Submitted:
24 November 2025
Posted:
25 November 2025
You are already at the latest version
Abstract
Background and objective. Low back pain (LBP) is one of the most prevalent musculoskeletal disorders globally, significantly impacting quality of life across diverse populations. Despite its association with middle-aged and older populations, evidence indicates that LBP is increasingly prevalent among younger age groups. Health science students are considered a potential risk factor for LBP; however, longitudinal studies are scarce. This study aims to determine the risk factors for LBP among health science students over a 2-year follow-up. Methods. One hundred ninety-seven of the third-class health science students (Nursing, Physiotherapy, Medical laboratory science, and Emergency Medical services) were contacted (May 2024). A self-administered modified version of the Standardized Nordic Questionnaire, and data about sedentary and physical activity behavior, as well as LBP/ or stress scores, were recorded. Results. A total of 172/197 (87.3%) respondents completed the questionnaire in the 2-year follow-up. Mean age of 25 ±3.5 (years) and body mass index (BMI) value of 23.5 ± 4.3 (kg/m2). About 49% (n= 84) and 20 % (n=34) of the participants had 1-month LBP and functional disability, respectively. No association was found between health science programs and the presence of 1-month LBP (χ²= 0.55, P>0.05). The logistic regression analyses found that males had a significantly lower likelihood of having LBP (OR 0.25, P = 0.03). Conclusions. This study shows a high prevalence of 1-month LBP (48.8%) among health science students at Zefat Academic College. LBP was over time, gender-dependent, and health science-independent.
Keywords: Health science, students, low back pain, stress, females.
Keywords:
health science
; students
; low back pain
; stress
; females
1. Introduction
Low back pain (LBP) represents one of the most prevalent musculoskeletal disorders globally, constituting a leading cause of disability and significantly impacting quality of life across diverse populations [1]. According to the World Health Organization (WHO) LBP affected over 619 million people in 2020, with projections suggesting more than 843 million cases by 2050 if current trends continue [2]. While traditionally associated with middle-aged and older populations, evidence indicates that LBP is increasingly prevalent among younger age groups [3,4]. The WHO statistics show that the annual prevalence of LBP in the young adults (20-44 years) is approximately 20–25%, much higher than in adolescents (10–19 years), where the prevalence is 10-15%, and lower than middle age (45–59 years), where the prevalence is 30-40%. Additionally, some studies reported that a point prevalence (i.e., at the time of the study) of LBP among university students, reached up to 41.2% [5,6,7,8,9,10,11] and this prevalence could be greater in the health science discipline [11,12].
Among health science students, LBP has emerged as a particularly concerning public health issue, with implications extending beyond individual wellbeing to potentially affecting the future healthcare workforce. Health science students, including those pursuing degrees in nursing, physiotherapy, and related fields, demonstrate alarmingly high prevalence rates of LBP that often exceed those observed in the general population of similar age groups [7,13,14,15]. This could be explained by the fact that health science undergraduates are at high risk for developing low back pain due to the demanding nature of their curriculum and lifestyle [10,16,17]. For example, nursing and physiotherapy students spend extended hours studying, attending lectures, and performing clinical practicing, which can result in prolonged sitting or standing postures, repetitive motions, and awkward body positions.
LBP is associated with multidimensional factors (e.g., physical and psychosocial), [18] with insufficient investigations among students in general and health science discipline in particular. Additionally, data regarding variables that are significantly associated with LBP are still ambiguous. Despite the growing recognition of LBP as a significant health concern among health science students, there is a notable absence of longitudinal studies that track the progression of LBP among students from their first class into the advanced years.
Thus, the aims of this study are (1) to establish whether health science programs are associated with LBP and (2) to define the predictive factors for LBP (new and persistent) among health science undergraduates through longitudinal study.
2. Materials and Methods
2.1. Study Design
This prospective study among health science undergraduates, including nursing, physical Therapy, medical laboratory science, and emergency medical services, was conducted during a 2-year follow-up period.
2.2. Sample and Instruments
This study included 172 participants in the follow-up (June 2024) and were part of a large prospective study (n= 197 in the baseline, 2022) at Zefat Academic College in the north of Israel. Subjects were followed up once in the third year of the prospective program, and all have completed at least half of their clinical practices. These participants were re-recruited (re-assigned) in their classrooms by one of the study`s assessors in the same way as it was done in the baseline stage [19]. The Department of Research Ethics Committee at Zefat Academic College (no. 19-2022) approved this study.
