Submitted:
18 November 2025
Posted:
19 November 2025
Read the latest preprint version here
Abstract
This article introduces the TrialUs Foundation, an innovative research ecosystem dedicated to generating rigorous evidence on everyday health and wellbeing practices. The platform enables individuals and communities to co-create large-scale randomised trials conducted outside traditional clinical settings. TrialUs™ operationalises co-creation as a structured scientific approach, supported by adaptive trial designs, evidence-based frameworks, and integrated digital technologies.
Keywords:
citizen science
; nutrition
; wellness
; fitness
; sleep
; community engagement
Every day, we make choices that shape our health and well-being: what to eat, when to rest, how to move. From best-selling books to podcasts and influencers, we are bombarded with conflicting and contradictory advice. Much of it rests on anecdote, observational studies, or small-scale, unrepresentative trials, often sensationalized in mainstream media or distorted through social media. In an increasing counter-science culture, fragments of partial truth can spread rapidly, amplifying uncertainty and feeding science sceptics. Commercial interests blur the lines further, with influencers weaving promotional material into content, making it harder to identify than traditional advertising. Similarly, AI chatbots and large language models are fast becoming the ‘go-to’ for health and medical advice but can obscure the origins of their guidance, which may stem from commercial or poorly informed sources.
Even when high-quality evidence exists, it often arises from trials conducted in controlled settings far removed from everyday life. As Milio (1976) observed, information alone rarely changes behaviour—people act within limits of time, context, and capacity. This persistent gap between knowing and doing reveals the limitations of conventional health research and education: our evidence often fails to reflect lived experience.
The gap in our understanding of the health benefits of everyday practices can be explained by both the focus and approach that dominate established research. Historically, research has focused primarily on disease treatment rather than prevention or lifestyle (Jones, 2012). Treatment interventions align more directly with clinical endpoints, pharmaceutical development, and established funding streams, whereas prevention trials require longer follow-up, larger populations, and yield less immediate commercial or policy reward. As a result, global health research investment and trial activity remain disproportionately weighted toward curative rather than preventive approaches (Hategeka et al., 2022). Moreover, the underrepresentation of women and ethnic minorities in health and medical research further limits the generalisability of existing evidence and constrains our understanding of how lifestyle interventions may impact diverse populations.
