
Submitted:
19 November 2025
Posted:
20 November 2025
You are already at the latest version
Abstract
Background/ Objectives; After negative results of the SAMMPRIS-trial the indication for endovascular treatment of atherosclerotic intracranial artery stenosis (ICAS) was widely restricted. It was the aim of our study to report whether intracranial arterial percutaneous transluminal angioplasty and stenting (PTAS) as ultima ratio therapy is still effective and safe enough. Methods: Between February 2011 and June 2019, 63 consecutive patients with and without emergent large vessel occlusion (ELVO) who received PTAS for symptomatic ICAS in the anterior or vertebrobasilar circulation were in-cluded in our study. Results: 32 patients had ELVO. In the remaining 31 patients, a known ICAS was treated with PTAS either because of recurrent stroke despite aggressive medical therapy with dual antiplatelet inhibition (n=24) or due to progressive hemodynamic ischemia (n=7). Stenting was successful in all 63 cases. Successful reperfusion was achieved in 94% of ELVO patients. Complications with new neurologic deficits, including dissection, subarachnoid hemorrhage, in-tracerebral hemorrhage (PH2), and stent-thrombosis, were seen in 5 ELVO patients (16%). At discharge, neuro-logical status improved in 16 patients (50%) and deteriorated in 7 patients (22%). In-hospital mortality happened in 5 of 32 ELVO cases (16%), all of them had lesions in the vertebrobasilar circulation. Regarding non-ELVO cases, two patients (6%) developed new neurologic deficits due to perforator strokes. There was no in-hospital mortality in this group. Conclusion: Even in unfavorable situations with acute atherothrombotic occlusions or recurrent strokes under ag-gressive medical therapy of known ICAS, PTAS remains a treatment option with reasonable efficacy and tolerable complication rates.
Keywords:
intracranial stenosis
; angioplasty
; stenting
; stroke
1. Introduction
In western countries atherosclerotic intracranial artery stenosis (ICAS) is a relatively rare but important cause of ischemic stroke. It is often a therapeutic challenge because of its high risk for recurrent stroke despite medical therapy and/or interventional stenting [1,2,3,4]. The SAMMPRIS trial (Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis) addressed this issue and randomized patients with high-grade ICAS to either aggressive medical therapy alone or aggressive medical therapy with intracranial arterial percutaneous transluminal angioplasty and stenting (PTAS) [2]. It was found that aggressive medical therapy alone was superior to the regime that included PTAS, mainly due to high periinterventional complication rates in the PTAS group [2,3,4,5].
The results of SAMMPRIS trial led to considerable changes of treatment strategies for symptomatic ICAS patients towards a clear primate of optimized medical therapy, limiting the indications for interventional treatment. According to current guidelines, PTAS may be considered only in cases with new symptoms and infarcts despite medical treatment with dual antiplatelet therapy (DAPT) or as rescue in cases with acute stroke due to emergent large vessel occlusion (ELVO) on the basis of underlying ICAS [6]. In most instances, ELVO patients with atherothrombotic occlusions are identified during failed thrombectomy procedures, ending up in emergency PTAS as ultima ratio with a need for sufficient antiplatelet therapy. In this case, associated risks of stent-thrombosis on one side and intracranial hemorrhage on the other side are difficult to control and may contribute to increased complication rates [7].
For the other group of patients with failure of medical therapy it is not clear whether PTAS as ultima ratio therapy is a source of further complications or if it would be helpful to avoid permanent disability [8,9,10].
It is a common impression among neurointerventionalists that the rate of unfavorable outcomes is high in both patient groups (ELVO; non-ELVO). However, literature data addressing real-life outcomes of PTAS after SAMMPRIS are scare and heterogeneous regarding inclusion criteria and outcome parameters [11,12,13,14,15,16,17,18].
This is why it was the aim of our study to review all PTAS procedures in the last mentioned two groups of indication in the period after publication of SAMMPRIS trial from 2011–2019 to evaluate the effectiveness and safety of PTAS regarding angiographic and in-hospital clinical outcomes.
2. Materials and Methods
Patients and Data Acquisition
This retrospective study was approved by our institutional ethics committee Nr, 430/18. For the analysis, we searched databases for patients who received PTAS in our institution between February 2011 and June 2019. We excluded all cases with intracranial stents that were not placed for ICAS, such as aneurysm or arterial dissection treatment. This left 63 consecutive patients to be included. Selection is shown in Figure 1. We assessed clinical and radiological data of these patients. All imaging data were reviewed by two independent neuroradiologists and a reference standard was established for statistical analysis.
We assigned cases with high-grade ICAS to one of two groups: 1) non-ELVO cases: after failure of medical therapy or in the case of hemodynamic strokes. 2) ELVO cases: acute stroke patients with emergent large vessel occlusion.
Study PopulationProcedures
All procedures were performed under general anesthesia in a biplane angiography suite (Axiom artis zee, Siemens Healthineers, Erlangen, Germany). Stenosis degree and the diameters of the adjacent normal arterial segments were determined using digital subtraction angiography (DSA) images and volume rendering reconstruction of an additional 3D rotational angiography. Stenosis degree was measured according to WASID criteria (Warfarin–Aspirin Symptomatic Intracranial Disease trial).