We used the same instruments and measures following the baseline recruitment as previously reported [18]. These measures included (a) a structured and anonymous modified questionnaire of the Nordic questionnaire [20], (b) data about sedentary lifestyle and physical activity [21,22], as well as (c) last-year LBP data scores (e.g., frequency, disability, seeking care, and medication use). The frequency of LBP was classified from high frequency (every day) to low frequency (rarely or none). Other LBP scores, such as disability and seeking care, were defined as yes/no answers. We also recorded functional disability following ODI (Oswestry disability index) [23] and variables related to stress score (e.g., education and society) [20] in the last month. Stress score was defined into four subgroups: a- very high, b- high, c- little, and d- none.1-month LBP was considered positive if it lasted at least 12 hours and its intensity scale according to the numeric rating is above five [24].
2.3. Statistical Analysis
We used statistical analysis methods with IBM SPSS version 25. We first checked whether the numerical data followed a normal distribution. Then, McNemar’s and Paired T-tests, as well as two one-way ANOVAs and logistic regression (Method- Enter, dependent variable- 1-month LBP, independent variable- age, gender, sedentary behavior, etc.) analysis were also used. Significant reference was set as P<0.05.
3. Results
3.1. Demographic Features
One hundred seventy-two out of 197 (87.3%), responded and completed the questionnaire at the end of 2-year follow-up (Figure 1). Seventy-six percent of participants were females (n=131), and 41.3% (n=71) were from the nursing program. The mean age and body mass index (BMI) values of the participants were 25 ±3.5 (years) and 23.5 ± 4.3 (kg/m2), respectively (Table 1). In addition, 58.7% of the study sample were involved in physical activity.
Our findings show that health science students in general have a significantly slight decrease in stress score over time (3.10 ± 1.10 vs. 3.33 ± 0.87, t(171) = -2.42, P= 0.016; Cohen`s d = 0.19). Notably, no significant difference was found in the stress relief between the departments (F(3, 168) = 1.34, p > .05, R² = .006).
3.2. Low Back Pain Characteristics
The results indicate that 48.8% (n= 84) and 19.8% (n=34) of the cases had 1-month LBP and functional disability, respectively. The features of 1-year LBP at the follow-up were 70.3% (n=121) with LBP, frequencies vary from every day to once a month, 27.9% (n=48) decreased their daily activity, 22.1% (n=38) sought care, and 25% (n=43) used medication (Table 2).
No association was found between health science programs and the presence of 1-month LBP (χ²= 0.55, P>0.05). For example, 36 participants (20.9%) reported a new onset of LBP compared to 29 cases (16.9%) who had recovered LBP at the follow-up. On the other hand, a remarkable decrease of 1-year LBP score was obtained over the follow-up with a large effect size (d = 0.19) (Table 3). This means that the 1-year LBP score reveals improvement over time in all participants. These improvements varied between the departments, albeit no significant difference was noted (F(3, 168) = 1.18, p = .319, R² = .003). For example, students in the physiotherapy program manifested the largest improvement in LBP score (M = -1.90, SD = 1.62), while those in the Emergency Medicine department showed the smallest one (M = -1.28, SD = 1.79) (Figure 2).
The logistic regression analyses (method- enter, dependent variable- 1-month LBP) found that males significantly (OR- 0.25, P=0.03) decrease the likelihood of having LBP at 2-year follow-up (Table 4). Neither the history of LBP nor the physical activity was associated with LBP. Notably, a similar result was obtained when the logistic regression analysis was conducted to predict only the new onset of LBP (male: OR- 0.28, P= 0.038).
4. Discussion
This 2-year prospective study design with a relatively high follow-up rate (87%), which shed light on the temporal patterns of LBP among future health professionals, investigated the prevalence and predictors of low back pain (LBP) among health science undergraduates in Zefat Academic College.
The findings revealed a high prevalence of both 1-month (48.8%) and 1-year (70.3%) LBP, aligning with our previous studies [19,25] as well as reports obtained from health science undergraduates worldwide [26,27,28,29,30]. These rates are substantially higher than those reported in the general young adult population [2], emphasizing the vulnerability of students in physically and mentally demanding programs such as nursing and physiotherapy. In addition, our outcomes showed that stress score has a remarkable decrease over time despite its small side effect (P= 0.016; Cohen`s d = 0.19).
