
Submitted:
21 November 2025
Posted:
24 November 2025
You are already at the latest version
Abstract
Various recurring medical events encourage innovative patient well-being through con-nected health strategies based on an elegant digital environment that prioritizes safety, comfort, and beneficial outcomes for both patients and medical staff. This article aims to investigate and highlight the potential of advanced, reliable, high-precision, and secure medical observation and intervention missions. These involve an intelligent digital envi-ronment integrating smart materials combined with intelligent digital monitoring. These medical implications concern robotic surgery and drug delivery through image-assisted implantation, as well as wearable observation and assistive tools. The former requires high-precision motion and positioning strategies, while the latter enables sensing, diag-nosis, monitoring, and central task assistance. Both advocate minimally invasive or non-invasive procedures and precise supervision through autonomously controlled processes with staff participation. The article analyzes the requirements and evolution of medical interventions, robotic actuation technologies for positioning actuated and self-moving in-stances, monitoring of image-assisted robotic procedures using digital twins and aug-mented digital tools, and wearable medical detection and assistance devices. A discussion including future research perspectives and conclusions terminate the article. The different themes addressed in the proposed paper, although self-sufficient, are supported by exam-ples of the literature, allowing a deeper understanding.
Keywords:
smart digital environment
; smart materials
; augmented digital tools
; medical interventions
; wearable observation and assistive tools
; image-assisted robotics
; patient well-being and staff ease
1. Introduction
Human society has always sought well-being in terms of health, safety, and comfort. The role of health in this context has evolved steadily, with among others, observation and detection on the one hand and treatment through medical assistance or intervention on the other. These different tasks are associated with dedicated instruments and specific skills of medical personnel. Definitely, observation and detection deeds concerning different measures such as body temperature, heart rate, etc. allow medical staff to diagnose and predict health problems and decide which organ needs assistance such as stimulation, support, etc. or intervention such as drug administration or surgery.
Indeed, originally, observations were based on the natural sensory capacities of man, namely vision, hearing, touch, etc., thus detecting internal disturbances of the body from the outside using sensory-assisted tools such as a flashlight for vision, a stethoscope for hearing, etc. The same goes for interventions, but through invasive cuts with strong light from external projectors and specific tools assisted by touch. These techniques are still used profitably but can be substituted advantageously in many specific situations. It should be noted that treatment progress depends generally on pathology evolution, see for example the historical dynamic of bone pathologies [1].
Actually, observation, detection, and assistance instruments ought to be non-invasive or minimally invasive and operate with precision in real time. Drug administration and surgical tools require the same conditions, in addition to increased precision regarding movement and positioning, thus allowing the delimitation of treatment to the affected areas without hurting healthy tissues [2]. These supreme conditions of medical care were once a dream and gradually advanced in medical history with the goal of being achieved one day in several specific circumstances.
Recent technological advances in sensors, actuated robotics, and imaging tools have enabled global advances in medical observation and treatment. The introduction of wearable [3] and assistive [4,5,6] body-based sensing tools, on the one hand, and the robotization of medical interventions, and autonomous image-assisted procedures [7] on the other, are indeed associated with this technological evolution.
Topical medical autonomous tasks controlled in a closed loop under staff supervision permitted valuable machine-man interaction in personalized healthcare. The reliability of the involved control can be affected by different factors, mainly the complexity of procedure interacting components, the uncertainties involved in their parameters evaluation, and unforeseen external threats. Accounting for such defies and for specific personal data are fundamental for a reliable operational procedure. Such targets might be attained via smart digital management as digital twin (DT) implement monitoring [8,9]. Such digital treatment participates in effect to the high-reliability precision of medical therapies allowing for patient security and staff ease. Furthermore, digital-augmented procedures involving artificial intelligence (AI) [10,11,12], and digital conversion via extended reality (xR) [13,14,15] - including augmented reality (AR), virtual reality (VR) and mixed reality (MR) - has come to be a central piece of the forthcoming of medical and interventional exercise. Such tools enable data processing reduction, progressing the whole procedure organization, personalized medical therapies, progressed interventional planning, tutoring, and cure adjusting, restructuring both individual and formal healthcare. The practice of such smart digital tools reflects an intelligent digital monitoring.
The use of smart materials [16,17] associated with intelligent digital monitoring [7] can significantly advance the abovementioned medical features, improving patient well-being and facilitating the work of medical staff. Such smart environments are increasingly integrated into industrial processes and have recently begun in medical applications [18]. These include smart materials in wearable or integrated sensing tools and actuators for robotics, as well as digital monitoring tools for medical interventions. Moreover, smart monitoring also enables treatment to be tailored to individual profiles thanks to precision medicine [19,20], which has revolutionized diagnosis and treatment, as well as the prescription of targeted drugs with extreme precision. This not only improves treatment effectiveness, but also reduces the common side effects of conventional therapies. In addition, different recent works on digital healthcare involving mobile and electronic health technologies could found in literature, see for example [21].
Furthermore, in the context of sustainability, the components involved in such smart environments must be protected from exposure to electromagnetic (EM) fields (EMFs), which are increasingly present in current everyday use [22]. This can be achieved by using materials immune to EM interference (EMI) or via smart shielding [23]. In this way, these components will be protected and, in turn, they will not disturb their surrounding environment and will therefore behave in a sustainable manner. Thus, such a smart medical environment can significantly contribute to the reliability and personalization of patient care, as well as the planning, training, forecasting and execution of tasks of medical staff, while reflecting a sustainable behavior.
In the above discussion, it is worth mentioning that the substitution of traditional medical environment with smart and sustainable environment is concerned at different levels, involving the procedure strategy, component materials and behavioral action. Regarding the strategy of both wearable and interventional tasks, the substitution concerns the replacement of complex repetitive tasks requiring long hospitalization periods by autonomous systems with staff in direct or remote monitoring. For component materials, substitution involves replacing complex commands converting a given energy into signals for sensing tasks and into mechanical energy for actuation tasks, with simple and direct conversions inherent in smart materials [24]. Regarding behavioral action, substitution consists of replacing manual and visual tasks with intelligent and reliable supervision [7].
It should be noted that this substitution does not correspond to an absolute hierarchy but, as previously indicated, is linked to specific situations. The traditional environment, therefore, retains its place and is used advantageously in many cases.
The proposed contribution aims to analyze and highlight the potential of tasks performing reliable, high-precision and safe advanced medical observations and interventions through management involving a smart digital environment. These concern medical robotic surgery and implanted drug delivery assisted by imaging and wearable sensing and assistance tools.
The next sections detail such objectives. Section 2 reviews the demands and evolution of medical interventions including surgical and assistive drug delivery procedures, based on the characteristics of different interventional techniques and leading to accurate and safe image-assisted robotic autonomous interventions. Section 3 discusses robotic actuation technologies including positioning actuated robotic and self-moving miniature robotic procedures as well as image-assistance in robotic procedures related to magnetic resonance imaging (MRI). Section 4 investigates the monitoring of MRI-assisted robotic procedures through DT supervision of procedure control and digital environment augmented tools. Section 5 examines appliances of wearable detecting and assistive medical devices including, multifunctional activities and flexible wearable instruments, and their EM compatibility (EMC) control. Section 6 shares out several discussions connected to added fine points on themes from the preceding sections, including research perspectives. Section 7 is dedicated to conclusions.
2. Requests and Evolution of Medical Interventions
Medical interventions essentially include surgical procedures and assistive drug administration procedures. Both interventions aim to be precise and safe, ensuring comfort and beneficial outcomes for patients. Patient well-being depends on various factors such as the degree of tissue intrusion, instrument positioning and accuracy, procedure duration, speed of recovery, etc. These factors are also related to the dexterity (vision and touch) of medical staff, their ergonomics, and ease of execution. Moreover, the execution of these interventions should be accurately restricted to the concerned zone, thus preserving healthy contiguous tissues. The prospect of safe and autonomous minimally invasive (MI) intervention, involving instruments replacing dexterity and visual abilities and fully supervised by staff, was a previous goal that has become achievable thanks to current digital intelligence. This digital environment is expanding with the evolution of interventional techniques, from open invasive intervention to MI laparoscopic, then to its robotic version, then to computerized robotics and, more recently, to image-assisted robotics interventions [7].
2.1. Features of Different Interventional Techniques
Since the dawn of surgery, the open procedure has been commonly used to “see the whole thing” and has been used to date in situations involving complex outline and difficult interventions. However, the intrusive nature of open procedures presents risks in certain specific situations, and MI interventions are preferred.
This long-established open procedure has been profoundly updated by the use of laparoscopy, which offers various advantages to patients in the context of MI practice [25,26]. The MI method converted the line of attack through a small cut to distinct regions of the body by providing an expanded perspective through a small camera and a mini-sized instrument equipped at its end with a light source [27,28]. Furthermore, the laparoscopic procedure is associated with reduced postoperative distress and faster healing, thus reducing hospitalization times [27,28,29]. In addition, it offers substantial advantages, such as improved incision aesthetics and reduced risk of injury [27], and also allows for laparoscopic diagnosis [30]. However, laparoscopic procedures employing elongated tools besides to 2-D picturing exposures may cause operational ergonomic risks [25,31] and likely amplified postoperative menace [32]. A robotized variety of such procedure can largely attenuate such risks through robotic tasks as stitch up, and tissue provide processes [33]. Subsequently, only a MI procedure supported by computerized robotics can circumvent all the aforementioned restrictions.
Regarding the computerized robotic procedure, operational proficiency and ergonomics are enhanced through 3D visualization, amplification of robotic degree of freedom as well as improvement for large-scale advancement in MI interventional exercise, e.g., [34,35,36]. Robotic process flow has evolved from slight passive actions such as tool retraction or camera pointing to dynamic machine engagements allowing for further execution and greater accuracy for finishing and sealing while using an MI approach in self-sufficient interventions, e.g., [37,38,39] in addition to personnel control, e.g., [40,41,42]. Moreover, it excludes tactile trembles and laparoscopic fulcrum upshots. Robotic wrist devices offer large degrees of freedom to overcome the limitation of laparoscopic instruments, which generally do not allow their pointer to reach anterior tissue and allow stitching in challenging ergonomic positions.
As mentioned before, safe, autonomous MI intervention [43] involving accurate positioning and visual skills smart substitute, alongside with staff supervision, can be accomplished owing to smart digital management. Accordingly, along with patient well-being, staff facility and MI advantages, the projected truthful positioning and 3D visualization facility could be profitably attained by means of consistent image-assisted robotic intervention. In fact, such interventional procedure appears to be a perceptible downward of other MI interventions together with an obvious skill amplification along with surgeon enfolding an easier deportment all through intervention [2,7,44,45]. Furthermore, such assisted interventions are well adjusted for complicated surgeries [46,47,48,49] or delimited drugs deliveries [50,51,52], both necessitate actions in a restricted zone, to preserve healthful tissues approaching the worried region.
2.2. Accurate and Safe Image-Assisted Robotic Autonomous Interventions
As abovementioned a safe, autonomous MI intervention involving precise positioning and visual skill can be helpfully achieved by reliable robotic system supported by imaging scanners. Such safety is associated to two factors related to the positioning accuracy and the intervention duration, which is closely linked to the choice of the scanner technology. In reality, the positioning accuracy guarantees a restricted action in the affected tissue area and can be achieved through an adequate actuation device, while relatively long imaging periods, as in interventional therapies, preclude the use of imaging techniques reflecting ionizing behaviors; the body tissues and robotic tools are close to or inside the scanner. Thus, magnetic resonance imaging (MRI) and ultrasound are generally used in this type of situation. [46,47,48,49].
MRI is increasingly being used in surgery and drug administration, mainly due to its greater capacity to differentiate tumors from healthy tissues in interventions such as tumor extraction [53,54,55,56] or drug administration [2,7]. In addition, MRI can be used on all types of tissues, dissimilar ultrasound, which is restricted to body tissues without air or bone. However, MRI practice is susceptible to EMI. Therefore, robotic machines and interventional instruments used in an MRI-assisted practice must be immune to such interference.
Comparing traditional intervention to image-assisted robotic intervention, the surgeon uses his vision combined with his fingers through brain processing control in the first case, while the action of the robotic tool is assisted by the scanner through digital image processing control in the second. Indeed, the therapeutic safety restriction related to the troubled area, is essentially related to the precision of the robotic actuation and, consequently, to the positioning of the interventional tool in space. Thus, a support organization including the scanner, the imaged restricted troubled zone including the tool position, image processing control, involving localization, and tasks, of robotic actuation, all executed in a closed-loop autonomous system, as illustrated in Figure 1.
It should be noted that the use of image assistance benefits in medical therapy is not limited to the robotic interventions mentioned above and is used in other different therapies to eradicate tumors such as image-guided focused ultrasound-generated hyperthermia and image-guided radiotherapy (IGRT), which uses directed energy beams such as X-rays or protons [57,58].
3. Robotic Actuation Technologies
The various robotic interventions presented in the last section, including robotic laparoscopy, computer-assisted robotics, and image-guided robotics, necessitate actuation for movement and positioning. Various actuation mechanisms are available, the most employed being hydraulic, pneumatic, EM, and intelligent devices, operating according to their mode of energy conversion into motion, such as piezoelectric, magnetostrictive, electroactive polymer, shape memory alloy, and photomechanical tools. They offer various specific features and requests associated to the precision, force, speed, environment, etc. Consequently, these robotic interventions would utilize the best actuation fitting the expected procedure regarding the movement resolution, positioning precision, response rapidity, rigidity, actuating force, arrangement complexity, EMI endurance, size, etc.
Based on the abovementioned actuation features, piezoelectric actuation appears to be an ideal candidate for robotic interventions [59]. Indeed, piezoelectric technology offers superior nanometer resolution (compared to other smart actuations), rapid responsiveness (compared to hydraulic and pneumatic systems), and immunity to EMI (compared to EM systems), thus outperforming other common and smart techniques. Moreover, given the obvious adoption of MRI-assistance in robotic procedures due to its advantages discussed in the previous section, piezoelectric actuation seems the most compatible in this case [59].
3.1. Positioning Actuated Robotic and Self-Moving Miniature Robotic Procedures
Robotic procedures actuated by piezoelectric materials, conditional to the expected medical request, are of two types: robotic structures actuated by integrated piezoelectric stuffs permitting self-movement and robotic junctions actuated by piezoelectric deformation converted into movement permitting the displacement of a robotic tool. Actually, the first type relates to traveling wave (TW) thin beams or plates, in general operated in miniaturized shape in requests engaging accurate and restricted shifts of slight, loads on a superficial or internal tissue [24,60,61,62] or fluids in conduits such as micro-pumps [63,64]. These micro robots are usually exploited in precision procedures that necessitate repeatability, dependability, superior movement range and soft shift, which suit assistive procedures. The second type uses repetition and/or stepping permitting higher strokes and degrees of freedom (DOF) [65], counting actuators as stepping [66,67] and ultrasonic [68], which are specifically appropriate for medical surgical interventions.
3.2. MRI-Assistance in Robotic Procedures
As previously stated, the proper functioning of MRI scanners requires an environment that is immune to EMI. This immunity includes protection from external EMFs and the prohibition of the presence of EMF-sensitive objects in or near the scaffold. Failure to follow these precautions can lead to serious disturbances and alter the image [2,7]. Therefore, the integrated robotic structures or robotic actuated junctions contained in the scaffold, respectively integrated or close to body tissues, must be MRI-compatible, i.e., free from materials sensitive to EMFs, such as magnetic or massive conductors. Most robotic devices, containing interventional instruments and structures, can be manufactured with MRI-compatible components. Regarding actuation materials, few types of high-performance actuators exhibit such compatibility. Among these, as previously mentioned, piezoelectric actuators such as ultrasonic motors stand out in several respects, especially in terms of responsiveness and EMI immunity [44,45,59].
The MRI-compatibility of an introduced object when required, can be verified by an EM compatibility (EMC) assessment [23]. Generally, such immunity happens when the distribution of the EMF in the MRI scaffold involving the object would be the same with and without such object [2].
In summary, a reliable medical intervention involving image-assisted robotics (integrated or junctional) would use an MRI scanner and a piezoelectric robotic actuation technique. Figure 2 schematically summarizes such a strategy.
Moreover, it should be noted that EMI immunity including protection from external EMFs and the prohibition of the presence of EMF-sensitive objects inside a device is concerned as well in wearable sensing and assistive tools (see Section 5) as well as implanted self-movement micro robots (see Section 3.1.).
4. Monitoring of MRI-Assisted Robotic Procedures
The precision involved in controlling the image-assisted robotic autonomous intervention discussed in Section 2.2. (Figure 1) would be shaped by various beating issues covering the degree of complexity of the constituents interacting in the procedure, their associated uncertainty characters, unexpected external threat events, as well as other system parameters related to intrinsic issues such as MRI-compatibility or external issues such as personalized patient characteristics. Only by monitoring these potentially distressing difficulties could consistent execution be accomplished.
4.1. Digital Twin Supervision of MRI-Assisted Robotic Control
Reducing the abovementioned threats, in addition to taking into account specific individualized data, are necessary for the successful functioning of an MRI-guided controlled operation. These objectives can be attained by administering the associated parameters in a matching real-virtual pair through a digital twin (DT) [69]. A DT comprises a real physical component, a virtual representation of this component, and a near-real-time bidirectional data flow between these two components. Thus, a DT is conceived as an integration of data in an experiment and its digital replica, thus forming a pair of bidirectional routines. This organization is realized in the management of the complexity of the controlled procedures [70] and planned as a real-virtual pair allowing self-adjusting actions. Thus, the real side allocates the processed identified data to the virtual side, while the latter transmits control orders to the former. These adaptation aids, together with complexity supervision (see Section 6.5.), reduce uncertainties within the pair and unexpected threats in the disruptive dynamics of robotic control.
