
Submitted:
20 November 2025
Posted:
27 November 2025
You are already at the latest version
Abstract
The aging of the population and the increasing prevalence of multimorbidity contribute to the widespread use of polypharmacotherapy, which in turn elevates the risk of adverse drug reactions and clinically significant drug–drug interactions. One of the key yet frequently underestimated issues in clinical practice is the prescribing cascade, which occurs when an adverse drug reaction is misinterpreted as a new medical condition, leading to the initiation of an additional medication. This phenomenon is particularly relevant in the elderly population, in whom altered pharmacokinetics and pharmacodynamics, together with reduced organ reserve, increase susceptibility to adverse drug events, including nephrotoxicity. The objective of this paper is to review current evidence on the mechanisms and clinical consequences of the prescribing cascade-with particular emphasis on renal function deterioration—as well as strategies for its prevention in the geriatric population. Analysis of the literature indicates that prescribing cascades remain insufficiently recognized in clinical practice, despite the availability of pharmacotherapy assessment tools such as the Beers Criteria and the STOPP/START criteria. Documented prescribing cascades have been shown to contribute to deterioration in health status and quality of life, an increased frequency of hospitalizations, and a greater burden on healthcare systems. Particularly concerning are cascades involving cardiovascular, neurological, and analgesic medications, which may induce or exacerbate renal injury, ultimately leading to chronic kidney disease and organ failure. Prescribing cascades represent a significant yet frequently underestimated threat to the efficacy and safety of pharmacotherapy in older adults. Their consequences may extend beyond reduced quality of life and increased treatment costs to include serious complications such as the development of renal failure. Enhancing clinicians’ awareness, conducting systematic medication reviews, and employing validated assessment tools are essential for the identification and prevention of prescribing cascades, thereby reducing the risk of renal injury and improving clinical outcomes.
Keywords:
prescribing cascade
; polypharmacy
; chronic kidney disease
; drug safety
1. Introduction
Population aging and the increasing prevalence of multimorbidity have led to a growing reliance on polypharmacotherapy, which substantially raises the risk of adverse drug reactions and clinically significant drug–drug interactions. Among the key yet still underappreciated challenges in clinical practice is the phenomenon known as the prescribing cascade. This occurs when an adverse drug reaction is misinterpreted as a manifestation of a new disease, prompting the initiation of an additional medication. Such an approach may trigger a vicious cycle of subsequent pharmacological interventions, markedly amplifying the risk of further complications [1,2]. This problem is particularly pronounced in geriatric patients, in whom altered pharmacokinetics and pharmacodynamics, reduced organ reserve, and the coexistence of multiple chronic conditions significantly increase the risk of adverse drug events, their accumulation, and drug–drug interactions [2,3]. Of particular concern are cascades involving cardiovascular, analgesic, and anti-inflammatory agents, which may contribute to renal impairment and even the development of chronic kidney disease and renal failure. The consequences of prescribing cascades therefore extend beyond reduced quality of life and increased risk of hospitalization, encompassing serious organ complications that place an additional burden on healthcare systems. Despite the availability of tools supporting the evaluation of pharmacotherapy appropriateness, such as the Beers Criteria and STOPP/START criteria, prescribing cascades remain insufficiently recognized and often overlooked in clinical practice. The aim of this paper is to review the current evidence regarding the mechanisms and clinical consequences—particularly with respect to renal function deterioration—as well as strategies to prevent prescribing cascades in the geriatric population.
2. Risk Factors for Prescribing Cascades
Identification of risk factors for the occurrence of prescribing cascades is a key element in limiting the prevalence of this phenomenon. It reduces negative health consequences for the patient and enables verification and improvement of treatment standards, particularly in patients with multimorbidity. Preventing and eliminating prescribing cascades is therefore an important step toward improving the quality of care and clinical outcomes [4]. Risk factors for adverse prescribing cascades can be grouped into categories related to the medical status of the patient and those that are “non-medical,” associated with the current ease of access to medications and other medical products. In the first category, we include advanced age, multimorbidity, polypharmacy, and overprescribing, often linked to multispecialist treatment provided by several physicians without mutual verification of ongoing pharmacotherapy. Within this group, particular attention should be paid to the risk of renal injury-both acute kidney injury (AKI) and chronic kidney disease (CKD). Many drugs prescribed concurrently as part of cascades (e.g., nonsteroidal anti-inflammatory drugs, ACE inhibitors, diuretics, and nephrotoxic antibiotics) may exert cumulative renal burden, resulting in progressive renal impairment, especially in geriatric patients. [5,6,7,8]. The second group of risk factors includes obtaining prescriptions online without direct physician consultation, easy availability of over-the-counter drugs (OTC), and, consequently, the possibility of self-medication and unnecessary supplementation (pathosupplementation). Additional contributing factors are the widespread promotion of medications and supplements in pharmacies, mass media advertising (television, internet), and pharmacy-based sales promotions. Table 1 summarizes the risk factors for the occurrence of prescribing cascades [5,6,9].