The logistic regression analysis showed that being a male was associated with a significantly lower likelihood of LBP (OR = 0.25, p = 0.03). This result indicates that females increase the risk factor for both new and persistent cases of LBP over time. Our finding is in agreement with many studies among students and general populations [15,27,31,32,33,34] but contradicts others [28,35,36]. A recent global burden of LBP from 1990 to 2021, has reported that females have higher prevalence rates of LBP than males across all ages [37]. Bizcoca and colleagues have noted in their concepts review that women are affected more frequently by LBP than men [38]. We attribute this outcome to the biological differences, psychosocial and metabolic aspects, as well as genetics and hormonal factors that contribute to the observed sex differences and act as sex-specific pain mediators [39,40,41].
No association was found between health science studies and the presence of 1-month LBP over 2 years of follow-up (χ²= 0.55, P>0.05). The finding indicates that 20.9% of participants reported a new onset of LBP, whereas about 17% had recovered from pain compared to the baseline. In contrast, a significant improvement in 1-year LBP scores (P<0.001, Cohen d= 0.859) has been recorded over time. Notably, physiotherapy students attained the greatest relief in 1-year LBP score compared with other programs. The plausible explanation of the lack of relationship between health science students and LBP in the current study is (1) a decrease in 1-month stress score, (2) about half of the participants are physically active, and (3) students in general, particularly in physiotherapy program receive a back school education during the academic program. In addition, the discrepancy in LBP outcomes (1-month vs. 1-year score) could be mainly attributed to recall biases and the fact that the 1-year scores included four variables, compared to just one for LBP at the last month (yes/no response).
Our finding challenges the uprising notion that health science studies increase the risk for LBP [10,26,42,43]. For example, Falavigna and colleagues have clearly demonstrated the association between physiotherapy undergraduates’ study and LBP [10]. Additionally, a review and meta-analyses study among nurses and medical students declared from strong and moderate evidence that students of the final year of study were associated with a higher 12-month low back pain prevalence in both student groups [42]. On the other hand, a literature review and prospective cohort study among undergraduates nurses, declared that there was no significant change on LBP prevalence over time [44].
Although factors related to LBP have been extensively investigated in the literature, to our knowledge, few prospective studies have been conducted in both general and student populations. A 1-year prospective study by Kanchanomai and colleagues (2015) among healthy Thai students previously reported that a lack of low-back support during computer work and quadriceps muscle tightness are significantly associated with LBP [45]. Another prospective study (2010) among female nursing students has demonstrated that smoking, increased physical activity, higher stress, greater pelvic rotation, and reduced muscle endurance were significant and independent predictors for new onset of LBP [46]. Two prospective studies among British schoolchildren (11-14 years) and newly female health care workers have previously reported that emotional problems and somatic symptoms, as well as high physical work load, were significantly associated with LBP, respectively [47,48]. The diversity of the studies` outcomes regarding the factors related to LBP is primarily due to the multi-dimensional nature of this phenomenon; therefore, researchers should consider all these variables. Additionally, reflecting the potential variations of the studies, such as the sample (e.g., students, schoolchildren), methodology, and design (e.g., cross-sectional or prospective study), is required.
4.1. Clinical Implication
Although no association has been mentioned between health science studies and LBP over time, educational programs should be implemented targeting females to reduce the high prevalence of LBP.
4.2. Limitations of the Study
This study has several limitations. First, it was conducted in a single academic institution, which may limit the generalizability of the results to other health science programs or populations. Second, the data were based on self-reported questionnaires, which could be influenced by recall or reporting bias. Third, no objective clinical/ or ergonomic assessments were included, preventing the verification of reported LBP through physical examination. Fourth, the participants were followed up only once, as data were collected/ or confirmed twice during the study (baseline and follow-up). Finally, the sample size within each department was relatively small, so no stratified group comparisons were conducted.
5. Conclusions
The results confirm the high prevalence of 1-month LBP (48.8%) among health science students. Being heath science undergraduates were not associated with LBP. Females increase the risk for new and persistent cases of LBP.
References
- Zhang, C.; Qin, L.; Yin, F.; Chen, Q.; Zhang, S. Global, regional, and national burden and trends of Low back pain in middle-aged adults: analysis of GBD 1990–2021 with projections to 2050. BMC Musculoskeletal Disorders. 2024 Nov 7;25(1):886.
- Ferreira, M.L., De Luca, K., Haile, L.M., Steinmetz, J.D., et al. Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. The Lancet Rheumatology, 2023, 5(6), pp.e316-e329.
- Al Amer, H.S. Low back pain prevalence and risk factors among health workers in Saudi Arabia: a systematic review and meta-analysis. Journal of occupational health, 2020, 62(1), p.e12155.
