Submitted:
23 November 2025
Posted:
26 November 2025
Read the latest preprint version here
Abstract
The subject of the title is discussed from personal experience in Galicia (Spain), with a brief allusion to the beginning of NBS, indicating that without diagnosis, there can be no treatment, in luding the outstanding role played by LI Woolf, who always advocated not limiting it to PKU, and ignorance of their work, even in the hospital itself, with a footnote referring to current situations. The beginnings of NBS programs in Spain are referred to, which were born expanded, with a methodology that I cal open, chromatographic techniques, and nonspecific reagents that originate open procedures, applicable, for example, in the detection of lysosomal storage diseases, demonstrating the importance of urine in our program. The methodology used determines the pathologies to be detected, and the professionals who choose one or the other according to the criteria that are maintained today are largely responsible for the current disparities. The administrations acted on the matter sometime later when it had been rolling and running in different ways, depeending on the territory. Like others, Galicia always had an expanded program and was almost always ahead. At one point, a “Dr. BESSMAN” appeared in our administration who discovered the systematic reviews and scientific evidence, ignoring our evidence; after maneuvering in different spaces, he ried to be coercive, reducing the program without knowing the i tended purpose; a petition on the Change.org platform stopped that claim. The approach is based on a universal public social and healthcare system with competent professionals to successfully address rare diseases and, in the event of unexpected findings, to seek the best option for the patient. What has been published on the subject and the peculiarities of Spain are discussed. It is suggested that epidemiologists who are dedicated to this matter mutate into rareologists, and the situation at the beginning of the NBS is recalled when organized opposition from doctors arose, highlighting Samuel P. Bessman. It was the parents, as happened with FØling and Bickel, who got them interested in looking for the cause and treatment; now, they (parents and relatives) are changing to continue expanding the NBS programs. In Galicia, it appears that the criteria set by political leaders have changed, which has resulted in the exclusion of potential candidates such as Bessman from this role. In Spain, there are still disparities, as in Europe and many other places; the approach will have to be different depending on the social-health system of origin. Prof. F. Mayor Zaragoza took steps to address the issue within the framework of the Universal Declaration of Human Rights. If the precursors of the NBS had waited for scientific evidence at its inception in 1956 and 1957, it would not exist today. It is not possible to look for differences in the health of populations with broad and narrow NBS programs because these diseases are rare and do not significantly influence global health. Seeking equity cannot curtail programmers where no harm caused by them is appreciated. The differences between programs allow them to be compared and to progress. The appearance of biomarkers, treatments, analytic l technology, etc., requires frequent changes in the programs, and the training, criteria, and mentality of those responsible for them will depend on whether these changes are adopted.
Keywords:
newborn screening
; disparities or inequities
; Galicia
; Spain
Open Analytical Methods and Procedures for Expanded NBS and Program Disparities
Introduction
The following comments are the result of personal experience in Galicia, a historical nationality in the Kingdom of Spain, northwestern corner of the Iberian Peninsula, the cradle of the Portuguese language, and the Finisterre of the Roman Empire.
The surface of the current Galicia is 29,574 km2, with 2,555 km of indented coastline. There are 2.7 million inhabitants. In 2022, 14,495 births were registered, of which 100% were analyzed; in 1978, 43,721; and in 1993, 21,248, with 21,148 analyzed (99%), the year with the highest number of analyzed newborns; and in 2018, 16,848 births were registered, with 100% of newborns analyzed.
I remind you that Sheila Jones was of irish origin; when Bickel detected PKU in her and, together with the pediatrician John Gerard and the head chemist of the laboratory, Evelyn Hickman, made the diagnosis, they were very happy to identify PKU, something new and rare. The mother did not understand this satisfaction if they could not cure it; the book and the article by A. Green [1,2] supply detailed information on what happened. It is evident that without diagnosis, there would be no treatment.
The dietary treatment and preparation methods were proposed by LI Woolf [3,4] when he was working at the Organic Chemistry Laboratory of the Hospital for Sick Children, Great Ormond Street, London (GOSH), arriving there in 1947 (ICI fellowship). He was the first in 1956 to treat a newborn with PKU (17 days), considering its need for lipids and the essential amino acid phenylalanine in the necessary quantity to build proteins●; this nutrient shortage causes catabolism and paradoxically increases its concentration; the latter was ignored by some, and the results were disastrous. Even at GOSH, Moncrieff and Wilkinson [5] reported in 1961 a newborn with PKU (1958 Woolf's last year at GOSH), Moncrieff wrote the 1955 paper [6] formulating the diet, but he has not discussed the newborn's diet with Woolf the following year, and he omitted the addition of lipids when he added them any problems that had arisen disappeared. This highlights the lack of attention that some pay to their work*, in this case, with the collaboration of a nutritionist. Woolf tried to clarify the reason for the high prevalence of PKU at birth in Ireland and western Scotland, suggesting that genetically determined phenylalanine levels might have a protective effect against some mycotoxinmycotoxins [7].
I have been interested for time in the contributions and figure of LI Woolf, a chemist like me, who opened the path we have made othersother pilgrimages, including Bickel and Guthrie, who isare very ignored. Perhaps because of their modesty, Prof. Mayor and Ugarte, who knew him at Oxford, were unaware of his time at GOSH in London, where everything that has brought us here was forged (they learned about it from me, consequence the article [3] prepared for his centenary; which means he did not tell them about). I inserted the translated page, which was included in the edition on his 100th birthday [8], with which to end the prologue (Figure 1).
She treated her non-PKU twin sister with the same formula to confirm that her diet was sufficient for normal development. The PKU patient reached an IQ of 90, and the non-PKU patient reached 110; the older sister (the index patient, PKU), who was not treated, did not exceed 20 [8]•pg 71.
*The following three articles are examples of today's lack of knowledge about what is done in the laboratory itself
In the first article, the procedure in citation 19 from 1981 was discontinued in 1982, and the procedure in citation 21 of this paper (did not use pyridine) has been used since 1997; [23] describes the evolution of the procedure in the laboratory on pages 170-194. In that paragraph, the references are incorrectly assigned.
----Couce ML, Bóveda MD, Castiñeiras DE, Vazquez-Mosquera ME, Barbosa-Gouveia S, De Castro MJ, Iglesias Rodriguez AJ, Colón C, Cocho JA, Sanchez-Pintos P. A Newborn Screening Programme for Inborn Errors of Metabolism in Galicia: 22 years of evaluation and follow-up. Orphanet J Rare Dis. 2024 May 17;19(1):202 https://doi.org/10.21203/rs.3.rs-3328532/v1
In the second article, of which I am coauthor and of which I was not informed, the same error was made in reference 27.
----Sánchez Pintos P, Cocho de Juan JA, Bóveda Fontán MD, Castiñeiras Ramos DE, Colón C, Iglesias Rodriguez AJ, de Castro López MJ, Alonso-Fernández JR, Fraga JM, Couce ML. Evaluation and perspective of 20 years of neonatal screening in Galicia. Program results. Rev Esp Salud Pública. 2020; 94: 16 de diciembre e202012161. PMID: 33323918 https://pubmed.ncbi.nlm.nih.gov/33323918
In the third article, from a year ago, the same error was made in reference8. Furthermore, the use of a urine reducer was not mentioned. tests were performed with the MANDELIN reagent [4,41,42].
---Sánchez-Pintos P, Camba-Garea MJ, Martin López-Pardo B, Cocho de Juan JA, Bóveda MD, Barbosa-Gouveia S, Vázquez- Mosquera ME, Barros-Angueira F, Fernández Patiño R and Couce ML Clinical and biochemical evolution after partial dietary liberalization of two cases of galactosemia due to galactose mutarotase deficiency. BMC Pediatrics (2024) 24:620 https://doi.org/10.1186/s12887-024-05074-6
Louis Isaac Woolf advocates an expanded Newborn Screening, not limited to PKU, as he wrote in 1968 to Prof. Federico Mayor Zaragoza. * (Figure 2).
F Mayor, who met Woolf at Oxford during the 1966-67 sabbatical with Krebs (with whom he had already been in 1959, Woolf was there, but they did not meet then), set up an NBS Laboratory financed by the Spanish Government in 1968 at the facilities of the Directorate General of Health in Granada. The inauguration in January 1969 was carried out by Dr. García Orcoyen, Director General of Health, the highest health authority in Spain (Figure 3).
Independently and unaware of F Mayor's initiative, Dr. Juan Sabater Tobella became interested in the same subject. One year later, in Barcelona, he started an NBS Laboratory funded by the provincial government and the Juan March Foundation. Inaugurated on 2/7/1970, chaired by HRH the then Princess Doña Sofia, later Queen, she went on in the subject, presiding over a Royal Board of Trustees on Disability that promoted a National Plan, which, in 1977, was driven by Prof. F. Mayor, during his tenure as Minister of Education, enabled the implementation of the NBS Program throughout Spain.
Open Metodology
Chromatography
The use of separation techniques such as planar chromatography allows the identification of multiple biomarkers using a single sample aliquot, which constitutes a window. We open the window and look at who is passing. If it is the usual one, the result is negative. If we see someone who is not but has already presented it to us, we must recognize him. If it is not known, we must determine who he is.
Chromatographic procedures are called “multiplex”, although they are often ignored in NBSs. All of those used in Galicia since 1978 and for which urine was available allow us to conduct various detection procedures, such as methylmalonic and ethylmalonic acidemia, leucinosis, alkaptonuria, tyrosinemia, and cystinuria, etc., and may reveal any unsuspected stains.
Unfortunately, Dr. A. Maya has not published his amino acid PC procedure, which is part of his doctoral thesis [9] and was described and commented upon in the cited monograph [8]•pp 111-121. This text [8] discusses how the introduction of NBS programs in Spain was exceptional since Guthrie's BIA was not initially used; however, expanding the use of planar chromatography resulted in the expansion of these programs, as Woolf advocated.
