
Submitted:
29 August 2023
Posted:
30 August 2023
You are already at the latest version
Abstract
Introduction: Drug interactions (DDIs) represent an important clinical problem particularly in elderly patients due to polytherapy, comorbidity and physiological change in pharmacodynamic and pharmacokinetic pathways. In this study we investigated the association between drugs prescribed during hospital or clinical room discharge and the development of DDIs with drugs daily used from each patient.
Methods: we performed an observational, retrospective, multicenter study on medical records of outpatients referred to general practitioners. Drug interactions (DDIs) were measured using the drug interactions probability scale. Collected data were analyzed using the Statistical Package for the Social Sciences. Results: During the study we evaluated 1,622 medical records. We recorded the development of DDIs in 10.3% of patients, of those 11.6% induced the hospitalization. Logistic regression showed an association between DDIs and sex and number of drugs used (P = 0.023). Conclusion: this real-life study shows that DDIs are common in elderly patients and physicians must take more attention after hospital discharge revaluating the treatment in order to reduce the risk of DDIs and hospitalization.
Keywords:
reconciliation
; deprescription
; elderly
; polytherapy
1. Introduction
Drug interactions (DDIs) represent an important clinical problem particularly in elderly patients due to polytherapy, multimorbidity and pharmacokinetic changes. Since a combination of drugs could be useful to manage multimorbidity, there is a risk of being prescribed potentially inappropriate medications, resulting in adverse drug reactions (ADRs), increased hospitalizations, and higher mortality [1].
Even if the role of advanced age on pharmacokinetic factors including gastrointestinal transit, pH, expression of metabolising enzymes and membrane transporters, permeability and the microbiome is limited [2], authors have documented some differences when compared with healthy adults [3], suggesting that age represent a risk factor for the development of ADRs (Table 1).
In elderly patients, comorbidity increases the risk of ADRs because induce a decrease in organ function and drug pharmacokinetic; on the other hand, the comorbidity induces an increase in drug consumption and or prescription with an increase in the development of DDIs [4,5] (Figure 1).
In this context, to reduce the risk of DDIs, drug prescription must be well evaluated also considering drugs or nutrients usually used. Several authors reported that medication errors (e.g., risk of duplication and DDIs) are common on hospital discharge due to ignorance of a patient’s current treatment, in which necessary information on outpatient medications is omitted [6,7,8].
This study aimed to investigate the association between drugs prescribed during the discharge from the hospital or clinical room and the development of DDIs with drugs daily used from each patient.
2. Materials and Methods
2.1. Study design
We conducted an observational retrospective and descriptive analysis using data recorded on medical records of outpatients referred to general practitioners of the ASP of Catanzaro (Italy) up to August 10, 2023.
2.2. Protocol
Data recorded in clinical records, including age, sex, ADRs (in agreement with the Naranjo probability score), morbidities, polytherapy, and laboratory findings, were analyzed in agreement with previous papers [9,10,11,12,13,14,15].
We collected information on several medical conditions and other clinical diagnostic events, e.g., cardiovascular, and respiratory diseases, diabetes, ostheoarthritis, metabolic and rheumatoid disorders, and hospitalizations.
In our study, clinical pharmacologists and neurologists retrospectively assessed each drug treatment. ADRs and DDIs were recorded in agreement with our previous studies [16,17,18,19,20]. The clinical research on possible drug interactions was performed using: https://intercheckweb.marionegri.it/; https://www.drug-pin.com/; www.druginteractions.org; https://janusinfo.se/; www.drugs.com
The drug interaction probability scale (DIPS) was used to evaluate the probability of a causal relationship between a potential drug interaction and an ADR. DIPS estimates the probability that an ADR was caused by an interaction; according to the total score of 10 questions, the relationship is doubtful (<2), possible (2–4), probable (5–8), or highly probable (> 8) [21].
The risk of DDIs was defined as: A (minor): not clinically relevant; B (moderate): associated with an uncertain or variable event; C (major): associated with a serious event but which can be managed (e.g., by adjusting the dose); D: (Contraindicated or Very Serious): associated with a serious event for which co-administration should be avoided or carefully monitored.
2.3. Inclusion and exclusion Criteria
Inclusion criteria were as follows: all patients of any age were enrolled. Data were included from patients who were 65 years of age or older at the time of their last office visit, had 2 documented visits in the outpatient primary care setting in the previous 2 years, and had been discharged from the hospital in the last year. Exclusion criteria included current residence in a skilled nursing facility, Alzheimer’s disease, and active cancer (if cancer is the cause of hospitalization).
2.4. Endpoints
The primary endpoint was the number of patients who developed drug interactions after hospital discharge. The secondary endpoint was the correlation between adverse drug reactions and drug interactions. Another secondary endpoint was the correlation between drug interactions and age, comorbidity, sex, and polytherapy.
2.5. Ethical considerations
The study was performed on clinical recorders of general practitioners; therefore, written informed consent was obtained from each general practitioner at the time of the first admission to the clinical room. All the procedures were performed according to the Declaration of Helsinki and in accordance with the Good Clinical Practice guidelines. The study protocol was approved by the local Ethics Committee, protocol number 2017/238.
2.6. Statistical analysis
Descriptive statistical analyses were performed to evaluate clinical and demographic characteristics, with continuous data presented as mean ± standard deviation (SD), while ordinal data expressed as number (percentage). Skewness of continuous variables was assessed by the Kolmogorov-Smirnov test, highlighting not normally distributed variables. Thus, a non-parametric approach was applied using the Mann- Whitney U test or the Independent-Samples Kruskal-Wallis Test for continuous variables and the two-tailed Pearson chi-squared test or the Fisher’s test for categorical variables as appropriate.
A p-value < 0.05 was considered as statistically significant. All tests were two-tailed. Statistical analysis was conducted with the Statistics Package for Social Sciences (SPSS) version 26.0 (IBM Corp. SPSS Statistics, Armonk, NY, USA).
3. Results
3.1. Demographic and clinical characteristics
During the study, we analyzed 10,596 clinical records. Using the paired sample test, we evaluated a significant difference (P<0.01) between men and women enrolled (men 4647, 43.9%; women, 5949, 56.1%), without regard to age (mean age total: 64.4 ± 16.6 years; range 19-100 years; men 64.4 ± 16.6 years; women 63.9 ± 17.8 years).