For non-ELVO cases, we usually deploy balloon-expandable stents. Diameter of balloon-expandable stents was at least 0.25 mm smaller than the normal vessel diameter to avoid over-dilatation. However, self-expanding stents were used if the target vessel diameter was below 2.5 mm or if the stenosis was not accessible with balloon-expandable stents. In cases of self-expanding stent-placement, stenoses were pre-dilated with an undersized balloon.
Non-ELVO Case
In ELVO cases, we usually deploy detachable self-expanding stents (Solitaire AB, Medtronic, Minneapolis, Minnesota, USA). If necessary, stenoses were dilated after stent-placement with an undersized balloon. In some cases, balloon-expandable stents were used for this indication, if feasible.
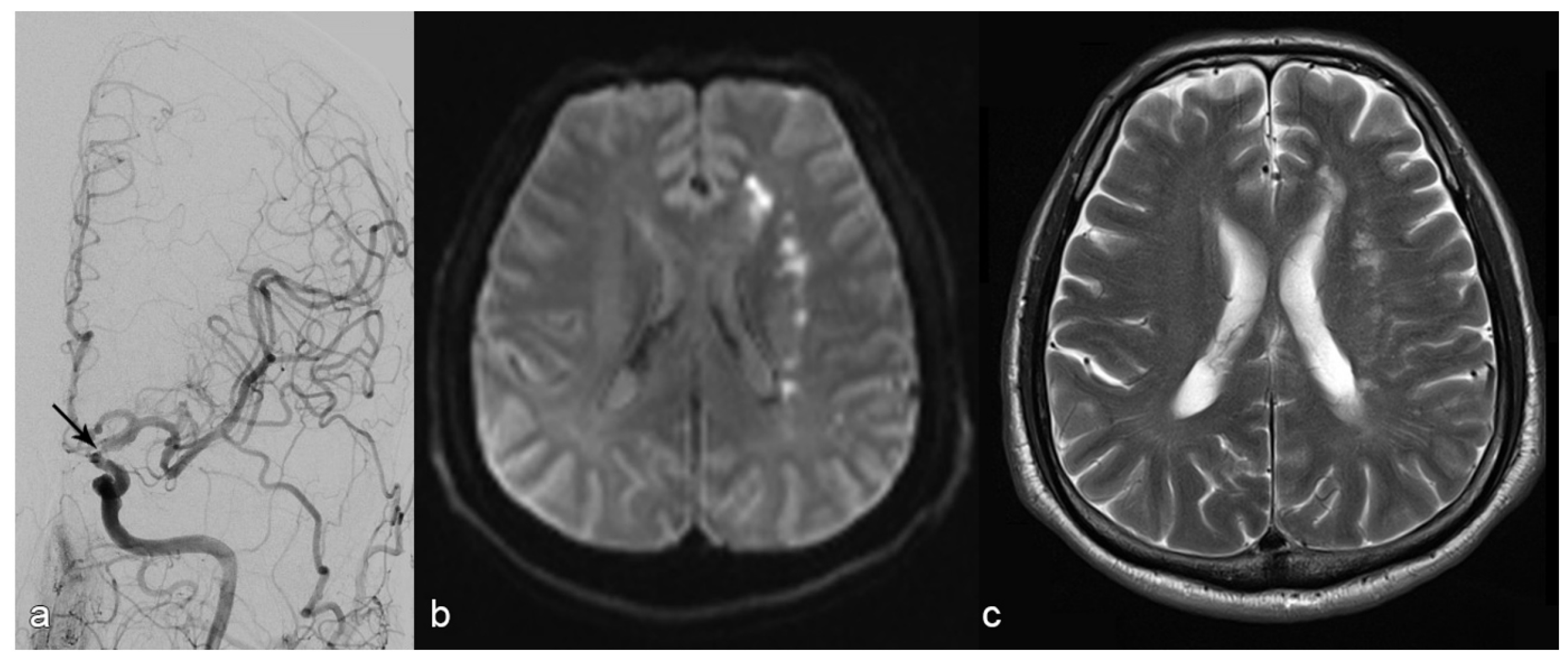
Figure 2.
Patient with stroke due to stenosis in the terminal segment of the left internal carotid artery (A: arrow). MR diffusion weighted imaging upon admission (B) shows subacute infarction in the white matter of the left centrum ovale with a hemodynamic pattern and without embolic cortical infarction. The decision is made to place a stent, which succeeds MRI upon discharge shows no additional infractions (C).
Figure 2.
Patient with stroke due to stenosis in the terminal segment of the left internal carotid artery (A: arrow). MR diffusion weighted imaging upon admission (B) shows subacute infarction in the white matter of the left centrum ovale with a hemodynamic pattern and without embolic cortical infarction. The decision is made to place a stent, which succeeds MRI upon discharge shows no additional infractions (C).
ELVO CaseAntiplatelet Management
All non-ELVO patients were already on DAPT with 100mg of Aspirin and 75mg of clopidogrel prior to the procedure. Antiplatelet treatment was not modified for stenting in these cases.
For emergency ELVO-patients, 70 I.U./kg of heparin and a bolus of .4µg/kg of Tirofiban were administered during the intervention before stenting, followed by a maintenance dose of Tirofiban of 1µg/kg/h and a loading dose of 600mg clopidogrel (oral) and 250mg of aspirin (intravenous) during the intervention. Tirofiban infusion was then stopped 4 hours after the procedure.
Outcome Parameters
Because of the different disease characteristics of these two groups (ELVO and non-ELVO), the outcome parameters were evaluated separately:
Outcome Parameters in ELVO Patients
Primary outcome parameters were technical success and reperfusion success as well as the occurrence of adverse events.