*Documentation provided by Prof. M Ugarte.
**The PC test for organic acids is exclusive to our laboratory [8]•pp 120-123, 10. So too is the MANDELIN reagent test for reducing agents in urine and the cTLC (without PYRIDINE) for sugars, which is mentioned in this text.
Paper chromatography (PC) under pressure on paperand pressure and/or vacuum to displace the mobile phase (MP), about which I have already published communications [11] and described the instruments, has the advantage that when using a liquid MP and applying pressure to the paper, capillary forces increase and, therefore, decrease the migration rate of the MP and the solutes (components of the sample to be separated). This reduces the pressure or vacuum required to displace the MP and compact the spots, in addition to considerably increasing the migration rate and shortening the process time.
It also allows the use of gaseous MPs, supercritical fluids, or fluids close to phase equilibrium between the triple point and the critical point. It also allows the temperature to be set and programmed. In addition, it is possible to use stationary phases (SPs), such as asbestos, silk or wool fabrics (protein), cotton, etc., in addition to paper {partitioning with water (SP) and cellulosic (SP)}. In this technique, it is also possible to stack layers of the stationary phase separated by inert films, which allows the simultaneous analysis of many hundred samples with solvent fronts (paper width) of up to 46 cm—experimental and large—and displacements as long as needed, depending on the number of components to be separated and their mobility, with the SF and MF used. This approach promises a great future.
The ability to perform sequential staining and the capacity to scan or photograph by directly illuminating with selected wavelengths, including fluorescence capture and transillumination, combined with the contributions of digital image processing, which allow, among other things, recording, creating digital archives, identification, triggering alerts, quantification, normalization, etc., in which we have experience, opens up a large range of possibilities. The main problem with the PC is the price. It is too cheap. It lacks prestige, and sellers are not motivated to offer it. Perhaps, with these proposals, interest will increase.
Evaporative paper chromatography,developed at the same time as conventional chromatography (17 h), improves this process, compacting the spots and obtaining very sharp separations [8]
Nonspecific Reagents (Nontarget Analysis)
Nonspecific reagents can react with unknown markers or are unexpected, leading to freak findings.
These are also what I call open procedures. Cl3Fe reacted with the PKU marker phenylpyruvic acid when FØling was added to the urine, which was unexpected.
In the same way, the reaction of groups of biomarkers—sulfatides, glycosphingolipids, glycosaminoglycans or oligosaccharides—with a reagent that produces, with any of the biomarkers of one of these groups, a detectable and measurable signal with analytical methodology will allow the detection of lysosomal storage diseases. Initially, a single agent could give a positive result for one of these groups of diseases; additionally, a single reagent could give different reactions with markers of each of these groups. In this manner, we could obtain a positive result and identify which group it belonged to in a single step.
If the sample is dry urine (DUS-dry urine sample; Berry-Woolf specimen-BWS-), in which the concentration of these compounds increases more rapidly than in blood, possible biomarkers are discarded in aliquots of the same eluate until the one responsible for one of these pathologies is identified. This process is similar to the use of successive levels (or chromatography of one or a few aliquots) and can be combined with blood enzyme measurements followed by DNA sequencing. Such an approach would lead to the identification of a biomarker and an unforeseen or unknown pathology, which Føling did in 1934.
I once saw it written that we still use urine samples; not only do we still use them, but we use them more. There are people who throw them away because they do not know what to do with them, but that is not the case [12-20].
Using urine, we were able to make the first detection of leucinosis, “maple syrup” or MSUD; it was detected in that sample. He had been transfused—very common in critical pathologies—in the neonatal ICU, where it quickly eliminates the toxin, so the blood is not useful. The BCAAs continue to be excreted in urine for some time; similarly, in galactosemia, galactose continues to be excreted when it has already been eliminated in blood; in this case, the transfused blood also provides the enzyme that is deficient in the newborn, which masks an enzymatic diagnosis; that sample with our procedures allowed us to detect an exanguinotransfused case and parenteral feeding with glucose. We are the only ones in Spain that detect all types of galactosemia and other carbohydrate IEMs using the MANDELIN reagent [4] to detect reducing sugars and cTLC with MF without pyridine [21-23].
We did not abandon the dried urine sample on paper; we collected it at the time of obtaining the blood sample, placed the blotting paper on the genitals, held it with the diaper, and then pricked the heel to deposit the drops of blood on the corresponding paper, letting it dry, and removed the paper with the urine (because of the newborn urinating by reflex when receiving the puncture), letting it dry, would like the industry to look at that sample and test the possibility of developing marketable processes.
Enzymatic reagents and immunoassay reagents—antibodies—are specific and react with only a single biomarker molecule substrate and antigen, respectively; the procedures that employ them involve the antithesis of open procedures. However, the fact that these reagents detect only a single disease marker does not always prevent them from being considered open if that biomarker is associated with multiple diseases.
Moreover, when nonspecific reagents are used to detect biomarkers that are also useful for several diseases, additional windows can be opened, and the horizons of detectable diseases can be widened. Using a marker that is altered in several diseases expands the range of pathologies that can be detected. If we can assess several of these markers, which are common to several diseases, via a single analytical procedure, the diagnostic landscape can be enormous.
When a biomarker is an enzyme that must act on a specific substrate and measure a product, in principle, the procedure is not open; rather, it involves detecting a single disease. To approximate what would be a half-open procedure, we must use the simultaneous analysis of several enzymatic biomarkers, which act on their respective substrates and measure the products in a single assay.
A recent method, reactomics, provides a powerful way to quickly study many enzymatic reactions at once in dried blood spot samples, creating a complete metabolic profile [24]. The disadvantage of this approach is that the enzyme is labile, which impairs sample preservation, unlike more stable molecular biomarkers.
Open procedures could be used to determine total oxysterols, which are known to be more abundant in the urine of newborns than in that of individuals of other ages, unlike in blood, where they are more abundant at older ages [25]. Pediatric liver disease patients had significantly greater total oxysterol levels in both the urine and serum than did healthy children. The levels of oxysterols, particularly 24(S)-hydroxycholesterol, are greater in the urine than in the serum in patients with liver disease. This article [25] is possibly the first to propose the use of oxysterols as biomarkers of disease (also known as IEM); there are currently many other articles on this topic. A reagent that reacts with all oxysterols can be used, and separation methods (TLC) can be used to identify this reagent.
Enzymesin enzymatic methods and antibodies in immunoassays are more labile and more expensive reagents than chemical reagents are; additionally, they are generally stable molecules and simpler to synthesize than enzymes and antibodies obtained from living beings.
The best biomarkeris the one that best discriminates between affected and unaffected values. The further apart these values are and the sooner this wide difference occurs, the better and earlier it will be.
The enzyme activity markeris expressed earlier than the accumulation of an unmetabolized substrate or the appearance of an abnormal metabolite. The enzyme marker must be present in the samples received and be stable under the conditions of the route traveled.
When the biomarker is an antigen determined with an immunoassay, the epitopes can change their conformation with the passage from the solid phase to the solution upon elution, and environmental conditions can affect the conformation; additionally, reactive antibodies also require delicate handling (lipoproteins are difficult to elute, and their epitopes require polyclonal antibodies to determine them and thus react with any variant).
The Methodology Used and the Pathologies Included
The professionals who created the laboratories and strived to maintain their criteria were primarily responsible for the methodology used. Today, there are still people with a restrictive mentality, which largely explains the disparities, or what they call inequities, in Spain.
The programs' possible pathologies to be included are linked to the methodology used, the samples received in the labs, and the scientific culture of the professionals who work there.
When we talk about iniquity in the Kingdom of Spain, we must go back to the beginnings of the NBS when some said that what was not indicated was contraindicated; we can see this in what was written in Memory of Antonio Maya [8]●pp 222-232, which was the cause of confrontation at the time and had a political background because it was a consequence of the decision of the professional (with a scientific training similar to mine) responsible for the NBS Laboratory in a Historical Nationality, to use the Guthrie BIA to detect only PKU (when years later I asked -via e-mail- a clinician who had participated in the initial organization of that Program why had they decided to only detect PKU?”, he answered that they also did it for CH¿? ), the person responsible for choosing that method became the political position and director of public health in that country. With what was given, that of maintaining it and not amending it, which continues to this day, in this case there is a chauvinistic component; it seems that only there was it done well, the rest of us were wrong. That Director General sent me a letter, in an aggressive tone, trying to disqualify me, when apparently, I dismantled his approaches without being present at a meeting of politicians in charge of public health, where my writings were brandished.
It is misleading to say that when phenylketonuria is detected, other aminoacidopathies can occur. I heard this statement once, it is true if you use planar chromatography, but not if you use the Guthrie test which, on the other hand, can produce false negatives due to the almost systematic use of antibiotics in hospitalized newborns. The change to the fluorometric method meant avoiding this problem, having greater analytical sensitivity with respect to the BIA, obtaining numerical results, which seemed to provide greater security, and being able to advance the date of sample collection, which was then between 5 and 8 days of life. In Galicia, we kept this until the introduction of MS/MS, although we had already detected a PKU in a sample taken two days after birth (for which we have no record of any false negatives). This approach was used in laboratories that use PCs and TLCs as a step backward since other pathologies were not detected. However, it was pricier, and sellers put significant effort into introducing it.
In 2000, while we inaugurated the laboratory installation in a new hospital, Prof. JM Fraga successfully introduced MS/MS tandem mass spectrometry into the laboratory, thereby expanding the already growing NBS program, which did not significantly change its perception among the Galician population.