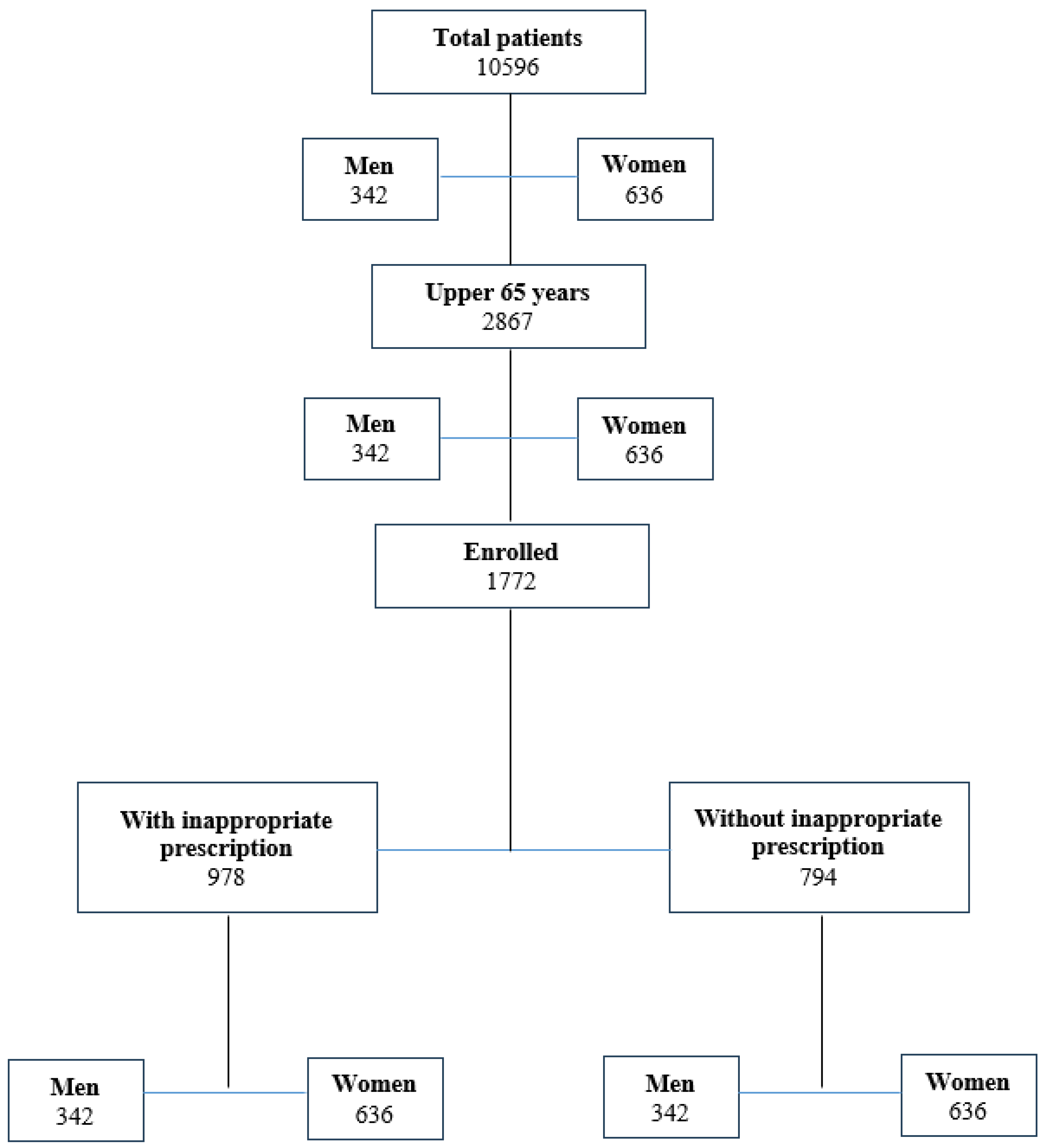
After inclusion criteria evaluation, 1772 patients (men 586, 33.1%, women 1186, 66.9%, P<0.01) aged 65 or older were enrolled (16.7%) (mean men 77.5 ± 7.7 years, women 77.2 ± 8.2 years, P>0.05) (Figure 2).
Of the 1772 enrolled patients, all patients at least one morbidity; the most common were cardiovascular diseases (82.3%; encloding blood hypertension and atrial fibrillation) and osteoarthritis (79.5%) (Table 2). The mean number of drugs daily used was 6 (range 3–12), with a mean of 5 tablets every day. The demographic characteristics of the enrolled patients are described in Table 3. All enrolled patients showed similar gender characteristics: Race (white), geographic region (Calabria, Italy), setting (urban), job (retirees), religion (Catholic).
Figure 2.
Flow-chart showing enrolled patients.
3.2. Inappropriate drug prescription
Clinical research performed through both PC software and clinical pharmacologist and neurologist consultants documented that, after hospital discharge (n: 1772), 55.2% of enrolled patients (n: 978) did not receive potentially inappropriate medications, while 44.8% (n: 794) received inappropriate prescription (P<0.01) able to induce potential DDIs (pDDIs).
3.3. DIPS score
Using the DIPS, we documented that ADRs were probable induced by DDIs (DIPS score 6-7). It is important to understand that we did not consider the rechallenge and we considered the elderly as a factor able to explain the ADR.
3.4. Risk evaluation
Both univariate and multivariate analyses show that both age and the number of chronic drugs are associated with an increasing risk of DDIs. The adjusted OR increased from 0.9 (95% CI 0.7–1.03) in patients aged 65–75 years to 1.09 (95% CI 1.05–1.22) in patients aged 76–85 years to 1.79 (95% CI 1.56–1.95) in those aged 85 or older. Patients treated with 3–5 chronic drugs have a lower risk (OR = 2.93; 95% CI 2.83–3.08). of pDDIs (OR = 5.69; 95% CI 5.58–5.91) than those receiving more than five chronic drugs. Finally, we documented that women have a statistically significant higher risk of developing pDDIs (OR = 2.85; 95% CI 2.37–3.46) than men (OR = 1.25; 95% CI 1.08–1.42).