Stenting was defined as successful (technical success) if a residual stenosis of ≤50% was achieved. Reperfusion was defined as successful (reperfusion success) if complete or almost complete reperfusion (mTICI ≥2b) was achieved. Adverse events included intervention-related complications such as 1) intracranial dissections, 2) acute and subacute stent thrombosis, 3) Subarachnoid hemorrhage (SAH) and 4) symptomatic intracranial hemorrhage (parenchymal hematoma type 2 “PH-2” according to the European Cooperative Acute Stroke Study “ECASS II” classification).
Secondary outcome parameters were early clinical neurological outcomes during hospital stay and at discharge. Neurological outcome was assessed using national institutes of health stroke scale (NIHSS), with early improvement (and deterioration) being defined as decrease (and increase) in NIHSS by at least 4 points at discharge, respectively. Furthermore, clinical outcome at discharge was assessed using modified Rankin scale (mRS), with good clinical outcome being defined as mRS=0-2.
To address the possible different natural courses of processes in anterior and vertebrobasilar circulations, we assessed all primary and secondary outcome parameters separately for both circulations [19].
Outcome Parameters in Non-ELVO Patients
Primary outcome parameters were technical success as well as the occurrence of adverse events (defined previously).
Secondary outcome parameter was the occurrence of newly occurred stroke after the procedure. In this group, the neurological situation was compared to the asymptomatic state before the procedure during clinical stability.
Also, here we assessed all primary and secondary outcome parameters separately for both circulations.
Statistics
Parametric variables are indicated as mean ± standard deviation (SD) and non-parametric variables are indicated as median and interquartile range (IQR). For comparison of these variables, we used a Student’s T test or a Mann–Whitney U tests after testing for normal distribution with a Shapiro-Wilk test. Nominal variables were tested with Fisher’s exact tests and χ2 tests depending on sample size. P values under the α-level of .05 were defined as significant. Multivariable analysis was performed with a binary logistic regression test indicating odds ratios (ORs) and 95%-confidence intervals (CI). All statistical analyses were performed with SPSS-25 software.
3. Results
Baseline Characteristics
Baseline characteristics of all patients can be found in Table 1. In summary, 32 of 63 patients (51%) had acute strokes with ELVO. In the remaining 31 patients (49%) (non-ELVO-group), intracranial stenosis was treated with PTAS either because of recurrent stroke with infarctions despite aggressive medical therapy with DAPT (n=24) or due to hemodynamic insufficiency with progressive symptoms and infarctions (n=7).
Except for the history of stroke and previous medication, there were no other significant differences between the two groups regarding demographic data and comorbidities (Table 1).
The distribution of anterior and vertebrobasilar circulation was also comparable (p=.319). Among patients with anterior circulation pathology, middle cerebral artery (MCA)-stenosis was more frequent in ELVO-group (38% vs. 16%), whereas internal carotid artery (ICA)-pathology was more frequent in non-ELVO-group (36% vs. 9%).
In ELVO cases, the diagnosis of an underlying stenosis was made after a median of 1 (Interquartile range: IQR, 1-3) thrombectomy maneuvers.
Outcome Parameters in ELVO Group
Regarding technical success, stenting was technically successful in all cases (Table 1)
Successful reperfusion (mTICI≥2b) was achieved in 94% of ELVO patients (Figure 3).
Intervention related complications and postinterventional imaging findings can be found in Table 2. Main complications are summarized as follows:
- Intracranial dissections with compromised side branch patency occurred in two out of 32 patients. Both cases were in the vertebrobasilar circulation and occurred after balloon angioplasty. In one of these two cases, there was subsequent in-stent thrombosis, which was fatal. In the other case, there were embolic and perforator infarction which led to worsening of the neurologic symptoms.
- Acute and subacute stent thrombosis were observed in two cases, both of which occurred in the vertebrobasilar circulation and were symptomatic: one of these two patients had progressive infarction, which led to neurological worsening (mRS=5); the other had stent-thrombosis after dissection, which was fatal (mentioned previously).
- There was no SAH.
- Symptomatic intracranial hemorrhage occurred in two ELVO patients, both of them in anterior circulation. Only one of these two patients had intravenous thrombolysis therapy before the procedure. One patient recovered and improved neurologically (mRS=2); the other one deteriorated (mRS=4).
According to NIHSS, 50% of patients had neurological improvement upon discharge. Death within 30 days occurred in 5 cases (16%) in this group. Secondary outcome parameters regarding good clinical outcome at discharge (mRS=0-2) was observed in 31% of ELVO cases. When only ELVO patients with stenosis in the anterior circulation were considered, good clinical outcomes were observed in 40% of the cases.
Outcome Parameters in Non-ELVO Group
Stenting was also technically successful in all cases in this group. Regarding intervention related complications, there were no intracranial dissections, acute or subacute in-stent thrombosis, SAH or symptomatic intracranial hemorrhage.
Two patients in this group (6%) had new stroke after the procedure because of periinterventional perforator infarctions. Deaths within the first 30 days did not occur in non-ELVO-group.
There was one severe pneumonia with necessity of prolonged postinterventional ventilation as non-neurologic complication.
Comparison of Anterior and Vertebrobasilar Circulation
All fatal cases were ELVO-cases in the vertebrobasilar circulation (p=.022).