Trials that are conducted (both for treatment and prevention) tend to take a “Mode 1” approach, whereby science produces rigorous knowledge under controlled conditions but abstracts from real-world complexity (Gibbons et al., 2003; Messiha, 2021). Mode 2 embeds inquiry in context, valuing relevance and co-creation (IBID; Messiha, 2021; Messiha et al., 2025). Yet the gap between theory and practice persists. Further, a third way—Mode 3 science—combines the analytical rigour of Mode 1 with the participatory ethos of Mode 2 (IBID). It is science with people: inclusive, adaptive, and grounded in real-world settings. TrialUs exemplifies this evolution, moving research from institution to community, from prescription to participation.
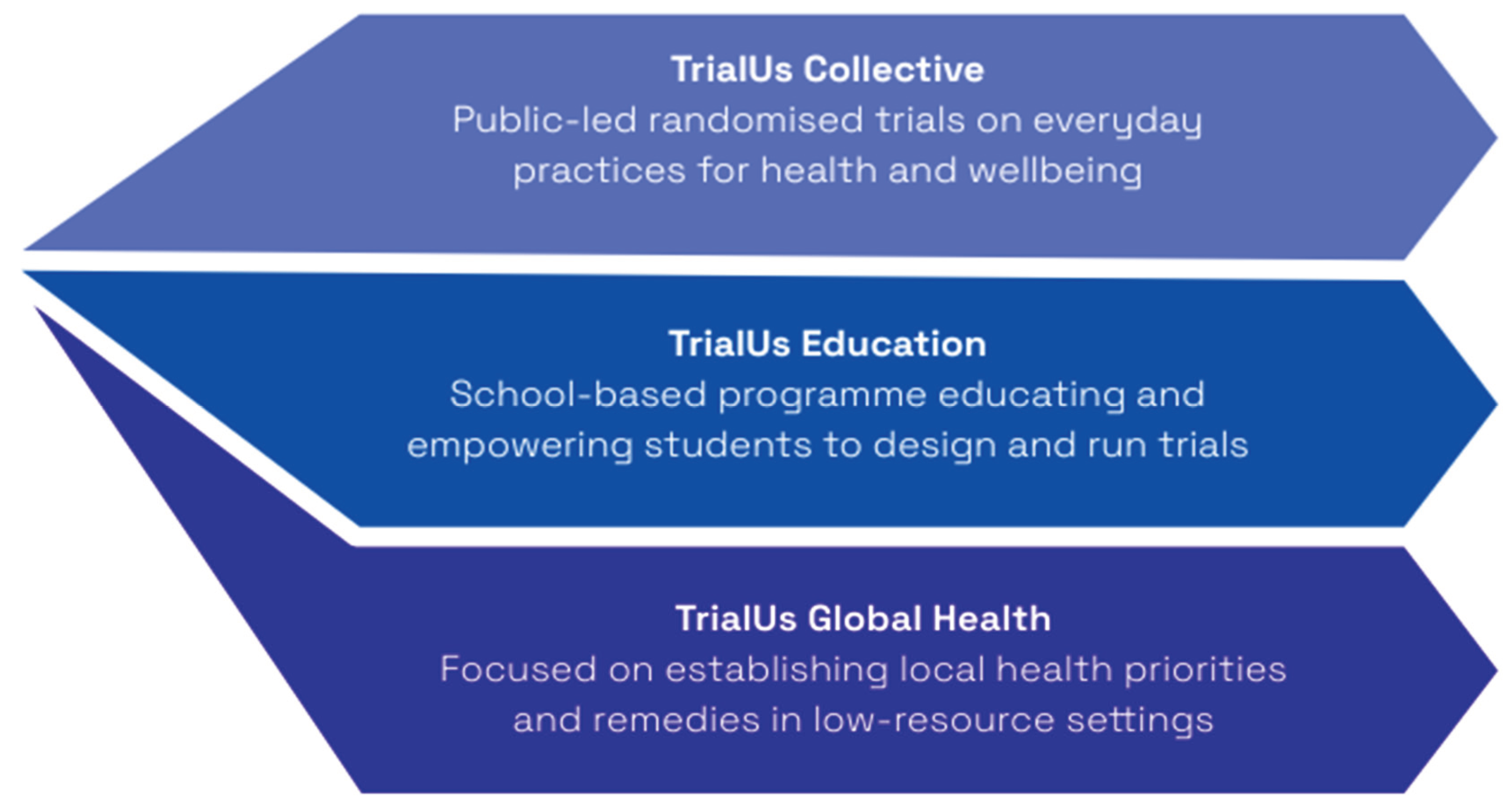
TrialUs democratizes the research process, making evidence-generational access and transparent to all communities. TrialUs functions in three domains: TrialUs Collective, TrialUs Education, and TrialUs Global Health, enabling communities, young people and global health practitioners to co-create and test ideas that matter to them (Figure 1). Artificial intelligence (AI) can accelerate co-creation and intervention development by facilitating translation, adaptive design, and automated data analysis.
At its core, TrialUs rests on a simple premise: the methods of science can and should belong to everyone. Communities, schools, and individuals can co-create randomised trials to test everyday practices, generating credible and meaningful evidence shaped by those who use it.
TrialUs Collective challenges the prevailing assumption that randomised controlled trials (RCTs), the methodological cornerstone of clinical research and the gold standard for generating unbiased, high-quality evidence should remain confined to clinical settings. Although RCTs have historically concentrated on curative and disease-oriented interventions, their intrinsic capacity to minimise bias (Guyatt et al., 2008) renders them equally suitable for evaluating everyday health and wellbeing practices with substantial population-level relevance. Despite this potential, the broader application of RCTs to behavioural and lifestyle interventions has been constrained by perceived methodological complexity, an overemphasis on mechanistic explanations, and the absence of enabling public infrastructure. TrialUs addresses these limitations through pragmatic, low-risk experimental designs that retain scientific rigour while expanding accessibility. Guided by expert oversight yet driven by community curiosity, it facilitates the continuous aggregation of public priorities and the coordinated design and implementation of large-scale trials assessing interventions of greatest collective interest.
TrialUs Education develops pedagogies to enable students to design, conduct and interpret their own studies, potentially contributing to decision-making affecting their health and well-being in their everyday lives. With the rise in counter-science sentiment and aggression, young people need to be equipped with skills to critically assess and interpret data, not only to make informed health decisions, but also discern misinformation and meaningfully contribute in democratic society. Through its innovative pedagogy, TrialUs bridges data literacy with rights education creating a transformative learning environment that empowers children as knowledge-creators and advocates for their own health, but also as rights-holders and global citizens in an increasingly polarized world.