Recently DT concept has been gradually introduced in healthcare, nursing and prolonged management of health disorders; see e.g., reviews enlightening therapies, monitoring, and managements [71,72,73,74,75,76]. A complete DT monitoring of the control of interventional MRI-assisted robotic via interactions among its real-virtual pair sides, implicates the distribution of sensed processed information by the real side, which is matched and adjusted by, outer data sources as Internet of Things “IoT” besides learnt data from the operational history. The outcome, after a data analysis training, is transmitted, accompanied by a fit model reduction, to the virtual side of the DT. Actually, a swift matching between the two DT parts commands a relatively realistic model but with little computation time. Therefore, the comprehensive coupled model, which truly symbolizes the physical combined procedure, would be condensed, allowing shorter completing time but preserving the picture of the physical procedure (see Section 6.5.).
DT monitoring is generally operated in individualized therapies, which can be illness treatment or interventions. It can be utilized for medical staff training, predicts via physical phantoms together with their virtual replicas, or a real patient–virtual model, involving autonomous matching added to staff supervision. Such staff involvement accompanying with robotics allows an innovative MRI-assisted interventional monitoring, thus lessening the patient peril and ensuring a staff reliable end [77,78,79].
4.2. Digital Environment Augmented Tools
DT exercise is part of smart digital environment and can be often connected to artificial intelligence (AI), augmented reality (AR) and virtual reality (VR) tools. Actually, AI performs in medical treatments strengthen moderate data acquisition and post-processing intricacies and achieving recurrent planned training tasks [10,80]. Regarding robotic control, an important progress has been performed in the modeling and control of robots through artificial neural networks (ANNs) over the last decades, however there are still numerous new defies to be managed [81]. These are related to robot fabrication and materials as well as mathematical concerns mostly related to complex computational hardware. An efficient solution for such complexity in the case of image-guided robotic control can be the implication of AI models [11]. Moreover, the intervention can be profoundly improved via extensive staff–robot connects, advancing the whole arrangement through AR-sustained robotic actions. Therefore, AR combined to an MRI can reduce complex interventional menaces, for example tissue damage, blood loss, and pain post-operation. Furthermore, DTs can perform an important duty in AR-aided robotically intervention. Thus, the possible sickness source and its therapy action can be correctly identified through individual patient inspection via deep learning databases. Similarly, an amount of additional benefits of merged AR-DT are allied to superior suturing accuracy, joining, and reconditioning compared to manual duties [82,83,84,85,86]. Moreover, DTs are often linked, besides AI and AR tools, with VR one, for example, VR tuition progresses the expertise to repeat daily training situations with the capacity to appropriately determine enactment. Likewise, the preparation of DTs allows staff to identify the maladies progress and regulate therapy approaches, selecting the greatest suitable treatment. Such preparation in individualized planning assists development prompt diagnosis and explore new therapies or interventions [8,9]. Figure 3 shows the features of a monitoring DT of an MRI-guided robotic intervention including model reduction, EMC analysis and digital augmented AI, AR and VR tools.
5. Wearable Detecting and Assistive Medical Devices
Wearable therapeutic devices are healthcare body adjacent or integrated, commonly relate to portable, detachable, or embedded tools. They can execute submissive or targeted functions contracted in body tissues. Such duties are associated to sensor detection or assistive deeds. These sensing and assistive tasks might be individual or interacted and self-sufficient or distantly piloted and execute incessantly in real-time. Plus jobs of observation, prediction, upkeep, stimulation, etc., of wearable devices, these permit the management of post-treatment circumstances behind former disorders. Thus, circumventing transfers, transpositions, relocations, etc., substituting face-to-face therapy with a merged linked supervise approach.
5.1. Sensing in Healthcare Wearable Tools
Sensing tasks can use portable pressure sensors or integrated biosensors (or antennas) both working, respectively in non- or minimally-invasive manner, in real-time and continuous supervision of basic health data. Thus allowing medical staff to bring together dependable and accurate knowledge. These sensing tools offer the benefit of authorizing patients to complete their daily achievements while remaining monitored. In such context, wearable sensing tools supported by smart materials and digital environment permit quick, precise health identifications and constant tailored therapeutics [3].
In the case of portable sensing through pressure monitoring, different parameters can be assessed such as heart rate, wrist pulse, as well as joint and muscle actions. As in the case of actuation (see Section 3) piezoelectric materials own as well in sensors great sensitivity, and high linear response, rendering them flawless for different extensive pressure-detecting requirements. For example, in precise wrist pulse indication acquirement [87], evaluation of Parkinson’s tremble [88], and force sensing in robot-assisted MI surgeries [89,90]. Sensing doings comprise revealing [91,92,93], diagnostic [94,95], monitoring [96,97,98], and handling [99,100], duties implicated in diagnosis, maintenance, health supervising and prediction, heart rate nursing, breathing observing, control of blood pressure, tailored pain medicine, etc.
Detection devices using implanted antennas or biosensors operate actively, for example as wireless radiofrequency pressure transducers, for real-time detection or monitoring. They can be used, for example, for in-stent restenosis detection, blood glucose and oxygenation monitoring, heart rate assessment, rapid disease diagnosis, and drug treatment monitoring, etc. [101,102,103,104,105]. An illustrative example of implanted antenna design is presented in [106] within the context of a radiative radio frequency (RF) wireless system for autonomous biomedical implants. The antenna design features are illustrated in Figure 4, Figure 5, Figure 6 and Figure 7, successively relating to its size, structure, adaptation to surrounding tissues, and a measurement scenario. Figure 4 compares the size of the antenna to that of a one-cent euro coin. The substrate is made of Rogers RO3210 material, a ceramic-filled laminate reinforced with woven glass cloth (temporarily heat-resistant), designed for high-frequency applications. A 17 µm thick copper layer covers the RO3210. The feed point is 0.3 mm in diameter. The antenna parameter size is very small (slot width: 0.15 mm).
Figure 5 shows the top and bottom views of the antenna where both sides are electrically connected through a vertical interconnect access (via) near the edge.
Since the antenna is intended to be integrated into an environmental tissue, to avoid any direct contact it must be covered with a superstrate that is the same size as the substrate but without metal. The two parts are glued, the thickness of the glue is 0.3 mm and its dielectric constant is 3.5. The adapted antenna with glue is shown schematically in Figure 6 where the glue is added between the radiating patch and the superstrate.
An experimental setup is used for measurements, utilizing a cylindrical phantom of a biological environment (animal tissues). This phantom must not have a thick outer layer that could generate reflections. Therefore, a plastic cup of negligible thickness is used, with the antenna implanted at a depth of 10 mm. Figure 7 schematically illustrates the measurement setup, the cup containing ground pork, and the integrated antenna.
5.2. Assistive Wearable Devices
Assistive devices include several functional categories including, tissues integrated tools for health repairs and different body elements stimulation, tissues enfolding for image-assisted procedures, and assisting tools for body members (superior and inferior limbs) with sensorimotor deficiencies. These assistive procedures are generally MI and robotically actuated directly [24,60,61,62,63,64] for the first category and indirectly (joint actuators) [65,66,67,68] for the two others.
Assistive occupations in these categories include activation as in a defibrillator and pacemaker [107], drug delivery as in implanted delivery devices [108], supervision as in a spinal cord implant [109], and support, e.g., of cardiac devices for constant blood flow [110], and e.g., MRI-guided robotic medical interventions [2,111], and for the assistance of upper and lower limbs with sensorimotor impairments [4,5,6].
5.3. Multifunctional Activities and Flexible Wearable Instruments
Smart materials operate according to their mode of energy conversion into motion as mentioned in Section 3. They present different specific characteristics and requirements linked to the precision, force, speed, environment, etc. Consequently, wearable tools would utilize the best deed fitting their expected functioning. As illustrated in Section 3, piezoelectric materials exhibit an excellent electromechanical two-way conversion matched to other smart materials. Consequently, they are largely used in actuation, sensing or combined [112]. In wearable tools, associated with actuation and sensing, piezoelectric flexible material (PFM) devices suitable for large deformations [113], allow the harvesting of energy produced by the movement activity of the humans involved. Such amalgamated tasks in the same device characterizes a multifunctional tool leading to more condensed result. In this case the combined sensing and harvesting via mechanical to electrical conversion results in a self-driven sensor.
The abovementioned flexibility relates to PFM as well as its support pieces and electrode substances, so offering a consistent multifunctional flexible piezoelectric device. In wearable tools, energy harvesting can contain different motion phenomena as respiration, pulse, gastric deformation, etc. [114,115,116,117,118,119].
There are different types of PFM, mainly organic polymers [120,121], thin films of inorganic crystalline materials [122,123] and composites of crystal-polymer adjustable mixture [124,125]. The polymers structures match mobility management, while thin-film or composite PFMs match superior actuation and energy harvesting requests.
5.4. Wearable EMC Digital Control
As mentioned in Section 3.2, immunity to EMI includes protection from external EMF and the exclusion of the presence of EMF-sensitive matters in or near the target device. Actually, EMI can perturb the target own field as in the case of MRI scanner or the target functioning due to the presence of EMF-sensitive in its interior. These disturbances may affect individuals with wearable skin sensors and embedded sensing or assistive devices [126], for example, those with active implantable medical devices [127,128]. The corresponding immunity can be verified by experimental EMC analysis [128] or digital assessment [23], (see Section 6.2.).
6. Discussion
In the analyses presented in the previous sections, a number of themes deserve further discussion.
6.1. Effects of Exposure to EMF
The daily use of artificial EM devices contributes beneficially to the well-being of society in general. However, these devices emit EMFs through their usual function or through the side effects of stray radiation. Exposure to these EMFs can produce various undesirable effects on surrounding objects. Indeed, the interaction of an EMF with an object induces fields inside the latter, which depend on the intensity and frequency of exposure, as well as the intrinsic physical and geometric characteristics of the exposed object.
Objects affected by such exposures include human tissues, their medical wearable tools, other close therapeutic devices and generally other nearby objects such as animals, plants, electronic devices, etc. Thus, the disturbing fields induced by the exposure can affect, directly the human tissues and indirectly the wearable observation and assistance devices involved as well as interventional implicated devices [22].
6.1.1. Biological Effects of EMF Exposure
Regarding living tissues, exposure-induced fields produce biological effects (BEs) characterized by the specific absorption rate (SAR) power density, exposure duration, and frequency level. The latter falls into two distinct ranges: non-ionizing and ionizing. The ionizing ones are used in specific situations and are recognized as hazardous to living tissues; for example, they are used in various medical imaging technologies, but in limited quantities and durations, and are excluded from relatively long imaging-assisted procedures (see Section 2.2). Artificial EM devices in daily use, responsible for EMF exposure, generally operate at non-ionizing frequencies. However, their use with relatively high SARs and durations would produce tissue BEs, which generally reflect thermal effects but could be hazardous in cases of excessive SARs and intervals [22,129].
6.1.2. Medical Devices Immunity to EMI
For wearable and interventional devices, including detection, assistance, and imaging tools, they should reflect the previously mentioned immunity to EMI. This immunity includes protection against external EMF, exclusion of the presence of EMF-sensitive materials inside or near the target wearable or interventional device, and possible shielding protection. In fact, EMF can disrupt the target’s own field, as in the case of an MRI scanner, or the target’s operation due to the presence of EMF-sensitive elements inside, as in the case of wearable devices [22].
6.2. Device Compatibility and EMC Analysis
The degree of immunity to EMI of detection, assistance and imaging devices measures their compatibility with regard to their operational behavior when exposed to EMFs. Reliable compatibility can be ensured by appropriate design or shielding of the target or source devices, depending on their specific operating conditions. For example, it is difficult to shield a wireless communication source or a remote sensing tool, but the design helps reduce stray fields of the source or EMF-sensitive substances in the tool.
The control of such compatibility verifying the sensitivity to EMI can be realized through EMC analysis based on, experimental approaches using particular test workbench capable to create regulated and adjustable fields, or numerical approaches using 3-D solutions of EMF governing equations accounting for the device features in its background and the exposure source [23,130]. As indicated in Section 4.1 concerning the supervision of TDs, which can operate with physical phantoms and their virtual replicas, these phantoms can also be used for EMC analysis (see Figure 3). Thus, the aforementioned experimental and numerical approaches would respectively use physical and digital phantoms of the tissues of the body part in question.
6.2.1. Example of EMC Analysis Using Experimental Means
Different experimental approaches can be used for EMC analysis depending on the operational conditions of the controlled device and the nature of the exposure [131]. For example, considering the case of active implanted pacemakers [128], a test technique based on an experimental methodology using a bench generating a regulated magnetic field in the 3-D space by means of three Helmholtz coils. A test setup made of non-magnetic material encloses a physical phantom containing the pacemaker immersed in a saline solution that simulates the electromagnetic properties of the human body. This setup permits the control and positioning of the pacemaker as well as the introduction of atrial contraction signal and the monitoring of ventricular stimulation. The test exposures with the adjusted strengths and directions use typical low frequencies (50 Hz to 3 kHz). Figure 8 and Figure 9 show respectively the test bench involving the set of coils, the phantom and power amplifiers, and the test setup controlling and positioning of the pacemaker within the phantom involving atrial contraction signal and monitoring of ventricular stimulation.
This study showed that the magnetic field direction has an impact on the pacemaker’s functioning in bipolar mode. The direction with the highest malfunction rate does not correspond to the direction considered as the reference for EMC testing by international standards and literature. Such reference direction corresponds to a magnetic field perpendicular to the plane formed by the pacemaker and its leads, a situation where a unipolar pacemaker senses the maximum of magnetic flux. The induced voltage cannot be derived easily from the evaluation of a flux through an inductive surface. These observations led to the hypothesis that the leads in bipolar mode are more sensitive to electric field than magnetic field. This assumption remains to be confirmed by further studies.
6.2.2. Digital EMC Analysis in Medical Devices
A digital EMC assessment is established on mathematical equations characterizing the conduct of EMFs. This control may involve field disturbances related to the introduction of a potentially EMF-sensitive substance into a medical device, for example, the scaffold of an MRI scanner (see Section 3), or related to the external EMF exposure of a device containing a potentially EMF-sensitive component, for example, a wearable device (see Section 5). In these cases, the field disturbances involved would be lower for materials with lesser EMF sensitivity and non-existent for materials that are not EMF-sensitive. The role of numerical EMF assessment is to ensure the control of the integrity of healthcare tools by calculating the 3-D local distribution of EMFs in the devices concerned.
The EMF equations used in EMC analysis are generally originated of Maxwell theory [132] and can be set in diverse forms depending on the involved request [23]. The solution of these equations permit the computations of local induced fields, accounting for matters behavior via the magnetic permeability, electrical conductivity and permittivity respectively for magnetic, conductor and dielectric phenomena. The local field solution is accomplished in general through numerical discretized methodologies considering the 3-D topology, material behavior and the source conditions.
The nature of the assessment relates to the object being tested. In the case of body tissue, the induced fields can be verified by comparing them to standard health thresholds [133,134,135]. In the case of devices incorporating external substances, such as MRI scaffolds, the integrity of the MRI’s own field will be verified [23]. The constancy of the field distribution will be verified in the presence of EMF-sensitive components in portable tools, as well as the effectiveness of possible shielding.
We will consider two applications of such assessments. The first concerns a demonstration of EMC digital analysis related to MRI-compatibility of external substances introduced in the scanner scaffold [23]. In this case the integrity of the MRI RF field, which is directly related to the image, will be checked through the constancy of the field while the absence and existence of external inserted matter. The second is related to EMF exposure emitted by a wireless charging device on human tissues [22]. In such situation, the body induced fields relative to the exposure will be checked against threshold values fixed by health standards mentioned above. The 3-D field computations in both applications were carried out using the finite element method (FEM) with edge tetrahedral elements.
Relating to the first example, Figure 10 shows a demonstrative comparison of the 3-D RF field distribution in the cross-section of a birdcage-shaped tubular structure integrated into an MRI scaffold, for situations involving the introduction of external bodies: compatible and incompatible with MRI. The corresponding field distributions are given for a structure without material (a), with a solid conductive aluminum cube (b), and with a piezoelectric cube (c). Detailed characteristics of the scanner and materials are available in reference [23].
As shown in the above figure, the dielectric piezoelectric cube displays no effect on the RF field distribution as anticipated MRI-compatible, while the aluminum one modifies such distribution. The three field distributions in the figure correspond to the same input states; they thus advocate behavioral suggestion and shed light on MRI EMC analysis for the assessment of disturbances in image-guided practices.
In the second example related to EMF exposure emitted by a wireless charging device on human tissues [22], the distributions of 3-D fields induced in human body will be computed and checked against threshold values. Such computations are generally achieved in numerical virtual body models (phantoms), which match properly with the used local field computations through numerical discretized methodologies mentioned above. Considerable investigation has been done into constructing human bodies’ models reflecting accurate and high-resolution tissue representation, see e.g., [136,137]. Figure 11 shows a demonstrative illustration of an exposure of EMFs from a wireless battery charging device of an electric vehicle (EV) to a human body located horizontally on the ground near the EV [22]. The figure shows the distributions of the magnetic induction B and electric field E induced in the body due to EMF exposure related to stay fields of the wireless charging device (3 kW at 30 kHz) [138,139]. The computed values of B and E fields in this case were checked with the above-mentioned thresholds of safety standards (corresponding since 2010 to 27 μT for B and 83 V/m for E), which were in conformity with these security rules.