Furthermore, all vessel dissections occurred in the vertebrobasilar circulation, and all intracranial hemorrhages happened in the anterior circulation. However, these two differences did not reach statistical significance.
4. Discussion
From the technical point of view, all stenting procedures were successful with less than 50% residual stenosis and no differences between both groups. In the group with ELVO and emergent intervention in the anterior and vertebrobasilar circulation, we achieved good reperfusion results (mTICI≥2b) in 94% of cases, which is higher than the cumulative reperfusion rate of 71% after thrombectomy of embolic stroke in anterior circulation without PTAS in the HERMES study [21]. This rate is comparable with other stenting trials in anterior cerebral circulation and is somewhat higher than the successful reperfusion rate of 80% reported by Baek et al. when varying rescue treatments for ICAS in anterior circulation were used (including balloon angioplasty, stenting, and intra-arterial glycoprotein IIb/IIIa inhibitor infusion) [21,22,23]. The periprocedural complication rate in our ELVO patients was significantly higher than in the more elective non-ELVO-cases. Severe adverse events like symptomatic hemorrhage or stent thrombosis as well as mortality was seen only in ELVO patients.
However, these complication rates are comparable to data reported from thrombectomy trials without stenting [20,21].
The rates of hemorrhagic complications in our ELVO-group were in accordance with results by Baek et al. who analyzed ELVO-patients and found no added bleeding risk when additional endovascular therapy was used [21]. Furthermore, with two cases (6%), the symptomatic hemorrhage rate was not higher than reported from thrombectomy trials [20]. In accordance with the literature, our findings support that administration of intravenous thrombolysis was no risk factor for hemorrhage despite DAPT, implying that thrombolysis should not discourage from stenting if necessary [24]. However, to avoid potential hemorrhagic risks of aggressive DAPT some authors proposed to use balloon angioplasty without stenting [25]. The limitation of this approach in terms of vessel patency is known [26]. In attempts to use angioplasty only, we frequently observed re-obstruction due to elastic recoil or dissection during the intervention. Due to the fact, that intracranial stent thrombosis is in most instances a catastrophic event, we preferred an adequate antiplatelet therapy with immediate action [27]. However, according to this data, it remains unclear, whether antiplatelet therapy including the use of glycoprotein (GP) IIb-IIIa-antagonists increases the rate of hemorrhagic complications.
Regarding vessel dissection and stent thrombosis, these are probably specific complications for procedures including angioplasty with a relatively high rate of 9% in our sample. Plaque alteration and rupture after stent retriever maneuvers or balloon dilation may play a role in the development of a highly thrombogenic surface. To the best of our knowledge, data about the rates of these complications among ELVO patients undergoing emergent PTAS don’t exist.
Favorable clinical outcome (mRS=0-2) upon discharge was achieved in 31% of patients in ELVO-group. This numbers appear relatively low given that good clinical outcome rates in ELVO-patients with embolic occlusion are higher in some of the thrombectomy trials (EXTEND-IA [28], SWIFT-PRIME [29]). However, a closer look into our data reveals that this is mainly because we included multimorbid patients with unfavorable neurological baselines, high-grade stenoses, and stenoses in the vertebrobasilar circulation (Table 1 and Table 2), which often have a worse clinical course.19 In fact, when only ELVO patients with stenosis in the anterior circulation are considered, our good clinical rate reaches 40% without mortality cases which occurred only in the vertebrobasilar circulation. This is comparable to the 46% indicated by Baek et al. in anterior circulation [21]. Approaching clinical outcome more pragmatically and taking into account patients’ individual baseline, our results are more favorable: 50% of ELVO-patients with PTAS improved neurologically, which is comparable to results in the HERMES study for embolic strokes. Thus, it seems to be worthwhile undertaking endovascular recanalization including acute PTAS in this group of patients.
In non-ELVO-patients, the procedure was again technically successful in all cases. However, with 6% the rate of in-hospital stroke and/or neurological deterioration was significantly lower in comparison to the ELVO cases (22%) (p =0,41). There were no death cases among the non-ELVO patients compared to an in-hospital mortality rate of 16% in the ELVO-group (p=.022). Importantly, no vessel dissection or stent thrombosis were seen, which support the consideration that these complications, which were seen in the ELVO-group, could be not directly related to the stent implantation, but more to the thrombectomy itself or to preceding balloon angioplasty. Emergent antithrombotic therapy may also play a role in this regard. We observed two perforator-strokes with new deficits which are typical PTAS complications in the posterior circulation [30].
Another patient, with multimorbidity, deteriorated due to hospital acquired pneumonia. The rates of strokes (6%) and deaths (0%) were lower than the periprocedural complication rate in the SAMMPRIS trial (16.3%); and interestingly comparable with the results reported by Meyer L et al., who founded periprocedural rate of stroke and death of 6.5% [31]. Our ischemic complication rate was comparable to rates reported by Aghaebrahim et al. in their analysis of patients with ICAS, who received PTAS with balloon-expandable and self-expanding stents after aggressive medical management [26]. However, the risk of ischemic complication after stenting in non-ELVO patients should be taken into consideration in comparison with the known high percentage of patients having further ischemic strokes in the territory of the stenotic artery despite aggressive medical management [32,33,34]. Importantly, there were no mortality in this group.