Galicia expanded the program. which was already broader and cheaper than others in Spain (which is unknown), made some regions interested in what we did; there was no interest in the previous procedures, which were cheap; in one, they introduced MS/MS; and when the political sign of their government changed, they stopped using it. I do not know what the contract with the suppliers was like; a journalist from a national newspaper published in Madrid (perhaps guided by some politician) asked me (by email) about the cost of the MS/MS analysis. I answered that it depended on what was done and how. I gave her the cost of the Galicia Laboratory per neonate (a low cost that did not interest him), had to explain to her that we did not buy kits, and the procedures that use MS/MS were developed by Dr. JA Cocho and D Castiñeiras. The consumables were obtained from various suppliers (not depending entirely on IVD companies allows costs to be reduced; at the 2013 Joint Meeting of the NBS and Genetic Testing Symposium and International Society for Neonatal Screening. 50 Years of Newborn screening, in Atlanta, USA, meeting, when I had been retired for just over a month, talking to a PerkinElmer salesman of Cuban origin, he did not understand how MS/MS was used in the NBS of Galicia, without using their kits); I told the journalist to ask the suppliers of the kits and not be surprised if the price was different depending on where it was sold.
Relationship of the Laboratory with the Administration Its Intervention in NBS Program
In Galicia, the NBS began with a research project at the University of Santiago de Compostela led by the pediatrician Prof. José Peña Guitian, in which I was the principal investigator. The laboratory was set up in Neonatology (congenital metabolic disease detection and treatment unit [UDyTEMC] and headed by Prof. JM Fraga at the hospital; now, in Clínico-CHUS, the physical situation changed in 2000, and the administrative situation changed several times. It is the first NBS laboratory in Spain to establish pediatrics and in a hospital, so the problem of lacking a pediatrician to take charge of the detected cases that others had in Spain is inevitable. see [8].●pp 225- …
The administration responsible for the NBS was transferred from the Ministry of Health of the Government of Spain to the Xunta de Galicia in 1983. He did not deal with the detections that were made and how they were made, in the case of Galicia, until 2003, when Dr. JM Barral Castro took charge of the General Directorate of Public Health. They were in charge of the laboratory staff, instruments, and logistics, but the laboratory staff scientists and pediatricians had been leading the NBS field until then. The details are given in [8]●pg 49.
Since then, the head of the newly created Population Screening Programs Service (SPPC) has become interested in what we did and how we did it. She was pleased with everything, and nothing changed.
On 02/08/2005, a coalition government came to govern Galicia, and the person who had been there in a previous period took over as head of the Service. I had a wonderful personal relationship with him (outside of work and teaching, as a medical student), and he knew perfectly well everything about the laboratory and the NBS in Galicia, but we did something wrong in the relationship with the SPPC.
At the meetings held by those responsible for the laboratories in Spain, we discussed the incorporation of new diseases, but the administrations barely participated in the decision-making process; on pages 223 to 232 of the aforementioned monograph [8], in the dedication in memory of Antonio Maya Victoria, an account of these meetings was given. From 1986 onward, the meetings were held annually, coinciding with the SEQC (Spanish Society of Clinical Chemistry) Congresses and sometimes coinciding with international events. Since 1995, it has rotated between different laboratory locations. At one time, there were 22 (today 15). The Royal Board of Disability sponsored the annual meeting starting in 1996. In 2006, it was held in Santiago de Compostela, Galicia.
Systematic Review and Scientific Evidence
On 20/11/2008, I participated in the first meeting of the working group for the preparation of the service charter for metabolic disorders, according to Decree 117/2008, of 22 May, regulating the service charters of the Xunta de Galicia and the Quality Observatory of the Electronic Administration of Galicia (DOG 12/06/2008; 113: 11268-11279), to which I was not initially invited because they did not transmit my name from the UDyTEMC of the CHUS to the SPPC. I asked the SPPC to participate, and it managed my participation with the UDyTEMC. This was the first study in which a public health program was applied to a service that was not purely administrative. The work was distorted, resulting in an evaluation of health technology in light of scientific evidence, which is not possible when we do is evidence-generating medicine. The decree insists on the participation of the affected population, and on this occasion, the participation of those affected—family, relatives, etc.—was avoided. After much work and bibliographical review, on 28/06/2010, when the 15th and last meeting was held, the last of the conclusions were reached. The working group views the tasks assigned to it as completed. The Directorate General of Public Health and Planning may call for a meeting to reach a consensus if there are important discrepancies in the evaluation of the final documents. The SPPC concluded, without the work group, what was included in the “Report on the review of compliance with criteria to establish a population screening programme by pathologies or conditions that are currently examined within the Galician Program for early detection of endocrine and metabolic diseases in the neonatal period”. That report was not made public, and the working group learned about it from people outside it (I refuted in [8]●pp 19).
At no point was there any interest in evaluating the Program or Laboratory's healthcare technology in light of our living evidence and our science. This is our unique approach, with very clear beneficial results for those affected, their families, and therefore society and the healthcare system. It is free of personal and social harm of any kind. It is fully incorporated into Galicia's healthcare culture and constitutes an acquired right of the Galician people. Its population coverage was growing to approximately 99%, and families facilitated the collection of urine and blood from newborns on paper. Pediatricians were also in agreement, collaborating without objection. Cutting the NBS would be unethical.
Those of us who ran the program resisted attempts to cut it. For a while it seemed that the desire to cut the NBS had calmed down.
The Galician government changed its political affiliation on 16/04/2009. In early 2015, I received news that the director of CHUS had said we were doing too much (Dr. Fraga has already retired). After attending the presentation of the AVALIACIÓN da Estratexia Sergas 2014 on February 23, I decided, after Rare Disease Day, the last day of February, to send a letter to the organizers Day, expressing my concern about the program's reduction and the elimination of urine testing. Additionally, I started a petition on Change.orgaddressed to the president of the Xunta to prevent these changes. It was successful on April 7.
At https://www.change.org/p/xunta-de-galicia-no-pongan-en-peligro-la-detección-de-enfermedades-en-galicia/u/10260701 address can be accessed through the petition on Change.org [accessed on09/10/2025], and updates can be followed by going back to the beginning and forward to the press release where the Administration accepts my petition. Translated Inserting (Figure 4).
In 2017, the issue was addressed in a similar way by the promoter of the development of the service charter, with the support of the Spanish Society of Epidemiology [26].
In the U.S., where there is no universal public health system, these NBS programs are an anomaly in health. The Scientific and Patient Societies provided responses; this can be found in the cited material [8]●pp179-181. We can even talk about a PUBLIC and UNIVERSAL SOCIO- HEALT SYSTEM.
The work from the UK [27] attempts to understand whether differences between countries in recommendations on NBS for rare diseases using newborn blood spot testing could be partly explained by the use of systematic review methods. In the introduction they review the current situation with expansive differences from one country to another; they do not know whether the differences between countries are due to genuine differences in disease prevalence, healthcare systems, and priorities, or differences in the process of reviewing the evidence used to generate policy, in particular the use of systematic reviews.
They mention overdiagnosis as one of the main harms of NBS because the detection of a disease that would never cause symptoms in a particular person's life {this is not a disease or a false positive; it is a characteristic such as having black hair, and it does not seem easy for such a thing to occur; we can think of pentosuria}. The authors analyzed a country's policy decisions on which diseases to include in the NBS to determine whether systematic reviews were carried out and whether this was associated with the final recommendation to implement screening. The authors rated the accuracy of the test, the benefit of early detection and overdiagnosis, and the relationship with the decision made.
A total of 134 policy documents were identified; 108 of them were from experts. A total of 41 studies were excluded, and the reasons for exclusion were provided. After the exclusions, 24 Spanish documents remained, and 23 were from the USA; none of the other countries kept more than 8 documents. Of the only 60 recommendations that used systematic review methods, 24 were from Spanish documents, and 21 covered test accuracy, the benefits of early detection, and overdiagnosis. They comment that the decision to carry out a systematic review could have been driven by factors internal to the country, and they can only draw tentative conclusions "It is curious that the 24 Spanish documents selected, all of them systematic reviews, top the list by country, surpassing other demographically much larger ones, and it is also curious that 9 are driven by Galicia, where I write, and another 9 by the Canary Islands, which demographically are below others, such as Andalusia or Catalonia; it would be necessary to consider what circumstances exist in them." In the monograph [8]●pp. 206-209, the article and the circumstances in Galicia and the disagreements that arose prior to the preparation of these studies, which did not change anything that already existed, are discussed in detail.
The researchers found that policy reports lacking systematic review methods were more likely to recommend screening, indicating that a rigorous assessment could reveal the absence or unreliability of the available evidence. Several studies have demonstrated discrepancies between expert opinion and research evidence; one study highlighted that professional treatment recommendations presented in review articles or textbooks often contradicted the best evidence from meta-analyses of trials available at the time of publication.
I see in this restrictive character something similar to what happened at the beginning of the NBS, when organized opposition to its implementation appeared; what was said about GALICIA and the CANARY ISLANDS, I relate to the presence in their administration, when the revisions were made, of "Dr. SAMUEL P. BESSMAN" [28]. I know the one from Galicia and the one from the Canary Islands; I greeted him once.
I conclude that we must avoid work, expense—misappropriation of public funds—and waste of time in useless reviews; however, they may be robust and promote the creation of evidence, provided that the principle of beneficence is complied with and that it is ethically advisable and allows for the participation of those affected, family members and friends, who laid the foundations for its initiation and continue to force the expansion and research in NBS programs—a situation that is no longer debatable since they are the best scientific evidence, evidence of efficacy, efficiency, effectiveness, evidence of need, and living evidence. Those who suffer adverse effects, if there are false positives and negatives, overdiagnoses, or overtreatments.