- Hoy, D., Bain, C., Williams, G., March, L., et al. A systematic review of the global prevalence of low back pain. Arthritis & rheumatism, 2012, 64(6), pp.2028-2037.
- Alshehri, M.M., Alqhtani, A.M., Gharawi, S.H., Sharahily, R.A., et al. Prevalence of lower back pain and its associations with lifestyle behaviors among college students in Saudi Arabia. BMC Musculoskeletal Disorders, 2023, 24(1), p.646.
- Daldoul, C., Boussaid, S., Jemmali, S., Rekik, S., Sahli, H., Cheour, E. and Elleuch, M. Low back pain among medical students: prevalence and risk factors. 2020. AB0962.
- AlShayhan, F.A. and Saadeddin, M. Prevalence of low back pain among health sciences students. European Journal of Orthopaedic Surgery & Traumatology, 2018, 28(2), pp.165-170.
- Vujcic, I., Stojilovic, N., Dubljanin, E., Ladjevic, N., Ladjevic, I. and Sipetic-Grujicic, S. Low Back pain among medical students in Belgrade (Serbia): a cross-sectional study. Pain Research and Management, 2018 (1), p.8317906.
- Aggarwal, N., Anand, T., Kishore, J. and Ingle, G.K. Low back pain and associated risk factors among undergraduate students of a medical college in Delhi. Education for health, 2013, 26(2), pp.103-108.
- Falavigna, A., Teles, A.R., Mazzocchin, T., de Braga, G.L., et al. Increased prevalence of low back pain among physiotherapy students compared to medical students. European Spine Journal, 2011, 20(3), pp.500-505.
- Hafeez, K., Memon, A.A., Jawaid, M., Usman, S., et al. Back pain–are health care undergraduates at risk?. Iranian journal of public health, 2013, 42(8), p.819.
- Nordin, N.A.M., Singh, D.K.A. and Kanglun, L. Low back pain and associated risk factors among health science undergraduates. Sains Malaysiana, 2014, 43(3), pp.423-428.
- Yucel, H.; Torun, P. Incidence and Risk Factors of Low Back Pain in Students Studying at a Health University. Bezmialem Sci, 2016, 4: 12-18.
- Crawford, R.J., Volken, T., Schaffert, R. and Bucher, T. Higher low back and neck pain in final year Swiss health professions’ students: worrying susceptibilities identified in a multi-centre comparison to the national population. BMC Public Health, 2018, 18(1), p.1188.
- Isa, S.N.I., Kamalruzaman, N.S.A., Sabri, T.A.T. and Zamri, E.N. Associated Factors of Lower Back and Neck Pain Among Health Sciences Undergraduate Students in a Public University in Malaysia. Malaysian Journal of Medicine & Health Sciences, 2022, 18.
- Algarni, A.D.; Al-Saran, Y.; Al-Moawi, A.; Bin Dous, A.; Al-Ahaideb, A.; Kachanathu, S.J. The prevalence of and factors associated with neck, shoulder, and low-back pains among medical students at university hospitals in Central Saudi Arabia. Pain Res. Treat. 2017, 1, 1235706.
- Feyer, A.M.; Herbison, P.; Williamson, A.M. The role of physical and psychological factors in occupational low back pain: A prospective cohort study. Occup. Environ. Med. 2000, 57, 116–120.
- O’Sullivan, P.; Smith, A.; Beales, D.; Straker, L. Understanding adolescent low back pain from a multidimensional perspective: implications for management. journal of orthopaedic & sports physical therapy. 2017 Oct;47(10):741-51.
- Abbas, J.; Yousef, M.; Hamoud, K.; Joubran, K. Low Back Pain Among Health Sciences Undergraduates: Results Obtained from a Machine-Learning Analysis. Journal of Clinical Medicine. 2025; 14(6):2046. [CrossRef]
- Kuorinka, I.; Jonsson, B.; Kilbom, A. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237.
- Jessor, R.; Turbin, M.S.; Costa, M.F. Survey of Personal and Social Development at CU; Institute of Behavioral Sciences, University of Colorado: Boulder, CO, USA, 2003; Volume 19, p. 2016. Available online: http://www.colorado.edu/ibs/jessor/questionnaires/ questionnaire_spsd2.pdf (accessed on 15 December 2021).
- Thompson, W.R.; Gordon, N.F.; Pescatello, L.S. American College of Sport Medicine. In ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2014.
- Fairbank, J.C.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 25, 2940–2952.