Limitations
The relatively small sample size is owed to the rare incidence of ICAS and the restricted indications for PTAS. However, we focused on a monocentric approach, as this limitation is an advantage at the same time: on the one hand our data are systematically biased by specific features of our institution (such as strict inclusion criteria). A further limitation is a lack of mid-term and long-term outcomes. 30-day results for non-ELVO patients were not available for a sufficient number of cases. For the ELVO group further evaluations of 3 months outcome data from a multicentric registry seems to be useful.34 Due to the fact that strokes in the follow-up play an important role in the assessment of the efficacy of PTAS procedures such systematic studies are necessary.
5. Conclusions
Even under restricted conditions such as ultima ratio therapy in unfavorable groups of patients, PTAS remains a valuable treatment option with reasonable angiographic and clinical results. Complication rates were lower than expected. Further multicentric studies with larger numbers of cases are necessary to define proper indications and technical proceedings with a higher level of evidence.
Ethics approval and consent to participate
This study was approved by the local Ethics Committee (Reference number: 430/18). It was conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments. Informed consent was waived due to the retrospective nature of the study.
Funding
No specific grant from any funding agency was received.
Availability of data and materials
The data sets used to analyze during the current study are available from the corresponding author on reasonable request.
Competing interests
None of the authors had any competing interests.
Declaration of generative AI and AI-assisted technologies in the manuscript preparation process Statement
During the preparation of this work, the authors did not use AI or AI-assisted technology beyond basic tools such as those used to check grammar, spelling, and references.
Abbreviations
The following abbreviations are used in this manuscript:
| ICAS | intracranial artery stenosis |
| PTA | percutaneous transluminal angioplasty |
| ELVO | emergent large vessel occlusion |
| DSA | digital subtraction angiography |
| DAPT | dual antiplatelet therapy |
References
- Holmstedt CA, Turan TN, Chimowitz MI. Atherosclerotic intracranial arterial stenosis: risk factors, diagnosis, and treatment. Lancet Neurol 2013;12:1106-1114. [CrossRef]
- Chimowitz MI, Lynn MJ, Derdeyn CP, et al. Stenting versus aggressive medical therapy for intracranial arterial stenosis. N Engl J Med 2011;365:993-1003. [CrossRef]
- Kasner SE, Chimowitz MI, Lynn MJ, et al. Predictors of ischemic stroke in the territory of a symptomatic intracranial arterial stenosis. Circulation 2006;113:555-563. [CrossRef]
- Zaidat OO, Klucznik R, Alexander MJ, et al. The NIH registry on use of the Wingspan stent for symptomatic 70-99% intracranial arterial stenosis. Neurology 2008;70:1518-1524. [CrossRef]
- Derdeyn CP, Chimowitz MI, Lynn MJ, et al. Aggressive medical treatment with or without stenting in high-risk patients with intracranial artery stenosis (SAMMPRIS): the final results of a randomised trial. Lancet 2014;383:333-341. [CrossRef]
- Kernan WN, Viscoli CM, Varughese MC. Litigation seeking access to data from ongoing clinical trials: a threat to clinical research. JAMA Intern Med 2014;174:1502-1504. [CrossRef]
- Kurre W, Berkefeld J, Brassel F, et al. In-hospital complication rates after stent treatment of 388 symptomatic intracranial stenoses: results from the INTRASTENT multicentric registry. Stroke 2010;41:494-498. [CrossRef]
- Sangha RS, Naidech AM, Corado C, et al. Challenges in the Medical Management of Symptomatic Intracranial Stenosis in an Urban Setting. Stroke 2017;48:2158-2163. [CrossRef]
- Alexander MJ, Zauner A, Chaloupka JC, et al. WEAVE Trial: Final Results in 152 On-Label Patients. Stroke 2019;50:889-894. [CrossRef]
- Fiorella D, Derdeyn CP, Lynn MJ, et al. Detailed analysis of periprocedural strokes in patients undergoing intracranial stenting in Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS). Stroke 2012;43:2682-2688. [CrossRef]
- Nardai S, Kis B, Gubucz I, et al. Coronary stent implantation in acute basilar artery occlusion with underlying stenosis: potential for increased effectiveness in endovascular stroke therapy. EuroIntervention 2019.