4. Discussion
Elderly patients show physiological changes that must be taken into consideration when other drugs are administered or prescribed to reduce the risk of ADRs. This is important because the common biomarkers commonly used to evaluate kidney activity in elderly patients can't be used. Despite the decline of glomerular filtration rate with age [22], there is no concomitant increase in plasma creatinine because of age-related loss of muscle mass. Creatinine isn't a reliable indicator of glomerular filtration rate in the elderly subject, and there is the risk that the concomitant administration of drugs excreted from the kidney (e.g., NSAIDs, some opioids, benzodiazepines) increases the risk of renal failure and ADRs.
In elderly patients, careful monitoring of polytherapy is necessary to reduce the risk of potentially inappropriate drug prescriptions that could induce DDIs. Polytherapy represents a criterion of frailty in the elderly and a risk factor for mortality and morbidity due to the increased risk of DDIs, ADRs (risk of falls and cognitive impairment), and greater use of health resources [23]. In our study, we demonstrated that adults aged 65 years and older take a mean of 5 tablets every day with an increased risk of pDDIs. Considering the comorbidities, we documented that all patients have more than one comorbidity, particularly cardiovascular diseases, and osteoarthritis. In these cases, pharmacological treatment must be evaluated due to the risk of pharmacodynamic pDDIs (e.g., Ace inhibitors and NSAIDs) with a decrease in blood pressure control.
In our study we recorded that the most common group of drugs involved in pDDIs were omeprazole and esomeprazole. The 2021 National Report on Medicines use in Italy, prepared by AIFA's Medicines Utilisation Monitoring Centre (OsMed), documented that proton pump inhibitors represent a group of drugs commonly prescribed, and we reported that this prescription is common during the discharge. Previously, we documented that omeprazole and esomeprazole are able to induce ADRs during hospitalization [24]. Now, we document that these drugs are involved in 198 pDDIs, even if we only recorded clinically relevant DDIs in 10 patients.
Interestingly, we documented that two patients with rheumatoid arthritis who were in treatment with methotrexate received a prescription of omeprazole. In these patients, an increase in methotrexate plasma levels was recorded due to the inhibition of the renal H+/K+ pump, with a decrease in excretion of methotrexate. This interaction (D class, DIPS: 7) is common to all proton pump inhibitors (omeprazole, esomeprazole, lansoprazole, rabeprazole and pantoprazole), so it is necessary to stop the drugs three days before the methotrexate administration or change it with a histamine H2 receptor antagonist (e.g., famotidine, which does not affect drug metabolism and is free of the antiandrogenic effects)
Other interactions of omeprazole or esomeprazole with drugs described in Table 4 and Table 5 (n: 199), did not induce any clinical effect (possible QT increase; C class).
A group of drugs commonly used in clinical practice for the prevention of heart disease, or its treatment is represented by statins. In our study, simvastatin and atorvastatin have been involved in 159 pDDIs without clinical effects. However, in 5 patients discharged on atorvastatin we documented the development of myalgia during the coadministrations with clarithromycin (C class, 1 patient) and sildenafil (D class, 4 patients).
These pDDIs are described in clinical settings [25,26,27,28] and is related to the inhibition of cytochrome P450 (CYP) 3A4. Therefore, in these patients, we suggest changing the type of statin (using statins not metabolized by CYP3A4, e.g., rosuvastatin, high potency, or pravastatin, low potency) or changing the type of antimicrobial drug (e.g., azithromycin) or phosphodiesterase-5 inhibitor (e.g., vardenafil). However, as reported in Table 7, other compounds can modify the activity of CYP3A4, increasing (inhibitors) or reducing (inductors) the blood concentration of statins (atorvastatin, lovastatin, simvastatin), and these must be considered during the hospital discharge.
We documented the pDDIs between clopidogrel and omeprazole (n: 7) or esomeprazole (n:1) who had been hospitalized due to the low effectiveness of clopidogrel. Clopidogrel is a prodrug that is biotransformed in the liver via CYP2C19 into an active metabolite that binds irreversibly to platelet ADP receptor P2Y12, preventing ADP-induced platelet aggregation [29]. Omeprazole, lansoprazole, and esomeprazole inhibit CYP2C19, reducing the antiplatelet effect of clopidogrel [30].
To reduce the risk of DDIs in elderly patients, we suggest using proton pump inhibitors without effects on CYP (e.g., pantoprazole). The same mechanism involves the DDIs of clopidogrel with fluoxetine (n: 5), therefore, it is useful to use SSRIs without action on CYP3A4 (e.g., sertraline, citalopram, and escitalopram).
Another group of drugs that must be evaluated during discharge are antibiotics. In fact, given the relative short duration of antibiotic treatments (usually less than 7–10 days), concomitant treatments are not considered in the choice of the antibiotic. Kusku et al. [31] documented in a multicentric study that quinolones, metronidazole, linezolid, and clarithromycin were responsible for 92% of the reported DDIs. Other authors documented that, in patients referred to intensive care units, the DDIs due to quinolones were associated with QT prolongation [32], suggesting particular attention during the prescription. Moreover, other authors reported that ciprofloxacin inhibits CYP1A2, with an increase in the blood concentration of victim drugs (e.g., olanzapine and tizandine) and an increase in ADRs (e.g., QT prolongation and somnolence, respectively) [33,34].
In our study, we documented 87 pDDIs in elderly patients with a prescription of ciprofloxacin or levofloxacin without clinical effects.