Prescribing cascades may occur in any patient experiencing health deterioration, but age-related physiological changes naturally predispose to worsening health status. Age is a parameter defining the biological and physiological aspects of aging and is associated with the natural predisposition to age-related diseases and their treatment. In this group, renal impairment is particularly prevalent, increasing susceptibility to adverse drug reactions from medications eliminated renally. Consequently, older adults are more likely to develop acute kidney injury as a result of prescribing cascades, and long-term exposure may even induce chronic kidney disease. Accurate data on the physiology and pathology of aging may help reduce unnecessary polypharmacy. However, clinical trials often exclude or insufficiently represent older adults with multimorbidity, resulting in a lack of evidence-based (EBM) guidelines for combination drug therapy in this population. This leads to suboptimal pharmacotherapeutic choices—frequently involving the use of “older” drugs with a high risk of adverse events, particularly nephrotoxic complications. The lack of data derived from clinical research also contributes to insufficient use of modern therapies in geriatric patients, often justified by concerns about poor tolerability due to age. On the other hand, unexpected cascades may occur when new medications are introduced without a thorough analysis of age-related pathophysiological changes. In summary, the underrepresentation of older adults with multimorbidity in clinical trials results in a lack of precise evidence-based pharmacotherapeutic guidelines for this population, fostering the occurrence of prescribing cascades and increasing the risk of renal insufficiency [5,6,7,10]. Verification of risk factors facilitates the recognition of prescribing cascades, yet practical tools to help physicians reliably identify cascades, assess them appropriately, and manage them effectively are still lacking. Polypharmacy, although considered a risk factor for prescribing cascades, is undoubtedly an essential element of good prescribing practice in aging populations. At the same time, the lack of systematic evaluation of renal function during therapy selection further exacerbates the risk of cascades leading to acute kidney injury or progression of chronic kidney disease. The classification of cascades as appropriate or inappropriate (intended/unintended) may evolve over time depending on the clinical status of the patient. [7,8,12]. Therapeutic regimens, typically designed with a disease- and organ-specific focus, often overlook an interdisciplinary assessment of renal function. Failure to account for this aspect promotes therapeutic decisions that result in additive adverse drug effects and, consequently, increase the risk of prescribing cascades. Thus, a key question arises: Why does the risk of prescribing cascades increase in clinical practice? Table 2 presents cause-and-effect relationships of prescribing cascades, including their association with renal injury progression. [5,6,7,8,9,11,12,15].
3. Examples of Prescribing Cascades and Their Clinical Significance
Prescribing cascades are a common but often underrecognized phenomenon in clinical practice, particularly among older adults. They occur when an adverse drug reaction is misinterpreted as a new medical condition, leading to the initiation of an additional drug rather than recognition of the underlying cause. In the long term, this process not only increases the risk of inappropriate polypharmacy but also heightens the likelihood of drug-related morbidity, hospitalizations, and healthcare costs [1,7,12]. The tables below summarize clinically important prescribing cascades described in recent consensus statements and systematic reviews. Table 3 and Table 4 presents cascades that are particularly relevant in older adults, identified through the ThinkCascades tool and the international list of potentially inappropriate prescribing cascades (PIPC) [1,7,12].
The clinical significance of these cascades is multifaceted. First, they frequently contribute directly to deterioration in patients’ functional status. For example, calcium channel blocker–induced peripheral edema treated with diuretics may result in dehydration and falls. Similarly, benzodiazepine-related cognitive impairment treated with cholinesterase inhibitors only adds to the pharmacological burden without addressing the underlying cause. Second, an important yet often underestimated aspect of prescribing cascades is their impact on renal function. The use of diuretics in response to adverse effects of other medications (e.g., edema caused by calcium channel blockers or NSAIDs) may lead to dehydration, electrolyte disturbances, and accelerated decline in glomerular filtration. Consequently, the risk of nephrotoxicity from additional medications, accumulation of drug metabolites, and further progression of kidney disease increases. In older adults, whose renal reserve is already limited, such cascades can significantly increase the risk of acute kidney injury (AKI) or accelerate the development of chronic kidney disease (CKD). Third, prescribing cascades often contribute to therapeutic inertia, as clinicians may attribute drug-related symptoms (such as dizziness, hypotension, or worsening renal function tests) to aging or disease progression rather than to adverse drug effects [7,12]. Recent systematic reviews emphasize that prescribing cascades are not random events but rather reproducible and predictable patterns observed across healthcare systems [1]. Recognition of these patterns is therefore critical for implementing preventive strategies such as medication review and deprescribing. In particular, the PIPC list developed by the international expert panel provides clinicians with a practical tool for identifying high-risk cascades, while the ThinkCascades tool offers a structured approach to evaluating drug–symptom associations in daily practice [7,12]. Ultimately, the presence of prescribing cascades highlights the importance of regular medication review, interdisciplinary collaboration, and patient education. Raising awareness of well-documented cascades such as those listed above may help clinicians distinguish adverse drug reactions from disease progression—including declining renal function and thereby reduce inappropriate polypharmacy and its associated risks.