- Dionne, C.E.; Dunn, K.M.; Croft, P.R. A consensus approach toward the standardization of back pain definitions for use in prevalence studies. Spine 2008, 33, 95–103.
- Abbas, J.; Hamoud, K.; Jubran, R.; Daher, A. Has the COVID-19 outbreak altered the prevalence of low back pain among physiotherapy students? J Am Coll Health. 2023 Oct;71(7):2038-2043. PMID: 34353241. [CrossRef]
- Nyland, L.J.; Grimmer, K.A. Is undergraduate physiotherapy study a risk factor for low back pain? A prevalence study of LBP in physiotherapy students. BMC Musculoskelet Disord. 2003 Oct 9;4:22. PMID: 14536021; PMCID: PMC270026. [CrossRef]
- Awad, M.Y.H., Warasna, H.J.M., Awad, B.Y.H., Shaaban, M.E. Prevalence of lower back pain and its associations with lifestyle behaviors among university students in the West Bank, Palestine: a cross-sectional study. Annals of Medicine, 2025, 57(1), p.2522974.
- Feleke, M., Getachew, T., Shewangizaw, M. et al. Prevalence of low back pain and associated factors among medical students in Wachemo University Southern Ethiopia. Sci Rep , 2024, 14, 23518. [CrossRef]
- Alrabai, H.M., Aladhayani, M.H., Alshahrani, S.M., Alwethenani, Z.K., Alsahil, M.J. and Algarni, A.D. Low back pain prevalence and associated risk factors among medical students at four major medical colleges in Saudi Arabia. Journal of Nature and Science of Medicine, 2021, 4(3), pp.296-302.
- Behairy, M., Odeh, S., Alsourani, J., Talic, M., et al. Prevalence of Lower Back Pain (LBP) and Its Associated Risk Factors Among Alfaisal University Medical Students in Riyadh, Saudi Arabia: A Cross-Sectional Study. In Healthcare 2025, June, p. 1490. MDPI. [CrossRef]
- Grimmer, K.; Williams, M. Gender-age environmental associates of adolescent low back pain. Appl Ergon. 2000 Aug;31(4):343-60. PMID: 10975661. [CrossRef]
- Cakmak, A.; Yücel, B.; Ozyalçn, S.N.; Bayraktar, B.; et al. The frequency and associated factors of low back pain among a younger population in Turkey. Spine (Phila Pa 1976). 2004 Jul 15;29(14):1567-72. PMID: 15247580. [CrossRef]
- Tavares, C., Salvi, C.S., Nisihara, R. et al. Low back pain in Brazilian medical students: a cross-sectional study in 629 individuals. Clin Rheumatol 38, 939–942 (2019). [CrossRef]
- Sany, S.A.; Tanjim, T.; Hossain, M.I. Low back pain and associated risk factors among medical students in Bangladesh: a cross-sectional study. F1000Res. 2021 Jul 30;10:698. PMID: 35999897; PMCID: PMC9360907. [CrossRef]
- Amelot, A.; Mathon, B.; Haddad, R.; Renault, M.C.; Duguet, A.; Steichen, O. Low Back Pain Among Medical Students: A Burden and an Impact to Consider! Spine (Phila Pa 1976). 2019 Oct 1;44(19):1390-1395. PMID: 31261281. [CrossRef]
- Ganesan, S.; Acharya, A.S.; Chauhan, R.; Acharya, S. Prevalence and Risk Factors for Low Back Pain in 1,355 Young Adults: A Cross-Sectional Study. Asian Spine J. 2017 Aug;11(4):610-617. Epub 2017 Aug 7. PMID: 28874980; PMCID: PMC5573856. [CrossRef]
- Li, Y.; Zou, C.; Guo, W.; Han, F.; Fan, T.; Zang, L.; Huang, G. Global burden of low back pain and its attributable risk factors from 1990 to 2021: a comprehensive analysis from the global burden of disease study 2021. Front Public Health. 2024 Nov 13;12:1480779. [CrossRef]
- Bizzoca, D.; Solarino, G.; Pulcrano, A.; Brunetti, G.; et al. Gender-Related Issues in the Management of Low-Back Pain: A Current Concepts Review. Clin Pract. 2023 Oct 30;13(6):1360-1368. [CrossRef]
- Dev, R.; Raparelli, V.; Bacon, S.L.; Lavoie, K.L.; Pilote, L.; Norris, C.M.; iCARE Study Team. Impact of biological sex and gender-related factors on public engagement in protective health behaviors during the COVID-19 pandemic: Cross-sectional analyses from a global survey. BMJ Open 2022, 12, e059673.