Only 1 patient treated with levofloxacin for acute exacerbations of chronic obstructive pulmonary disease was hospitalized for a QT prolongation due to a DDI with Lenvatinib (D class). Lenvatinib is an oral active tyrosine kinase inhibitor that represents a promising targeted therapeutic for several types of cancer [35]. Lenvatinib is metabolized by CYP1A1 and CYP3A4, so strong inducers or inhibitors of these CYPs could pose a risk of DDIs, potentially resulting in a reduction in anticancer efficacy or an increase in drug-related toxicity [36]. A QT interval prolongation was also reported in 3 patients hospitalized for a DDI between citalopram (n: 2) or escitalopram (n: 1) and Lenvatinib. The analysis of DDIs suggests that it is not related to a pharmacokinetic DDI but to a potentiation of their ADRs (QT prolongation). In fact, Shah and Morganroth [37], reviewing literature data, documented that lenvatinib can induce QT interval prolongation, left ventricular dysfunction, and hypertension. QT interval prolongation represents the risk of a pDDI that we recorded during the prescription of citalopram (and SSRIs) in patients treated with amitriptyline (C class). However, we also demonstrated a pDDI after the prescription of SSRIs in patients using NSAIDs, amitriptyline, triptans, or tramadol. SSRIs increases the levels of serotonin, and together with other drugs able to do it (tramadol and triptans), they can induce the development of serotonin toxicity (C and D classes, respectively). Nelson and Philbrick [38] documented the risk of an interaction between tramadol and SSRIs related to an increase in serotonin toxicity. Moreover, in our study, we documented an interaction (C class) between amytriptiline and tramadol. Even if this interaction could be related to a pharmacodynamic DDI, due to the increase in serotonin concentrations, it is also possible to have a pharmacokinetic DDI. In fact, the main metabolic pathway of tramadol is through the CYP 2D6 enzymes, which may be partially inhibited by amitriptyline, with an increase in tramadol concentration and in serotonin effects. In our study, we documented the prescription of fluoxetine in patients treated with triptans for headache management. Even if it is a D class DDI, we did not record any hospitalization in these patients, probably due to the low duration of treatment with triptans (e.g., sumatriptan, frovatriptan), even if we are not able to demonstrate this.
Another pDDI recorded during the study was related to the prescription of paroxetine or fluoxetine (n: 6) in patients with autoprescription of diclofenac for pain treatment. This is a C class DDI, and Anglin et al., [39] in a meta-analysis of 19 observational studies, reported an increase in gastrointestinal bleeding rates in patients using both SSRIs and NSAIDs compared to non-users (OR 4.25, 95% CI 2.82–6.42). More recently, Haghbin et al. [40], in a systematic review and network meta-analysis, documented an increased risk of gastrointestinal bleeding in patients treated with SSRI and NSAIDs, compared to patients treated with SSRI alone (36.9% vs. 22.8%, OR 2.14, 95% CI 1.52–3.02, p<0.001), or with NSAIDs alone (40.9% vs 34.2%, OR 1.49, 95% CI 1.20–1.84, p<0.001), suggesting caution when administering NSAIDs and SSRIs concurrently.
Another cause of severe bleeding may be the association of NSAIDs with enoxaheparin due to pharmacodynamic mechanisms (C class). In our study, we documented this pDDI in 8 patients, but we failed to document the development of ADRs. However, we suggest avoiding these drugs together. In the presence of coadminsitraton, we suggest carefully monitoring the clinical conditions.
Finally, we need to pay attention during the pain treatment. In fact, we recorded 2 prescriptions of tramadol and 3 of tapentadol for pain management in patients using oxycodone (C class) that required careful observation. Moreover, we documented four prescriptions of tramadol and oxycodone in patients using at-home benzodiazepines (C class). Even if in our study these DDIs did not induce the development of ADRs, the respiratory function must be evaluated as well as the comorbidity (e.g., chronic obstructive respiratory disease, overlap sleep syndrome) to reduce the risk of respiratory failure.
Statistical evaluation documented a significant correlation between pDDIs, age, number of drug use, and sex (women), but we failed to document a correlation with gender because the population was enrolled in the same country without differences with respect to country, race (all patients were white), economy (all patients were retirees and worked in public offices or in the countryside), or religion (all people were Catholics).
As previously reported, the number of drugs used increases the possibility of drug pharmacokinetic and pharmacodynamic drug interactions [4]. Regarding sex, Zucker and Prendergast [41] documented that women are exposed to higher blood drug concentrations and longer drug elimination times than men, and this could explain the difference in drug safety between the sexes. Even if we are not able to demonstrate the difference in drug concentrations between men and women (this is a retrospective study), our data suggest that women show a high risk, so careful monitoring is suggested for elderly women.
Our study has some limitations related to the design (data recorded on clinical records) and the use of software. In fact, since the use of computerized software is highly desirable, its value depends on both its sensitivity (in detecting DDIs) and accuracy (in assessing the type and severity of DDIs). However, it is important to highlight that the evaluation of DDIs was performed by specialists in this topic. We think that an approach to the management of these pDDIs might be represented by a clinical pharmacology consult at the bedside before discharge that, involving the caregiver and the general practitioner and using drug interaction software and therapeutic drug monitoring, could reduce the risk of new hospitalizations in this group of patients. However, it is important that physicians and general practitioners take the time for the discussion with caregivers and with patients, considering lowering doses and deprescribing where possible.
Author Contributions
C.V., A.S., V.R. C.G., A.C., L.C.: conceptualization, data curation, software; G.M., C.P.: write the original version; A.S., C.G., R.C.: Validation; L.G., B.D., G.D.S.: Formal Analysis, review and editing; I.G., M.L., L.M., G.N., A.S., R.C.B., I.F., A.G., G.L.: Investigation.
Acknowledgments
This research received no funding.
Conflicts of Interest
All other authors have no conflicts to declare.
References
- Wastesson, J.W.; Morin, L.; Tan, E.C.K.; Johnell, K. An update on the clinical consequences of polypharmacy in older adults: A narrative review. Expert Opin. Drug Saf. 2018, 17, 1185–1196. [CrossRef]
- Khan, M.S.; Roberts, M.S. Challenges and innovations of drug delivery in older age. Adv. Drug Deliv. Rev. 2018, 135, 3–38. [CrossRef]
- Mangoni, A.A.; Jackson, S.H.D. Age-related changes in pharmacokinetics and pharmacodynamics: Basic principles and practical applications. Br. J. Clin. Pharmacol. 2004, 57, 6–14. [CrossRef]
- Palleria, C.; Di Paolo, A.; Giofrè, C.; Caglioti, C.; Leuzzi, G.; Siniscalchi, A.; De Sarro, G.; Gallelli, L. Pharmacokinetic drug-drug interaction and their implication in clinical management. J. Res. Med. Sci. 2013, 18, 601–610.