6.3. Smart Protection of Medical Devices
As mentioned in the previous section, reliable immunity to EMI can be ensured by appropriate design or shielding of devices. The design strategy mainly consists of reducing, where possible, the stray fields of the emitting source and constructing the target device with materials insensitive to EMF exposures, such as piezoelectric materials. Otherwise, the target device, when operating near EM environments, must be protected by appropriate shielding.
Simple and economical shielding can be achieved by placing a thin layer of conductive material around the device. In this case, the exposed EMF induces currents in the conductive layer that are a function of the source’s intensity, frequency, direction, and the conductivity of the shielding material. The skin effect of the induced currents in the conductive layer of the shield produces a shielding effect, preventing the fields from penetrating into the device. At the same time, these induced currents could cause a temperature rise due to their dissipated energy in the conductive layer. This temperature rise depends on the characteristics and duration of exposure, as well as the physical properties of the layer. In the case of a wearable device, such heating of the shield can impair the operation of the device and cause heating of body tissues by conduction, in addition to possible thermal BEs due to exposure to EMF. This problem can be overcome by modifying the conductive nature of the shielding using smart shielding materials.
Such adaptation can be achieved by using multifunctional fitted constituents for low-reflectivity shielding, thus reducing the great EM reflection triggered by the material elevated conductivity. Moreover, a particular fabricating procedure allowing the reduction of the material reflected power coefficient can be also used, see e.g., [140,141,142,143,144].
The effectiveness of the shielding can be verified by an EMC analysis based on EMF equations combined with heat transfer equations (in the material) or bio-heat (in body tissues) depending on the situation [145].
6.4. Digital Augmented Tools and Personalized Committed Assignments
The use of DT, AI, AR, VR, etc. digital augmented tools, in addition to medical treatments supervision, enables other various differentiated tasks like procedure planning, staff training, treatment investigation, general tutoring, etc.
DT monitored medical procedures require planning to adjust and authenticate the involved medical actions, which would be reached using physical phantoms and their digital copies in the DT tool. Such pre-assignments consist of intervention and patient individual information [146], compliant adapting of procedure involved matters, as scanner parameters and compatibility [147], robotic actuation and management, etc. Moreover, such personalized planning allows staff to judge choices and be conscious of possible errors of assessment [148,149].
Different medical involvements practicing digital augmented tools could be found in the literature, as cognitive control e.g., [150], surgical training e.g., [151], medical education and learning e.g., [152,153], developments in surgery [154], rehabilitation e.g., [155,156], and ethics frameworks related to the use of digital tools e.g., [157].
6.5. DT Interventional Complexity Management and Reduction of Complete Models
In the preceding analysis, the DT management of the inherent complexity of system-controlled medical interventions was addressed in Section 4.1. This complexity arises from the interaction of interdependent phenomena involved in the various components of the procedure, illustrated in Figure 1. Among these components is the body part targeted by the intervention. The body involved living tissues play a significant role in this complexity (see Section 6.6.1.). An example of such complexity is ocular components tissues, where ocular fluid dynamics and heat transfer phenomena are essential for eye function. Consequently, the virtual part of the DT would include a coupled model of the corresponding equations [158]. Thus, a biophysical model, with its boundary and interface conditions, would be integrated into the global virtual replicas of the DT. Section 4.1 also discussed the reduction of the coupled mathematical representation of these interdependent phenomena. Indeed, the speed of execution imposed by DT matching precludes the use of a fully coupled model. A sensitivity analysis must therefore be carried out on the complete model factors followed by a reduction strategy to moderate the computation time while preserving the physical representation of the procedure and retaining the aspects necessary for a correct physical description.
6.6. Future Perspectives
Future projections fall into two categories relating to the objectives of the work and the means of achieving them. The first two points concern the development of these means, while the last two relate to the expansion of the objectives.
6.6.1. Living Tissues Dynamic Mechanical Representation
Throughout this article, the physical and mathematical representations of living tissues, corresponding respectively to physical and virtual phantoms, have been studied using approximate static behavioral features capable of accurately representing many realistic situations. In reality, living tissues are composed of soft materials irrigated by fluids that enable them to function. This structure reflects dynamic mechanical displacements and distortions that are not exactly represented by the static behavior of living tissues mentioned above. In studies involving intrinsic mechanical features such as blood circulation, function alteration, or tissue injury [159], the static representation of the tissue would be ineffective, and a dynamic mechanical analysis (DMA) becomes necessary [160]. DMA is a major practice in biomechanics used to represent the viscoelastic properties of matter, thereby creating real-time, person-specific, and multi-scale possible phantoms. Research on these mechanical representations appears important and corresponds to the multiphysics coupling of tissues with other phenomena involved in medical treatments.
6.6.2. Compatibility of Smart Materials and Digital Tools
This article focuses on a smart digital environment integrating smart materials and intelligent digital monitoring. The innovations involved, both in smart devices and augmented digital tools, require careful attention to tissue-device compatibility and personalized digital patient safety.
Regarding tissue-device questions, generally in tasks performed close or inside tissues non-toxicity and biocompatibility are compulsory and specific situations biodegradability is also necessary. In consequence, biosecurity and nonappearance of immune rejection are guaranteed. Thus, increased therapeutics suggest the investigation of compatible materials in medical involvements [161].
Concerning the use of smart digital tools in general, which reflects an immersive societal equipment introduces ethical issues [157]. In healthcare field, the concerned patient safety involves different questions related to the use of digital technology as data transfer [162]. Moreover, in addition to patient concerns, other societal alarms merit attention as digital tools energy consumption and all activities reducing human capacity for reflection and deliberation. These topics put forward as well more exploration.
6.6.3. Smart Digital Wearable Technologies and Swing from Therapy to Preclusion
The forthcoming evolution of healthcare is presumed to be marked by an increasing elderly population, a swing from a curative to a preventive approach, greater use of digital health tools and telemedicine, and a progressive focus on disease prevention and more proactive patient care [163].
The actual study focuses specifically on intelligent digital environments integrated with wearable therapeutic technologies. It should be noted that wearable technological devices with AI capabilities have the potential to become game changers for digital health with great importance in remote patient care. These technologies contribute to improved patient outcomes, optimized healthcare delivery by enabling continuous monitoring, personalized interventions, and data driven decision-making. The significant evolution of these technologies, from treatment to prevention, appears to coincide with the aging population. This trend justifies further research to confirm the effectiveness and safety of digital health and telemedicine tools in preventive care. This enables remote monitoring and tailored care, fostering a more patient-centered approach and more systematic use of data for prevention; the result is more accessible, faster, and less expensive care.
6.6.4. Smart Digital Monitoring of Medical Robotics Beyond Interventions
In the present study DT monitoring of image-assisted robotic surgery and drug delivery interventions are investigated. The use of smart digital tools in general (DT, AI, and/or xR) for monitoring of robotized procedures generally (computer or image assisted) can be extended to medical utilities beyond interventions. These medical uses include personnel training [151], student education [152] and research explorations [164,165,166]. Research may focus on the robotic procedure itself (control strategy, robotic routines, new materials, imaging, and actuation resources). It may also encompass new therapies, pharmaceutical innovation, telemedicine, intraoperative assistance, postoperative outcomes, and more.
6.6.5. Future Perspectives Integrated in the Contribution Background
Figure 12 summarizes the objectives of this contribution, the means of achieving them and the place of future projections in such context.
7. Conclusions
The analyses and investigations conducted in this contribution have highlighted the potential for reliable, accurate, and dependable observation and intervention therapies through the integration of a smart digital environment. The medical implications explored include image-assisted interventions in robotic surgery and drug delivery, as well as monitoring and assistance approaches using wearable devices.
The analysis corroborates that technological advances in smart material, wearable sensing, robotic actuation, and imaging, combined with intelligent digital monitoring, are shaping smart digital management. The latter is integrated into autonomous systems, reflecting valuable interaction between machines and personnel. This improves medical functionality, patient well-being, and staff convenience.
Diverse future research perspectives in, smart digital environments for medical interventions and wearable therapeutic strategies, propose more research on the following topics (for details, see Section 6.6.):
- Living tissues dynamic mechanical physical and digital representations
- Compatibility of smart materials and digital tools
- Smart digital wearable technologies and swing from therapy to preclusion
- Smart digital monitoring of medical robotics beyond interventions
As a final remark, the analysis presented in this article concerning intelligent digital tools focuses on medical therapies and obviously does not travel over all uses that have a negative impact on ecology, biodiversity, global security and human capacities for reflection and discernment.
Author Contributions
A.R. and L.P. have contributed equally to all items. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hernigou, P.; Hosny, G.A.; Scarlat, M. Evolution of orthopaedic diseases through four thousand three hundred years: From ancient Egypt with virtual examinations of mummies to the twenty-first century. Int. Orthop. 2023, 48, 865–884. [Google Scholar] [CrossRef]
- Razek, A. Image-Guided Surgical and Pharmacotherapeutic Routines as Part of Diligent Medical Treatment. Appl. Sci. 2023, 13, 13039. [Google Scholar] [CrossRef]
- Chen, S.; Fan, S.; Qiao, Z.; Wu, Z.; Lin, B.; Li, Z.; Riegler, M.A.; Wong, M.Y.H.; Opheim, A.; Korostynska, O.; et al. Transforming Healthcare: Intelligent Wearable Sensors Empowered by Smart Materials and Artificial Intelligence. Adv. Mater. 2025, 37, e2500412. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Hernandez, U.; Metcalfe, B.; Assaf, T.; Jabban, L.; Male, J.; Zhang, D. Wearable Assistive Robotics: A Perspective on Current Challenges and Future Trends. Sensors 2021, 21, 6751. [Google Scholar] [CrossRef]
- Li, Y.; Luo, S.; Luo, R.; Liu, H. A novel real-time assistive hip-wearable exoskeleton robot based on motion prediction for lower extremity rehabilitation in subacute stroke: A single-blinded, randomized controlled trial. BMC Neurol. 2025, 25, 1–12. [Google Scholar] [CrossRef]
- Winterbottom, L.; Chen, A.; Mendonca, R.; Nilsen, D.M.; Ciocarlie, M.; Stein, J. Clinician perceptions of a novel wearable robotic hand orthosis for post-stroke hemiparesis. Disabil. Rehabilitation 2024, 47, 1577–1586. [Google Scholar] [CrossRef]
- Razek, A. From Open, Laparoscopic, or Computerized Surgical Interventions to the Prospects of Image-Guided Involvement. Appl. Sci. 2025, 15, 4826. [Google Scholar] [CrossRef]
- Kukushkin, K.; Ryabov, Y.; Borovkov, A. Digital Twins: A Systematic Literature Review Based on Data Analysis and Topic Modeling. Data 2022, 7, 173. [Google Scholar] [CrossRef]
- Giansanti, D.; Morelli, S. Exploring the Potential of Digital Twins in Cancer Treatment: A Narrative Review of Reviews. J. Clin. Med. 2025, 14, 3574. [Google Scholar] [CrossRef]
- Cusumano, D.; Boldrini, L.; Dhont, J.; Fiorino, C.; Green, O.; Güngör, G.; Jornet, N.; Klüter, S.; Landry, G.; Mattiucci, G.C.; et al. Artificial Intelligence in magnetic Resonance guided Radiotherapy: Medical and physical considerations on state of art and future perspectives. Phys. Medica 2021, 85, 175–191. [Google Scholar] [CrossRef]
- Boeken, T.; Lim, H.-P.D.; Cohen, E.I. The Role and Future of Artificial Intelligence in Robotic Image-Guided Interventions. Tech. Vasc. Interv. Radiol. 2024, 27, 101001. [Google Scholar] [CrossRef] [PubMed]
- Han, F.; Huang, X.; Wang, X.; Chen, Y.; Lu, C.; Li, S.; Lu, L.; Zhang, D. Artificial Intelligence in Orthopedic Surgery: Current Applications, Challenges, and Future Directions. Medcomm 2025, 6, e70260. [Google Scholar] [CrossRef] [PubMed]
- Oyama, S.; Iwase, H.; Yoneda, H.; Yokota, H.; Hirata, H.; Yamamoto, M. Insights and trends review: Use of extended reality (xR) in hand surgery. J. Hand Surg. 2025, 50, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Angrisani, L.; D’arco, M.; De Benedetto, E.; Duraccio, L.; Regio, F.L.; Sansone, M.; Tedesco, A. Performance Measurement of Gesture-Based Human–Machine Interfaces Within eXtended Reality Head-Mounted Displays. Sensors 2025, 25, 2831. [Google Scholar] [CrossRef]
- Guerra-Armas, J.; Roldán-Ruiz, A.; Flores-Cortes, M.; Harvie, D.S. Harnessing Extended Reality for Neurocognitive Training in Chronic Pain: State of the Art, Opportunities, and Future Directions. Healthcare 2025, 13, 1338. [Google Scholar] [CrossRef]
- Ganeson, K.; May, C.T.X.; Abdullah, A.A.A.; Ramakrishna, S.; Vigneswari, S. Advantages and Prospective Implications of Smart Materials in Tissue Engineering: Piezoelectric, Shape Memory, and Hydrogels. Pharmaceutics 2023, 15, 2356. [Google Scholar] [CrossRef]
- Bocchetta, G.; Fiori, G.; Sciuto, S.A.; Scorza, A. Performance of Smart Materials-Based Instrumentation for Force Measurements in Biomedical Applications: A Methodological Review. Actuators 2023, 12, 261. [Google Scholar] [CrossRef]
- Giansanti, D. The Future of Healthcare Is Digital: Unlocking the Potential of Mobile Health and E-Health Solutions. Healthcare 2025, 13, 802. [Google Scholar] [CrossRef]
- Wang, R.C.; Wang, Z. Precision Medicine: Disease Subtyping and Tailored Treatment. Cancers 2023, 15, 3837. [Google Scholar] [CrossRef]
- Allen, B. The Promise of Explainable AI in Digital Health for Precision Medicine: A Systematic Review. J. Pers. Med. 2024, 14, 277. [Google Scholar] [CrossRef]
- Special Issue: Healthcare Goes Digital: Mobile Health and Electronic Health Technology in the 21st Century. Available online: https://www.mdpi.com/journal/healthcare/special_issues/0P14J89UOQ (accessed on 10 October 2025).
- Razek, A. Biological and Medical Disturbances Due to Exposure to Fields Emitted by Electromagnetic Energy Devices—A Review. Energies 2022, 15, 4455. [Google Scholar] [CrossRef]
- Razek, A. Assessment of a Functional Electromagnetic Compatibility Analysis of Near-Body Medical Devices Subject to Electromagnetic Field Perturbation. Electronics 2023, 12, 4780. [Google Scholar] [CrossRef]
- Hariri, H. Design and Realization of a Piezoelectric Mobile for Cooperative Use. PhD Thesis, University of Paris XI, Paris, France, 2012. (In English). Available online: https://theses.hal.science/tel-01124059v1/file/2012PA112321.