- Nielsen, M.W.; Stefanick, M.L.; Peragine, D.; Neilands, T.B.; Ioannidis, J.P.A.; Pilote, L.; Prochaska, J.J.; Cullen, M.R.; Einstein, G.; Klinge, I.; et al. Gender-related variables for health research. Biol. Sex Differ. 2021, 12, 23.
- Fillingim, R.B.; King, C.D.; Ribeiro-Dasilva, M.C.; Rahim-Williams, B.; Riley III, J.L. Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain. 2009 May;10(5):447-85. PMID: 19411059; PMCID: PMC2677686. [CrossRef]
- Wong, A.Y.L; Chan, L.L.Y; Lo, C.W.T; Chan, W.W.Y.; et al. Prevalence/Incidence of Low Back Pain and Associated Risk Factors Among Nursing and Medical Students: A Systematic Review and Meta-Analysis. First Published: 25 January 2021.
- Wami, S.; Mekonnen, T.; Yirdaw, G.; Abere, G. Musculoskeletal problems and associated risk factors among health science students in Ethiopia: a cross-sectional study. J. Public Health. 2020;29(2):1-7.
- Menzel, N.; Feng, D.; Doolen, J. Low Back Pain in Student Nurses: Literature Review and Prospective Cohort Study. Int J Nurs Educ Scholarsh. 2016 May 13;13:/j/ijnes. PMID: 27176750. [CrossRef]
- Kanchanomai, S.; Janwantanakul, P.; Pensri, P.; Jiamjarasrangsi, W. Risk factors for the onset and persistence of neck pain in undergraduate students: 1-year prospective cohort study. BMC Public Health. 2011 Jul 15;11:566. [CrossRef]
- Mitchell, T.; O’Sullivan, P.B.; Burnett, A. Identification of modifiable personal factors that predict new-onset low back pain: a prospective study of female nursing students. Clin J Pain. 2010, 26, 275-283.