- Ma N, Zhang Y, Shuai J, et al. Stenting for symptomatic intracranial arterial stenosis in China: 1-year outcome of a multicentre registry study. Stroke Vasc Neurol 2018;3:176-184. [CrossRef]
- Miao Z, Zhang Y, Shuai J, et al. Thirty-Day Outcome of a Multicenter Registry Study of Stenting for Symptomatic Intracranial Artery Stenosis in China. Stroke 2015;46:2822-2829. [CrossRef]
- Park SC, Cho SH, Kim MK, et al. Long-term Outcome of Angioplasty Using a Wingspan Stent, Post-Stent Balloon Dilation and Aggressive Restenosis Management for Intracranial Arterial Stenosis. Clin Neuroradiol 2019. [CrossRef]
- Gao P, Wang D, Zhao Z, et al. Multicenter Prospective Trial of Stent Placement in Patients with Symptomatic High-Grade Intracranial Stenosis. AJNR Am J Neuroradiol 2016;37:1275-1280. [CrossRef]
- Meyer T, Nikoubashman O, Kabelitz L, et al. Endovascular stentectomy using the snare over stent-retriever (SOS) technique: An experimental feasibility study. PLoS One 2017;12:e0178197. [CrossRef]
- Chimowitz MI, Kokkinos J, Strong J, et al. The Warfarin-Aspirin Symptomatic Intracranial Disease Study. Neurology 1995;45:1488-1493. [CrossRef]
- Zhang Y, Sun Y, Li X, et al. Early versus delayed stenting for intracranial atherosclerotic artery stenosis with ischemic stroke. J Neurointerv Surg 2019. [CrossRef]
- Nordmeyer H, Chapot R, Aycil A, et al. Angioplasty and Stenting of Intracranial Arterial Stenosis in Perforator-Bearing Segments: A Comparison Between the Anterior and the Posterior Circulation. Front Neurol 2018;9:533. [CrossRef]
- Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet 2016;387:1723-1731. [CrossRef]
- Baek JH, Kim BM, Heo JH, et al. Outcomes of Endovascular Treatment for Acute Intracranial Atherosclerosis-Related Large Vessel Occlusion. Stroke 2018;49:2699-2705. [CrossRef]
- Stracke CP, Meyer L, Fiehler J, et al. Intracranial bailout stenting with the Acclino (Flex) Stent/NeuroSpeed Balloon Catheter after failed thrombectomy in acute ischemic stroke: a multicenter experience. J Neurointerv Surg 2020;12:43-47. [CrossRef]
- Wu C, Chang W, Wu D, et al. Angioplasty and/or stenting after thrombectomy in patients with underlying intracranial atherosclerotic stenosis. Neuroradiology 2019;61:1073-1081. [CrossRef]
- Gory B, Haussen DC, Piotin M, et al. Impact of intravenous thrombolysis and emergent carotid stenting on reperfusion and clinical outcomes in patients with acute stroke with tandem lesion treated with thrombectomy: a collaborative pooled analysis. Eur J Neurol 2018;25:1115-1120. [CrossRef]
- Karanam LSP, Sharma M, Alurkar A, et al. Balloon Angioplasty for Intracranial Atherosclerotic Disease: A Multicenter Study. J Vasc Interv Neurol 2017;9:29-34.
- Aghaebrahim A, Agnoletto GJ, Aguilar-Salinas P, et al. Endovascular Recanalization of Symptomatic Intracranial Arterial Stenosis Despite Aggressive Medical Management. World Neurosurg 2019;123:e693-e699. [CrossRef]
- Kim B, Kim BM, Bang OY, et al. Carotid Artery Stenting and Intracranial Thrombectomy for Tandem Cervical and Intracranial Artery Occlusions. Neurosurgery 2020;86:213-220. [CrossRef]
- Campbell BC, Mitchell PJ, Kleinig TJ, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med 2015;372:1009-1018. [CrossRef]
- Saver JL, Goyal M, Bonafe A, et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med 2015;372:2285-2295. [CrossRef]
- Nordmeyer H, Chapot R, Haage P. Endovascular Treatment of Intracranial Atherosclerotic Stenosis. Rofo 2019;191:643-652. [CrossRef]
- Meyer L, Leischner H, Thomalla G, et al. Stenting with Acclino(R) (flex) for symptomatic intracranial stenosis as secondary stroke prevention. J Neurointerv Surg 2020. [CrossRef]
- Wabnitz AM, Derdeyn CP, Fiorella DJ, et al. Hemodynamic Markers in the Anterior Circulation as Predictors of Recurrent Stroke in Patients With Intracranial Stenosis. Stroke 2018:STROKEAHA118020840. [CrossRef]
- Derdeyn CP, Fiorella D, Lynn MJ, et al. Nonprocedural Symptomatic Infarction and In-Stent Restenosis After Intracranial Angioplasty and Stenting in the SAMMPRIS Trial (Stenting and Aggressive Medical Management for the Prevention of Recurrent Stroke in Intracranial Stenosis). Stroke 2017;48:1501-1506. [CrossRef]
- Wollenweber FA, Tiedt S, Alegiani A, et al. Functional Outcome Following Stroke Thrombectomy in Clinical Practice. Stroke 2019;50:2500-2506. [CrossRef]
Figure 1.
Chart illustrating causes for stenting in our cohort.