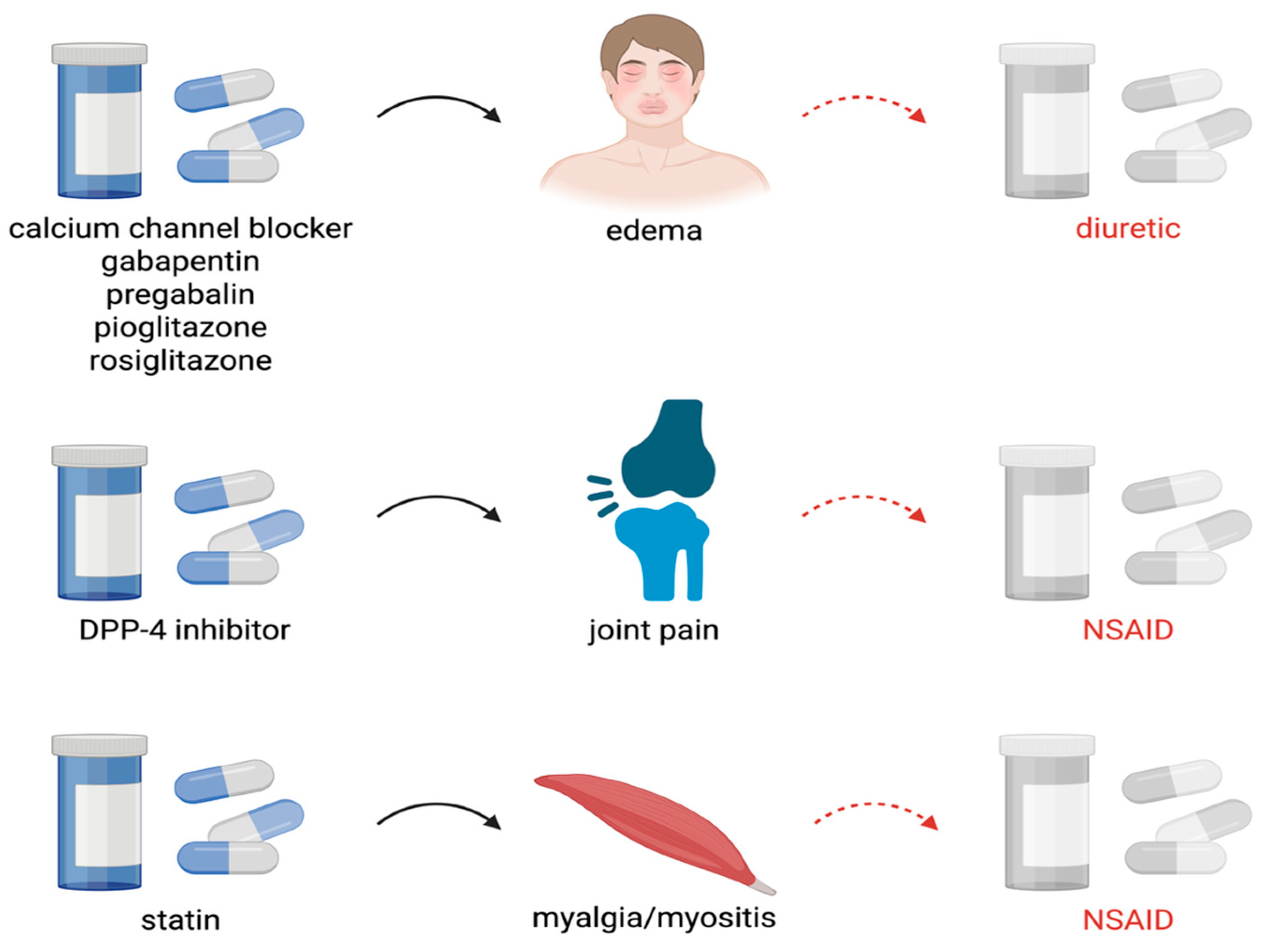
Figure 1.