On 06/10/2023, in the development of newborn screening policies in Spain from 2003– 2022, what do we actually need to reach an agreement? [29] was published*, which is clear evidence of how systematic review articles searching for evidence, when published, are outdated. The error in writing that the number of NBS laboratories in Spain was 20, when there were 15, is, in my opinion, a palpable demonstration of what was said. Having counted on the participation of those involved and having published on 02/23/2021: [START, EVOLUTION AND CURRENT SITUATION OF NEONATAL SCREENING PROGRAMS IN SPAIN] [30], where it clearly states that there are 15 laboratories (in my case, I determined years before during a visit to the laboratory), it can be deduced that the wording is prior to its publication. The journal in which it is published contains more articles in which that number of laboratories is mentioned and the authors of the mentioned article [29] also write in that journal about NBS, so I do not understand the error.
In 2003, there were 20 patients, but these numbers decreased according to the following report: [Activity of neonatal screening programs in Spain. Review from its beginning until 2016. According to the Ministry of Health, 2021] [31], on page 18: "in 2020, the reorganization carried out over the 50 years leaves 15 neonatal screening laboratories in operation in Spain, whose population coverage reaches 100% of newborns in Spain". The bibliography of the article [29]** is outdated in several sections, and the one cited in the following paragraph is not included.
Rarologist
On another note, the work of epidemiologists who abuse scientific evidence but who do not offer the option of obtaining it, since we are evidence producers and, through open screening methods, we can detect unsuspected or unknown pathologies or conditions, must mutate into ‛Ararologist.
I now discuss the work of RAROLOGIST, who, without knowledge, are beginning their work, driven by those affected, parents, relatives, etc.; possibly the first were those who suffer from Duchenne muscular dystrophy (DMD) to argue the relevance of the NBS, for which they articulate the form of participation of those concerned in decision making [32], to develop the evidence that supports the implementation of NBS for DMD. In this work, they review the organization and the effort put into what was done in the U.S., where there is no universal public SNS. Another project [33] developed a new online method to include patients and their caregivers in this process, using the DMD care guidelines as an example. The expected completion date of the study was May 2020. In 2020 [34], the authors concluded that they developed a new online approach that makes it feasible and convenient to engage large numbers of patients and their caregivers in a rigorous and culturally appropriate manner, consistent with how clinicians engage in guideline development in clinical settings. The procedure produces results that, during the process, highlight the ability to facilitate learning and provide students with the opportunity to review their responses, which is important for achieving consensus.
The best practices they identified could help engage patients and their caregivers in the guideline development process in other clinical areas, thus facilitating the work of guideline developers. A year earlier, they published an article [35] in the same vein. In the USA, the number and type of inherited disorders included in newborn screening currently vary from state to state, and as early as 2017 [36], an attempt was made to include all of the Recommended Uniform Screening Panel (RUSP).
However, this approach has not been adopted by all states, creating a geographic disparity in opportunities to receive timely intervention for life-threatening inherited conditions. Raralogists are doing significant work in this direction. The processes for reviewing evidence to add new conditions to state NBS panels rely on data from pilot studies that assess the potential benefits and harms of screening. However, consideration of the ethical, legal, and social implications (ELSI) of screening within this research has been limited. One article [37] described important ELSI-related issues in relation to newborn screening policies and practices as a resource to help researchers integrate the ELSI into NBS pilot studies. Integrating ELSI questions into pilot studies will help NBS programs better understand the potential impact of screening for a new condition on newborns and families and make critical policy decisions aimed at maximizing the benefits and mitigating potential negative medical or social implications of screening. This issue is discussed further in the cited monograph [8].
*When I read this article [29], I was correcting the galley proofs of the one referred to here with [4]; I cited it in that one with reference 45, indicating an error in the number of existing laboratories. Once published, I put it in RG and sent the authors some initial observations by RG, which I put as DATE[accessed on 09/10/2025] https://www.researchgate.net/publication/395008864_Acabo_de_poner_en_RG_un_articulo_en_el_que_os_cito.
Later, I elaborated more extensive comments, insisting on the obsolescence of its publication. Titled TRABAJOS DE RARÓLOGOS and sent by the same means; and in DATE https:///www.researchgate.net/publication/395005676_TRABAJOS_DE_RAROLOGOS [accessed on 09/10/2025].
**If these two documents were excluded for not meeting the epidemiological criteria for inclusion or were not sought by origin, the problem is of "Aurora borealis”.
Current Situation in Galicia
The situation has changed in Galicia since “Dr BESSMAN” stopped leading the SPPC, and currently, the president of the Xunta de Galicia boasts are the ones who include the most pathologies in the NBS. In the twelve years that I have retired, the pathologies or conditions detected have been increasing, reaching what is being done now, which can be consulted in Galician at the link: https://www.sergas.gal/Saude-publica/documents/7090/Listado_enfermedades_gallego.pdf [accessed on 09/10/2025]
The methodology, procedures, and analyzed samples determine potential congenital pathologies for detection. In Galicia, urine and blood are analyzed simultaneously, and more than 60 diseases can be detected in samples taken between 24 and 48 hours after birth. Analytical procedures can be used to detect unforeseen or even unknown pathologies.
On 12/24/2023, the local newspaper “El Correo Gallego” reported that the Metabolopathies Laboratory is now able to detect 60 diseases with the NBS in babies from all over Galicia. Dr. JA Cocho, my successor at the head of the laboratory, stated in the interview that if any of the 34 included pathologies are detected, we can add three more pathologies, allowing up to 60 to appear on our list of diagnoses. This is practically double because “in the case of a child with a metabolic problem related to an amino acid, the cause of that problem can be more than one, and we very quickly look for the pathology that needs to be treated immediately, but if there is another, we also detect it”. At the NBS, blood and urine samples on paper are analyzed in a very well-linked way so that, in two or three days, if a special test needs to be done, the diagnosis can be made, and the child can be treated. She says that when the baby is 24 hours old, the heel is pricked, and samples are soaked in absorbent blotting paper, which is sent by suitcase so that every day before 8 in the morning, they have a suitcase from each hospital with samples from those who were pricked the day before and were born a couple of days ago; the work lasts between one and three days, and normally between four and six days after the child is born, they have the diagnostic hypothesis.
https://www.elcorreogallego.es/santiago/2023/12/24/chus-logra-detectar-60-enfermedades-96207265.html [accessed on 09/10/2025]
Current Situation in Spain
In Spain, there is a significant disparity in access to universal newborn screening (NBS) programs for newborns who are users of the public National Health System (SNS), depending on the nationality or region of residence.
When the SNS is universal, it avoids having to create the necessary [38] financial infrastructure in the USA to study the incorporation of new pathologies, and when unexpected findings or possible undescribed pathologies occur, the SNS is competent to study the case, and healthcare ethics committees channel it to achieve the maximum benefit without causing any harm; thus, express consent is not necessary for each pathology identified; there is already generic consent when consenting to the collection of the sample, which is reported at that time and described in the NBS program documentation.
The SNS benefits from detection by eliminating diagnostic difficulties and is also spared from suffering and associated expenses. This allows the study of the natural history of disease and sociohealth and psychological interventions, which will facilitate the performance of these public structures and the family.
We have experience with a patient with MSUD, using the diagnosis to modify the death certificate and offer genetic counseling.
The family called us, truly grateful for having that information. The family can consider reproductive options they might not have otherwise. Where there are no SNSs universal, this possibility is not considered.
Those who complain about the lack of equity in NBSs in Spain have an effortless solution: by emulating those they consider to be in a better situation. If this does not improve the situation according to the others, they will have to prove the former wrong.
The differences in NBSs among populations, regions, nationalities, nations, or countries enhance our ability to evaluate various policies against one another in the spirit of healthy competition and progress. These differences serve as an incentive to enhance our understanding of the advantages and disadvantages of each population, region, nationality, nation, or country; in all cases, the ethical principles of beneficence and nonmaleficence must be respected.
It is my duty to make known the letter from Prof. F. Mayor* to Mr. Volker Turk, High Commissioner for Human Rights of the United Nations Office, dated February 1, 2023. Finally, Section 2 refers to our matter. We have recently heard from you that you are working to include the NBS in the Universal Declaration of Human Rights.
https://www.docdroid.net/dJPCwVj/carta-mayor-zaragoza-0038-volker-turk-high-commisioner-for [accessed on 09/10/2025]
Pursuing Global Equity in This, as in so Many Other Aspects, is Difficult to Achieve
* Professor Federico Mayor Zaragoza, who passed away on December 20, 2024, leaves us a final article [43], which, in the last paragraphs, refers to the fact that on October 30, 2024, he contacted Michelle Bachellet, former United Nations Commissioner for Human Rights and closely related to Volker Turk, requesting her help in processing this new human right.
I disagree with your approach to centralizing the decision to introduce an ipatoñogie in the Neonatal Screening Program to achieve uniformity. programs; differences stimulate progress on the matter, as I have written.
Her Majesty Queen Letizia is interested in those suffering from rare diseases and supports their demands for the expansion of newborn screening
The text preceding the title of the monograph [8] is from the first draft, and the editor of an article [39] moved it to the abstract;. inserting it translated (Figure 5).
The pursuit of equity in NBS programs cannot in any way restrict a program in which no harmr is caused or for which the detection of a pathology or condition or group of the m is questioned, as doing so is beneficial to the country.
Differences in health outcomes cannot be expected between individuals who benefit from an NBS program for a few disorders and those whose programs cover many conditions or pathologies. Since these are minority diseases and sufferers belong to the social minority, they go unnoticed. Professor Mayor Zaragoza states that a single affected child in every 10,000 has a 100% impact on both the family and the affected child.
Therefore, precisely because these are irreversible situations, there is no room for percentages. We must ensure that birth is considered, from both a medical and social care perspective, as an event at least as significant as death. We must continue to address the needs that cause suffering, regardless of their nature [8].
This subject is constantly evolving and rapidly evolving due to advances in analytical methodologies, such as genetics, chemistry and biochemistry, as well as in treatments such as personalized precision medicine (CRISPR/Cas9), enzyme replacement, and substrate restriction. In this case, it is not possible to obtain scientific evidence quickly, as was the case at the beginning of the COVID-19 pandemic when the evidence changed every hour; on the other hand, additional time is needed to allow the screening of large populations. Therefore, it will be necessary to work to create a tool for screening, for which it is essential to implement said screening (this demonstrates the great difference between an epidemic or pandemic and rare diseases; these are antithetical situations).