- Di Mizio, G.; Marcianò, G.; Palleria, C.; Muraca, L.; Rania, V.; Roberti, R.; Spaziano, G.; Piscopo, A.; Ciconte, V.; Nunno, N. Di; et al. Drug – Drug Interactions in Vestibular Diseases , Clinical Problems , and Medico-Legal Implications. Int. J. Environ. Res. Public Health 2021, 18, 12936. [CrossRef]
- Breuker, C.; Macioce, V.; Mura, T.; Castet-Nicolas, A.; Audurier, Y.; Boegner, C.; Jalabert, A.; Villiet, M.; Avignon, A.; Sultan, A. Medication Errors at Hospital Admission and Discharge. J. Patient Saf. 2017, Publish Ah, 1–8. [CrossRef]
- Andreoli, L.; Alexandra, J.F.; Tesmoingt, C.; Eerdekens, C.; Macrez, A.; Papo, T.; Arnaud, P.; Papy, E. Medication reconciliation: A prospective study in an internal medicine unit. Drugs and Aging 2014, 31, 387–393. [CrossRef]
- Chiewchantanakit, D.; Meakchai, A.; Pituchaturont, N.; Dilokthornsakul, P.; Dhippayom, T. The effectiveness of medication reconciliation to prevent medication error: A systematic review and meta-analysis. Res. Soc. Adm. Pharm. 2020, 16, 886–894. [CrossRef]
- Gallelli, L.; Cione, E.; Siniscalchi, A.; Vasta, G.; Guerra, A.; Scaramuzzino, A.; Longo, L.; Muraca, L.; De Sarro, G.; Group, G.S.W.; et al. Is there a Link between Non Melanoma Skin Cancer and Hydrochlorothiazide? Curr Drug Saf 2022, 17, 211–216. [CrossRef]
- Staltari, O.; Cilurzo, F.; Caroleo, B.; Greco, A.; Corasaniti, F.; Genovesi, M.; Gallelli, L. Annual report on adverse events related with vaccines use in Calabria (Italy): 2012. J. Pharmacol. Pharmacother. 2013, 4, 61–65. [CrossRef]
- Rende, P.; Paletta, L.; Gallelli, G.; Raffaele, G.; Natale, V.; Brissa, N.; Costa, C.; Gratteri, S.; Giofrè, C.; Gallelli, L. Retrospective evaluation of adverse drug reactions induced by antihypertensive treatment. J. Pharmacol. Pharmacother. 2013, 4, 47–50. [CrossRef]
- Zanon, D.; Gallelli, L.; Rovere, F.; Paparazzo, R.; Maximova, N.; Lazzerini, M.; Reale, A.; Corsetti, T.; Renna, S.; Emanueli, T.; et al. Off-label prescribing patterns of antiemetics in children: A multicenter study in Italy. Eur. J. Pediatr. 2013, 172, 361–367. [CrossRef]
- Caglioti, A.; Rania, V.; Vocca, C.; Marcianò, G.; Arcidiacono, V.; Catarisano, L.; Casarella, A.; Basile, E.; Colosimo, M.; Palleria, C.; et al. Effectiveness and Safety of ANTI SARS-CoV-2 Vaccination in Transplant Patients Treated with Immunosuppressants: A Real-World Pilot Study with a 1-Year Follow-Up. Appl. Sci. 2022, 12, 1–8. [CrossRef]
- Gallelli, L.; Ferreri, G.; Colosimo, M.; Pirritano, D.; Flocco, M.A.; Pelaia, G.; Maselli, R.; De Sarro, G.B. Retrospective analysis of adverse drug reactions to bronchodilators observed in two pulmonary divisions of Catanzaro, Italy. Pharmacol. Res. 2003, 47, 493–499. [CrossRef]
- Gallelli, L.; Colosimo, M.; Pirritano, D.; Ferraro, M.; De Fazio, S.; Marigliano, N.M.; De Sarro, G. Retrospective evaluation of adverse drug reactions induced by nonsteroidal anti-inflammatory drugs. Clin. Drug Investig. 2007, 27, 115–122. [CrossRef]
- Gallelli, L.; Ferreri, G.; Colosimo, M.; Pirritano, D.; Guadagnino, L.; Pelaia, G.; Maselli, R.; De Sarro, G.B. Adverse drug reactions to antibiotics observed in two pulmonology divisions of Catanzaro, Italy: A six-year retrospective study. Pharmacol. Res. 2002, 46, 395–400. [CrossRef]
- Gallelli, L.; Nardi, M.; Prantera, T.; Barbera, S.; Raffaele, M.; Arminio, D.; Pirritano, D.; Colosimo, M.; Maselli, R.; Pelaia, G.; et al. Retrospective analysis of adverse drug reactions induced by gemcitabine treatment in patients with non-small cell lung cancer. Pharmacol. Res. 2004, 49, 259–263. [CrossRef]
- Muraca, L.; Scuteri, A.; Burdino, E.; Marcianò, G.; Rania, V.; Catarisano, L.; Casarella, A.; Cione, E.; Palleria, C.; Colosimo, M.; et al. Effectiveness and Safety of a New Nutrient Fixed Combination Containing Pollen Extract plus Teupolioside, in the Management of LUTS in Patients with Benign Prostatic Hypertrophy: A Pilot Study. Life 2022, 12, 965. [CrossRef]
- Gallelli, G.; Di Mizio, G.; Palleria, C.; Siniscalchi, A.; Rubino, P.; Muraca, L.; Cione, E.; Salerno, M.; De Sarro, G.; Gallelli, L. Data recorded in real life support the safety of nattokinase in patients with vascular diseases. Nutrients 2021, 13, 2031. [CrossRef]
- Gareri, P.; Gallelli, L.; Cotroneo, A.M.; Manfredi, V.G.L.; De Sarro, G. The art of safe and judicious deprescribing in an elderly patient: A case report. Geriatr. 2020, 5, 57. [CrossRef]
- Horn, J.R.; Hansten, P.D.; Chan, L.N. Proposal for a new tool to evaluate drug interaction cases. Ann. Pharmacother. 2007, 41, 674–680. [CrossRef]
- DAVIES, D.F.; SHOCK, N.W. Age changes in glomerular filtration rate, effective renal plasma flow, and tubular excretory capacity in adult males. J. Clin. Invest. 1950, 29, 496–507. [CrossRef]