Examples of prescribing cascades affecting kidney function. DPP-4, Dipeptidyl peptidase 4; NSAID, Nonsteroidal anti-inflammatory drug. Created in BioRender. Miedziaszczyk, M. (2025) https://BioRender.com/welwul.
Figure 1.
Examples of prescribing cascades affecting kidney function. DPP-4, Dipeptidyl peptidase 4; NSAID, Nonsteroidal anti-inflammatory drug. Created in BioRender. Miedziaszczyk, M. (2025) https://BioRender.com/welwul.
4. Consequences of Prescribing Cascades
A prescribing cascade can lead to serious health, social, and economic consequences. Although this phenomenon may appear to result from concern for the patient, it often worsens their clinical condition, leads to inappropriate treatment (so-called "therapeutic vicious circles") and polypharmacotherapy, which turns into polypragmasy. As a result, patients may experience intensified symptoms such as dizziness, drug-induced headaches, falls, delirium, cognitive impairment, balance disorders, orthostatic hypotension, or painsomnia. Importantly, some of these symptoms—such as delirium, balance disturbances, or hypotension—are often mistakenly attributed to the “natural” aging process or progression of the underlying disease, which further delays appropriate intervention. These are only some of the potential consequences of prescribing cascades, which negatively affect patients’ quality of life, leading to reduced mobility and independence and, quite often, the need for hospitalization [12]. Findings from observational studies and systematic reviews, as well as daily clinical practice, clearly indicate that prescribing cascades are a significant risk factor for hospitalization, especially in older adults, where the reason for hospital admission is not the primary disease but rather adverse drug reactions introduced in response to symptoms caused by previous pharmacotherapy. Examples include falls due to hypnotics or dehydration caused by diuretics prescribed in response to edema induced by NSAIDs or certain antidepressants. In the long term, prescribing cascades also contribute to rising healthcare costs, both direct (such as hospitalizations, diagnostics, and additional specialist consultations) and indirect (loss of independence, the need for continuous care). According to Farrell B and McCarthy LM, deprescribing and early identification of prescribing cascades can significantly reduce systemic expenditures as well as ease the burden on medical staff [7,14].
5. Identification and Prevention of Prescribing Cascades
Currently, there is a lack of practical tools to help physicians and pharmacists reliably detect, correctly assess, and manage prescribing cascades. Ponte et al. developed an 8-point (4 questions) scale to assess the prescribing cascade. Prescribing cascade is assumed to occur if the score is 4 or higher, reflecting the severity of the prescribing cascade. Table 5 presents a tool for assessing the occurrence of drug cascade prescription [15].
Dreischulte et al. proposed a tool that assesses whether the prescribing cascade is appropriate or inappropriate [6]. The tool is based on the following 6 questions. Although prescribing cascades are most often perceived as problematic, they may be appropriate and therapeutically beneficial in certain clinical situations. McCarthy et al. point out two important issues to consider when deciding on a prescribing cascade. First, consider whether the intentional initiation of a prescribing cascade aligns with the patient's treatment goals (patient well-being and improved quality of life). Second, consider whether the risks and benefits of the prescribing cascade have been discussed with the patient and whether the patient has been informed of the long-term effects [16]. Table 6 presents the Prescription Cascade Benefit Assessment Tool.
Analyzing everything that has been described, with particular emphasis on the risk factors for the occurrence of prescribing cascades, as well as clinical practices that increase the risk of their occurrence, we made an attempt to formulate general principles which, when implemented in clinical practice, may help prevent prescribing cascades. Table 7 presents the key points of clinical practice, which we can refer to as a list of good clinical practices [3].
6. Conclusions
Prescribing cascades constitute a clinically significant yet underrecognized problem in geriatric pharmacotherapy. Their occurrence not only promotes inappropriate polypharmacy but also contributes to deterioration in patients’ functional status, an increased risk of hospitalization, and higher healthcare costs. Particularly alarming are cascades involving cardiovascular, analgesic, and neurological agents, which may accelerate the decline of renal function and predispose to acute kidney injury or chronic kidney disease. The findings of this review highlight the urgent need to raise awareness among healthcare professionals about the mechanisms and consequences of prescribing cascades. Regular medication reviews, systematic monitoring of renal function, and the use of validated assessment tools—such as the Beers Criteria, STOPP/START, and PIPC—are essential steps toward minimizing the risk of inappropriate prescribing and preventing renal complications. Interdisciplinary collaboration and patient education further strengthen preventive strategies. Ultimately, addressing prescribing cascades is not only a matter of improving medication safety but also a prerequisite for enhancing the quality of life and clinical outcomes in older adults.