- Jensen, J.N.; Holtermann, A.; Clausen, T.; Mortensen, O.S.; et al. The greatest risk for low-back pain among newly educated female health care workers; body weight or physical work load? BMC Musculoskelet Disord. 2012 Jun 6;13:87. [CrossRef]
- Jones, G.T.; Macfarlane, G.J. Predicting persistent low back pain in schoolchildren: a prospective cohort study. Arthritis Rheum. 2009 Oct 15;61(10):1359-66. [CrossRef]
Figure 1.
Flow chart for the study sample after 2-year follow up.
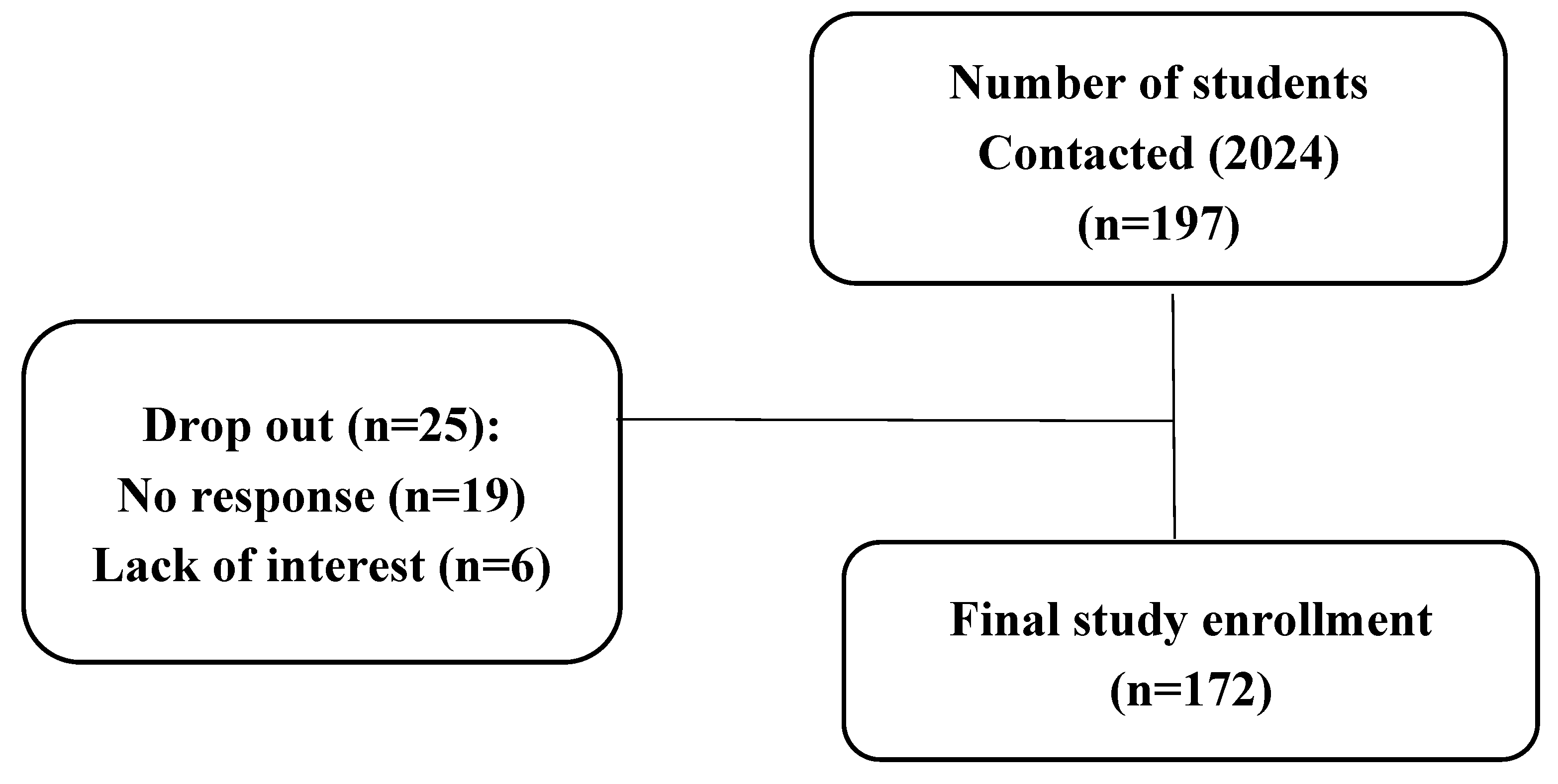
Figure 2.
Mean differences of 1-year LBP scores by department (baseline vs. follow up). Negative values depict improvement in LBP score.
Figure 2.
Mean differences of 1-year LBP scores by department (baseline vs. follow up). Negative values depict improvement in LBP score.
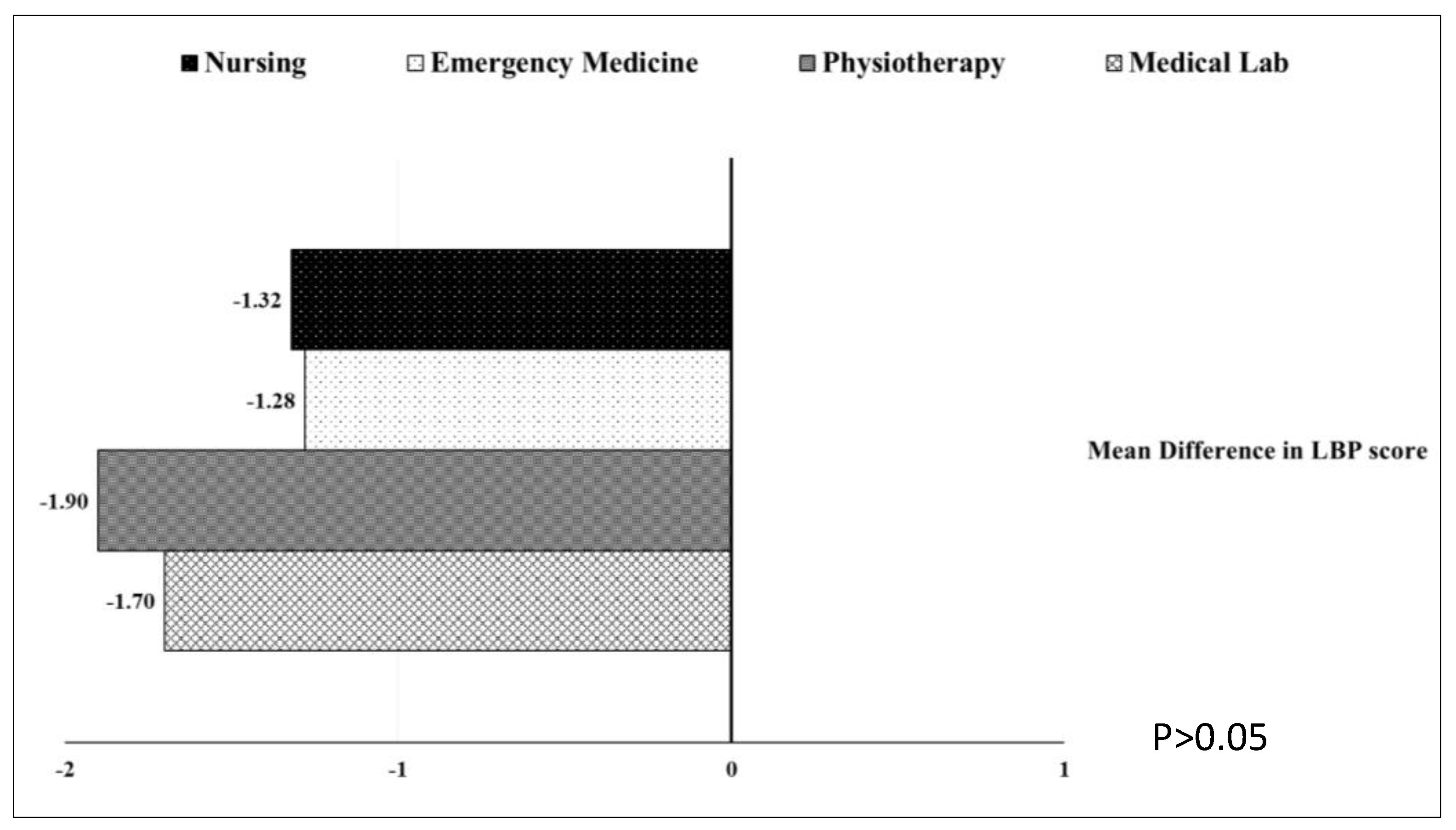

Table 1.
Sample size characteristics at 2-year follow up.
| Variable | n (%)/ or mean ± SD |
| Male Female |
41 (23.8) 131 (76.2) |
| Mean age (year) | 25.1 ± 3.5 |
| Mean BMI (kg/m2) | 23.5 ± 4.3 |
| Physical activity | 101 (58.7) |
| Department: Nursing Physical therapy Medical Lab Emergency Medical Services |
71 (41.3) 39 (22.7) 33 (19.2) 29 (16.9) |
BMI- Body mass index, SD- standard deviation.
Table 2.
Low back pain characteristics of the study sample at 2-year follow up.
| N (%) | |
| 1-year LBP: 1. Frequency of LBP:
3. Seeking-care 4. Medication consumption |