- Tetteh, E.; Wang, T.; Kim, J.Y.; Smith, T.; Norasi, H.; Van Straaten, M.G.; Lal, G.; Chrouser, K.L.; Shao, J.M.; Hallbeck, M.S. Optimizing ergonomics during open, laparoscopic, and robotic-assisted surgery: A review of surgical ergonomics literature and development of educational illustrations. Am. J. Surg. 2023, 235, 115551. [Google Scholar] [CrossRef] [PubMed]
- Alkatout, I.; Mechler, U.; Mettler, L.; Pape, J.; Maass, N.; Biebl, M.; Gitas, G.; Laganà, A.S.; Freytag, D. The Development of Laparoscopy—A Historical Overview. Front. Surg. 2021, 8, 799442. [Google Scholar] [CrossRef]
- Barrios, E.L.; Polcz, V.E.; Hensley, S.E.; Sarosi, G.A.; Mohr, A.M.; Loftus, T.J.; Upchurch, G.R.; Sumfest, J.M.; Efron, P.A.; Dunleavy, K.; et al. A narrative review of ergonomic problems, principles, and potential solutions in surgical operations. Surgery 2023, 174, 214–221. [Google Scholar] [CrossRef]
- Bittner, R. Laparoscopic Surgery—15 Years After Clinical Introduction. World J. Surg. 2006, 30, 1190–1203. [Google Scholar] [CrossRef]
- Bracale, U.; Corcione, F.; Pignata, G.; Andreuccetti, J.; Dolce, P.; Boni, L.; Cassinotti, E.; Olmi, S.; Uccelli, M.; Gualtierotti, M.; et al. Impact of neoadjuvant therapy followed by laparoscopic radical gastrectomy with D2 lymph node dissection in Western population: A multi-institutional propensity score-matched study. J. Surg. Oncol. 2021, 124, 1338–1346. [Google Scholar] [CrossRef]
- Bizzarri, N.; Anchora, L.P.; Teodorico, E.; Certelli, C.; Galati, G.; Carbone, V.; Gallotta, V.; Naldini, A.; Costantini, B.; Querleu, D.; et al. The role of diagnostic laparoscopy in locally advanced cervical cancer staging. Eur. J. Surg. Oncol. (EJSO) 2024, 50, 108645. [Google Scholar] [CrossRef]
- Pérez-Salazar, M.J.; Caballero, D.; Sánchez-Margallo, J.A.; Sánchez-Margallo, F.M. Comparative Study of Ergonomics in Conventional and Robotic-Assisted Laparoscopic Surgery. Sensors 2024, 24, 3840. [Google Scholar] [CrossRef]
- Li, S.-Y.; Ji, L.-Q.; Li, S.-H.; Jiang, W.-D.; Zhang, C.-M.; Zhang, W.; Lou, Z. Laparoscopic surgery is associated with increased risk of postoperative peritoneal metastases in T4 colon cancer: A propensity score analysis. Int. J. Color. Dis. 2025, 40, 1–11. [Google Scholar] [CrossRef]
- Taghavi, K.; Glenisson, M.; Loiselet, K.; Fiorenza, V.; Cornet, M.; Capito, C.; Vinit, N.; Pire, A.; Sarnacki, S.; Blanc, T. Robot-assisted laparoscopic adrenalectomy: Extended application in children. Eur. J. Surg. Oncol. (EJSO) 2024, 50, 108627. [Google Scholar] [CrossRef] [PubMed]
- Williamson, T.; Song, S.-E. Robotic Surgery Techniques to Improve Traditional Laparoscopy. JSLS J. Soc. Laparosc. Robot. Surg. 2022, 26. [Google Scholar] [CrossRef]
- Rivero-Moreno, Y.; Echevarria, S.; Vidal-Valderrama, C.; Stefano-Pianetti, L.; Cordova-Guilarte, J.; Navarro-Gonzalez, J.; Acevedo-Rodríguez, J.; Dorado-Avila, G.; Osorio-Romero, L.; Chavez-Campos, C.; et al. Robotic Surgery: A Comprehensive Review of the Literature and Current Trends. Cureus 2023, 15, e42370. [Google Scholar] [CrossRef]
- Lima, V.L.; de Almeida, R.C.; Neto, T.R.; Rosa, A.A.M. Chapter 72—Robotic ophthalmologic surgery. In Handbook of Robotic Surgery; Academic Press: Cambridge, MA, USA, 2025; pp. 701–704. [Google Scholar] [CrossRef]
- Rivero-Moreno, Y.; Rodriguez, M.; Losada-Muñoz, P.; Redden, S.; Lopez-Lezama, S.; Vidal-Gallardo, A.; Machado-Paled, D.; Guilarte, J.C.; Teran-Quintero, S. Autonomous Robotic Surgery: Has the Future Arrived? Cureus 2024, 16, e52243. [Google Scholar] [CrossRef]
- Han, J.; Davids, J.; Ashrafian, H.; Darzi, A.; Elson, D.S.; Sodergren, M. A systematic review of robotic surgery: From supervised paradigms to fully autonomous robotic approaches. Int. J. Med Robot. Comput. Assist. Surg. 2021, 18, e2358. [Google Scholar] [CrossRef]
- Lee, A.; Baker, T.S.; Bederson, J.B.; Rapoport, B.I. Levels of autonomy in FDA-cleared surgical robots: A systematic review. npj Digit. Med. 2024, 7, 1–8. [Google Scholar] [CrossRef]
- Wan, Q.; Shi, Y.; Xiao, X.; Li, X.; Mo, H. Review of Human–Robot Collaboration in Robotic Surgery. Adv. Intell. Syst. 2024, 7. [Google Scholar] [CrossRef]
- Liu, T.; Wang, J.; Wong, S.; Razjigaev, A.; Beier, S.; Peng, S.; Do, T.N.; Song, S.; Chu, D.; Wang, C.H.; et al. A Review on the Form and Complexity of Human–Robot Interaction in the Evolution of Autonomous Surgery. Adv. Intell. Syst. 2024, 6. [Google Scholar] [CrossRef]
- Schreiter, J.; Schott, D.; Schwenderling, L.; Hansen, C.; Heinrich, F.; Joeres, F. AR-Supported Supervision of Conditional Autonomous Robots: Considerations for Pedicle Screw Placement in the Future. J. Imaging 2022, 8, 255. [Google Scholar] [CrossRef] [PubMed]
- Dagnino, G.; Kundrat, D. Robot-assistive minimally invasive surgery: Trends and future directions. Int. J. Intell. Robot. Appl. 2024, 8, 812–826. [Google Scholar] [CrossRef]
- Chinzei, K.; Hata, N.; Jolesz, F.; Kikinis, R. Surgical assist robot for the active navigation in the intraoperative MRI: Hardware design issues. In Proceedings of the 2000 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS 2000) (Cat. No.00CH37113), Takamatsu, Japan, 31 October–5 November 2000; pp. 727–732. [Google Scholar] [CrossRef]
- Tsekos, N.V.; Khanicheh, A.; Christoforou, E.; Mavroidis, C. Magnetic Resonance–Compatible Robotic and Mechatronics Systems for Image-Guided Interventions and Rehabilitation: A Review Study. Annu. Rev. Biomed. Eng. 2007, 9, 351–387. [Google Scholar] [CrossRef] [PubMed]
- Faoro, G.; Maglio, S.; Pane, S.; Iacovacci, V.; Menciassi, A. An Artificial Intelligence-Aided Robotic Platform for Ultrasound-Guided Transcarotid Revascularization. IEEE Robot. Autom. Lett. 2023, 8, 2349–2356. [Google Scholar] [CrossRef]
- Su, H.; Kwok, K.-W.; Cleary, K.; Iordachita, I.; Cavusoglu, M.C.; Desai, J.P.; Fischer, G.S. State of the Art and Future Opportunities in MRI-Guided Robot-Assisted Surgery and Interventions. Proc. IEEE 2022, 110, 968–992. [Google Scholar] [CrossRef]
- Padhan, J.; Tsekos, N.; Al-Ansari, A.; Abinahed, J.; Deng, Z.; Navkar, N.V. Dynamic Guidance Virtual Fixtures for Guiding Robotic Interventions: Intraoperative MRI-guided Transapical Cardiac Intervention Paradigm. In Proceedings of the 2022 IEEE 22nd International Conference on Bioinformatics and Bioengineering (BIBE), Taichung, Taiwan, 7–9 November 2022; pp. 265–270. [Google Scholar] [CrossRef]
- Singh, S.; Torrealdea, F.; Bandula, S. MR Imaging-Guided Intervention: Evaluation of MR Conditional Biopsy and Ablation Needle Tip Artifacts at 3T Using a Balanced Fast Field Echo Sequence. J. Vasc. Interv. Radiol. 2021, 32, 1068–1074.e1. [Google Scholar] [CrossRef]
- Xu, L.; Pacia, C.P.; Gong, Y.; Hu, Z.; Chien, C.-Y.; Yang, L.; Gach, H.M.; Hao, Y.; Comron, H.; Huang, J.; et al. Characterization of the Targeting Accuracy of a Neuronavigation-Guided Transcranial FUS System In Vitro, In Vivo, and In Silico. IEEE Trans. Biomed. Eng. 2022, 70, 1528–1538. [Google Scholar] [CrossRef]
- Navarro-Becerra, J.A.; Borden, M.A. Targeted Microbubbles for Drug, Gene, and Cell Delivery in Therapy and Immunotherapy. Pharmaceutics 2023, 15, 1625. [Google Scholar] [CrossRef]
- Delaney, L.J.; Isguven, S.; Eisenbrey, J.R.; Hickok, N.J.; Forsberg, F. Making waves: How ultrasound-targeted drug delivery is changing pharmaceutical approaches. Mater. Adv. 2022, 3, 3023–3040. [Google Scholar] [CrossRef]
- Jia, X.; Zhang, Y.; DU, H.; Yu, Y. Experimental study of double cable-conduit driving device for mri compatible biopsy robots. J. Mech. Med. Biol. 2021, 21. [Google Scholar] [CrossRef]
- Li, X.; Young, A.S.; Raman, S.S.; Lu, D.S.; Lee, Y.-H.; Tsao, T.-C.; Wu, H.H. Automatic needle tracking using Mask R-CNN for MRI-guided percutaneous interventions. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 1673–1684. [Google Scholar] [CrossRef]
- Bernardes, M.C.; Moreira, P.; Lezcano, D.; Foley, L.; Tuncali, K.; Tempany, C.; Kim, J.S.; Hata, N.; Iordachita, I.; Tokuda, J. In Vivo Feasibility Study: Evaluating Autonomous Data-Driven Robotic Needle Trajectory Correction in MRI-Guided Transperineal Procedures. IEEE Robot. Autom. Lett. 2024, 9, 8975–8982. [Google Scholar] [CrossRef]
- Wu, D.; Li, G.; Patel, N.; Yan, J.; Kim, G.H.; Monfaredi, R.; Cleary, K.; Iordachita, I. Remotely Actuated Needle Driving Device for MRI-Guided Percutaneous Interventions: Force and Accuracy Evaluation. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 1985–1989. [Google Scholar]
- Lane, S.A.; Slater, J.M.; Yang, G.Y. Image-Guided Proton Therapy: A Comprehensive Review. Cancers 2023, 15, 2555. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Shin, N.Y.; Lee, S.J.; Cho, Y.J.; Jung, I.H.; Sung, J.W.; Kim, S.J.; Kim, J.W. Development of Magnetic Resonance-Compatible Head Immobilization Device and Initial Experience of Magnetic Resonance-Guided Radiation Therapy for Central Nervous System Tumors. Pr. Radiat. Oncol. 2024, 14, e324–e333. [Google Scholar] [CrossRef] [PubMed]
- Razek, A.; Bernard, Y. Potential of Piezoelectric Actuation and Sensing in High Reliability Precision Mechanisms and Their Applications in Medical Therapeutics. Actuators 2025, 14, 528. [Google Scholar] [CrossRef]
- Ding, Z.; Cui, M.; Wu, J.; Wei, W.; Rong, X.; Li, Y. Development of an Untethered Self-Moving Piezoelectric Actuator With Load-Carriable, Fast, and Precise Movement Driven by Piezoelectric Stack Plates. IEEE Trans. Ind. Electron. 2025, 72, 11635–11646. [Google Scholar] [CrossRef]
- Hariri, H.; Bernard, Y.; Razek, A. 2-D Traveling Wave Driven Piezoelectric Plate Robot for Planar Motion. IEEE/ASME Trans. Mechatronics 2018, 23, 242–251. [Google Scholar] [CrossRef]
- Hariri, H.; Bernard, Y.; Razek, A. A traveling wave piezoelectric beam robot. Smart Mater. Struct. 2013, 23, 025013. [Google Scholar] [CrossRef]
- Yang, Z.; Dong, L.; Wang, M.; Liu, G.; Li, X.; Li, Y. A wearable insulin delivery system based on a piezoelectric micropump. Sensors Actuators A: Phys. 2022, 347. [Google Scholar] [CrossRef]
- Hernandez, C.; Bernard, Y.; Razek, A. Design and manufacturing of a piezoelectric traveling-wave pumping device. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2013, 60, 1949–1956. [Google Scholar] [CrossRef]
- Spanner, K.; Koc, B. Piezoelectric Motors, an Overview. Actuators 2016, 5, 6. [Google Scholar] [CrossRef]
- Ghenna, S.; Bernard, Y.; Daniel, L. Design and experimental analysis of a high force piezoelectric linear motor. Mechatronics 2022, 89. [Google Scholar] [CrossRef]
- Wang, S.; Rong, W.; Wang, L.; Xie, H.; Sun, L.; Mills, J.K. A survey of piezoelectric actuators with long working stroke in recent years: Classifications, principles, connections and distinctions. Mech. Syst. Signal Process. 2019, 123, 591–605. [Google Scholar] [CrossRef]
- Tian, X.; Liu, Y.; Deng, J.; Wang, L.; Chen, W. A review on piezoelectric ultrasonic motors for the past decade: Classification, operating principle, performance, and future work perspectives. Sensors Actuators A: Phys. 2020, 306. [Google Scholar] [CrossRef]
- Tao, F.; Sui, F.; Liu, A.; Qi, Q.; Zhang, M.; Song, B.; Guo, Z.; Lu, S.C.-Y.; Nee, A.Y.C. Digital twin-driven product design framework. Int. J. Prod. Res. 2019, 57, 3935–3953. [Google Scholar] [CrossRef]
- Grieves, M.; Vickers, J. Digital Twin: Mitigating Unpredictable, Undesirable Emergent Behavior in Complex Systems. In Transdisciplinary Perspectives on Complex Systems; Springer: Cham, Switzerland, 2017; pp. 85–113. [Google Scholar] [CrossRef]
- Sun, T.; He, X.; Li, Z. Digital twin in healthcare: Recent updates and challenges. Digit. Heal. 2023, 9. [Google Scholar] [CrossRef] [PubMed]
- De Benedictis, A.; Mazzocca, N.; Somma, A.; Strigaro, C. Digital Twins in Healthcare: An Architectural Proposal and Its Application in a Social Distancing Case Study. IEEE J. Biomed. Heal. Informatics 2022, 27, 5143–5154. [Google Scholar] [CrossRef] [PubMed]
- Haleem, A.; Javaid, M.; Singh, R.P.; Suman, R. Exploring the revolution in healthcare systems through the applications of digital twin technology. Biomed. Technol. 2023, 4, 28–38. [Google Scholar] [CrossRef]
- Mohamed, N.; Al-Jaroodi, J.; Jawhar, I.; Kesserwan, N. Leveraging Digital Twins for Healthcare Systems Engineering. IEEE Access 2023, 11, 69841–69853. [Google Scholar] [CrossRef]
- Ricci, A.; Croatti, A.; Montagna, S. Pervasive and Connected Digital Twins—A Vision for Digital Health. IEEE Internet Comput. 2021, 26, 26–32. [Google Scholar] [CrossRef]
- Wickramasinghe, N.; Ulapane, N.; Sloane, E.B.; Gehlot, V. Digital Twins for More Precise and Personalized Treatment. Stud. Health Technol. Inform. 2024, 310, 229–233. [Google Scholar] [CrossRef]
- Song, Y. Human Digital Twin, the Development and Impact on Design. J. Comput. Inf. Sci. Eng. 2023, 23, 1–28. [Google Scholar] [CrossRef]
- Burattini, S.; Montagna, S.; Croatti, A.; Gentili, N.; Ricci, A.; Leonardi, L.; Pandolfini, S.; Tosi, S. An Ecosystem of Digital Twins for Operating Room Management. In Proceedings of the 2023 IEEE 36th International Symposium on Computer-Based Medical Systems (CBMS), L’Aquila, Italy, 22–24 June 2023; pp. 770–775. [Google Scholar] [CrossRef]
- Hagmann, K.; Hellings-Kuß, A.; Klodmann, J.; Richter, R.; Stulp, F.; Leidner, D. A Digital Twin Approach for Contextual Assistance for Surgeons During Surgical Robotics Training. Front. Robot. AI 2021, 8. [Google Scholar] [CrossRef]
- Katsoulakis, E.; Wang, Q.; Wu, H.; Shahriyari, L.; Fletcher, R.; Liu, J.; Achenie, L.; Liu, H.; Jackson, P.; Xiao, Y.; et al. Digital twins for health: A scoping review. npj Digit. Med. 2024, 7, 1–11. [Google Scholar] [CrossRef]
