootstrap 95% CI | ||
| Social participation | Income | 18.294*** | 12.759*** | 0.307~0.461 |
| Occupation | 8.487*** | 4.088** | 0.313~0.471 | |
| Education | 11.120*** | 7.481*** | 0.316~0.472 | |
| Social support | Income | 18.294*** | 16.301*** | 0.005~0.053 |
| Occupation | 8.487*** | 8.258*** | 0.013~0.058 | |
| Education | 11.120*** | 9.594*** | 0.008~0.054 | |
*P<0.05, **P<0.01, ***P<0.001 after controlling age, marital status, smoking, drinking, nutrition status and sleep quality. CI=confidence intervals; the bootstrap 95% CI was for omnibus mediation effect.
Table 5.
Relative mediation effect of the mediation variables.
| Mediation variables | Socioeconomic conditions | Cognitive function | |||
| ci | aib | Bootstrap 95% CI | |aib/ci| | ||
| Social participation | Income (ref:<2000 yuan/month) | ||||
| 2000~6000 | 1.949*** | 0.358 | 0.110~0.614 | 18.36% | |
| >6000 | 3.799*** | 0.777 | 0.349~1.222 | 20.45% | |
| Occupation(ref:<53scores) | |||||
| 53~90 | 1.262** | 0.358 | 0.123~0.614 | 28.36% | |
| >90 | 1.574** | 0.561 | 0.299~0.851 | 35.64% | |
| Education (ref:<6 scores) | |||||
| 6~10 | 1.814*** | 0.311 | 0.058~0.572 | 17.14% | |
| >10 | 1.511*** | 0.562 | 0.294~0.853 | 39.19% | |
| Social support | Income (ref:<2000 yuan/month) | ||||
| 2000~6000 | 1.949*** | 0.132 | 0.019~0.282 | 6.77% | |
| >6000 | 3.799*** | 0.160 | 0.017~0.372 | 4.21% | |
| Occupation(ref:<53scores) | |||||
| 53~90 | 1.262** | 0.011 | -0.073~0.103 | -- | |
| >90 | 1.574** | 0.034 | -0.042~0.132 | -- | |
| Education (ref:<6 scores) | |||||
| 6~10 | 1.814*** | 0.096 | 0.013~0.214 | 5.29% | |
| >10 | 1.511*** | 0.156 | 0.035~0.318 | 10.32% | |
Ref=reference category, ci=the relative total effects of every category in categorical variables on the dependent variable, aib=the quantity of relative mediation effect, |aib/ci|=the proportion of relative mediation effect, CI=confidence interval. *P<0.05, **P<0.01, ***P<0.001 adjustment for age, marital status, smoking, drinking, nutrition status and sleep quality.
Table 6.
Relative direct effect of each variable in the serial mediation model.
| Relative direct effects | β | S.E | t | P | 95%CI of β | |
| LLCI | ULCI | |||||
| Income (refer=low income level) | ||||||
| Medium income →social support | 4.610 | 1.144 | 4.029 | <0.001 | 2.365 | 6.855 |
| Medium income →social participation | 0.760 | 0.319 | 2.384 | 0.017 | 0.134 | 1.385 |
| Medium income →cognitive function | 1.531 | 0.394 | 3.887 | <0.001 | 0.758 | 2.303 |
| High income →social support | 5.605 | 1.937 | 2.894 | 0.004 | 1.805 | 9.406 |
| High income →social participation | 1.813 | 0.537 | 3.373 | 0.001 | 0.758 | 2.868 |
| High income →cognitive function | 2.954 | 0.666 | 4.437 | <0.001 | 1.647 | 4.261 |
| Social support →social participation | 0.037 | 0.009 | 4.175 | <0.001 | 0.020 | 0.055 |
| Social support →cognitive function | 0.015 | 0.011 | 1.321 | 0.184 | -0.007 | 0.036 |
| Social participation →cognitive function | 0.378 | 0.04 | 9.535 | <0.001 | 0.300 | 0.455 |
| Occupation (refer=low level of occupation complexity) | ||||||
| Medium occupation →social support | 0.313 | 1.123 | 0.278 | 0.781 | -1.891 | 2.516 |
| Medium occupation →social participation | 0.898 | 0.307 | 2.928 | 0.003 | 0.296 | 1.499 |
| Medium occupation →cognitive function | 0.907 | 0.383 | 2.366 | 0.018 | 0.155 | 1.660 |
| High occupation →social support | 0.956 | 1.137 | 0.841 | 0.401 | -1.276 | 3.188 |
| High occupation→ social participation | 1.387 | 0.311 | 4.465 | <0.001 | 0.777 | 1.997 |