TrialUs Global Health focuses on low-resource settings, where evidence gaps are the widest and the need for more inclusive and concrete pathways to achieving equity in the ownership of and participation in health research are most needed. Alongside chronic underinvestment in health research in low- and middle-income countries (LMICs), Global Health research agendas primarily reflect the priorities of funders and researchers from the Global North. In addition, structural barriers to LMIC researchers’ opportunities to access funding, training and resources have further impeded progress in sustainably establishing locally driven research. TrialUs Global Health will challenge these obstacles by providing tailorable tools to enable locally owned, Community-Based Participatory Research across different LMIC contexts. Starting with co-conceptualization of a ‘living’ research agenda, TrialUs Global Health will embody community priorities and lived realities in real-time. Studies on low-risk, everyday habits will be established through shared decision-making at each stage of the research process, from culturally appropriate data collection methods to the dissemination of context-specific, tangible research outputs. Expanding access, however, raises ethical challenges: ensuring fairness, reciprocity, and respect for local researchers and participants alike. As Cheah and Parker (2025) note, advancing health equity requires engaging deeply with the social and structural factors shaping participation and benefit.
Across its platforms, TrialUs connects community-led initiatives with formal research institutions. Academics provide mentorship and oversight to ensure studies are rigorous, ethical, and publishable, while community insights enrich theory and practice. Each study begins with co-creation, identifying the question, defining outcomes, and shaping interventions (Vargas et al., 2022). Adaptive trials evolve as new data emerge, creating a living evidence base. Technology underpins this process: wearables, mobile applications, and AI-powered analytics enable rapid data collection and remote participation. These tools not only accelerate iterative feedback and adaptive intervention design but also allow stakeholders to engage continuously, translating real-world experiences into actionable insights over time due to the excellent knowledge distillation capabilities.
AI is central to TrialUs’ democratic ethos, breaking down technical barriers and enabling meaningful, equitable stakeholder engagement. Translation tools, adaptive designs, and automated analysis can simplify complex processes, while a researcher directory connects local investigators with expert mentors, fostering collaboration and capacity building. Co-created online spaces empower communities to direct inquiry - and for young people, AI makes scientific methods tangible and engaging, transforming curiosity into actionable evidence that drives co-created interventions.
Despite global calls to enhance openness and collaboration among the “Quadruple Helix” actors - government, academia, industry, and civil society, scientific knowledge production remains largely closed, fragmented, and institutionally siloed (Mačiulienė et al., 2022). TrialUs represents a paradigm shift in the organisation of health and wellbeing research, reconceptualising it as a process conducted with people rather than for them. By combining open protocols, transparent dissemination of results, and structured community participation, TrialUs preserves scientific integrity while expanding accessibility and inclusivity. The platform provides a practical mechanism for systemic reform, embedding public collaboration within rigorous methodological and ethical frameworks. Although the ethical, technical, and regulatory challenges are considerable, TrialUs is designed to evolve iteratively as it navigates these complexities. Notwithstanding these challenges, it offers a credible and scalable model for producing high-quality, transparent evidence, an alternative to the fragmented and commercially influenced information that currently dominates the health and wellbeing landscape.
References
- Cheah, P.Y. and Parker, M., 2025. How should health researchers advance health equity?. Trends in Microbiology.
- Gibbons, M., 2003. A new mode of knowledge production. In Economic geography of higher education (pp. 243-257). Routledge.
- Guyatt G H, Oxman A D, Vist G E, Kunz R, Falck-Ytter Y, Alonso-Coello P et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations BMJ 2008; 336:924. [CrossRef]
- Hategeka C, Adu P, Desloge A, Marten R, Shao R, Tian M, et al. (2022) Implementation research on noncommunicable disease prevention and control interventions in low- and middle-income countries: A systematic review. PLoS Med 19(7): e1004055. [CrossRef]
- Jones, A. C., & Geneau, R. (2012). Assessing research activity on priority interventions for non-communicable disease prevention in low- and middle-income countries: a bibliometric analysis. Global Health Action, 5(1). [CrossRef]
- Mačiulienė, M., 2022. Beyond open access: conceptualizing open science for knowledge co-creation. Frontiers in communication, 7, p.907745. [CrossRef]
- Messiha, K. (2021). D1.1 - ESR1 Preliminary Synthesis. Zenodo. [CrossRef]
- Messiha, K., Altenburg, T.M., Giné-Garriga, M., Chastin, S. and Chinapaw, M.J., 2025. Enriching the existing knowledge about co-creation: identifying dimensions of co-creation using explicit theory in various research fields. Minerva, pp.1-24. [CrossRef]
- Milio, N., 1976. A framework for prevention: changing health-damaging to health-generating life patterns. American Journal of Public Health, 66(5), pp.435-439. [CrossRef]
- Vargas, C., Whelan, J., Brimblecombe, J. and Allendera, S., 2022. Co-creation, co-design and co-production for public health: a perspective on definitions and distinctions. Public health research & practice, 32(2). [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