- Liu, Z.; Peng, K.; Han, L.; Guan, S. Modeling and Control of Robotic Manipulators Based on Artificial Neural Networks: A Review. Iran. J. Sci. Technol. Trans. Mech. Eng. 2023, 47, 1307–1347. [Google Scholar] [CrossRef]
- Seetohul, J.; Shafiee, M.; Sirlantzis, K. Augmented Reality (AR) for Surgical Robotic and Autonomous Systems: State of the Art, Challenges, and Solutions. Sensors 2023, 23, 6202. [Google Scholar] [CrossRef]
- Avrumova, F.; Lebl, D.R. Augmented reality for minimally invasive spinal surgery. Front. Surg. 2023, 9, 1086988. [Google Scholar] [CrossRef]
- Long, Y.; Cao, J.; Deguet, A.; Taylor, R.H.; Dou, Q. Integrating Artificial Intelligence and Augmented Reality in Robotic Surgery: An Initial dVRK Study Using a Surgical Education Scenario. In Proceedings of the 2022 International Symposium on Medical Robotics (ISMR), Atlanta, GA, USA; 2022; pp. 1–8. [Google Scholar]
- Fu, J.; Rota, A.; Li, S.; Zhao, J.; Liu, Q.; Iovene, E.; Ferrigno, G.; De Momi, E. Recent Advancements in Augmented Reality for Robotic Applications: A Survey. Actuators 2023, 12, 323. [Google Scholar] [CrossRef]
- Qian, L.; Wu, J.Y.; DiMaio, S.P.; Navab, N.; Kazanzides, P. A Review of Augmented Reality in Robotic-Assisted Surgery. IEEE Trans. Med Robot. Bionics 2019, 2, 1–16. [Google Scholar] [CrossRef]
- Gao, T.; Qiu, X.; Xu, P.; Hu, Z.; Yan, J.; Xiang, Y.; Xuan, F.-Z. Piezoelectret-based dual-mode flexible pressure sensor for accurate wrist pulse signal acquisition in health monitoring. Measurement 2024, 242. [Google Scholar] [CrossRef]
- Xie, Q.; Han, L.; Liu, J.; Zhang, W.; Zhao, L.; Liu, Y.; Chen, Y.; Li, Y.; Zhou, Q.; Dong, Y.; et al. Kirigami-Inspired Stretchable Piezoelectret Sensor for Analysis and Assessment of Parkinson’s Tremor. Adv. Heal. Mater. 2024, 14, e2402010. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Zhang, H.; Zhang, Z.; Hu, C.; Shi, C. Development of Force Sensing Techniques for Robot-Assisted Laparoscopic Surgery: A Review. IEEE Trans. Med Robot. Bionics 2024, 6, 868–887. [Google Scholar] [CrossRef]
- Wang, W.; Wang, J.; Luo, Y.; Wang, X.; Song, H. A Survey on Force Sensing Techniques in Robot-Assisted Minimally Invasive Surgery. IEEE Trans. Haptics 2023, 16, 702–718. [Google Scholar] [CrossRef]
- Liu, E.; Cai, Z.; Ye, Y.; Zhou, M.; Liao, H.; Yi, Y. An Overview of Flexible Sensors: Development, Application, and Challenges. Sensors 2023, 23. [Google Scholar] [CrossRef] [PubMed]
- Devi, D.H.; Duraisamy, K.; Armghan, A.; Alsharari, M.; Aliqab, K.; Sorathiya, V.; Das, S.; Rashid, N. 5G Technology in Healthcare and Wearable Devices: A Review. Sensors 2023, 23, 2519. [Google Scholar] [CrossRef]
- Mukhopadhyay, S.C.; Suryadevara, N.K.; Nag, A. Wearable Sensors for Healthcare: Fabrication to Application. Sensors 2022, 22, 5137. [Google Scholar] [CrossRef]
- Chakrabarti, S.; Biswas, N.; Jones, L.D.; Kesari, S.; Ashili, S. Smart Consumer Wearables as Digital Diagnostic Tools: A Review. Diagnostics 2022, 12, 2110. [Google Scholar] [CrossRef]
- Escobar-Linero, E.; Muñoz-Saavedra, L.; Luna-Perejón, F.; Sevillano, J.L.; Domínguez-Morales, M. Wearable Health Devices for Diagnosis Support: Evolution and Future Tendencies. Sensors 2023, 23, 1678. [Google Scholar] [CrossRef]
- Pantelopoulos, A.; Bourbakis, N.G. A Survey on Wearable Sensor-Based Systems for Health Monitoring and Prognosis. IEEE Trans. Syst. Man Cybern. Part C Appl. Rev. 2010, 40, 1–12. [Google Scholar] [CrossRef]
- Ahmed, R.; Newby, S.; Potluri, P.; Mirihanage, W.; Fernando, A. Emerging Paradigms in Fetal Heart Rate Monitoring: Evaluating the Efficacy and Application of Innovative Textile-Based Wearables. Sensors 2024, 24, 6066. [Google Scholar] [CrossRef]
- Moon, K.S.; Lee, S.Q. A Wearable Multimodal Wireless Sensing System for Respiratory Monitoring and Analysis. Sensors 2023, 23, 6790. [Google Scholar] [CrossRef]
- Mamun, M.M.R.K.; Sherif, A. Advancement in the Cuffless and Noninvasive Measurement of Blood Pressure: A Review of the Literature and Open Challenges. Bioengineering 2022, 10, 27. [Google Scholar] [CrossRef]
- Xing, Y.; Yang, K.; Lu, A.; Mackie, K.; Guo, F. Sensors and Devices Guided by Artificial Intelligence for Personalized Pain Medicine. Think. Ski. Creativity 2024, 5, 0160. [Google Scholar] [CrossRef]
- Ding, S.; Pichon, L.; Chen, Y. A Low-Cost Microwave Stentenna for In-Stent Restenosis Detection. IEEE Trans. Antennas Propag. 2025, 73, 8681–8692. [Google Scholar] [CrossRef]
- Mohan, A.; Kumar, N. Implantable antennas for biomedical applications: A systematic review. Biomed. Eng. Online 2024, 23, 1–29. [Google Scholar] [CrossRef]
- Aliqab, K.; Nadeem, I.; Khan, S.R. A Comprehensive Review of In-Body Biomedical Antennas: Design, Challenges and Applications. Micromachines 2023, 14, 1472. [Google Scholar] [CrossRef]
- Alyami, A.M.; Kirimi, M.T.; Neale, S.L.; Mercer, J.R. Implantable Biosensors for Vascular Diseases: Directions for the Next Generation of Active Diagnostic and Therapeutic Medical Device Technologies. Biosensors 2025, 15, 147. [Google Scholar] [CrossRef]
- Kudłacik-Kramarczyk, S.; Kieres, W.; Przybyłowicz, A.; Ziejewska, C.; Marczyk, J.; Krzan, M. Recent Advances in Micro- and Nano-Enhanced Intravascular Biosensors for Real-Time Monitoring, Early Disease Diagnosis, and Drug Therapy Monitoring. Sensors 2025, 25, 4855. [Google Scholar] [CrossRef]
- Ding, S. Design of a Power-Efficient Radiative Wireless System for Autonomous Biomedical Implants. PhD Thesis, Bioengineering, Université Paris-Saclay, Paris, France, 2021. (In English). [Google Scholar]
- Bhuva, A.N.; Moralee, R.; Brunker, T.; Lascelles, K.; Cash, L.; Patel, K.P.; Lowe, M.; Sekhri, N.; Alpendurada, F.; Pennell, D.J.; et al. Evidence to support magnetic resonance conditional labelling of all pacemaker and defibrillator leads in patients with cardiac implantable electronic devices. Eur. Hear. J. 2021, 43, 2469–2478. [Google Scholar] [CrossRef]
- Joo, H.; Lee, Y.; Kim, J.; Yoo, J.-S.; Yoo, S.; Kim, S.; Arya, A.K.; Kim, S.; Choi, S.H.; Lu, N.; et al. Soft implantable drug delivery device integrated wirelessly with wearable devices to treat fatal seizures. Sci. Adv. 2021, 7, eabd4639. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Xie, D.; Han, Y.; Guo, S.; Sun, Z.; Jing, L.; Man, W.; Liu, D.; Yang, K.; Lei, D.; et al. Precise management system for chronic intractable pain patients implanted with spinal cord stimulation based on a remote programming platform: Study protocol for a randomized controlled trial (PreMaSy study). Trials 2023, 24, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J.S.; Maynes, E.J.; O’mAlley, T.J.; Pavri, B.B.; Tchantchaleishvili, V. Electromagnetic interference between implantable cardiac devices and continuous-flow left ventricular assist devices: A review. J. Interv. Card. Electrophysiol. 2021, 61, 1–10. [Google Scholar] [CrossRef]
- Liu, D.; Li, G.; Wang, S.; Liu, Z.; Wang, Y.; Connolly, L.; Usevitch, D.E.; Shen, G.; Cleary, K.; Iordachita, I. A magnetic resonance conditional robot for lumbar spinal injection: Development and preliminary validation. Int. J. Med Robot. Comput. Assist. Surg. 2023, 20, e2618. [Google Scholar] [CrossRef]
- Du, P.; Chen, W.; Deng, J.; Liu, Y. Sensing–Actuating Integrated Ultrasonic Device for High-Precision and High-Efficiency Burnishing. IEEE Trans. Ind. Electron. 2024, 72, 5199–5209. [Google Scholar] [CrossRef]
- Chen, B.; Feng, Z.; Yao, F.-Z.; Zhang, M.-H.; Wang, K.; Wei, Y.; Gong, W.; Rödel, J. Flexible piezoelectrics: Integration of sensing, actuating and energy harvesting. npj Flex. Electron. 2025, 9, 1–26. [Google Scholar] [CrossRef]
- Dagdeviren, C.; Yang, B.D.; Su, Y.; Tran, P.L.; Joe, P.; Anderson, E.; Xia, J.; Doraiswamy, V.; Dehdashti, B.; Feng, X.; et al. Conformal piezoelectric energy harvesting and storage from motions of the heart, lung, and diaphragm. Proc. Natl. Acad. Sci. 2014, 111, 1927–1932. [Google Scholar] [CrossRef] [PubMed]
- Hwang, G.-T.; Byun, M.; Jeong, C.K.; Lee, K.J. Flexible Piezoelectric Thin-Film Energy Harvesters and Nanosensors for Biomedical Applications. Adv. Healthc. Mater. 2015, 4, 646–658. [Google Scholar] [CrossRef]
- Raj, N.P.M.J.; Alluri, N.R.; Vivekananthan, V.; Chandrasekhar, A.; Khandelwal, G.; Kim, S.-J. Sustainable yarn type-piezoelectric energy harvester as an eco-friendly, cost-effective battery-free breath sensor. Appl. Energy 2018, 228, 1767–1776. [Google Scholar] [CrossRef]
- He, Q.; Briscoe, J. Piezoelectric Energy Harvester Technologies: Synthesis, Mechanisms, and Multifunctional Applications. ACS Appl. Mater. Interfaces 2024, 16, 29491–29520. [Google Scholar] [CrossRef]
- Kang, S.; Kim, S.H.; Lee, H.B.; Mhin, S.; Ryu, J.H.; Kim, Y.W.; Jones, J.L.; Son, Y.; Lee, N.K.; Lee, K.; et al. High-power energy harvesting and imperceptible pulse sensing through peapod-inspired hierarchically designed piezoelectric nanofibers. Nano Energy 2022, 99. [Google Scholar] [CrossRef]
- Dagdeviren, C.; Javid, F.; Joe, P.; von Erlach, T.; Bensel, T.; Wei, Z.; Saxton, S.; Cleveland, C.; Booth, L.; McDonnell, S.; et al. Flexible piezoelectric devices for gastrointestinal motility sensing. Nat. Biomed. Eng. 2017, 1, 807–817. [Google Scholar] [CrossRef]
- Murayama, N.; Nakamura, K.; Obara, H.; Segawa, M. The strong piezoelectricity in polyvinylidene fluroide (PVDF). Ultrasonics 1976, 14, 15–24. [Google Scholar] [CrossRef]
- Mohammadpourfazeli, S.; Arash, S.; Ansari, A.; Yang, S.; Mallick, K.; Bagherzadeh, R. Future prospects and recent developments of polyvinylidene fluoride (PVDF) piezoelectric polymer; fabrication methods, structure, and electro-mechanical properties. RSC Adv. 2023, 13, 370–387. [Google Scholar] [CrossRef]
- Kum, H.S.; Lee, H.; Kim, S.; Lindemann, S.; Kong, W.; Qiao, K.; Chen, P.; Irwin, J.; Lee, J.H.; Xie, S.; et al. Heterogeneous integration of single-crystalline complex-oxide membranes. Nature 2020, 578, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Ren, Z.; Deng, S.; Shao, J.; Si, Y.; Zhou, C.; Luo, J.; Wang, T.; Li, J.; Li, J.; Liu, H.; et al. Ultrahigh-power-density flexible piezoelectric energy harvester based on freestanding ferroelectric oxide thin films. Nat. Commun. 2025, 16, 1–11. [Google Scholar] [CrossRef]
- Verma, K.; Kumar, A.; Sharma, R. Development of flexible piezoelectric nanogenerator based on PVDF/KNN/ZnO nanocomposite film for energy harvesting application. J. Mater. Sci. Mater. Electron. 2024, 35, 1–17. [Google Scholar] [CrossRef]
- Sasmal, A.; Patra, A.; Maiti, P.; Sahu, B.; Krahne, R.; Arockiarajan, A. Microstructuring of conductivity tuned piezoelectric polydimethylsiloxane/(Ba0.85Ca0.15)(Ti0.90Hf0.10)O3 composite for hybrid mechanical energy harvesting. Polym. Compos. 2025, 46, 11387–11402. [Google Scholar] [CrossRef]
- Kranold, L.; Xi, J.; Goren, T.; Kuster, N. Dosimetric Electromagnetic Safety of People With Implants: A Neglected Population? Bioelectromagnetics 2025, 46, e70023. [Google Scholar] [CrossRef]
- Hammen, L.; Pichon, L.; Le Bihan, Y.; Bensetti, M.; Fleury, G. Testing immunity of active implantable medical devices to industrial magnetic field environments. In .Proceedings of the International Symposium and Exhibition on Electromagnetic Compatibility—EMC Europe, Göteborg, Sweden, 5–8 September 2022; Available online: https://hal.science/hal-03779559/document.
- Hammen, L. Electromagnetic compatibility of active implantable medical devices at the workplace: The case of pacemakers. PhD Thesis, Université Paris-Saclay, Paris, France, 2024. [Google Scholar]
- Laganà, F.; Bibbò, L.; Calcagno, S.; De Carlo, D.; Pullano, S.A.; Pratticò, D.; Angiulli, G. Smart Electronic Device-Based Monitoring of SAR and Temperature Variations in Indoor Human Tissue Interaction. Appl. Sci. 2025, 15, 2439. [Google Scholar] [CrossRef]
- De Leo, A. Special Issue on Advanced Technologies in Electromagnetic Compatibility. Appl. Sci. 2022, 12, 8975. [Google Scholar] [CrossRef]
- Cai, S.; Li, Y.; Zhu, H.; Wu, X.; Su, D. A Novel Electromagnetic Compatibility Evaluation Method for Receivers Working under Pulsed Signal Interference Environment. Appl. Sci. 2021, 11, 9454. [Google Scholar] [CrossRef]
- Maxwell, J.C. VIII. A dynamical theory of the electromagnetic field. Philos. Trans. R. Soc. Lond. 1865, 155, 459–512. [Google Scholar] [CrossRef]
- International Commission on Non-Ionizing Radiation Protection. Guide-lines for limiting exposure to time-varying electric and magnetic fields for low frequencies (1 Hz–100 kHz). Health Phys. 2010, 99, 818–836. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Non-Ionizing Radiation Protection. Guidelines for limiting exposure to electromagnetic fields (100 kHz to 300 GHz). Health Phys. 2020, 118, 483–524. [Google Scholar]
- IEEE Standard C95.1-2019; IEEE Standard for Safety Levels With Respect to Human Exposure to Electric, Magnetic, and Electromagnetic Fields, 0 Hz to 300 GHz. IEEE Standards Association: Piscataway, NJ, USA, 2019. [CrossRef]
- Makarov, S.N.; Noetscher, G.M.; Yanamadala, J.; Piazza, M.W.; Louie, S.; Prokop, A.; Nazarian, A.; Nummenmaa, A. Virtual Human Models for Electromagnetic Studies and Their Applications. IEEE Rev. Biomed. Eng. 2017, 10, 95–121. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Gao, N.; Wu, B.; Chen, Z.; Xu, X.G. A Review of Computational Phantoms for Quality Assurance in Radiology and Radiotherapy in the Deep-Learning Era. J. Radiat. Prot. Res. 2022, 47, 111–133. [Google Scholar] [CrossRef]
- Ibrahim, M. Wireless Inductive Charging for Electrical Vehicles: Electromagnetic Modelling and Interoperability Analysis. PhD Thesis, University of Paris-Sud, Orsay, France, 2014. Available online: https://theses.hal.science/tel-01127163/file/2014PA112369.