Author Contributions
Conceptualization, A.B. and M.M.; formal analysis, A.B. and M.M.; data curation, A.B., J.W., M.M., B.L.Z., B.B.G.; writing—original draft preparation, A.B. J.W., M.M., B.L.Z., B.B.G., D.O., P.P., W.P.; writing—review and editing, A.B. and M.M.; visualization, A.B.; J.W.: M.M; supervision, A.B and M.M.; project administration, A.B. and M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interests.
Abbreviations
The following abbreviations are used in this manuscript:
| AKI | Acute Kidney Injury |
| CKD | Chronic Kidney Disease |
| ACEI | Angiotensin Converting Enzyme Inhibitors |
| OTC | Over The Counter |
| EBM | Evidence Based Medicine |
| PIPC | Potentially Inappropriate Prescribing Cascades |
| GERD | Gastroesophageal Reflux Disease |
| DDP-4 | Dipeptidyl Peptidase 4 |
| SGLT-2 | Sodium Glucose Cotransporter 2 |
| NSAID | Nonsteroidal Antiinflammatory Drug |
| ADR | Adverse Drug Reaction |
References
- Adrien, O.; Mohammad, A.K.; Hugtenburg, J.G.; et al. Prescribing Cascades with recommendations to Prevent or Reverse Them: A Systematic Review. Drugs and Anging. 2023, 40, 1085–1100. [Google Scholar] [CrossRef] [PubMed]
- Shahid, F.; Moriarty, F.; Boland, F.; et al. Prescribing cascades in ambulatory care: A structured synthesis of evidence. Pharmacotherapy, 2024, 44, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Woroń, J.; Tymiński, R.; Drygalski, T.; et al. Farmakoterapia nieprawidłowo dobrana, co to znaczy w praktyce, a także w Oddziale Intensywnej Terapii. Anestezjologia i Ratownictwo 2023, 17, 42–48. [Google Scholar]
- Rochon, P.A.; Gurwitz, J.H. The prescribing cascade revisited. Lancet 2017, 6, 1778–1780. [Google Scholar] [CrossRef] [PubMed]
- Doherty, A.S.; Shahid, F.; Moriarty, F.; et al. Prescribing cascades in community-dwelling adults: A systematic review. Pharmacol. Res. Perspect. 2022, 10, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Dreischulte, T.; Shahid, F.; Muth, C.; et al. Prescribing Cascades: How to Detect Them, Prevent Them, and Use Them Appropriately. Dtsch. Arztebl. Int. 2022, 119, 745–752. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, L.M.; Savage, R.; Dalton, K.; et al. A Tool for Identifying Clinically Important Prescribing Cascades Affecting Older People. Drugs Aging. 2022, 39, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Shahid, F.; Doherty, A.; Wallace, E.; et al. Prescribing cascades in ambulatory care: A structured synthesis of evidence. Pharmacotherapy. 2024, 44, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Liu, Z.; Zeng, L.; et al. Research on prescribing cascades: A scoping review. Front. Pharmacol. 2023, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jennings, A.A.; Doherty, A.S.; Clyne, B.; et al. Stakeholder perceptions of and attitudes towards problematic polypharmacy and prescribing cascades: A qualitative study. Age Ageing. 2024, 53, 1–12. [Google Scholar] [CrossRef] [PubMed]
- O'Mahony, D.; Rochon, P.A. Prescribing cascades: We see only what we look for, we look for only what we know. Age Ageing. 2022, 51, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Rochon, P.A.; O'Mahony, D.; Cherubini, A.; et al. International expert panel's potentially inappropriate prescribing cascades (PIPC) list. Eur. Geriatr. Med. 2025, 1–12. [Google Scholar] [CrossRef] [PubMed]
- American Geriatrics Society Beers Criteria. Update Expert Panel. American Geriatrics Society 2023. Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2023, 71, 923–947. [Google Scholar]
- Farrell, B.; Tsang, C.; Raman-Wilms, L.; et al. What are priorities for deprescribing for elderly patients? Capturing the voice of practitioners: A modified Delphi process. PLoS ONE. 2015, 10, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Ponte, M.L.; Wachs, L.; Wachs, A.; Serra, H.A. Prescribing cascade. A proposed new way to evaluate it. Medicina (B Aires). 2017, 77, 13–16. [Google Scholar] [PubMed]
- McCarthy, L.M.; Visentin, J.D.; Rochon, P.A. Assessing the Scope and Appropriateness of Prescribing Cascades. J. Am. Geriatr. Soc. 2019, 67, 1023–1026. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Risk factors for the occurrence of a prescribing cascade.