40 (23.3) 46 (26.7) 35 (20.3) 51 (29.7) 48 (27.9) 38 (22.1) 43 (25) |
| 1-month LBP | 84 (48.8) |
| 1-month functional disability | 34 (19.8) |
Table 3.
Paired t-test for 1- year LBP score over time.
| Period | Mean | SD | T | P | Cohen’s d | |
| 1-year LBP Score | Pre | 3.26 | 0.812 | -11.25 | <0.001 | 0.859 |
| Post | 1.74 | 1.558 |
SD- standard deviation.
Table 4.
Variables that were associated with LBP over years (new and persist LBP).
| Predictor | OR | 95% CI | P |
| Department | .892 | ||
| Medical Lab (reference) | - | - | - |
| Physiotherapy | 1.19 | [0.47, 2.98] | .715 |
| Emergency Medicine | 0.81 | [0.31, 2.10] | .663 |
| Nursing | 1.19 | [0.43, 3.31] | .737 |
| Gender (Male) | 0.25 | [0.10, 0.62] | .003* |
| Physical activity pre (Yes) | 0.88 | [0.43, 1.81] | .723 |
| Daily continuously sitting (> 5 hr) | 0.62 | [0.30, 1.28] | .194 |
| Daily average sitting (> 8hr) | 0.61 | [0.29, 1.31] | .206 |
| LBP history pre (Yes) | 2.06 | [0.92, 4.59] | .077 |
| Hospitalization history pre (Yes) | 0.86 | [0.12, 5.96] | .878 |
| Disability history pre (Yes) | 0.82 | [0.36, 1.89] | .645 |
| Seeking care history pre (Yes) | 1.95 | [0.61, 6.29] | .261 |
| Medication use pre (Yes) | 1.01 | [0.37, 2.72] | .991 |
| Stress due to family pre (Yes) | 0.66 | [0.29, 1.50] | .324 |
| Stress due to personal life pre (Yes) | 0.57 | [0.14, 2.30] | .432 |
| Stress due to social life pre (Yes) | 1.19 | [0.55, 2.57] | .649 |
| Nagelkerke R² = .19 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