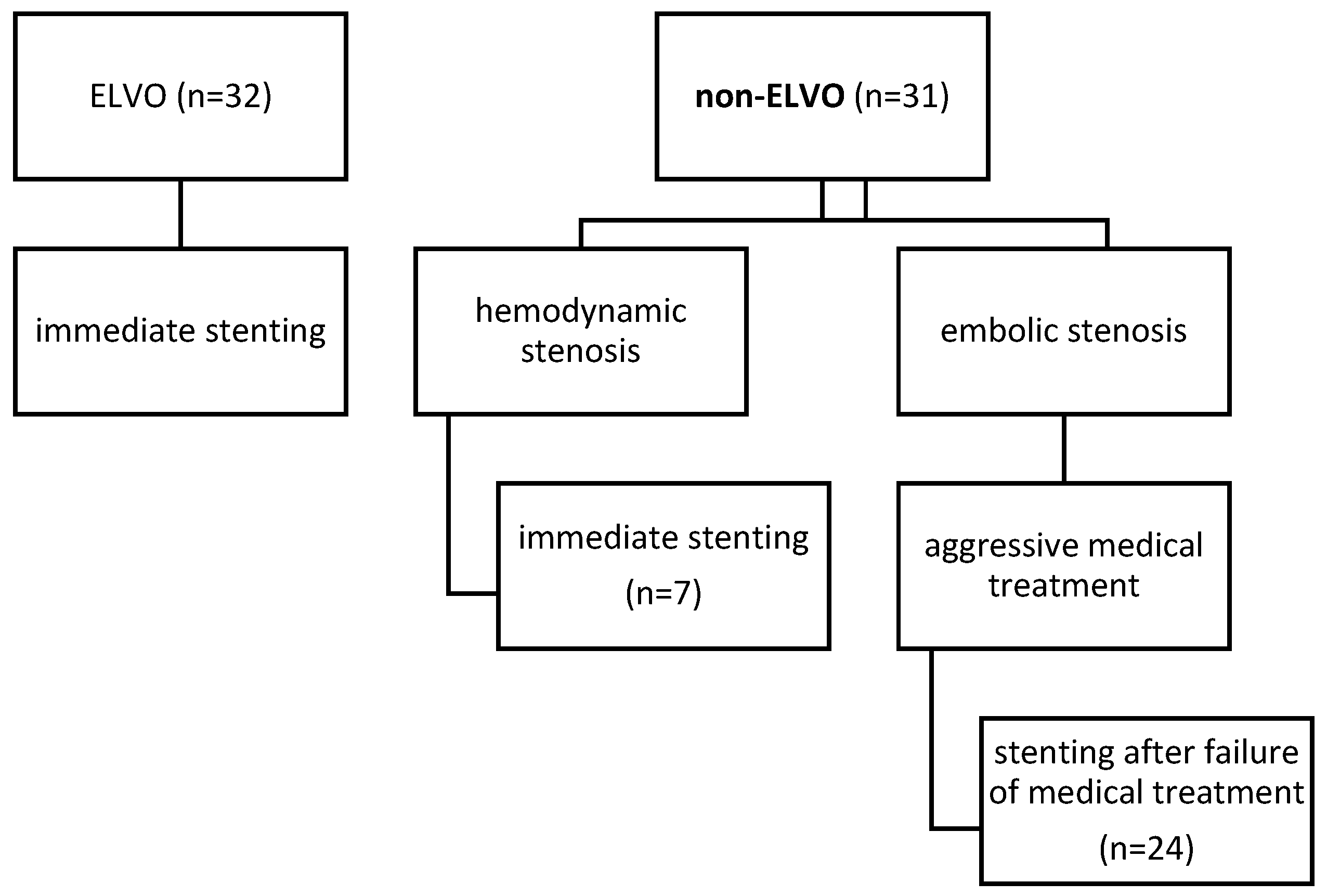
Figure 3.
Patient with acute stroke due to acute occlusion of the basilar artery (A). After mechanical thrombectomy, there is a high-grade stenosis, which is stented successfully (B). There is no infarction on MRI upon discharge.
Figure 3.
Patient with acute stroke due to acute occlusion of the basilar artery (A). After mechanical thrombectomy, there is a high-grade stenosis, which is stented successfully (B). There is no infarction on MRI upon discharge.
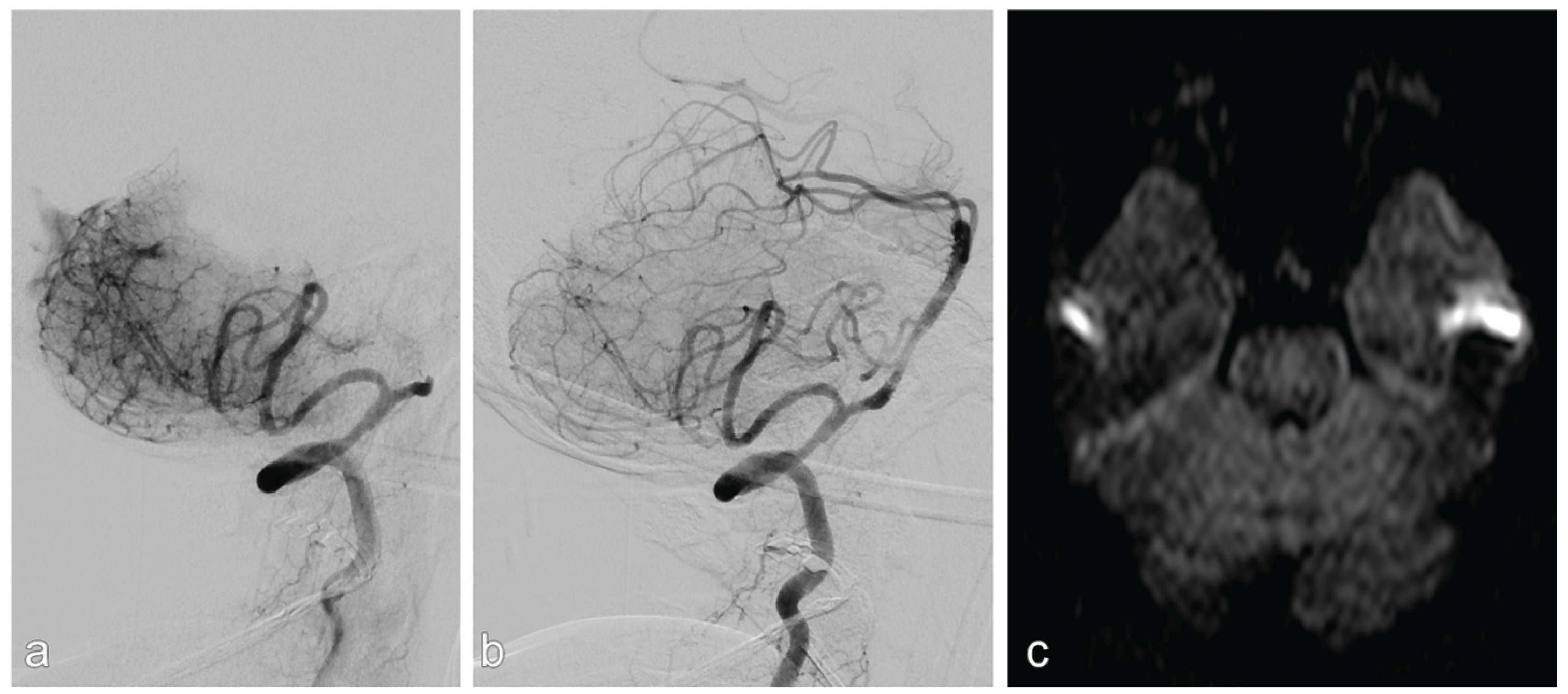

Table 1.