| Risk factor | A mechanism promoting the prescribing cascade |
| Patient age | Age-related changes in drug metabolism and excretion (pharmacokinetics) as well as tissue responsiveness to drugs (pharmacodynamics) increase susceptibility to adverse drug reactions. Use of high-risk medications in geriatric populations. |
| Sex | In certain therapies, women have a higher likelihood of developing prescribing cascades, due to differences in drug absorption rates, hormonal regulation, and metabolic pathways. |
| Polypharmacy | A large number of concurrently used drugs increases the probability of drug–drug interactions and adverse events, which may be mistakenly interpreted as new diseases. |
| Multimorbidity | The coexistence of multiple comorbidities predisposes to multi-organ dysfunction of varying severity, which affects drug metabolism and elimination. Multiple diseases often require multiple medications. |
| Chronic use of multiple medications |
Long-term therapies promote the accumulation (“overlapping”) of adverse effects and increase the risk of their misinterpretation. |
| Lack of comprehensive medication review |
Lack of regular assessment of the appropriateness of a given therapy (the entire treatment regimen) perpetuates the use of unnecessary medications and fosters the development of prescribing cascades. Additionally, the absence of dose reassessment maintains adverse drug effects. Prescribing more drugs instead of minimizing doses, and the failure to consider non-pharmacological alternatives before initiating drug therapy, further contribute to the problem. |
| Overprescribing | Insufficient communication about pharmacological interventions implemented by various specialists involved in patient care, including primary care physicians. |
| Misinterpretation of symptoms | Adverse drug reactions are misinterpreted as new disease entities, and the patient receives additional medications instead of therapeutic modification. |
| Insufficient knowledge of prescribing cascades among healthcare professionals |
Insufficient knowledge of the relationship between drugs and symptoms results in a failure to recognize that a new symptom is an adverse effect of a medication rather than a new disease. |
| Self-medication | The trend toward a “healthy lifestyle,” widespread availability of OTC drugs, and self-directed treatment, often reinforced by lack of trust in physicians and insufficient pharmacological knowledge. |
| Pathosupplementation (unnecessary supplementation without clinical indication) |
Dietary supplements as part of alternative treatment approaches. Easy access to various supplements, combined with aggressive marketing, promotes their use. Supplements are often perceived as an element of a “healthy lifestyle” and part of pro-health trends. |
Table 2.
Why is the risk of prescribing cascades rising in clinical practice.
| Treating the disease rather than the patient with the disease | In the context of appropriately tailored pharmacotherapy, patient characteristics play a crucial role and may constitute significant risk factors for the occurrence of adverse drug reactions, including complex, multifactorial complications arising from the specific nature of the pharmacotherapy employed |
| Uncritical and context-free application of therapeutic guidelines | A therapeutic guideline must address not only individual diseases, but its appropriate application in a given patient should always be considered within the full spectrum of multimorbidity |
| Assumption of a class effect within specific drug groups used in the patient | Within specific drug classes, a uniform class effect does not exist, which results from differences in pharmacokinetic and pharmacodynamic (PK/PD) parameters, as well as variability in adverse effect profiles and the associated risk factors for their occurrence. |
| Fragmentation of multimorbidity in pharmacological decision-making | Decisions regarding the initiation of pharmacotherapy for individual disease entities should always be guided by consideration of the overall spectrum of multimorbidity in the patient |
| Lack of benefit–risk assessment prior to initiation of pharmacotherapy | Before initiating any medication, the benefit–risk balance must be assessed, as it is influenced by patient-specific characteristics, coexisting risk factors for adverse events, concomitant pharmacotherapy, the use of complementary or alternative medicines, and dietary supplements. Equally relevant is the consumption of broadly defined recreational substances, as well as a history of prior drug-induced adverse reactions |
| Self-medication and supplementation | They may trigger drug interactions and complications, ultimately modifying the benefit–risk balance of the ongoing pharmacotherapy |
| Lack of awareness of the adverse effect profiles of prescribed drugs | In the context of polypharmacotherapy, clinicians must have a thorough understanding of the adverse effect profiles of prescribed agents and the risk factors predisposing to their development |
| Misinterpretation of drug-induced adverse effects as disease symptoms without consideration of ongoing pharmacotherapy | When new symptoms occur in a patient receiving pharmacotherapy, the primary consideration should be whether they are attributable to the treatment itself. If confirmed, appropriate modifications of the pharmacotherapy are required |
| Uncritical use of electronic tools for assessing the risk of drug–drug interactions in polypharmacotherapy | Most drug–interaction prediction tools fail to indicate the dosage thresholds at which interactions become clinically relevant, and only a limited number report interactions arising from the additive adverse effects of concomitantly used medications |
| Cumulative adverse effects of drugs in polypharmacotherapy as a source of complications in patients with multimorbidity | The additive effects of adverse reactions represent one of the most frequent forms of drug interactions in clinical practice. The symptoms that emerge through this mechanism frequently initiate a prescribing cascade. |
Table 3.