However, the emergence of new biomarkers, treatments and research introduces new evidence that is increasingly dynamic and can change over several days, weeks or months. This phenomenon causes the evidence to reverse and change rapidly.
The mentality, ideas and training of scientists, health professionals, administrators and political leaders (family members or close friends affected?) competent in the matter, together with social acceptance, as expressed by doctors in consultations and in the media, play a fundamental role when introducing a detection or a policy related to these programmes (their treatment in the budget).
Epilogue
The ability of a newborn screening laboratory to detect pathologies depends on the samples received in the solid phase on adsorbent paper (desk blotting paper from the first experiences with this type of sample), urine, blood (serum, plasma, saliva, sweat, tears), and the methodology used to perform the analyses based on these samples.
If the methodology allows for the discovery and evaluation of multiple analytes—biomarkers for various diseases—with a single procedure in a single sample aliquot, chromatography, electrophoresis, or tandem mass spectrometry (MS/MS), etc., they are now called multiplex methods. These methods can detect multiple diseases and identify biomarkers that could indicate an unexpected or unknown disease or condition, not necessarily classified as such (such as pentosuria).
If the methodology involves the use of sequential maneuvers, one or more unidentified analytes of a type or group of molecules that are biomarkers of possible pathologies in anomalous proportions are detected in successive steps, continuing with the same aliquot (acting on what was obtained in the previous step) or another sample type (blood, urine, etc.), these molecules or others are identified and assessed, depending on the sample.
This process is now called second-level testing, but successive levels can be concatenated, similar to what analytical chemists call analytical marching. This methodology is amenable to the detection of multiple pathologies, whether anticipated, unexpected or even unknown.
The markers and reagents that affect the robustness of the procedures are discussed. The importance of having a urine sample available was emphasized.
It is recommended to review the work of Efron et al. [40] to see how NBS was born with an open methodology; this can be improved with few changes and reduced costs.
After a diagnosis is reached, regardless of how disastrous the prognosis is always beneficial. Occasionally, the intervention of a psychologist will be necessary to determine how, when, and where to communicate. In some cases, the presymptomatic stage can be extended, and palliative and social care can be provided. The family benefits from being able to plan new pregnancies using assisted reproduction to prevent recurrence of the disease. It is not a question of looking for pathologies without treatment but rather those that are found with open procedures.
Having a diagnosis is essential for receiving treatment; today, we are moving closer to genetic correction.
In one instance, we used laboratory results to alter the patient’s death certificate. The family called to thank us for the information. They noticed a noticeable change in the doctors' attitude, from evasive and uncommunicative to providing all the necessary explanations and guidelines. This means that the doctors were also relieved. There is nothing left unsaid regarding the diagnostic odyssey, which disappears.
I know that my approaches may seem unorthodox, but I believe they can be valid, effective, and efficient.
This is a partial view from the biochemical laboratory, since only the aspects related to the biochemical phenotype are considered, I think that starting by doing these analyses is a good way to do it. The study did not address relevant laboratories of genetics, microbiology, immunology, etc. In addition, we must consider other aspects of the program, such as diagnostic confirmation, treatment, and follow-up.
Today, the author's techniques, methods, and procedures are no longer used in the Galician laboratory.
They continue to develop and use his procedures for urine analysis; the rest are purchased.
I
The test for reducing agents with the MANDELIN reagent could be performed by kinetic reading, quantification and normalization with creatinine [44,45], which allows the detection of reducing agents in urine at 24 h of life.
The BOLETÍN OFICIAL DE LAS CORTES GENERALES●CONGRESO DE LOS DIPUTADOS, [The OFFICIAL BULLETIN OF THE GENERAL PARLIAMENT●CONGRESS OF DEPUTIES] reported that at its meeting on June 13, 2025, the Bureau of the Chamber agreed to admit for processing the document exercising the initial processing of the INICIATIVA LEGISLATIVA POPULAR (ILP), [POPULAR LEGISLATIVE INITIATIVE (PLI)], and the Bill for the Regulation of Universal and Equitable Neonatal Screening in Spain.
The text of the proposal is two pages long, has eight articles and two final provisions, and does not contribute anything new. It proposes a mandatory minimum panel of diseases subject to neonatal screening throughout Spain, established by a Commission, reviewable at least every two years, using traditional criteria: scientific evidence, treatment, technical feasibility of screening, and cost- effectiveness. This approach does not address issues such as the methodology used in the laboratory, which constitutes the bulk of this article and would be difficult to introduce. Perhaps an addition could be made to "technical feasibility of screening, including nontarget analysis, analytical procedures open todetection of unforeseen or unknown pathologies or conditions. The text still has a long way to go before it reaches its final draft.
Ethical Aspects
Detecting the detection of an unforeseen or unknown pathology or potential pathology as a result of using an open methodology can raise ethical issues. In some situations, communicating the findings to the pediatrician and family will present difficulties. In the first case, it does not seem to be overly problematic. Second, the intervention of a psychologist is required to try to maximize the benefit of detection and minimize harm, preparing the family for what lies ahead, especially when deterioration cannot be avoided. However, this is the first step toward obtaining some benefit, such as prolonging the presymptomatic stage and studying possible treatments. In any case, communicating to parents about the impact of the findings, which may be unknown or known to be heterogeneous, and the possible decisions to be made are complex.
This consequence, in some cases, may present the ethical dilemma of whether to inform the family of their genetic characteristics when no possible intervention that would improve the newborn's prognosis is in sight. By informing the family, they can consider reproductive options and consider having more children, which they might not have done without this information. They can also encourage the screening of relatives.
This is a clinical-care approach, and a Clinical-Care Ethics Committee will resolve each case (which will be rare), considering the right of those affected to remain unaware. Information can also be found pending advances in treatment or the emergence of a plausible treatment approach.
Close monitoring of these children will allow for the study of the natural history of the disease and attention to any emerging social and health needs.
Data Availability Statement
Acknowledgments
To Dr. Magdalena Ugarte. I could not imagine that those who knew Dr. LI Woolf in Oxford were unaware of her time at GOSH in London, where the work that brought us here was conceived, as was expressed to me by Malene Ugarte, who was totally unaware of this circum-stance. I became aware of the fact that (after the special issue was published, on the occasion of the 100th anniversary of LI WOOLF https://www.mdpi.com/journal/IJNS/special_issues/neonatal_screening, which I had the honor of promoting and initiating, we exchanged e-mails to try to get her to participate in that issue to which she had not sent any work, an issue for which she had informed Prof. Mayor). She told me in an e-mail that she had been with Dr. Charles Enrique Dent Colsa (I put the names in Spanish because he was born in Burgos to a Spanish mother and that is his full name) in the hospital where Dr. Sir Archibald Garrod was from 1892 to 1913, when he described some “Innate Errors of Metabolism” and introduced this concept; I told her that it was where LI Woolf had done the initial work that brought us here and she was shocked, she had not heard anything from This means that Woolf did not comment on what she did in London before going to Oxford, which gives us an idea of her modesty. Dr. Charles Robert Scriver, a physician and researcher, acquired the chromatographic technique from Dent in London. He introduced new laboratory techniques in the USA. Later, along with others, he implemented a pioneering newborn screening program for congenital disorders in Quebec in 1969. It was then that she sent me, among other documents, Woolf's letter and the Health Department letter. To the “Asociación Enfermedades Raras Más Visibles”• “More Visible Rare Disease Association” and his spokesperson Pedro Lendinez Ortega, for allowing us to include its link that allows access to the documentary “La vida en una gota” [“Life in a drop”]. Supporting the research in Open Programs of NBS, advocated in this writing. www.masvisibles.com. The editor of this magazine for shaping the presentation.
References
- Green A. Sheila. BREWIN BOOKS, ISBN: 978-1-85858-714-1 https://www.espku.org/2020/10/12/sheila-unlocking-the-treatment-for-pku/.
- Green A. The first treatment for PKU: The Pioneers-Birmingham 1951. Int J Neonatal Screen. 2021; 7: 19. [CrossRef]
- Alonso-Fernández JR. Dr. Louis Isaac Woolf: At the Forefront of Newborn Screening and the Diet to Treat Phenylketonuria- Biography to Mark His 100th Birthday. Int J Neonatal Screen. 2020; 6: 61. [CrossRef]
- Alonso-Fernández JR. Four Decades of Newborn Screening: A Historical Perspective of Laboratory Practices. OBM Genetics. 2023; 7. [CrossRef]
- Moncrieff A, Wilkinson RH. Further experiences in the treatment of phenylketonuria. Br Med J. 1961; 1: 763-767. [CrossRef]
- Woolf LI, Griffths R, Moncrieff A. Treatment of Phenylketonuria with a diet low in phenylalanine. Br Med J. 1955; 8: 57-64. [CrossRef]
- Woolf LI. The heterozygote advantage of phenylketonuria. Am J Hum Genet. 1986; 38: 773-775. https://pmc.ncbi.nlm.nih.gov/articles/.
- Alonso-Fernández JR. Colón Mejeras C. Aportaciones de Louis Isaac Woolf al Tratamiento y Diagnóstico Precoz de la Fenilcetonuria y otros Errores Congénitos del Metabolismo. Los comienzos de la Tría Neonatal en España, con referencia al Programa de Galicia. CENTENARIO DE LOUIS ISAAC WOOLF. 2024. /1 file:///I:/LIBRO_impresion2025-XIVAportacionesLIWoolfTratamientoDiagnosticoPrecozdeFenilcetonuria2%20(1).pdf. [CrossRef]
- Maya A. Aportaciones al Diagnóstico Precoz de Alteraciones Metabólicas Congénitas en el Recién Nacido. Tesis Doctoral.Facultad de Farmacia. Universidad de Barcelona. 1974 https://www.researchgate.net/publication/379732142_LIBRO_Aportaciones_LI_Woolf_Tratamiento_Diagnostico_Precoz_de_Fenilcetonuria_2.