- Garrido-Garrido, E.M.; García-Garrido, I.; García-López-Durán, J.C.; García-Jiménez, F.; Ortega-López, I.; Bueno-Cavanillas, A. Estudio de pacientes polimedicados mayores de 65 años en un centro de asistencia primaria urbano. Rev. Calid. Asist. 2011, 26, 90–96. [CrossRef]
- Gallelli, L.; Siniscalchi, A.; Palleria, C.; Mumoli, L.; Staltari, O.; Squillace, A.; Maida, F.; Russo, E.; Gratteri, S.; De Sarro, G.; et al. Adverse drug reactions related to drug administration in hospitalized patients. Curr. Drug Saf. 2017, 12, 171–177. [CrossRef]
- Kunakorntham, P.; Pattanaprateep, O.; Dejthevaporn, C.; Thammasudjarit, R.; Thakkinstian, A. Detection of statin-induced rhabdomyolysis and muscular related adverse events through data mining technique. BMC Med. Inform. Decis. Mak. 2022, 22, 1–14. [CrossRef]
- Hughes, J.E.; Russo, V.; Walsh, C.; Menditto, E.; Bennett, K.; Cahir, C. Prevalence and Factors Associated with Potential Drug-Drug Interactions in Older Community-Dwelling Adults: A Prospective Cohort Study. Drugs and Aging 2021, 38, 1025–1037. [CrossRef]
- Blom, D.J.; Hala, T.; Bolognese, M.; Lillestol, M.J.; Toth, P.D.; Burgess, L.; Ceska, R.; Roth, E.; Koren, M.J.; Ballantyne, C.M.; et al. A 52-Week Placebo-Controlled Trial of Evolocumab in Hyperlipidemia. N. Engl. J. Med. 2014, 370, 1809–1819. [CrossRef]
- Montastruc, J.-L. Rhabdomyolysis and statins A pharmacovigilance comparative study between statins. Br J Clin Pharmacol 2023, 89, 2636–2638. [CrossRef]
- Cuisset, T.; Frere, C.; Quilici, J.; Poyet, R.; Gaborit, B.; Bali, L.; Brissy, O.; Morange, P.E.; Alessi, M.C.; Bonnet, J.L. Comparison of Omeprazole and Pantoprazole Influence on a High 150-mg Clopidogrel Maintenance Dose. The PACA (Proton Pump Inhibitors And Clopidogrel Association) Prospective Randomized Study. J. Am. Coll. Cardiol. 2009, 54, 1149–1153. [CrossRef]
- Zou, J.J.; Chen, S.L.; Tan, J.; Lin, G.; Zhao, Y.Y.; Xu, H.M.; Lin, S.; Zhang, J.; Fan, H.W.; Xie, H.G. Increased risk for developing major adverse cardiovascular events in stented Chinese patients treated with dual antiplatelet therapy after concomitant use of the proton pump inhibitor. PLoS ONE 2014, 9, 1–6. [CrossRef]
- Kuscu, F.; Ulu, A.; Inal, A.S.; Suntur, B.M.; Aydemir, H.; Gul, S.; Ecemis, K.; Komur, S.; Kurtaran, B.; Kuscu, O.O.; et al. Potential drug–drug interactions with antimicrobials in hospitalized patients: A multicenter point-prevalence study. Med. Sci. Monit. 2018, 24, 4240–4247. [CrossRef]
- Bakker, T.; Dongelmans, D.A.; Nabovati, E.; Eslami, S.; de Keizer, N.F.; Abu-Hanna, A.; Klopotowska, J.E. Heterogeneity in the Identification of Potential Drug-Drug Interactions in the Intensive Care Unit: A Systematic Review, Critical Appraisal, and Reporting Recommendations. J. Clin. Pharmacol. 2022, 62, 706–720. [CrossRef]
- Bolhuis, M.S.; Panday, P.N.; Pranger, A.D.; Kosterink, J.G.W.; Alffenaar, J.W.C. Pharmacokinetic drug interactions of antimicrobial drugs: A systematic review on oxazolidinones, rifamycines, macrolides, fluoroquinolones, and beta-lactams. Pharmaceutics 2011, 3, 865–913. [CrossRef]
- Cattaneo, D.; Gervasoni, C.; Corona, A. The Issue of Pharmacokinetic-Driven Drug-Drug Interactions of Antibiotics: A Narrative Review. Antibiotics 2022, 11, 1–17. [CrossRef]
- Glen, H.; Mason, S.; Patel, H.; Macleod, K.; Brunton, V.G. E7080, a multi-targeted tyrosine kinase inhibitor suppresses tumor cell migration and invasion. BMC Cancer 2011, 11, 309. [CrossRef]
- Vavrová, K.; Indra, R.; Pompach, P.; Heger, Z.; Hodek, P. The impact of individual human cytochrome P450 enzymes on oxidative metabolism of anticancer drug lenvatinib. Biomed. Pharmacother. 2022, 145. [CrossRef]
- Shah, R.R.; Morganroth, J. Update on Cardiovascular Safety of Tyrosine Kinase Inhibitors: With a Special Focus on QT Interval, Left Ventricular Dysfunction and Overall Risk/Benefit. Drug Saf. 2015, 38, 693–710. [CrossRef]
- Nelson, E.M.; Philbrick, A.M. Avoiding serotonin syndrome: The nature of the interaction between tramadol and selective serotonin reuptake inhibitors. Ann. Pharmacother. 2012, 46, 1712–1716. [CrossRef]
- Anglin, R.; Yuan, Y.; Moayyedi, P.; Tse, F.; Armstrong, D.; Leontiadis, G.I. Risk of upper gastrointestinal bleeding with selective serotonin reuptake inhibitors with or without concurrent nonsteroidal anti-inflammatory use: A systematic review and meta-analysis. Am. J. Gastroenterol. 2014, 109, 811–819. [CrossRef]
- Haghbin, H.; Zakirkhodjaev, N.; Husain, F.F.; Lee-Smith, W.; Aziz, M. Risk of Gastrointestinal Bleeding with Concurrent Use of NSAID and SSRI: A Systematic Review and Network Meta-Analysis. Dig Dis Sci 2023, 68, 1975–1982. [CrossRef]
- Zucker, I.; Prendergast, B.J. Sex differences in pharmacokinetics predict adverse drug reactions in women. Biol. Sex Differ. 2020, 11, 32. [CrossRef]
Figure 1.
Schematic representation of the risk of polytherapy during hospitalization Each specialist gives a different drug to treat a patient's morbidity with a daily house treatment.
Figure 1.