- Ding, P.-P.; Bernard, L.; Pichon, L.; Razek, A. Evaluation of Electromagnetic Fields in Human Body Exposed to Wireless Inductive Charging System. IEEE Trans. Magn. 2014, 50, 1037–1040. [Google Scholar] [CrossRef]
- Ma, Z.; Deng, Z.; Zhou, X.; Li, L.; Jiao, C.; Ma, H.; Yu, Z.-Z.; Zhang, H.-B. Multifunctional and magnetic MXene composite aerogels for electromagnetic interference shielding with low reflectivity. Carbon 2023, 213. [Google Scholar] [CrossRef]
- Jang, J.M.; Kim, J.H.; Lee, J.; Hong, J.; Kim, D.W.; Kim, S.J. Gradient-structured MXene/ZIF/CNT hybrid films for largely enhanced electromagnetic absorption in EMI shielding. Chem. Eng. J. 2024, 503. [Google Scholar] [CrossRef]
- Yun, J.; Zhou, C.; Guo, B.; Wang, F.; Zhou, Y.; Ma, Z.; Qin, J. Mechanically strong and multifunctional nano-nickel aerogels based epoxy composites for ultra-high electromagnetic interference shielding and thermal management. J. Mater. Res. Technol. 2023, 24, 9644–9656. [Google Scholar] [CrossRef]
- Verma, R.; Thakur, P.; Chauhan, A.; Jasrotia, R.; Thakur, A. A review on MXene and its’ composites for electromagnetic interference (EMI) shielding applications. Carbon 2023, 208, 170–190. [Google Scholar] [CrossRef]
- Song, P.; Cai, Z.; Li, J.; He, M.; Qiu, H.; Ren, F.; Zhang, Y.; Guo, H.; Ren, P. Construction of rGO-MXene@FeNi/epoxy composites with regular honeycomb structures for high-efficiency electromagnetic interference shielding. J. Mater. Sci. Technol. 2024, 217, 311–320. [Google Scholar] [CrossRef]
- Razek, A. Eco-Management of Wireless Electromagnetic Fields Involved in Smart Cities Regarding Healthcare and Mobility. Telecom 2025, 6, 16. [Google Scholar] [CrossRef]
- Vallée, A. Digital twins for cardiovascular diseases: Towards personalised and sustainable care. Acta Cardiol. 2025, 80, 1055–1062. [Google Scholar] [CrossRef]
- Kantor, T.; Mahajan, P.; Murthi, S.; Stegink, C.; Brawn, B.; Varshney, A.; Reddy, R.M. Role of eXtended Reality use in medical imaging interpretation for pre-surgical planning and intraoperative augmentation. J. Med Imaging 2024, 11, 062607. [Google Scholar] [CrossRef] [PubMed]
- Elkefi, S.; Asan, O. Digital Twins for Managing Health Care Systems: Rapid Literature Review. J. Med Internet Res. 2022, 24, e37641. [Google Scholar] [CrossRef] [PubMed]
- Cellina, M.; Cè, M.; Alì, M.; Irmici, G.; Ibba, S.; Caloro, E.; Fazzini, D.; Oliva, G.; Papa, S. Digital Twins: The New Frontier for Personalized Medicine? Appl. Sci. 2023, 13, 7940. [Google Scholar] [CrossRef]
- Song, H.; Oh, Y.; Choi, J.; Ohm, S.-Y. Effectiveness of Virtual Reality–Based Cognitive Control Training Game for Children With Attention-Deficit/Hyperactivity Disorder Symptoms: Preliminary Effectiveness Study. JMIR Pediatr. Parent. 2025, 8, e66617. [Google Scholar] [CrossRef]
- Kayaalp, M.E.; Konstantinou, E.; Karaismailoglu, B.; Lucidi, G.A.; Kaymakoglu, M.; Vieider, R.; Giusto, J.D.; Inoue, J.; Hirschmann, M.T. The metaverse in orthopaedics: Virtual, augmented and mixed reality for advancing surgical training, arthroscopy, arthroplasty and rehabilitation. Knee Surgery, Sports Traumatol. Arthrosc. 2025, 33, 3039–3050. [Google Scholar] [CrossRef]
- Siddiqui, M.F.; Jabeen, S.; Alwazzan, A.; Vacca, S.; Dalal, L.; Al-Haddad, B.; Jaber, A.; Ballout, F.F.; Zeid, H.K.A.; Haydamous, J.; et al. Integration of Augmented Reality, Virtual Reality, and Extended Reality in Healthcare and Medical Education: A Glimpse into the Emerging Horizon in LMICs—A Systematic Review. J. Med Educ. Curric. Dev. 2025, 12. [Google Scholar] [CrossRef]
- Pantusin, F.J.; Ortiz, J.S.; Carvajal, C.P.; Andaluz, V.H.; Yar, L.G.; Roberti, F.; Gandolfo, D. Digital Twin Integration for Active Learning in Robotic Manipulator Control Within Engineering 4.0. Symmetry 2025, 17, 1638. [Google Scholar] [CrossRef]
- Sang, A.Y.; Wang, X.; Paxton, L. Technological Advancements in Augmented, Mixed, and Virtual Reality Technologies for Surgery: A Systematic Review. Cureus 2024, 16, e76428. [Google Scholar] [CrossRef]
- Ai, X.; Agrawal, S.K. Remote Extended Reality With Markerless Motion Tracking for Sitting Posture Training. IEEE Robot. Autom. Lett. 2024, 9, 9860–9867. [Google Scholar] [CrossRef]
- Morimoto, T.; Hirata, H.; Ueno, M.; Fukumori, N.; Sakai, T.; Sugimoto, M.; Kobayashi, T.; Tsukamoto, M.; Yoshihara, T.; Toda, Y.; et al. Digital Transformation Will Change Medical Education and Rehabilitation in Spine Surgery. Medicina 2022, 58, 508. [Google Scholar] [CrossRef]
- Cox, S.; Kadlubsky, A.; Svarverud, E.; Adams, J.; Baraas, R.C.; Bernabe, R.D. A scoping review of the ethics frameworks describing issues related to the use of extended reality. Open Res. Eur. 2025, 4, 74. [Google Scholar] [CrossRef]
- Saigre, T.; Prud’Homme, C.; Szopos, M.; Chabannes, V. A coupled fluid-dynamics-heat transfer model for 3D simulations of the aqueous humor flow in the human eye. arXiv 2024, arXiv:2404.19353. Available online: https://arxiv.org/abs/2404.19353.
- Qiu, Y.; Gao, T.; Smith, B.R. Mechanical deformation and death of circulating tumor cells in the bloodstream. Cancer Metastasis Rev. 2024, 43, 1489–1510. [Google Scholar] [CrossRef]
- Wu, L.; Huang, R.; Zhu, J.; Ma, X. A Dynamic Mechanical Analysis Device for In Vivo Material Characterization of Plantar Soft Tissue. Technologies 2025, 13, 191. [Google Scholar] [CrossRef]
- Vinchurkar, K.; Bukke, S.P.N.; Jain, P.; Bhadoria, J.; Likhariya, M.; Mane, S.; Suryawanshi, M.; Veerabhadrappa, K.V.; Eftekhari, Z.; Onohuean, H. Advances in sustainable biomaterials: Characterizations, and applications in medicine. Discov. Polym. 2025, 2, 1–35. [Google Scholar] [CrossRef]
- Oh, C.; Kim, Y.-M.; Lee, T.; Lee, S.-M.; Jung, J.; Bae, H.-M.; Kim, C.; Lee, H.J. Patch-type capacitive micromachined ultrasonic transducer for ultrasonic power and data transfer. Microsystems Nanoeng. 2025, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- De la Torre, K.; Min, S.; Lee, H.; Kang, D. The Application of Preventive Medicine in the Future Digital Health Era. J. Med Internet Res. 2025, 27, e59165. [Google Scholar] [CrossRef] [PubMed]
- Mizna, S.; Arora, S.; Saluja, P.; Das, G.; Alanesi, W.A. An analytic research and review of the literature on practice of artificial intelligence in healthcare. Eur. J. Med Res. 2025, 30, 1–11. [Google Scholar] [CrossRef]
- Gowri, V.; Uma, M.; Sethuramalingam, P. Machine learning enabled robot-assisted virtual health monitoring system design and development. Multiscale Multidiscip. Model. Exp. Des. 2024, 7, 2259–2288. [Google Scholar] [CrossRef]
- Gitto, S.; Giuliani, G.; Lasciarrea, A. A Digital Twin System to Enable Better Healthcare Management. In Hybrid Human-AI Collaborative Networks. PRO-VE 2025. IFIP Advances in Information and Communication Technology; Camarinha-Matos, L.M., Ortiz, A., Boucher, X., Lucas Soares, A., Eds.; Springer: Cham, Swirzerland, 2026; p. 770. [Google Scholar] [CrossRef]
Figure 1.
Schematics of a closed-loop autonomous procedure counting the, scanner, imaged restricted troubled zone including the tool position, image processing, localization and tasks and control of robotic actuation.
Figure 1.
Schematics of a closed-loop autonomous procedure counting the, scanner, imaged restricted troubled zone including the tool position, image processing, localization and tasks and control of robotic actuation.
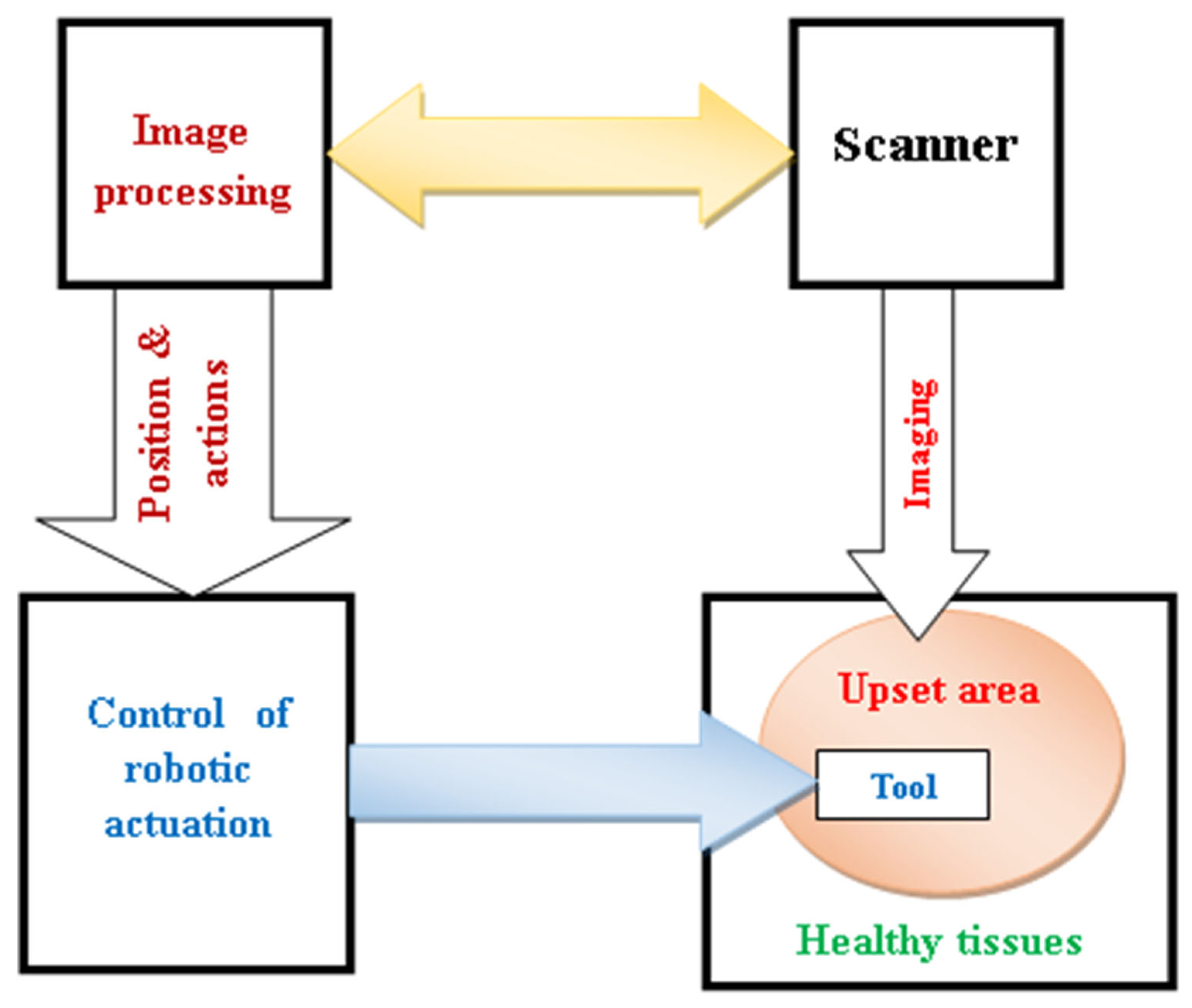
Figure 2.
Schematics of the scanner and robotic actuating means adoption in a reliable image-assisted robotic intervention.
Figure 2.
Schematics of the scanner and robotic actuating means adoption in a reliable image-assisted robotic intervention.
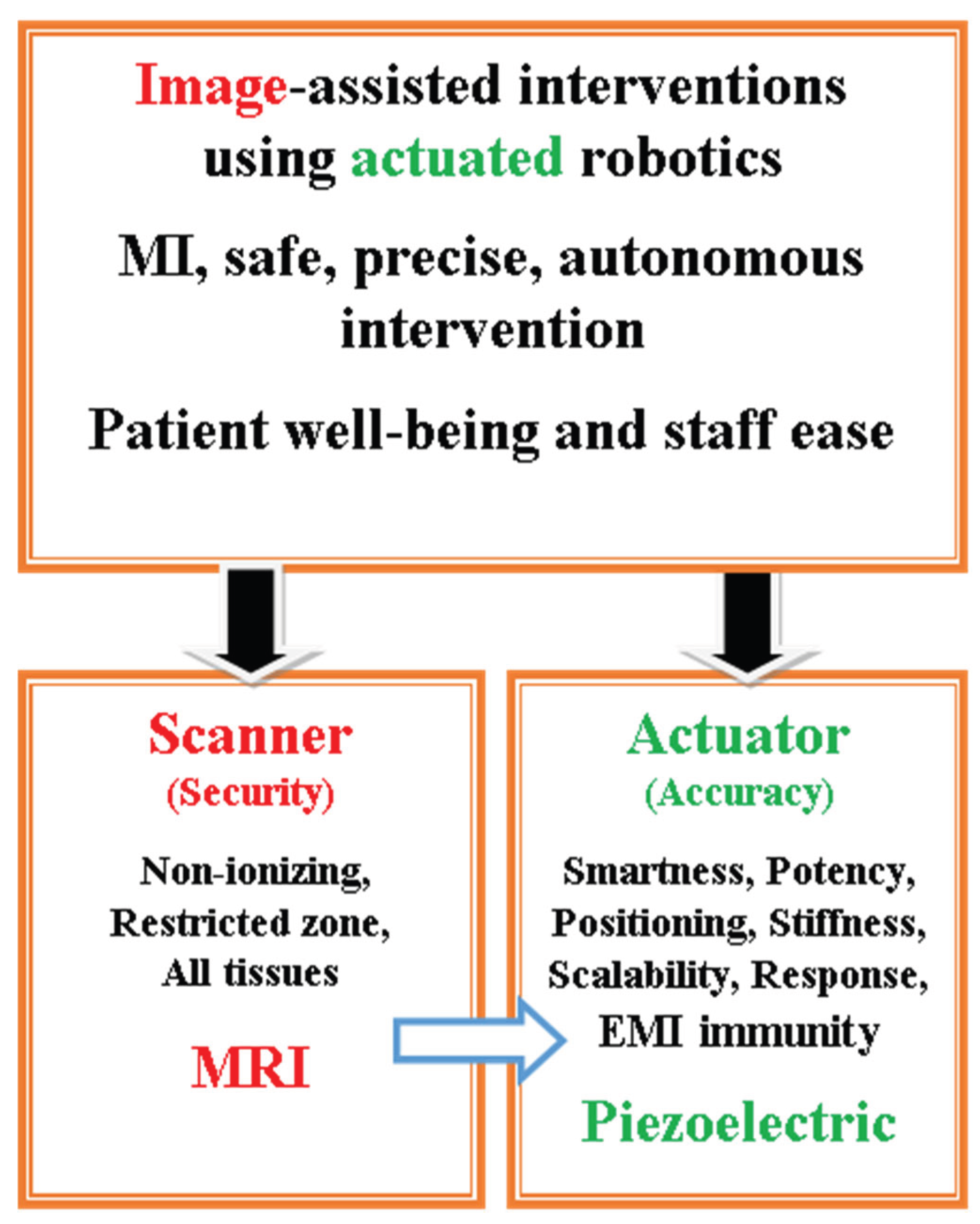
Figure 3.
Summarized schematics of DT monitoring of MRI-assisted robotic intervention with model reduction, EMC analysis digital routine and AI, AR and VR digital tools.
Figure 3.
Summarized schematics of DT monitoring of MRI-assisted robotic intervention with model reduction, EMC analysis digital routine and AI, AR and VR digital tools.
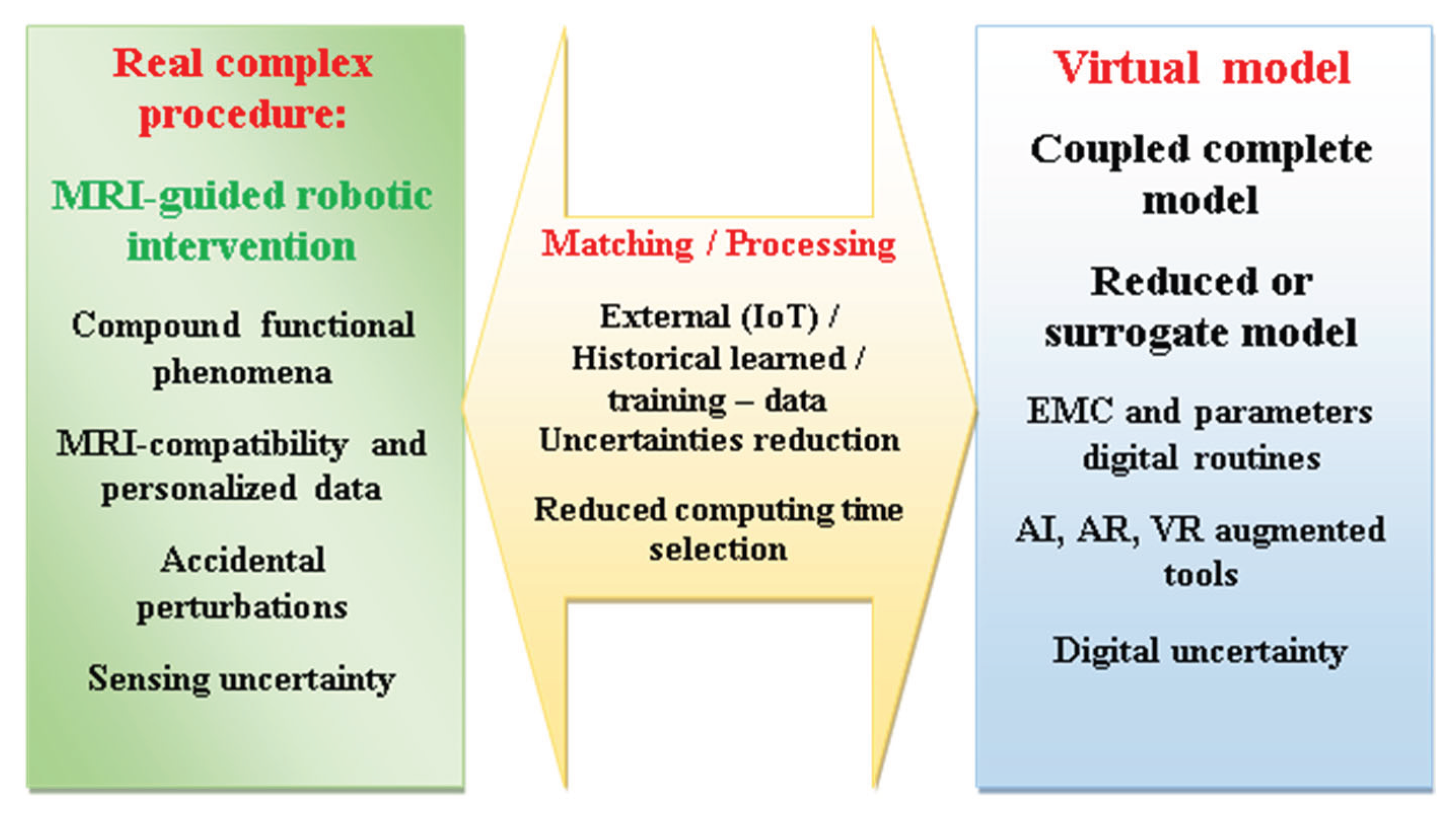
Figure 4.