Clinically important prescribing cascades.
| Drug A | Adverse effect | Drug B |
| Calcium Channel Blocker | Peripheral edema | Diuretic |
| Diuretic | Urinary incontinence | Overactive bladder medication |
| Antipsychotic | Extrapyramidal symptoms | Antiparkinsonian agent |
| Benzodiazepine | Cognitive impairment | Cholinesterase Inhibitor or memantine |
| Benzodiazepine | Paradoxical agitation or agitation secondary to withdrawal | Antipsychotic |
| Selective Serotonin Reuptake Inhibitor (SSRI) / Serotonin-norepinephrine Reuptake Inhibitor (SNRI) | Insomnia | Sleep agent (e.g., Benzodiazepines, Benzodiazepine Receptor Agonists, Sedating antidepressant, Melatonin) |
| NSAID | Hypertension | Antihypertensive |
| Urinary Anticholinergics | Cognitive impairment | Cholinesterase inhibitor or memantine |
| Alpha-1 Receptor Blocker | Orthostatic hypotension, dizzines | Vestibular sedative (e.g., betahistine, Antihistamines, Benzodiazepines) |
Table 4.
Other prescribing cascades.
| Drug A | Adverse effect | Drug B |
| Cardiovascular system | ||
| Angiotensin converting enzyme inhibitor | Cough | Cough remedy |
| Antihypertensive | Orthostatic hypotension/dizziness | Antiemetic |
| Drug-induced hypertension | Hypertension | Antihypertensive drugs |
| Beta-blocker (particularly lipophilic e.g., propranolol) | Depression | Antidepressant |
| Beta-blocker (particularly lipophilic e.g., propranolol) | Erectile dysfunction | Phosphodiesterase-5 inhibitor, alprostadil |
| Calcium channel blocker, Gabapentin, Pregabalin | Peripheral edema | Diuretic |
| Calcium channel blocker | Constipation | Laxative |
| Diuretic | Gout or Hyperuricemia | Anti-gout agent |
| Diuretic | Urinary incontinence | Overactive bladder medication |
| Hydroxymethylglutaryl-coenzyme A (HMG Co-A) reductase inhibitor (statin) | Myalgia/myositis | Pain reliever |
| HMG Co-A reductase inhibitor | Myalgia/myositis | Mineral suplement, Quinine sulfate |
| HMG Co-A reductase inhibitor | Insomnia | Sleep agent |
| Digoxin | Nausea | Antiemetic |
| Midodrine | Hypertension | Antihypertensive |
| Central nervous system | ||
| Anticonvulsant | Rash | Topical corticosteroid |
| Anticonvulsant | Nausea | Antiemetic |
| Antipsychotic | Extrapyramidal symptoms | Beta-blocker, Antiparkinsonian agent, Anti-tremor antimuscarinic |
| Antipsychotic | Akathisia or tardive movements | Sedative |
| Antipsychotic | Arrhythmia | Antiarrhythmic |
| Antipsychotic | Hyperglycemia | Antihyperglycemic |
| Benzodiazepine | Cognitive impairment | Cholinesterase Inhibitor |
| Cholinesterase inhibitor | Urinary incontinence | Overactive bladder medication |
| Cholinesterase inhibitor | Insomnia | Sleep agent |
| Cholinesterase inhibitor | Gastrointestinal upset | Antiemetic, Bismuth subsalicylate |
| Cholinesterase inhibitor | Diarrhea | Antidiarrheal |
| Cholinesterase inhibitor | Rhinorrhea | Antihistamine |
| Dopaminergic Antiparkinsonian agent | Psychotic symptoms, hallucinations | Antipsychotic |
| Selective serotonin reuptake inhibitor/Serotonin and norepinephrine reuptake inhibitor (SSRI/SNRI) | Urinary Incontinence | Overactive bladder medication |
| Tricyclic antidepressant | Cognitive Impairment | Cholinesterase Inhibitor |
| Tricyclic antidepressant | Constipation | Laxative |
| Tricyclic antidepressant | Urinary incontinence | Overactive bladder medication |
| Flunarizine | Depression | Antidepressant |
| Lithium | Extrapyramidal symptoms | Antiparkinsonian agent |
| Venlafaxine | Hypertension (dose-related) | Antihypertensive |
| Venlafaxine | Tremor | Benzodiazepine |
| Anticholinergics | Dyspepsia/reflux (gastroesophageal reflux disease — ‘GERD’) | Proton pump inhibitor |
| Drug-induced movement disorders | Movement disorders | Antiparkinsonian drugs |