- Alonso-Fernández JR, Bóveda MD, Peña J, Fraga JM. Screening of organic acid disorders. The use of acridine dye as a neonatal screening method. A comparative study with fast garnet dye. International Meeting on Neonatal Screening. August1982. Tokio https://www.researchgate.net/publication/397706092_Screening_of_organic_acid_disorders_The_use_of_ACRIDINE_dye_as_a_neo natal_screening_method_A_comparative_study_with_FAST_GARNET_dye.
- Alonso-Fernández JR. Neonatal Screening for Metabolopthies in Less than an Hour by Pressure Paper Chromatography. November 1991, 8th International Neonatal Screening Symposium and Inaugural Meeting of the International Society for Neonatal Screening. Leura Blue Mountains, N.S.W. Australia https://www.researchgate.net/publication/318280742_Neonatal_Screening_for_Metabolopthies_in_Less_than_An_Hour_by_Pressure_Paper_Chromatogrphy.
- Alonso-Fernández JR, Javier Fidalgo López J. Review and Proposal of Alternative Technologies for Comprehensive and Reliable Newborn Screening Using Paper Borne Urine Samples for Lysosomal Storage Disorders: Glycosphingolipid Disorders. JIMS. 2021; 9: 20200011 https://doi.org/10.1590/2326-4594-jiems-2020-0011.
- Alonso-Fernández JR. Pregnanetriolone in paper-borne urine for neonatal screening for 21-hydroxylase deficiency: The place of urine in neonatal screening. Mol Genet Metab Rep. 2016; 18: 99-102. [CrossRef]
- Jiao X, Gong P, Niu Y, Xu Z, Zhou Z, Qin J, et al. Evaluating the suitability of 6-oxo-PIP as a novel biomarker for pyridoxine dependent epilepsy in multiple samples. Research Square Platform LLC. 2024 https://doi.org/10.21203/rs.3.rs-3843855/v1.
- Merino-Hernández A, Sánchez-Barrio Pedro L, Villar-Castro S, Aguado-Del Hoyo A, Marsinyach-Ros I, Sánchez-Luna M. Cost effectiveness of a cytomegalovirus screening strategy in neonates born after 34 weeks small for gestational age. An Pediatr (Engl Ed). 2023; 98: 41-47. [CrossRef]
- Rebollido M, Cocho JA, Castiñeiras DE, Boveda MD, Fraga JM. Aplicación de la Espectrometría de Masas en Tándem al análisis de aminoácidos, acilcarnitinas, acilglicinas y ácidos orgánicos en muestras de orina en papel. Química Clínica. 2006;25:64-74. https://www.seqc.es/download/revista/102/345/627712070/1024/cms/QC_2006_64-74.pdf/.
- Newborn Screening for Congenital Cytomegalovirus. Canadian J Health Technologies. 2024; 4. https://www.cda-amc.ca/sites/default/files/pdf/htis/2024/RC1533_Final_Review.pdf.
- Newborn Screening for Congenital Cytomegalovirus. Rapid Review CADTH Health Technology Review. Canadian Agency for Drugs and Technologies in Health. 2024. https://www.ncbi.nlm.nih.gov/books/NBK604833/.
- Sheila C. Dollard, Mark R. Schleiss, Scott D. Grosse. Public health and laboratory considerations regarding newborn screening for congenital cytomegalovirus. JIMD. 2010; 33: 249-254. https://onlinelibrary.wiley.com/doi/10.1007/s10545-010-9125-3. [CrossRef]
- Jiao X, Gong P, Niu Y, Xu Z, Zhou Z, Qin J, et al. Evaluating the suitability of 6-oxo-PIP as a novel biomarker for pyridoxine dependent epilepsy in multiple samples. Research Square. 2024. https://www.researchsquare.com/article/rs-3843855/v1. [CrossRef]
- Alonso-Fernandez JR, Carpinteiro MI, Baleato J, Fidalgo J. Vertical Sandwich-Type Continuous/Evaporative TLC with Fixed Mobile Phase Volume for Separating Sugars of Clinical Relevance in Paper-Borne Urine and Blood Samples in Newborn Screening. J Clin Lab Anal. 2010; 24: 106-112. [CrossRef]
- Alonso-Fernandez JR, Patel VB. Dietary sugars: TLC screening of sugars in urine and blood samples. In book: Food and Nutritional Components in Focus. Dietary Sugars. Chemistry, Analysis, Function and Effects Edition: 1. Chapter: 12. Publisher: Royal Society of Chemistry Publishing. 2012. [CrossRef]
- Alonso-Fernández JR. DETECCIÓN, ESTIMACIÓN Y CUANTIFICACIÓN DE AZÚCARES EN FLUIDOS BIOLOGICOS, SU SEPARACIÓN POR CROMATOGRAFÍA EN PAPEL (PC) Y CAPA FINA (TLC). REVISIÓN HISTORICA Y PROPUESTAS DE.
- NUEVOS PROCEDIMIENTOS. Aplicación en Tría Neonatal de Errores Innatos del Metabolismo de los Carbohidratos. [CrossRef]
- Hall K, Schielen PCJI, Platis D. Oral and Poster Abstracts of the 13th ISNS European Regional Meeting. March 2025 International Journal of Neonatal Screening 11(1):21///2. Invited Presentations I01. Keynote Lecture: Reactomics and Its Future in Newborn Screening. Raquel Yahyaoui. [CrossRef]
- Takaki Y, Mizuochi T, Takei H, Eda K, Konishi KI, Ishihara J, Kinoshita M, Hashizume N, Yamashita Y, Nittono H, Kimura.
- A. Urinary and serum oxysterols in children: developmental pattern and potential biomarker for pediatric liver disease. Sci Rep. 2020 Apr 21;10(1):6752. PMID: 32317688; PMCID: PMC7174363. [CrossRef]
- Grupo de Trabajo de Cribado de la Sociedad Española de Epidemiología. Personas de contacto: Raquel Zubizarreta.
- CRIBADO NEONATAL DESDE LA PERSPECTIVA DE SALUD PÚBLICA. Situación y recomendaciones.
- https://www.seepidemiologia.es/documents/dummy/SEE%20Recomendaciones%20programas%20de%20cribado%20pat.pdf.
- Taylor-Phillips S, Stinton C, Ferrante di Ruffano L, Seedat F, Clarke A, Deeks JJ. Association between use of systematic reviews and national policy recommendations on screening newborn babies for rare diseases: Systematic review and metaanalysis. BMJ. 2018; 361: k1612. [CrossRef]
- Levy HL. Robert Guthrie and the Trials and Tribulations of Newborn Screening. Int J Neonatal Screen. 2021; 7: 5. [CrossRef]
- Valcárcel-Nazco C, García-Pérez L, Linertová R, Guirado-Fuentes C, Hernández-Yumar A, Paz-Valiñas L, et al. Development of newborn screening policies in Spain 2003-2022: what do we actually need to reach an agreement? Rare Dis Orphan Drugs J. 2023; 2: 19. [CrossRef]
- Marín Soria JL, González de Aledo Castillo JM, Argudo Ramírez A, López Galera RM, Pajares García S, Ribes Rubió A,.
- García Villoria J, et al. INICIO, EVOLUCIÓN Y SITUACIÓN ACTUAL DE LOS PROGRAMAS DE CRIBADO NEONATAL EN. ESPAÑA Rev Esp Salud Pública. 2021;95: 23. file:///C:/Users/Jose%20Ramon/Downloads/Dialnet-InicioEvolucionYSituacionActualDeLosProgramasDeCri-7957665.pdf.
- Dulín Iñiguez E, Eguileor Gurtubai I, Espada Sáez-Torre M, Pàmpols Ros T, Zubizarreta Alberdi R. Actividad de los programas de cribado neonatal en España. Revisión desde sus inicios hasta 2016. Ministerio de Sanidad, 2021. Edita: © MINISTERIO DE SANIDAD CENTRO DE PUBLICACIONES PASEO DEL PRADO, 18-20. 28014. https://cpage.mpr.gob.es/.
- https://www.sanidad.gob.es/bibliotecaPub/repositorio/libros/28943_actividad_de_los_programas_de_cribado_neonatal_en_Espana_-_revision_desde_sus_inicios_hasta_2016.pdf.
- Al-Zaidy SA, Lloyd-Puryear M, Kennedy A, Lopez V, Mendell JR. A Roadmap to Newborn Screening for Duchenne Muscular Dystrophy. Int J Neonatal Screen. 2017; 3: 8. [CrossRef]
- Khodyakov D, Kinnett K, Grant S, Lucas A, Martin A, Denger B, et al. Engaging Patients and Caregivers Managing Rare Diseases to Improve the Methods of Clinical Guideline Development: A Research Protocol. JMIR Res Protoc. 2017; 6: e57. [CrossRef]
- Khodyakov D, Kinnett K, Denger B, Grant S, Armstrong C, Martin A, et al. Developing a Process for Getting Patient and Caregiver Input on Clinical Practice Guidelines [Internet]. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2020. [CrossRef]
- Khodyakov D, Grant S, Denger B, Kinnett K, Martin A, Booth M, et al. Using an Online, Modified Delphi Approach to Engage Patients and Caregivers in Determining the Patient-Centeredness of Duchenne Muscular Dystrophy Care Considerations. Med Decis Making. 2019;39: 1019-1031. [CrossRef]
- Starkweather A, Coleman B, Barcelona de Mendoza V, Fu M, Taylor J, Henderson W, et al. Policy brief: Improve coverage of newborn genetic screening to include the Recommended Uniform Screening Panel and newborn screening registry. Nurs Outlook. 2017; 65: 480-484. [CrossRef]
- Goldenberg AJ, Lloyd-Puryear M, Brosco JP, Therrell B, Bush L, Berry S, et al, Including ELSI research questions in newborn screening pilot studies. Genet Med. 2019; 21: P525-533. [CrossRef]
- Kelly NR, Orsini JJ, Goldenberg AJ, Mulrooney NS, Boychuk NA, Clarke MJ, et al. ScreenPlus: A comprehensive, multidisorder newborn screening program. Mol Gen Metab Reports. 2024; 38: 101037https://doi.org/10.1016/j.ymgmr.2023.101037.