| High occupation →cognitive function | 1.010 | 0.391 | 2.583 | 0.010 | 0.243 | 1.776 |
| Social support →social participation | 0.040 | 0.009 | 4.559 | <0.001 | 0.023 | 0.057 |
| Social support →cognitive function | 0.020 | 0.011 | 1.841 | 0.066 | -0.001 | 0.042 |
| Social participation →cognitive function | 0.383 | 0.040 | 9.562 | <0.001 | 0.304 | 0.461 |
| Education (refer=low educational level) | ||||||
| Medium education →social support | 3.108 | 1.138 | 2.732 | 0.006 | 0.875 | 5.341 |
| Medium education →social participation | 0.676 | 0.316 | 2.141 | 0.033 | 0.056 | 1.296 |
| Medium education →cognitive function | 1.456 | 0.392 | 3.713 | <0.001 | 0.687 | 2.226 |
| High education →social support | 5.043 | 1.138 | 4.431 | <0.001 | 2.810 | 7.276 |
| High education →social participation | 1.241 | 0.318 | 3.906 | <0.001 | 0.618 | 1.865 |
| High education →cognitive function | 0.874 | 0.397 | 2.203 | 0.028 | 0.096 | 1.653 |
| Social support →social participation | 0.036 | 0.009 | 4.044 | <0.001 | 0.019 | 0.053 |
| Social support →cognitive function | 0.017 | 0.011 | 1.529 | 0.127 | -0.005 | 0.039 |
| Social participation →cognitive function | 0.387 | 0.040 | 9.704 | <0.001 | 0.309 | 0.465 |
SE=standard error, β=regression coefficient, CI=confidence intervals, LLCI=lower level confidence interval, ULCI=upper level confidence interval.
Table 7.
Relative mediation effect of the serial mediation variables.
| Socioeconomic conditions | Mediation path | Cognitive function | |||
| ci | aib | Bootstrap 95% CI of aib | |aib/ci| | ||
| Income (ref: low income level) | |||||
| Medium level | Social support | 1.949*** | 0.067 | -0.032~0.193 | --- |
| Social participation | 1.949*** | 0.287 | 0.042~0.539 | 14.7% | |
| Social support→social participation | 1.949*** | 0.065 | 0.025~0.115 | 3.3% | |
| High level | Social support | 3.799*** | 0.082 | -0.038~0.243 | --- |
| Social participation | 3.799*** | 0.685 | 0.261~1.136 | 18.0% | |
| Social support→social participation | 3.799*** | 0.078 | 0.023~0.152 | 2.0% | |
| Occupation (ref: low level of occupation complexity) | |||||
| Medium level | Social support | 1.262** | 0.006 | -0.047~0.070 | --- |
| Social participation | 1.262** | 0.344 | 0.117~0.591 | 27.3% | |
| Social support→social participation | 1.262** | 0.005 | -0.030~0.044 | --- | |
| High level | Social support | 1.574** | 0.019 | -0.028~0.090 | --- |
| Social participation | 1.574** | 0.531 | 0.277~0.824 | 33.7% | |
| Social support→social participation | 1.574** | 0.015 | -0.019~0.055 | --- | |
| Education (ref: low educational level) | |||||
| Medium level | Social support | 1.814*** | 0.053 | -0.013~0.150 | --- |
| Social participation | 1.814*** | 0.262 | 0.020~0.515 | 14.4% | |
| Social support→social participation | 1.814*** | 0.043 | 0.010~0.089 | 2.4% | |
| High level | Social support | 1.511*** | 0.086 | -0.022~0.223 | --- |
| Social participation | 1.511*** | 0.480 | 0.224~0.761 | 31.8% | |
| Social support→social participation | 1.511*** | 0.070 | 0.027~0.129 | 4.6% | |
ref=reference, ci=the relative total effects of every category in categorical variables on the dependent variable, aib=the quantity of relative mediation effect, |aib/ci|=the proportion of relative mediation effect, CI=confidence interval. *P<0.05, **P<0.01, ***P<0.001 adjustment for age, marital status, smoking, drinking, nutrition status and sleep quality.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