Mechanically constructed antenna compared to one-euro cent [106].
Figure 4.
Mechanically constructed antenna compared to one-euro cent [106].
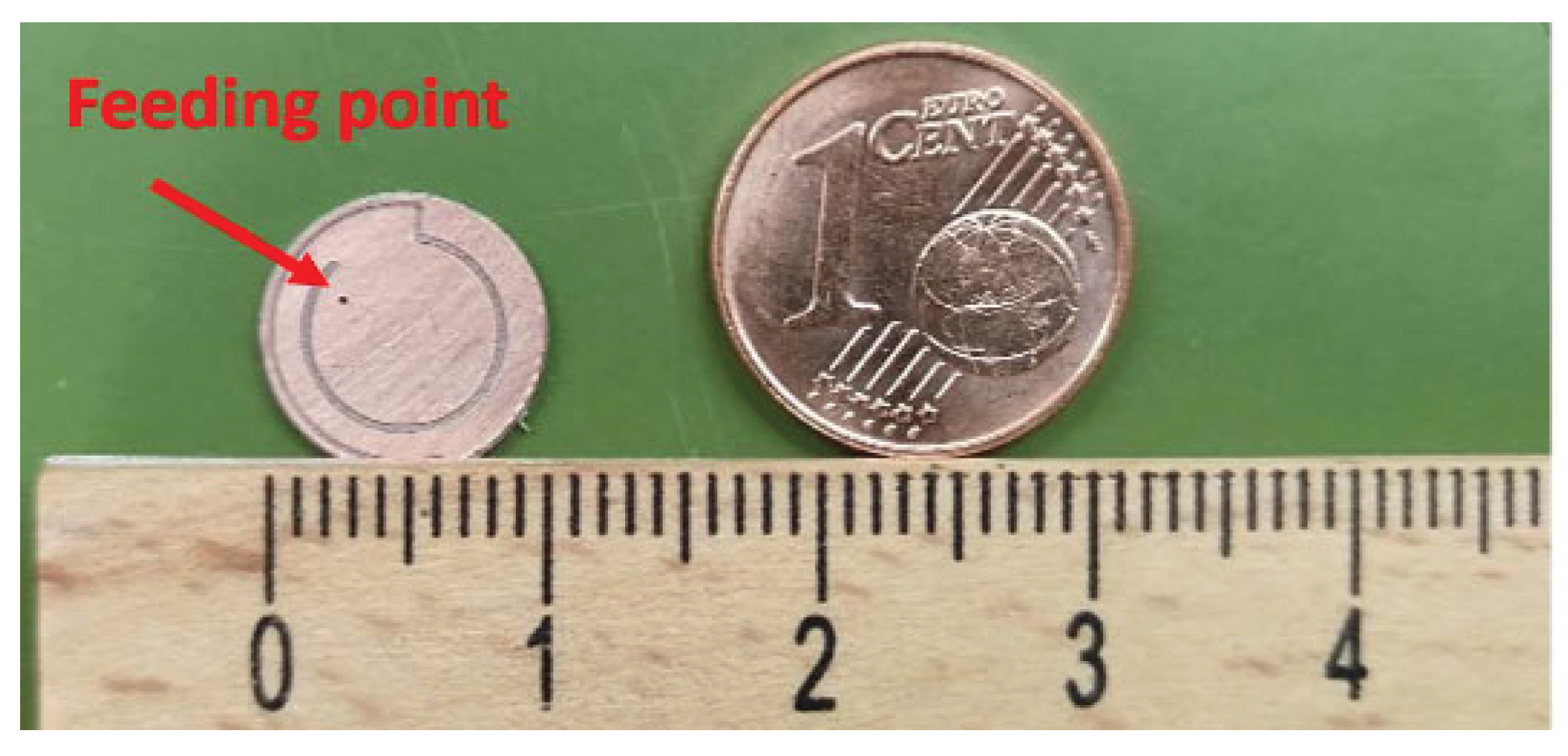
Figure 5.
Illustration of antenna structure details involving top and bottom sides [106].
Figure 5.
Illustration of antenna structure details involving top and bottom sides [106].
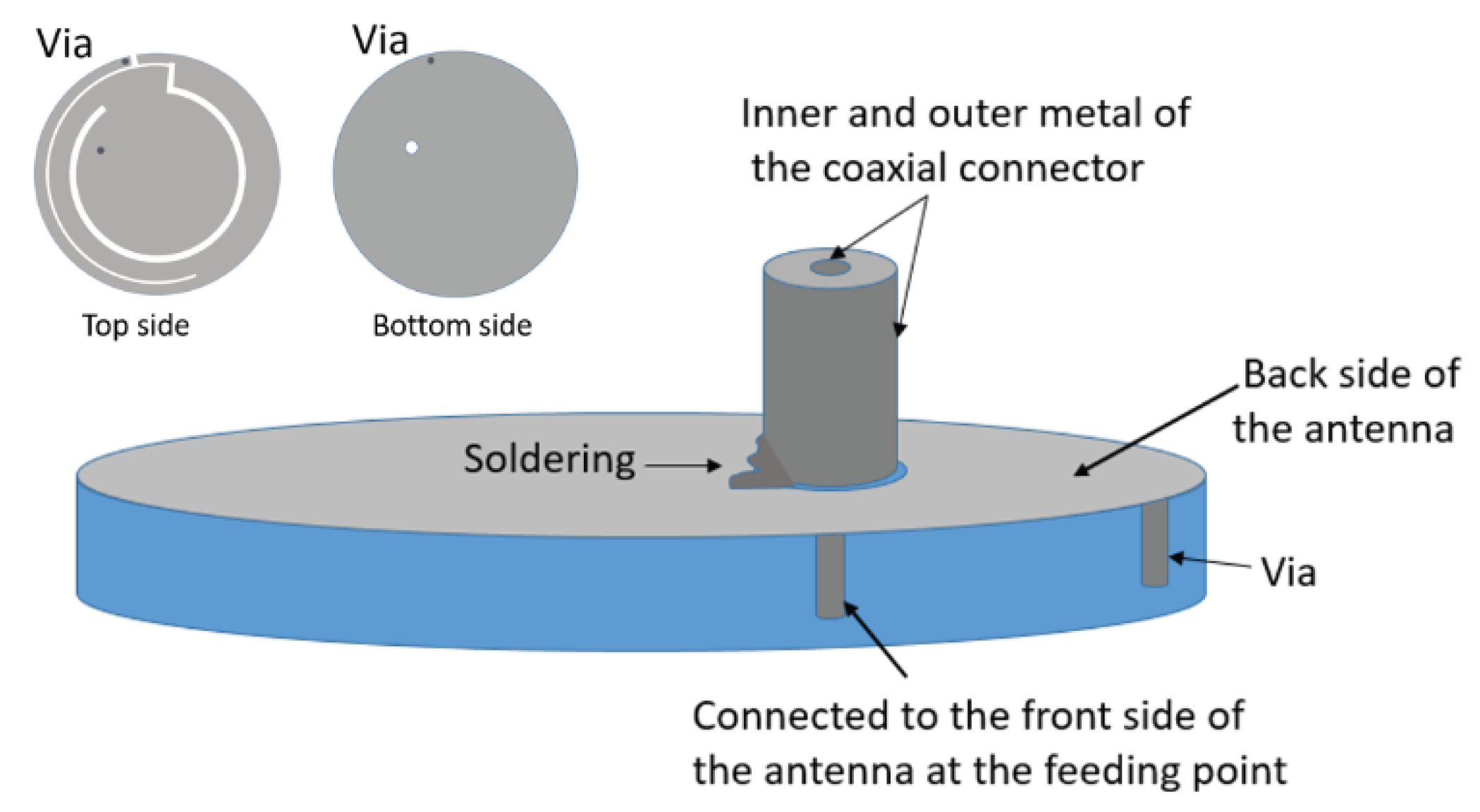
Figure 6.
Schematics of an environmental adapted antenna with a superstrate glued with its substrate [106].
Figure 6.
Schematics of an environmental adapted antenna with a superstrate glued with its substrate [106].
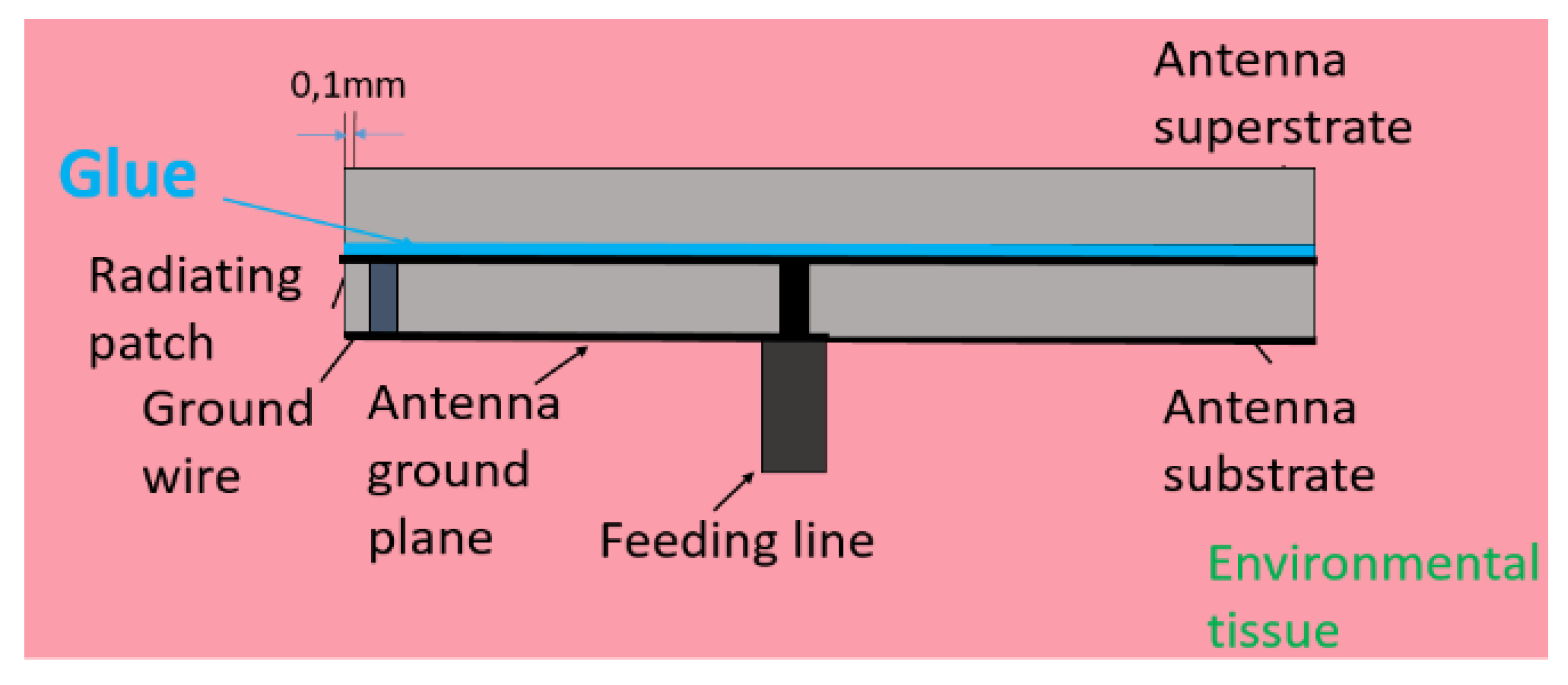
Figure 7.
Measurement scenario with the plastic cup including ground pork and the embedded antenna [106].
Figure 7.
Measurement scenario with the plastic cup including ground pork and the embedded antenna [106].
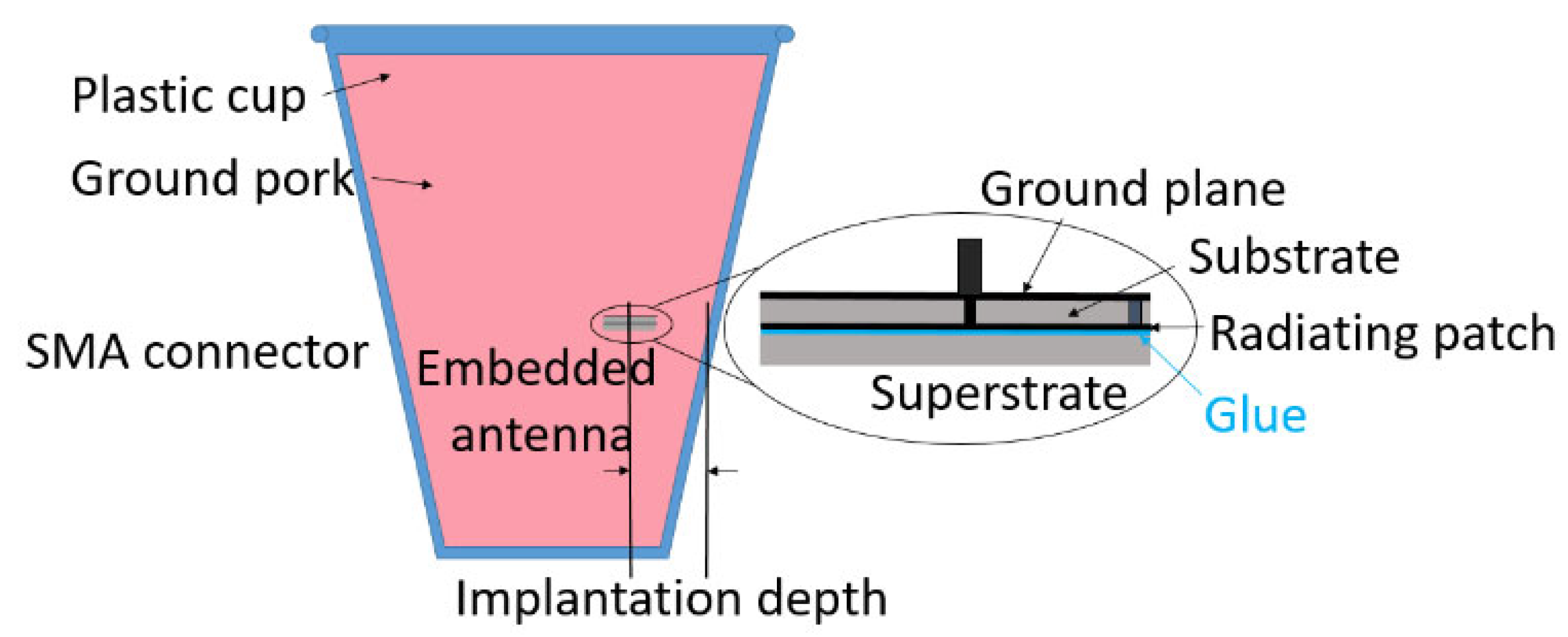
Figure 8.
Test bench involving the set of coils, the phantom and power amplifiers, [128].
Figure 8.
Test bench involving the set of coils, the phantom and power amplifiers, [128].