- Alonso-Fernández JR, Colón C. The contributions of Louis I Woolf to the treatment, early diagnosis and understanding of phenylketonuria. J Med Screen. 2009; 16: 205-211. https://www.researchgate.net/publication/40870034_The_contributions_of_Louis_I_Woolf_to_the_treatment_early_diagnosis_and_understanding_of_phenylketonuria [accessed May 29, 2024]. http://msc.sagepub.com/content/16/4/205. [CrossRef]
- Efron ML, Young D, Moser HW, Maccready RA. A SIMPLE CHROMATOGRAPHIC SCREENING TEST FOR THE DETECTION OF DISORDERS OF AMINO ACID METABOLISM. A Technic Using Whole Blood or Urine Collected on Filter Paper. N Engl J Med. 1964;270(26):1378-1383. PMID: 14152868. [CrossRef]
- Alonso-Fernández JR. Tría neonatal de galactosemia: situación del ensayo en orina: Neonatal galactosaemia screening. Urine assay situation. Rev Lab Clín. 2008; 1: 133-134. [CrossRef]
- Alonso-Fernández JR, Castiñeiras Ramos DE, Parrado C, Fraga JM, Peña J. Galactose Newborn Screening: Test for Reducing Sugars in Urine samples Impregnated on Paper. Nov 1986. 6th Intern NBS Symp. 5° Nat NBS Symp. Austin, Texas https://www.researchgate.net/publication/332780669_Galactose_Newborn_Screening_Test_for_Reducing_Sugars_in_Urine_samples_Impregnated_on_Paper.
- Mayor Zaragoza F. Prevención en el neonato de enfermedades que cursan con daño cerebral irreversible, derecho humano. Prevention of irreversible brain damage in newborns, a human right. An RANM. 2024; 141: 80-85.
- Alonso-Fernández JR. Four Decades of Newborn Screening: A Historical Perspective of Laboratory Practices. OBM Genetics 2023; 7(4):1-1. [CrossRef]
- Alonso-Fernández JR, Iglesias AJ, Bóveda MD, Colón C. The vanadium test for reducing sugars in paper-borne urine samples: Conversion from qualitative test to quantitative assay, and application to the detection of galactosemias and other disorders of sugar metabolism. December 2009, 7th International and Latin American Congress Inborn Errors of Metabolism and Neonatal Screening, Cancun, Mexico. https://www.researchgate.net/publication/326319448_The_vanadium_test_for_reducing_sugars_in_paper_borne_urine_samples_Conversion_from_qualit ative_test_to_quantitative_assay_and_application_to_the_detection_of_galactosemias_and_other_disorders_of_sugar.
Figure 1.
Insertion of the translated page, included in the edition of the monograph on the occasion of the centenary of the birth of L I. Woolf [8] with which the prologue ends.
Figure 1.
Insertion of the translated page, included in the edition of the monograph on the occasion of the centenary of the birth of L I. Woolf [8] with which the prologue ends.
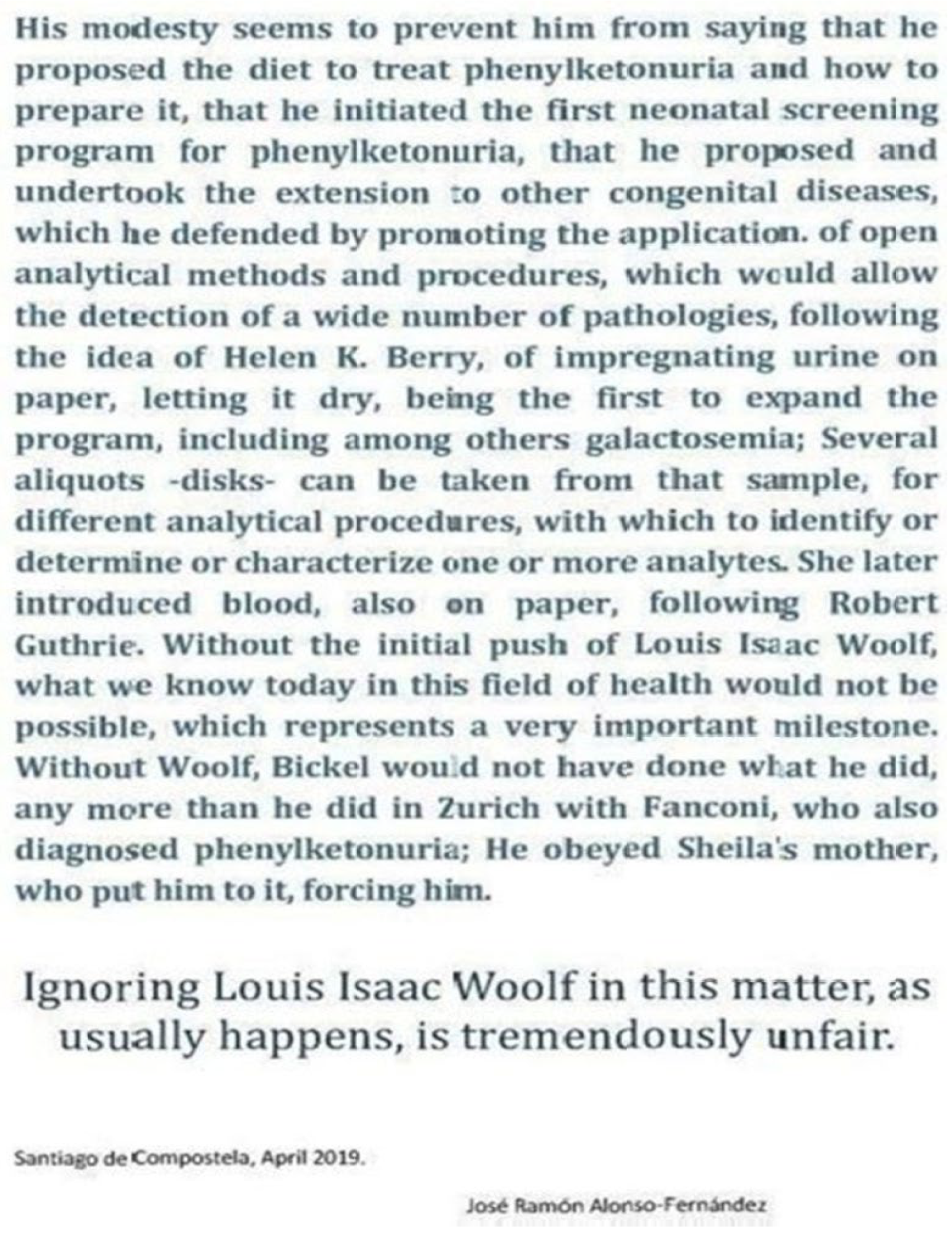
Figure 2.
Louis Isaac Woolf advocates an expanded NBS not confined to PKU, as he wrote in 1968 to Prof. F Mayor.
Figure 2.
Louis Isaac Woolf advocates an expanded NBS not confined to PKU, as he wrote in 1968 to Prof. F Mayor.
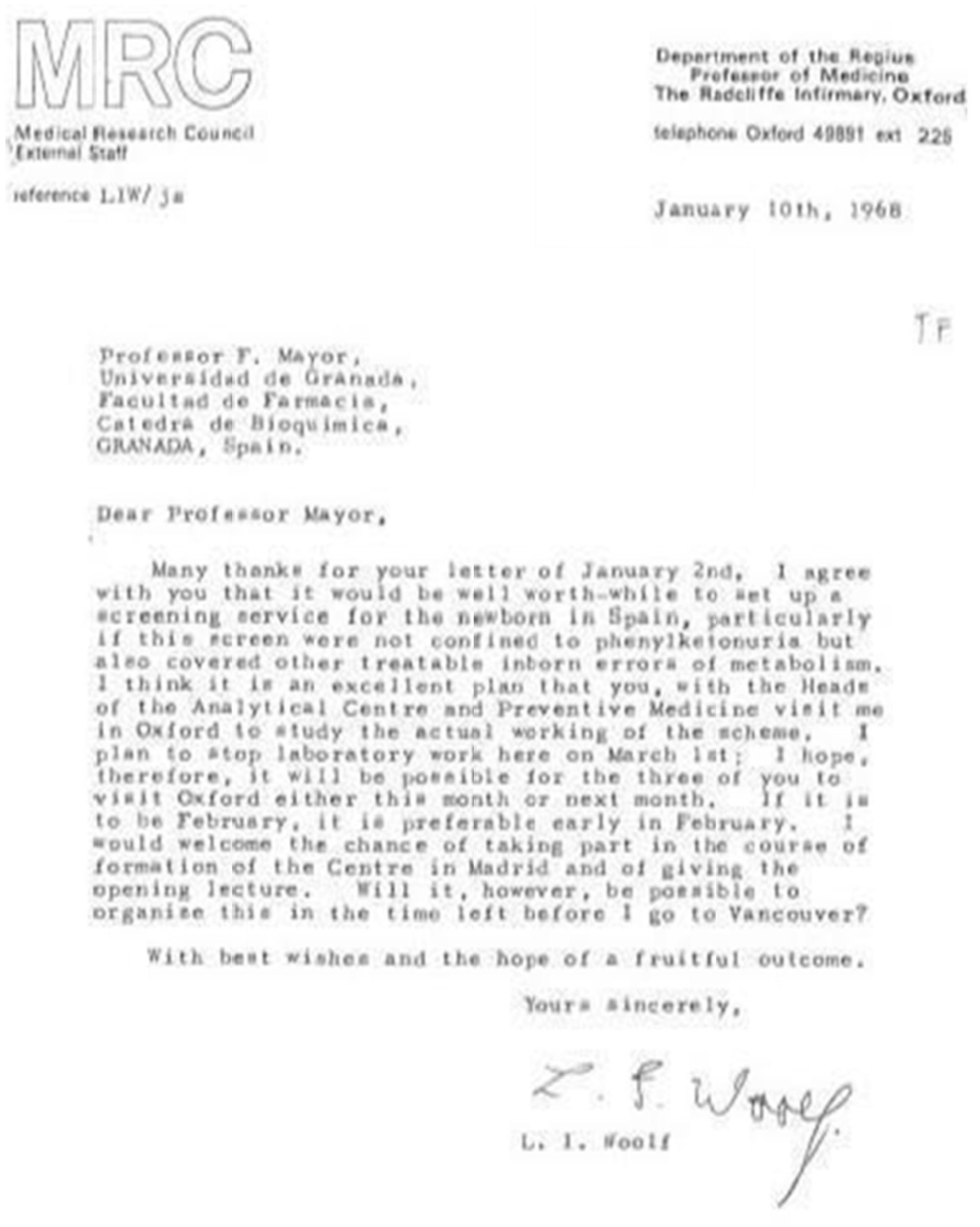
Figure 3.