Schematic representation of the risk of polytherapy during hospitalization Each specialist gives a different drug to treat a patient's morbidity with a daily house treatment.


Table 1.
Physiologic pharmacokinetic change in elderly patients. ADRs: adverse drug reactions.
| Phase | Change | Effect | Clinical risk |
|---|---|---|---|
| Absorption | Reduced active transport mechanisms | Reduced absorption of magnesium, calcium, iron, vitamin B 12 | Increased risk of osteopenia, osteoporosis, anemia |
| Reduced P-glycoprotein activity | Increased absorption of victim drugs | Development of ADRs | |
| reduced amount of dopadecarboxylase in the gastric mucosa | Increased absorption of levodopa | Development of ADRs | |
| Decreased secretion of secretion of hydrochloric acid and pepsin | Reduced absorption of basic drugs | Risk of undertreatment | |
| Distribution | polar drugs (water-soluble) have smaller volumes of distribution | Increased serum levels (eg., Gentamicin, digoxin, ethanol, theophylline, and cimetidine) | Development of ADRs |
| nonpolar drugs (lipid-soluble) have higher volumes of distribution | Increased in half life (eg., diazepam, thiopentone, lignocaine, and chlormethiazole) | Development of ADRs | |
| Metaboolism | reduction in first-pass metabolism | Increased bioavailability of drug undergoing extensive first-pass metabolism. Reduced bioavailability of pro-drugs | Increased risk of ADRs from propranolol and labetalol. Rediuced clinical effects of several pro-drugs (eg., enalapril and perindopril) |
| Renal Excretion | Reduced renal plasma flow and glomerular filtration rate | Reduced renal excretion | Development of ADRs |
Table 2.
Morbidity in patients enrolled in this study Data are expressed as a percentage of enrolled patients (n.1346).
Table 2.
Morbidity in patients enrolled in this study Data are expressed as a percentage of enrolled patients (n.1346).
| Disease | Percentage |
|---|---|
| Cardiovascular diseases (Blood Hypertension, Atrial fibrillation) |
82.3 |
| Osteoarthritis | 79.5 |
| Diabeted mellitus type 2 | 26.2 |
| Depression | 18.7 |
| Impaired cognition, dementia | 16.8 |
| Gastroesophageal reflux disease | 13.3 |
| Urological diseases | 12.8 |
| COPD | 8.4 |
| Rheumatological diseases | 6.9 |
| Osteoporosis or osteopenia | 4.8 |
| Asthma | 1.2 |
| Hypothiroidism | 1.1 |
| Other | 1.6 |
Table 3.
The demographic characteristics of the enrolled patients (n. 1772) with and without potentially inappropriate prescriptions (PIP) were evaluated after hospital discharge. The data are expressed as percentages with respect to the enrolled patients. *P<0.01 women vs men. §P<0.01 women with PIP vs Women without PIP.
Table 3.
The demographic characteristics of the enrolled patients (n. 1772) with and without potentially inappropriate prescriptions (PIP) were evaluated after hospital discharge. The data are expressed as percentages with respect to the enrolled patients. *P<0.01 women vs men. §P<0.01 women with PIP vs Women without PIP.
| Characteristics | With PIP (n:794) | Without PIP (n: 552) |
|---|---|---|
| Age (mean ± SD) | 76.3±7.3 | 76.8±8.5 |
| Men (%) | 41.3 | 46.6 |
| Women (%) | 58.7*§ | 53.4* |
| Current Smokers (%) | 5.2 | 4.8 |
| Overweight (%) | 53.6 | 52.8 |
| Chronic diseases (mean ± SD) | 4±2 | 5±2 |
Table 4.
Inappropriate drug prescription during hospital discharge, in enrolled patients (n 794). Data are expressed as percentage respect to the enrolled patients and absolute number. SSRIs, Serotonin selective reuptake inhibitors, SNRIs, Serotonin Noradrenalin reuptake inhibitors; NSAIDs: non-steroidal antinflammatory drugs.
Table 4.
Inappropriate drug prescription during hospital discharge, in enrolled patients (n 794). Data are expressed as percentage respect to the enrolled patients and absolute number. SSRIs, Serotonin selective reuptake inhibitors, SNRIs, Serotonin Noradrenalin reuptake inhibitors; NSAIDs: non-steroidal antinflammatory drugs.
| Drugs | Percentage | number |
|---|---|---|
| Omeprazole and esomeprazole | 25 | 199 |
| Atorvastatin and Simvastatin | 20 | 159 |
| Clopidogrel | 12,9 | 102 |
| Ciprofloxacin and levofloxacin | 11 | 87 |
| SSRIs | 10,1 | 80 |
| Opioids | 9 | 71 |
| SNRIs | 6 | 48 |
| Benzodiazepines | 3 | 24 |
| NSAIDs | 3 | 24 |
Table 5.
Potential drug interactions in enrolled patients (n 794). In parenthesis the number of patients using the drugs. SSRIs, Serotonin selective reuptake inhibitors, SNRIs, Serotonin Noradrenalin reuptake inhibitors; NSAIDs: non-steroidal antinflammatory drugs.
Table 5.
Potential drug interactions in enrolled patients (n 794). In parenthesis the number of patients using the drugs. SSRIs, Serotonin selective reuptake inhibitors, SNRIs, Serotonin Noradrenalin reuptake inhibitors; NSAIDs: non-steroidal antinflammatory drugs.