Baseline and procedural characteristics of all patients.
| non-ELVO group (n=31) | ELVO group (n=32) | p-value | |
| Baseline characteristics | |||
| Age [median] | 71 (IQR, 59-73) | 64 (IQR, 58-71) | .239 |
| Female sex [n] | 8 (25%) | 8 (36%) | .365 |
| History of TIA [n] | 6 (19%) | 4 (13%) | .457 |
| History of stroke [n] | 28 (90%) | 5 (17%) | <.001 |
| Arterial hypertension [n] | 30 (97%) | 29 (91%) | .317 |
| Current smoker [n] | 8 (26%) | 7 (22%) | .714 |
| Diabetes mellitus [n] | 11 (34%) | 12 (38%) | .721 |
| Hyperlipidemia [n] | 9 (29%) | 7 (22%) | .514 |
| CHD [n] | 6 (19%) | 5 (16%) | .697 |
| Atrial fibrillation [n] | 4 (13%) | 6 (19%) | .525 |
| Previous medication | |||
| Anticoagulation [n] | 5 (16%) | 3 (9%) | .421 |
| None / mono / dual antiplatelets [n] | 4 / 6 / 21 (13% / 19% / 68%) | 20 / 9 /3 (63% / 28% / 9%) | <.001 |
| Statins [n] | 25 (81%) | 10 (31%) | <.001 |
| Stenosis characteristics | |||
| MCA [n] | 5 (16%) | 12 (38%) | |
| ICA [n] | 11 (36%) | 3 (9%) | .023 |
| Vertebrobasilar [n] | 15 (48%) | 17 (53%) | |
| Degree [median] | 82 (79-89) | 80 (71-90) | .448 |
| Clinical characteristics | |||
| mRS pre stroke [median] | 1 (IQR, 0-2) | 0 (IQR, 0-1) | .001 |
| NIHSS upon admission [median] | 4 (IQR, 1-10) | 13 (IQR, 5-21) | <.001 |
| Infarction Characteristics | |||
| Embolic infarction [n] | 12 (39%) | 22 (68%) | |
| Hemodynamic infarction [n] | 4 (13%) | 0 (0%) | |
| Mix type: embolic and hemodynamic infarction [n] | 9 (29%) | 5 (16%) | .018 |
| Perforator infarction [n] | 6 (19%) | 5(16%) | |
| Procedural characteristics | |||
| Balloon-expandable stents vs. self-expanding [n] | 27 / 4 (87% / 13%) | 14 /18 (44% / 56%) | <.001 |
| Dilatation before vs. after deployment [n] | 2 / 5 (7% / 16%) | 15 / 8 (47% / 25%) | <.001 |
ELVO, emergent large vessel occlusion; IQR, Interquartile range; TIA, transient ischemic attack; CHD, coronary heart disease; MCA, middle cerebral artery; ICA, internal carotid artery; mRS, modified Rankin scale; NIHSS, national institutes of health stroke scale.
Table 2.
Outcome of all patients.
| non-ELVO group (n=31) | ELVO group (n=32) | p-value | |
| Primary outcome | |||
| Technical success* [n] | 31 (100%) | 32 (100%) | |
| Reperfusion success** [n] | - | 30 (94%) | |
| Periinterventional complications (dissection, SAH, intracerebral hemorrhage (PH2), and stent -thrombosis) [n] | 0 (0%) | 5 (16%) | .022 |
|
0 (0%) | 2 (6%) | .157 |
|
0 (0%) | 0 (0%) | |
|
0 (0%) | 2 (6%) | .157 |
|
0 (0%) | 2 (6%) | .157 |
| Secondary outcome | |||
| Neurological improvement [n] | 13 (42%) | 16 (50%) | .521 |
| Neurological deterioration[n] | 2 (6%) | 7 (22%) | .041 |
| Death (in-hospital) [n] | 0 (0%) | 5 (16%) | .022 |
| mRS at discharge [median] | 2 (IQR, 1-3) | 4 (IQR, 2-5) | .02 |
| mRS 0-2 at discharge [n] | 17 (55%) | 10 (31%) | .059 |
ELVO,emergent large vessel occlusion; PH2, parenchymal hemorrhage type 2 according to the ECASS classification; mRS, modified Rankin scale; IQR, Interquartile range. *Technical success defined as a residual stenosis of <50%; **Reperfusion success defined as complete or almost complete reperfusion (mTICI ≥2b).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