| Endocrine system | ||
| Dipeptidyl peptidase 4 (DPP-4) inhibitor (e.g., sitag- liptin, saxagliptin) | Joint pain | Nonsteroidal anti-inflammatory drug |
| Sodium-glucose cotransporter-2 (SGLT-2) inhibitor | Mycotic genital infections | Antifungal |
| Metformin | Diarrhea | Antidiarrheal |
| Pioglitazone or Rosiglitazone | Edema | Diuretic |
| Rosiglitazone | Heart failure | Diuretic |
| Gastrointestinal system | ||
| Anticholinergic antiemetic | Urinary retention | Alpha-1 receptor blocker |
| Antidopaminergic antiemetic | Extrapyramidal symptoms | Antiparkinsonian agent |
| Laxative | Diarrhea | Antidiarrheal agent |
| Proton pump inhibitor | Osteoporosis, fractures | Vitamin supplement |
| Proton pump inhibitor | Vitamin or Mineral Deficiency | Vitamin supplement |
| Musculoskeletal system | ||
| Bisphosphonate | Gastritis | Gastroprotective agent |
| Nonsteroidal anti-inflammatory drug (NSAID) | Gastritis/gastric ulcer/gastrointestinal bleed | Gastroprotective agent |
| NSAID | Nausea | Antiemetic |
| NSAID | Hypertension | Antihypertensive |
| NSAID | Worsening of heart failure | Heart failure agent |
| Opioid | Depression | Antidepressant |
| Urogenital system | ||
| Alpha-1 receptor blocker | Orthostatic hypotension, dizziness | Vestibular suppressant |
| Urinary anticholinergic | Dry mouth | Saliva substitute |
| Miscellaneous system | ||
| Carbapenem (e.g., imipenem, meropenem, ertapenem) | Seizures | Anticonvulsant |
| Corticosteroid | Insomnia | Sleep agent |
| Corticosteroid | Psychosis | Antipsychotic |
| Corticosteroid | Hypertension | Antihypertensive |
| Acitretin | Vulvo-vaginal candidiasis | Antifungal |
| Erythromycin | Arrhythmia | Antiarrhythmic |
| Fludrocortisone | Hypertension | Antihypertensive |
| Iron supplement | Constipation | Laxative |
Table 5.
Prescribing cascade assessment tool.
|
Existence of ADR, either expected or unknown: Doubtful 0 Yes 1 Yes, but misunderstood 2 |
|
Action followed against the ADR: Treatment discontinuation 0 Continued with dose reduction 1 Continued unchanged or with another drug of the same group 2 |
|
Existence of a second drug treatment for the ADR: No 0 Yes 1 |
|
Overall result of this new treatment: Patient improves 0 Patient worsens or remains unchanged 1 A new ADR appears 2 The new ADR requires a third drug treatment 3 |
Table 6.
Prescribing cascade benefit assessment tool.
| Does/did the precipitating drug cause or pose a risk for a clinically relevant adverse drug reaction? |
| Is the precipitating drug still indicated? |
| Can a treatment adjustment of the precipitating drug prevent adverse drug reactions |
| Can switching the precipitating drug prevent adverse drug reactions? |
| Can the second drug have a beneficial effect on adverse drug reactions? |
| Is the benefit–risk balance of the prescribing cascade positive? |
Table 7.
How to Prevent Prescribing Cascade – Table of Good Practice.
| Area | Principle / Clinical Practice |
| Oligopharmacotherapy | Use only absolutely essential medications. |
| Zero tolerance for unnecessary drugs | Eliminate therapies without clinical indications. |
| Contextual pharmacotherapy | Take into account comorbidities and the individual situation of the patient. |
| Patient assessment | Before introducing a new drug, evaluate the entire pharmacotherapy, risk of interactions, and potential adverse effects. |
| Deprescribing | Regularly discontinue unnecessary or harmful medications. |
| Adverse drug reactions | - First, consider discontinuing dietary supplements; - Limit unnecessary self-medication; - Respond immediately to new symptoms. |
| Informed patient | Educate the patient: treatment goals, risks of polypharmacy, and the need to report adverse effects. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