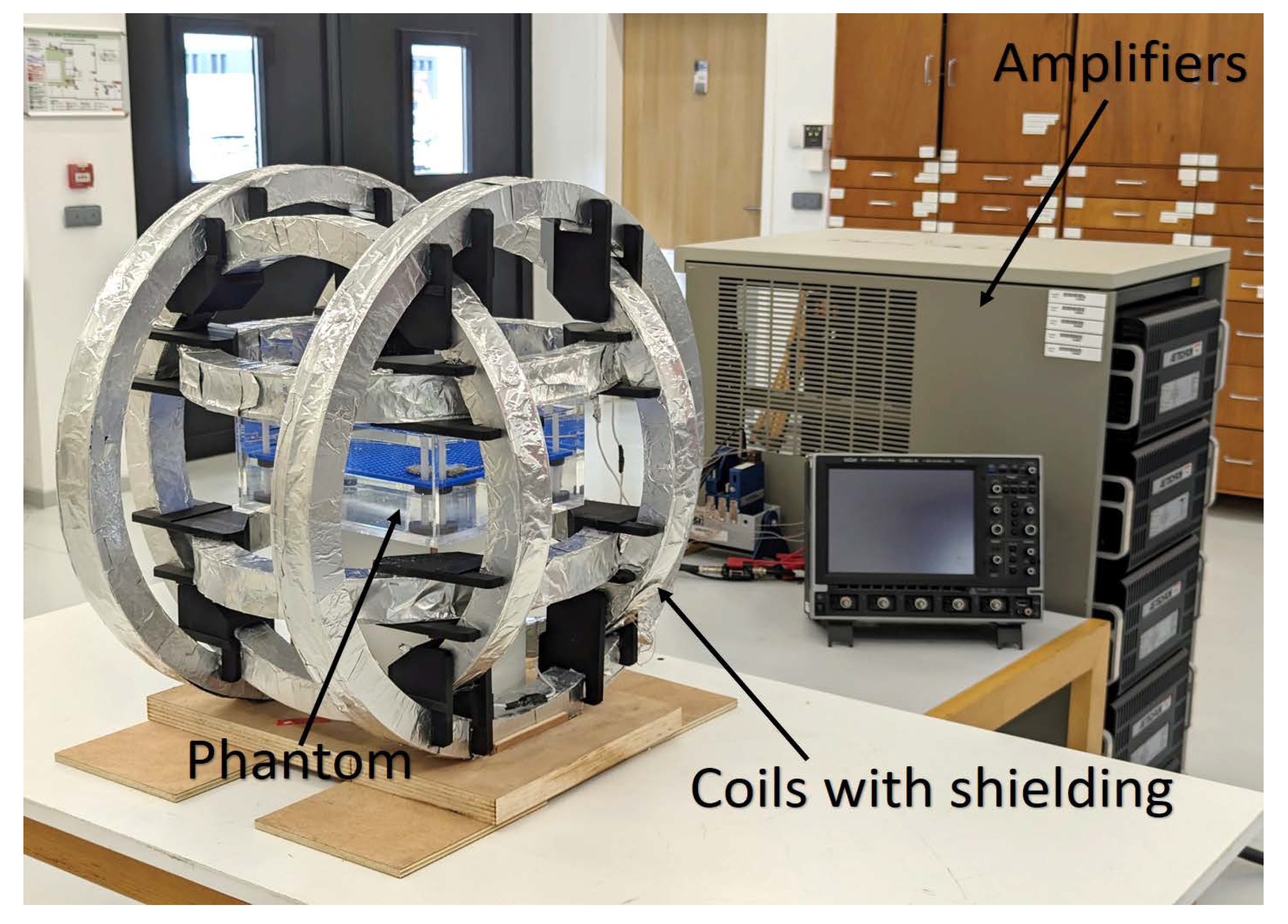
Figure 9.
Setup controlling and positioning of the pacemaker within the phantom involving atrial contraction signal and monitoring of ventricular stimulation, [128].
Figure 9.
Setup controlling and positioning of the pacemaker within the phantom involving atrial contraction signal and monitoring of ventricular stimulation, [128].
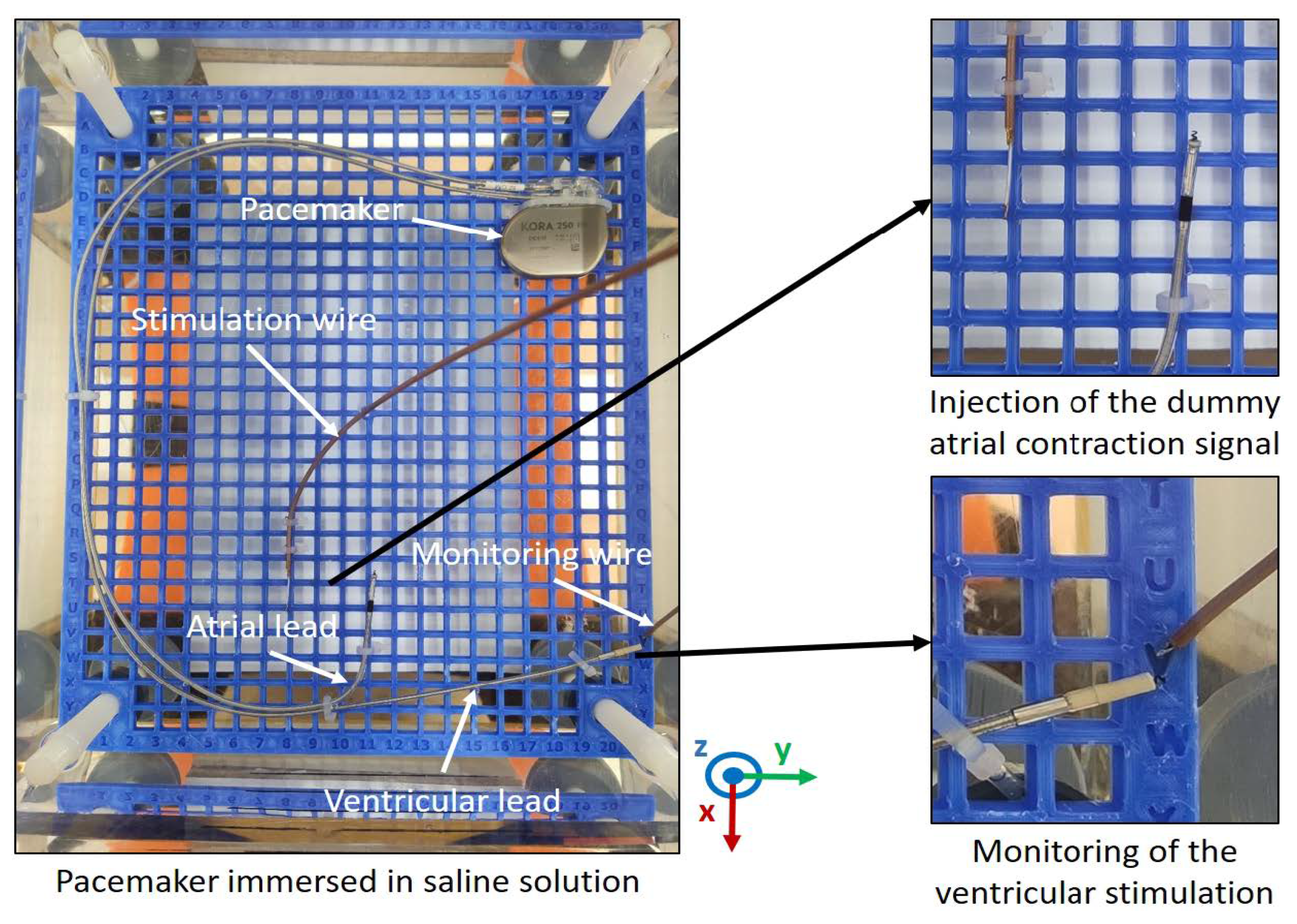
Figure 10.
Distribution of the RF field (vertically oriented) in the cross section of tunnel birdcage: (a) no material, (b) massive conductor, (c) piezoelectric [23].
Figure 10.
Distribution of the RF field (vertically oriented) in the cross section of tunnel birdcage: (a) no material, (b) massive conductor, (c) piezoelectric [23].
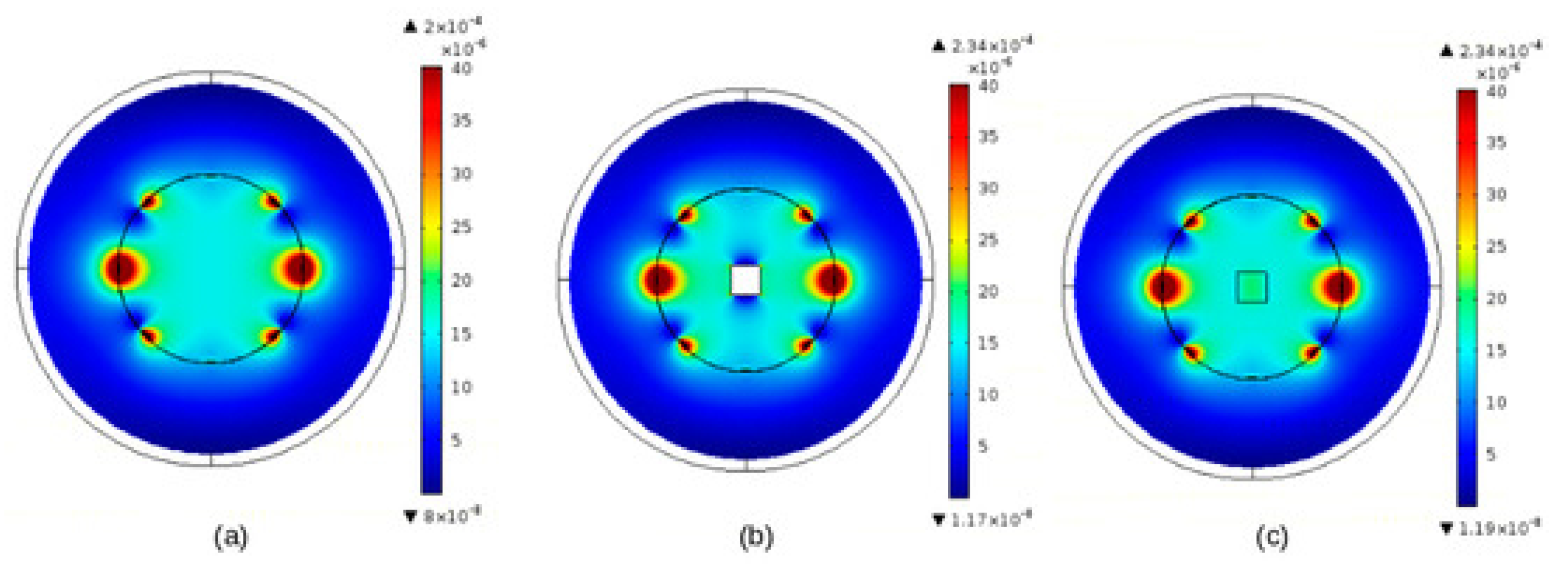
Figure 11.
Distribution of induced fields in a horizontal ground positioned body alongside an EV, (a) magnitude of B (T), (b) magnitude of E (V/m) [22].
Figure 11.
Distribution of induced fields in a horizontal ground positioned body alongside an EV, (a) magnitude of B (T), (b) magnitude of E (V/m) [22].
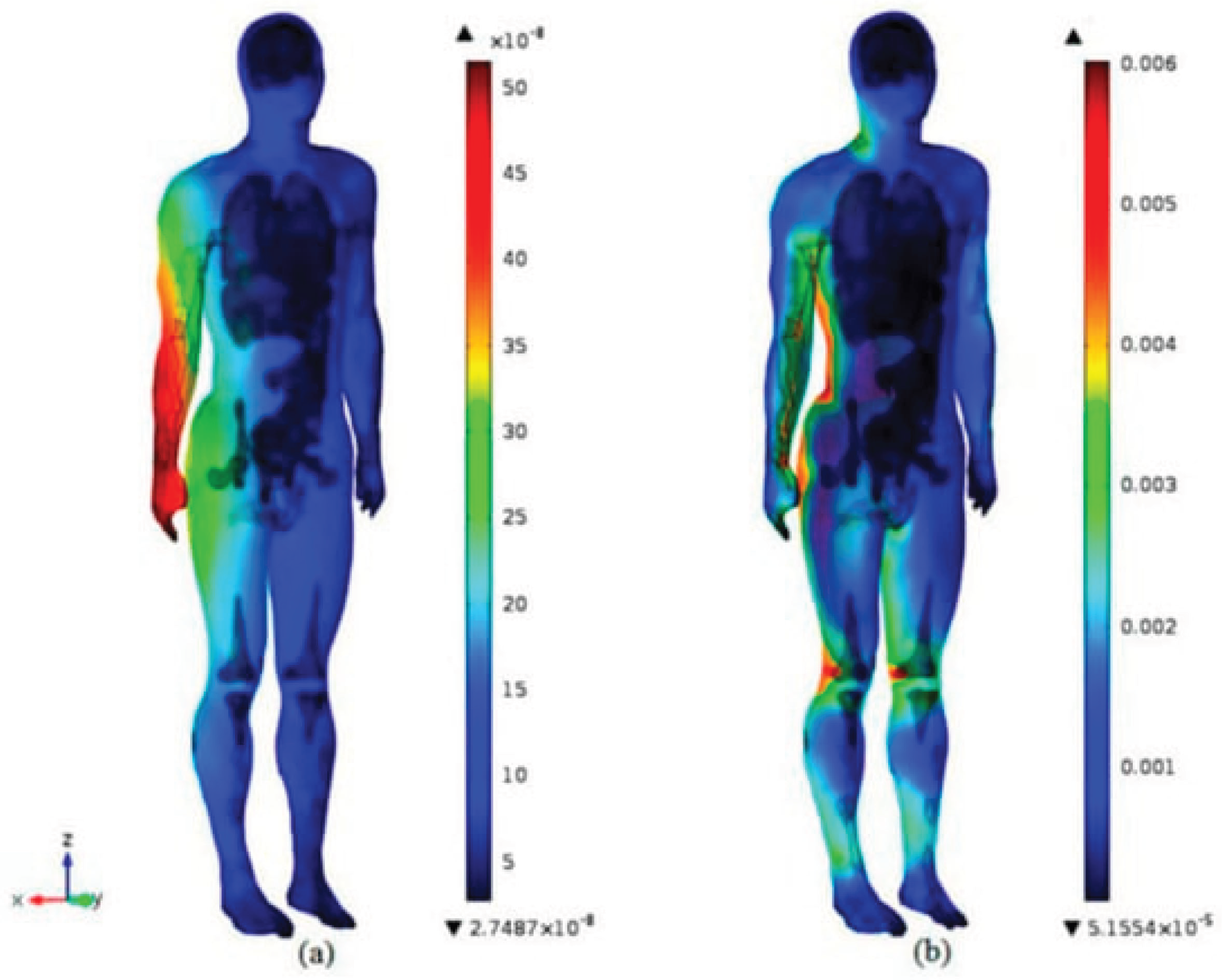
Figure 12.
Summary of the contribution objectives (left), the means of achieving them (right) and the corresponding future forecasts (down in italic).
Figure 12.
Summary of the contribution objectives (left), the means of achieving them (right) and the corresponding future forecasts (down in italic).
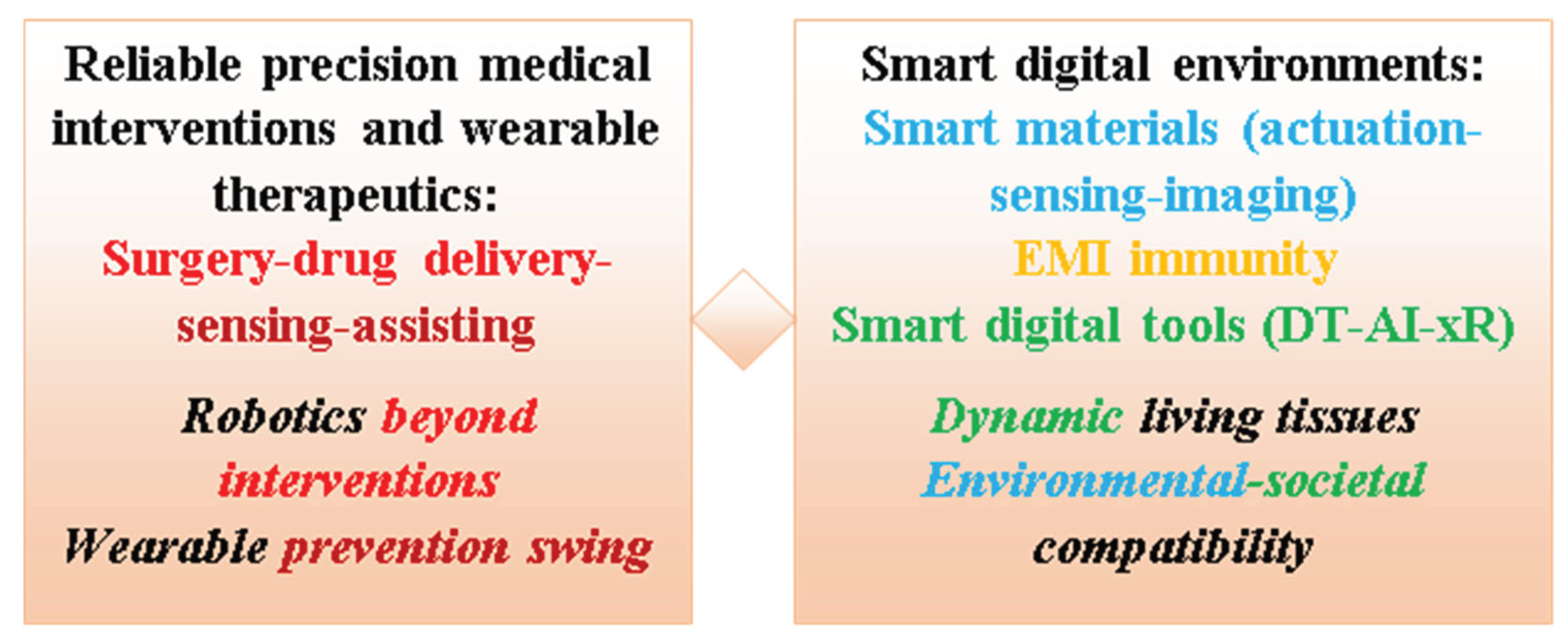
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