F Mayor set up an NBS Laboratory financed by the Spanish Government in 1968 in Granada.
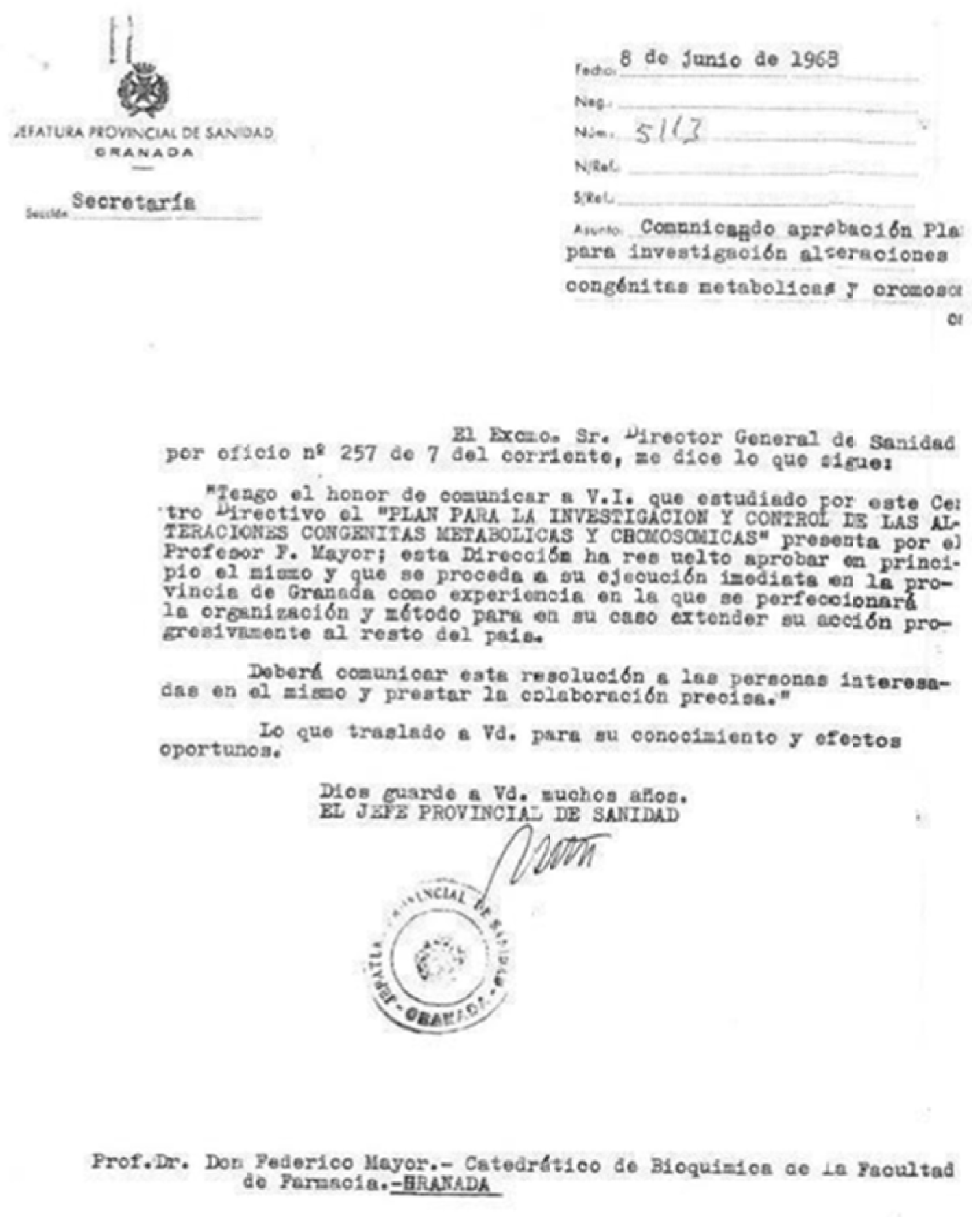
Figure 4.
The outcome of the Change.org petition to the president of the Xunta de Galicia, which aimed to prevent the program's reduction and elimination of urine, is shown.
Figure 4.
The outcome of the Change.org petition to the president of the Xunta de Galicia, which aimed to prevent the program's reduction and elimination of urine, is shown.
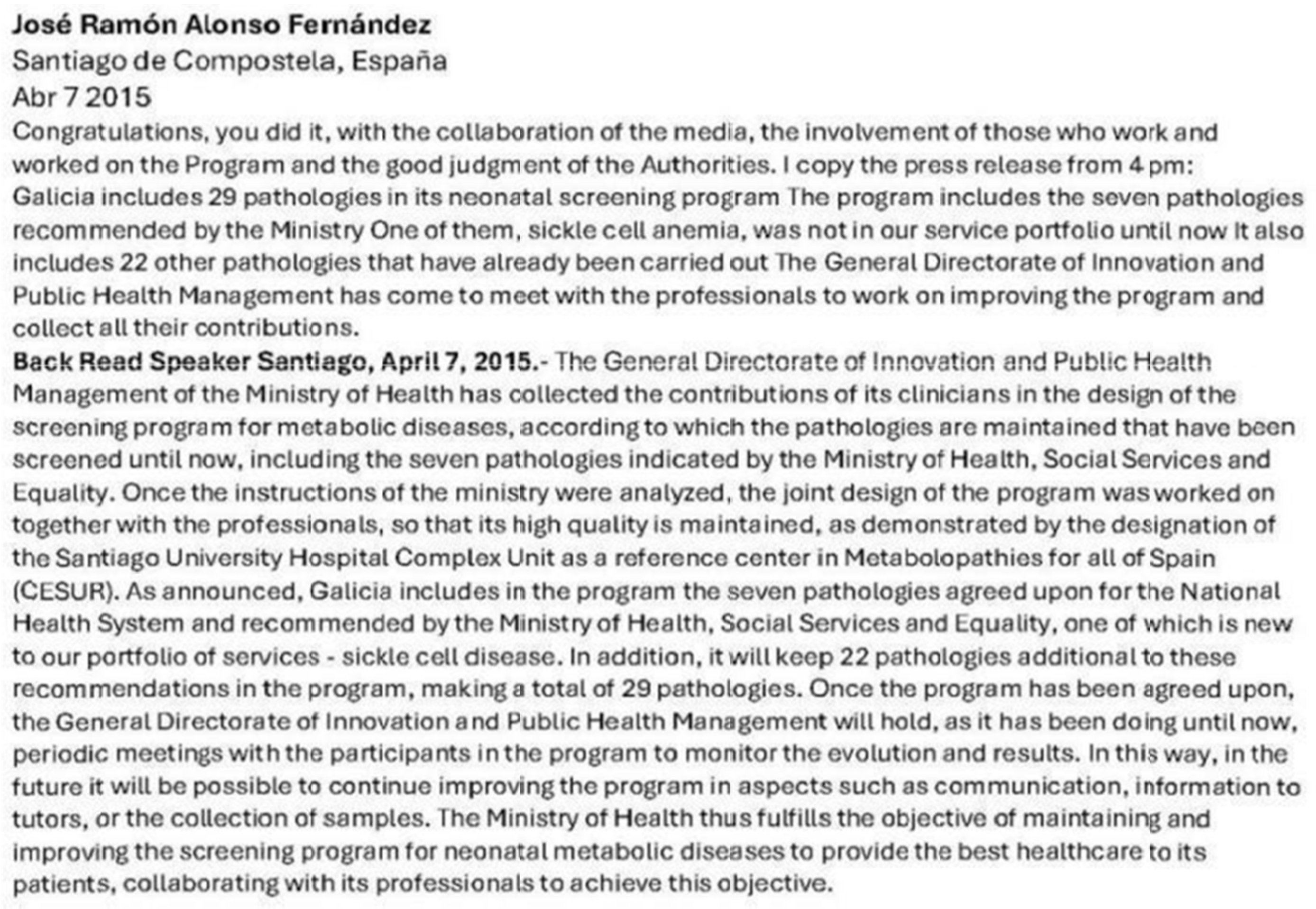
Figure 5.
The textprecedes themonograph title.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