| Drugs prescribed during hospital discharge | Drugs in therapy |
|---|---|
| Omeprazole and esomeprazole | citalopram (28), escitalopram (26), venlafaxine (25), tramadol (21), trazodone (12), aripiprazole (11), tizanidine (10), alfuzosine (9), domperidone (9), ciprofloxacin (9), amiodarone (9), vardenafil (8), levofloxacin (7), haloperidol (6), clopidogrel (5), moxifloxacin (4) |
| Atorvastatin or Simvastatin | esomeprazole (59), amlodipine (16), Sacubitril Valsartan (14), sitagliptin (12), ranolazine (9), amiodarone (9), tadalafil (8), dronedarone (6), warfarin (6), sildenafil (6), clopidogrel (3), diltiazem (3), ticagrelor (3), carbamazepine (2), everolimus (2), domperidone (1) |
| Clopidogrel | Omeprazole (22), esomeprazole (18), lansoprazole (16), rosuvastatin (12), repaglinide (9), fluoxetine (6), paroxetine (5), tramadol (5), tapentadol (4), venlafaxine (3), amiodarone (2), |
| Ciprofloxacin and evofloxacin | escitalopram (14), duloxetine (9), venlafaxine (6), tramadol (4), |
| omeprazole (10), metformin (9), simvastatin (7), betamethasone (3), paroxetine (3), fluoxetine (3), warfarin (2), furosemide (2), propafenone (1), ranolazine (1), zolpidem (1) | |
| diclofenac (6), ibuprofen (4), dutasteride (2) | |
| Fluoxetine and paroxetine | rivaroxaban (6), apixaban (4), dabigatran (4), diclofenac (6), clopidogrel (6), tizanidine (4), tramadol (4), triazolam (3), frovatriptan (3), furosemide (2), trazodone (2), oxycodone (2), triazolam (2), amiodarone (2), almotriptan (1), eletriptan (1) |
| Citalopram and escitalopram | omeprazole (7), tramadol (3), tizanidine (3), apixaban (2), trazodone (2), diclofenac (2), ibuprofen (2), ketoprofen (2), amitriptyline (2), buprenorphine (2), almotriptan (1) |
| Tramadol | omeprazole (7), gabapentin (7), paroxetine (6), amytriptiline (6), duloxetine (4), fluoxetine (2), oxycodone (2), alprazolam (1), diazepam (1) |
| Tapentadol | citalopram (6), escitalopram (3), paroxetine (3), Oxycodone (3), almotriptan (2), trazodone (2), sertraline (2), risperidone (2) |
| Oxycodone | escitalopram (6), paroxetine (3), Triazolam (2), gabapentin (1) |
| Venlafaxine | omeprazole (9), esomeprazole (9) flecainide (6), ciprofloxacina (5), azythromicin (4), zolmitriptan (2) buprenorphine (1) |
| Duloxetine | Trazodone (3), clobazam (2), rozatriptan (2), naproxene (2), etoricoxib (1) |
| Diazepam | omeprazole (16), tramadol (4), tapentadol (2), olanzapine (2) |
| Alprazolam and triazolam | tramadol (2) |
| Diclofenac and ketorolac | enoxaparin (8), venlafaxine (5), valsartan (5), furosemide (4), levofloxacin (2), |
Table 6.
Drug interactions, n: 24, recorded in the study requiring hospitalization. DIPS Drug interaction probability scale. Drug 1 is the drug prescribed during the discharge, Drug 2 is the drug commonly used at home.
Table 6.
Drug interactions, n: 24, recorded in the study requiring hospitalization. DIPS Drug interaction probability scale. Drug 1 is the drug prescribed during the discharge, Drug 2 is the drug commonly used at home.
| Drug 1 | Drug 2 | ADRs | Mechanism | Action | N patients | DIPS score |
|---|---|---|---|---|---|---|
| Citalopram 20 mg once day | Lenvatinib 10 mg once day | Increase in heart rate | QT interval prolongation | Change citalopram to duloxetine | 2 | 6 |
| Esitalopram 20 mg once day | Lenvatinib 10 mg once day | Increase in heart rate | QT interval prolongation | Change escitalopram to duloxetine | 1 | 6 |
| Levofloxacin 500 mg once day | Lenvatinib 10 mg once day | Increase in heart rate | QT interval prolongation | Change Levofloxacin to Piperacillin/tazobactam | 1 | 6 |
| Clopidogrel 75 mg once day | Omeprazole 40 mg once day | Decreased activity of clopidogrel | Reduced liver activation of clopidogrel | Change omeprazole to pantoprazole | 7 | 6 |
| Clopidogrel 75 mg once day | Esomeprazole 40 mg once day | Decreased activity of clopidogrel | Reduced liver activation of clopidogrel | Reduce the dosage of esomeprazole to 10 mg | 1 | 6 |
| Clopidogrel 75 mg once day | Fluoxetine 20 mg daily | Decreased activity of clopidogrel | Reduced liver activation of clopidogrel | Change fluoxetine to sertraline | 5 | 6 |
| Omeprazole 20 mg daily | Methotrexate | Increased methotrexate toxicity | Reduced renal secretion of methotrexate | Stop omeprazole three days before the administration of methotrexate | 2 | 7 |
| Atorvastatin 20 mg daily | Sildenalfil 20 mg | Muscolar pain | CYP3A4 inhibition | Stop sildenafil change to vardenafil | 4 | 6 |
| Atorvastatin 20 mg daily | Clarithromycin 500 mg very 12 hours | Muscolar pain | CYP3A4 inhibition | Change clarithromycin to azythromicin | 1 | 6 |
Table 7.
Drug inducers and inhibitors of cytochrome P450 3A4.
| Inhibitors | Inductors | ||
|---|---|---|---|
|
Calcium antagonists Amlodipine, Diltiazem, Felodipine, Nicardipine Nifedipine Verapamil Statins Simvastatin |
Antibiotics Clarithromycin, Erithromycin, Josamycin, Oleandromycin, Roxithromycin Telithromycin Ciprofloxacin, Norfloxacin |
Anticancer Imatinib, Irinotecano, Tamoxifene Hormonal therapies Ethinyl estradiol Levonorgestrel Raloxifene |
Atorvastatin Fluvastatin Lovastatin Simvastatin Tioglitazone Pioglitazone Rifampicin |
|
Central nervous system drugs Haloperidol, Bromocriptine Clonazepam, Desipramine Fluoxetine Fluvoxamine Nefazodone Norclomipramine Nortriptiline Sertraline |
Antifungals Fluconazole, Itraconazole, ketoconazole, miconazole, voriconazole Antiretrovirals Amprenavir, atazanavir, delaviridine, efavirenz, indinavir, lopinavir, ritonavir, nelfinavir, nevirapine, saquinavir, tipranavir |
Other drugs Cimetidine, Disulfiram, Phenelzine Sildenafil Tadalafil Methylprednisolone Antiarrhythmics Amiodarone quinidine Food Bergamot Grapefruit juice |
Antiretrovirals Efavirenz Lopinavir Nevirapina Antiepileptics Valproate, Carbamazepine Oxcarbazepine, Phenobarbital Phenytoin Primidone Topiramate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



